
Abstract
The Industry Committee of the Tissue Engineering Regenerative Medicine International Society, Americas Chapter (TERMIS-AM) administered a survey to its membership in 2013 to assess the awareness of science requirements in the U.S. Food and Drug Administration (FDA) regulatory process. One hundred forty-four members responded to the survey. Their occupational and geographical representation was representative of the TERMIS-AM membership as a whole. The survey elicited basic demographic information, the degree to which members were involved in tissue engineering technology development, and their plans for future involvement in such development. The survey then assessed the awareness of general FDA scientific practices as well as specific science requirements for regulatory submissions to the Center for Biologics Evaluation and Research (CBER), the Center for Drug Evaluation and Research (CDER), the Center for Devices and Radiological Health (CDRH), and the Office of Combination Projects (OCP). The FDA-specific questions in the survey were culled from guidance documents posted on the FDA web site (www.fda.gov). One of the answer options was an opt-out clause that enabled survey respondents to claim a lack of sufficient awareness of the topic to answer the question. This enabled the stratification of respondents on the basis of confidence in the topic. Results indicate that across all occupational groups (academic, business, and government) that are represented in the TERMIS-AM membership, the awareness of FDA science requirements varies markedly. Those who performed best were for-profit company employees, consultants, and government employees; while students, professors, and respondents from outside the USA performed least well. Confidence in question topics was associated with increased correctness in responses across all groups, though the association between confidence and the ability to answer correctly was poorest among students and professors. Though 80% of respondents claimed involvement in the development of a tissue engineering technology, their responses were no more correct than those who were not. Among those developing tissue engineering technologies, few are taking advantage of existing standards organizations to strengthen their regulatory submissions. The data suggest that early exposure to regulatory experts would be of value for those seeking to bring their technology to the market. For all groups studied but especially for students and professors, formal initial or continuing education in Regulatory Science should be considered to best support translational tissue engineering research and development. In addition, the involvement of standards development organizations during tissue engineering technology development is strongly recommended.
Introduction
T 1. Define the demographics and technical involvement, by stage, of members of TERMIS-AM. 2. Determine the degree of their awareness of the role of science in regulatory decisions. 3. Identify gaps in understanding of regulatory science policy that lend themselves to repair through both formal education and targeted training approaches.
Materials and Methods
Survey design
The survey was designed to determine the following:
1. The demographics of those responding, including their occupations (including academic), geographic locations, degree of experience in fields other than those in which they are presently employed, and any past history of work in the FDA. 2. The member's degree of involvement in the development of a tissue engineering technology, including the type of technology (Biologic, non-cellular, Biologic, cellular, Medical device, Drug or Combination Product), the state of development of the technology (from Conception Stage to Market Stage Commercialization), their involvement in the development of standard assays, and their future plans for tissue engineering technology development. 3. Understanding of General FDA guidelines. 4. Understanding of specific requirements for effective scientifically based submissions to the Center for Biologics Evaluation and Research (CBER), Center for Drug Evaluation and Research (CDER), Center for Devices and Radiological Health (CDRH), and Office of Combination Projects (OCP).
Selection and design of survey questions
In nearly all instances, questions regarding specific assessments of FDA science practices were derived from existing guidance documents obtainable on the FDA web site (www.fda.gov - see Appendix for the full set of general and specific FDA questions included in the survey). For question selection, guidance documents were chosen, when possible, that pertained especially to the development of tissue engineering technologies.
Three types of FDA-specific questions were presented:
1. Quantitative measures of opinion 2. Single-answer questions 3. Multiple-answer questions
Questions of the first type were used to determine the respondent's stance with regard to the criticality of FDA science requirements in the regulatory process. Questions of the second type were designed to determine the specific awareness of discrete FDA science requirements. Questions of the third type were designed to assess the ability to discriminate such awareness at more subtle levels. Since the questions were designed to be fairly difficult to answer for the casual observer of FDA activities, in the latter two categories, one of the answers that could be chosen was
“I am not prepared to answer this question with sufficient certainty.”
In sum, the structure of the survey allowed for three possible responses to each question:
1. Answer without opting out - Such an answer implied confidence in the ability to answer correctly, because an opt-out answer was available. 2. Opt Out - The respondent could opt out by selecting “I am not prepared to answer this question with sufficient certainty.” 3. No Answer - The respondent could provide no answer whatsoever. This could only occur when a survey was incomplete: Since answers to every question were required, failure to respond to one question meant that the respondent did not see or have an opportunity to respond to any of the subsequent questions.
In the first case, when a respondent provided an answer to a question, it was graded on a scale of 0–100%. 100% credit was given when a single-choice question was answered correctly. Percent correctness in multiple-choice questions was computed by dividing the number of correct responses by the number of available choices, defining a “correct” response as either marking a right answer or not marking a wrong one. In the second and third cases, opt-out responses or unanswered questions were counted as incorrect (assigning a grade of 0 for that question).
All of the questions that were designed to assess the awareness of FDA structure and regulatory science practices are listed in the Appendix, along with their sources.
All responses were entered into an Excel spreadsheet that enabled the correlation of demographic data with responses to individual questions. Although this enabled an almost limitless number of probes of the data, the set of questions and responses that are set forth in the Results were considered most significant to the present study.
