
Abstract
Current osseointegrated dental implants have been widely used for the rehabilitation of tooth loss. Although dental implants are considered an available treatment in the paradigm shift from traditional dental therapies, such as fixed dental bridges and removable dentures, the fundamental problems must be overcome before their clinical use in young patients who are still undergoing jawbone growth. Here, we show a novel bioengineering method for a functional biohybrid implant that is combined with adult-derived periodontal tissue and attached with bone tissue as a substitute for cementum. This biohybrid implant was successfully engrafted using the bioengineered periodontal ligament, and it restored physiological function, such as orthodontic movement through bone remodeling and appropriate responsiveness to noxious stimuli. Thus, this study represents the functional biohybrid implant's potential for clinical use as a next-generation dental implant using adult-derived tissues.
Introduction
T
To restore the occlusal function after tooth loss, conventional dental treatments that replace the tooth with artificial materials, such as fixed dental bridges or removable dentures, have been widely performed.5,6 Recently, osseointegrated dental implants that are able to stand alone in the jawbone without invading the adjacent teeth have been used to rehabilitate tooth loss.7,8 Dental implants are expected to have one of the highest growth rates among all dental device submarkets, because the demand for effective treatment and aesthetic dentistry worldwide is rising across all age groups. 8 However, because of the absence of natural periodontal tissue, the currently used dental implants that are directly connected to the surrounding alveolar bone do not provide the same function as the physiological tooth, such as the alleviation of excessive occlusal force, orthodontic movement through bone remodeling, and the ability to perceive noxious stimuli.4,7,8 Although dental implants are available treatment in the paradigm shift from the traditional dental therapies, such as dental bridges and dentures, fundamental problems must be overcome before implants can be clinically used in young patients who are still undergoing jawbone growth.4,8 It is therefore necessary to develop a functional dental implant that cooperates with the maxillofacial region and satisfies physiological functions through a biological connection with a bioengineered PDL.
Current advances in future regenerative therapies have been influenced by many previous studies, including those in the fields of embryonic development, stem cell biology, and tissue engineering technologies.9–11 Stem cell transplantation, which targets structural and functional diseases, has been attempted to repair damaged tissues.12–15 In the dental field, recent studies of stem/progenitor cells have provided new insights concerning tooth tissue-derived stem cells, including dental pulp stem cells, stem cells from human exfoliated deciduous teeth, and stem cells from apical papilla that have been isolated from the dental pulp tissue.16–18 These stem cells are thought to be a potential resource for stem cell-mediated tissue repair, including dentin or pulp regeneration, based on their high proliferation and multidifferentiation capacity. 19 Periodontal ligament-derived stem cells (PDLSCs), which can differentiate into all periodontal cell types after transplantation, have also been identified.19,20 Recently, researchers have attempted to develop cell sheet engineering using PDLSCs for clinical use in periodontal tissue regeneration.21,22 Although these treatments contribute to partial tissue repair, researchers anticipate the development of further therapeutic technologies using dental stem cells that can regenerate lost teeth.9,23
To restore tooth loss through the use of dental implants and stem cells, some studies reported periodontal tissue formed on implants using PDL stem cells.24,25 However, PDL structure, which was equivalent to natural tooth, and physiological functions were not demonstrated. Then, a novel fibrous connected implant that uses embryonic dental follicle stem cells has been successfully demonstrated as a proof-of-concept for a next-generation biohybrid dental implant. 26 As a critical issue for the realization of the biohybrid implant, suitable cell sources in adult tissue and applicable bioengineering technology should be found and used to construct the functional tissue similar to periodontal tissue around the implant. And, it includes proper cementum formation on the implant surface and the utilization of suitable adult tissue cell sources. 26
In this study, we focused on the substitution of alveolar bone for cementum because the structural and biological properties of cementum are almost similar to those of alveolar bone. We aimed to develop a novel bioengineering method consisting of adult-derived PDL tissue and a dental implant attached with bone tissue as a substitute for the cementum. We used rat PDL tissues for adult-derived tissue, and bone-attached implants that were osseointegrated in advance. Then, we transplanted them to immunodeficient mouse, and evaluated engraftment through a PDL-like connection. In addition, we examined recovery of physiological functions such as orthodontic movement through bone remodeling and appropriate responsiveness to noxious stimuli. This study thus represents the functional implant's potential as a next-generation dental implant therapy using adult-derived tissues in a clinical setting.
