
Abstract
On activation, platelets secrete an array of growth factors that contribute to bone regeneration. Combining platelet-rich plasma (PRP) with bone graft substitutes has the potential to reduce or replace the reliance on autografts. Lack of standardization and improper use may contribute to the conflicting outcomes reported within both preclinical and clinical investigations using PRP. This study investigates the effect of PRP dose on bone augmentation. Eighty critical-sized defects were created in the cancellous bone of the medial proximal tibia and the distal femur of 20 five-year-old female sheep. The defects were treated with three doses of an autologous thrombin-activated PRP combined with a biphasic calcium phosphate (BCP) or autograft and empty defects. Radiography, micro-computed tomography, histology, histomorphometry, and fluorochrome bone labels were examined at 4 weeks. The empty defects did not spontaneously heal. The highest dose of PRP treatment had a significantly greater micro-CT bone volume/total volume compared with the BCP alone (PRP: 30.6%±1.8%; BCP: 24.5%±0.1%). All doses of PRP treatment were significantly greater than the BCP alone for histomorphometric new bone area (PRP: 14.5%±1.3%; BCP: 9.7%±1.5%) and bone ingrowth depth (PRP: 2288±210 μm; BCP:1151±268 μm). From week 2 onward, PRP had a significant effect on the weekly bone ingrowth compared with BCP; however, autografts had the highest amount of weekly fluorescent bone labeling. PRP induces new bone formation with a dose-dependent response at 4 weeks when used with a BCP in sheep.
Introduction
B
The basic elements for bone tissue engineering are signaling molecules, cells, and matrices. 5 During normal hemostatic mechanisms, a fibrin network is formed and platelets are activated, establishing the hematoma. 6 On activation, platelets release a variety of signaling molecules that orchestrate bone healing.7,8 The basis of platelet-rich plasma (PRP) relies on the ability to concentrate and activate platelets, and to deliver a supra-physiologic concentration of the released growth factors to a defect site.
The separation of blood components for surgical application has a long history. The collection of fibrinogen to use as an intraoperative fibrin glue for topical hemostasis found applications in many clinical settings. 9 While the advantages of a hemostatic and adhesive fibrin glue are known, in 1994, Tayapongsak et al. 10 reported that the formation of the fibrin matrix also supported mandibular bone regeneration. The identification of platelet-released growth factors led to the development and use of PRP, initially reported in 1998 by Marx as beneficial for use in bone regeneration of mandibular defects. 11 This positive finding led to an increased interest and use of PRP within the oral and maxillofacial surgical fields.12–14 Since this early application during the 1990s, PRP has seen prolific use across an increasing variety of surgical fields, and it now includes applications ranging from soft tissue healing,15,16 cosmetic surgery,17,18 burns, 19 nervous tissue,20,21 and chronic skin ulcers. 22 In spite of the increasing use, contrasting outcomes,8,23,24 compounded with inconsistent terminology and descriptions,25,26 have hindered the progression of PRP use. The present study evaluated the efficacy of activated PRP combined with a biphasic calcium phosphate (BCP) to treat established critical-sized cancellous bone defects in older-aged sheep. Three PRP dosages were compared with a constant graft volume to provide insights into the effect of the PRP to graft ratio. In addition, to appreciate the role of platelets and other plasma constituents, platelet-poor plasma (PPP) combined with the BCP, and the BCP alone, were evaluated as reference groups. Iliac crest autograft and empty defects provided the positive and negative control groups. Overall, this study was undertaken to investigate the potential of PRP, and to provide a clearer indication for the surgical use of PRP to augment bone healing.
Materials and Methods
Surgery and PRP preparation
An a-priori power analysis (G*Power 3.1.3) was conducted to estimate the sample sizes (Table 1). All treatments were evenly spread across L/R femur and tibia; however, the treatment allocation was not randomized for animal welfare concerns regarding the total blood loss to produce PRP and autograft harvest quantity. This approach also ensured a balanced study design. Approval from the University of New South Wales Animal Care and Ethics was obtained before the start of this study. The PRP preparation protocol adopted was similar to that reported by Araki et al. 27 After the animal was anesthetized, 106 mL of whole blood was drawn via the jugular vein and mixed with 14 mL of anticoagulant citrate dextrose, solution A (ACD-A). The anticoagulated whole blood was centrifuged at 270 g for 10 min (5804; Eppendorf ). All of the plasma above the red blood cell layer was collected, and was spun for a second time at 2000 g for 10 min. PPP was collected from the uppermost region after the second spin. The platelet pellet that had formed after the second spin was resuspended within 11 mL of plasma by vortex mixing to form the PRP (Fig. 1). Autologous thrombin (AT) was prepared using a method described by Everts et al., 28 in which 4 mL of PRP was added to 0.17 mL of sterile 10% w/v CaCl2. After gelation, the supernatant was collected as AT. The PRP and PPP was activated with the produced AT shortly before implantation at a 4:1 ratio.
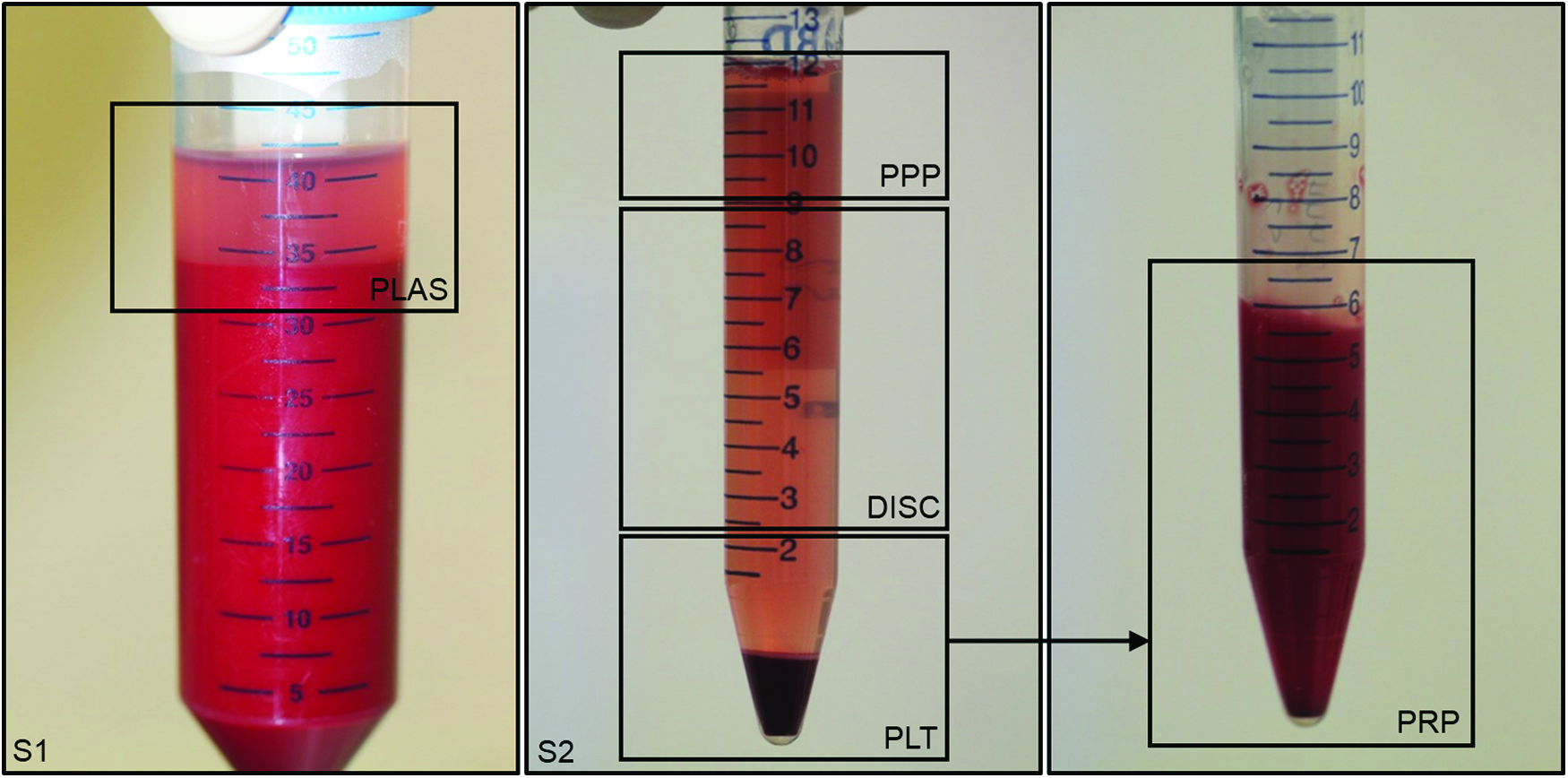
The platelet-rich plasma (PRP) preparation method. The first spin (S1) was at 270 g for 10 min. The top portion of plasma (PLAS) was collected and underwent a second spin (S2) at 2000 g for 10 min. After centrifugation, platelet-poor plasma (PPP) was collected for use. The middle portion was discarded (DISC), and the platelet pellet (PLT) was resuspended to prepare the PRP. Color images available online at www.liebertpub.com/tea
BCP, biphasic calcium phosphate; PPP, platelet poor plasma; PRP, platelet rich plasma.
Eighty cylindrical defects that were 11 mm in diameter, and 20 mm deep, were placed with a cannulated surgical acorn drill bit bilaterally in the cancellous bone within the epiphyseal region of the proximal tibia and distal femur in 25 year-old ewes (Fig. 2). Two cubic centimeter of a BCP (15%HA/85%β-TCP, MASTERGRAFT granules; Medtronic) was mixed with 0.7 mL (PRP-33), 1.3 mL (PRP-66), or 2.0 mL (PRP-100) of AT-activated PRP, or with 2.0 mL (PPP) of AT-activated PPP (Fig. 3). Two cc of autograft was harvested from the iliac crest using a rongeur into 1–3 mm particles. Graft materials were softly compacted into the defect void (Fig. 4). The soft tissue was closed with a 2-0 absorbable suture, and the skin was closed with a 3-0 suture. All surgeries were performed by a single surgeon (C.C.), and all tissue and graft preparation was performed by a single operator (A.M.). All animals received Cephalothin (0.024 mg/kg IV) and Benacillin (0.122 mL/kg IM) after induction as antibiotic prophylaxis. Animals also received Temgesic (buprenorphine, 0.005 mg/kg IM) and Carprofen (4 mg/kg SC) for pre-emptive pain relief before the surgery. For fluorescent bone labeling, calcein green (10 mg/kg), alizarin complex one (28 mg/kg), and oxytetracyline (23 mg/kg) were injected IM into the hind legs at week 1, 2, and 3, respectively. Animals received carprofen (2–4 mg/kg) orally once a day for 5–7 days postoperatively, and an intramuscular injection of Temgesic (0.005 mg/kg) once a day for 1–3 days postoperatively. At 4 weeks postoperatively, the animals were euthanized by a lethal overdose of sodium pentobarbitone (Lethabarb; 1 mL/2 kg). The hind legs were harvested for endpoint processing. In addition, samples of heart, liver, lungs, kidney, and spleen were taken for routine histology.
