
Abstract
Osteochondral defects are difficult to treat because the articular cartilage and the subchondral bone have dissimilar characteristics and abilities to regenerate. Bioinspired scaffolds are designed to mimic structural and biological cues of the native osteochondral unit, supporting both cartilaginous and subchondral bone repair and the integration of the newly formed osteochondral matrix with the surrounding tissues. The aim of this review is to outline fundamental requirements and strategies for the development of biomimetic scaffolds reproducing the unique and multifaceted anatomical structure of the osteochondral unit. Recent progress in preclinical animal studies using bilayer and multilayer scaffolds, together with continuous gradient scaffolds will be discussed and placed in a translational perspective with data emerging from their clinical application to treat osteochondral defects in patients.
Introduction
O
Biomimetic scaffolds are engineered to reflect anatomical and physiological hierarchical structures.9–14 In theory, this aim can be achieved by a defined structure or chemical composition of a material. For osteochondral repair to occur, highly specialized scaffolds mimicking the hierarchical anatomical architecture of the natural osteochondral unit are needed. 14 While classically biphasic materials consisting of a single cartilage and bone part have been described, it is now clear that many other anatomical aspects of these both tissues combined in the osteochondral unit need to be reproduced.
The aim of this review is to outline fundamental requirements and strategies for the development of biomimetic scaffolds reproducing the unique and multifaceted anatomical structure of the osteochondral unit. Recent progress in preclinical animal studies using bilayer and multilayer scaffolds, together with continuous gradient scaffolds will be discussed and placed in a translational perspective with data emerging from their clinical application to treat osteochondral defects in patients.
Clinical Aspects of Osteochondral Repair
By definition, osteochondral defects disrupt the integrity of both the articular cartilage and the subchondral bone, in contrast to chondral defects, where the subchondral bone is not damaged (partial-thickness), or merely exposed (full-thickness) (Fig. 1). Pain is often the key clinical symptom, together with an impaired joint function and quality of life. Moreover, untreated osteochondral lesions can lead to OA 15 resulting from the joint incongruence and the abnormal biomechanical loading patterns of the adjacent articular cartilage. 16 From a clinicopathological standpoint, the underlying problem causing an osteochondral defect is of high importance. 8 The subchondral bone lesions that are the hallmark of osteochondral defects mainly occur in the course of diseases of the subchondral bone such as osteochondritis dissecans (OCD) or as a result of osteochondral fractures (Fig. 2).17,18 As these defects are well defined and often deep, they represent the best indications to implant bioinspired osteochondral scaffolds. In general, the paramount goal is to reconstruct an anatomical joint surface, resembling as closely as possible the normal structure of the osteochondral unit. Currently, small osteochondral lesions may be treated using osteochondral transplants, while the sandwich technique (comprising the grafting of compacted autologous cancellous bone into the subchondral bone defect together with the implantation of articular chondrocytes (ACI) in a three-dimensional bioresorbable matrix) is an excellent option for large defects.19,20 Ideally, a single type of bioinspired osteochondral scaffold would be applicable to both small and large defects, although fixation requirements may differ: small osteochondral lesions could be treated with a press-fit approach, while larger lesions might necessitate an additional fixation.