Materials and Methods
Animals
C57BL/6 mice (n = 50) and Wister rats (n = 60) were purchased from SLC, Inc. (Shizuoka, Japan). C.B-17-scid mice (n = 45) were purchased from CLEA Japan, Inc. (Tokyo, Japan). All animal care and handling conformed with the NIH guidelines for animal research, and all experimental protocols involving animals were approved by the Tokyo University of Science Animal Care and Use Committee (Approval No. N13010) and Tokyo Dental College Animal Care and Use Committee (Approval No. 273205). All surgeries were performed under the general anesthesia, and efforts were made to minimize suffering.
Tissue isolation of rat PDL tissue
The lower incisors were extracted from 5- to 6-week-old male rats. The PDL tissues were separated using a surgical knife and tweezers in Dulbecco's modified Eagle's medium (Kohjin Bio, Saitama, Japan) supplemented with 10% fetal calf serum (Gibco, Grand Island, NY), 100 U/mL penicillin (Sigma, St. Louis, MO), and 100 mg/mL streptomycin (Sigma).
Implant fabrication and surface analysis
The implants were 1.5 mm in length and 0.6 mm in diameter, with 99.5% titanium wire (Nilaco, Tokyo, Japan), and their apical sides were shaved into a conical shape. These implants were coated with hydroxyapatite (HA; 1–2 μm thickness) using the sputtering method (Yamahachi Dental Mfg., Co., Aichi, Japan). 27 The HA implants were coated with platinum and their surfaces were observed using an S-4700 (Hitachi High-Tech, Tokyo, Japan) scanning electron microscope operated at 5 kV.
Transplantation of implants
The lower first molars of 4-week-old C57BL/6 mice or 5-week-old C.B-17-scid mice were extracted under deep anesthesia, and the resulting bone wounds were allowed to heal for 3 weeks. An incision ∼2.0 mm in length was made through the oral mucosa at the extraction site with a surgical knife. A dental engine (NSK, Tochigi, Japan) and root canal files (MANI) were used to create a bony hole in the exposed alveolar bone surface. The HA implants were transplanted into the bony holes of the C57BL/6 mice, and the oral mucosa was sutured with 8-0 nylon (Bear Medic, Chiba, Japan). 26 Twenty-eight days after transplantation, the HA implants, which were attached to the surrounding alveolar bone tissue in 100–200 μm thicknesses, were extirpated using a dental engine (NSK). The bone-attached implants were wrapped with two or three pieces of PDL tissue and then transplanted into the bony holes of the C.B-17-scid mice. After transplantation, the oral mucosa was sutured with 8-0 nylon (Bear Medic) using the ePTFE membrane (Gore-Tex PSM; Japan Gore, Tokyo, Japan).
Microcomputed tomography
Radiographic imaging was performed using a microcomputed tomography (micro-CT) device (R_mCT; Rigaku, Tokyo, Japan) with exposure at 90 kV and 150 mA. Each implant and mouse was set on the object stage and imaging performed over a full 360° rotation with an exposure time of 2 min. The CT images were captured using i-view R (Morita, Kyoto, Japan).
