
Abstract
Following the coordinated efforts of five established scientific organizations, this report, the sixth of its kind, describes activity in Europe for the year 2013 in the area of cellular and engineered tissue therapies, excluding hematopoietic stem cell (HSC) treatments for the reconstitution of hematopoiesis. Three hundred eighteen teams from 31 countries responded to the cellular and engineered tissue therapy survey; 145 teams from 25 countries reported treating 2187 patients, while a further 173 teams reported no activity. Indications were musculoskeletal/rheumatological disorders (45%; 89% autologous), cardiovascular disorders (20%; 99% autologous), hematology/oncology, predominantly prevention or treatment of graft versus host disease (GvHD) and HSC graft enhancement, (19%; <1% autologous), neurological disorders (3%; 100% autologous), gastrointestinal disorders (2%; 32% autologous), and other indications (11%; 67% autologous). The majority of autologous cells (88%) were used to treat musculoskeletal/rheumatological (57%) and cardiovascular (27%) disorders, whereas allogeneic cells were used mainly for hematology/oncology (64%). The reported cell types were mesenchymal stem/stromal cells (MSC) (49%), HSC (28%), chondrocytes (11%), dendritic cells (2%), keratinocytes (1%), and others (9%). In 46% of the grafts, cells were delivered following ex vivo expansion, sorted in 17% of the reported cases and transduced in only 3%. Thirty three percent of treatments were delivered intravenously or intra-arterially, and of the remaining 67%, 37% used a membrane/scaffold, 28% a suspension, and 2% a gel. The data are compared to those previously collected to identify trends in a still unpredictably evolving field.
Introduction
C
Against a background of innovations in science, together with the above-mentioned regulatory environment concerning the use of cellular and engineered tissue therapies, the European sections of the Tissue Engineering and Regenerative Medicine International Society (TERMIS-EU), of the International Society for Cellular Therapy (ISCT), of the International Federation for Adipose Therapeutics (IFATS), and of the International Cartilage Repair Society (ICRS), in a joint initiative with the European group for Blood and Marrow Transplantation (EBMT), established a survey of cellular and engineered tissue therapies. Since 2008, the number of patients treated in Europe with cells or engineered tissues has been collected and sorted by specific therapeutic indications, cell/tissue and donor types and, together with the processing and delivery modes, analysed to describe the evolving situation at the European level.3–7 It is thanks to the continued efforts of the different working groups that this yearly collection of data represents a means of monitoring changes and capturing trends in a complex and still rather unpredictably developing field.
In this study, we report the results of the sixth survey for the activity, related to patients treated in 2013. The information presented is generally available ahead of published studies, since safety/efficacy data are not required and is complementary to that available in public databases (e.g., www.clinicaltrials.gov), the survey specifying the number of treatments effectively conducted opposed to those planned.
Patients and Methods
Definitions
For the purpose of this survey, cellular and engineered tissue therapy is any clinical treatment based on living cells, excluding donor lymphocyte infusions and nonmanipulated hematopoietic cells, for hematological reconstitution.
Data collection and validation
Participating teams were, as in previous years, requested to report their data for 2013 by indication, cell type and source, donor type, processing method, and delivery mode. Some modifications were made to the survey form: dendritic cells were added to the cell type and source, the delivery mode was amended (intravenous/intra-arterial [i.v./i.a.] and intra-organ—either suspension, gel or membrane/scaffold), and a new question included to identify the number of patients treated as part of a clinical trial, as individualized/single cases or as a routine therapy.
The survey followed the traditional principles of the EBMT transplant activity survey, which concentrates on numbers of patients with a first cellular therapy. Six hundred eighty-seven teams known to be actively transplanting in 48 countries (39 European and 9 affiliated countries) were contacted for the 2013 EBMT survey, to which were added members of the other participating societies and teams who had contributed to any earlier survey. The non-European countries affiliated with the EBMT activity survey are Algeria, Iran, Israel, Jordan, Lebanon, Nigeria, Saudi Arabia, South Africa, and Tunisia. Extended questionnaires, in the format displayed in Supplementary Table 1 (Supplementary Data are available online at www-liebertpub-com.web.bisu.edu.cn/tea), were received in paper form and electronically.
Transplant rates
Transplant rates, defined as the reported numbers of patients receiving cellular or engineered tissue therapies and the number of teams reporting treatments per 10 million inhabitants, were computed for each country, without adjustments for patients who crossed borders or received treatment in a foreign country. Population numbers were obtained from the 2013 US census office database (www.census.gov).
