
Abstract
Background:
Absorbable collagen sponge (ACS) loaded with bone morphogenetic protein-2 (BMP-2) is approved for selected clinical applications; however, burst release limits its widespread use. Therefore, nanofiber (NF)–based scaffold with ACS backbone was developed to sustain release of loaded BMP-2 to improve the outcomes of bone grafting in a rodent model of cleft palate.
Methods:
BMP-2 was loaded on ACS scaffold and then NF hydrogel with different densities (1–2%) was added to sustain the BMP-2 release. The release profiles of BMP-2 from constructs with different NF densities were evaluated in vitro to explore the optimum NF density that could recapitulate physiological bone healing process. Subsequently, scaffold with the appropriate NF density was implanted into a rodent model of cleft palate. Wistar rats, with surgically induced maxillary cleft defects, were then assigned to one of the following groups (n=6/group): no scaffold (control), ACS, ACS+BMP-2, NF+ACS, and NF+ACS+BMP-2. Micro-computed tomography (μCT) was utilized to evaluate percent bone filling (%BF) at defect site as well as changes in anteroposterior and transverse dimensions of the maxilla at weeks 0, 4, and 8. Histological assessment of bone healing was performed at week 8.
Results:
In vitro release experiments showed that scaffolds containing 2% NF exhibited a release profile conducive to the natural stages of bone healing and, hence, it was utilized for subsequent in vivo studies. Bone healing occurred at the defect margins leaving a central bone void in the control, ACS, and NF+ACS groups over the 8-week study period. BMP-2-treated groups demonstrated higher %BF as compared with other groups at week 8 (p<0.05). Whereas the NF+ACS+BMP-2 group showed bone bridging of the defect as early as 4 weeks, which was not evident in ACS+BMP-2 group. In all groups, bone grafts did not disrupt anteroposterior and transverse growth of maxilla. Based on histological evaluations together with μCT data, NF+ACS+BMP-2 treatment resulted in clinically significant and consistent bone healing throughout the implanted scaffold when compared with the ACS+BMP-2 group.
Conclusion:
NF+ACS+BMP-2 constructs exhibited osteoinductive properties together with preparation simplicity, which makes it a novel approach for BMP-2 delivery for cleft palate reconstruction.
Introduction
S
Several studies demonstrated the efficacy of BMP-2 for enhancing bone healing; thus, it was approved by the Food and Drug Administration (FDA) for selected human applications. 13 However, its use for cleft palate reconstruction has been done in an off-label capacity. The main benefit of ACS+BMP-2 construct is to provide bone formation similar to autografts, but without donor site morbidity.6–10 The major issue of this strategy is that milligram doses (1.5 mg/mL) of BMP-2 were needed to achieve those therapeutic effects, when ACS was utilized. Recently, a study employed a chemically crosslinked hydrogel in patients with cleft palate and demonstrated moderate bone formation at a reduced BMP-2 concentration (250 μg/mL). 14 However, severe gingival inflammation and initial exposure of BMP-2 hydrogel construct occurred in two participants of this study 14 and, therefore, the study was prematurely terminated. Reducing BMP-2 concentration needed for bone formation is a major goal of continuing research, as it will reduce both the adverse effects and the overall therapeutic cost. However, successful clinical application of this strategy largely depends upon the use of an appropriate carrier.
Scaffold properties of concern are biocompatibility, biodegradability, cell adhesiveness, and interconnectivity. Self-assembling peptide, nanofiber (NF)–based hydrogel RADA4, (Arg-Ala-Asp-Ala)4, is a biologically inspired biomaterial that is comprised of natural amino acids, which can be safely metabolized by the body. Moreover, its 3D structure is similar to the natural extracellular matrix with ∼10-nm fiber diameter and 5–200-nm pore size. 15 Studies have reported that NF-based scaffolds support proliferation and osteogenic differentiation of osteoprogenitor cells, suggesting possible application in bone tissue engineering.16,17 NF sustained release of incorporated growth factors, where the release profiles of loaded proteins could be adjusted by altering NF concentrations.18,19 Recent work has evaluated the efficacy of a self-assembling heparan binding peptide amphiphile (HBPA) combined with ACS to deliver BMP-2 in femoral defects in rats. 20 In this study, one of six femoral defects showed bone bridging the defect in BMP-2-treated group and four of six defects showed bridging with the addition of heparan sulfate (HS). Although this study was able to show bone bridging with low BMP-2 concentration (1 μg), this required high HS concentration (1.2 mg). However, literature regarding the influence of HS on bone growth is controversial. For example, another recent study reported that a low HS concentration (5 μg) enhanced bone formation as compared with 50-μg HS group; values that are vastly different than the 1.2 mg reported with BMP-2 incorporation. 21 In fact previous work has reported that HS has positive, negative, and/or no effect on bone healing.22,23 Moreover, unlike BMP-2, HS is not approved for clinical use. Therefore, the efficiency of HS was not investigated in our study.
Toward that end, we developed an NF-based scaffold (with ACS backbone) to control the BMP-2 release for improved bone healing in a rodent model of cleft palate. The main aim of this study was to provide the necessary “proof-of-principle” for developing and transferring NF and BMP-2 technology in cleft palate defects. The release profiles of BMP-2 from constructs with different NF densities were evaluated in vitro to explore the optimum NF density that could recapitulate physiological bone healing process. Subsequently, scaffold with the appropriate NF density was implanted into a rodent model of cleft palate and bone healing was assessed using micro-computed tomography (μCT) and histology.
Materials and Methods
Materials
ACS was purchased from BARD, Davol, Inc., BioXclude™; placental resorbable membrane (PRM) was obtained from Citagenix, Inc. Self-assembling peptide RADA4 was purchased from RS Synthesis, LLC., and used without further purification. Stock peptide was reconstituted in ddH2O. BMP-2 was obtained from an Escherichia coli expression system, and its activity has been testified in the literature.24,25 Stock BMP-2 solution was prepared in ddH2O. Fluorescein isothiocyanate (FITC) was obtained from Sigma-Aldrich, and it was used to label the BMP-2 according to manufacturer's instructions.