Histochemical analysis and immunohistochemistry
For tissue preparation, the experimental animals were perfused transcardially with 10% formalin (Mildform 10N; Wako, Osaka, Japan), and tissues were removed and further postfixed for 3–10 h at 4°C. After fixation, the tissues were decalcified in 10% sodium citrate and 22.5% formic acid for 4 days at 4°C. Tissue sections (5–8 μm) were made after embedding in paraffin and stained with hematoxylin-eosin and azan staining. The stained sections were observed using Axioimager A1 (Carl Zeiss) with AxioCAM MRc5 (Carl Zeiss) microscopes. For fluorescent immunohistochemistry, the tissues were decalcified in 10% EDTA at 4°C, and 50 μm frozen sections were prepared and immunostained as previously described. 28 The sections were incubated with the neurofilament (NF) SMI312 (1:1000, mouse; Abcam, Cambridge, MA) as the primary antibody. The primary antibody was detected using highly cross-adsorbed Alexa Fluor® 594 goat antirabbit IgG (1:500; Life Technologies, Carlsbad, CA). Fluorescence images were observed using laser confocal microscope (LSM780; Carl Zeiss). The oblongatal sections were incubated with anti-c-Fos Ab (1:10,000; Santa Cruz Biotechnology, Dallas, TX). The sections were immunostained with peroxidase-labeled goat antirabbit IgG (1:300; Cappel Laboratories, Cochranville, PA) and peroxidase anti-peroxidase (PAP) immune complex (1:3000; Cappel Laboratories). The sections were observed using Axioimager (Carl Zeiss) with AxioCAM MRc5 (Carl Zeiss) microscopes.
Experimental orthodontic treatment
Orthodontic treatment was performed as described previously. 28 Experimental tooth movements consisted of a horizontal orthodontic force of ∼15–20 g applied continuously for 7 days in a buccal direction to the implants of the mice in the experimental group using a dial tension gauge (Mitutoyo, Kanagawa, Japan). In the control group, orthodontic force was applied in the buccal direction to the first molars of 9-week-old normal C57BL/6 mice in the same manner that was used for the experimental group. On day 7, serial sections were analyzed using in situ hybridization analysis for macrophage colony-stimulating factor-1 (Csf-1) and osteocalcin (OCN) mRNA. In situ hybridizations were performed using 10 μm frozen sections, and digoxigenin-labeled probes for specific transcripts were prepared using polymerase chain reaction with primers designed with published sequences (Csf-1; GenBank ID: NM_007778, OCN; GenBank ID: NM_007541). Primers were as follows: OCN (sense, 5′-AAGCCCAGCGACTCTGAGT CT-3′; antisense, 5′-CCGGAGTCTATTCACCACCTTACT-3′) and Csf-1 (sense, 5′-TACTGAACCTGCCTGCTGAA-3′; antisense, 5′-CCAGAGCTTGTGA-CAGGACA-3′).
Results
Fabrication of the bone-attached implant
Our experimental design is shown in Figure 1A. The bone-attached implant was enveloped with isolated adult-derived PDL tissues and transplanted into the first molar region in the mandible of an immunodeficient mouse. To produce a biohybrid implant with bioengineered periodontal tissue, it is necessary to use the alveolar bone formation on the implant surface as a substitute for cementum. We investigated whether a bone-attached implant could be generated by using the current osseointegrated implant as an alternative tissue for cementum. To adhere the alveolar bone to the implant, HA sputtering was used to create a ragged structure on the titanium implant surface, and the implants were transplanted into the lower first molar region of mice in a murine tooth-loss model (Fig. 1B). The HA-coated implant was osseointegrated in the lower jawbone at 30 days after transplantation (Fig. 1C), and micro-CT and histological analysis revealed proper bone formation and bone attachment around the implant (Fig. 1D, E). After the osseointegration of the HA-coated implant, we isolated a bone-attached implant with a thin layer of bone tissue (∼100–200 μm thickness) around the implant surface as a result of the surgical procedure (Fig. 1F).
