
Abstract
Cell sheet engineering has developed as a remarkable method for cell transplantation. In the field of cartilage regeneration, several studies previously reported that cartilage defects could be regenerated by transplantation of a chondrocyte sheet using cell sheet engineering. However, it remains unclear how such a thin cell sheet could repair a deep cartilage defect. We, therefore, focused on the mechanism of cartilage repair using cell sheet engineering in this study. Chondrocyte sheets and synovial cell sheets were fabricated using cell sheet engineering, and these allogenic cell sheets were transplanted to cover an osteochondral defect in a rat model. Macroscopic and histological evaluation was performed at 4 and 12 weeks after transplantation. Analysis of the gene expression of each cell sheet and of the regenerated tissue at 1 week after transplantation was performed. In addition, green fluorescent protein (GFP) transgenic rats were used as donors (transplanted chondrocyte sheets) or recipients (osteochondral defect models) to identify the cell origin of regenerated cartilage.
Cartilage repair was significantly better in the group implanted with a chondrocyte sheet than in that with a synovial cell sheet. The results of gene expression analysis suggest that the possible factor contributing to cartilage repair might be TGFβ1. Cell tracking experiments using GFP transgenic rats showed that the regenerated cartilage was largely composed of cells derived from the transplanted chondrocyte sheets.
Introduction
A
Materials and Methods
All procedures were performed according to an institutionally approved protocol in accordance with the National Institute of Health Guide for Care and Use of Laboratory Animals. All of the experimental research protocols were reviewed and approved by the ethics committee of Hiroshima University.
Fabrication of chondrocyte and synovial cell sheets
Articular cartilage and synovial tissue were harvested from the hip and knee joints of 4 week-old Sprague–Dawley (SD) rats. After cutting the cartilage and synovium into pieces, the tissue was digested with trypsin (TrypLE Express; Life Technologies, Carlsbad, CA) for 30 min followed by 0.25% collagenase (Sigma, St. Louis, MO) for 4 h at 37°C. After passing through a cell strainer (70 μm; BD Biosciences, San Jose, CA), the cells were suspended in culture medium and seeded into temperature-responsive culture dishes (UpCell, CellSeed, Tokyo, Japan). Culture medium consisted of Dulbecco's modified Eagle's medium and Ham's F-12 (DMEM/F12; Life Technologies) containing 20% fetal bovine serum (FBS) and 1% antibiotics. The medium for chondrocyte sheets also contained 50 μg/mL L-ascorbic acid (Sigma, Tokyo, Japan). The cells were incubated at 37°C in a humidified atmosphere of 95% air and 5% CO2 for 2 weeks, at the end of which the chondrocyte sheets and synovial cell sheets could be detached simply by reducing the temperature from 37°C to below 32°C. In addition, triple-layered sheets of each cell type could be fabricated using a simple pipetting method 12 followed by culture for a further 1 week.
Transplantation of cell sheets onto the cartilage defect
Thirty-six SD rats, 12 weeks of age, were anesthetized with an intraperitoneal injection of 1 mL/kg sodium pentobarbital. Using a medial parapatellar approach, the patella groove of the distal femur was exposed. A defect that was 2 mm in diameter and 1 mm in depth was created in the patella groove using a biopsy punch and a metallic drill with a globe-shaped tip of 1 mm diameter. The osteochondral defect that was created affected both articular cartilage and underlying subchondral bone. After lowering the temperature of the culture dishes prepared in advance to a temperature threshold of 32°C, the cultured cell sheets were detached from the dishes using an artificial support membrane(Cell Shifter™ CellSeed, Tokyo, Japan). After cutting the cell sheets and the Cell Shifter to the size of 4 mm square, these allogenic cell sheets were then transplanted to cover the osteochondral defect. The cell sheet was transplanted without suture, because it has a good adhesion property. 10 Animals were divided into the following six groups: 1 sham group (without cartilage defect) (n=12), 2 defect group (without cell sheet) (n=12), 3 monolayer chondrocyte sheet group (n=12), 4 monolayer synovial cell sheet group (n=12), 5 triple-layered chondrocyte sheet group (n=12), 6 and triple-layered synovial cell sheet group (n=12) (Fig. 1). After transplantation, the joint capsule and wound was sutured and all rats were allowed to move freely in their cages.