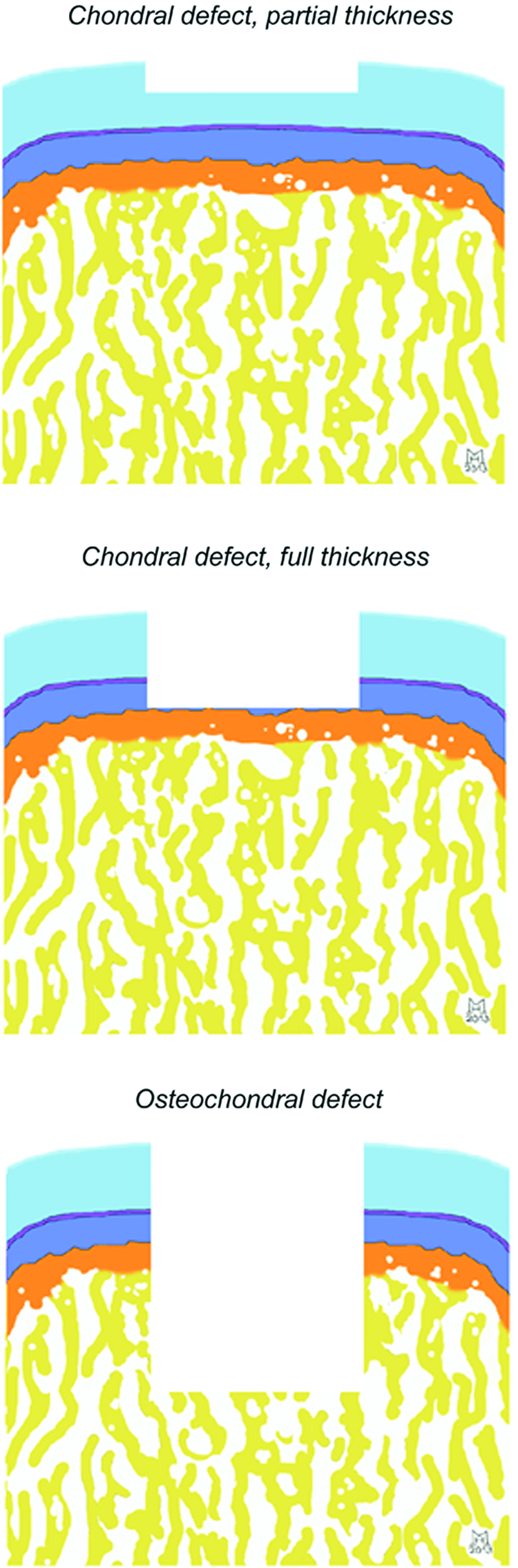
Classification of articular cartilage defects. In chondral defects, the subchondral bone is not damaged (partial-thickness), or only exposed (full-thickness). Osteochondral defects, in contrast, disrupt the integrity of both the articular cartilage and the subchondral bone. Color images available online at www.liebertpub.com/tea

Macroscopic view of an osteochondral defect resulting from osteochondritis dissecans (OCD) in a 30-year-old man. The osteochondral defect (arrow) is located in the lateral aspect of the medial femoral condyle, a typical location. The circular articular cartilage defect has a diameter of about 35 mm. The subchondral lesion reaches about 20 mm deep into the subarticular spongiosa. Color images available online at www.liebertpub.com/tea
Applied Anatomy of the Osteochondral Unit
The osteochondral unit is composed of the articular cartilage and the underlying subchondral bone. 8 This vital region has a multifaceted structure, 21 connecting the articular cartilage through the calcified cartilage with the subchondral bone.
Articular cartilage
Articular cartilage is a highly specialized connective tissue that provides joints with a low friction environment. Lack of vascularization, low cellularity, and the limited metabolic activity of mature chondrocytes, which are the unique cellular component resident within cartilage, are key features of this tissue. 22 Type-II collagen is the main type of collagen present. 23 Proteoglycans are another fundamental component of the cartilage extracellular matrix (ECM). Because of their negative charges, proteoglycans are able to retain water molecules (65–80% of wet weight) within cartilage. This allows the load-dependent deformation of the cartilage. 24
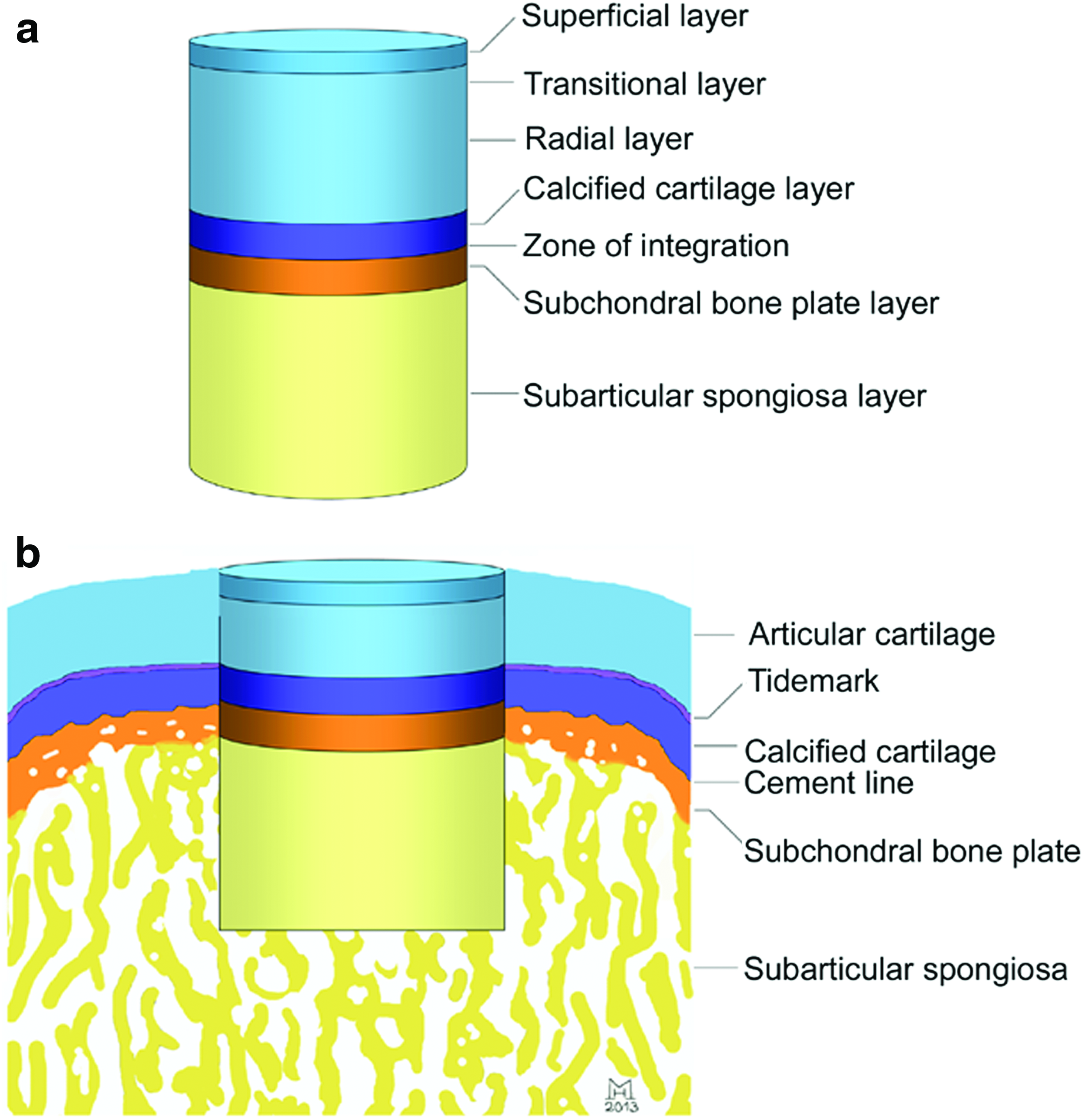
Articular cartilage has a highly anisotropic architecture, being composed of multiple layers that differ in terms of cell and collagen fibril orientation. The superficial zone contains small flattened chondrocytes and collagen fibrils tangentially oriented to the articular surface that provide resistance to compressive loads and the gliding surface. The transition zone encloses rounded chondrocytes that secrete type-II collagen and aggrecan and includes obliquely oriented collagen fibrils. The deep radial zone of articular cartilage presents chondrocytes arranged in columns and collagen fibrils perpendicular to the articular surface and in parallel to each other.24,25 The layer of calcified cartilage 26 connects the articular cartilage with the subchondral bone plate and is about 20–250 μm thick. 27 It is separated from the articular cartilage by the tidemark, a basophilic line on histological sections.28,29 The calcified cartilage contains also type-X collagen. Type-II collagen fibrils extend from the noncalcified articular cartilage into the calcified cartilage. As organization of the ECM is fundamental to grant functionality of articular cartilage, one of the main challenges for cartilage tissue engineering remains the high fidelity reproduction of these layers with proper orientation of collagen fibers. 4
