
Abstract
The articular cartilage layer of synovial joints is commonly lesioned by trauma or by a degenerative joint disease. Attempts to repair the damage frequently involve the performance of autologous chondrocyte implantation (ACI). Healthy cartilage must be first removed from the joint, and then, on a separate occasion, following the isolation of the chondrocytes and their expansion in vitro, implanted within the lesion. The disadvantages of this therapeutic approach include the destruction of healthy cartilage—which may predispose the joint to osteoarthritic degeneration—the necessarily restricted availability of healthy tissue, the limited proliferative capacity of the donor cells—which declines with age—and the need for two surgical interventions. We postulated that it should be possible to induce synovial stem cells, which are characterized by high, age-independent, proliferative and chondrogenic differentiation capacities, to lay down cartilage within the outer juxtasynovial space after the transcutaneous implantation of a carrier bearing BMP-2 in a slow-release system. The chondrocytes could be isolated on-site and immediately used for ACI. To test this hypothesis, Chinchilla rabbits were used as an experimental model. A collagenous patch bearing BMP-2 in a slow-delivery vehicle was sutured to the inner face of the synovial membrane. The neoformed tissue was excised 5, 8, 11 and 14 days postimplantation for histological and histomorphometric analyses. Neoformed tissue was observed within the outer juxtasynovial space already on the 5th postimplantation day. It contained connective and adipose tissues, and a central nugget of growing cartilage. Between days 5 and 14, the absolute volume of cartilage increased, attaining a value of 12 mm3 at the latter juncture. Bone was deposited in measurable quantities from the 11th day onwards, but owing to resorption, the net volume did not exceed 1.5 mm3 (14th day). The findings confirm our hypothesis. The quantity of neoformed cartilage that is deposited after only 1 week within the outer juxtasynovial space would yield sufficient cells for ACI. Since the BMP-2-bearing patches would be implanted transcutaneously in humans, only one surgical or arthroscopic intervention would be called for. Moreover, most importantly, sufficient numbers of cells could be generated in patients of all ages.
Introduction
I
Given the advisability of removing only a small mass of healthy tissue and the intrinsically very low cellularity of adult human articular cartilage, 6 only limited numbers of cells can be generated by the in vitro expansion step that precedes ACI or MACI. Another disadvantage of the ACI and the MACI approaches is that two surgical or arthroscopic interventions are necessary (one to harvest the cells and the other to implant them after their in vitro expansion), which not only raises the cost of the undertaking but also heightens the risk of infection.
Against this background, the availability of an alternative approach whereby the aforementioned problems and restrictions could be circumvented would be welcome.
In a number of studies, cells that have been derived from the synovium or the synovial membrane of adult human patients, with or without osteoarthritic joint pathologies, have been shown to sustain their very high proliferative and differentiative capacities with increasing age. 7 Moreover, the synovial membrane is capable of healing spontaneously, even after the removal of relatively large portions of the layer. 8 Furthermore, experimental comparisons of the structural and the biomechanical properties of cartilaginous tissue that was generated by stem cells of different tissue origins, such as the bone marrow, the perichondrium, adipose tissue, muscle or the synovium, have revealed these to resemble most closely the native situation when using the latter source.9,10
On the basis of these data, we hypothesize that it should be possible to induce the formation of cartilaginous tissue within the outer juxtasynovial space of a joint in a human patient—by the local and temporary subcutaneous deposition (to avoid an opening of the joint cavity) of a spatially confinable carrier bearing the signaling agent BMP-2 in a freely soluble form to stimulate the proliferation of the synovial cells and in a delayed-release system to trigger their timely chondrogenic differentiation. The mass of synovium-derived cartilaginous tissue thereby generated could then be used for ACI or MACI, for which purpose only one arthrotomy would be necessary (to implant the construct [MACI] or the isolated chondrocytes [ACI]). By this means, a sufficient number of autologous chondrocytes could be generated in all patients, irrespective of their age.
The principles of this hypothesis were tested in Chinchilla rabbits. BMP-2 was trapped within small, fibrin-impregnated collagenous patches in both a freely soluble (for immediate availability) and a liposome-encapsulated form (for slow release). The tissue mass that was generated within the outer juxtasynovial space was excised 5, 8, 11 and 14 days later for an analysis of its volume and composition. The data thereby gleaned revealed the neogenerated tissue masses within the outer juxtasynovial space to contain significant amounts of cartilaginous tissue, which could be readily implemented for synovium-based (sb) ACI (sb-ACI) or MACI (sb-MACI).
Materials and Methods
Experimental design
To test our hypothesis that significant amounts of cartilaginous tissue can be generated within the outer juxtasynovial space of a joint by the local deposition of a carrier containing a proliferative and a chondrogenic-differentiation agent, small, fibrin-impregnated collagenous patches bearing BMP-2 as a freely soluble agent and in a liposome-encapsulated form were implanted within the inner juxtasynovial compartment. Owing to the small size of the knee joint and the outer juxtasynovial space in rabbits, the patches were surgically sutured to the inner face of the synovial membrane, namely, they were implanted within the inner juxtasynovial compartment (Fig. 1). In larger mammals, direct placement within the outer juxtasynovial space would not be a problematic procedure. The patch-associated tissues were excised 5, 8, 11 and 14 days later for histological typing and for a histomorphometric analysis of their volume fractions.