In vitro release study
To identify the proper NF concentration suitable to sustain BMP-2 release, different NF concentrations (1% and 2% w/v) were prepared by diluting stock peptide solution in PBS. Aliquots (30 μL) from the prepared solutions were applied onto 6-mm ACS discs impregnated with FITC-labeled BMP-2 (8 μg). ACS discs that were infused with FITC-labeled BMP-2 (8 μg) were used as controls. Constructs were incubated overnight at 4°C to form the gel. Then, 200 μL of PBS was slowly added as a release media. At predetermined time points, supernatant was sampled (40 μL) and replaced with fresh PBS to determine the amount of BMP-2 released as a function of time using florescent spectroscopy (λExcitation=495 nm and λEmission=525 nm). The average diffusion coefficient was calculated using the following equation
26
:
Where Mt and M∞ are the total mass of diffusing BMP-2 released from the NF after time t and infinite time, respectively. D is the diffusion coefficient of BMP-2 in the NF. H is the gel thickness. The average diffusion coefficient is estimated through linear regression of the Mt/M∞ as a function of t0.5 using GraphPad Prism, version 5.00, GraphPad Software, Inc.
Bone grafting surgery
Steps for standardization and scaffold preparation
Several steps were completed to develop a standardized surgical defect and scaffold to minimize variation (Fig. 1). An impression was taken of the rat maxillary arch with a prepared surgical defect (7 transversely×2.5 anteroposterior×1 depth mm3) from which a stone model was fabricated and a surgical template was created. Multiple templates were prefabricated, sterilized, and used intraoperatively to standardize the MPC defect size for all animals in the study. Moreover, a customized rectangular punch measuring 7×2.5 mm2 was developed and used to precut sterile ACS and PRM into pieces of standardized size. ACS+BMP-2 scaffold was prepared by adding 12 μg of BMP-2 to ACS and allowed to dry for 30 min. Prefabricated rectangular molds (7×2.5 mm2) were then used to prepare NF+ACS and NF+ACS+BMP-2 scaffold of standardized size. ACS+PBS or ACS+BMP-2 scaffold was placed in the mold and rehydrated with 30 μL from aseptically prepared NF solution.

Tools developed to aid standardization for the grafting procedure. MPC preoperative defect (7 transverse×2.5 anterioposterior×1 depth mm3) was developed on a model of rat maxilla
Experimental setup
Animal ethics committee at the University of Alberta approved all experimental procedures (approval No. 703/05/13). Sample size calculation, based on Mariner et al. study 27 with a power of 80%, suggested that 30 animals were necessary to decrease type II error. A total of 34, 16-week-old (375–400 g), Wistar rats were obtained from Charles River Laboratories International, Inc. Animals were kept in standard environment (room temperature, two rats/cage with 12 h light/dark cycle). Animals were provided with soft diet and liquid gel 2 days preoperative and continued for 1 week postoperative and then gradually advanced to regular diet.
Surgery
Intraperitoneal injections of ketamine (75 mg/kg) and domitor (0.5 mg/kg) were used to anesthetize animals before surgery. Lidocaine (0.25 mL of 0.4%) was also injected locally. Then, using a No. 15c sterile surgical blade, a U-shaped incision was performed in a transverse direction posterior to the incisive foramen, following the arch form, and a full-thickness mucoperiosteal flap was elevated to expose the maxillary bone. The MPC defect of 7×2.5×1 mm3 was then created using both No. 699 straight fissure and No. 4 round burs. The surgical template was utilized to ensure defect size standardization in all animals. Description of the bone grafting technique is illustrated in Figure 2. Hemostasis was maintained using a surgical suction and manual pressure. Initially, PRM was inserted into the defect to create a barrier with the nasal mucosa (in all groups except control) and the rats were randomly assigned to one of the following groups (n=6 per group): control (no scaffold), ACS alone, ACS+BMP-2, NF+ACS, and NF+ACS+BMP-2. At the end of surgery, the flap was closed in a primary fashion, using 4-0 polyglactin absorbable sutures, and 1 mg/kg of Revertor (atipamezole hydrochloride) was injected subcutaneously to reverse the sedative effects. Pain management included subcutaneous injections of Metacam at 2 mg/kg (once/day) and Butorphanol at 0.2 mg/kg (twice/day). Subsequently, daily follow-up assessments were performed for 1 week, to evaluate the animals for proper postoperative pain control and stress, which was assessed based on grooming habits, activity, porphyrin staining, level of appetite, or weight changes. Bone healing in the different treatment groups was evaluated by μCT and histology.
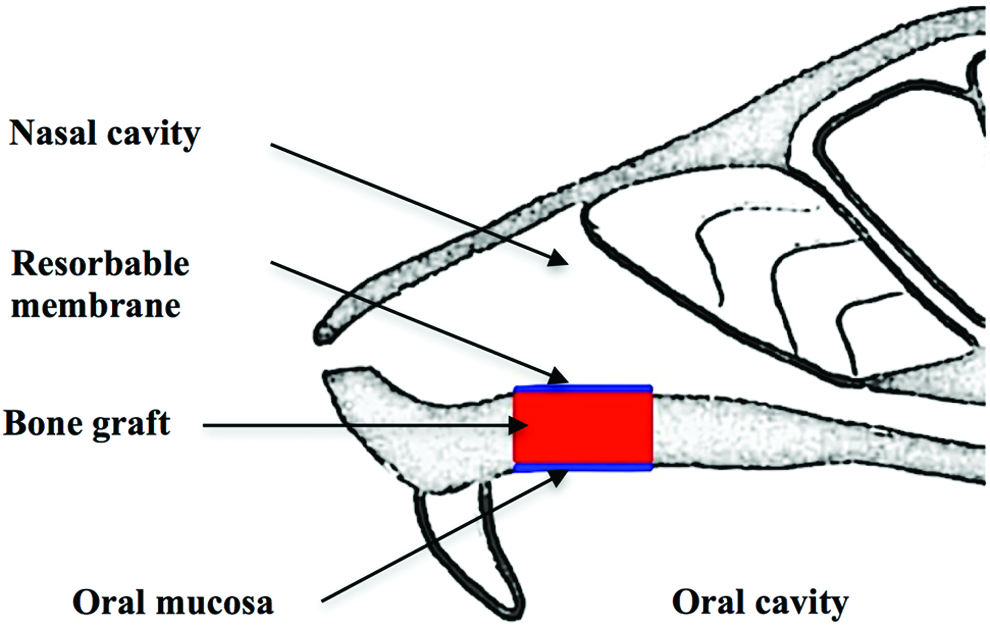
Diagram showing alveolar bone grafting technique viewed from sagittal aspect. PRM was placed as a lining for the nasal cavity, the scaffold was then placed into the developed MPC defect, and oral mucosa was closed with watertight sutures. Color images available online at www.liebertpub.com/tea
In vivo μCT imaging
In vivo μCT scans (Skyscan 1176; SkyScan NV) of rat maxillae were performed at weeks 0, 4, and 8. Rats were anesthetized with 2% isoflurane in oxygen during imaging. All μCT scans were done at 100 kV through 180° with 0.5° rotation step to produce serial cross-sectional images of 18-μm resolution. Projected images of the maxillae were reconstructed using NRecon 1.6.1.5 software (SkyScan NV).