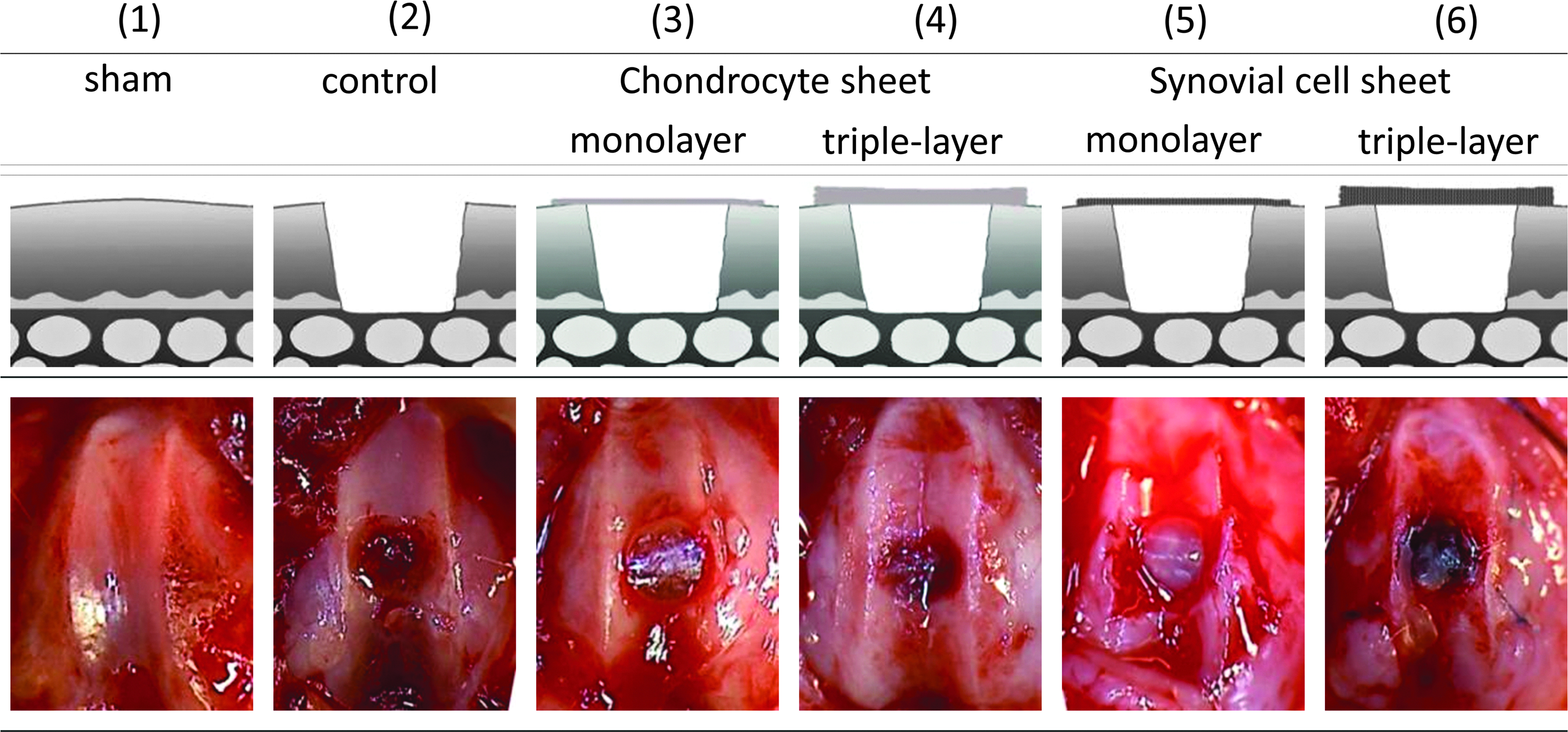
Full-thickness cartilage defects were created in the articular cartilage of rats, and the efficacy of different cell layers in promoting repair when used to cover the defect was assessed, including the schema and gross appearance of each group after transplantation. (1) Sham group: arthrotomy only. (2) Control group: creation of an osteochondral defect without transplantation. (3) Transplantation of a monolayer chondrocyte sheet. (4) Transplantation of a triple-layered chondrocyte sheet. (5) Transplantation of a monolayer synovial cell sheet. (6) Transplantation of a triple-layered synovial cell sheet.
Histological analysis of the cell sheets
After fabrication of the cell sheets, these were fixed overnight in 4% paraformaldehyde. After cutting to the desired size, pieces were mounted with O.C.T. compound (Sakura Finetek, Tokyo, Japan) and frozen at −20°C. The blocks were then cut into 5 μm sections using a cryostat. After air drying at room temperature, these sections were stained with Hematoxilin and Eosin or Safranin-O/Fast green.