Experimental groups
Thirty-four sexually mature Chinchilla rabbits (male and female) were utilized for this study. In this species, sexual maturity is attained after the 3rd postnatal month, by which time growth of the knee joint cartilage has ceased. 11 Two groups were established: (1) an experimental one, in which the collagenous patch contained BMP-2 in a freely soluble (275 μg/mL) and in a liposome-encapsulated form (780 μg/mL), and (2) a negative control, in which both the freely soluble and the liposome-encapsulated forms of the signaling agent were replaced with physiological (0.9%) saline. Each of the two groups consisted of 16 animals, 4 of which were sacrificed at each of the 4 time points. For the time points 8 and 14 days, an additional (reserve) animal was included in the experimental group.
Animals and surgery
The study was conducted with the approval of the cantonal authorities for animal experimentation, and the rabbits were husbanded in accordance with the stipulations of the animal welfare acts at the cantonal, national and international levels. For the surgical placement of the collagenous patches within the inner juxtasynovial space, the rabbits were anesthetized with an intramuscular injection of ketamine hydrochloride (25 mg/kg of body weight) and xylazine (5 mg/kg of body weight). Sedation was maintained by the intravenous administration of ketamine (5 mg/kg of body weight) and gaseous nitrous oxide.
Following the exposure of the two knee joints by lateral arthrotomy, one patch was sutured to the inner face of the synovial membrane covering the infrapatellar fat pad in each. Per animal, one knee joint was destined to receive an experimental (BMP-2-containing) patch and the contralateral one a negative control (saline-containing) patch, whereby the influence of cross effects (via the systemic transportation of BMP-2) could be excluded. The surgical wound was closed in layers. Postoperatively, the animals were intravenously injected with a single prophylactic dose of tetracycline (Vibranvenös® [5 mg/kg of body weight]). The rabbits were permitted free cage movement until the time of sacrifice. They were killed in a generally anesthetized state by an intravenous injection of potassium chloride (2 mEq/kg of body weight), which induced cardiac arrest.
BMP-2-release system
Collagenous patches (6×2×0.9 mm) were excised under sterile conditions from commercially available sheets of Helistat® (13×0.9×25 mm). They were then immersed in phosphate-buffered physiological (0.9%) saline (pH 7.4) containing bovine fibrinogen (21 mg/mL), freely soluble BMP-2 (275 μg/mL) and liposome-encapsulated BMP-2 (780 μg/mL). BMP-2-encapsulated liposomes were prepared according to a standard procedure. 12 The uptake of BMP-2 by the liposomes was estimated to be 75%, thereby resulting in a total loading dose of 8.4 μg per patch. Given that the average volume of a patch was 10.8 μL, the amount of freely soluble BMP-2 contained by each was estimated to be 3.0 μg.
Shortly before implantation, one drop of thrombin (1 U/mL) was added to each patch to induce fibrin polymerization within its volume and to enhance the retention of the soluble components in situ. 13 The human recombinant BMP-2 was of clinical grade (Infuse®; Medtronic). The chosen BMP-2 concentrations (freely soluble and liposome-encapsulated) were estimated from preclinical literature data to be high enough to induce proliferative and chondrogenic effects, but sufficiently low to avoid the triggering of undesired side effects.
The biological rationale for combining freely soluble BMP-2 at a low concentration with liposome-encapsulated BMP-2 at a high one is based on the findings of earlier studies.
The biological effects of BMP-2 are known to be highly concentration dependent. 13 The recruitment and the proliferation of chondroprogenitor cells are triggered at low concentrations of BMP-2 (a few ng/mL), 14 whereas their chondrogenic differentiation is stimulated at high activity levels (several hundred μg/mL). 15 While low concentrations of freely soluble BMP-2 are locally well tolerated, higher ones are associated with deleterious consequences that must be averted.16,17 Hence, to satisfy the biological needs of chondrogenic differentiation, BMP-2 is encapsulated at a high concentration within liposomes, wherefrom it is liberated gradually, at a steady rate, and in a timely cell-mediated manner, after the peak proliferative response of the chondroprogenitor cells to the low concentration of the agent in a freely soluble form has been attained. 14
Tissue processing and analysis
All but one of the 34 rabbits survived the postoperative course in a disease-free state. Following sacrifice, the knee joints were surgically opened and inspected for signs of pathology (e.g., synovitis, effusion or osteophyte formation). The synovial membrane, as well as the juxtasynovial tissue in the subpatellar area where the patch had been placed, were excised well beyond the lateral extensions of the patch and deep towards the outer surface of the limb.