Subchondral bone plate and subarticular spongiosa
The subchondral bone is composed of the subchondral bone plate and the subarticular spongiosa. Cancellous bone plates join together in the subchondral bone plate to enclose few narrow intervening spaces. While denser than the subarticular spongiosa, the subchondral bone plate is relatively thin in normal human subchondral bone. 30 It is broader and denser in osteoarthritic joints. The intervening spaces are gradually enlarged and become elongated in a direction parallel to the diaphysis in deeper regions of the subchondral bone, forming the subarticular spongiosa. 8 Thus, the subchondral bone plate has a low total porosity, while the porosity of the subarticular spongiosa is much larger.
Connection of the articular cartilage with the subchondral bone
The junction of the calcified cartilage with the subchondral bone is called cement line. 8 This connection is of major importance for maintaining the osteochondral integration. Here, no collagen fibrils extend from the calcified cartilage (containing mainly type-II and -X collagen) into the subchondral bone plate (containing mainly type-I collagen). This junction is also a site of active remodeling. 8 Of note, a surprisingly high number of arteries, veins, and nerves send minute branches through canals in the subchondral bone plate into the calcified cartilage. Nutrients can therefore reach chondrocytes in the calcified and articular cartilage. 31 Thus, the osteochondral connection is not impermeable, but a structural and functional unit allowing both mechanical and biochemical interactions. 8
Requirements of Biomimetic Scaffolds for Osteochondral Repair
Biomimetic scaffolds need to provide the multifaceted signals in a spatial and temporal pattern allowing the regeneration of the entire osteochondral unit. The presence of the articular cartilage and the subchondral bone as the two major tissues commands the design of biphasic, monolithic scaffolds. Here, the cartilage part supports chondrogenesis, while the bone part serves as a template for osteogenesis. Although such scaffolds diminish limitations of homogeneous single phase scaffolds that lack the structure required to regenerate the entire osteochondral unit, 32 they do not resemble its complex structure, necessitating biomimetic scaffolds composed of multiple integrated layers corresponding to the different components of the osteochondral unit (Fig. 3). The design of a unique scaffold reflecting both the complexity of the osteochondral unit and satisfying all requirements is particularly challenging, since the subchondral bone and articular cartilage are characterized by distinct features of matrix composition and organization, vascularization, and metabolic requirements (Table 1). Interestingly, many of these needs have been individually addressed so far and even found entry into the clinics, for example by using bone substitutes to fill large bone defects and by applying bioresorbable matrices seeded with autologous chondrocytes in the case of ACI for large cartilage defects.19,33,34 In contrast, only case reports are available for the treatments of osteochondral defects.