Macroscopic and histological evaluation
At 4 and 12 weeks after creation of the defects and treatment, the rats were sacrificed by an intraperitoneal injection of a lethal dose of sodium pentobarbital. The distal femur was resected and evaluated macroscopically using a macroscopic scoring system that was established by Wayne. 13 The scale is composed of four categories and assigns a score ranging from 0(worst) to 16(best) points (Table 1). After that, the cartilage was fixed in 4% paraformaldehyde for 24 h and decalcified with EDTA for 3 weeks. After embedding in paraffin, the blocks were cut into 5 μm sections in the sagittal plane. The sections were stained with Safranin-O/Fast green and were evaluated histologically using Pineda's semiquantitative scale, which ranges from 0(best) to 14(worst) points (Table 2). 14 Furthermore, immunohistochemical staining of type II collagen was performed using the Avidin Biotin Complex (ABC) method with a Vectastain Elite ABC Mouse IgG kit (Vector Laboratories, Burlingame, CA). The primary antibody was a purified mouse monoclonal antibody anti-human type II collagen (Daiichi Fine Chemical, Toyama, Japan).
Analysis of gene expressions in cell sheets in vitro and regenerated tissues in vivo
To elucidate the factors contributing to cartilage repair, the gene expression patterns of chondrocyte sheets and synovial cell sheets in vitro and regenerative tissues in vivo were analyzed.
In vitro: Triple-layered chondrocyte sheets and synovial cell sheets were fabricated using temperature-responsive culture dishes. These sheets were homogenized with TRIzol Reagent (Life Technologies), and total RNA was obtained according to the manufacturer's instructions. For cDNA synthesis, reverse transcription of total RNA was performed using reverse transcriptase (SuperScript VILO MasterMix, Life Technologies). A PCR reaction mix containing the primers for the target genes, the cDNA of each sample, and Fast SYBR® Green Master Mix (Life Technologies) was prepared, and real-time PCR was performed using StepOne® (Life Technologies). The mRNA expression levels of these samples were normalized to β-actin (ACTB) that served as an endogenous control. Data were analyzed using the comparative ΔΔCT method.
In vivo: The triple-layered chondrocyte sheet and triple-layered synovial cell sheet were prepared as described earlier. One week after transplantation, we harvested the tissue formed in the osteochondral defect of each group. Gene expression in these tissues was analyzed by real-time PCR in the same way as for cell sheets in vitro.
The target genes associated with cartilage metabolism were as follows: collagen type I (COL1), COL2, COL10, Sox9, bone morphogenetic protein-2 (BMP2), fibroblast growth factor-2 (FGF2), transforming growth factor-β (TGFβ), insulin-like growth factor-1 (IGF1), cartilage-derived morphogenetic protein-1 (CDMP1), fibronectin, aggrecan, matrix metalloproteinase 13 (MMP13), a disintegrin and metalloproteinase with thrombospondin motifs-4 (ADAMTS4), ADAMTS5, tumor necrosis factor (TNF), interleukin-1β (IL1b), and osteocalcin. The primer sequences are shown in Table 3.
Identification of the cell origin of repaired tissue using GFP transgenic rats
GFP transgenic animals have been widely used in cell tracking studies.15–17 To identify the cell origin of repaired cartilage, GFP transgenic rats were utilized in this study. We used GFP transgenic rats and SD rats at 4 weeks of age. After chondrocytes were harvested from these rats, the triple-layered chondrocyte sheets were fabricated as described earlier. GFP transgenic rats and SD rats at 12 weeks of age were prepared as the recipients. The cartilage defects of GFP transgenic rats were covered with triple-layered chondrocyte sheets from wild-type SD rats (Group I). In the reverse experiment, the cartilage defects of wild-type SD rats were covered with triple-layered GFP-positive chondrocyte sheets (Group II). These models were also allogenic models. At 4 weeks after transplantation, all rats were sacrificed for histological evaluation. The specimens were prepared in the manner described earlier. To preserve GFP signal for histological analysis, they were embedded in plastic resin (Technovit 8100; Heraeus Kulzer, Wehrheim, Germany). Sections were evaluated under a typical light microscope with Safranin-O/fast green staining for cartilage regeneration and under a fluorescent microscope for GFP fluorescence analysis and DAPI nucleic acid staining.
Statistical analysis
The results of histological scoring are expressed as mean value and standard deviation. Multiple comparisons were performed for the data of each group using the Steel–Dwass method. Gene expression data were analyzed using the Mann–Whitney U test. p Values less than 0.05 were considered statistically significant.
Results
Histology of cell sheets
Comparing the monolayer sheet with the triple-layered sheet, we found that the latter was more than thrice thicker than the former, measuring about 100 μm. Spherical cells surrounded by lacunae with abundant extracellular matrix were observed in the triple-layered chondrocyte sheet. There was good staining with Safranin-O (Fig. 2C, D). In contrast, fibroblastic cells showed good proliferation in the triple-layered synovial sheet, but the amount of extracellular matrix was relatively poor (Fig. 2G, H).