Given the nature of responses to the survey and the way in which each response was graded, there naturally arose three different ways to express the overall percent correctness of a given group's collective responses:
A. The percentage of correct responses by all people who entered the survey (i.e., assigning a grade of 0 whenever a respondent opted out or did not answer). B. The percentage of correct responses by all people who responded to the questions (i.e., assigning a grade of 0 whenever a respondent opted out, but ignoring those who did not answer). C. The percentage of correct responses by all people who felt confident enough to answer (i.e., ignoring both those who opted out and those who did not answer).
The survey intake mechanism was designed to be anonymous, so no feedback regarding individual scores was possible. Respondents were informed that only composite scores of all participants would be presented in the form of a later publication.
Statistical evaluation
Differences between occupations
For-Profit, Students, Professors, and Present/Past FDA occupation groups each had enough respondents to be reasonably included in a statistical analysis (10 or more respondents). A one-way ANOVA was used to determine whether or not there were significant differences between their overall correct response rates. ANOVA was performed once on the “B” scores and again on the “C” scores.
Differences between those developing TE technologies and those not developing TE technologies
Two-sample t-tests were used to compare the overall correct response rates achieved by each of these groups, which were also of sufficient size to enable statistical analysis.
Survey administration
Using the Survey Monkey® online system (www.surveymonkey.com), an email invitation to participate in the survey was sent to all 1164 members of TERMIS-AM using the email addresses they provided on joining TERMIS-AM. After the initial invitation, two follow-up reminders were sent over a 3-week period. The survey was left open for a total of 4 weeks. It was closed when the proportionate demographic representation of the respondents matched or nearly matched that of the membership as a whole.
Results
Survey participants
One hundred forty-four members of TERMIS-AM (12% of 1164 overall members) responded to the online survey.
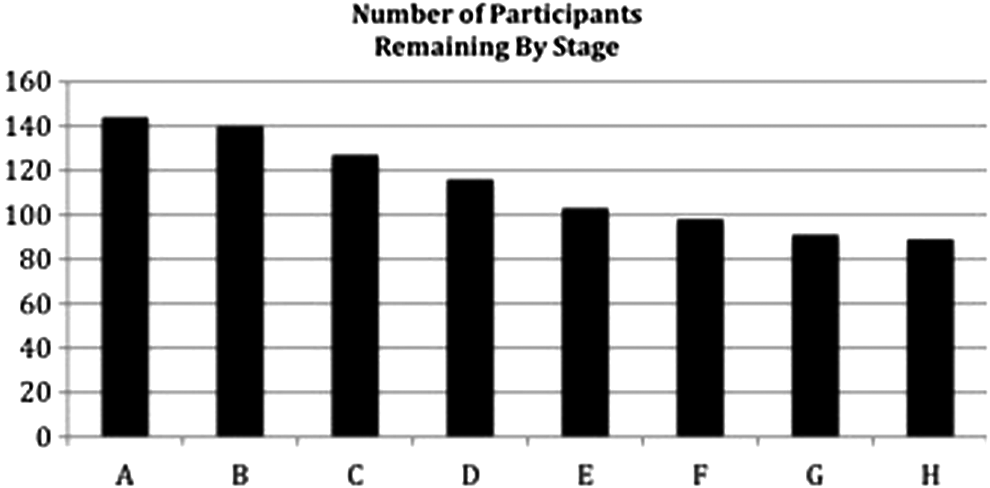
Continuity of survey participation
Due to the difficulty of its questions, participation was expected to decline in the final stages of the survey. Tracking of the degree of participation throughout the survey provided a sense of where participants stopped answering the questions. Figure 1 illustrates the number of participants who remained active at the end of each stage of the survey.
The stages are as follows:
Demographics
Occupation
Survey respondents were first stratified by occupation (Table 1) and they were then sub stratified by their roles in academia (Table 2), industry (Table 3), and by their degree of crossover experience (Table 4).
Of academics, 36 were students (25% of 144 respondents) and 47 were professors (32.6% of 144 respondents).
TERMIS-AM, Tissue Engineering Regenerative Medicine International Society, Americas Chapter.
The number of respondents who claimed to have ≥3 years of experience in the disciplines listed, different from their present occupation. Note that some have had multiple such experiences.
Geographic location
Respondents were also stratified by their geographic location (Table 5). As indicated in the Table, the proportions of survey respondents from the major geographical regions in the western hemisphere mirrored those of the overall TERMIS membership.
TERMIS-AM is composed of the nations constituting Central, North, and South America. The proportions of survey participants from Canada, Central America, South America, and the United States are shown, adjacent to their proportionate TERMIS-AM membership from each region. One hundred forty respondents participated at this stage of the survey.
N/A, not applicable.
Involvement in TE/RM technology development
Of the 139 active respondents remaining at this stage in the survey, 111 (80%) indicated that they were actively developing a tissue engineering technology, while 28 (20%) indicated that they were not. The type(s) of technology under development are listed in Table 6. The stage of technology development is listed in Table 7.
Regulatory interface
The regulatory path(s) for the Tissue Engineering/Regenerative Medicine (TE/RM) technologies under development are shown in Table 8 and their regulatory requirements, when known, are shown in Table 9.