Bioinspired design of osteochondral multiphasic scaffolds.
Requirements to restore the articular cartilage
Requirements for scaffolds solely aimed at restoring the articular cartilage have been the subject of excellent reviews.35–37 Toward the joint surface, a smooth gliding part needs to protect the opposing cartilage, to allow for gliding of the joint and to protect to some extent the cartilaginous repair tissue that is developing within the scaffold. Next, a layer resembling more or less the transitional zone may follow. Then, a layer mimicking the columnar orientation of the radial zone with scaffold fibers that are aligned rectangular to the articular surface is needed. Here, it remains to be seen whether the commonly used type-I collagen scaffolds could not be further improved, for example by incorporating type-II collagen. 38 Very recent studies have demonstrated that a distinct superficial layer in engineered cartilage can be generated applying oriented nanofibrous scaffolds 39 or hydrodynamic stimulation mimicking the flow motion between the articulating surfaces in the synovial joint. 40 Moreover, Thorpe et al. have reported that the radial confinement of agarose hydrogel-based scaffolds and the simultaneous application of a dynamic compressive load generate an oxygen gradient and increase strains across the top of the construct, resulting in a depth-dependent zonal variation in both the biochemical composition and compressive properties of the engineered tissue. 41
Requirements to restore the calcified cartilage
This part of the scaffold should allow mineralization. Specific material compositions can direct bone marrow-derived mesenchymal stem cells (BMSC) into distinct types of chondrocytes 42 and layer-by-layer organization of these materials results in a gradient of type-II and -X collagen that translates into an increased compressive modulus from the superficial to bottom layer. 43 The group of Rita Kandel mimicked the zonal organization of the osteochondral unit in biphasic constructs composed of cartilaginous tissue anchored to the top surface of porous calcium polyphosphate with a calcified interface as a bone substitute in vitro. 44 Of note, the shear properties of the cartilage–subchondral bone interface were enhanced as a result of the presence of a calcified cartilage layer, highlighting the importance of such a mineralized zone.
Requirements to restore the subchondral bone–cartilage interphase
The union between the chondral and subchondral bone layers needs to be stable enough to withstand the shear stress related to joint movement, to allow optimal load bearing 45 and to prevent a possible delamination of the cartilage layer that would be deleterious in vivo.46,47 The design of heterogeneous scaffolds composed of a single material displaying differential growth factor enrichment, porosity, or composition in the two integrated layers, or the generation of scaffolds with continuous interfaces may help to overcome this limitation.48–51 It has also been suggested that the bilayer interface should be capable of preventing any upward migration of the subchondral bone plate 52 into the chondral layer. 53 The insertion of a mineralized compact and dense phase 54 or the use of a functional barrier enriched with anti-angiogenic growth factors 55 may represent viable strategies to limit the advancement of the subchondral bone plate.
Requirements to restore the subchondral bone
Fundamental requirements such as the de novo formation of the subchondral bone plate and subarticular spongiosa, the integration without formation of a sclerotic rim or subchondral bone cysts are of key importance and need to be met by the scaffold. Particularly for large subchondral bone defects, implant vascularization plays a crucial role to achieve this goal.56–59 The delivery of angiogenic or growth factors may represent a valid approach, 60 even though their activity needs to be confined to the subchondral bone layer to avoid hypertrophy and endochondral ossification in the chondral layer. 61 Recently, magnetic biohybrid devices composed of bioactive factors conjugated to magnetic nanoparticles have been suggested to obtain a targeted delivery, 62 a strategy that could be exploited to improve subchondral bone neo-vascularization.
Important structural parameters to grant bone tissue ingrowth and vascularization include porosity, pore size, and interconnectivity.63–66 These features need to be balanced with other key parameters, such as mechanical properties, material composition, and degradation rate, which need to be compatible with functional requirements of the implant.67–69 Over time, scaffold parameters are modified by the healing process and scaffold pores are filled with newly formed bone matrix that integrates the scaffold with the subarticular spongiosa. 70
A variety of both natural and synthetic materials have been studied in animal models for subchondral bone repair.45,71–73 In the clinical situation, however, the critical requirement of subchondral bone substitutes to induce and support osteogenesis64,71,74–76 is often not fulfilled.74,75 Therefore, a key challenge that remains yet to be solved is the elucidation of the effect of distinct scaffold parameters on subchondral bone and articular cartilage repair.