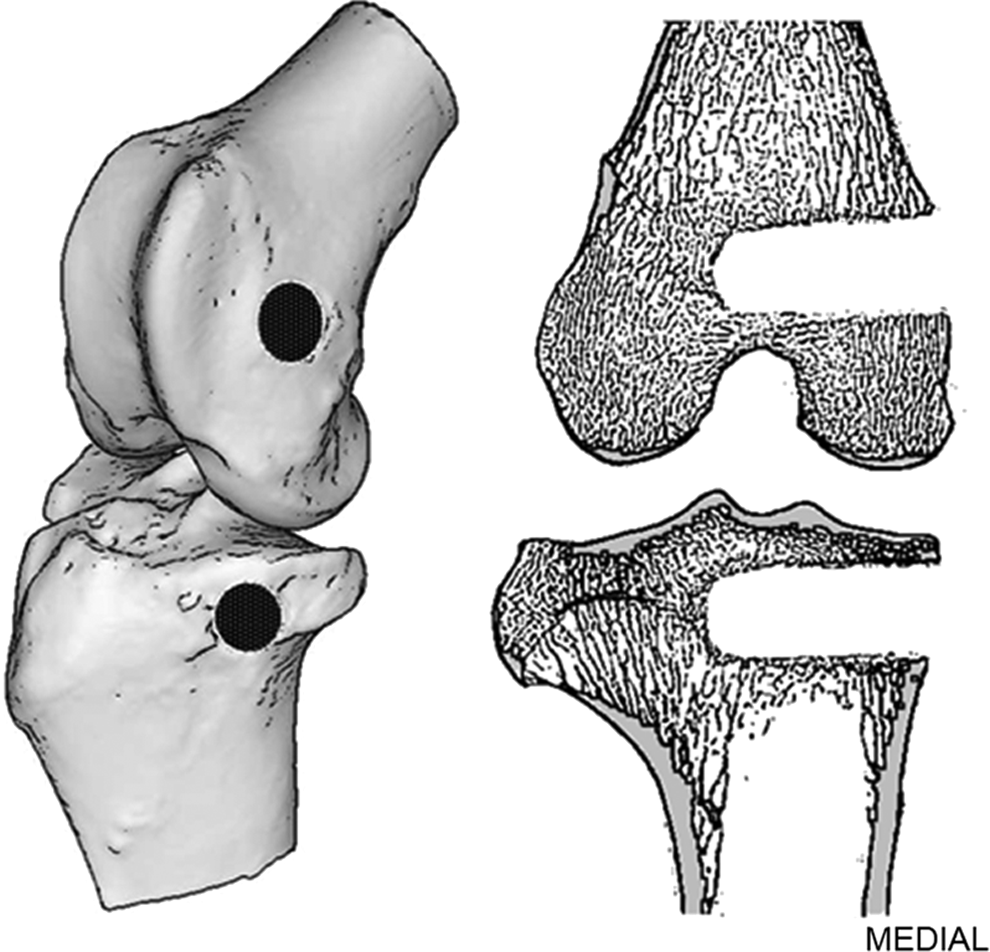
The location of defects illustrated in the right hind leg.
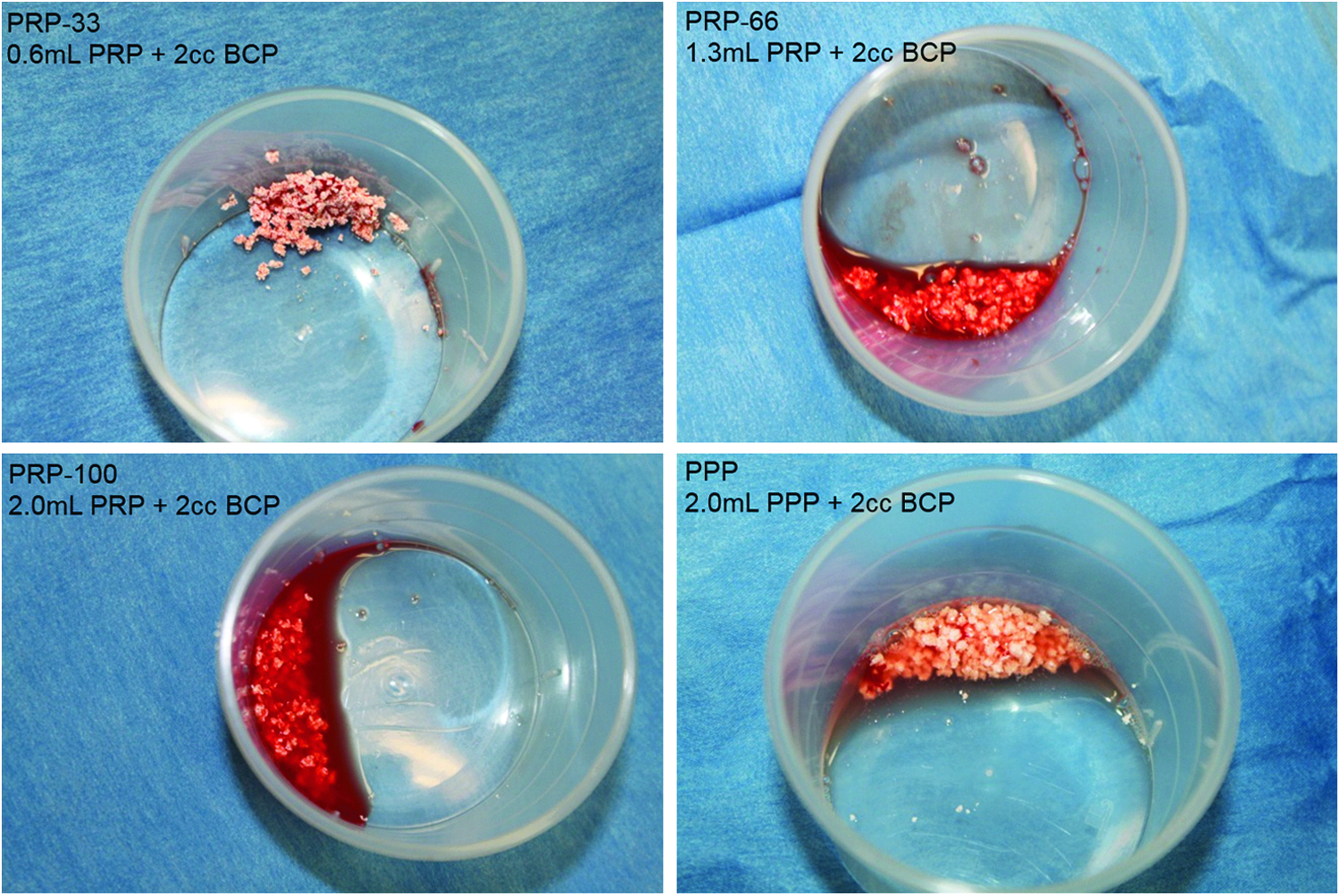
The PRP and PPP groups after activation shortly before implantation. Color images available online at www.liebertpub.com/tea
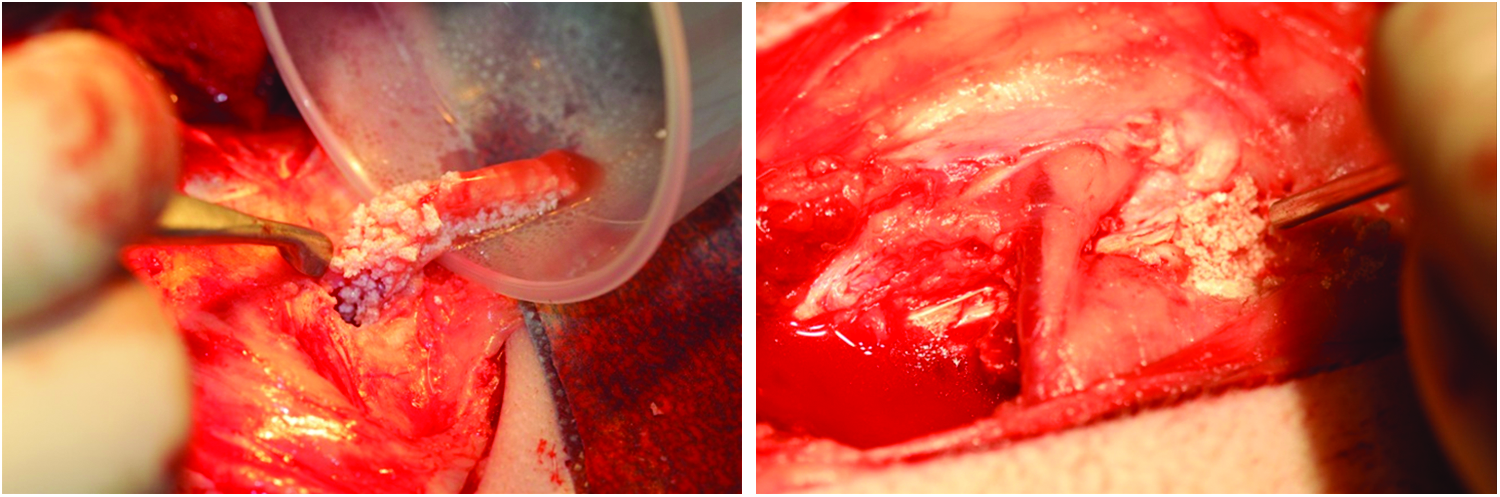
Graft implantation after clotting (left), and soft compaction into the defect void (right). Color images available online at www.liebertpub.com/tea
Endpoints
Platelet concentrations were measured using a standard manual hemocytometer counting method. 29 The leukocyte (XT-2000iV; Sysmex Corporation) and fibrinogen (AU680; Beckman Coulter, Inc.) concentrations were measured using automated analyzers. During the surgery, the time to clot was measured, and the handling of each graft was assessed by the surgeon according to a qualitative handling grading scale of 1–4 (1=difficult to handle, 4=easy to handle). On the day of the surgery, whole blood was centrifuged at 2000 g for 10 min, and plasma was collected as the circulating baseline transforming growth factor (TGF)-β1 concentration. PRP and PPP samples were activated with AT, and the samples were allowed to clot. Clotted samples were centrifuged at 2000 g for 10 min, and the serum was collected. The baseline plasma, PRP serum, and PPP serum samples were stored at −80°C for later processing. After thawing, TGF-β1 concentrations were measured using a standard ELISA kit according to the manufacturer's instructions at a final dilution of 20:1 (Quantikine TGF-β1; R&D Systems). Samples were measured in duplicate with a microplate absorbance reader (Tecan Sunrise; Tecan Group Ltd.), and unknowns were interpolated using curve fitting software (MyAssays Ltd. 2009).
Four weeks after surgery, the hind legs were radiographed in both anteroposterior and lateral views using a high-resolution X-ray device (MX20; Faxitron Bioptics), and they were graded by three blinded observers according to a qualitative grading scale of 1–5 (1=no healing, 5=complete healing). The tibial and femoral defects were cut by hand from the surrounding bone. Each of the blocks was scanned at a high resolution on a micro-computed tomography (μCT) scanner (Siemens microPET-CT System, Seimens Medical Solutions) with a resulting slice thickness of 28 μm. Bone volume/total volume (BV/TV) was quantified through intensity thresholding (Fig. 7) using the μCT software (Inveon Research Workplace).