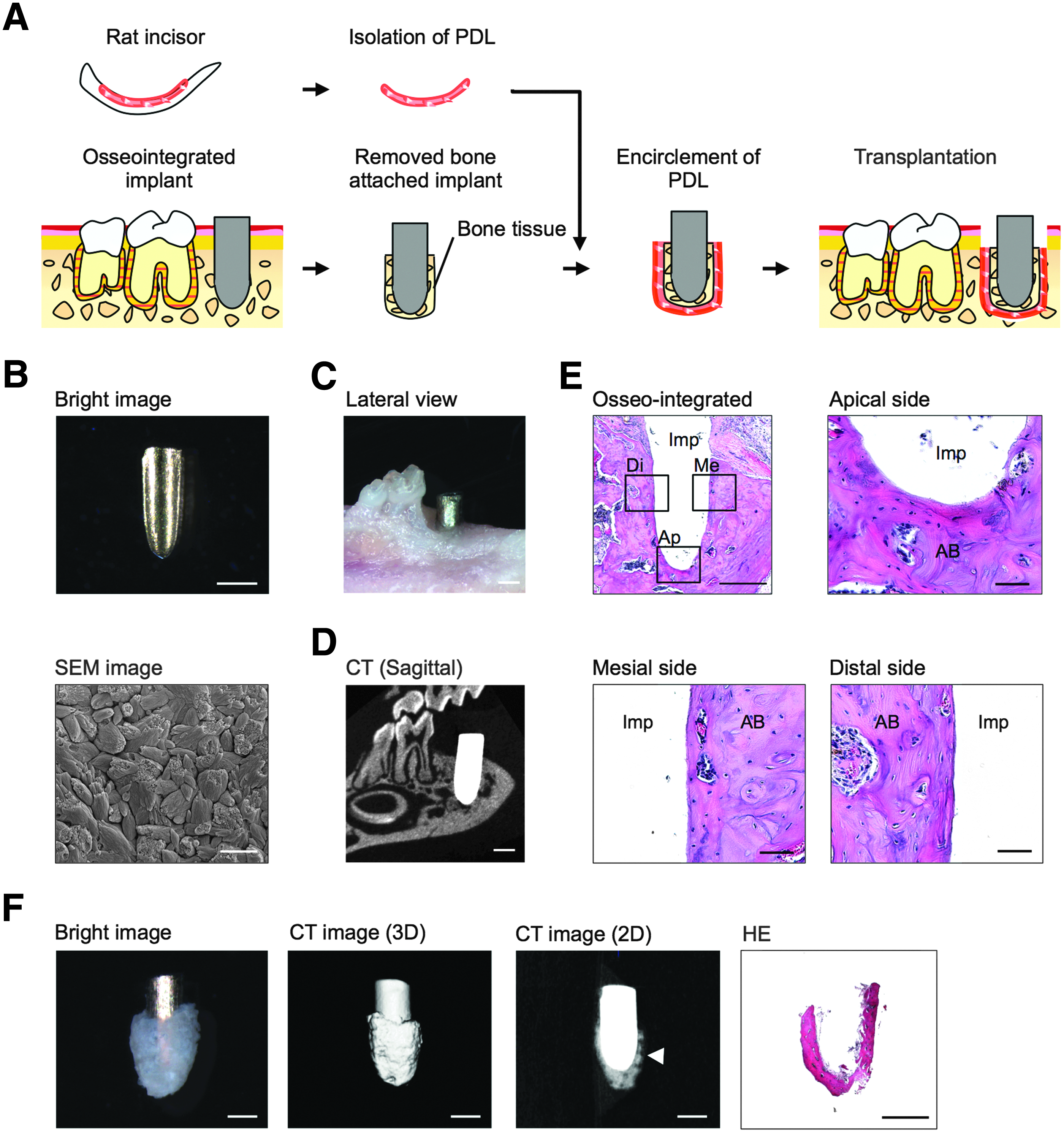
Fabrication of the bone-attached implant.
Transplantation of a biohybrid implant into a tooth-loss region
To remove an enough adult-derived PDL tissue, we focused on the rat incisor. PDL tissues were isolated from extracted incisors in a 5-week-old rat by surgical procedure. These tissues were observed as a typical fibrous tissue structure (Fig. 2A, B). We next evaluated whether a bone-attached implant combined with adult-derived PDL tissues could serve as functional implant-formed periodontal tissue after engraftment in a tooth-loss region in the adult murine oral environment. Micro-CT images revealed that the PDL space was observed around the bone-attached implant at 40 days after transplantation (Fig. 2C). Samples that have PDL space on more than 50% area of bone-attached implant from CT images could be seen in frequencies of 23/42. In other samples, implants fell out of mandibular or got the osseointegration. Fallen out samples could have been primarily caused by inflammation of graft rejection. Histological analyses demonstrated that the correct periodontal tissue structure was observed on the bone-attached implant at 40 days after transplantation (Fig. 2D). The PDL fiber structure of the engrafted bone-attached implant, which consisted of transverse collagen fibers, was equivalent to that of a natural molar tooth.