Quantitative and radiomorphometric analysis
Assessment of bone healing
CT images were utilized to assess bone healing in longitudinal scans of the same animal overtime. A fixed rectangular region of interest of 4×9 mm2 was used to section an identical volume of the palatine bone to standardize the analyses. Incisor roots were utilized as the reference anatomical landmarks to sample the same region from all specimens. Skyscan CT-Analyzer software (CTAn 1.10.0.1; SkyScan NV) was used to binarize 2D coronal images with a gray scale threshold of 36/255 to measure bone volume (BV, mm3). Difference between BV at baseline (W0) and subsequent time points (W4 and W8) was described as bone-filling volume, and the percentage ratio between the bone-filling volume and initial defect volume at baseline was defined as percent bone volume (%BV).
Growth measurements
Mimics software (Materialise) was used to measure anteroposterior and transverse dimensions of the maxillae in operated animals (n=6/group). Nonoperated animals were used as control (n=4). Anatomical landmarks established by Gomes et al. 28 were utilized in an axial viewing position. The distances between infraorbital foramen (IF) and incisal point (IP) were measured bilaterally to represent the anteroposterior dimension (IF-IP) while the distance between right and left IF was used for transverse dimensions (IF-IF). All μCT measurements were conducted and reassessed after 1 week by one calibrated examiner.
Histological analysis
All rats were euthanized at the end point (8 weeks) using CO2. Maxillae were dissected and fixed in 10% neutral buffered formalin. Then, samples were washed with PBS and immersed in decalcification solution (Cal-Ex II®; Fisher Scientific) for 4 weeks. Samples were sectioned and stained with hematoxylin and eosin (H&E) and Masson's Trichrome stains (bone=dark blue, cortical bone=red) 29 to assess bone formation at the cleft defect site.
Statistics
In vitro release study was done in triplicate for each scaffold at each time point, while animal experiments were conducted in six animals per group. The results were expressed as mean±standard deviation. Normality of the data was tested using the Q-Q plot in SPSS version 18.0 software package. The Kruskal–Wallis test was then used to determine significant differences between the groups, since this data was not normally distributed. Significance was expressed as p-values<0.05. Additionally, intraclass correlation coefficient (ICC) was used to estimate the intrarater reliability for μCT measurements.
Results and Discussion
In vitro release
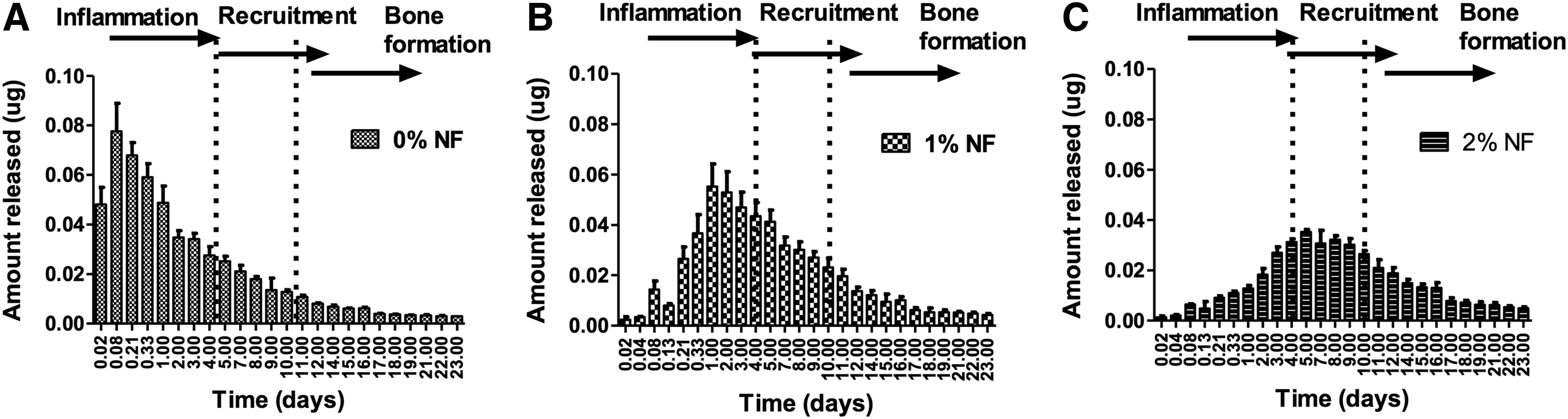
The release rate of BMP-2 has a significant impact on the speed and efficacy of the bone healing process. In vitro release studies were aimed at exploring the optimum NF density that could sustain BMP-2 release to recapitulate physiological bone healing process. BMP-2 was loaded on ACS scaffold and layered with NF hydrogel with different peptide densities. ACS was utilized to provide structural integrity for the hydrogel, to facilitate handling, and to prevent NF migration away from the defect site. The release of BMP-2 from NF+ACS scaffolds into PBS was evaluated at room temperature for 23 days (Fig. 3). ACS alone (0% NF) was used as control. The BMP-2 release demonstrated a dose response with increasing NF concentration. ACS alone exhibited quick BMP-2 release during the initial phase and∼9% (∼78 ng) of its BMP-2 content was released during the first 2 h (Fig. 4A). This was followed by release of gradually decreasing amounts over the 23 days of the study giving a total of 601 ng or 37% of its BMP-2 content. While hydrogel containing 1% and 2% NF released BMP-2 in a slower fashion, and only 9% and 3% of BMP-2 content was released after 24 h, respectively. Constructs containing 1% NF exhibited maximum BMP-2 release after 24 h (∼55 ng or ∼9% of initial BMP-2 content), followed by a gradual sustained release of BMP-2 over 23 days (Fig. 4B). By the end of the experiment, 1% NF released ∼35% (∼541 ng) of its initial BMP-2 content. Constructs containing higher NF (2%) density further delayed the rate and extent of BMP-2 released (Fig. 4C). Scaffold containing 2% NF exhibited maximum BMP-2 release after 5 days: ∼35 ng or ∼10% of initial BMP-2 content. After 23 days, 2% NF scaffold allowed only ∼26% of its BMP-2 content to be released. In conclusion, ∼37%, 34%, and 25% of BMP-2 was released from 0%, 1%, and 2% NF after 23 days, respectively.