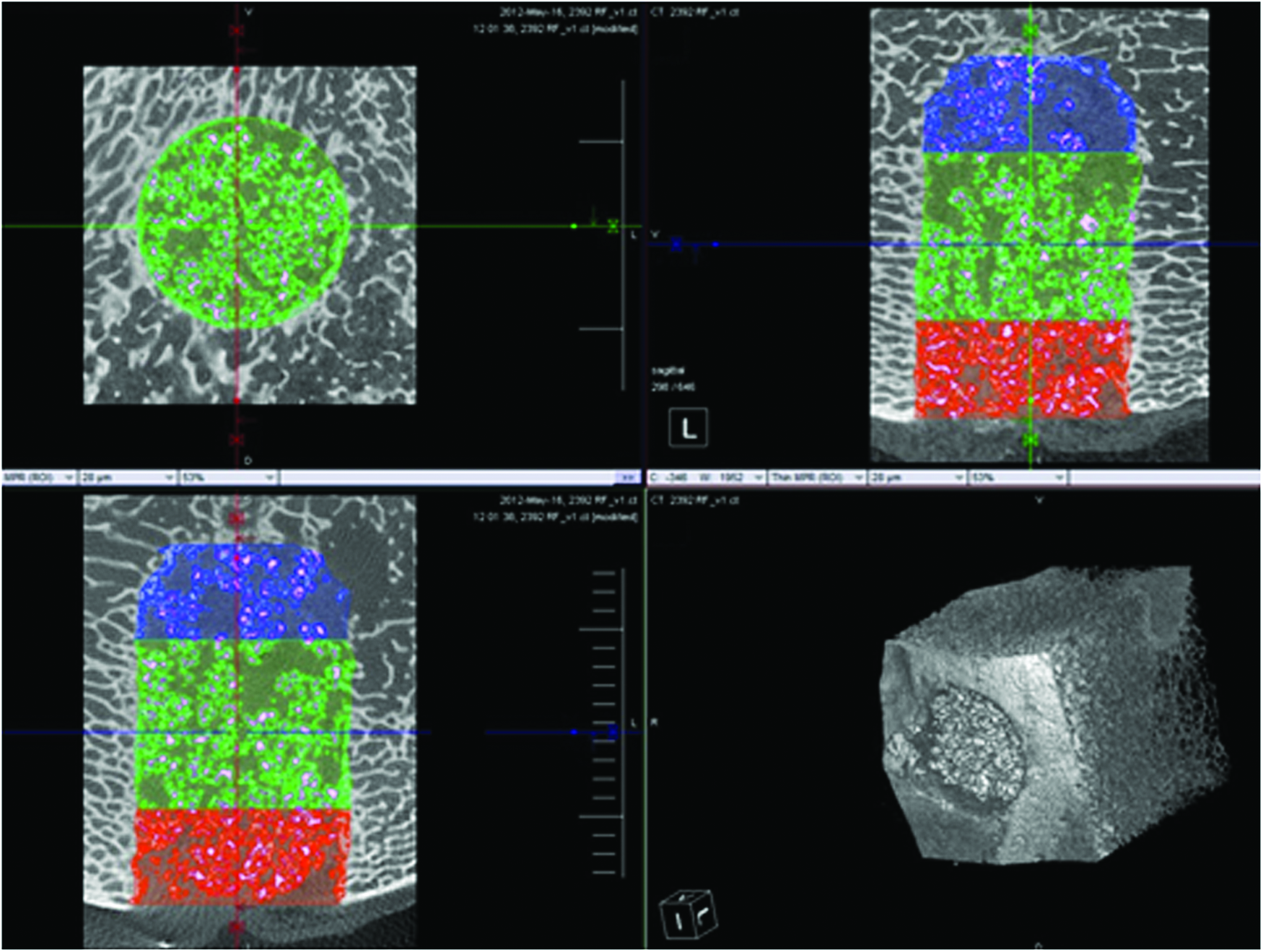
Representative μCT image of reconstructed defect block used for quantification. The red region is the medial portion of the defect. Color images available online at www.liebertpub.com/tea
Each of the defect blocks was fixed in 10% buffered formalin, dehydrated, and embedded in poly(methyl methacrylate) for hard tissue histology. Four 40 μm sagittal sections were cut along the 20 mm defect depth at 3–4 mm intervals with a saw microtome (Leica SP1600; Leica Microsystems), and they were stained with basic fuschin and methylene blue. All sections were analyzed using normal transmitted light microscopy (Olympus). Two regions of interest (ROI) were defined for the qualitative and quantitative histology. The margin region was defined as the 2 mm-wide region at the peripheral margin of the defect, and the central region was the 7 mm-diameter concentric circle in the central region (Fig. 5).
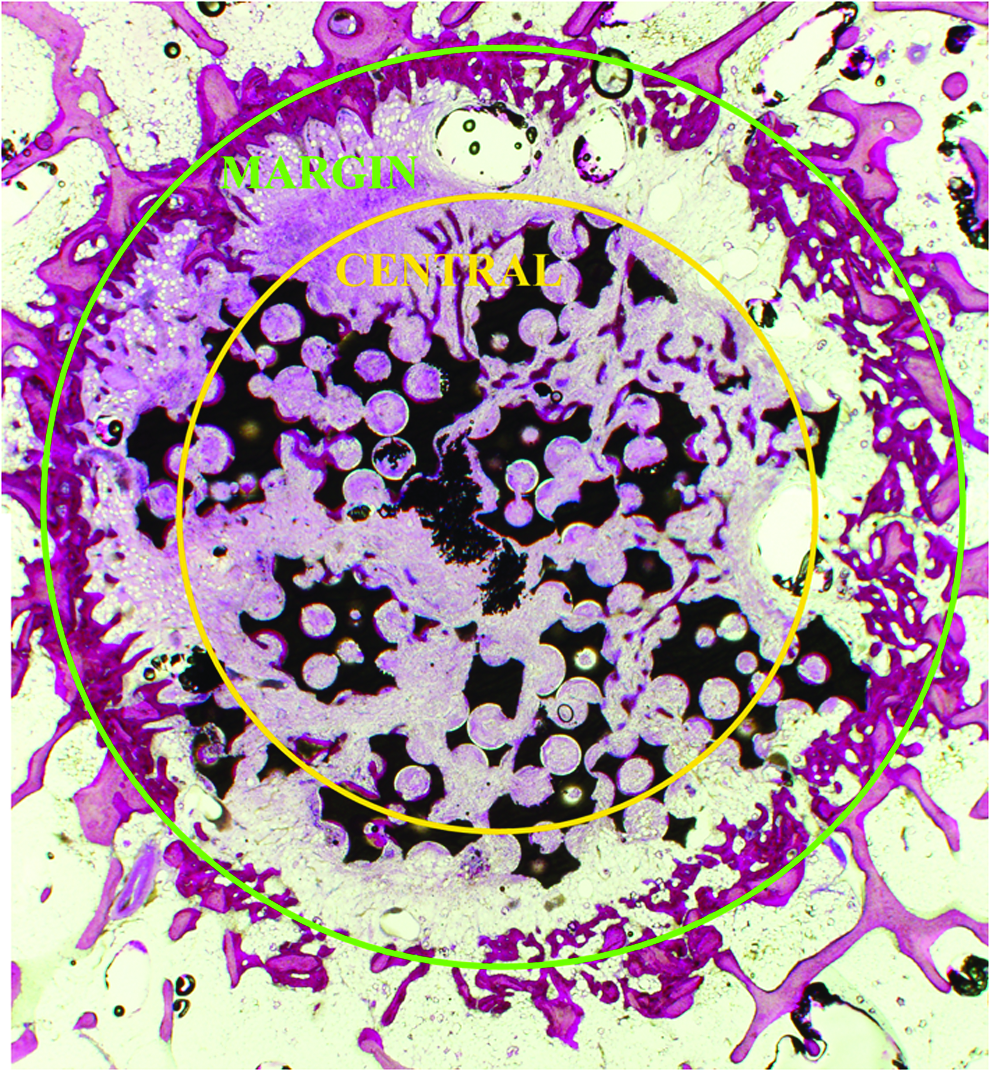
Regions of interest (ROI) created in the 11 mm diameter defect for histology grading and quantification (1.25×). Color images available online at www.liebertpub.com/tea
Osteoblast shape and density were blindly graded by scanning the central and margin regions, and grading each region according to a grading scale of 0–4 (0=no osteoblasts, 1=flat osteoblasts at <80cells/mm, 2=flat osteoblasts at >80cells/mm, 3=plump osteoblasts at <80 cells/mm, and 4=plump osteoblasts at >80cells/mm). The maturity of the bone was assessed with polarized light microscopy. The percentage of new bone area within the specific ROIs was quantified using histomorphometric analysis with an in-house image analysis program (MATLAB; The MathWorks, Inc.). Bone ingrowth was radially measured at eight evenly spaced points around the defect margin using the program of the microscope camera (DP72; Olympus). The eight radial measurements were averaged to provide a bone ingrowth depth value for each section. The weekly formation of new bone was assessed with fluorescent microscopy using the measurement tool within the program of the microscope camera (DP72; Olympus). The section 8–10 mm from the medial side of the defect was used for quantification. The perpendicular distance from the margin to the deepest point of the specific fluorochrome label was averaged over a minimum of eight points for each defect.
Statistical methods
To account for the hierarchical data structure, mixed-effects modeling using PASW Statistics 18.0.0 or later versions (IBM SPSS) was used for all the statistical analyses. Normally distributed data, based on the Shapiro–Wilk test for normality, were analyzed using linear mixed-effects modeling; otherwise, all grading data and any data not normally distributed were analyzed using the generalized linear mixed-effects modeling method. Bonferroni corrections were used for any multiple pairwise comparisons. For linear regression, partial correlations were used to control for the within-animal dependency of the data. A p-value of less than 0.05 was considered statistically significant. All data are reported as the mean (±standard error).
Results
Platelet, leukocyte, and fibrinogen concentration
The PRP produced had a mean increase in platelets of 2.9-fold above baseline, and lower than baseline leukocyte and fibrinogen concentrations (Table 2).
Statistically significant difference compared with the whole blood baseline (p<0.05). The data represent the average and standard deviations for N=18.
Time to clot and handling
The mean time for production of the PRP and PPP was 70±1.5 min. PRP-33 (7.5±1.3 min) had a significantly lower time to clot than both PRP-100 (10.7±2.2) and PPP (12.5±2.4). The addition of both PRP-100 (3.9±0.1) and PRP-66 (3.4±0.2) significantly improved the handling grades of the BCP (2.5±0.3), while the autograft was consistently graded as the easiest to handle (4.0±0.0).
TGF-β1 release
The TGF-β1 serum concentration of the activated PRP was significantly higher than the circulating whole blood baseline (Table 3). The TGF-β1 concentration of the activated PPP was greater than the whole blood; however, this did not reach statistical significance (p=0.054). A weak significant relationship was detected between the PRP platelet concentration and TGF-β1 concentration (r=0.502, p=0.04). However, no significant relationship was found to exist between circulating whole blood platelet concentrations and TGF-β1 levels (r=− 0.204, p=0.42), or between PPP platelet concentration and TGF-β1 concentration (r=0.108, p=0.71).
Statistically significant difference compared with the whole blood baseline (p<0.05).
TGF, transforming growth factor.
Macroscopic evaluation
All organs and surgical sites appeared normal and healthy within all animals. Superficial scar tissue surrounding the defect was common. There was no indication of a prolonged inflammatory response or an adverse reaction to any of the grafts. Two of the sheep were euthanized before the 4 weeks due to animal welfare concerns. Both of these animals had luxating patellas, and on both animals it was found that the standard 2-0 suturing material had failed to secure the soft tissue. Both animals underwent a second surgery with soft tissue closed by continuous suturing with #0 suture. This was unable to improve the patella stability, and the animals were euthanized at day 7 and 10 due to an inability to eat and drink freely. This breakdown did not appear to be caused by treatment, as each of the two pairs of hind legs had different treatments assigned. There was no sign of infection at any of the defect sites, and organs appeared normal and healthy. Six of the 80 (7.5%) defects had fractures, all of which were depressed tibial plateau (Schatzker type) fractures that resulted in a deformed tibial defect and removal from the dataset. These fractures affected groups PPP (2), PRP-33 (1), HA (1), Empty (1), and Autograft (1).
Radiographic grading
Both PRP-100 (3.6±0.1) and PRP-66 (3.5±0.1) were graded significantly higher than PRP-33 (3.1±0.1). PRP-33 was graded lower than PPP (3.5±0.2, p=0.052). Overall, the PRP dose had a significant effect on the radiographic grade. For the pairwise comparisons, none of the PRP or PPP groups were significantly different to BCP alone (3.4±0.1, p>0.109). Both autograft (2.7±0.3) and empty group (1.3±0.1) were graded significantly lower than all other groups, and the autograft was graded significantly higher than the empty group (Fig. 6). However, comparisons of any groups containing BCP to either the autograft or empty groups are confounded due to the radiographic density of the BCP.