Macroscopic evaluation
At 4 and 12 weeks after transplantation in each group, some regenerated tissues were found in the cartilage defects (Fig. 3A). There was significant difference between the triple-layered chondrocyte sheet model and the monolayer synovial cell sheet model at 4 weeks after transplantation in the macroscopic score among the five groups excluding the sham group (p<0.05)(Fig. 3B). The categorical values of Wayne's macroscopic scale are shown in Table 4. The results show that the total values of each group improved from 4 weeks to 12 weeks. However, at 12 weeks, there was no significant difference among these groups.
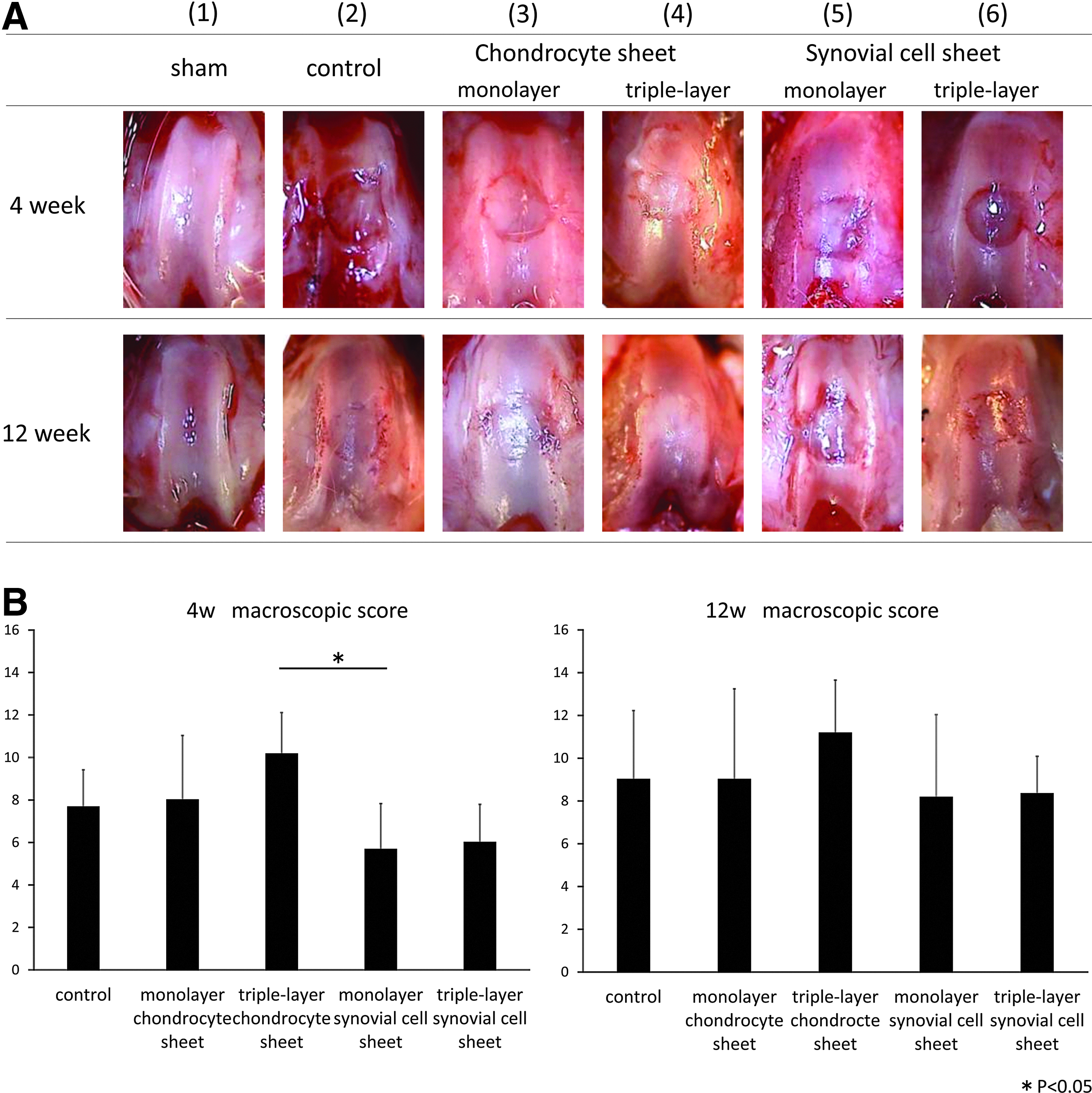
Values are the mean±SD.