Transplantation and engraftment of the functional implant.
The biohybrid implant's response to mechanical stress
It has been considered that a functional implant could be achieved by fulfilling physiological tooth functions in the oral environment, such as cooperation with the oral and maxillofacial regions through the PDL. Thus, we investigated whether an engrafted biohybrid implant combined with a bone-attached implant and adult-derived PDL tissues could respond to mechanical stress as a physiological periodontal function. When we evaluated orthodontic movement using mechanical force in an experimental tooth movement model, the engrafted biohybrid implant moved in a manner similar to that of natural teeth in response to orthodontic force. During an experimental tooth movement model, Csf-1 mRNA-positive and OCN mRNA-positive osteoblasts were observed individually on the compression and tension sides as a result of gene expression patterns (Fig. 3).
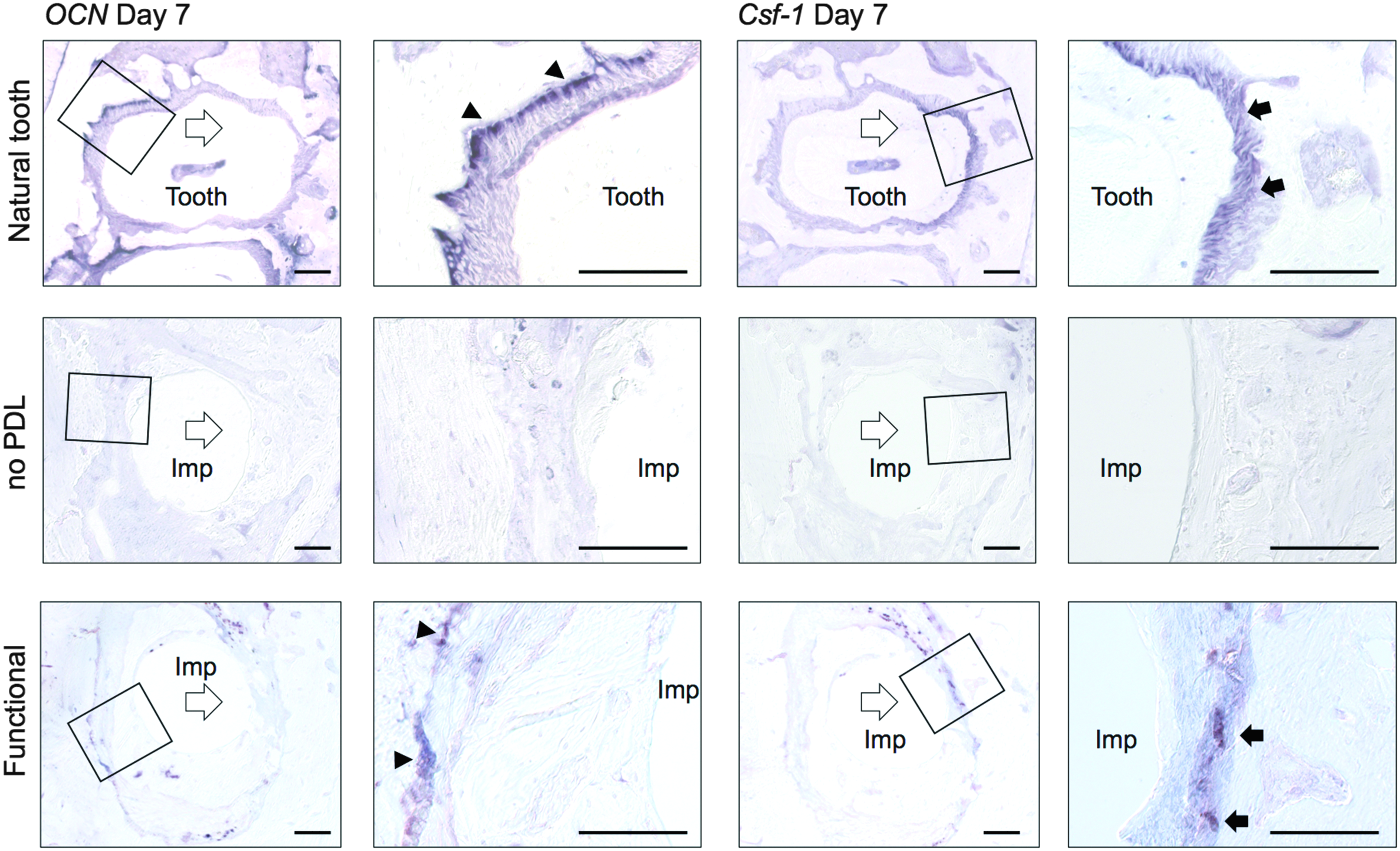
A functional implant's response to mechanical stress. Sections of natural tooth, bone-attached implant without PDL tissue, and functional implant were analyzed using in situ hybridization analysis for OCN and Csf-1 mRNA at day 7 of orthodontic treatment. OCN mRNA-positive cells (arrowhead) and Csf-1 mRNA-positive cells (arrow) are indicated. Scale bar, 100 μm. Csf-1, colony-stimulating factor-1; OCN, osteocalcin.