Radiographs were blindly graded by three independent observers. Eight defects over two separate animal hind legs are shown with treatment groups displayed in yellow. The green arrows align with the defect axis to indicate the defect location. Color images available online at www.liebertpub.com/tea
μCT quantification
Both PRP-100 (30.6%±1.8%) and PRP-66 (28.7%±1.0%) had a significantly greater μCT BV/TV than the BCP alone (24.5%±0.8%). Both PRP-33 (28.4%±1.6%, p=0.18) and PPP (27.5%±1.5%, p=0.78) had higher mean μCT BV/TV than the BCP alone; however, these differences were not statistically significant. While a trend was apparent, the PRP dose was not detected to have a significant effect on the μCT BV/TV (p=0.664). There was a significant difference between the autograft (22.4%±2.4%) and empty group (9.6%±3.2%); however, comparisons with the autograft would be confounded due to the inability of this method to differentiate between new bone and residual autograft.
Histology
In general, the defects contained the implant material surrounded with fibrous tissues, and bone ingrowth from the surrounding trabeculae. Woven bone at the margin was commonly found across all groups (Fig. 8). New bone formed from at the margin of the defect with a lining of osteoblasts. The ingrowth bone closer to the margin had an irregular collagenous matrix regardless of the treatment group, with very few regions of lamellae bone. This woven bone was often surrounded with bone marrow structure.

Pattern of bone formation. The BCP (green arrow) is surrounded by fibrous tissue (FT). New bone formed at the defect margin (blue arrow) regardless of treatment. The defect in the image contains the BCP alone (1.25×). Color images available online at www.liebertpub.com/tea
Fibrous tissues were found at the center of all defects. New bone formation within the central region was greater in the PRP groups compared with the BCP alone, while the empty group did not have any new bone formation in the central region (Figs. 9 and 10). The autograft group had a high percentage of bone within the defect; however, this may have been residual autograft and not necessarily new bone. Within the central region, the new bone commonly formed directly on the BCP surface within the PRP and PPP groups.
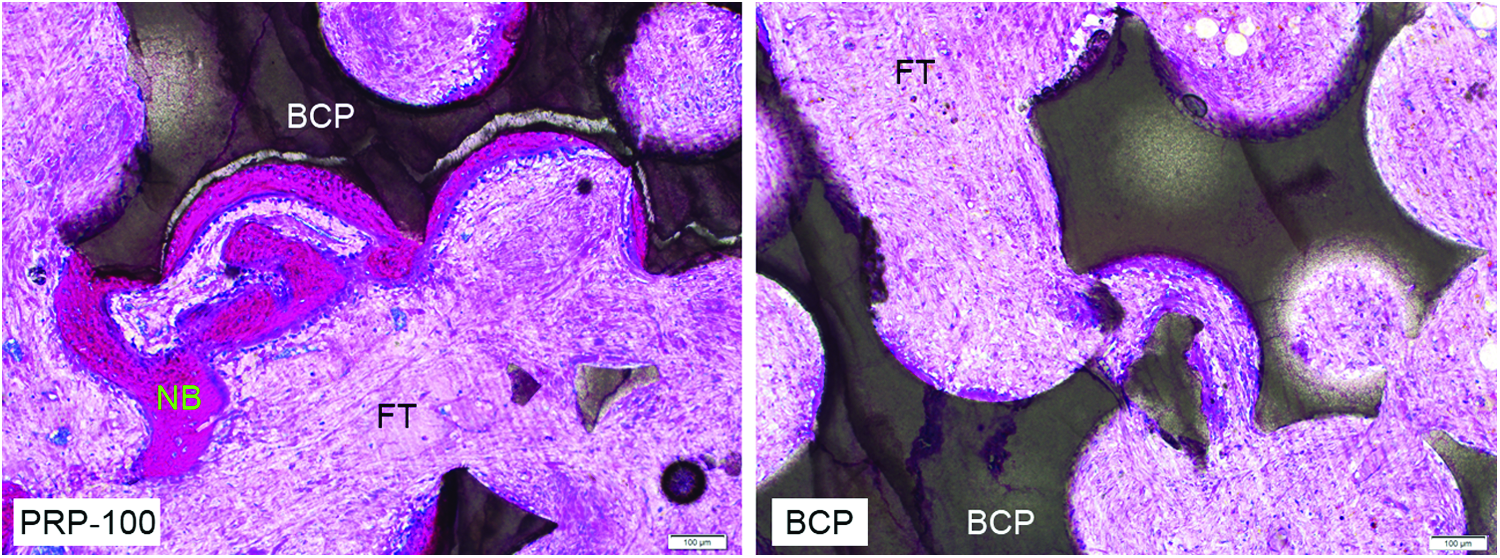
Representative micrographs (10×) of PRP-100 (left) and BCP alone (right) groups at the central regions. New bone (NB) formed directly on the BCP in the PRP groups. The BCP group was commonly surrounded with fibrous tissue (FT). Color images available online at www.liebertpub.com/tea
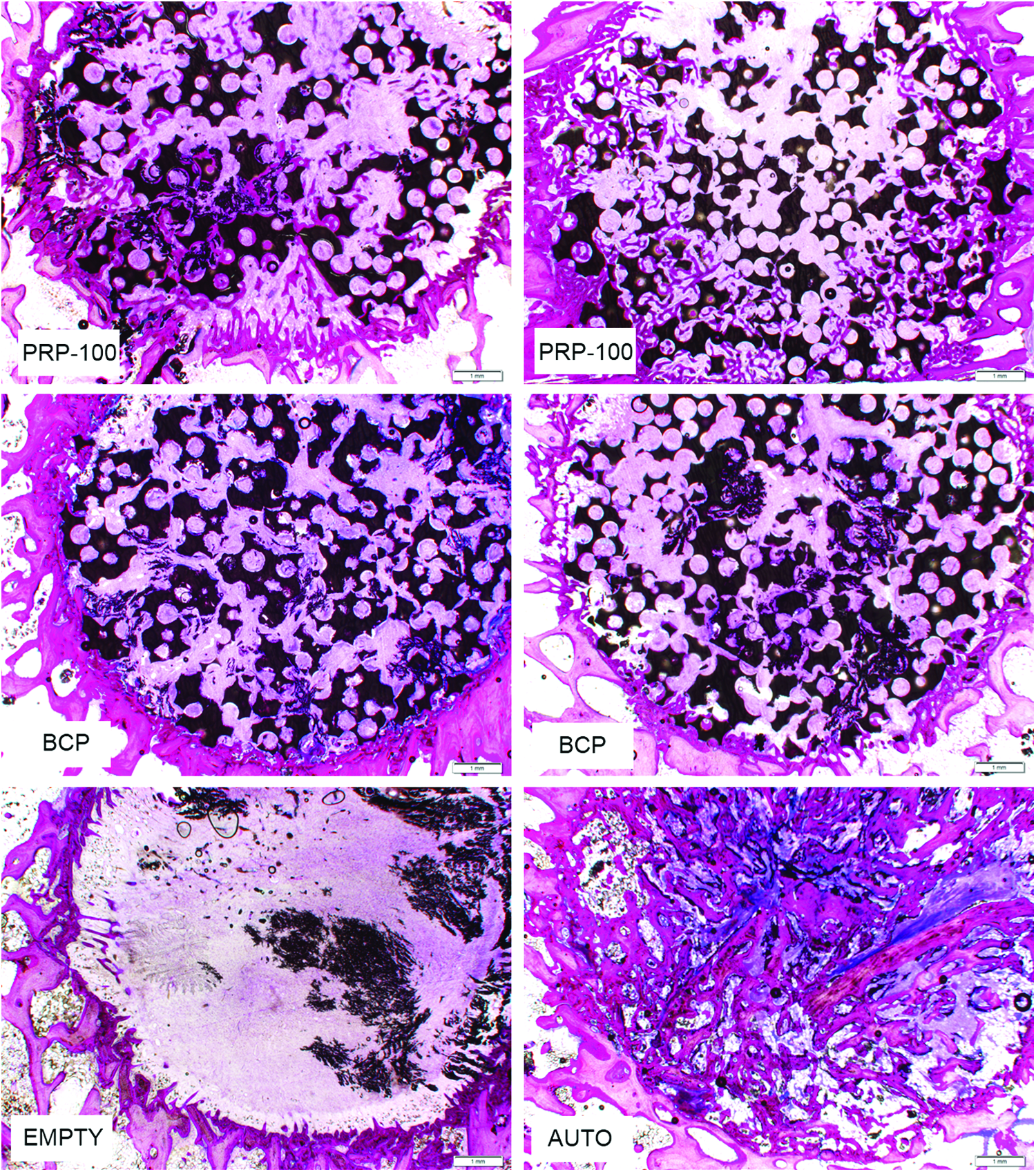
New bone formed within the PRP groups (top row), which did not occur within the BCP alone (middle row) groups. The empty (bottom left) groups confirmed the nonhealing nature of the defect. The autograft (bottom right) groups contained a combination of new and residual bone (1.25×). Color images available online at www.liebertpub.com/tea
The PRP, PPP, and autograft groups often had new bone formation at the center of the defects, with a lining of plump osteoblasts and minimal collagen deposition. Within some of the PRP and autograft groups, there was a high density of osteoblasts that did not occur within the empty or BCP groups (Fig. 11).