Histological evaluation
In the groups treated with a chondrocyte sheet, the area of Safranin-O staining in the regenerated tissues was larger than that in all other groups except the sham group. Especially in the triple-layered chondrocyte sheet group, larger areas of hyaline-like cartilage and good integration of the surrounding cartilage were observed compared with other groups (Fig. 4A). Assessment using Pineda's semiquantitative scale revealed that cartilage repair was significantly better in the chondrocyte sheet groups than that in the synovial cell sheet groups at 4 weeks (p<0.05). Furthermore, at 12 weeks after transplantation, it revealed that cartilage repair in the triple-layered chondrocyte sheet group was better than in any other group (p<0.05) (Fig. 4B). The immunohistochemical staining also showed better expression of type II collagen in the repaired tissue of the triple-layered chondrocyte sheet group at 12 weeks after transplantation. The categorical values of Pineda's semiquantitative scale are shown in Table 5.

Values are the mean±SD.
Gene expression of the cell sheets in vitro and the repaired tissues in vivo
When the chondrocyte sheets and synovial cell sheets were compared in vitro, relative expression levels of COL1, FGF2, IGF1, and ADAMTS4 were significantly higher in the synovial cell sheet group than in the chondrocyte sheet group (p<0.05) (Fig. 5). However, when regenerated tissues were compared between rats treated by chondrocyte sheet transplantation and those treated by synovial cell sheet transplantation in vivo, the relative expression level of TGFβ1 was significantly higher in the chondrocyte sheet group than in the synovial cell sheet group (p<0.05). By contrast, the relative expression levels of COL1, FGF2, IGF1, ADAMTS4, and ADAMTS5 were significantly higher in the synovial cell sheet group than in the chondrocyte sheet group (p<0.05) (Fig. 6). In short, the expression levels of TGFβ1 and ADAMTS5 were different between in vitro and in vivo conditions.

Comparison of gene expression between triple-layered chondrocyte sheets and triple-layered synovial sheets in vitro, analyzed by real-time PCR. The expression of COL1, FGF2, IGF1, and ADAMTS4 was significantly higher in the synovial sheet group than in the chondrocyte sheet group (p<0.05).

Comparison of gene expression in the regenerative tissue at 1 week after transplantation in vivo between the triple-layered chondrocyte sheet and the triple-layered synovial sheet, analyzed by real-time PCR. Expression of TGFβ1 was significantly higher in the chondrocyte sheet group than in the synovial sheet group (p<0.05). In contrast, the expression of COL1, FGF2, IGF1, ADAMTS4, and ADAMTS5 was significantly higher in the synovial sheet group than in the chondrocyte sheet group (p<0.05).
