
Abstract

O
Regenerative therapy research for partial or complete replacement of diseased myocardium by means of tissue engineering has led to remarkable results during the past 15 years. Engineered heart tissue consisting of a collagen matrix and neonatal cardiomyocytes has been transplanted into small animals resulting in the improvement of ventricular function, and whole heart tissue engineering has been performed by decellularization and reseeding of cells, essentially restoring the myocardial function.6,7 The technique has been improved and refined over several years with an increase in the size and generated force of the engineered heart tissue, although generated contractility does not come close to developing adequate blood pressure in mammals. Myocardial patches also have been created from embryonic stem cells. 8
However, several challenges need to be overcome that have slowed down progress in this field of research in comparison with VADs. The myocardium is more complex and heterogeneous than other cardiac structures such as heart valves where first products have been introduced to the market. Finding the optimal cell source remains a challenge. Fetal and neonatal cardiomyocytes are not available in large numbers and embroynic stem cell derived- or induced pluripotent stem cell-derived cells may cause teratoma. 9 Additionally, nutrition of the constructs is dependent on diffusion as no effective vascularization concept is available. Mass production of cells for large-scale therapeutic measures needs to be developed too.
Due to the still limited force that can be generated, the low- pressure system of the circulation is the most likely target of myocardial tissue engineering approaches. The right ventricle as an important part of this system represents a suitable initial target for the study of myocardial regeneration by tissue engineering.
Prevention of Cardiac Remodelling by Restriction
Some groups have investigated the use of a restrictive mesh which is wrapped around the heart in order to prevent and possibly reverse ventricular remodeling by reducing wall tension. These studies were based on observations in patients who underwent dynamic cardiomyoplasty where heart containment seemed to have a beneficial effect. 10 One example is the CorCap™, a polyester mesh, which is wrapped around both ventricles. In the “Acorn trial” and its follow up study, the use of this device improved quality of life, reduced left ventricular size over several years.11,12 The concomitant prophylactic use of this device in patients at risk for cardiac remodeling during surgical procedures is a conceivable strategy for a broad range use.
Ideally, a contractile patch or restraint could achieve both positive inotropy and prevention of remodeling. Also here, most technical approaches for the augmentation of myocardial function will most likely target the low- pressure system of the heart (right ventricle) due to the limited power these constructs. A conceivable clinical application would be in the “Fontan circulation” where a moderate increase in right atrial pressure would significantly improve lung perfusion. Voss et al. achieved this goal by dynamic cardiomyoplasty using a skeletal muscle in a canine model. 13 Another challenge will be the elimination of fatigue and increase of durability, which is at this point limited to several hours. New-generation polymers which can generate considerable mechanical forces will eventually enable applications in the high-pressure system of circulation as well. 14
Do We Have Tunnel Vision?
A more integrated and comprehensive approach is needed. Perhaps it is time introduce “smart materials” or nano-technology to myocardial tissue engineering either as stand alone technology or in combination with living tissue. For instance, in search for artificial muscle, electrically contractile fibers have been developed that could well complement our traditional “puristic” myocardial tissue engineering approaches using only cells and biological matrices.
In analogy to cardiomyocytes, it could be demonstrated that application of polymers that are contractile upon low-voltage electrical stimulation could provide an additional tool for systolic augmentation of ventricular function. 15 These could act as a contractile myocardial patch to repair a defective heart or be wrapped around the heart as an active co-contractor which inhibits additional remodeling as well without the need for anticoagulation in absence of contact with blood. A quick glance at the microstructure of the electrically contractile polymer reveals large spaces between the fibers where cardiomyocytes conceivably can be embedded between the electrically conducting and contractile structures providing synergistic forces as well as higher mechanical stability (Fig. 1).
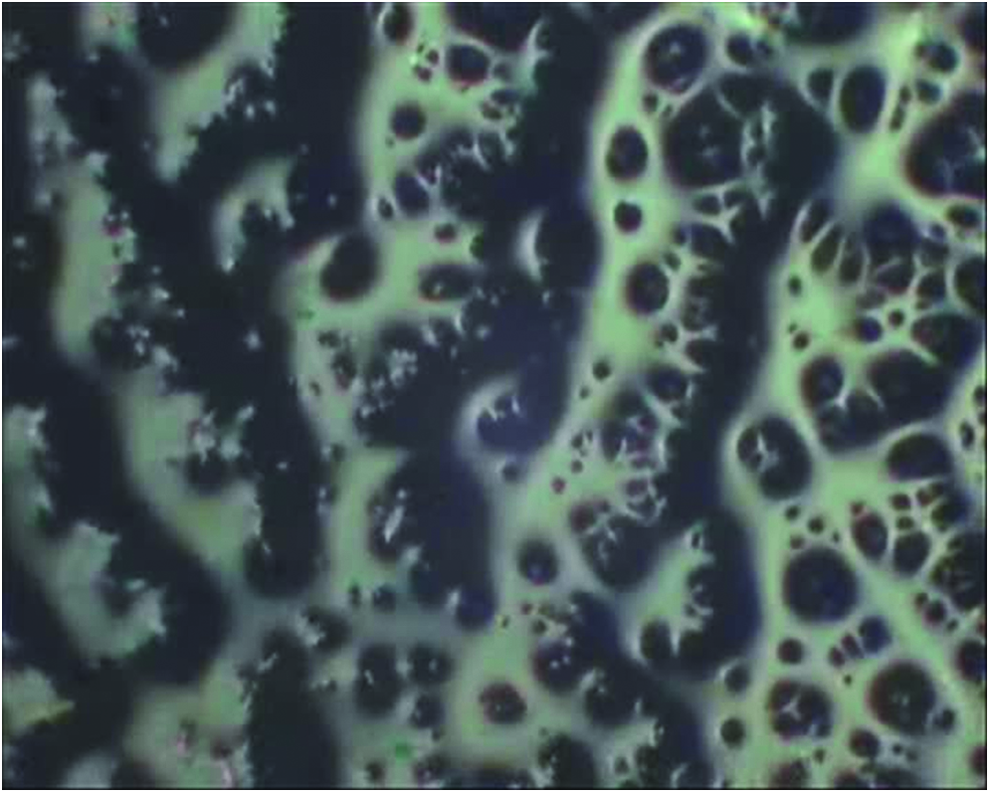
10×magnification of the contracting polymer reveals spaces between the fibers, possibly allowing for seeding of cardiomyocytes onto the polymer with the potential of synergistic effects. Adapted from Ruhparwar et al. 15 Color images available online at www.liebertpub.com/tea
This change of philosophy has already happened the other way around. A biological interphase in mechanical circulatory support devices (VADs) created by “traditional” tissue engineering would theoretically minimize the risk of thromboembolic events and reduce the need for massive anticoagulation jeopardizing patients through bleeding events. VAD companies have been relying on textured surfaces in their devices for years, using the body of the recipient as a bioreactor, enabling coverage of the surface of VAD cannulae by autologous blood cells. This reduces the need for anticoagulants after implantation. 16 The gridlock of limited success in myocardial tissue engineering in comparison with VADs that have changed the landscape of heart failure treatment dramatically over the past 10–15 years can be overcome with more cross talk between traditional engineering, myocardial tissue engineering and various other disciplines. In the end, it is all about transporting blood from one point to another with least side effects. Whether the pump resembles our native pump in phenotype is secondary. It is about restoring function, not morphology.
Footnotes
Disclosure Statement
No competing financial interests exist.