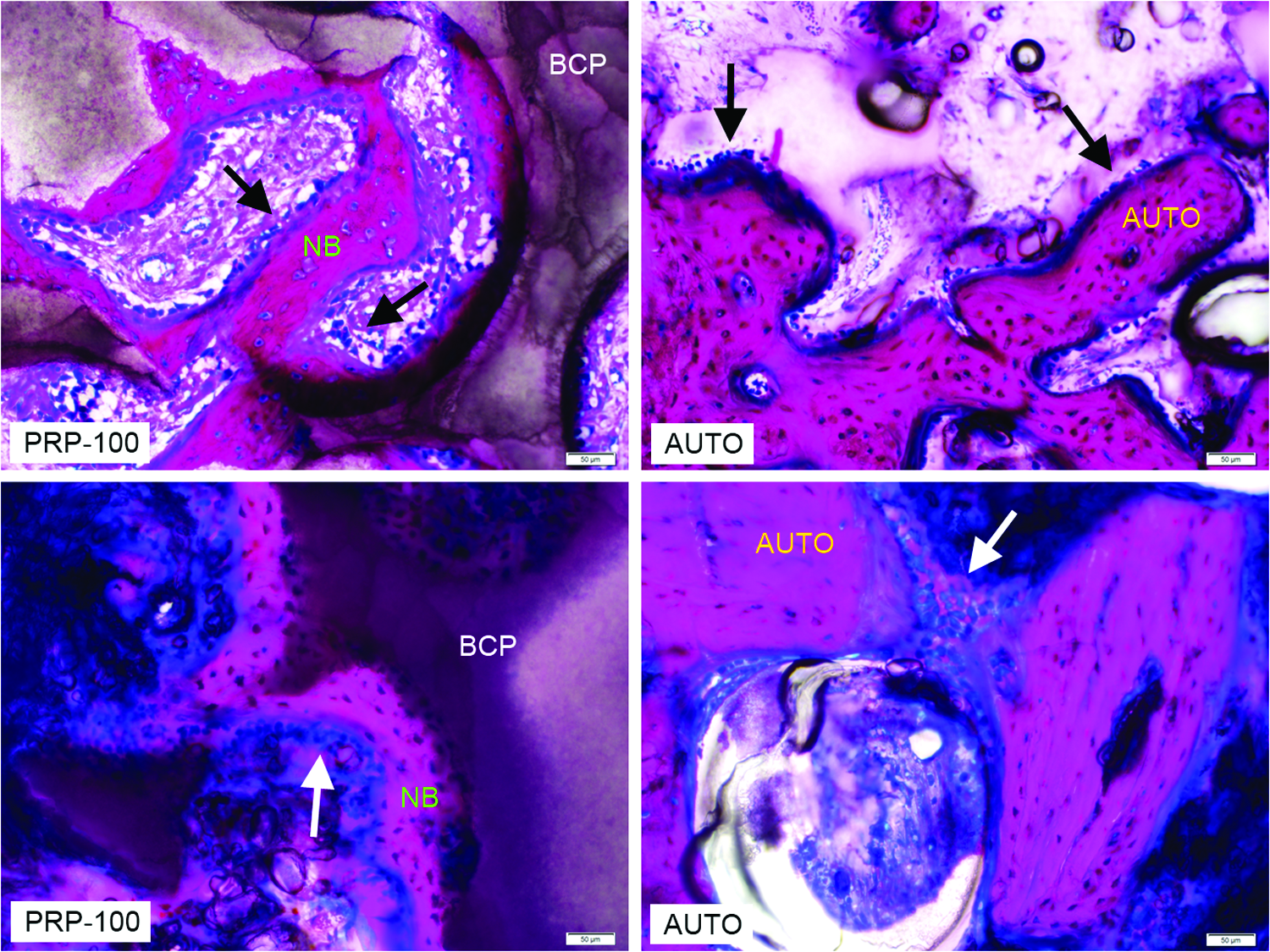
Representative micrographs (20×) of the central regions of PRP-100 (left) and autograft (right) groups. Plump osteoblasts (black arrows) were found lining the new bone (NB), which formed directly on the biphasic calcium phosphate (BCP). Plump osteoblasts also lined the autograft (AUTO). Regions of densely layered osteoblasts (white arrows) were found within both the PRP-100 and autograft groups. Color images available online at www.liebertpub.com/tea
Histomorphometry
Central region
The PRP dose was detected to have a significant effect on the central region new bone area. Within the central region of the defect, the PRP-100 (3.8%±0.3%), PRP-66 (2.8%±0.2%), PRP-33 (2.2%±0.2%), and PPP (1.8%±0.2%) had significantly greater central new bone area than both the BCP alone (0.3%±0.1%) and the empty defects (0.1%±0.03%). All pairwise comparisons within the PRP dose groups were detected to be significantly different from each other. No significant difference was detected between the BCP alone and empty (p=0.882) groups. The autograft central new bone area (13.2%±1.0%) was significantly higher than all other groups.
Total region
There was a significant dose-dependent effect in the new bone area within the total defect area (Fig. 12). PRP-100 (15.1%±0.8%), PRP-66 (14.0%±0.6%), and PRP-33 (11.9%±0.6%) had significantly greater new bone area than the BCP alone (8.9%±0.7%) and empty (10.8%±0.8%) groups. PPP (11.7%±0.6%) was higher than both the BCP alone and empty groups; however, these differences were not statistically significant (p=0.080 and p=0.481, respectively). The autograft (34.3%±1.7%) had a substantially and significantly greater new bone area than all groups; however, these comparisons were confounded, as the histomorphometric method was not able to differentiate between new bone and residual autograft.
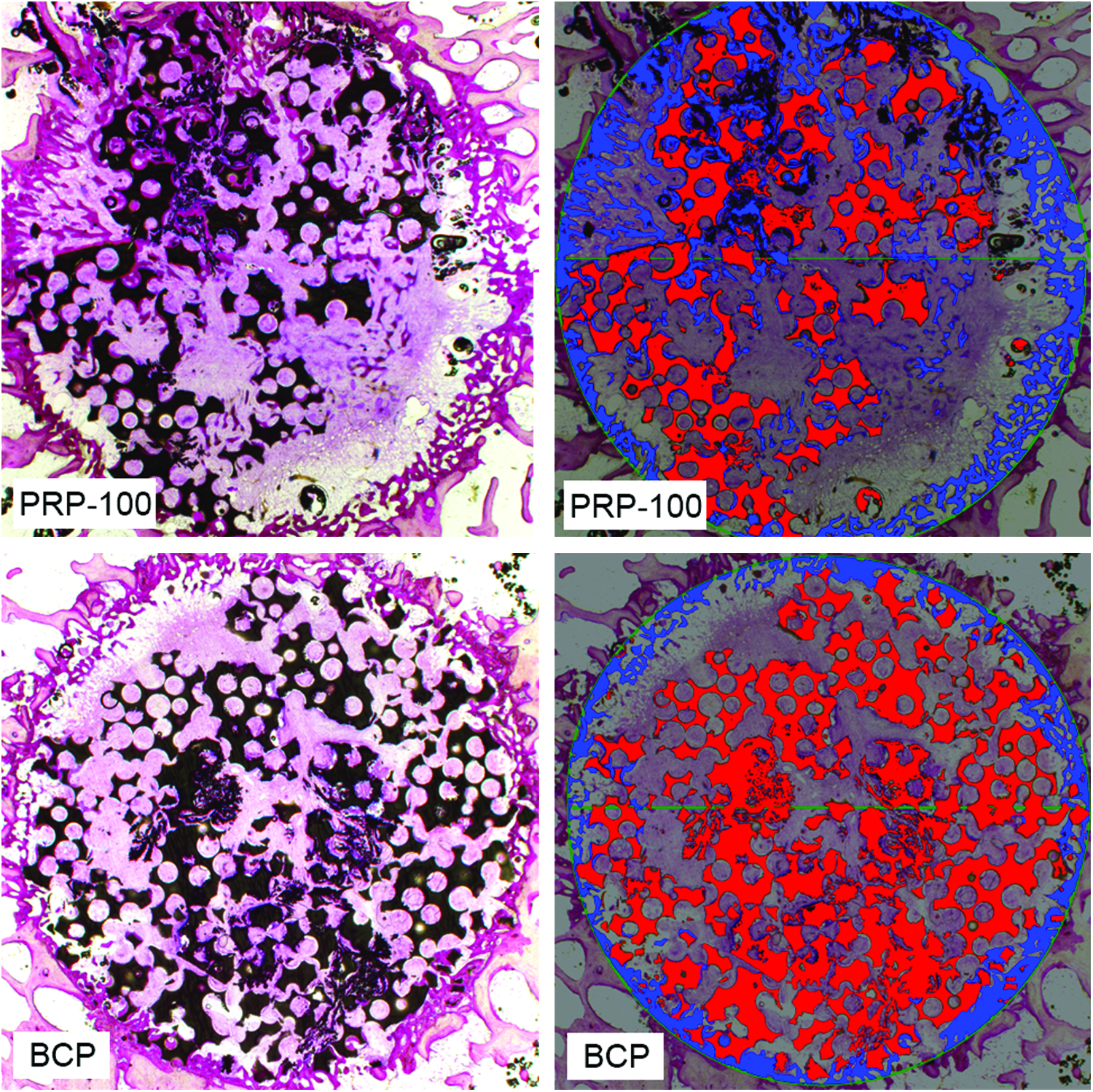
Representative histomorphometry of PRP-100 (top row) and BCP (bottom row). The left side images are unprocessed, and the respective right side images are postprocessing. Blue selection is bone within the 11 mm-diameter ROI (1.25×). Color images available online at www.liebertpub.com/tea
Bone ingrowth depth
PRP-100 (2306±141 μm), PRP-66 (1978±136 μm), PRP-33 (2215±149 μm), and PPP (2200±158 μm) had a significantly greater new bone ingrowth depth than the BCP alone (1357±301 μm) and empty (848±89 μm) groups. The PRP dose was not found to have a significant effect on the new bone ingrowth depth (p=0.128). There was a relatively small difference between BCP alone and empty groups; however, this difference was not detected to be significant (p=0.439).
Osteoblast shape and density
Central region
The mean central grades of PRP-100 (3.1±0.2), PRP-66 (2.2±0.2), PRP-33 (2.8±0.2), PPP (3.2±0.2), and autograft (2.8±0.3) were significantly greater than the BCP alone (1.0±0.3) and empty (0.0±0.0) groups. The difference between the BCP alone and empty group did not reach significance (p=0.07). No statistically significant difference in the mean central osteoblast grade was detected between the PRP dose groups, PPP, and autograft groups (p>0.566). The proportions of central grades are shown in Figure 13.
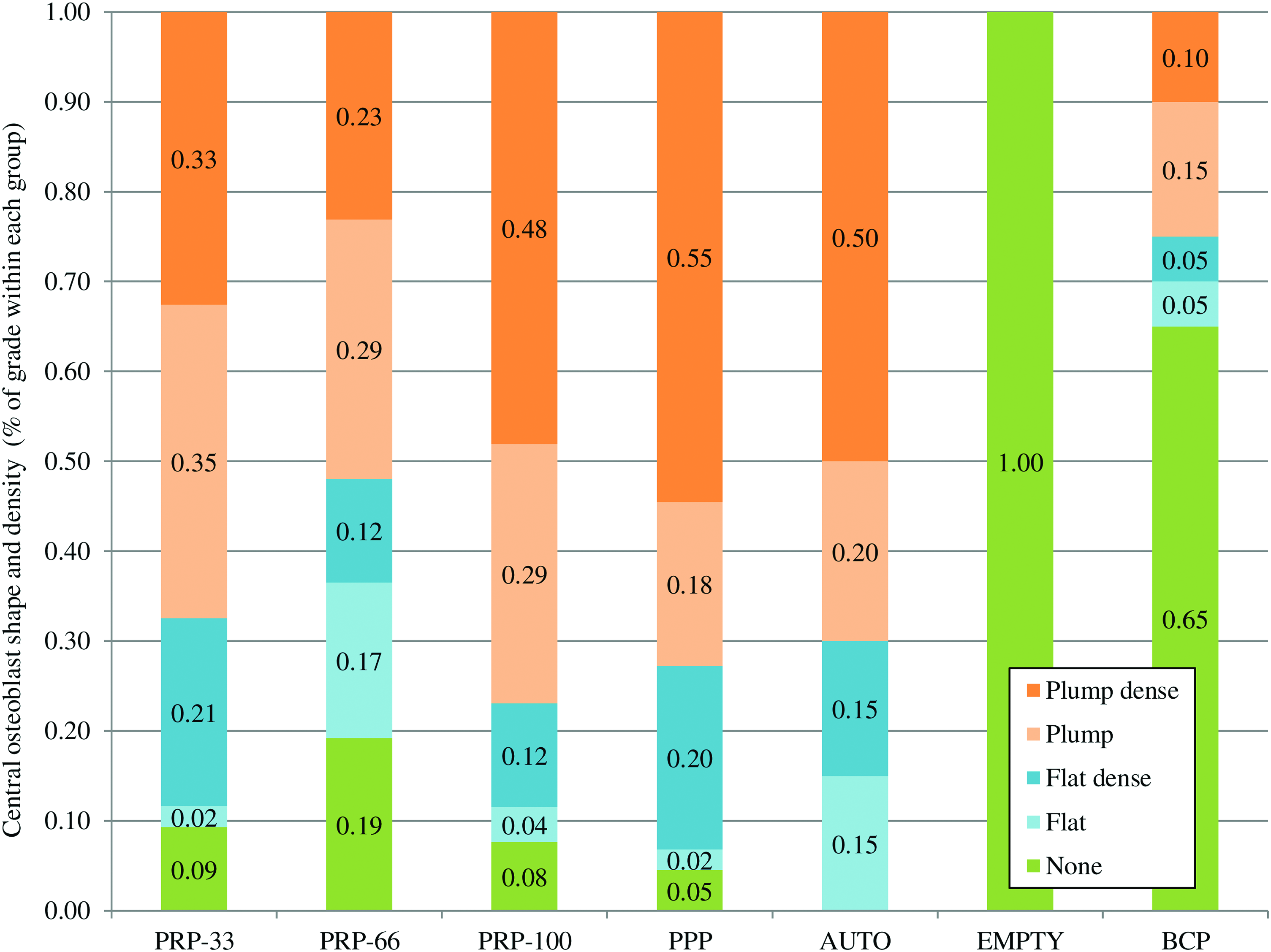
Proportion of allocated osteoblast grades within the central region of the defect. Plump osteoblasts were more commonly reported in the PRP-100, PPP and AUTO groups. The AUTO group was always reported to contain osteoblasts. The PRP dose groups had a high ratio of osteoblasts (>80%) within the central region compared with BCP alone (<35%). Color images available online at www.liebertpub.com/tea
Margin region
The mean margin grade of PRP-100 (2.4±0.2) was significantly greater than the BCP alone (1.6±0.2). The mean margin grade of the BCP alone was lower than PRP-66 (2.0±0.1, p=0.45), PRP-33 (2.2±0.2, p=0.19), PPP (2.4±0.2, p=0.11), and the autograft (2.5±0.2, p=0.06); however, these differences did not reach significance. The autograft margin grade was significantly different from PRP-66 and PRP-33, but not from PPP (p=0.74). The BCP alone and empty (1.5±0.1) margin grades were not found to be significantly different (p=0.76). The proportions of grades at the defect margins are shown in Figure 14.