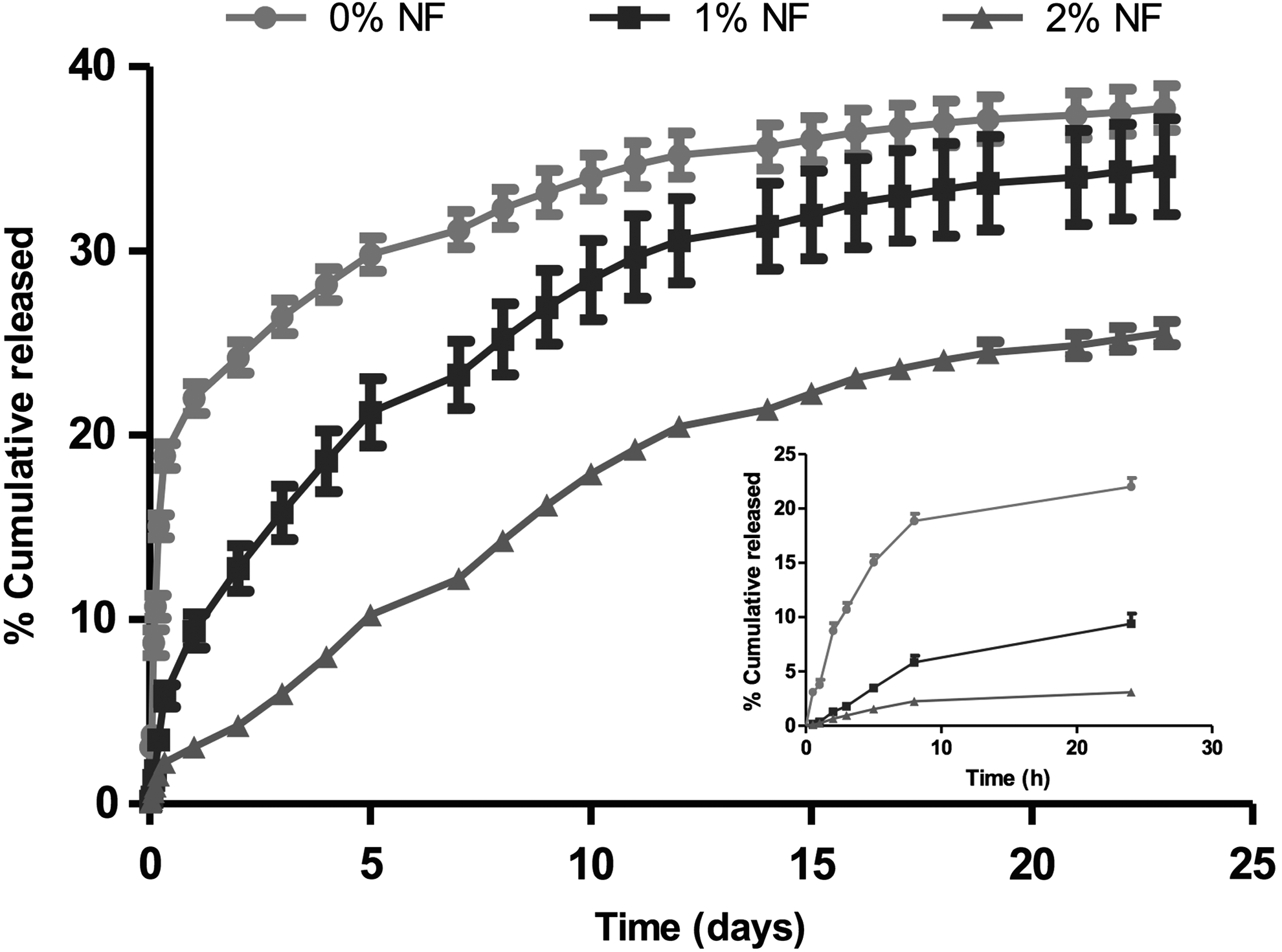
Release profile of fluorescein isothiocyanate (FITC)–labeled BMP-2 from scaffolds with different NF densities (0–2% w/v) over 23 days. Release experiments were performed into PBS at room temperature. Data points represent the mean of % cumulative BMP-2 released±SD (n=3). Inset: Release profile of FITC-labeled BMP-2 from scaffolds having different NF densities (0–2% w/v) over first 24 h.