The excised tissue mass was chemically fixed as a whole for 4 to 6 days at ambient temperature in a solution containing glutaraldehyde (2.5%) and formaldehyde (2.5%), which was buffered with 0.1 M sodium cacodylate (pH 7.4). 18 The specimens were then dehydrated in a graded series of increasing ethanol concentration and embedded in methyl methacrylate. Serial cuts through each tissue block were produced perpendicular to its longitudinal axis, at a fixed interval of 1 mm, using a Leco® diamond saw (Leco corporation). The specimens were then glued to polished Plexiglas object holders, milled to a thickness of ∼80 to 100 μm with a Reichert Polycut E apparatus (Reichert-Jung), polished, and surface stained with McNeil's Tetrachrome/Toluidine Blue O/basic Fuchsin. 13
The specimens were examined in a Nikon Eclipse microscope. Neoformed tissue that was associated with the collagenous patches was identified on the basis of morphological criteria. Well-established criteria were implemented to identify chondrocytes and a cartilaginous matrix as follows: rounded cell profiles with surrounding lacunae, metachromatically stained pericellular rims, metachromasia of the intercellular substance, and the absence of a vascular supply. 19 The findings appertaining to these features were internally cross checked against the corresponding ones in normal articular cartilage.
The first to the last sections of the series in the identified areas were collected for further microscopic and histomorphometric analyses.
Using a low magnification (×4-objective), the total spatial area that was occupied by transformed and/or neoformed tissue was determined; this value was used to estimate the reference volume of the transformed tissue area.
At a higher magnification (×10-objective), a systematic random sampling protocol 20 was applied to sample the areas for the tissue typing analysis. At each time point, the volume of the neoformed tissue was estimated using Cavalieri's principle. 21 The volume fraction and the absolute volumes of the different tissue types within the reference volume were estimated using the point-counting technique that was elaborated by Delesse and by Gundersen (for review, see Ref. 21 ). For the point-counting procedure, appropriate test systems were designed to ensure accuracy and to satisfy statistical needs.
Statistics
The numerical data are presented in Figure 3 as mean values together with the standard error of the mean, and in Tables 1 and 2 as mean values in absolute terms together with the coefficient of error (Tables 1 and 2) and the coefficient of variation (Table 1). Data appertaining to each group were compared using a one-way analysis of variance. The level of significance was set at p<0.05. The SPSS statistical software (version 11.0.4) for Apple McIntosh computers was used for the statistical evaluation. Post-hoc comparisons were made using Bonferroni corrections
CE, coefficient of error; CV, coefficient of variation.
Results
To test the hypothesis that synovial tissue can be induced to undergo chondrogenic differentiation by the placement of a BMP-2-bearing, slow-release carrier system within the juxtasynovial space, collagenous patches containing a freely soluble and a liposome-encapsulated depot of BMP-2 were sutured to the inner face of the synovial membrane (viz., they were introduced into the inner juxtasynovial compartment) (Fig. 1A) in the knee joints of sexually mature (3- to 4-month-old) Chinchilla rabbits.
Each of the 34 animals recovered fully from the surgical intervention, and all but one survived the postoperative course in a disease-free state. The sole exception (in the negative-control group) died suddenly for unknown reasons before the scheduled time of sacrifice (day 8). During the postoperative phase, the rabbits manifested no unusual behavioral traits, were not feverish, and underwent no weight loss. Postmortem, the amputated knee joints evinced neither macroscopic nor microscopic signs of effusion, of synovial irritation or swelling, or of osteophyte formation within joint-associated structures. Within the outer juxtasynovial space, a dense mass of tissue was observed in close topographic proximity to each of the patches that were deposited within the inner juxtasynovial compartment. The patches themselves had undergone considerable shrinkage and/or degradation and, in some instances, had been completely resorbed.
On the 5th postoperative day, the tissue mass that had been excised from the experimental group of animals had a histological appearance that is typified in Figure 1B. Within the immediate outer juxtasynovial space, a central core of densely packed cells was observed, which manifested the typical morphological characteristics of chondrocytes (Fig. 2). These chondrocytes were embedded within an intercellular substance that evinced the typical metachromatic staining properties of a cartilaginous matrix. The nugget of cartilaginous tissue was mantled by a lower density zone of chondroprogenitor cells, which, in turn, was skirted by vascularized adipose and connective tissues that invaded the outer juxtasynovial compartment. In Figures 1B and 2, small remnants of the deposited collagenous patch can be identified.