Although great attention has been paid to the zonal organization of articular cartilage, the different components of the subchondral bone are often neglected when designing scaffolds. Indeed, bone scaffolds are usually characterized by an isotropic macroporous structure mimicking the architecture of trabecular bone. Very recently, Despang et al. 77 have designed an anisotropic bone scaffold with parallel-aligned pores mimicking the microstructure of cortical bone. A similar bioinspired approach could be applied to design multilayer scaffolds resembling the structure of the subchondral bone. Keeping the structure of the subchondral bone in mind, a layer mimicking the laminated sheets of the subchondral bone plate (with a high bone volume) that also seals the subarticular spongiosa from the synovial fluid and thus may prevent cyst formation78,79 is mandatory. A second layer resembling the porous structure of the subarticular spongiosa, perhaps with trabeculae aligned in parallel to the diaphysis, is additionally needed.
Integration of the scaffold with the surrounding osteochondral tissue
The lateral integration of the implant with the surrounding osteochondral tissue continues to be difficult.80,81 Several preclinical studies have reported an efficient bonding of the subchondral bone layer, but complete integration of the chondral layer to the surrounding articular cartilage remains a challenging goal.82,83
Bioinspired Strategies for Osteochondral Repair in Preclinical Models
The increasing number of preclinical studies evaluating the in vivo performances of osteochondral scaffolds attests to the growing interest in regenerating the entire osteochondral unit, as widely reviewed.32,45,72,84–86 In general, such bioinspired osteochondral scaffolds are composite structures composed either of synthetic or natural materials or representing combinations thereof (Tables 2 and 3). This section first gives a general overview of the principles of translational animal models to study osteochondral repair. Next, the results of studies focusing on bioinspired bilayer scaffolds are given (Table 2). Considering the complexity of the osteochondral unit, multilayer scaffolds (Table 3) and continuous gradient scaffolds representing a step forward toward the design of bioinspired osteochondral scaffolds are also discussed.
BMSC, bone marrow-derived mesenchymal stem cells; BMP, bone morphogenetic protein; CT, computed tomography; GAG, glycosaminoglycans, Hyal, hyaluronic acid; HA, hydroxyapatite; OPF, oligo(polyethylene-glycol)fumarate; PCL, polycaprolactone; PEG, polyethylene glycol; PGA, polyglycolic acid; PLA, polylactic acid; PLGA, polylactic-co-glycolic acid, TGF, transforming growth factor; TCP, tricalcium phosphate.
ASC, adipose-derived stem cells; ECM, extracellular matrix; PRP, platelet-rich plasma.
General translational aspects of animal models for osteochondral repair
Small animal models (e.g., rabbits) are primarily used to translate promising in vitro developments. 87 Next, promising approaches are tested in larger animals (e.g., mini-pigs, goat, or sheep). 88 Differences in the composition of the osteochondral unit have to be kept in mind, such as the cartilage thickness and its relation to the thickness of the subchondral bone plate. 89 Observation times that are long enough to account for possible pathological events such as the degeneration of the cartilaginous repair tissue, the advancement of the subchondral bone plate, and the formation of intralesional osteophytes are needed.52,90 A thorough analysis of cartilage repair is mandatory, including semi-quantitative macroscopic scoring, 91 molecular biology, 92 biochemical, 93 histological, and immunohistochemical 94 analyses. The subchondral bone is depicted and quantified by micro-computed tomography (micro-CT).38,90 Biomechanical testing reveals whether the restored osteochondral unit is similar to the normal situation.67,95 Although skeletally immature animals reproduce the problem of children and adolescents suffering from OCD, skeletally mature animals are preferred in preclinical studies to reflect the clinical problem of osteochondral repair in adults. 87 Interestingly, possible complications may occur in skeletally immature animals, for example a subchondral depression of the implant due to joint enlargement. 96
Bioinspired biphasic scaffolds
The most common strategy tested so far in preclinical models mimics the osteochondral structure through biphasic materials combining synthetic or natural hydrogels with biomaterials used as bone substitute, as highlighted by the list of preclinical studies reported in Table 2.47–49,82,83,92,96–121 Natural hydrogels have been the most used materials to generate the chondral layer of preclinically tested biphasic scaffolds. In particular, natural materials such as fibrin, hyaluronic acid (Hyal), collagen, chitosan, chondrotin sulphate, alginate, and their combinations have been applied in a wide range of osteochondral scaffolds.47,83,92,97,100,101,103,107,108,110,112,114–117,121 One of the main advantages of natural hydrogels is their enhanced biological interaction with cells compared with synthetic materials. This feature makes natural hydrogels very appealing candidates for the fabrication of biphasic osteochondral scaffolds although their synthesis and their final properties are less controllable compared to synthetic materials. From a clinical standpoint, an initial high mechanical strength of the articular cartilage compartment might not be immediately needed, as demonstrated by the clinical success of ACI to cover very large defects. 122 Here, bioresorbable soft matrices are commonly used, indicating that in the absence of high loads (as achieved by postoperative nonweight bearing), the chondral layer does not need to have a high mechanical strength. 34
Polymeric materials such as polylactic acid, polyglycolic acid (PGA), polylactic-co-glycolic acid (PLGA), and polycaprolactone have been used to generate both the chondral and the subchondral bone layer of biphasic osteochondral scaffolds. The advantage of using synthetic polymers consists in the possibility to up-scale the scaffold manufacturing at the industrial level and in the high control over their synthetic parameters. For example, different porosities in the two layers can be obtained by using different-sized porogens during the synthetic process, thus generating an integrated PLGA bilayer scaffold. 49 The effect of the differential porosity in the chondral and subchondral bone layer has been also investigated in vivo by Duan et al. 120 using PLGA biphasic scaffolds. Chondral and subchondral bone phases characterized by 100–200 μm and 300–450 μm pores, respectively, led to superior osteochondral repair compared with other combinations of porosity. Thus, the use of highly controllable polymers can be exploited not only for the production of novel scaffolds, but also to test parameters that affect the repair process, thus gaining better insights for a rational scaffold design.