PMA, pre market approval process; BLA, biologics license application; NDA, new drug application; CE Mark is the European approval process.
IDE, investigational device exemption; NDA, new drug application.
Standard assay development
Of the 107 respondents at this stage of the survey who had indicated that they were developing a tissue engineering technology, 62 (58%) indicated that they were developing or had developed a standard assay to validate the safety or efficacy of their technology. Table 10 depicts the frequency of categories within which such assays are being developed. Eleven respondents indicated that they are or have been working with one or more standards development organizations in the development of their assays (Table 11).
ASTM, American Society for Testing and Materials; ISO, International Standards Organization; USP, United States Pharmacopoeia.
In Table 10, example “Tissue Function” assays included vascularization indices, tumorogenicity, and gene expression after tissue transfection. Example “Composition and Process” assays included tests of cell and tissue viability, cell lot constancy assessment, and cell scale-up processes. Examples of “Animal Studies” included tissue engraftment assessments, in vivo cellular homing, and pharmacologic assessments. Examples of “Biological Response to Biomaterials” assays included efficiency of cancer cell trapping scaffolds, thrombosis responses, and biocompatibility assessments. Examples of “Drug Delivery” assays included measurement of drug release from antibody arrays and device-associated drug elution assessments.
Future intentions in tissue engineering technology development
In order to ascertain the degree to which respondents were oriented toward activities that would require their future interaction with the FDA in the development of technology, the following options were provided. One hundred twenty seven respondents chose from among these options. The results are presented in Table 12.
“I plan to perform academic research and license any resulting technology for commercialization.” (ACADEMIC-LICENSE)
“I plan to actively commercialize FDA-regulated technology.” (COMMERCIALIZE)
“I plan to serve as a consultant to businesses commercializing FDA-regulated tissue engineering technologies.” (CONSULT)
“I plan to teach only.” (TEACH)
“I plan to provide other administrative support to the field.” (ADMIN)
“None of the above.” (NONE)
Awareness of FDA science submission requirements
The results to the following queries are expressed in Tables 13–21 as percentages A/B/C, where the percentages shown correspond to the three categories indicated in the “Materials and Methods” section.
Note that the “All Respondents” row is calculated as a weighted average for all groups and in all cases, “B” group results are in bold. The groups A, B, and C were constituted as follows:
Group A: The percentage of correct responses by all people who entered the survey (i.e., assigning a grade of 0 whenever a respondent opted out or did not answer).
Group B: The percentage of correct responses by all people who responded to the question (i.e., assigning a grade of 0 whenever a respondent opted out, but ignoring those who did not answer).
Group C: The percentage of correct responses by all people who felt confident enough to answer (i.e., ignoring both those who opted out and those who did not answer).
Any past or present FDA employee is accounted for in this row, and not in any of the other rows.
Four people did not respond to the question about past FDA experience, and are, therefore, not included in this table at all. Two of them were for-profit employees, and two of them were students.
CBER, Center for Biologics Evaluation and Research; CDER, Center for Drug Evaluation and Research; CDRH, Center for Devices and Radiological Health; FDA, Food and Drug Administration; OCP, Office of Combination Projects.
Any past or present FDA employee is accounted for in this row, and not in any of the other rows.
Both respondents opted out of all CDER questions.
Neither respondent provided any answers in the CDER, CDRH, or OCP sections.
Table 13 depicts the percent of correct responses by occupation. The results indicate that the mean correct responses for the full survey among all who at least started the survey (“A” Group) was very low—21%. In contrast, among those who felt confident in responding, the percent correctness was 66%, which was only slightly below that of present or previous FDA employees who expressed confidence in their responses, which was 67%. Perhaps the most important measure was that of the “B” group, that is, those who responded to all questions but formally opted out when lacking confidence in answers. Overall, this group scored only 32% correct.
Questions were segmented into those pertaining to General FDA, CBER, CDER, CDRH, and OCP-specific requirements. Among the “A” group, the rank order of correctness fell from 31% to 15% across the series: General FDA>CBER=OCP>CDRH>CDER. The “B” group's correctness declined from 39% to 23% across the series: OCP=General FDA>CBER>CDRH>CDER, while the “C” groups correctness fell from 77% to 57% across the series: OCP>CDRH>CBER=CDER>General FDA.
The “C” group was thrice as likely to provide correct responses as the “A” group and twice as likely to provide correct responses as the “B” group. This suggests that there is a knowledgeable subset of TERMIS-AM members having broad regulatory knowledge. Interestingly, this applies to a subset of students as well. Their “C” group had 59% correct responses, that is, only eight points below the present and previous FDA employees; whereas the student “A’ and “B” groups had only 13% and 19% correct, respectively.
When stratifying by occupation and using the “B” group as an index, neglecting groups having small numbers (Consultants (4), non-FDA government employees (2), and Undefined Others (13), overall correctness ranged from the high of 47% among For-Profit employees>Present or previous FDA employees (39%)>Professors (28%)>Non-Profit employees (27%)>Students (19%). In all “B” group instances, For-Profit employees had the highest scores across all FDA divisions (from 58% to 33% OCP>CDRH>CBER>CDER) except for General FDA questions that were led by present or former FDA employees (55%). For-Profit employee correct “B” group response rates were significantly higher than those of Professors and Students (p<0.001). Present or former FDA employees and For-Profit employees were closely grouped, however, in both the “B” and “C” groups.