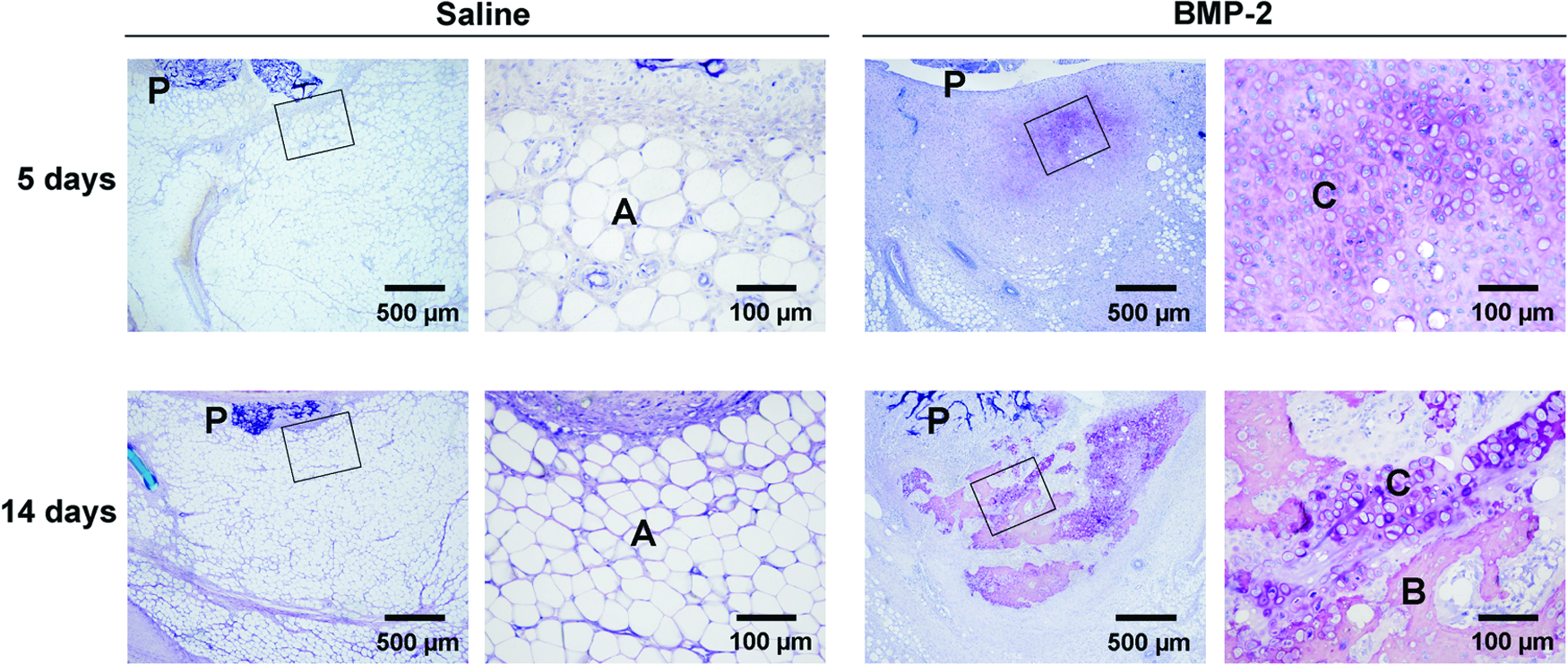
Light micrographs of sections through neoformed tissue masses that were generated within the outer juxtasynovial space of the knee joints of Chinchilla rabbits in the control (saline) and the experimental (BMP-2) groups, 5 and 14 days after the suturing of a collagenous patch to the inner surface of the synovial membrane (within the inner juxtasynovial compartment). In the control group, adipose tissue (A) is associated with remnants of the collagenous patch (P), but neither cartilaginous nor osseous tissue has been deposited. The boxed areas in the left-hand images are represented at a higher magnification in the right-hand ones. In the experimental group, a nugget of cartilaginous tissue (C) is apparent close to the collagenous patch (P) already on the 5th day; by the 14th day, its area had expanded. The boxed areas in the left-hand images are represented at a higher magnification in the right-hand ones. The latter reveal the features that are typically manifested by chondrocytes in conventionally processed histological sections that have been stained with Toluidine Blue; an intensely stained shrunken perikaryon is surrounded by a pale-staining (empty) lacuna (a shrinkage artifact), which in turn is adumbrated by a metachromatically stained pericellular rim; the cartilaginous matrix is likewise metachromatically stained. By the 14th day, signs of chondrocytic hypertrophy (an increase in cell profile size) and matrical calcification (an increase in staining intensity), as well as osseous tissue formation (B), are evident. The bony tissue is typical of its kind; it contains osteocytes and is delimited by an epithelium-like layer of osteoblasts. Eighty-micrometer-thick sections, surface stained with McNeil's Tetrachrome/Toluidine Blue O/basic Fuchsin. Color images available online at www.liebertpub.com/tea
On the 14th day, the mean absolute volume of neoformed tissue in the experimental group of animals was 70.0 mm3 (Table 1). The coefficient of error was high (up to 63.0%). The reason thereof could lie in the special positioning of the patch within the inner juxtasynovial compartment, which renders it differentially susceptible to interanimal variations in biomechanical-loading influences during the postoperative phase of free cage movement. Individual differences in the degree of firmness with which a patch is affixed to the inner face of the synovial membrane could also be a contributory factor. In larger mammals, these model-associated problems would be circumvented, in so far as the patches would be transcutaneously placed directly within the outer juxtasynovial space, in which case the coefficient of error would be expected to fall within a narrower range.