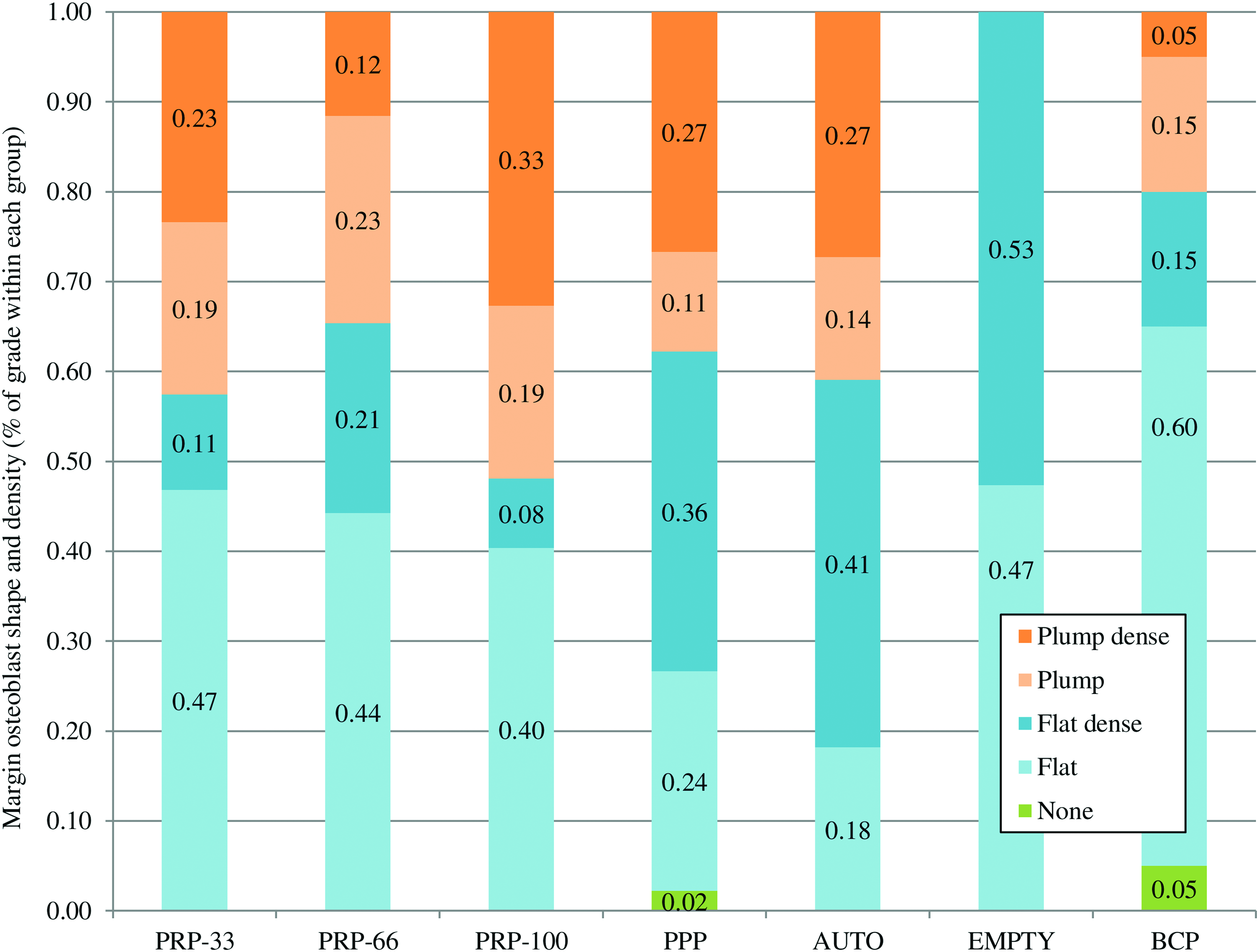
Proportion of allocated osteoblast grades within the margin region of the defect. There were very few sections identified that had no osteoblast presence on the margin. Plump osteoblasts were more commonly present on the PRP dose and autograft groups when compared with BCP alone and empty groups. Color images available online at www.liebertpub.com/tea
Weekly fluorescently labelled bone ingrowth
The autograft had a significantly greater ingrowth depth than all other groups at each of the first 3 weeks (Fig. 15). No significant differences were detected at week 1 between any other groups. PRP-100 had a significantly greater ingrowth depth than the BCP alone at both week 2 and 3. From week 2 onward, all of the PRP dose groups had deeper ingrowth than BCP alone. This effect was significant for PRP-100 and PRP-33; however, significance was not reached for PRP-66 (p=0.082) or PPP (p=0.075). BCP alone did not improve the ingrowth depth significantly over the empty group (p=0.942), while all PRP and PPP groups had a significant effect compared with the empty group (p<0.05). A trend appeared within the PRP dose groups over the 3 weeks; however, the effect within the PRP dose groups did not reach significance (p=0.20). Representative bone labeling is shown in Figure 16.
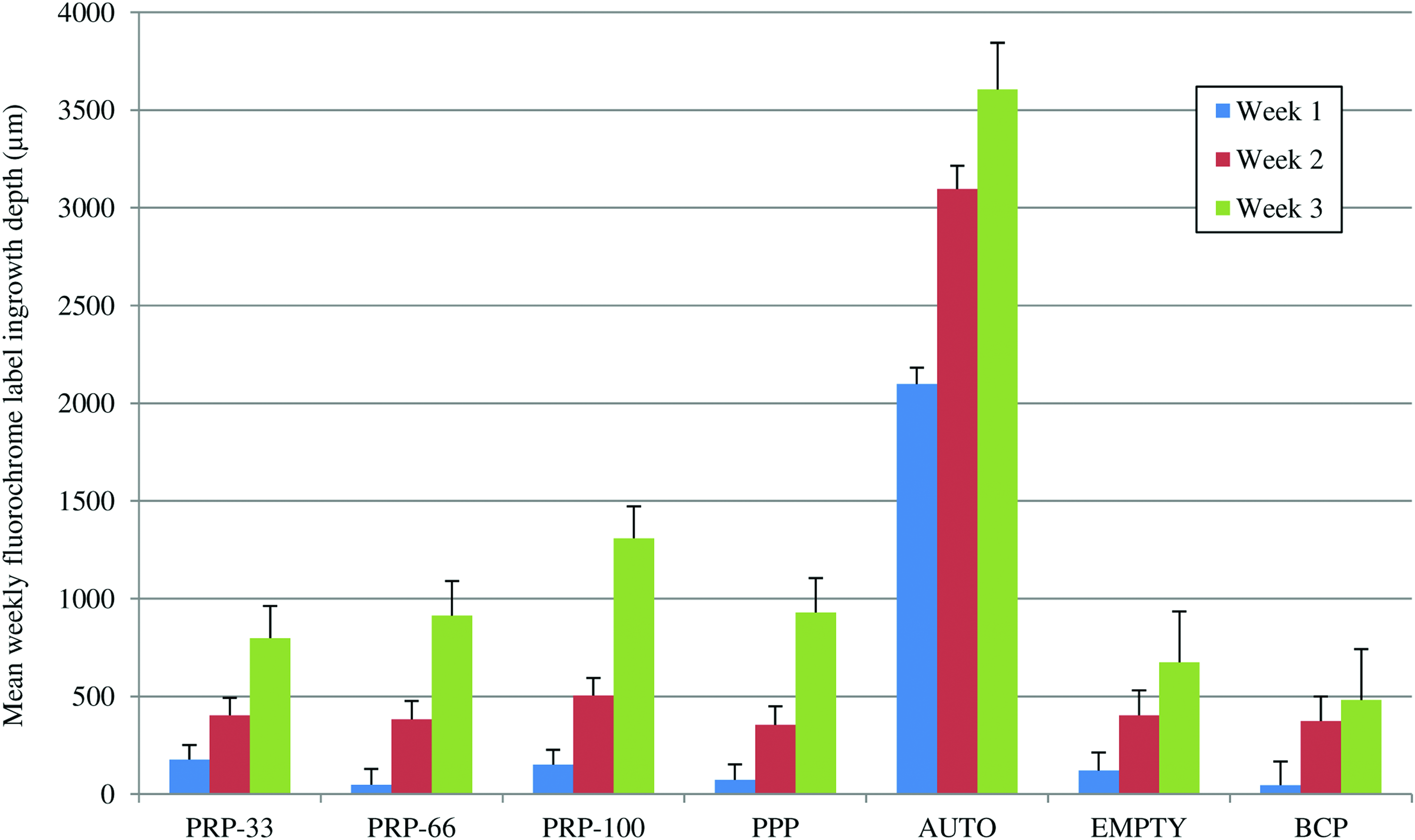
Mean fluorochrome bone label ingrowth depth at weeks 1, 2, and 3. For clarity, associated significant differences are discussed within the text. Color images available online at www.liebertpub.com/tea
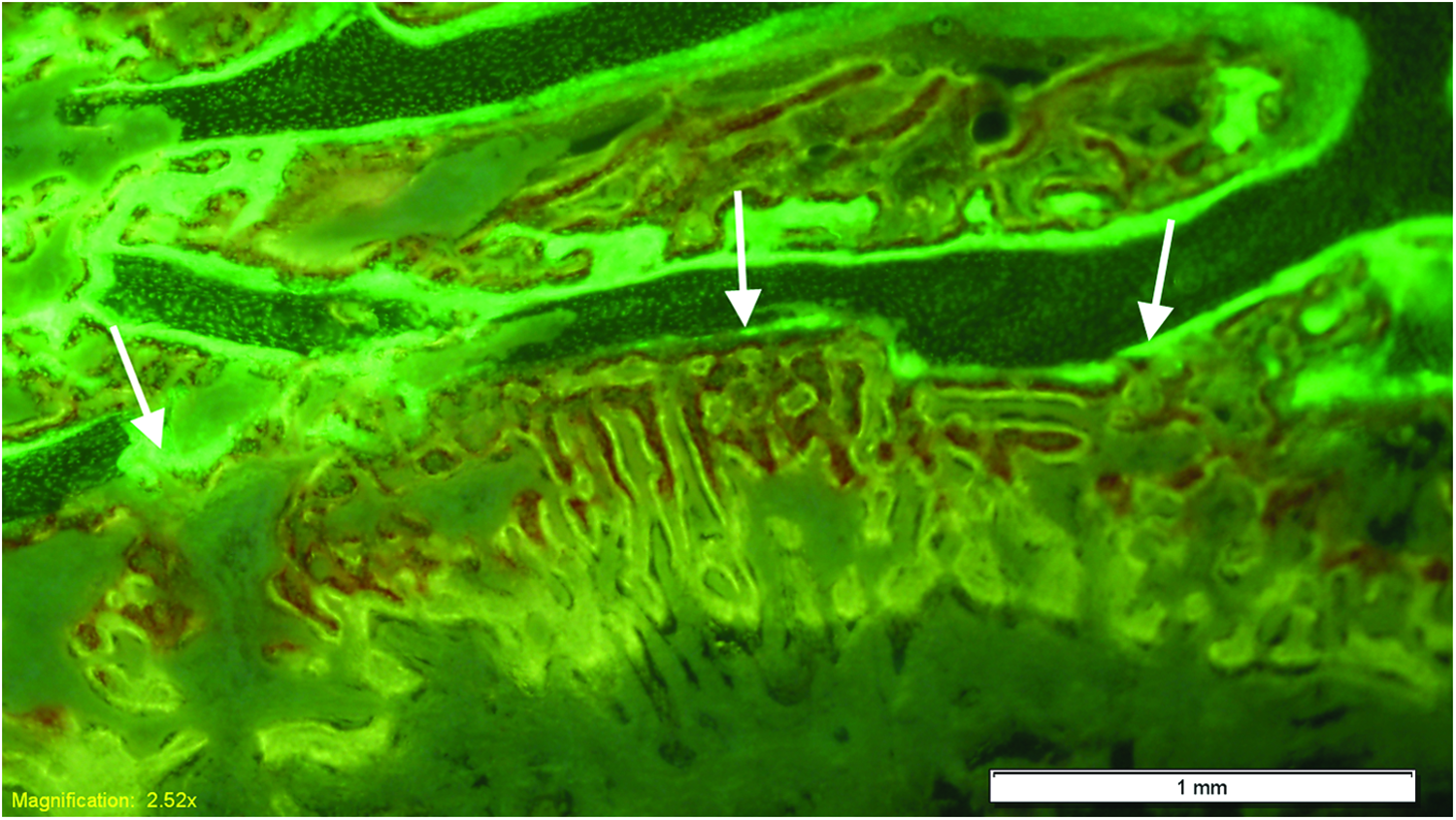
Fluorochrome bone labeling for autograft. There was minimal bone formation in the defect at week 1 (green); while at week 2 (red) and week 3 (yellow), new bone progressed toward the center of the defect (white arrows). Color images available online at www.liebertpub.com/tea
Platelet dose correlations
When the BCP alone group was considered as having an activated platelet number of zero, the PRP platelet number was detected as being significantly related to the radiographic grade (r=0.275, p=0.04), the μCT BV/TV (r=0.261, p=0.045), and the histomorphometric new bone area (r=0.305, p=0.02). A significant relationship was also reported between the PRP platelet dose and the week 3 ingrowth (r=0.323, p=0.21); however, no relationship was found at week 1 (r=− 0.06, p=0.36), week 2 (r=0.157, p=0.17), or week 4 (r=0.133, p=0.21). A relationship appeared to exist with the osteoblast grade at the central region; however, this was not significant (r=0.213, p=0.085). No relationship was detected between platelet number and the osteoblast grade at the margin (r=−0.056, p=0.361). While some of the correlation coefficients are significant, the strength of the coefficients is relatively weak (r<0.324), indicating that the platelet concentration accounts for less than 11% of the variance in that respective endpoint.
Discussion
Tissue engineering relies on three fundamental properties, being signaling molecules, cells, and matrices. 5 The production and activation of PRP provides access to one of these elements, being the cell signaling molecules released on platelet degranulation. Application of these PRP-released chemotactic, mitogenic, and differentiating factors has been reported in a variety of bone-healing applications when used alone,30–33 and in combination with autograft,11,31,34–37 allograft,30,38–44 and bone graft substitutes.45–48 Despite the ongoing use, there is no consensus on the clinical efficacy of PRP23,49 due to the conflicting outcomes that are commonly reported.
BCP alone
The BCP used in this study did not illicit any adverse reaction, and it was able to support cellular attachment, which was evident by the immediate lining of osteoblasts on the graft surface. Both hydroxyapatite (HA) and beta-tricalcium phosphates (β-TCP) have been previously reported to have this osteoconductive property that supports bone healing.47,50–53 Due to differences in solubility between HA and β-TCP, the development of BCPs has enabled further control on degradation rates, mechanical integrity, and cellular attachment.54–59 This study used a BCP which was a 15% HA/85% β-TCP BCP, which is a similar ratio that was reported optimal by Arinzeh et al. 55
The osteoconductive nature of the biphasic grafting material was evident within this study. However, the scaffold on its own was incapable of stimulating a greater amount of new bone formation over the empty defect at 4 weeks. Calcium and phosphate ion dissolution can support bone healing,60–62 and this osteoinductive potential has been previously reported in ectopic models.59,62–65 This effect has been reported in large animal studies that were more than 12 weeks in duration in sheep, 59 goats, 64 and pigs. 66 The time point of 4 weeks within this study may have been too early to appreciate any such feature of the BCP used. This study found that new bone within the BCP alone group predominantly occurred at the margin, appearing to be an extension of the appositional bone. There was little evidence of sporadic de novo bone formation at the central region, which would have been more suggestive of any promoting effect by the BCP. The BCP is able to facilitate bone formation; however, it requires additional components to stimulate new bone formation. Without this, the purely osteoconductive scaffold on its own is of minimal benefit for early healing.
PRP and PPP provide biological components that support bone formation