Release profile of FITC-labeled BMP-2 from scaffolds having different NF densities:
Lee et al. 20 reported the release of ∼75% of BMP-2 from HBPA after 8 days, which was substantially quicker than that observed in this study: 14.2% from 2% NF in 8 days. A structural comparison between HBPA and our NF reveals that NF carries an overall net neutral charge, while HBPA is positively charged. This difference in net charge might explain the rapid release of the positively charged BMP-2. This is in accordance to Gelain et al. study, which demonstrated the charge effect on the release of proteins from hydrogel scaffolds. 18 Moreover, it has been reported that positively charged carriers might have potential systemic toxicity and immunogenicity.30–32
Bone healing consists of well-coordinated series of events, including inflammation, cellular migration, endochondral and/or intramembranous bone formation, and remodeling. 33 The initial inflammation lasts for 3–4 days and migration of stem cells in response to growth factor release initiates the reparative phase; their proliferation and osteogenic differentiation ultimately results in bone formation.33,34 Given this temporal sequence of events, we tried to correlate the timeline of the bone healing cascade reported by Strohbach et al. 34 with our release data (Fig. 4). In this analysis it was apparent that both 0% and 1% NF-ACS scaffolds released larger quantities of BMP-2 during the inflammatory phase, while 2% NF released minimal BMP-2 concentrations during the inflammatory phase and maintained maximal concentrations during the cell recruitment phase. High BMP-2 concentrations during the inflammatory phase could increase inflammation and might adversely inhibit or delay the tissue regeneration process.35,36 Therefore, constructs containing 2% NF were utilized for subsequent animal studies.
Mass-released fraction (Mt/M∞) as a function of square root of time (t) is presented in Figure 5. It demonstrated a linear relationship (r2>0.98), indicating that the release of the BMP-2 from NF hydrogels is diffusion dominated. Average diffusion coefficients were calculated from the slope of the straight line for the three concentrations of NF. The diffusion of BMP-2 from scaffold containing 0% NF showed rapid diffusion exhibiting average 91.92±17.00×10−2 m2·h−1 that was significantly higher than other NF (1–2%) scaffolds. Moreover, the diffusion coefficient was significantly decreased from 32.58±1.09×10−2 m2·h−1 to 24.95±0.66×10−2 m2·h−1 by increasing NF concentration from 1% to 2% (p<0.05).
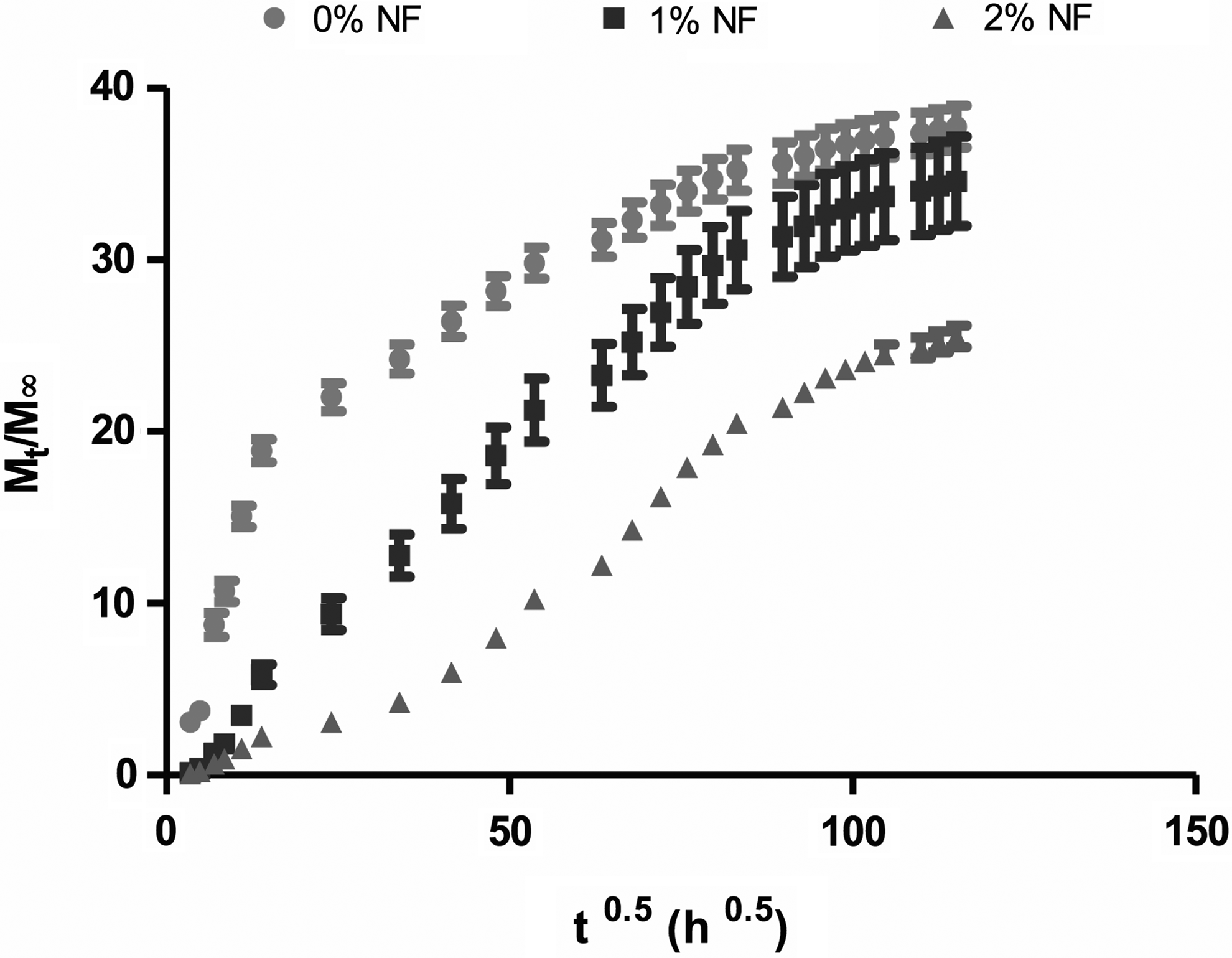
Plot of Mt/M∞ as a function of t0.5 for the release of FITC-labeled BMP-2 from scaffolds with different NF densities (0–2% w/v) over 23 days. Data points are average of n=3 and error bars represent±SD.