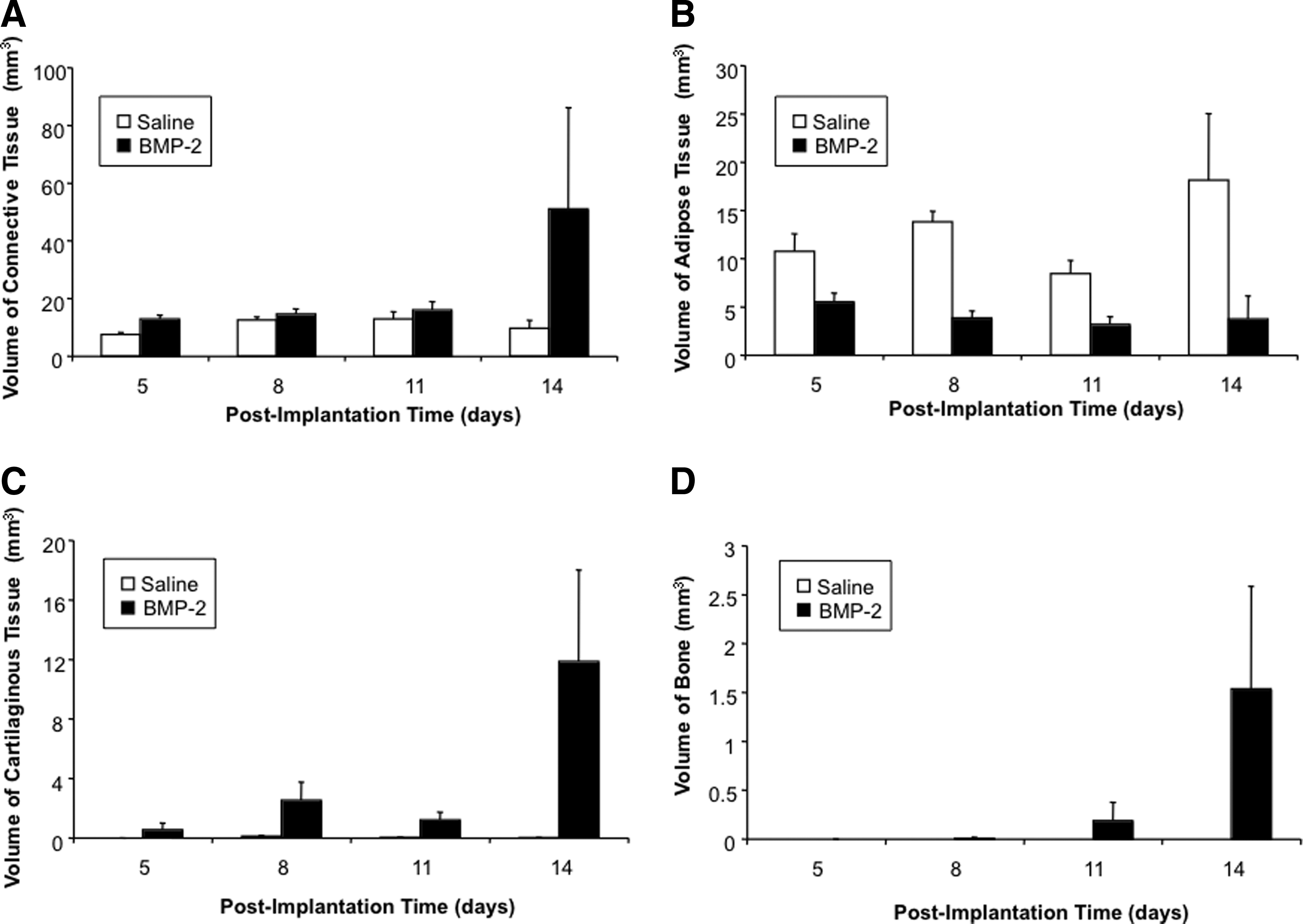
The results of the histomorphometric analysis of the neoformed tissue are summarized in Figure 3. The absolute volumes of connective tissue (Fig. 3A), adipose tissue (Fig. 3B), cartilaginous tissue (Fig. 3C) and osseous tissue (Fig. 3D) are represented as a function of time for the experimental group (BMP-2-bearing patch) and the negative control.
Absolute volumes of connective tissue
Figure 3A reveals that in the negative control group, the mean absolute volume of connective tissue peaked on day 8, a value of ∼12.6 mm3 having been attained by this juncture. Thereafter, no significant change in this parameter was observed, although the coefficient of error increased with time. In the experimental group, the mean absolute volume of connective tissue likewise peaked on day 8 (14.6 mm3) and the coefficient of error similarly increased with time. The higher mean value on day 14 (51 mm3) is attributable to an outlier, in which rabbit, a value of 190 mm3 was attained; if this animal is excluded, the mean value would be 16.2 mm3.
Figure 3B depicts temporal changes in the absolute volumes of adipose tissue in the two groups. In the negative control group, the mean absolute volume of adipose tissue changed erratically with time, although the differences were not statistically significant. The mean value over the entire monitoring period was 12.8 mm3. In the experimental group, the mean absolute volume of adipose tissue was generally much lower than in the negative control and decreased steadily with time up to day 11, from a value of 5.5 mm3 on day 5 to one of 3.1 mm3 on day 11; the coefficient of error consistently increased with time (16.4% to 62.8%). The progressive decrease in the absolute volume of adipose tissue in the experimental group may be suggestive of either a direct antilipogenic effect or an indirect anti-inflammatory influence.