Table 14 depicts the percent of correct responses as a function of geographic location. In considering geography, leaving out Central America (one respondent), “B” group results overall were USA (34%)>South America (22%)>Canada (20%). Highest correct responses by U.S. respondents were to OCP questions (42%), whereas South Americans did best with General FDA questions (34%) and Canadians did best with CBER questions (29%). Note that for Tables 14–21, “B” group responses are in bold for ease of reading.
Table 15 depicts the percent of correct responses as a function of crossover occupational experience. In addition to their present occupations, respondents also listed other occupations that they had held for more than 3 years in the past. Interestingly, previous Non-Profit experience provided the greatest correlation with overall correctness in the “B” group (56%) and the least correlation with the “Other” experience (22%). However, the N of the former (9) is likely to be too low to be statistically significant. When occupational experience was combined, augmentation of correct responses was only seen among For-Profit employees having previous experience as Consultants (from 47% to 68% in the “B” group and from 69% to 78% in the “C” group) and for Professors who had previous For-Profit experience (from 28% to 39% in the “B” group and from 68% to 71% in the “C” group). However, in each case, the N (4 and 9, respectively) did not allow the results to be statistically treated (data not shown).
Table 16 depicts the percentage of correct responses as a function of involvement in the development of a tissue engineering technology. Among the 111 respondents who indicated that they were involved in tissue engineering technology development, the “B” group percent correctness was not different across all categories from the 28 respondents who indicated that they were not developing a tissue engineering technology (32% and 29% overall correct, respectively—a statistically nonsignificant difference). When these data were analyzed by profession, the declining series of percent correctness was For-Profit employees (50%)>Professors (29%)>Present or previous FDA employees (27%)>Non-Profit employees (26%)>Students (22%). The data suggest that a large number of respondents are involved in technology development but that most have a poorly developed understanding of regulatory requirements.
Table 17 depicts the percentage of correct responses among those developing a tissue engineering technology as a function of occupation. When compared with Table 13, the overall “B” and “C” group correct response rates are not appreciably different from those of the occupational groups at large.
Table 18 depicts the percentage of correct responses as a function of involvement in the development of a validation assay for a tissue engineering technology. Results were only slightly better for those who claimed to be developing validation assays that they would use in FDA submissions, with those in the “B” group who were developing assays having a 34% overall correctness versus a 29% correctness among those who were not. Results were also similar across all FDA categories. Very few reported that they were working with an FDA-recognized standards development agency (ASTM—American Society for Testing and Materials; ISO—International Standards Organization; USP—United States Pharmacopoeia), despite FDA commitment to such activities. 9
Table 19 depicts the percentage of correct responses as a function of the state of development of a tissue engineering technology. When the state of development of a tissue engineering technology was considered among “B” group respondents, as one might expect, those having a product On The Market (63%) fared better than those having products at the following stages: Mid-Level Commercialization (40%)>Prototype (35%)>Early Commercialization (24%)>Conception (23%) and, surprisingly,>Late-Stage Commercialization (19%—although only two respondents were in the latter category).
Table 20 depicts the percentage of correct responses as a function of the type of tissue engineering technology under development. There was minimal difference seen in the “B” group when considering the types of tissue engineering technologies being developed, all types having values in the 28–39% range, with Medical Devices being the highest and Cellular Biologics being the lowest. In general, the highest percent correctness was seen for that part of the FDA to which the respondent's particular technology's regulatory submission would be sent (CDRH for a Medical Device, for example).
Table 21 depicts the percentage of correct responses as a function of the respondent's perceived future role in the field of TE/RM. When the “B” group respondents were stratified based on their anticipated future directions, those wishing to commercialize products had the highest overall scores (44%), while those preferring an Academia-Licensing route had the lowest (25%).
Table 22 depicts the confidence that the various occupations expressed in their ability to respond correctly to the FDA-specific questions. As shown, there was a fairly constant tendency of all occupations to leave the survey (32%±4%). Since there were gross disparities in the ability to answer questions correctly between occupations, this suggests that the failure to complete the survey was for other reasons—as yet unknown—than as a function of confidence in one's ability to answer the questions which were presented. The occupations varied sharply when it came to the selection of the opt-out clause in questions (e.g., “B” group behavior), from a high of 67% for students to a low of 25% for non-FDA government employees. This correlated inversely with the degrees to which occupations declared their confidence in the ability to answer questions without opting out (e.g., “C” group behavior): 33% for students and 75% for non-FDA government employees.
Note that columns 2 and 3 refer to questions which were actually answered among those who remained after the proportions of questions that were skipped (Column 2) were subtracted away.
Table 23 depicts a confidence ratio between one's certainty in the ability to answer a question correctly and the ability to actually execute the correct response. Here, it becomes clear that students and professors are the least strong when it comes to self-evaluation of a capacity to answer correctly.
Statistical Evaluation Results
Differences between occupations
Results of the ANOVA
“B” scores: p-value is <0.001, indicating significance (all of them are not equal to one another).
An interval plot reveals that For-Profit employees performed better than Students and better than Professors.