In vivo bone grafting
Postoperative recovery
Operated rats tolerated the surgery and maintained normal body weight similar to nonoperated rats. There were no intraoperative mortalities; only one rat in BMP-2 group died postoperatively. This mortality rate (∼4%) is still smaller than other studies that utilized rodent model of cleft palate (∼10%).37,38 All operated rats were scored with mild-to-moderate pain during the first postoperative week that reduced over time. Other studies that utilized rodent model of cleft palate37–39 did not report evaluations of postoperative pain, which is an important addition with our study.
Bone healing following different treatments
Bone regeneration following different treatments was monitored using in vivo μCT imaging that enabled longitudinal assessment of the same rat at weeks 0, 4, and 8 simulating clinical studies. Conversely, other studies37,39 euthanized the animals at 4, 8, and 12 weeks for ex vivo μCT evaluation.
Figure 6 illustrates %BV filling the defect following different treatments. Figure 7 demonstrates bone healing based on 3D reconstructed μCT images. Minimal bone healing occurred at the defect margins in control, ACS, and NF+ACS groups over the 8 weeks of the study. None of the animals in these groups had complete defect closure with new bone formation. There were no significant differences in the %BV between control, ACS, and NF+ACS groups at week 4 (29.43±6.51, 27.09±15.71, and 23.94±7.99, respectively) and week 8 (37.72±12.00, 40.14±15.12, and 22.43±5.98, respectively). Nguyen et al. 39 compared bone formation with the following treatments: ACS, ACS+BMP-2, hydroxyapatite tricalcium phosphate (HA-TCP), and HA-TCP plus BMP-2. They reported significant bone healing in ACS-treated groups as compared with untreated control based on percent bone formation at week 8 (79±9 vs. 53±8, respectively). However, the Nguyen study 39 utilized 8-week-old Sprague Dawley rats while our study utilized 16-week-old Wistar rats. Young animals are expected to heal faster than older animals due to the increased proliferative capacity of younger cells. This is consistent with Ekeland et al. 40 study that reported that healing femoral fractures regained the mechanical properties of normal bones after 4 weeks in young rats (3-week-old rats) and after 12 weeks in adult rats (14-week-old rats).
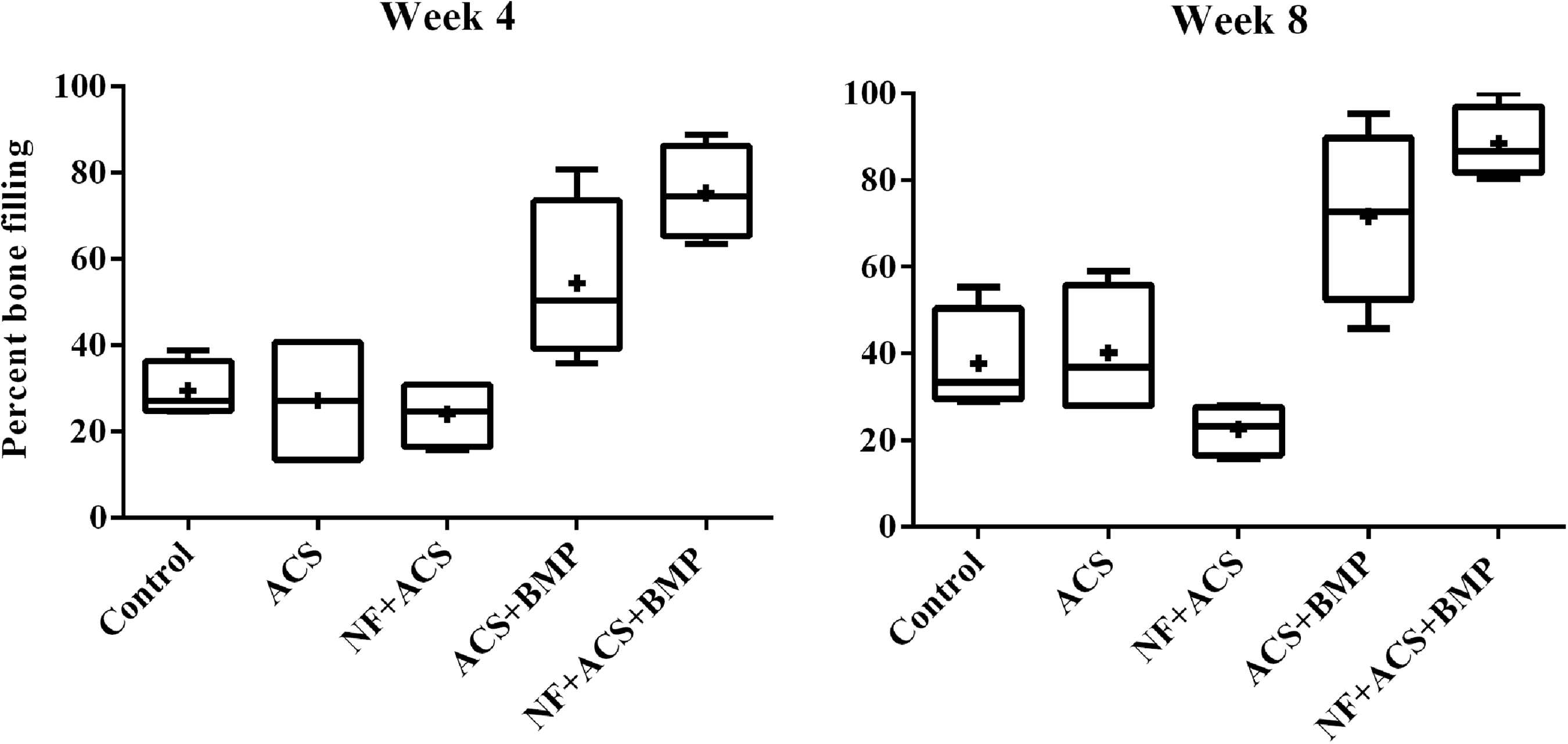
Box plot diagram for percent bone filling following different treatments at weeks 4 and 8. Comparison of 5 treatments: - represents median,⊥represents minimum, T represents maximum, and+represents mean. Boxes: 25th and 27th percentiles.