Results
Participating teams
Three hundred eighteen teams from 31 countries (28 European, 3 EBMT affiliated countries) responded to the cellular and engineered tissue therapy survey of patients treated in 2013. One hundred forty-five teams (25 countries: 23 European, 2 EBMT affiliated—Iran, Israel) reported performing cellular or tissue-engineered therapies: 142 of these teams provided detailed information on indication, cell source and type, donor type, cell/tissue processing, and delivery mode. A further 173 teams reported no activity. Teams who reported treating patients for the previous survey edition (treatments in 2012) and did not respond this year were directly contacted with repeated personal messages. Teams that responded with detailed information on their activity are listed in Appendix 1 in alphabetical order of country, then city. In addition, their EBMT CIC code (if applicable), the total number of reported cellular or tissue-engineered therapies, and the split between allogeneic and autologous donors is included.
Number of cellular or tissue-engineered therapies and disease indications
According to the received reports, 2187 patients were treated with cellular or engineered tissue therapies: data on six patients were excluded from the analysis due to the absence of complete information. Of the remaining 2181 patients, 1552 (71%) were treated with autologous cells and 629 (30%) with allogeneic cells (Table 1). Indications were musculoskeletal/rheumatological disorders (45%; 89% autologous), cardiovascular disorders (20%; 99% autologous), hematology/oncology (predominantly prevention or treatment of graft versus host disease [GvHD], and hematopoietic stem cell [HSC] graft enhancement) (19%; <1% autologous), neurological disorders (3%; 100% autologous), gastrointestinal disorders (2%; 32% autologous), and other indications (11%; 67% autologous).
HSC, hematopoietic stem cell; MSC, mesenchymal stromal/stem cell; GvHD, graft versus host disease.
As in the previous year, cartilage and bone repair were by far the most frequently reported indications among the musculoskeletal/rheumatological disorders, comprising almost half of all treatments in this group, followed by reconstructive surgery/tissue enhancement (21% of treatments). Treatments for decubitus and leg ulcers were the main reasons for a cellular or engineered tissue therapy among the cardiovascular disorders, closely followed by peripheral artery disease, together accounting for 62% of treatments in this group of indications. The number of patients treated for neurological and gastrointestinal indications was fairly small (114) and mostly confined to Crohn's disease (gastrointestinal) followed by multiple sclerosis and amyotrophic lateral sclerosis (neurological). Among the remaining indications, most patients were treated for skin reconstruction (burns) or for solid tumor excision (Table 1). One hundred eighteen patients were reported under miscellaneous, that is, they were treated for indications other than those mentioned in the form, for example, for hemorrhagic cystitis.
Cell type, source, and donor type
The reported cell types were mesenchymal stem/stromal cells (MSC) (49%), HSC (28%), chondrocytes (11%), dendritic cells (2%), keratinocytes (1%), and others (9%). This year, no treatments were reported using dermal fibroblasts. From 1074 MSC-based therapies, 53% were autologous transplants, and of the 618 HSC treatments, 94% were autologous transplants (Table 1). Of the remaining cell sources, all chondrocyte transplants, 93% of dendritic cells, 21% of keratinocytes and 70% of other cell sources, were autologous.