The addition of an activated three-fold PRP to a BCP significantly improved early bone healing compared with the BCP alone in this large animal model. Both Kasten et al. 45 and Jungbluth et al. 67 reported similar results with calcium phosphates, in which the addition of PRP to HA improved the healing of bone defects in rabbits at 16 weeks, and in mini-pigs at 6 weeks, respectively. Similarly, Kanthan et al. 46 reported that PRP improved the healing of segmental defects in rabbits when combined with a coral-based osteoconductive scaffold. During platelet activation and degranulation, a myriad of chemotactic and mitogenic signaling proteins are released68,69 that are associated to many critical steps within bone-healing pathways. 70 When these signals are combined with an appropriate scaffold, the increased presence of cell signaling molecules released by the platelets can promote osteogenesis; while the migrating mesenchymal stem cell (MSC) and precursor cells are facilitated by the BCP. This was demonstrated by the significant formation of bone within the central region of the defect within the PRP groups, whereas very little central bone was present when BCP was used on its own.
The results of the present in vivo study demonstrate that osteoblast proliferation and activity was enhanced with the PRP treatments. In vitro, PRP has been reported to induce osteoblast proliferation,71–74 and stem cell proliferation75,76 and differentiation.77,78 Growth factors have a well-established role in cellular chemotaxis, proliferation, and osteogenic differentiation,7,70 and this activity appeared to be evident in this study. Many growth factors are released from platelets during degranulation, of which TGF-β1 was quantified in this study. TGF-β1 concentrations were found to be significantly higher than those of baseline circulating levels. TGF-β1 has been previously demonstrated to stimulate MSC proliferation and osteogenic differentiation.79–83 These results support the theory that growth factors released from the platelet α-granules during platelet activation positively influence bone healing, and they are accountable for the significantly increased in vivo osteoblast activity which was evident within the PRP groups.
This study reports the beneficial effect of PRP combined with BCP; however, the combination of PRP and calcium phosphates for bone healing has also been reported to be of no benefit. Both Wiltfang et al. 84 and Plachokova et al.85,86 reported that the addition of PRP did not provide any benefit to the calcium phosphate bone graft substitute. However, the animal model selections may have confounded their results. Well-characterized bone defect models are critical to ensure treatments are suitably assessed. The present study included empty control defects (negative controls) to assess the normal healing response, which confirmed that the defect did not heal at 4 weeks. Wiltfang et al. 84 reported that the addition of PRP to HA or β-TCP was not able to significantly improve the healing of critical-sized cranial bone defects in mini-pigs at 2, 4, or 12 weeks. However, the very close proximity of defects to one another may have confounded the results of their study, in which the chemotactic and mitogenic factors being investigated may have inadvertently influenced all defects, and contributed to the inability to detect differences between the study groups. Plachokova et al.85,86 reported that PRP was unable to improve the bone healing of a biphasic 60%HA/40%β-TCP in rats. However, the authors themselves identified that the very young, 11–12 week-old animal's defects were not critical in size, with even the empty defects healing spontaneously.
The present study also used 5 year-old female sheep to reduce any incidence of spontaneous healing. In addition, the older-aged animals in this study were considered as providing a more challenging healing environment than their younger counterparts, thus placing greater emphasis on the efficacy of PRP. Aged animals have a lower capacity for bone repair than their younger counterparts, 87 possibly due to an age-related decline in stem cell function, and a decrease in growth factor efficacy and receptor expression.88–90 Factors such as this may contribute to the difficulties found when translating therapies from preclinical to clinical scenarios. Hence, this study was designed to use older-aged, skeletally mature animals.
In this study, the PPP had a platelet concentration of approximately one-tenth of the PRP, and one-third the TGF-β1 concentration; however, both the PRP and PPP significantly improved the healing outcomes over the BCP alone. Therefore, other plasma constituents may contribute to an increase in the bone-healing ability. The PPP had a significantly higher fibrinogen concentration than the PRP. When PPP was combined with the BCP, a greater osteoblast presence and increased bone ingrowth depth was found in the central region of the defect. However, while a different pattern of healing was evident, this did not result in a significant difference in the actual new bone volume when quantified with histomorphometry. Therefore, the addition of PPP to BCP appeared to influence the location of the new bone within the defect, and, to a lesser extent, the actual quantity of bone. This may be attributable to the fibrin. During normal healing, both fibrin and platelets form the basic elements of the hematoma, providing structural and biological components that are necessary for healing. 6 Fibrin, while incapable of supporting critical-sized bone defect healing on its own,30,32,91 may work synergistically with the BCP and provide an enhanced cell supporting graft. The result of this study aligns with studies by Torigoe et al. 92 and Le Nihouannen et al., 93 both of whom reported that the fibrin matrix has the potential to further support bone formation when used in conjunction with calcium phosphates. Fibrinogen appears to be an important feature of PRP that is often overlooked and not reported. The seminal work by Marx et al. 11 cites Tayapongsak's et al. 10 novel use of fibrin adhesive for mandible continuity reconstruction, before the development of PRP, highlighting the potential benefit of the fibrinogen within the PRP. The concentration of fibrinogen within the plasma should be reported in future comparative studies to appreciate the role of fibrin. Based on the results of this study, the fibrin matrix that forms appears to contribute to, and possibly enhance, the osteoconductivity of the BCP.