More frequently, biocompatible and degradable ceramic materials, such as hydroxyapatite (HA) and/or tricalcium phosphate (TCP), are used for the subchondral bone phase. These materials are able to support bone ingrowth into the implant, leading in most of the cases to satisfying regeneration of the subchondral bone.47,103,104,107–109 Metallic materials for subchondral bone reconstruction have also been proposed, among which porous titanium and tantalum that have been combined with synthetic hydrogels for chondral repair.98,105,106 However, issues based on their lack of degradation, which hamper the substitution of the scaffold with native bone matrix and may thus interfere with the regeneration of the osteochondral unit, have to be kept in mind. Indeed, the degradation rate of materials used for both chondral and subchondral bone layer a key parameter in the healing process and it should be compatible with the regeneration rate of the corresponding tissue to prevent inefficient osteochondral repair. Also, being the stable union of chondral and subchondral bone layers a major challenge when the scaffold is subjected to mechanical stress related to joint function, suturing, press-fitting, or simple apposition of the chondral layer upon the bone layer that are reported in most of the analyzed preclinical studies, still appear a suboptimal solution, and major efforts need to focus on the development of new strategies to face this limitation.
Among the biphasic scaffolds, Chondromimetic™ and Trufit™ are currently clinically used to treat osteochondral defects. The first one combines type-I collagen and chondroitin-6-sulfate for the chondral phase and calcium phosphate for the subchondral bone phase, whereas Trufit™ is a bilayered porous scaffold containing PLGA and PGA fibers in the chondral phase and calcium sulphate in the subchondral bone phase. These biphasic implants have been recently compared in a goat model. 117 After 6 months, a significantly higher histological score and lower incidence of subchondral bone cysts were seen for the type-I collagen/GAG-based biphasic scaffold, thus supporting the concept that natural composites better support osteochondral repair. Rapid translation to the clinical situation of these results in well-designed studies over a long period of time will determine the optimal strategy.
Incorporation of growth factors into biphasic scaffolds
The spatially defined incorporation of growth factors represents a bioinspired strategy that provides the scaffold with fundamental cues to induce progenitor cells toward chondro- or osteogenesis. Only few studies have investigated the effect of biphasic scaffold enrichment with growth factors on the in vivo osteochondral regenerative process. Holland et al. 48 have shown that the incorporation of transforming growth factor (TGF)-β1-loaded microparticles in the chondral phase of a oligo(poly(ethylene glycol)fumarate) bilayer scaffold promotes the formation of a continuous cartilage layer yielding a superior histological score compared with TGF-β1-free scaffolds. Recently, an alginate matrix (representing the chondral phase of a bilayer scaffold), has been combined with PLGA microspheres loaded with either TGF-β1 or BMP-2 and used to treat osteochondral defects in the rabbit model. 114 A pilot study (three animals per experimental group) showed better histological repair at 24 weeks when TGF-β1 and BMP-2 implants were applied. The differential inclusion of growth factors in the two layers has been proposed by Re'em et al. who bound alginate to TGF-β1 and BMP-4 in the chondral and subchondral bone layer, respectively and implanted the scaffold into lapine subchondral defects. 116 Although no histological scoring and no control group with a growth factor-free implant was included, this study may serve as a starting point to further evaluate the simultaneous incorporation of different growth factors for osteochondral repair.
Bioinspired multiphasic scaffolds
Compared to biphasic scaffolds, multiphasic scaffolds have been less studied in vivo so far, as reported in Table 3.54,123–126 A bioinspired approach was applied by Da et al. 54 who designed a multiphasic scaffold with the calcified cartilage zone mimicked by a compact phase fabricated from PLGA/β-TCP. The chondral phase was derived from bovine decellularized articular cartilage matrix with an oriented structure designed to resemble the vertical orientation of the fibers in the deep zone. The subchondral bone phase consisted in a PLGA/β-TCP skeleton wrapped in type-I collagen obtained by computer-controlled rapid prototyping technique. Interestingly, the presence of the compact layer significantly increased the biomechanical properties of the multiphasic scaffold in terms of tensile and shear strength. Further, when used to treat rabbit osteochondral defects and compared to the compact layer-free scaffold group, the triphasic scaffold led to improved macroscopic and histological scores with neo-formed cartilaginous and bone tissue integrating with the host tissues. However, before moving toward a clinical application, it will be fundamental to reproduce these impressive results in a large animal model more reflective of the clinical situation.