Cell tracking study using GFP transgenic rats
In both groups, regenerated cartilage-like tissues, containing spherical cells and extracellular matrix with good Safranin-O staining could be observed. Under the fluorescent microscope, GFP-positive cells could be observed in the region of regenerated subchondral bone but almost none were found in the repaired hyaline-like cartilage area in group I (Fig. 7). In contrast, GFP-positive cells were found to correspond closely to the repaired cartilage-like area in group II (Fig. 8). These results suggest that the majority of regenerated hyaline-like cartilage consists of cells derived from the transplanted chondrocyte sheets.
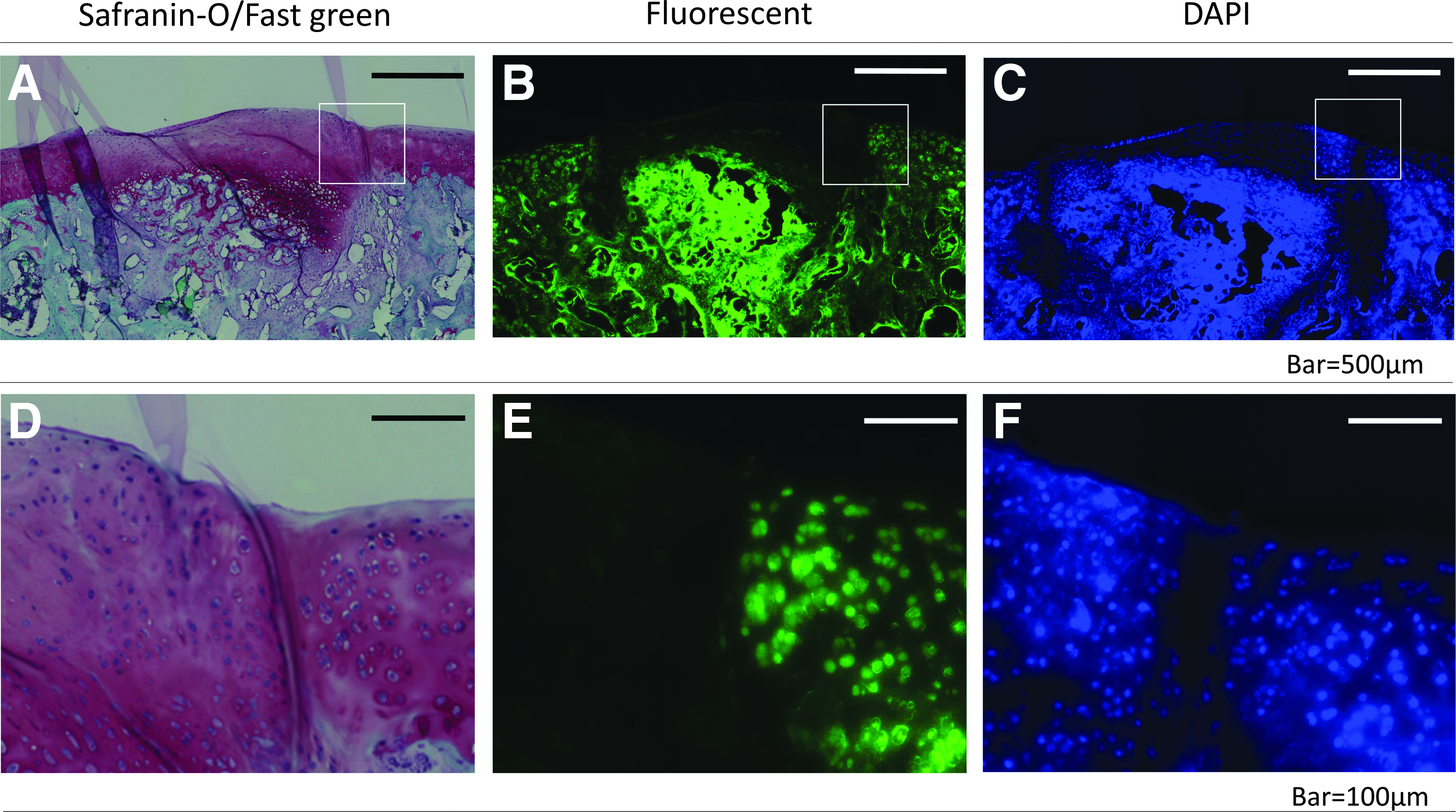
In Group I, the cartilage defects created in GFP transgenic rats were treated by covering them with a transplanted triple-layered chondrocyte sheet from control SD rats.
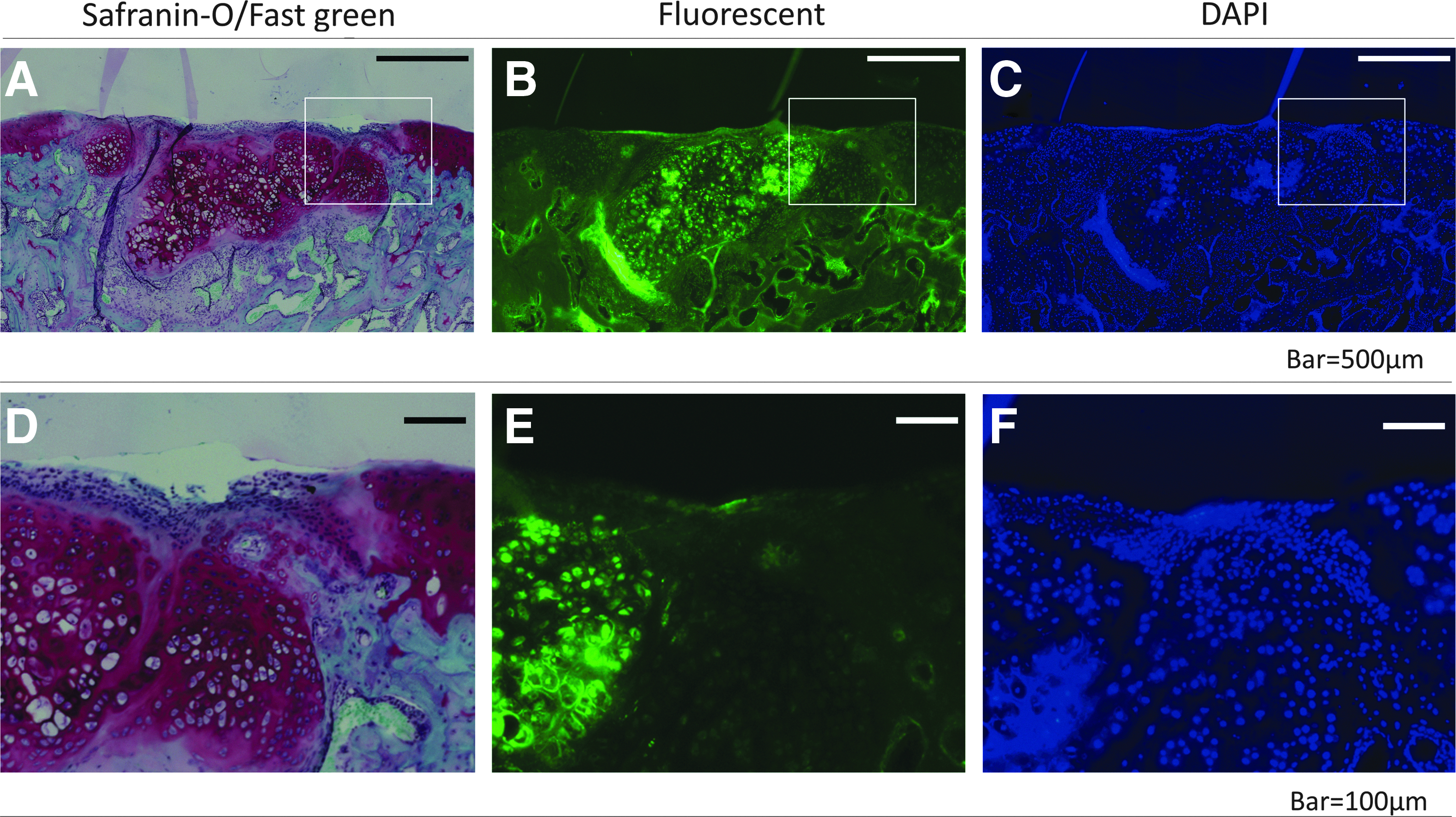
In Group II, the cartilage defects created in the SD rats were treated by covering them with a transplanted triple-layered chondrocyte sheet from GFP transgenic rats.
Discussion
This study demonstrates that covering osteochondral defects with chondrocyte sheets but not synovial cell sheets promotes cartilage repair, and that the regenerated hyaline-like cartilage is largely composed of cells derived from transplanted chondrocyte sheets.
Previously, some studies tried to investigate cartilage regeneration in cartilage defects covered with periosteum or artificial membrane. The transplantation of periosteum was reported to be effective for cartilage repair in some studies.15,18 Zantop and Petersen demonstrated cartilage regeneration with microfracture when a large chondral defect was covered by resorbable polymer felt and sodium hyaluronan. 19 However, a previous study in our group showed that covering defects with atelocollagen membrane is not effective for cartilage repair but induces osteogenesis. 20 Therefore, the effect of the coverage of cartilage defects on cartilage repair remains controversial. In this study, although covering the defects with chondrocyte sheets led to marked cartilage repair, coverage with synovial cell sheets was not so effective. If cartilage defects are mainly repaired as a result of coverage causing the accumulation of bone marrow cells and protection against the catabolic factors in synovial fluid, articular cartilage should be repaired when covered not only by chondrocyte sheets but also by synovial cell sheets. These findings suggest that simply covering the cartilage defect might not be the main mechanism of cartilage repair.