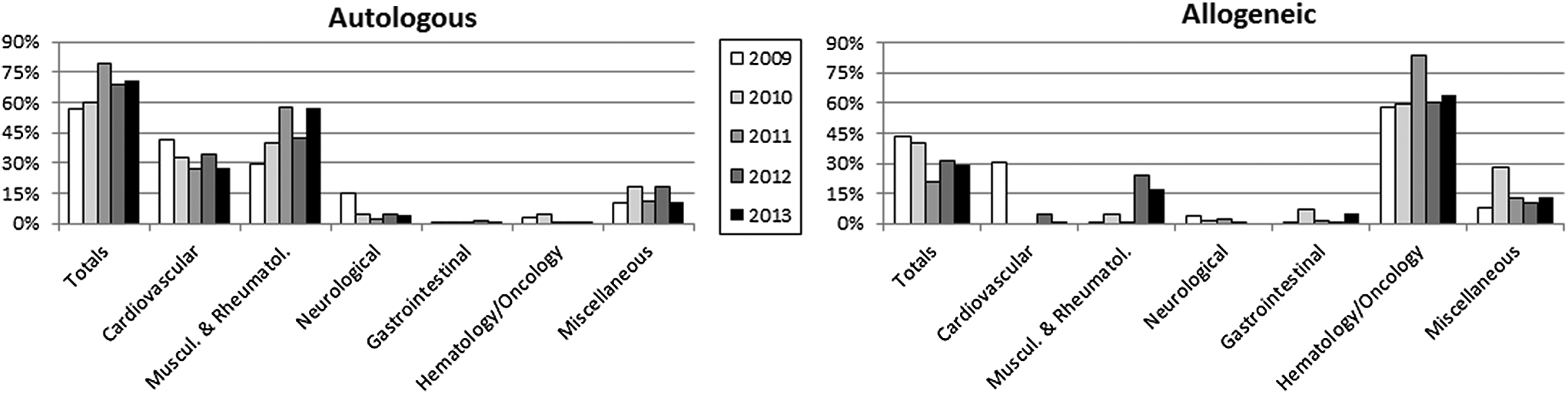
The majority of autologous cells (88%) were used to treat musculoskeletal/rheumatological, cardiovascular, or neurological indications (57%, 27%, and 4%, respectively). Although only a small number of patients (67) had neurological disorders, all treatments used autologous cells. The main uses of allogeneic cells were, as in previous years, for hematology/oncology (64%) and for musculoskeletal/rheumatological indications (17%), almost all of which were for cartilage repair (Fig. 1). The trends for the various therapy areas over the last 5 years are shown in Figure 2.

Percentage of indications for cellular and engineered tissue therapies in Europe in 2013, sorted by donor type. Data used for this chart were derived from the extended questionnaire and the standard European Group for Blood and Marrow Transplantation (EBMT) survey sheet.
In 2013, MSC were mostly obtained from bone marrow (69%) or adipose tissue (30%). MSC were used mainly for GvHD (32%) or for two musculoskeletal indications, namely cartilage repair (24%) and reconstructive surgery/tissue enhancement (19%). For the HSC treatments, cells were derived from peripheral blood (70%) or bone marrow (29%): 61% of them were used to treat cardiovascular disorders, mainly periperhal artery disease or decubitus and leg ulcers, and 25% for musculoskeletal/rheumatological indications, mainly bone repair. All chondrocyte preparations were for cartilage and bone repair. Keratinocytes were almost exclusively used for either skin reconstruction or reconstructive surgery/tissue enhancement. Only a small number of patients (40) were treated with dendritic cells, here identified as a cell source for the first time. These cells were used for solid tumor (29 patients), arthritis and liver insufficiency. The cell source “other” (i.e., not among those foreseen in the form) was reported for 183 (8%) patients. The teams also reported the use of combinational treatments, for example, fat cells augmented with monocytes from peripheral blood cells (in reconstructive surgery/tissue enhancement or chondrocytes with allogeneic MSC for cartilage repair). These could not be consistently captured by the format of the questionnaire and data display, but are worth being qualitatively mentioned here since they are in line with recently published trends.8,9 The use of hybrid products such as these, combining cell types or combining cells with bone marrow fraction or blood-derived additives, is clearly on the rise and will need to be monitored in a revised survey edition in future years.
Cell processing and delivery mode
Of all the grafted products, just under half underwent cell expansion (46%), 3% (55 patients only) were transduced, and 17% were sorted (Table 2). Ninety-two percent of cardiovascular, 53% of musculoskeletal/rheumatological, and 45% of neurological indications were treated with nonexpanded cells, while gastrointestinal indications were mainly treated (60%) with expanded cells. Expanded cells were also used for 94% of hematology/oncology treatments and 35% of treatments for skin reconstruction.
nonexp, nonexpanded.
Cell sorting was applied predominantly for musculoskeletal/rheumatological (69% of all sorted cells) and cardiovascular indications (18% of all sorted cells). 264 patients with musculoskeletal/rheumatological indications (27% of all patients in this group), of whom 201 were treated for cartilage repair, received treatment with sorted cells as did 69 patients with cardiovascular indications (16% of all patients in this group).
Of the 39% of cells reported to be processed using an automated device, most were used to treat musculoskeletal/rheumatological (50%) and cardiovascular (39%) indications.
Thirty-three percent of the cells were delivered intravenously or intra-arterially. Of the remaining 67% (intra-organ delivery), 37% used a membrane/scaffold, 28% a suspension, and 2% a gel (Table 3). Intravenous (i.v.) or intra-arterial (i.a.) delivery was reported for all hematology/oncology treatments (56% of all i.v. and i.a. treatments) and for 74% of gastrointestinal indications. Eighty-five percent of treatments delivered through a gel were for musculoskeletal/rheumatological indications (for either bone and cartilage repair or scleroderma). The use of a suspension for cell delivery was reported mainly for musculoskeletal/rheumatological (55%) and cardiovascular (28%) indications, while the use of a membrane/scaffold was split between musculoskeletal/rheumatological (64%), decubitus and leg ulcers (16%), peripheral artery disease (11%), and skin reconstruction (burns) (7%).
i.a, intra-arterial; i.v., intravenous.