An inspection of Figure 3C reveals that in the negative control group, no cartilaginous tissue was formed during the 14-day monitoring period. In the experimental group, the mean absolute volume of cartilaginous tissue increased erratically with time, from a value of 0.5 mm3 on day 5 to one of 11.9 mm3 on day 14. The coefficient of error was high, ranging from 41% to 80.6%, which would account for the lower mean volume on day 11. Between days 5 and 8, the mean absolute volume of cartilaginous tissue increased nearly 5-fold and likewise between days 8 and 14. However, when the different sizes of the time windows are taken into account (Δt=3 days vs. Δt=6 days), the mean absolute volume of cartilaginous tissue was found to increase at a rate of 0.7 mm3/day between days 5 and 8, and at one of 1.5 mm3/day between days 8 and 14, namely, at an almost doubled daily rate during the later phase.
In accordance with our expectations, the BMP-2-induced process of chondrogenic differentiation continued along a downstream course, culminating in cartilage hypertrophy, mineralization of the extracellular matrix, and the formation of bone (Fig. 3D). Due to the absence of a stable mechanical stress field and to a depletion of the BMP-2 depot, the osteogenic activity would be expected to ultimately cease.22,23
Osseous tissue was first observed on day 8 (Fig. 3D), albeit at a negligible level (0.01 mm3) and in only one animal. Thereafter, the mean absolute volume of bone increased steadily, but with a high coefficient of error (100% on day 11 and 68.2% on day 14). Compared to the mean absolute volume of cartilaginous tissue on day 14 (11.8 mm3), the mean absolute volume of bone was 8-fold lower (1.5 mm3) at the same juncture. While the rate of cartilaginous tissue formation was estimated to be 1.5 mm3/day (between days 8 and 14), the rate of bone formation was, at 0.25 mm3/day (between days 8 and 14), 6-fold lower. Since the values represented in Figure 3D are net bone volumes, the lower levels could conceivably embrace concomitant bone resorption activity (see Discussion). It is possible that after day 14, the mean absolute volume of bone might again increase. 22 However, owing to the high coefficient of error at this latter juncture, a reasonable prediction of such an event is not possible.
These data, which are summarized numerically in Table 2, reveal particularly the temporal stability of the connective tissue volume in the negative control group. In the experimental group, the temporal increase in the mean absolute volume of cartilaginous tissue and the time lag in the formation of bone at a much lower level are worthy of note; so, too, is the temporal decrease in the mean absolute volume of adipose tissue.
Discussion
In clinical practice, tissue-engineering-based therapeutic approaches are nowadays commonly instigated to induce the repair of damaged articular cartilage. One of the currently used strategies is ACI, 1 in which suspensions of cells are employed, and a more recently introduced alternative, namely, MACI,2,4 in which the cells are trapped within a suitable carrier material.
The drawbacks that are associated with these approaches include the narrowness of the age bracket of the patient group that is likely to derive benefits from the interventions, the limited availability of healthy autologous cartilage, surgically induced damage to the healthy tissue from which the autologous chondrocytes are derived, and the need for intra-articular surgery (or arthroscopy) on two separate occasions, which heightens the risk of joint infection.2,4 Most of these drawbacks could be avoided if the autologous chondrocytes could be locally and nascently generated in vivo from an alternative tissue source, such as the synovial membrane. There exists a wealth of data in support of the contention that stem cells within the synovium manifest chondrogenic potential (for recent reviews of this topic, see Refs.9,10,24). The precise topographical location of this pool of chondroprogenitor cells has not, as yet, been unequivocally identified. Albeit so, existing evidence points to the synovial lining and to the outer juxtasynovial perivascular space, wherein indeed the nuggets of neoformed cartilage were observed (Fig. 1B). The pool of chondroprogenitor cells appears to be of heterogeneous composition.9,10,24
The synovium harbors stem cells that manifest not only a high proliferative capacity but also a great potential to differentiate into chondrocytes,9,10 and these capabilities do not decline with increasing age. 7 Furthermore, the chondrocytes that are generated by the differentiation of synovial stem cells lay down an extracellular matrix that compositionally resembles that of the cartilage in the host joint. 9 Owing to the high proliferative capacity of the synovial stem cells, adequate quantities of autologous chondrocytes for autotransplantation could be speedily generated, and the destruction of healthy cartilage could be avoided.
Last but not least, if the cartilaginous tissue could be induced to form within the outer juxtasynovial space by the transcutaneous introduction of a chondrogenic agent-bearing carrier material, then such an sb-ACI approach could be executed in its entirety during the course of a single surgical arthrotomy or arthroscopic intervention. If sufficient quantities of cartilaginous tissue could be thereby generated, then the need for tissue shipping as well as for cell culturing and expansion would be obviated, since adequate numbers of autologous chondrocytes could be prepared on-site by the instigation of a simple, intraoperative isolation procedure. 25
Sufficient quantities of cells could be generated in the outer juxtasynovial space within 1 week of the chondrogenic induction process, thereby curtailing the waiting time by several weeks between the initial intervention (which would involve only the transcutaneous placement of a chondrogenic patch within the outer juxtasynovial space) and the second intervention (relative to the time span that must be reckoned with for the conventional ACI and MACI approaches). The risk of joint infection and the healthcare costs of the therapy would be likewise reduced. One of the greatest advantages of sb-ACI would be that it could be instigated in patients of all ages, which would considerably broaden the currently narrow scope of clinical indications 4 to embrace also other fields of pathology. 26
Our data reveal that in the experimental group (patch bearing freely soluble and liposome-encapsulated BMP-2), the mean absolute volume of neoformed tissue had peaked by the 5th day (Table 1), and thereafter no further significant changes in this parameter were sustained (excluding the outlier on day 14). We assume that postimplantation, the foreign body type of inflammatory response to the collagenous patch was similar to that triggered by any other alien material. 27 Support for this contention is afforded by the observation that, on the 5th day, the compositional make-up of the neoformed tissue was similar in the experimental and the negative-control groups. Indeed, since the basic components of the patches were the same in each group (collagen, fibrins, liposomes), the response of the synovium thereto would not be expected to be otherwise than similar in each case.