In this study, gene expression in the chondrocyte or synovial cell sheets in vitro and in regenerated tissues in vivo was analyzed to investigate production of paracrine factors from cell sheets that could contribute to cartilage repair. Previous studies also reported gene expression in chondrocyte sheets. Mitani et al. investigated the properties of chondrocyte sheets and showed that expression of Sox 9, collagen type 2 and 27, integrin α10, and fibronectin were higher in layered chondrocyte sheets than in a single chondrocyte sheet in vitro. 21 In addition, Hamahashi et al. showed that layered chondrocyte sheets produced higher levels of TGFβ and PGE2 as humoral factors compared with monolayer chondrocyte sheets and suspected that these factors might contribute to cartilage repair. 22 However, these previously reported results might not accurately reflect in vivo phenomena, because all these data were collected from cell sheets in vitro. In this study, we investigated gene expression in triple-layered chondrocyte and synovial cell sheets not only in vitro but also in vivo. We found that gene expression patterns of the cell sheets were a little different between in vitro and in vivo conditions. In particular, the expression of TGFβ1 in chondrocyte sheets did not differ significantly from that of synovial sheets in vitro. In contrast, in vivo, TGFβ1 expression was higher in chondrocyte sheets than in synovial cell sheets. TGFβ1 is well known as an essential factor for chondrogenesis and has been reported to contribute to chondrogenesis both in vitro and in vivo. 23 These results indicate that TGFβ1 expression in chondrocyte sheets could have been activated in vivo and might play an important role in cartilage repair. On the other hand, the expression of FGF2, IGF1, and ADAMTS family members was at a higher level in synovial cell sheets than in chondrocyte sheets both in vitro and in vivo. Since FGF2 and IGF1 have been reported to be growth factors which enhance the proliferation or differentiation of chondrocytes and their progenitors, it could be expected that high expression of these factors contributes to repair of a cartilage defect.24,25 However, FGF2 may also be disadvantageous for cartilage formation because of its pro-angiogenic and pro-osteogenic potential. Miyakoshi et al. demonstrated that intra-articular administration of FGF2 induced inflammation and osteophyte formation. 26 Simultaneously, the expression of both ADAMTS4 and ADAMTS5, which are known as aggrecanases and contribute to cartilage destruction, is at a higher level in synovial cell sheets. 27 These differences in the expression of various factors between chondrocyte sheets and synovial cell sheets might be one possible explanation for the difference in the effects of these cell sheets on cartilage repair.
Elucidation of the cell origin of repaired cartilage is one of the important questions that needs to be answered to understand the mechanisms of cartilage regeneration. It is thought that several types of cells around the defect could contribute to the regenerated tissue, because there are many different types of progenitor cells in the synovial joint compartment. 28 Recent studies have demonstrated that the superficial layer of articular cartilage contains cells with progenitor characteristics. 29 In addition, intra-articular tissues, such as synovium and infrapatellar fad pad, have also been demonstrated to contain mesenchymal stem cells.30,31 Bone marrow-derived mesenchymal stem cells could also migrate to the osteochondral defect area. In the case of transplanted chondrocytes as a cell sheet, it was reported that the transplanted cells survived and could be detected for more than 21 months by in vivo imaging. 32 In this study, cell tracking experiments using GFP transgenic rats revealed that the regenerated hyaline cartilage-like tissues consisted largely of cells derived from the transplanted chondrocyte sheets. We suspect that differences in differentiation capacity between the chondrocyte sheets and synovial cell sheets as a cell source could be responsible for the difference in the effects of these cell sheets on cartilage repair. However, it was reported that synovial tissue contains the synovial mesenchymal stem cells which has chondrogenic differentiation potential and cartilage repair was previously demonstrated by transplantation of synovial mesenchymal stem cells.33,34 In this study, if we used mesenchymal stem cells as a cell source, cartilage repair might be promoted.
This study has some limitations. The first limitation is that all experimental models were allotransplantation models. The difference in immune reactions between chondrocytes and synovial cells can induce a difference in repair among those models. According to the GFP rat histology results, transplanted chondrocytes were still alive at 12 weeks after transplantation. Previous studies have demonstrated good repair using cell sheet engineering with animal allotransplantation models. However, there are no clinical data regarding cell sheet allografts. Chondrocyte sheet allografts might be feasible clinically after overcoming allograft-related problems, including immune response and infection. The second limitation is that these defects were made in the rat trochlear groove which is the most conducive model for good repair. However, our control model did not show good repair at 4 and 12 weeks after transplantation. We thought that this model was not conducive to self-repair because of its deep osteochondral defect. The third limitation is the limited evaluation of the repaired tissue. In this study, macroscopic and histological evaluation were performed using the semi-quantitative scale. We have to take into consideration that these evaluations are likely to be subjective. This study's repaired tissue with its transplantation by the triple-layered chondrocyte sheet did not resemble normal cartilage. Alternative evaluations are necessary, not only histologically but also functionally. Although the results of an ongoing clinical trial using autograft chondrocyte sheet transplantation are yet to be published, when confirmed they will provide more information for cell sheet engineering.
According to our histological analysis of the cell sheets, the thickness of the triple-layered chondrocyte sheet is about 100 μm (Fig. 2). In this study, we have demonstrated that osteochondral defects of 1000 μm in depth are filled with repaired tissue with good staining with Safranin-O and type-2 collagen after being covered with a chondrocyte sheet. In other words, the transplanted chondrocyte sheet is able to fill a defect that is ten times its thickness even without the need for a scaffold. Moreover, even thin chondrocyte sheets could be a cell source for the treatment of full-thickness cartilage defects. However, the repaired tissue far from resembles normal articular cartilage, because of the low level of the subchondral bone along with the fact that osteochondral junction is still not reconstructed. We surmise that these issues would be resolved by improvement in the subchondral bone level, which is a matter of time. Although further investigation is necessary, cell sheet engineering might have a positive impact on clinical application of cartilage regenerative cellular therapy, because chondrocyte sheets can be applied to articular cartilage defects with an area larger than the area of the actual defects, which in the past has been solely treated with conventional thickness tissue-engineered cartilage along with scaffold materials.
Conclusions
Transplantation of chondrocyte sheets but not synovial cell sheets contributes to the repair of full-thickness cartilage defects when used as the cell source. In addition, the high level of expression of TGFβ1 in chondrocyte sheets in vivo compared with that in synovial cell sheets might also participate in the promotion of cartilage repair.
Footnotes
Disclosure Statement
No competing financial interests exist.