The biohybrid implant's potential for perceiving noxious stimuli
Teeth are a peripheral target organ in the maxillofacial region for the perception of the trigeminal and sympathetic nerves, which play essential roles in homeostasis and protection. The potential for perceiving noxious stimuli, including occlusal force and pain, is important for proper tooth function. Trigeminal neurons, which innervate the pulp and PDL, can respond to these stimuli and transduce the perceptions to the central nervous system. We therefore used immunohistochemical analysis to investigate whether an engrafted biohybrid implant had neural functions. Anti-NF immunoreactive nerve fibers were detected in the PDL of the biohybrid implant (Fig. 4A). c-Fos immunoreactivity is induced in the superficial layers of the medullary dorsal horn by noxious stimuli; for example, electrical, mechanical, and chemical stimulation of intraoral receptive fields involving the tooth pulp and the peripheral nerves of the PDL. In the engrafted biohybrid implant, c-Fos immunoreactive neuron expression was detectable as much as natural tooth in the superficial layers of the medullary dorsal horn after noxious stimulation 2 h after orthodontic treatment (Fig. 4B).

Neural function analysis of an engrafted functional implant.
Discussion
We have demonstrated the successful engraftment of a functional dental implant through the biological fibrous connectivity system using a bone-attached implant and adult-derived PDL tissues. We have also shown the subsequent restoration of physiological tooth functions, such as the response to mechanical stress and the potential for perceiving noxious stimuli. This study indicates the potential for dental regenerative therapy using a novel bioengineering method and the application of current dental implant treatments.
Cementum is a characteristic hard tissue covering the surface of the tooth root. It contributes to essential tooth functions, including protecting the dentin and ensuring a tight connection between the tooth and alveolar bone through the insertion of PDL fibers.2,29 Periodontal tissues, which are composed of cementum, the PDL, and alveolar bone, arise from dental follicle tissue that is derived from the dental mesenchyme in the developing embryo. 29 After tooth development, immature cementoblast cells are thought to be maintained by a self-repair system in cases of tooth and periodontal tissue injuries.29,30 Based on the understanding of cementum development, many previous studies have attempted to reconstruct bioengineered periodontal tissue through cementum formation onto tooth root or dental implant surfaces using scaffolds and dental stem cells.24,25,31,32 However, no bioengineering method has yet been able to create functional cementum. 29 It is well known that the structural and biological properties of cementum, such as the component ratio of organic (e.g., collagens) to inorganic (e.g., HA) matters and the gene expression patterns in calcified tissue formation, are similar to those of alveolar bone.29,33 It is also thought that alveolar bone might be substituted for cementum because cementum has a potential for a physiological reaction to mechanical stress and because alveolar bone exhibits remodeling in the case of orthodontic treatment.34,35 In this study, we developed the functional implant with adult-derived PDL tissue and the therapeutic dental implant attached to bone tissue as a substitute for cementum. The engrafted functional implant showed the proper insertion of PDL fibers as a result of bone remodeling. These findings suggest that the bioengineering method used for our functional implant has potential as an available dental implant treatment in the future.