“C” scores: The p-value is 0.213, indicating no significant differences. All four groups performed equally well when they were confident in their ability to respond correctly.
Differences between those developing TE technologies and those not developing TE technologies
Results of the t-tests
“B” scores The p-value is 0.466, indicating no significant differences. Both groups performed equally well.
“C” scores: The p-value is 0.459, indicating no significant differences. Both groups performed equally well.
Discussion
One hundred forty-four members of TERMIS-AM took a comprehensive survey of FDA regulatory science practices to assess their understanding of this important regulatory submission requirement. Eighty-nine people completed the survey. A proportionate representation of the occupations and geographical locations of the TERMIS-AM membership as a whole took the survey, including consultants, For- and Nonprofit corporate employees, non-FDA government employees, students, professors, and present and past FDA employees. The survey broadly addressed science submission requirements for CBER, CDER, CDRH, and the OCP. All FDA-related questions were sourced from materials (including guidance documents) that were available on the FDA web site (www.fda.gov).
The survey was structured so that the proportion of correct responses could be analyzed on the basis of occupation, geographical location, involvement in technology development, and the like. Correct responsiveness could also be determined for all entrants to the survey (whether they completed the survey or not—analysis group “A”), for all of those who completed the study, though electing to formally opt out of certain responses (analysis group “B”), and for all of those who felt sufficiently confident to answer questions without formally opting out (analysis group “C”).
The results indicate that the mean correct responses for the full survey among all who at least started the survey (“A” Group) were very low. In contrast, among those who felt confident in responding, the percent correctness was only slightly below that of present or previous FDA employees who expressed confidence in their responses. Perhaps the most important measure was that of the “B” group—those who responded to all questions but formally opted out when lacking confidence in answers. Overall, this group scored only 32% correct. The “C” group was thrice as likely to provide correct responses as the “A” group and twice as likely to provide correct responses as the “B” group. This suggests that there is a knowledgeable subset of TERMIS-AM members having broad regulatory knowledge. Interestingly, this applies to a subset of students as well. When stratifying by occupation and using the “B” group as an index, For-Profit employee correct response rates were significantly higher than those of Professors and Students. Interestingly, in the “C” group, their correct response rates did not differ.
In addition to their present occupations, respondents also listed other occupations that they had held for more than 3 years in the past, thereby providing meaningful exposure which might affect their knowledge base with regard to the FDA. When occupational experience was combined, augmentation of correct responses was only seen among For-Profit employees having previous experience as Consultants (from 47% to 68% in the “B” group and from 69% to 78% in the “C” group) and for Professors who had previous For-Profit experience (from 28% to 39% in the “B” group and from 68% to 71% in the “C” group). However, in each case, the N (4 and 9, respectively) did not allow the results to be statistically treated.
Among the 111 respondents who indicated that they were involved in tissue engineering technology development, “B” group percent correctness was not significantly different across all categories from the 28 respondents who indicated that they were not developing a tissue engineering technology. These data suggest that a large number of respondents are involved in technology development but that most have a poorly developed understanding of regulatory requirements.
Results were only slightly better for those who claimed to be developing validation assays that they would use in FDA submissions. Results were also similar across all FDA categories. Very few reported that they were working with an FDA recognized standards development agency (ASTM—American Society for Testing and Materials; ISO—International Standards Organization; USP—United States Pharmacopoeia), despite FDA commitment to such activities. 9 This is a troubling finding. These organizations have worked closely with the FDA for many years to provide systems for collaborative standards development, and careful consideration should be given to leveraging them in the course of tissue engineering technology development.
When the state of development of a tissue engineering technology was considered among “B” group respondents, as one might expect, those having a product On The Market fared better than those having products at earlier stages. Minimal difference was seen in the “B” group when considering the types of tissue engineering technologies being developed, with Medical Devices having the highest percent correctness and Cellular Biologics having the lowest percent correctness.
When the “B” group respondents were stratified based on their anticipated future directions, those wishing to commercialize products had the highest overall scores while those preferring an Academia-Licensing route had the lowest.
It is worth noting that one subset of questions which pertained to software as a product or as a component of a medical device met with very poor results in the “B” group, with only 9% responding correctly overall. This is important, because these questions included the critical concepts of validation (does the product meet the needs of its intended user) and verification (does the product function according to its outlined specifications).
When asked general questions regarding the importance of science in the content of FDA submissions, respondents indicated that it was either “Important” (36%) or “Critical” (53%). Identical numbers indicated that science was an important factor in the FDA decision-making process with regard to tissue engineered medical products. The data also indicated that respondents felt that the quality of science held across the full continuum of activities was involved in product commercialization (i.e., proof of concept, preclinical bench studies animal model selection and preclinical studies, clinical studies, and manufacturing and quality control). It seems, therefore, that there is a general understanding of the importance of science in regulatory submissions—but detailed understanding seems to be missing.