At a later juncture, a fibrotic response to the implanted patches would be mounted. However, if the material was biocompatible with the synovial compartment, then this response to it would be constrained. Indeed, no signs of fibrotic encapsulation were apparent at any stage, either morphologically or histomorphometrically. The inflammatory response of a tissue compartment to BMP-2 has been previously shown to be low provided the signaling agent is liberated gradually, at a low-concentration level, from a delayed-release system, 28 which was the case using our setup. The sequestration of BMP-2 within liposomes protects the milieu within which they are implanted from being swamped in a single abrupt burst with a massive dose of the agent, which carries the risk of inducing untoward side effects.
It is worthy of mention here that the human recombinant BMP-2 that was used in our study is the only chondrogenic factor that is commercially available in a 100%-pure unadulterated form, as a clinically approved medical-grade product. Moreover, in a previous study, we demonstrated that the chondrogenic differentiation of synovial stem cells in vivo can be induced only by members of the TGF-β superfamily. 15 Among the members of the TGF-β superfamily, BMP-2 was considered to be the candidate of choice, in so far as its use is associated with the lowest risk of inducing untoward side effects.
In the experimental group, the mean absolute volume of cartilaginous tissue increased progressively with time (Fig. 3C), and after the 8th day, bone was deposited (Fig. 3D). This course of events was expected, and accords with the classical BMP-2-induced differentiation cascade that has been described in detail by Urist and Reddi. 22 Ultimately, the neoformed cartilaginous and osseous tissues would be resorbed in the absence of a stable mechanical stress field upon the depletion of the patch-borne depot of BMP-2. Hence, the neoformed cartilaginous tissue would need to be removed from the outer juxtasynovial space before this event. The time window could be readily protracted by ensuring that the stimulus for chondrogenesis is sustained for a sufficient period.
In nature, joint-associated osteophytes are formed within the outer juxtasynovial space during the course of osteoarthritis, 29 even though the cartilaginous and the osseous tissues are undergoing continual degradation. Indeed, it is these very degradative processes that are responsible for the maintenance of osteophyte formation, since they free up at a steady rate and at low doses intrinsic supplies of BMP-2. 30
One concern that may be expressed regarding our setup is that, within an osteoarthritic environment, the release of BMP-2 from a collagenous patch, placed within the outer juxtasynovial compartment (in humans), could trigger the neoformation of osteophytes or the further growth of pre-existing ones. However, the low-dose pool of freely soluble BMP-2 that is immediately available would be rapidly eliminated, and the higher dose liposome-encapsulated depot of the agent that is liberated gradually at a steady rate of about 1 μg/day (see below), in a cell-mediated manner, would be exhausted after about a week.
Given that the local application of a high dose of BMP-7 (500 μg) to an osteoarthritic joint fails to trigger either the neoformation of osteophytes or the growth of pre-existing ones, even after repeated injections on a weekly basis,31,32 it is unlikely that our setup with BMP-2 would pose a problem in this respect. Indeed, BMP-2 is deemed to play only a subsidiary role in the formation of osteophytes. 33 Also, although the chronic production of BMP-2 within the synovium and vicinal tissues of osteoarthritic joints can severely aggravate the development of pre-existing osteophytes, 34 the agent's mode of delivery from the higher dose depot (liposomes) in our setup would not conduce to this end.
The patterns of cartilaginous and osseous tissue formation suggest that the optimal juncture for the removal of the former is about 1 week after implantation. At this time point, the absolute volume of bone is still negligible. If particularly large articular cartilage defects are to be repaired, thereby necessitating the generation of higher numbers of chondrocytes, the harvesting time could be delayed by a week. However, owing to the increased volume of bone within the outer juxtasynovial space, the patient might experience some local discomfort. Moreover, the cell isolation procedure would be thereby rendered more complex.
Instead of profiting from the higher rate of cartilaginous tissue formation during the 2nd postimplantation week, several smaller patches could be inserted at different sites within the outer juxtasynovial space and then removed after 1 week. Moreover, since larger patches could be implanted in humans than in rabbits, much larger masses of tissue could be generated within the optimal 1-week time frame. The use of an alternative drug-release system would be another option open to consideration, for example, an injectable suspension of BMP-2-bearing granules, which would undergo solidification in situ and be only slowly resorbed. Such a system would offer the advantages of flexibility and adaptability to individual patient needs.