Dose-dependent response
The characterization of PRP is complex due to the number of variables, and the optimal dose of activated platelets for bone healing is yet to be elucidated. Reporting a concentration does not indicate a dose without reporting the volume of that concentration delivered. As such, reported therapeutic platelet concentrations of >200×109/L 94 or 1000×109/L 95 may not properly translate to a PRP dose. This study used a PRP of a mean 2.9-fold (2.9f) increase, at three different volumes, and combined this with 2 cc of graft material. These resulted in three groups: 1 mL@2.9f:1 cc of graft volume for the maximum-dose group (PRP-100), 1 mL@2.9f:1.5 cc for the medium group (PRP-66), and 1 mL@2.9f:3 cc for the low-dose group (PRP-33). Since PRP has had limited success without an osteoconductive scaffold,30,32,46,91 its use is described here as a ratio of PRP volume to graft volume. Values within similar animal bone defect healing studies using PRP and synthetic bone graft substitutes have been 1 mL@5.0f:0.05 cc, 96 1 mL@4.1f:1.25 cc, 1 mL@6.5f:1.25 cc, 84 1 mL@5.1f:5 cc, 45 1 mL@4.5f:0.13 cc, 97 1 mL@2.0f:0.3 cc, 30 and 1 mL@5.5f:1.5 cc 98 ; however, while platelet concentrations are always provided, actual dose:graft ratios cannot be derived from many studies.46,67,85,99–101 It is apparent that a very wide range of preclinical variations have been applied to bone defect healing studies. No preclinical standard has been set with regard to PRP volume and concentration to graft volume; hence, clinical investigations have no clear indication for use.23,49
Despite a thorough review of the literature, no in vivo studies were found that have compared dosages in a comparable method within a single large animal study using synthetic bone graft substitutes. The results, though, are comparative with Nagata et al., 36 who have previously reported a similar dose-dependent effect when combining autograft and PRP in rats. Their study used a very high ratio of PRP to autograft compared with this study, which was at 1 mL@5.7f:0.067 cc, while using 50–150 μL of PRP. Weibrich et al. 102 have also reported a dose-dependent effect on implant osseointegration; however, they reported that the highest concentration group was inferior to a lower concentration group. In vitro studies have reported a PRP dose-dependent effect on osteoblast proliferation, 103 and also suggested that an upper threshold exists in vitro.71,73,74 However, due to the inability of MSC chemotaxis to occur in vitro, it is difficult to directly translate these in vitro findings to an in vivo dose effect. The in vitro effects due to growth factors are limited to proliferation and differentiation of a preselected number of cells. Conversely, the cellular density is an unknown within the in vivo system. Therefore, the effect of the dose requires further comparative in vivo investigations to provide an additional context to the dose data within this study.
Within the scope of this study, for a given defect volume, the optimal dose of PRP is delivered when the PRP volume and graft volume are matched, and a three-fold PRP is used. In order to reproduce the results of this study, a 1:1 volume ratio of PRP to graft can be considered a suitable indication for PRP use when used in combination with a BCP. This study has shown that the PRP dose should be considered when using PRP. The potential of higher doses can only be confirmed with further investigation.
Since growth factors released from platelets remain the ultimate governors of cellular processes, platelet concentration itself may be misleading. The TGF-β1-fold increase within this study is in the range commonly reported for TGF-β1in PRP.28,67,96,104,105 The results of this study indicate that TGF-β1 concentrations are not strongly correlated to the platelet concentration, which is in agreement with other studies.28,104,106,107 Conversely, a strong correlation between platelet and growth factor concentrations has also been reported.27,95,108 Dugrillon et al. 109 reported a correlation between platelet number and TGF-β1 to 800 g, above which no correlation was found. In addition, since granular release is dependent on distinct intracellular signaling pathways from specific agonists, 110 growth factor release may be influenced by the processing methods, not only the platelet concentration.
This study was not able to find any effect from the leukocyte dose. The PRP had a lower-than-baseline leukocyte concentration, while the PPP had no detected leukocytes. Both neutrophils and monocytes play essential roles in immunity, and while they can destroy necrotic tissue, 111 they can also assist in the healing of many tissues.112,113 Since the PPP did not contain any leukocytes, nor any noticeably different inflammatory response, the effects of neutrophils, monocytes, or any other leukocytes are difficult to assess within this study. Whether or not to include leukocytes in the PRP remains in question. 25 Further studies are needed to justify the inclusion of leukocytes in PRP when used for bone healing.
Comparison to autograft
The autograft has a long history of use, and it is commonly accepted as the gold standard in bone grafting, against which alternatives are judged.2,50,59,114,115 However, the use of autograft needs to be considered as a panoptic process, and not purely as an implantable product. Ideally, the autograft would have unlimited availability, and it would be free from any associated morbidity. However, it is limited in quantity and can have considerable complications.3,4 While the autograft may consistently improve bone healing at a defect site, it also consistently diminishes the form and function of another site within the body. Therefore, comparative treatments may not necessarily need to outperform the autograft to justify their surgical use.
Within both the BCP and empty groups, bone progressed through appositional formation, in which bone formed from the peripheral margin inward. The autograft, however, induced bone formation via both appositional formation and creeping substitution from the central axis the defect outward, though this orthotopic site is not proof of osteoinductivity. 116 The dense layering of osteoblasts on the surface of the autograft bone was suggestive of a high expression of cell signaling molecules that induced these cellular responses. However, the results of this study did not indicate that the overall chemotactic and mitogenic effect was superior to the PRP groups; however, the pathways inducing this activity may be very different. Bone morphogenetic proteins (BMP) are embedded within the extracellular matrix by osteoprogenitors, osteoblasts, and MSC during bone remodeling.117,118 On implantation, osteoclastic resorption of the matrix releases these BMPs into the environment to stimulate new bone formation.119,120 Since platelets release many factors other than BMPs,121,122 the signal transduction pathways within the responder cells may have been quite different between the two groups. Based on these histological findings, it did not appear that the different signaling mechanisms between PRP and the autograft had a substantially different effect on the osteoblastic response at 4 weeks.
A difference in the temporal response was found between the autograft and PRP. As detected by fluorochrome staining, the autograft was found to have much greater bone activity within the central region of the defect at week 1; whereas the PRP groups had fluorochrome staining that was evident only at week 2 and from three onward. Autograft is considered as providing osteogenic cells,1–3 and any osteogenic precursors available within the autograft may be responsible for the early response within the autograft group. Autograft bone healing occurs in two phases, in which cells from the graft first contribute to the new bone formation, and during the second phase, infiltrating cells contribute. 2 Harvested bone has been shown to express BMP and vascular endothelial growth factor (VEGF) receptors 123 and also contain mesenchymal progenitors,124,125 indicating that the autograft is highly receptive to any signals on harvest. This may account for the early activity within the autograft groups that was not evident in any of the other groups.
PRP mechanisms of bone healing
During the inflammatory phase of healing, MSC chemotaxis occurs in which MSCs accumulate at the site, driven by platelet-derived growth factor (PDGFs), fibroblast growth factor (FGF), and BMPs.126,127 This inflammatory phase may be the cause of the low bone formation during the first week, at which time the main purpose of the phase was MSC recruitment. This inflammatory phase is the point at which MSC fate is decided by the stability of the defect,128,129 which in this study, was mechanically stable and resulted in the direct transition to osteogenesis. During this next phase, angiogenesis and the osteogenic proliferation and differentiation of MSC occurs, being driven by VEGF, PDGFs, FGF, TGF-βs, and other supporting factors.79–81,127,130–138 It may be that within the first 2 weeks, the platelet-released growth factors had the greatest contribution by supporting MSC chemotaxis, proliferation, and differentiation. This process could account for the higher density of osteoblasts within the PRP-treated groups, while the BCP did not benefit from this early additional expression of cytokines. This timeline could also help explain the high staining of the week 3 fluorochrome labeling in the defect, in which at week 3 osteoblasts were actively laying osteoid. Before this, the osteoblasts may have been predominantly undergoing mitosis or being differentiated. Bone-healing pathways follow a specific temporal pattern,128,139 in which inflammation peaks within the first week and cytokines that are responsible for osteogenic response peak many days later, followed by a down-regulation. 81 Hence, the addition of the activated PRP may have had an early influence during the inflammatory and early osteogenic phases of healing. These additional growth factors may be responsible for the increased number of osteoblasts found within the PRP groups that were not found when the BCP was used alone. This possible explanation is based on the data available from this and previous studies; however, more detailed investigations at shorter timepoints are needed to confirm this process.
Recombinant alternatives
The growth factors present or released by the PRP appear to have provided cellular signals that have induced new bone formation. However, any advantage of this combination of platelet-released factors compared with an exogenous application of single growth factors remains uncertain. The application of recombinant growth factors, especially BMP, has previously been reported to be beneficial for bone healing in preclinical models140–144 ; however, as with PRP, studies also report no benefit.145,146 One of the most advantageous features of recombinant growth factors is the ability to accurately control the dose, which enables a greater ability to interpret and compare outcomes. The dose of PRP is commonly differentiated by the platelet concentration, which was shown in this study to be unable to fully characterize the PRP's capability.
An advantage of PRP is that it provides a range of factors which may support healing, whereas recombinant factors often only provide one factor. It is not yet clear whether a single factor can serve the temporal needs of the bone-healing environment. While comparisons have been made in previous studies between the BMPs and platelet-released growth factors, 147 it has not yet been elucidated whether there is an optimal combination of these factors. Since platelets release none to very low concentrations of BMPs,121,122 combination therapies with both recombinant BMP and autologous PRP may provide improved treatment options.
Limitations
Highly concentrated PRPs have been reported to have an inhibitory effect on osteoblast function.73,102 However, only one study could be identified that supports this theory in vivo. 102 Since the platelet concentration in this present study was well within the normal range, whether such an upper threshold exists could not be confirmed. Growth factors induce cellular signals on receptor expressing cells, and the application of excessive signals may not provide any further benefit if there is a saturation of ligands. Whether an overdose of PRP would result in no added benefit, or inhibit new bone formation, requires further in vivo studies.
This study only quantified TGF-β1, which is involved in MSC proliferation and osteogenic differentiation, and possibly osteoclast inhibition. Enumeration of other factors, such as PDGF-BB and VEGF, may have provided further insights into the ability of specific growth factors to influence specific endpoints. However, since many factors have been shown to influence bone healing, such as FGF,80,130–133,138 hematopoietic growth factor (HGF),135,148 insulin-like growth factor (IGF),130,149,150 and many other chemokines and pro-inflammatory cytokines,69,130,151,152 it would not be feasible to fully characterize all PRP products. TGF-β1 has provided a useful insight into the correlation between platelet count and growth factor concentrations. It has also provided an insight into the relationship between TGF-β1 dose and healing outcomes.
The time point of 4 weeks was selected based on the review of the literature combined with an understanding of the bone-healing timeline and theoretical potential of PRP. Whether PRP had an early effect on bone healing needed to be investigated. Since this study has investigated the early benefit of PRP, later time points could now be used to demonstrate and confirm any longer-term benefits of PRP application and dosing. Finally, mechanical testing is relevant to a load-bearing tissue such as the bone and has been applied in similar models, 153 but was not applied here. Destructive testing would not have allowed the level of investigation that was achieved in this study. Even minimally destructive tests such as nanoindentation require tissue to be removed to expose the bone and would have again negatively affected results.
Conclusion
This study examined the in vivo response of a BCP with and without PRP and PPP. The addition of PRP significantly improved the bone-healing ability of the graft material in a critical-sized defect in aged sheep. The optimal use of activated PRP was achieved when a three-fold PRP was mixed at a 1:1 volume ratio of PRP (mL) to graft (cc). At lower PRP volume ratios, PRP still provides a significant improvement compared with the graft material alone. Further investigation is required to determine whether higher PRP doses have even greater benefits. However, it remains pertinent to consider dose as a product of the concentration and the volume. Furthermore, platelet dose may not be an accurate measure of the growth factor dose. The BCP failed to induce bone formation over an empty defect, suggesting that its use is limited for bone healing without the addition of growth factors. Both autograft and PRP provided comparable cellular signals at 4 weeks; however, bone formation within the defect occurred earlier with the autograft. Fibrinogen concentration and activation protocols are important considerations, and they appear to affect PRP efficacy for bone healing. Further investigations are required to elucidate the effect of the leukocyte concentration. Overall, this study found that activated autologous PRP provides access to growth factors which are able to induce new bone formation in vivo, and that this effect is dose dependent.
Footnotes
Disclosure Statement
No competing financial interests exist.