Some caveats with regard to the survey include its mainly semi-quantitative nature, the degree of fall-off among participants, and the low numbers of respondents among non-FDA Government Employees, Consultants, and Others. While only 12% of the TERMIS-AM registered membership took the survey, this is a common response rate among voluntary surveys and proportionate representation of the membership was achieved (Tables 1 and 5). It is important to keep in mind when reviewing correct response rates that it is rare for any one individual to have a full grasp of the workings of the entire FDA with regard to science submission requirements—even among present or former FDA employees. The latter group is often specialized within one FDA division, whereas the survey tested science requirements broadly across all divisions. As one might expect, those among this group who expressed the highest confidence in their knowledge (the “C” group) achieved a 67% correct response rate—a high level for this survey. Importantly, since the questions were derived primarily from guidance documents, the responses are not hard and fast, as each technology has its unique issues that can require guidance to be modified during the regulatory evaluation process. Finally, the order in which questions were presented was not randomized, potentially influencing the point at which a participant might give up if, say, unfamiliar topics were presented earlier on, creating a lack of confidence to proceed to more comfortable topics yet to come.
Nonetheless, taking these concerns and issues into consideration, the data suggest that the membership of TERMIS-AM, while recognizing the importance of regulatory science, could benefit substantially from more formalized training with regard to FDA science submission requirements. The FDA itself has recently released its report on Regulatory Science strategy that presents a roadmap for at least a part of this critical education. 8 Several others have weighed in on the importance of regulatory science education as well.10–13 Although the FDA web site is replete with guidance and other materials designed to assist the technology developer in preparation for regulatory assessment, it can be difficult to navigate a path through these documents that pertains to any specific technology. Unless one is actively commercializing a product, the inhibitors to segregating the important from the unimportant regulatory guidance can potentially prevent one's committed exposure to such materials at all.
In reviewing the data, it is obvious that For-Profit industry has the best grasp of FDA Science policies, which is most likely because they need this knowledge daily to move their products to the marketplace. Academics, on the other hand, theoretically have the least need to connect with the FDA in most cases and, as such, are less knowledgeable in general than their For-Profit colleagues with regard to these requirements, despite being in the best position to educate future scientists and engineers regarding FDA policies.
Of course, the overarching question in a study of this design is in three parts: Did all respondents from different occupations fail to complete the survey at the same or different rates? What was the extent of opt-out behavior among the various occupations and finally, what was the level of confidence in the ability to answer correctly as a function of occupation? As shown in Table 22, each occupation left the survey at approximately the same rate. However, their response opt-out and confidence levels are sharply different. An interesting way to approach such data is to ask the question: “How correct were responses when the respondent felt confident in the ability to answer correctly?”—essentially constituting a self-knowledge evaluation. This was approached through a ratio of Proportion Correct Answers/Degree of Confidence, as shown in Table 23. Here, it becomes obvious that students and professors are the least strong when it comes to self-evaluation of a capacity to answer the presented questions correctly.
The TERMIS-AM Industry Committee runs workshops at annual TERMIS meetings in the Americas and worldwide to teach what has been learned from multiple surveys of this type that address impediments to commercialization. Future workshops will deal, among other issues, with FDA science submission requirements. However, while helpful, such workshops are insufficient to achieve the level of awareness of FDA science policies that appear to be needed. To achieve success, such awareness is critical to avoid long delays in the regulatory portion of the commercialization process.
While the FDA has well-established regulatory science internships (see Appendix), the numbers of participants that can be reached through such programs is limited—and their target is more likely to be those who plan to pursue full regulatory professional development for their careers. What is needed is a way to broadly educate the emerging technology development workforce regarding the fundamentals of regulatory science so that they can incorporate an orientation for compliance needs early in the technology development process. One suggestion is to incorporate courses in Regulatory Science into all degree-bearing programs in engineering, business, and the sciences that will potentially direct employees into the tissue engineering product development stream. A suggestion would be to incorporate experienced For-Profit company Regulatory Affairs professionals in the design of such academic curricula and, even better, have them also serve as teachers. Advanced “Continuing Education” curricula for nonacademics (including For-Profit personnel) would also be of benefit, as it appears from the data that all groups can improve their understanding of these issues. Using existing FDA guidance and other materials, curricula can be constructed using “Case Study” or other methodologies so that students, rather than having the extremely low levels of awareness that we have measured in this survey, become an asset having substantial regulatory awareness at an early stage.
Regulatory knowledge is generally acquired through a honing process after multiple interactions with the FDA regarding specific products. If approached in this fashion, didactics and judgment can be communicated at once—potentially thwarting for the long term what one might call the “Regulatory Awareness Gap” that has been one of the largest concerns regarding commercialization of tissue engineering technologies thus far.
Disclaimer Statement
The opinions expressed in this article are those of the members of the TERMIS-AM Industry Committee and not necessarily those of the institutions with which the authors are affiliated.
Footnotes
Acknowledgments
The authors would like to thank Sarah Wilburn and Kay Desmond for their administrative assistance.
Disclosure Statement
No competing financial interests exist.
Appendix
The questions that pertain to the FDA were constructed based on accessible guidance documents found at www.fda.gov. The following is a list of these questions and the answers that were deemed to be correct (in italics) based on the guidance document or other URL referenced below each question. The reader is encouraged to follow the links to these documents for additional studies.
Alcohol
Cosmetics
Dietary Supplements
Food
Human Drugs
Medical Devices
Non-Vaccine Biological Products
Vaccines
Veterinary Drugs
Tobacco
Radiation-Emitting Products
I am not prepared to answer this question with sufficient certainty.