Tampieri et al. developed a three-layered scaffold composed of type-I collagen and nanostructured HA that supported cartilage and bone formation.127,128 This osteochondral scaffold is composed of a type-I collagen layer with a smooth surface for cartilaginous repair, an intermediate layer based on a combination of type-I collagen and HA (60:40) reflecting the calcified zone, and a lower layer composed of a mineralized blend of type-I collagen and HA (30:70) to replicate the subchondral bone. The intermediate and lower layers were obtained by nucleating HA into self-assembling collagen fibers through a bioinspired synthetic process mimicking the natural ossification process. Remarkably, this triphasic scaffold (MaioRegen®) has been tested by Marcacci and co-workers in pilot studies in a sheep and horse model.123–125 Macroscopic, histological, and immunohistochemical observations, and high resolution X-rays showed that the multiphasic scaffold induced osteochondral repair with an ordered architecture. 124 Interestingly, the addition of cells did not significantly improve the repair process, indicating that the scaffold itself is able to support the intrinsic ability of progenitor cells recruited at the implant site to produce specific matrix.
Continuous gradient osteochondral scaffolds
Continuous gradient scaffolds are a principal alternative to bilayer and multilayer scaffolds, displaying intermediate features in terms of material composition and growth factors in the transitional region of the scaffold. These scaffolds may overcome the problem of inefficient binding between different layers. The group of Michael Detamore has obtained promising results with continuous gradient scaffolds. Here, an osteochondral scaffold with continuous opposing gradients of TGF-β1 and BMP-2 was generated using growth factor-loaded PLGA microspheres.129,130 This scaffold, with opposing gradients of microspheres encapsulating TGF-β1 or BMP-2 without or with HA nanoparticles, led to optimal rabbit osteochondral repair after 3 months compared to control groups, demonstrating that the simultaneous spatial patterning of bioactive signals and materials is advantageous compared with a single gradient of bioactive signals. 51
Cell-free versus cell-based approaches
Do additional autologous cells need to populate osteochondral scaffolds? Although some studies report no significant improvement when using cell-seeded scaffolds,92,99,107,124 most of the preclinical studies have reported a positive effect of transplanted cells in comparison to cell-free scaffolds.49,82,83,100,102,104,112,115,120 The effect of cells implantation is particularly evident when cells are precultured in the chondral layer to obtain in vitro engineered cartilaginous tissue prior to implantation, leading to improved cartilage repair in vivo.82,112,113 In particular, Miot et al. 112 demonstrated that the maturation state of in vitro engineered cartilaginous tissue obtained culturing articular chondrocytes into a hyaluronic acid mesh (HYAFF-11®) affects the healing outcomes, when implanted as chondral layer in association to HA/HYAFF-11 subchondral bone layer.
As the basis for implantation of autologous articular chondrocytes and BMSC is well established, it would be easy to seed either cell type into the cartilaginous scaffold part, either before or during implantation. Both articular chondrocytes and BMSCs seeded in the layers of biphasic scaffolds have been tested in rabbit and equine osteochondral defect models.115,131 Similarly, co-culture of osteoblasts and chondrocytes has been investigated both in vitro 132 and in vivo. 109 However, as the subchondral bone part will always be exposed to BMSC and osteoblasts, already existing osteoinductive scaffolds might omit the need for additionally implanted cells enabling subchondral bone repair. 133 Considerations about the need for cell transplantation should also take in account additional procedures related to cell harvesting, safety requirements, and the overall increase in costs, necessitating high-quality clinical studies to answer this important question.
Clinical Application of Bioinspired Osteochondral Scaffolds
Although several invigorating avenues are being followed in the field of in vitro and preclinical in vivo tissue engineering, no optimal strategy has been described that is clinically accepted. Here, only a few scaffolds for osteochondral regeneration are currently commercially available for clinical application to the best knowledge of the authors.
The biphasic scaffold Chondromimetic™ 117 is currently under clinical investigation (ClinicalTrials.gov identifier: NCT01209390) in a prospective postmarketing study to confirm the clinical efficacy and safety outcome of its application for the treatment of osteochondral defects over a 3 year postimplantation follow-up period.
The biphasic scaffold Trufit™ is tested in a prospective randomized, multicenter, clinical trial, evaluating its effectiveness for the treatment of single cartilage defects in the knee compared to the microfracture technique (ClinicalTrials.gov identifier: NCT01246635). First short-term results of Trufit are inconclusive. 75 For example, Barber et al. demonstrated by CT that no bone ingrowth, osteoconductivity, or integration with the adjacent subchondral bone occurred. 74 In contrast, a sclerotic rim often surrounded the lesion and subchondral cyst formation was frequent and recently confirmed in another study. 76 Unfavorable short-term magnetic resonance imaging (MRI) results have been reported, 75 although it has been suggested that the clinical outcome may improve over time.134,135 Nevertheless, the evidence for delayed subchondral incorporation of the implants warrants further long-term investigation.
MaioRegen®, an osteochondral biomimetic scaffold with a trilayered structure containing only type-I collagen in the chondral layer and a mixture of type-I collagen and HA combined in different ratios to mimic the tidemark zone (60:40) and the subchondral layer (30:70),123–125 was recently tested in a pilot study involving 28 patients with chondral and osteochondral lesions and sizes ranging from 1.5 to 6.0 cm2. 76 In another study, 27 patients affected by knee OCD (average defect size: 3.4±2.2 cm2) were treated. 136 Good clinical outcomes were seen at 2-year follow-up in both studies. Specifically, MRI evaluation revealed a complete filling of the cartilage defect and complete integration of the scaffold in most of the cases. Of note, the subchondral bone was never completely restored, and subchondral bone changes such as cysts and sclerosis were often present.76,136 This multilayer scaffold is currently under evaluation in a prospective, randomized, multicenter clinical trial (ClinicalTrials.gov identifier: NCT01282034) to compare its effectiveness with standard marrow stimulation techniques for the treatment of both chondral and osteochondral lesions.
Altogether, these clinical reports suggest that an insufficient integration with the subchondral bone and a limited overall restoration of this tissue are the major technical limitations of current scaffolds. Interestingly, this important finding is in contrast with the observations derived from the preclinical studies, where the subchondral bone part was reported to be well integrated with the native tissue. More research is therefore needed to elucidate the reasons for these differences between the human applications and the animal models and to build more knowledge to support better clinical decisions in the future. The development of novel bone scaffolds137,138 that permit an enhanced de novo subchondral bone formation is therefore of considerable importance to design bioinspired scaffolds with improved potential for osteochondral integration and repair.
Outlook
Innovative biofabrication techniques will be of great value to design scaffolds with a complex pattern mimicking the structural organization of the osteochondral unit. Computer-aided rapid prototyping techniques allow the fabrication of 3D scaffold with a highly reproducible architecture in terms of pore size, geometry, and interconnectivity. Material composition in the different layer of the scaffold can also be highly controlled through these techniques, generating compositional variation within a single scaffold. Further, as recently reported by Fedorovich et al. 139 these techniques can be exploited to achieve a controlled incorporation of different cell types in different layers of the construct, thus creating osteochondral grafts that can recapitulate the complex distribution of cells and matrix observed in native tissues. Also, the combination of rapid prototyping techniques with advanced high resolution imaging analysis, such as CT, enables the generation of biomimetic scaffolds on the basis of microanatomical data. Recently, bioprinting has been used to precisely deliver chondrocytes combined with polyethylene glycol (PEG) hydrogel into a cartilage defect created within an osteochondral plug, thus demonstrating the feasibility of in situ thermal inkjet-based cartilage bioprinting. 140 These results suggest that further advances in the field of biofabrication techniques could allow the design of complex bioinspired osteochondral scaffolds and possibly the development of novel treatments where the osteochondral defect could be treated by the in situ assembly of cell-laden biomaterials.
As indicated by the promising results obtained in preclinical studies, future avenues might also be achieved by combining bioactive molecules supporting bone and/or cartilage repair either through the use spatially controlled incorporation of specific growth factors in the different layers or through the generation of gradients of bioactive signals that can be sensed by resident cells.
From a clinical point of view, it will be important to address recently emerged problems of the subchondral bone such as the formation of intralesional osteophytes, the advancement of the subchondral bone plate, formation of subchondral bone cysts, or lack of integration with the adjacent subchondral bone. 6 Thus, continued monitoring through noninvasive imaging methods of cartilage and subchondral bone repair in patients treated with multiphasic implants that are currently in clinical use is vital to evaluate the long-term outcomes of each scaffold. Precise information on the physiological response to the different osteochondral constructs may help to understand which of these undesired events is more often associated with each treatment and possibly reduce their frequency through the improved design of novel scaffolds.
The successful application of biomimetic multiphasic scaffolds for osteochondral repair will continue to require a combined effort of orthopedic, clinical, and basic science investigators, among which are biomaterial scientists, cell, molecular, and developmental biologists, biochemists, biotechnologists, and biomechanical engineers. To bring such individuals together, it will be critical to supplement the promising preclinical and clinical accomplishments with the scientific rigor of well-designed long-term randomized controlled trials.
Footnotes
Disclosure statement
No competing financial interests exist for all authors.