Representative ventral view of three-dimensional (3D) reconstructed micro-computed tomography (μCT) images illustrating MPC defect healing over 8 weeks following different treatments. Color images available online at www.liebertpub.com/tea
Interestingly, the addition of BMP-2 considerably enhanced bone healing at the defect site as compared with other groups. Bone formation in ACS+BMP-2 group was significantly different from control, ACS, and NF+ACS groups at week 8 (p<0.05) but not at week 4. Whereas %BV in NF+ACS+BMP-2 group was significantly higher than control, ACS, and NF+ACS groups at weeks 4 and 8 (p<0.01). Bone-filling percentage in NF+ACS+BMP-2 group was higher than ACS+BMP-2 group at week 4 (75.31±10.86 vs. 54.29±18.90, respectively) and at week 8 (88.4±8.32 vs. 71.59±20.29, respectively), but this difference was not statistically significant. Most importantly, however, the NF+ACS+BMP-2 group showed significant bone bridging across the defect as early as 4 weeks, which was not evident in ACS+BMP-2 group.
Histological assessments of bony defects at week 8 confirmed the μCT results (Fig. 8). H&E staining for ACS and NF+ACS groups displayed fibrous tissue filling the defect with limited bone regrowth at the defect margins, while BMP-2-containing constructs exhibited osteoinductive properties. ACS+BMP-2 treatment resulted in partial closure of the defect, while NF+ACS+BMP-2 treatment showed central and peripheral bone formation in the defect site. The thickness of the regenerated bone was greater in the latter group. Masson trichrome staining (Fig. 8) was performed to further characterize the maturation of the newly formed bone. ACS+BMP-2 group demonstrated both woven bone (blue) and mature bone (red), but NF+ACS+BMP-2 group showed more mature bone and increased bone thickness in the regenerated area.
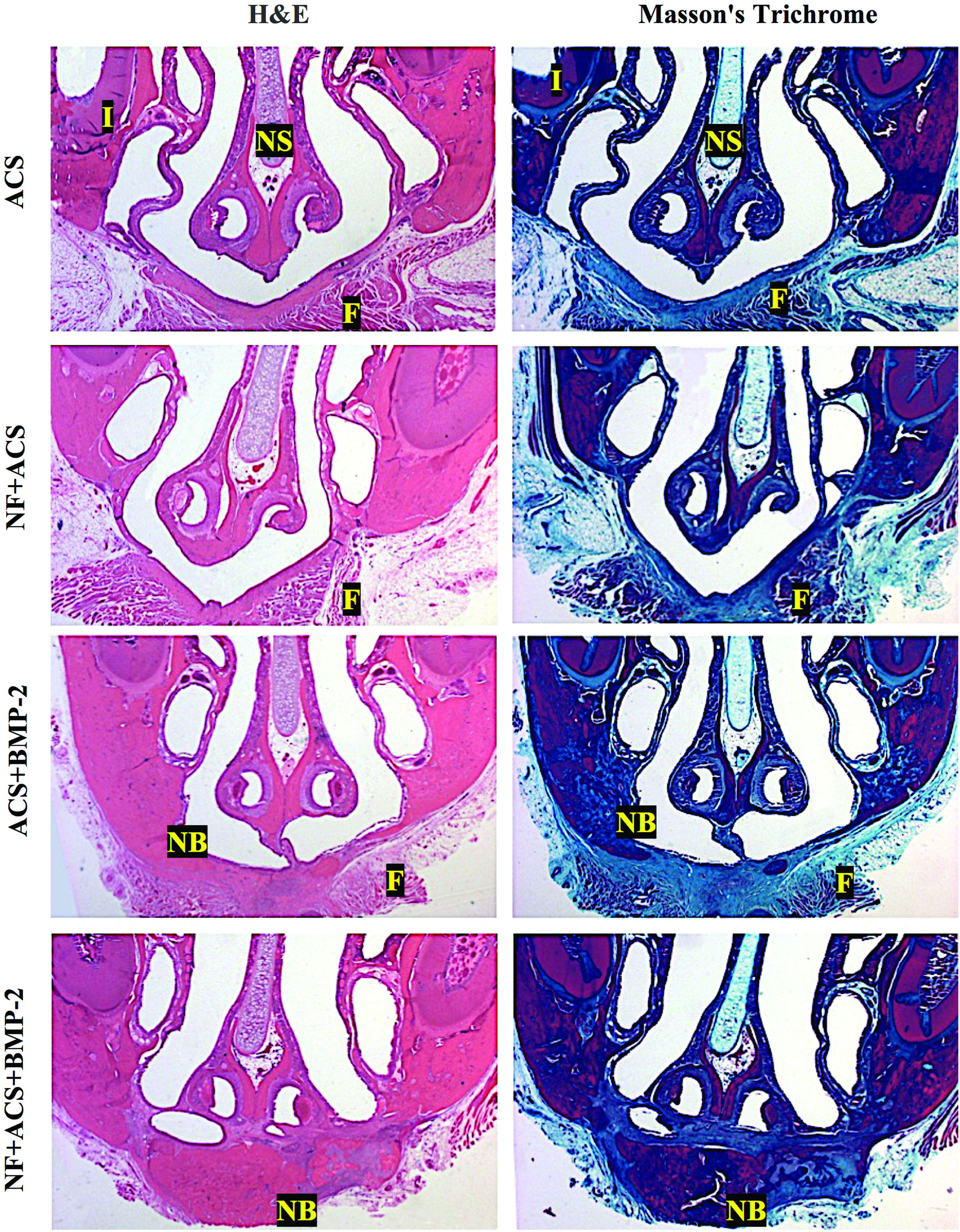
Representative coronal histological sections (1.6×) of MPC defect comparing bone healing between different treatments at week 8. Sections are stained with hematoxylin & eosin (H&E) and Masson's trichrome stain (bone=dark blue, cortical bone=red). I, incisors; NS, nasal septum; F, fibrous tissue, and NB, new bone. Color images available online at www.liebertpub.com/tea
In our study, four of six clefts treated with NF+ACS+BMP-2 demonstrated bone bridging based on both radiographic and histologic assessments, which almost restored the osseous defects at week 8. The other two animals presented fibrous healing with minimal bone formations at the defect margin similar to ACS and NF+ACS groups. Within the ACS+BMP-2 group, three defects had substantial bone formation extending from each margin with a central residual defect while the other three defects progressed to fibrous healing based on both radiographic and histologic evaluations. These results could explain why there were no statistically significant differences in bone volume between NF+ACS+BMP-2 and ACS+BMP-2 groups, obviously due to the sample size. However, the most important clinical and radiographic criteria for successful bone grafting in cleft palate is the formation of bone bridging the cleft defect. 3 Based on histological evaluations and both H&E and trichrome staining, together with cross-sectional μCT images (Fig. 9), NF+ACS+BMP-2 treatment resulted in more clinically significant and consistent bone healing throughout the implanted scaffold when compared with ACS+BMP-2 group.