Sources: http://www.fda.gov/AboutFDA/Transparency/Basics/ucm194879.htm, http://www.fda.gov/AboutFDA/Transparency/Basics/ucm203499.htm
Access
Effectiveness
Quality
Reimbursement
Safety
Security
I am not prepared to answer this question with sufficient certainty.
CDRH
Office of Combination Products
CDER
Diagnostic Testing Division
CBER
I am not prepared to answer this question with sufficient certainty.
Type A meetings are any meetings of a sponsor or applicant with CDER or CBER that are not Type B or C meetings, which are focused on product development and review.
Type B meetings are pre-IND meetings and end of Phase (I, II, and II) meetings.
Type C meetings are held with sponsors to discuss stalled product development paths. None of the earlier descriptions is correct.
I am not prepared to answer this question with sufficient certainty.
Source:
Potential for differentiation into cell types having unpredictable behaviors.
Elicitation of an immune response with the potential to trigger autoimmune disease. Microparticle phagocytosis leading to inflammatory disease.
Unpredictable cell behavior in distant sites.
Potential to require future tissue transplantation.
I am not prepared to answer this question with sufficient certainty.
Source:
ECG testing to determine whether cardiomyocyte augmentation is producing aberrant loci of cardiac excitability.
Brain CT to determine whether peripherally administered somatic cells are creating cerebral tumors.
Radiolabeling of administered stem cells for chronic whole-body scanning.
Liver function tests to determine whether non-hepatic cell administration is causing liver function impairment.
CT-guided serial thin needle biopsy of non-target organs.
I am not prepared to answer this question with sufficient certainty.
Source:
Unpredictable persistence of the product after single administration.
Potential placebo effect of administered product(s).
Extended duration of effect when the product is no longer present.
Variable effects due to evolution of the product.
Training required for those administering the therapy.
Invasive administration procedures.
Manufacturability within cost constraints.
Potential requirement for administration using an investigative device.
I am not prepared to answer this question with sufficient certainty.
Source:
During preclinical development in in-vitro cell models.
During preclinical development in animal models.
Immediately after product administration to the host.
One week after product administration to the host.
Three months after product administration to the host.
None of what has been stated earlier.
I am not prepared to answer this question with sufficient certainty.
Source:
2 years
5 years
10 years
15 years
Until death of the host
I am not prepared to answer this question with sufficient certainty.
Source:
Reproductive
Immunologic
Neurologic
Skeletal
Psychological
I am not prepared to answer this question with sufficient certainty.
Source:
Processing and Process Controls
Labeling
Donor eligibility determination
Donor payment
Shipping
I am not prepared to answer this question with sufficient certainty.
Source:
Bone grafts.
Vascularized organs for transplant.
Whole blood and blood components.
Minimally manipulated bone marrow not combined with another article.
Animal cells and tissues and in-vitro diagnostics.
I am not prepared to answer this question with sufficient certainty.
Source:
True
False
I am not prepared to answer this question with sufficient certainty.
Source:
Animal type to reflect comparable joint loading.
Similarity to the human immune system.
Duration of observation.
Rationale for interval sacrifice versus MRI or arthroscopic assessments.
Genomic analysis.
I am not prepared to answer this question with sufficient certainty.
Source:
Accuracy
Precision
Efficacy
Sensitivity
Selectivity
Reproducibility
Safety
Stability
I am not prepared to answer this question with sufficient certainty.
Source:
General Reactivity and Sensitivity (to drugs).
General Regulations to Amend Submissions.
Generally Regarded As Safe.
Good Regulatory Affairs Science.
I am not prepared to answer this question with sufficient certainty.
Biodistribution (BD)
Bioequivalence (BE)
Biometabolism (BM)
Biopartition (BP)
I am not prepared to answer this question with sufficient certainty.
Source:
Facilities in which a drug is manufactured.
Drug recalls.
Drug manufacturing processes.
Drug packaging.
Drug storage.
I am not prepared to answer this question with sufficient certainty.
FDA-specific regulation.
Other Federal legislation.
None of what has been stated earlier.
I am not prepared to answer this question with sufficient certainty.
Process Equivalence
Process Design
Process Qualification
Continuous Process Improvement
Continued Process Verification
I am not prepared to answer this question with sufficient certainty.
Source:
Chemical, physical, and biopharmaceutical characteristics of a drug.
Patient population.
Product packaging.
Therapeutic objectives.
Design of manufacturing processes.
I am not prepared to answer this question with sufficient certainty.
Source:
Quaternary structure
Protein glycosylation
Primary amino-acid structure
Protein ethylation
Protein phosphorylation
I am not prepared to answer this question with sufficient certainty.
Source:
Animal studies
Computer models
Reference protein PK/PD
Functional assays
None of what has been stated earlier
I am not prepared to answer this question with sufficient certainty.
Source:
Functional tests, including complement-mediated cell lysis assays.
Prolonged post-market surveillance.
Comparative animal studies vs. reference standard.
Head-to-head clinical trial vs. reference.
Biosimilar clinical trial to assess neutralizing antibody titer.
I am not prepared to answer this question with sufficient certainty.
Source:
An IDE
An IND
A 510K
A PMA
An RFD
I am not prepared to answer this question with sufficient certainty.