Treatments for both musculoskeletal/rheumatological and cardiovascular indications were predominantly delivered through membrane/scaffold (53% and 52%, respectively) or suspension (40% and 34%, respectively), with 92% of treatments for skin reconstruction (burns) administered through membrane/scaffold. No neurological or gastrointestinal indications were treated using a gel or membrane/scaffold. As this revised approach to recording the mode of delivery was introduced with this survey, no identification of trends is possible.
Transplant rates and active teams
Reported cellular and engineered tissue therapies were performed in a limited number of countries and with different intensity. Figure 3 displays the reported transplants per 10 million inhabitants in the different European and EBMT-associated countries. The highest transplant rates (i.e., >40 per 10 million population) were reported in (in decreasing order) Slovenia, the Netherlands, Italy, Spain, Belgium, Denmark, the Czech Republic, Norway, and Switzerland.

Number of cellular and engineered tissue therapies per 10 million inhabitants reported in Europe in 2013.
The number of teams reporting cellular and tissue-engineered therapies were also mapped in the different European and EBMT-associated countries after normalization to the inhabitant numbers (Fig. 4). The number of reporting teams per 10 million inhabitants were higher than 4 in Slovenia, Finland, Belgium, Lithuania, the Netherlands, Switzerland, and Spain (again in decreasing order).

Number of teams per 10 million inhabitants reporting cellular and engineered tissue therapies in Europe in 2013.
As of last year, the top 10 countries (out of 31 total) accounted for 85% of all patients treated.
Treatments as part of a clinical trial versus individualized treatment or routine therapy
With this survey, teams were asked for the first time to report if patients were treated with cells/engineered tissues in the context of a clinical trial, as individualized/single case treatment, or as a routine therapy. Where information was provided (from 77 teams for 1479 patients, 70% of total patient number), 46% of patients were treated as routine therapy, 34% as part of a clinical trial, and 20% as individualized/single cases. Fourteen teams reported treating 675 patients with routine therapies: most (58%) were treated for musculoskeletal and rheumatological indications (of which 38% for reconstructive surgery/tissue enhancement and 50% for cartilage and bone repair), followed by cardiovascular disorders (32%, of which 60% for decubitus and leg ulcers and 40% for peripheral artery disease) and 6% for skin reconstruction following burns. Importantly, 64% of the treatments reported as “routine therapy” involved the use of fat- and/or peripheral blood-derived cells. Of the 33 teams who reported treating 502 patients as part of a clinical trial, most (59%) were treated for musculoskeletal and rheumatological indications (of which 53% for cartilage repair), followed by cardiovascular disorders (15%).
Discussion
The data collected for this sixth edition of the cellular and engineered tissue therapy survey show a modest increase from the previous year in both the number of reporting teams and number of patients treated. Since the survey's inception, the total number of teams reporting the use of cellular and engineered tissue therapies has risen from 143 in 2008 to 318 in 2013, with the number of teams reporting full data rising from 33 in 2008 to 142 in 2013. At the same time, the total number of patients treated has risen from 1040 in 2008 to 2187 in 2013 (Fig. 5).

We have compared the results obtained from patients treated in 2013 for specific indications with previous years and found few significant differences. Although no patients were treated for bypass graft in 2013, numbers in previous years were also rather limited (six in 2012 and nine in 2011). The treatments for patients with heart failure accounted for 9% of all cardiovascular ones, compared to 13% and 17%, in 2011 and 2012 respectively. This reduction can most likely be attributed to changes in a limited number of highly active teams, who did not respond to the survey this time.
As in the previous 2 years, the most used cell source in 2013 was MSC, accounting again for around 50% of the treatments. The most represented indication for their use was again GvHD prevention or treatment (15% of all patients, 333 in all). The use of dermal fibroblasts, employed almost exclusively for skin reconstruction in previous surveys, was not reported in 2013, indicating that the promise of bilayered or composite tissue-engineered skin10,11 is still not reflected in the clinical scenario, which is dominated by the more conventional use of keratinocytes only. The primary use of dendritic cells, although for a small number of patients (29 patients), was related to solid tumor, consistent with last year's report, followed by arthritis and liver insufficiency.
Analysis of treatments reported as being carried out in the context of clinical trials or as a routine therapy was combined with data on associated indications and cells used. Collectively, such assessments indicate that intra-operative isolation and use of cells, predominantly in the context of plastic and reconstructive surgery, are considered a routine treatment, while procedures employing cell expansion, and therefore subject to registry under ATMP (Advanced Therapy Medicinal Product) regulations, are prevalently considered experimental and thus part of a clinical trial. This trend is consistent with the fact that ATMPs are only allowed in the routine clinical practice after having passed cell quality and efficacy indicator checks, to assure patient, provider, payer, and policy maker of the safe and effective application of expensive and personalized treatments. In the specific context of cell-based cartilage repair, we received reports indicating a roughly 50-50 split between the use within a clinical trial or as a routine therapy. Underlying this dichotomy could be the fact that cartilage cell therapy is part of the reimbursement system only in some European countries. There is currently no way to predict the development of reimbursement of cell therapy for specific indications (e.g., cartilage repair) in individual EU regions and/or countries. This will have a considerable influence on the field and affect the number of patients who can be treated in future. Such considerations indicate that treatment selection and growth, or decline of treatment choice, is greatly influenced by both political and local economic factors and related to the social healthcare systems.
The fact that 66% of patients were treated as either individualized/single cases or part of routine therapy rather than as part of a clinical trial indicates that data from clinical trials represent a subset of those presented here. Nevertheless, analysis of trends from registered clinical studies (e.g., www.clinicaltrials.gov) and of market data from companies providing expansion of cells intended for cell therapy as a service would, although challenging, be highly informative to complement the yearly survey reports. We are aware that centers where cellular therapy treatments are performed likely in significant numbers did not participate in the survey and a personalized team-hunting strategy (e.g., toward previously active or publishing teams) is only partially effective. However, the program is based on answers supplied on a voluntary basis. The most convincing incentive for active teams to report through our survey will be (1) to demonstrate the increased recognition of the initiative by the field and (2) to convey the importance to further develop it through contributions which are transparently acknowledged without compromising opportunities to publish or protect clinical data.
Toward the end of 2014, IFATS, the International Federation for Adipose Therapeutics and Science, became a supporting society. This addition underlines that the survey program is continuing to receive growing recognition as a reference platform for the collection and dissemination of information that is not available in public databases or scientific publications. ISCT with its other sister societies has also been increasingly supportive of this European initiative since its inception. The international nature of most of the involved societies represents a push for widening the data collection to other world regions, with global repository of data, as well as for accelerating the process of data collection and analysis, toward more timely dissemination of the information to the Regenerative Medicine and Tissue Engineering Community. Indeed a larger collective effort will be necessary to guarantee that cell-based and tissue-engineered therapies, despite the challenges to be overcome, will seriously develop into global opportunities to counteract still lethal diseases and unmet clinical needs.
Footnotes
Acknowledgments
We greatly appreciate the cooperation of all participating teams and their staff (listed in ![]() ) and the engagement of the different working groups and their highly committed representatives, namely TERMIS-EU (Sarah Wilburn), ISCT-Europe (Edwin Wagena), ICRS (Stephan Seiler), IFATS (Marco Helder), and EBMT. We are also grateful to Dietlinde John for her database support.
) and the engagement of the different working groups and their highly committed representatives, namely TERMIS-EU (Sarah Wilburn), ISCT-Europe (Edwin Wagena), ICRS (Stephan Seiler), IFATS (Marco Helder), and EBMT. We are also grateful to Dietlinde John for her database support.
This project has received funding from the European Union's Seventh Programme for research, technological development, and demonstration under grant agreement No. 278807 (BIO-COMET). EBMT is supported by grants from the corporate sponsors: Gentium S.p.A., Molmed S.p.A., AstellasPharma Europe Ltd., Celgene International SARL, Clinigen Group Ltd., Gilead Sciences Europe Ltd., GlaxoSmithKline plc, Hospira Inc., Medac Hematology GmbH, MiltenyiBiotec GmbH, MSD Sharp&Dohme GmbH, Neovii Biotech GmbH, Sanofi Oncology, Takeda, Terumo BCT, Therakos Photopheresis, Alexion, Amgen Oncology GmbH, Exem Consulting SA, Kiadispharma, Macropharma, Mundipharma, and Pierre Fabre Médicament SAS.
Disclosure statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.