Representative μCT images comparing bone healing at week 8 in MPC defects (arrow) treated with ACS+BMP-2 and NF+ACS+BMP-2 in the three reference planes (coronal, axial, and sagittal).
Conversely, Nguyen et al. 39 could not reveal significant effect for BMP-2 (4.4 μg/implant) loaded on ACS and HA-TCP when compared with ACS and HA-TCP alone over 12 weeks. This could be due to quick release of BMP-2 from the scaffolds used, low BMP-2 concentration, and/or ineffective handling of the soft tissue closure leading to substantial early loss of BMP-2. These shortcomings were addressed in our study through the utilization of NF hydrogel scaffold to sustain BMP-2 release in vivo. Our decision to utilize a higher BMP-2 concentration (12 μg/implant) was based on osteoinductive concentrations used in other animal studies that investigated bone healing in maxillofacial41–43 and femoral defects 44 that were normalized to MPC defect size. However, future studies are needed to investigate the minimum effective BMP-2 dose required for bone formation in MPC model. It is also important to mention that temporal sequence of bone healing differs between rodents and humans; therefore, further optimization of effective BMP-2 and NF concentration is a possible consequence before transferring this technology into clinical setting to accommodate larger defects and slower healing capacity in humans.
Effective soft tissue handling is essential to maintain BMP-2 at the defect site and to prevent early loss of BMP-2 into nasal and/or oral cavities. Thus, PRM was placed to seal the nasal cavity, the scaffold was then placed into the defect, and oral mucosa was closed with watertight sutures. These modifications appeared valid and enabled the appraisal of the osteoinductive potential of BMP-2-loaded constructs. Although all of the experimental groups were implanted with PRM except controls, bone healing was similar between ACS and NF versus untreated control. This rules out the possibility that PRM plays a role in bone formation and confirms that its main function was to provide nasal seal. To our knowledge, this is the first animal report to employ a nasal seal to improve the outcomes of bone grafting. Although the functionality of released BMP-2 was not directly assessed in this study, NF+ACS+BMP-2 treatment improved bone healing in vivo when compared with ACS+BMP-2 group, suggesting BMP-2 activity.
Effect of different treatments on maxillary growth
Comparing the anteroposterior and transverse dimensions in operated rats with different bone grafts versus nonoperated (control) rats revealed no differences over 8 weeks (Table 1). Additionally, there were no significant differences in IF-IP or IF-IF dimensions between weeks 0, 4, and 8 within each group. Moreover, there was no significant difference in IF-IP dimensions between right and left sides in each group confirming palatal symmetry. All dimensions were measured and re-examined after 1 week by one operator. The intrarater ICC was 0.99 with narrow confidence interval, indicating accuracy and reliability of the measurement method.
IF-IP represents the anteroposterior dimension, while IF-IF represents the transverse dimensions.
ACS, absorbable collagen sponge; BMP-2, bone morphogenetic protein-2; IF, infraorbital foramen; IP, incisal point; NF, nanofiber.
The effects of BMP on craniofacial growth remain understudied. To our knowledge, only one study was completed in growing minipigs (2 months old), which compared bone healing in 2×4 cm2 parietal defects reconstructed with BMP-7+ACS+carboxymethyl cellulose versus autografts. 45 That study reported that BMP-7 implantation did not disrupt cranial growth and development, which is consistent with our results.
Conclusions
Every attempt was made to simulate the clinical situation to facilitate future translation to human applications. In vitro studies demonstrated that the release profile of 2% NF construct recapitulated physiological bone healing process. In the in vivo studies, PRM was placed to seal the nasal cavity, followed by the scaffold, and oral mucosa was closed with watertight sutures. In vivo μCT imaging allowed longitudinal analysis of bone regrowth of the same animal overtime.
The presented modifications appeared valid and enabled the evaluation of the osteogenic potential of our constructs. NF and BMP-2 in the concentration and conditions utilized enhanced de novo bone formation. NF+ACS+BMP-2 group demonstrated bone bridging the defect, which was not evident in the ACS+BMP-2 group. Bone bridging is the most important radiographic criteria for successful cleft palate reconstruction.
In conclusion, NF+ACS+BMP-2 constructs exhibited osteoinductive properties together with incredible simplicity of the preparation, which makes it a novel approach for BMP-2 delivery for cleft palate reconstruction.
Footnotes
Acknowledgments
This study was supported by Fund for Dentistry, CIHR and AIHS grants. The authors would like to thank K.L.S. Martin for providing Bien Air surgical hand piece (free of charge) during surgery times and Citagenix, Inc., for providing sample PRM. We also thank Prosthodontics lab technicians (University of Alberta) for the surgical templates.
Disclosure Statement
No competing financial interests exist.