Even in Chinchilla rabbits, the mean absolute volume of cartilaginous tissue that can be generated during the 1st postimplantation week is, at 2.54 mm3, large. Given that the average volume of a newly formed chondrocyte with its surrounding matrix is about 5,000 μm3, 6 then this small mass of cartilaginous tissue would contain totally about 500,000 chondrocytes, and the production level could be readily scaled up. After 2 weeks, the mass of neoformed cartilaginous tissue would contain about 2.4 million chondrocytes.
In humans, the biopsy of articular cartilage that is removed for ACI weighs about 280 mg, 3 which corresponds to a volume of about 280 mm3. This volume of tissue is ∼110-fold greater than that generated after the juxtasynovial implantation of one small BMP-2-bearing patch.
The human biopsy delivers about 730,000 chondrocytes from the different zones of cartilage, and probably only those originating from the transitional and the upper radial layers undergo proliferation, namely, about 50% of the population (365,000 cells), and only in young patients. The same pool size of proliferating chondrocytes could be obtained from a 1.8-mm3 volume of the cartilaginous tissue that is generated by a BMP-2-bearing synovial patch in less than 8 days, and in patients of all ages, which is a minuscule amount compared to the mass of human articular cartilage that is needed to generate sufficient cells for ACI 35 or MACI (a 150-fold greater volume). This volume of neoformed cartilaginous tissue could be produced within less than a week by the placement of one small BMP-2-bearing patch within the outer juxtasynovial compartment.
During the first 11 days, the coefficients of error for the volumes of connective and adipose tissues in the experimental group fell within the expected interanimal variation range (10.9% to 25.3%). However, on day 14, the values increased dramatically (Table 2). Although we cannot account for this unexpected observation, the finding nevertheless reinforces the view that, following the instigation of an articular cartilage repair strategy, the neoformed tissue (entire mass) should be harvested for analysis about one week after the surgical intervention, during which time frame, the interanimal variation would be expected to fall within a predictable range.
For ACI or MACI, a few dozen million cells are needed, 3 which are generated by in vitro expansion. Similar numbers of chondrocytes could be generated by a simple upgrading of the juxtasynovial patch approach without the need for an in vitro expansion step, and the cells could be readily isolated from the tissue on-site using a simple intraoperative procedure. 25
On the basis of these approximate quantitative estimations, it is evident that sb-ACI or sb-MACI would offer many advantages over the classical approaches. Since only one surgical or arthroscopic intervention would be required for intra-articular access, the risk of joint infection would be reduced and the duration of the treatment period curtailed, which would lower the expense of the therapy. Moreover, most importantly, sb-ACI or sb-MACI could be performed in patients of all ages with the expectation of a successful outcome.
Using the Chinchilla rabbit as an animal model to test the feasibility of the juxtasynovial patch approach, it was not possible to set up the situation that would be established in humans, owing to the small size of the knee joint, which approximates to that of the basal thumb joint in humans. However, even though the patches could not be placed within the outer juxtasynovial space, the yield of chondrocytes was high. Placement within the outer juxtasynovial space instead of suturing to the inner surface of the synovial membrane would undoubtedly enhance the yield of cells.
The gradual liberation of BMP-2 from the delayed-release system (liposomes) within which the agent was initially confined at a high concentration was obviously advantageous, in so far as no untoward side effects (such as osteophyte formation, effusion, irritation or synovitis) were observed either macroscopically or microscopically. The local containment of BMP-2 within liposomes at a high activity level and its gradual liberation therefrom at a steady rate through the mediation of local cell populations are necessary to avoid the deleterious consequences of high local concentrations of the agent in a freely diffusable form, 36 which are particularly conducive to the formation of osteophytes, 37 as aforementioned.
On the basis of kinetic studies appertaining to the liposome-release profile of another member of the TGF-β superfamily, 38 we estimated that the passive leakage of BMP-2 from the liposomes would not exceed the low-concentration level of 3% (250 ng)/day. The BMP-2 that would be liberated through the mediation of local cell populations during the resorption and the remodeling of the collagenous patch, and which would be to a large extent spatially confined (not freely diffusable) during these processes, would amount to ∼1 μg/day, 38 assuming them to occupy a time span of about 8 days, which still falls well within the bounds of a clinically safe range.
It is known that when BMP-2 is delivered gradually in a controlled manner and at a low dose, it exerts an anti-inflammatory effect, which may be indirectly linked to the antilipogenic one. 28 A possible mechanistic explanation of this phenomenon has been proposed, 28 but the postulate has not yet been experimentally confirmed. It should also be borne in mind that the chondrogenic activity in such a system may be positively influenced (not impaired) by the local conditions of mechanical instability, 23 as exemplified in fracture healing when chondrogenesis proceeds to completion and results in a pseudoarthrotic state. 39 Indeed, even osteogenic activity can be sustained under adverse conditions of mechanical stability provided that BMP-2 is delivered gradually at a low dose and in a cell-mediated manner. 28
Our data reconfirm existing evidence that synovial tissue harbors stem cells that are capable of undergoing chondrogenic differentiation into cartilage-producing chondrocytes. This former evidence has been gleaned both from in vitro studies7,10 and under pathological conditions in vivo.30,40
Footnotes
Acknowledgments
This work was financially supported by the University of Bern. The authors acknowledge the surgical help of Dr. Iris Driesang.
Disclosure Statement
No competing financial interests exist.