The PDL, which can cooperate with the maxillofacial region through the fibrous connection with the cementum and the alveolar bone, plays important roles in biological tooth functions, including the absorption of occlusal force and tooth movement through bone remodeling.2,4 Many studies have attempted to restore the periodontal tissue structure on an implant surface, for example, using material-based approaches that were incorporated into the subsidence mechanism against occlusal force 36 and biochemical approaches coated by inducible factors.37,38 Some studies demonstrated that periodontal tissue formed on dental implants using PDL stem cells by tissue-engineering approaches.24,25 However, these technologies could not completely replace the correct structure and restore the proper functions of periodontal tissue. 4 In our recent study, we developed a biohybrid implant that restored physiological functions through the proper PDL connection. However, critical issues with suitable adult cell sources and bioengineering technology must be resolved for the biohybrid dental implant. 26 In this study, we demonstrated the successful engraftment of a functional bone-attached implant with adult-derived PDL tissues that could replicate both the correct periodontal structure on the implant surface and the PDL's function of responsiveness to mechanical stress through bone remodeling. These findings indicate the fulfillment of a therapeutic concept through a next-generation biohybrid implant that can achieve functional cooperation by reconstructing fibrous connective tissue, such as the PDL.
Teeth are a peripheral target organ for the sensory trigeminal and sympathetic nerves,39,40 and the proper function of the nervous system in the maxillofacial region plays essential roles in the regulation of tooth physiological functions and the perception of external stimuli, such as pain and mechanical stress.1,39 These physiological functions regarding oral and general health are achieved by the functional cooperation of the teeth, masticatory muscles, and temporomandibular joint under the control of the central nervous system. 39 It is thus thought that the recovery of the nervous system, which is associated with the re-entry of nerve fibers after the transplantation of a tooth germ or autologous tooth, is critical to fully physiological dental therapy for tooth loss.28,41 Current dental implants that are directly connected to the alveolar bone are not able to sense noxious stimuli because of the absence of nerve innervation in periodontal tissue7,40; therefore, it is anticipated that a next-generation biohybrid implant will realize the functional recovery of the neuronal perceptive potential for noxious stimuli.4,26,40 In this study, we demonstrated that the functional implant was successfully innervated with the peripheral nerves through bioengineered periodontal tissues, and the responsiveness to orthodontic stimulation was restored. These findings indicate that biohybrid implants offer the potential for the recovery of neuronal function through proper innervation.
This bioengineering technique might be early applicable to clinical site because there is no time for cell culture. However, to establish novel treatment with biohybrid implants, identification of tissue/cell source should be needed. Previous studies used stem cells derived from third molar tooth or tooth germ tissue, including the dental pulp, PDL, and dental follicle, to repair damaged tissues. 19 The PDL tissues derived from the third molar tooth might be a potential source for treatment with biohybrid implant. Further studies that optimize bioengineering methods in combination with current dental implant procedures and available stem cells and apply practical analyses in a large animal model will be required before biological dental regenerative therapy can be used clinically.
In conclusion, this study shows that the transplantation of a bone-attached implant with adult-derived PDL tissues can achieve the formation of proper periodontal tissue-like structures similar to those of the natural tooth, and the engrafted implant has physiological PDL functions that can cooperate with surrounding tissues. This study represents a substantial advance in the development of biohybrid implants as a next-generation dental implant therapy using adult-derived tissue.
Footnotes
Acknowledgments
We are grateful to Y. Shin and T. Takasu (Yamahachi Dental Mfg., Co., Aichi, Japan) for coating technique of dental implant. We thank A. Iwadate, K. Yamashita, and K. Yamaguchi for technical assistance. This work was supported by Organ Technologies, Inc.
Disclosure Statement
This work was funded by Organ Technologies, Inc. T.T. is a director at Organ Technologies, Inc. This work was performed under the condition of Invention Agreement between Tokyo University of Science and Organ Technologies, Inc.