None, Mild, Moderate, Severe.
None, Level A, Level B, Level C.
Class I, Class II, Class III.
Acceptable, Acceptable With Controls, Not Acceptable.
I am not prepared to answer this question with sufficient certainty.
Code of Federal Regulations (CFR) 21 101.
International Organization for Standardization (ISO) ISO 10993.
American Society of Testing and Materials (ASTM) D5910-05 (2012).
United States Pharmacopeia (USP) USP-NF.
I am not prepared to answer this question with sufficient certainty.
Source:
Identify the specific consensus standard(s) used.
Specify that all requirements of the standard were met, except for those aspects which do not apply to the medical device that was developed.
List all of the consensus standards that apply to the device in question and provide a justification for why they were not used.
Provide the name and address of any testing organization that was involved in conforming to the standard.
I am not prepared to answer this question with sufficient certainty.
Source:
Device Users.
Device Fabrication Environment.
Device Use Environment.
Device-User Interface.
Device Recall System.
I am not prepared to answer this question with sufficient certainty.
ISO 10993 Biocompatibility Guidelines.
Current Good Manufacturing Practice (cGMP) Guidelines of the Quality System Regulation (21 CFR Part 820).
Federal Register General Recommendations for Manufactured Devices.
Recommended Practice Methods overseen by Recognized Standards Development Agencies (ex: ASTM, ISO).
American Association of Tissue Banks (AATB) biobanking recommendation.
I am not prepared to answer this question with sufficient certainty.
Source:
The design of a medical device.
Patent protection of a medical device.
The distribution of a medical device.
Market assessment of medical device effectiveness.
The manufacture of a medical device.
I am not prepared to answer this question with sufficient certainty.
Source:
Engineering prototype drawings.
Qualitative Voice of the Customer surveys obtained by Marketing.
In-depth specifications that have been weighed for their appropriateness by an engineering-driven product development team in collaboration with other business elements (i.e., Marketing).
I am not prepared to answer this question with sufficient certainty.
Source:
The Medical Device.
Its Packaging.
Its Distribution Plan.
Its Labeling.
The Device Master Record.
I am not prepared to answer this question with sufficient certainty.
Source:
User Needs Assessment.
Design Inputs.
Staff Changes.
Design Process.
Design Outputs.
At the Completion of Medical Device Manufacture.
I am not prepared to answer this question with sufficient certainty.
Source:
Marketing
Engineering
Chief Medical Officer
General Management
Manufacturing
I am not prepared to answer this question with sufficient certainty.
Source:
Software Quality
Verification
Robustness
Validation
Usability
I am not prepared to answer this question with sufficient certainty.
Source:
Software Quality
Verification
Robustness
Validation
Usability
I am not prepared to answer this question with sufficient certainty.
Source:
Software used as a component of a medical device.
Software that is itself a medical device.
Software used for training.
Software that is used in the production of a medical device.
Software used to manage the manufacturer's Quality System.
I am not prepared to answer this question with sufficient certainty.
Source:
A drug and a device.
A biological product and a device.
A drug and a biological product.
A drug, a device, and a biological product.
Two medical devices.
I am not prepared to answer this question with sufficient certainty.
A drug combined with a monoclonal antibody.
An artificial heart attached to an aortic artery prosthesis.
A drug-eluting cardiovascular stent.
A hip implant bearing growth factors.
A tissue-engineered bladder containing biomaterials, growth factors, and cells.
I am not prepared to answer this question with sufficient certainty.
Ensure consistency of postmarket surveillance of combination products.
Resolve disputes regarding timeliness of a premarket review of combination products.
Assign an FDA Center with primary jurisdiction for regulation of a combination product. Suggest subpopulations in which combination products may be most effective.
Submit annual reports to Congress regarding the activities and effectiveness of its office.
I am not prepared to answer this question with sufficient certainty.
The experience of the reviewers.
The relative volume of the product that consists of a drug, a biological or a medical device.
The primary mode of action of the combination product.
Predicate products having similar properties to the combination product.
All of what has been stated earlier.
I am not prepared to answer this question with sufficient certainty.
The Office of Combination Products
CBER
NIH
CDER
Office of the Ombudsman
CDRH
I am not prepared to answer this question with sufficient certainty.
Medical Device cGMP will be sufficient when a medical device is a part of a combination product, and the primary mode of action is via the medical device.
Biologics cGMP will be sufficient when a biologic is a part of a combination product, and the primary mode of action is via the biologic.
cGMP does not apply to combination products per se.
Each component of the combination product will be developed under the cGMP principles applicable to it (Drug, Device, Biologic).
The most stringent of the three types of cGMP regulations will apply in the case of combination products, regardless of the relative presence of different components in the product.
I am not prepared to answer this question with sufficient certainty.
Source:
Changes in the bioavailability of the drug when combined with the device.
Alterations in device function as a result of drug presence or local tissue reaction to the drug.
Identification of leachables from either the drug or device as a consequence of combined manufacturing conditions.
Availability of each component of the combination product from low-cost cGMP laboratories.
Demonstration of combination efficacy of the product within the subject population studied.
I am not prepared to answer this question with sufficient certainty.
Source:
Fellowship, Internship, Graduate, & Faculty Programs: