
Abstract
Tissue engineering based on cell seeding, bioscaffolds, and growth factors has been widely applied for the reconstruction of tissue defects. Recent progress has fueled in vivo tissue engineering techniques in becoming hot topics in regenerative medicine and reconstructive surgery. To improve the efficacy of tissue engineering, we here investigated the roles of cell seeding, bioscaffolds, growth factors, and in vivo microenvironment (IM) in tissue regeneration. Bone marrow-derived stem cells, allogeneic demineralized bone matrix as bioscaffold, and growth factor bone morphogenetic protein 2/transforming growth factor, and the IM of rib periosteum and perichondrium were used in different combinations for the generation of osteochondral composite tissue. Self-regenerated neocomposite tissue based on the IM alone exhibited excellent anatomical configuration, vascularization, biomechanical stability, and function similar to native controls. Our findings indicate that the IM is a crucial factor in biofunctional tissue generation. Further refinement and development of this technique may enable transfer to clinical application with broad spectrum of application.
Introduction
S
Over the decades, tissue engineering has considerably evolved, now covering a spectrum from in vitro tissue engineering to in vivo-generated tissue constructs. Recently, further development has rendered either cell seeding or bioscaffolds dispensable, by regenerating tissues in the in vivo microenvironment (IM) using implanted bioscaffolds/seeded cells.1,2 Successful fabrication of customized bioscaffolds to regenerate bone and articular cartilage in vivo without the need of in vitro cell expansion reveals the role of the IM in cell homing and tissue regeneration during wound healing.1,3 Others showed the repair of tissue defects based on cell seeding in vivo without the use of bioscaffolds to achieve tissue regeneration and wound healing by mobilizing the self-microenvironment.4–6
These developments stimulated us to hypothesize whether complete self-regeneration may be achieved through the IM. By creating an artificial closed space involving the microenvironment of costal perichondrium and periosteum for the in vivo generation of osteochondral composite tissue, we aimed to determine the role and specific effects of cell seeding, bioscaffolds, and growth factors in in vivo tissue regeneration, whether essential or dispensable.
Materials and Methods
Study design, isolation, and culture of bone marrow-derived stem cells
A total of 24 healthy skeletally mature swine, 12 male and 12 female, age range 4–5 months with an average weight of 20.0 ± 2.5 kg were included in the study. To eliminate individual differences, the sides were randomly assigned. This study was approved by the Animal Care and Experimental Ethics Committee of Shanghai Jiao Tong University Medicine School ([2009], 179).
The bone marrow-derived stem cells (BMSCs) were harvested from swine. After induction of anesthesia, bone marrow aspirates were collected from the iliac bone. Cells were cultured and passaged to the second generation as previously described 7 and were further sorted by flow cytometry using anti-CD34, CD45, CD29, CD105, CD44, and CD90.
Decellularized and demineralized bone matrix scaffold preparation
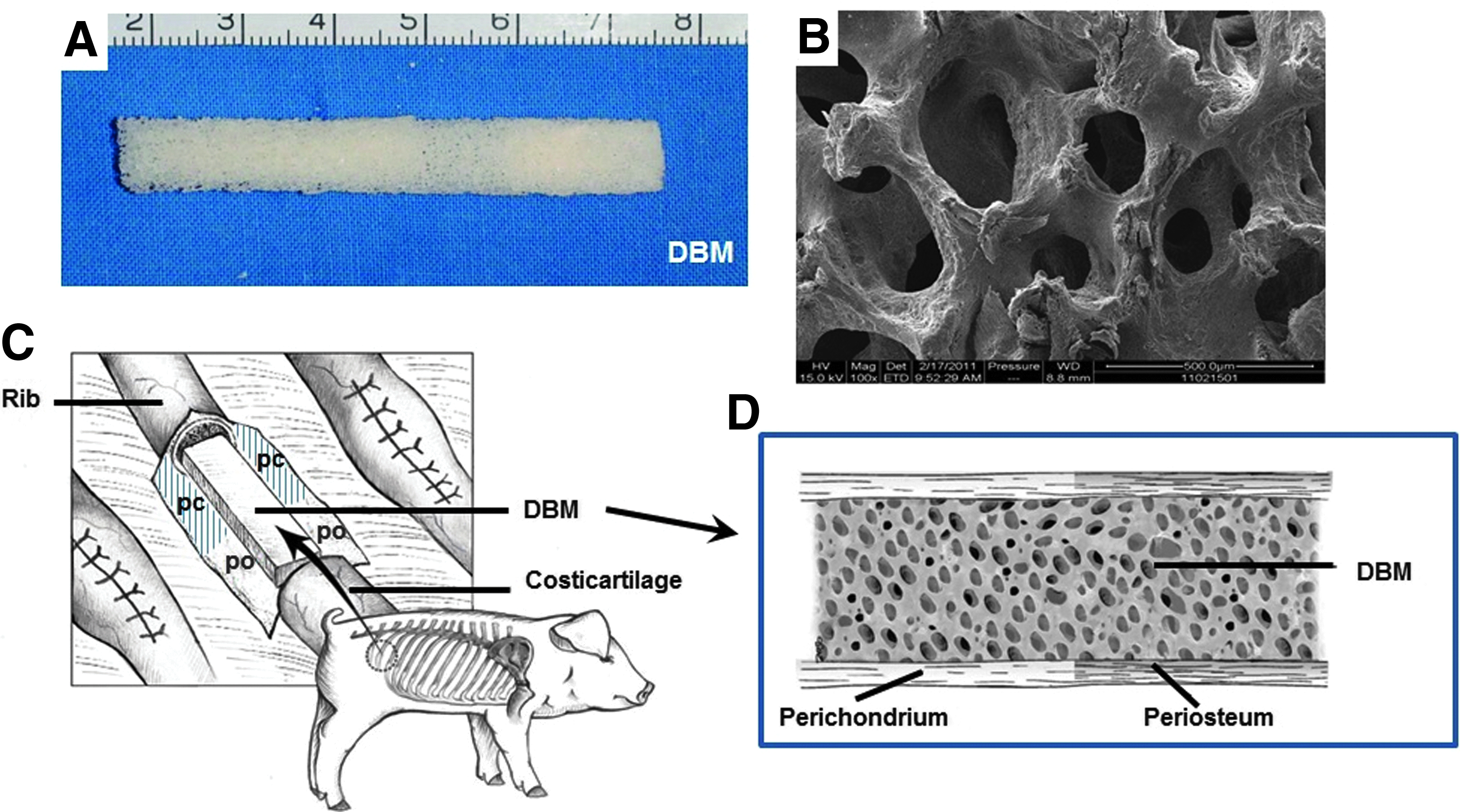
Decellularized and demineralized bone matrix (DBM) (JiangSu Unitrump Biomedical Company, China) was prepared as previously reported.8–10 Briefly, allogeneic bones were harvested, residual soft tissues removed, and the cortical bone trimmed to form a cuboid with a size of 6 × 1.0 × 1.0 cm3 (Fig. 1A). After repeated washing, the trimmed bone specimens were extracted with a mixture of chloroform and methanol (1:1 ratio) for 24 h followed by demineralization with Triton X-100 Tris–HCl for 72 h at 4°C. Following sequential washing with deionized water, the specimens were immersed in ethylenediaminetetraacetic acid (EDTA) solution (0.5 M, pH 8.3) at 4°C for 2 weeks, while the solution was replaced on a daily basis. After decellularization, demineralization, and defatting, scanning electron microscopy (PhilipsXL-30, Amsterdam) was performed to determine DBM microstructure and porosity (Fig. 1B). Finally, the prepared bioscaffold was routinely sterilized before use.
Preparation of the DBM scaffold for the guided generation procedure in a swine model.
Seeding of BMSCs and biocompatibility tests
For every DBM scaffold, 2 mL of enriched BMSCs (5 × 106/mL) and, after 2 h of incubation, were implanted in swine. For in vitro studies, DBM seeded with BMSCs were cultured and examined at 2 h and 2 weeks after seeding regarding adhesion and proliferation of BMSCs on the bioscaffold.
Creation of the IM
After exposure of the chondro-osseous transition of third or fourth rib counting from caudally, periosteum and perichondrium were incised along the curve of the rib (Fig. 1C). A segment of rib and costal cartilage was removed to obtain periosteum of 3.5 cm and perichondrium of 3.5 cm in length. Two pieces of silicone membranes were used for coverage of the rib/costal cartilage fragment ends to prevent ingrowth of the surrounding tissue and create a closed space comprising the IM (Fig. 1D).
Each animal was randomly assigned to five study groups as summarized in Table 1. The IM was present in groups I–IV, whereas group V without IM served as control. In group I BMSCs−DBM−bone morphogenetic protein-2 (BMP-2)/transforming growth factor β1 (TGF-β1)−IM were applied, in group II DBM−BMP-2/TGF-β1−IM, in group III BMSCs−BMP-2/TGF-β1−IM, and in group IV only the IM alone. In group V BMSCs−DBM−BMP-2/TGF-β1 were embedded in the intercostal muscle tissue without IM. Growth factors, BMP/TGF, were used with the following concentrations: BMP-2: 200 ng/mL (R&D Systems) and TGF-β1: 10 ng/mL (R&D Systems).
BMP, bone morphogenetic protein; BMSCs, bone marrow-derived stem cells; DBM, demineralized bone matrix; TGF, transforming growth factor.
All animals recovered from surgery and were kept according to animal care standards. Samples were harvested at 1.5, 3, 6, and 12 months after operation implantation, before animals were humanely euthanized.
Fluorescent labeling of osteogenesis
All animals received i.m. injection of 25 mg/kg hydrochloride tetracycline (TE), 20 mg/kg calcein (CA), and 25 mg/kg Alizarin Red (AL) 21, 14, and 7 days before sample collection at 1.5, 3, 6, and 12 months (all reagents from Sigma). Excitation/emission wavelengths (Ex/Em) were as follows: 405/580 nm (TE, yellow), 488/517 nm (CA, green), and 543/617 nm (AL, red).
Samples were fixed and embedded in methylmethacrylate as previously described. 11 Sections of 100 μm were examined using a confocal laser scanning microscope (Leica TCS Sp2 AOBS, Germany) to identify mineralization deposition and direction of new bone as an indicator of osteogenesis.
Imaging analyses
Thoracic 3D CT (GE LightSpeed Ultra 16, Milwaukee, WI) was performed at 1.5, 3, 6, and 12 months postoperatively to analyze de novo tissue formation. Bone formation was examined based on micro-CT of the generated tissues after harvest according to a previously reported protocol. 4 Microtomographic slices were acquired for structural assessment and calculation of morphometric data of osteogenesis, including mineral density, volume, trabecular number, and thickness.
Anatomical morphology
The entire generated osteochondral composite neotissue, along with its periosteum, perichondrium, neurovascular bundle, and surrounding muscle, was harvested. The transition zone of newly formed bone and cartilage was chosen as midpoint. For analysis excess tissue was removed on both sides at 2.5 cm from the midpoint. Specimens were photographed and transverse sections of the tissues prepared to calculate the area of new bone and cartilage, and evaluate the differences between the groups. The mean area of the newly formed tissues was used to calculate the volume for each group by Image-Pro Plus Version 6.0 (Media Cybernetic).
Histological analysis of osteogenesis, chondrogenesis, and angiogenesis
Samples of generated bone, cartilage, and their transition zone were collected and processed. Sections of 5 μm were made and 20 slices randomly chosen from each sample for staining with Hematoxylin and Eosin (HE), Toluidine Blue and Fast Green, Van Gieson (VG), and Alcian Blue to examine osteogenesis, chondrogenesis, and vascularization. Under a light microscope (Olympus, Japan), 10 fields were randomly chosen from each slice for software-based analysis (Origin 8.0) of trabecular bone areas and blood vessel density. Immunohistochemical assessment of osteogenesis, chondrogenesis, and vascularization was performed using anti-osteocalcin (OC, 1:100), anti-collagen II (Col II, 1:100), and anti-Von Willebrand Factor (vWF, 1:400) antibodies (all from Abcam) as previously described. All of the antibodies were incubated overnight at 4°C with the DBA coloration (all from Abcam).
Biomechanical analyses
Bending tests were performed to evaluate biomechanical properties at every time point. Bending load strength and Young's modulus testing of generated bone and cartilage specimens were conducted using a biomechanical analyzer (Instron-8874, Canton, MA) according to a previously described protocol. 12
Statistical analysis
All results are presented as mean ± standard error. Statistical analysis was performed using one-way analysis of variance for comparison between groups using SPSS software (SPSS, Inc.). Significant differences were indicated as *p < 0.05 and #p < 0.01.
Results
BMSCs preparation, adhesion, and proliferation on DBM scaffold
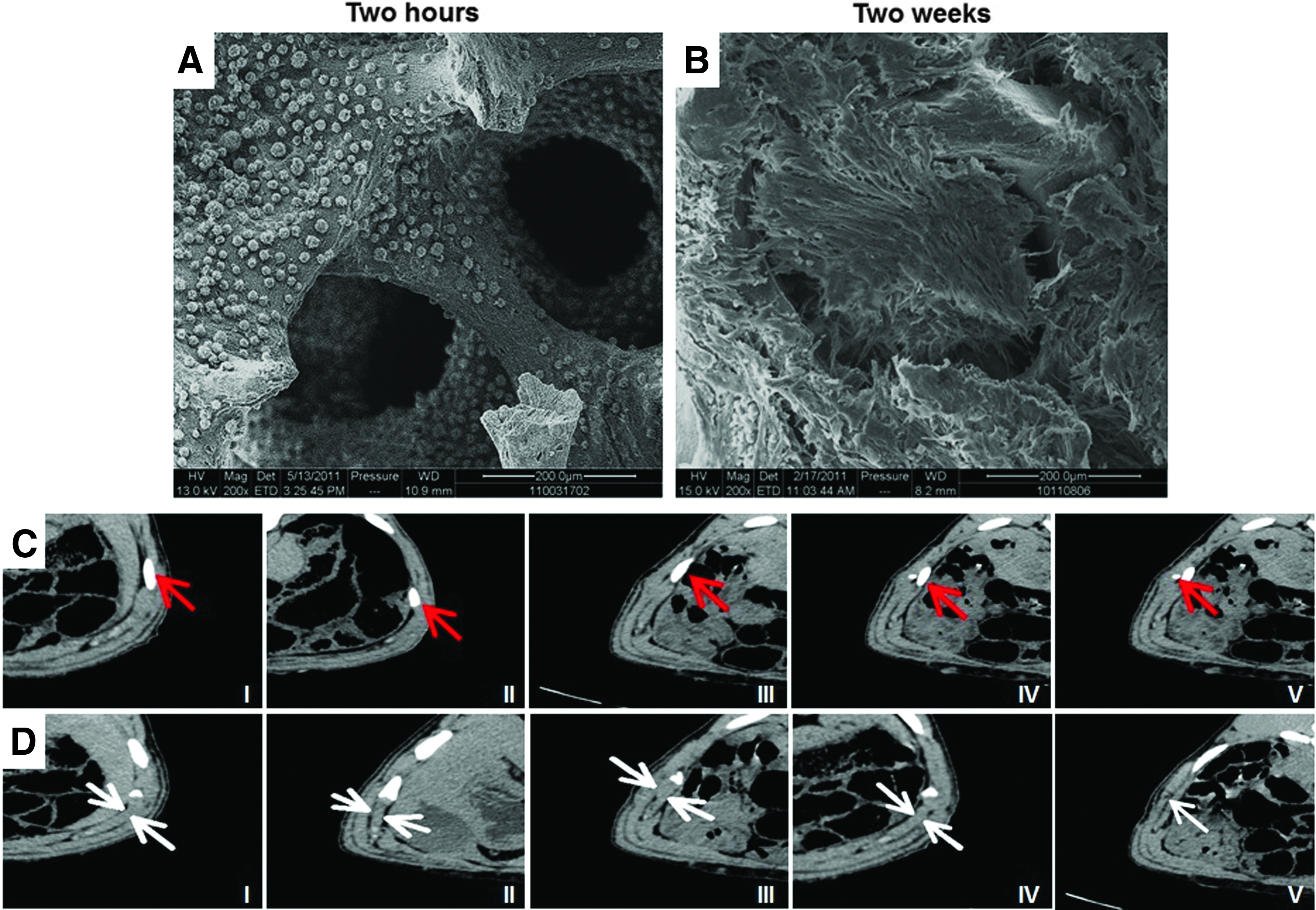
BMSCs were characterized as previously described (data not shown). After seeding on the prepared DBM scaffold, cells were shown to adhere on the scaffold 2 h after inoculation (Fig. 2A). After 2 weeks culture in vitro, seeded cells were shown to have secreted extracellular matrix (Fig. 2B).
Cell proliferation on demineralized bone matrix scaffold and osteochondral composite neotissue generation.
Radiographic analysis
In all groups, neobone and neocartilage formation were observed as visualized by 3D CT (Fig. 2C, D). Isolation of the newly formed bone from native rib using silicone successfully prevented the ingrowth of surrounding normal bone into the regenerated tissues. It is important to note that without the adequate IM (group V) neobone tissue formation was observed 3 months after implantation, but no longer detectable 6 months later due to resorption.
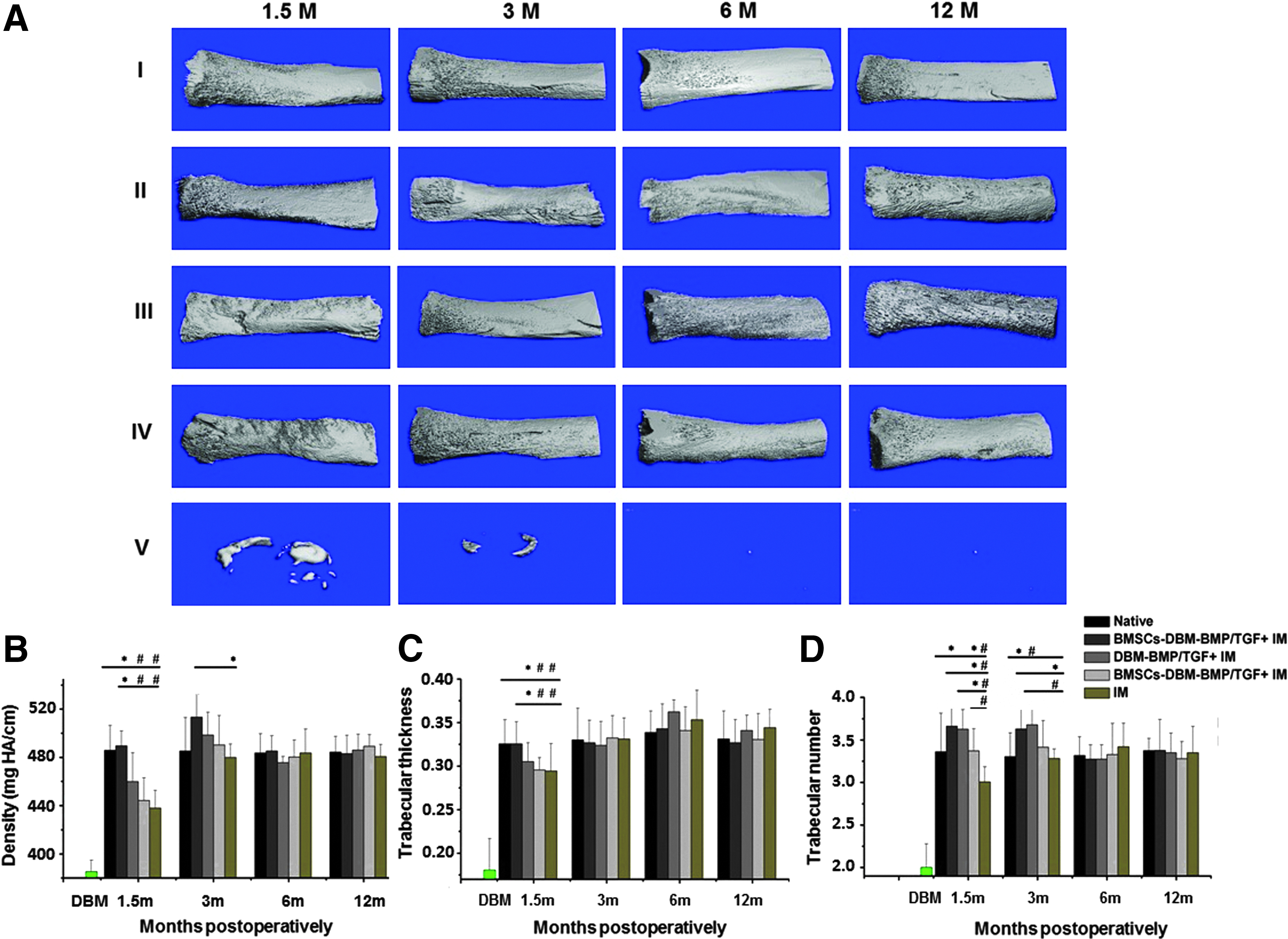
Micro-CT analysis showed that newly formed bone surfaces in groups I–IV were rough with a slight irregular shape at 1.5 months (Fig. 3A). Moreover, cancellous and cortical bone boundaries were less distinct in groups I–III compared with group IV. However, rough surfaces smoothened over time and no significant differences were seen after 3 months. Mineral density (Fig. 3B), trabecular thickness (Fig. 3C), and neotissue number (Fig. 3D) in all groups increased during follow-up. Thickness of newly formed bone tissues in group I was similar to native rib at 1.5 months postoperatively (p > 0.05), whereas trabecular number and thickness were reduced in group IV (p < 0.01). No significant statistical difference was found between groups II–IV and native rib (p > 0.05). For groups I–IV, the morphological index for the newly formed bone showed no statistically significant difference compared with native rib 6 and 12 months postoperatively. In group V, the trabecular number was only 1.49/mm at 1.5 months and further declined to 1.01/mm at 3 months, trabecular thickness was 0.112 and 0.089 mm after 1.5 and 3 months, respectively. Mineral density was reduced from 217.32 mg HA/ccm at 1.5 months to 187.72 mg HA/ccm at 3 months. However, after 6 and 12 months, these parameters seemingly further declined and were no longer detectable.
Micro-CT examination of newly generated osteochondral composite tissue.
Anatomical analysis of osteogenesis and chondrogenesis
For groups I–IV, all harvested specimens showed neobone and neocartilage formation at 1.5 months. Longitudinal sections of the neobone demonstrated the existence of cortical and cancellous bone structures and a chondro-osseous transition zone (Fig. 4A, B). At the first 3 months, the cortical and cancellous bone structure in group I was clearer than in groups II–IV. The neocartilage in group III showed partly ossification at 1.5 months. No residual scaffold material was found after 1.5 months in groups I and II. Macroscopically, there was no significant difference between groups I–IV and in comparison to native controls after 6 months (Fig. 4C, D).

Macroscopic analysis of generated neotissue. An osteochondral transition zone was found in generated neotissue in groups I–IV after dissecting the periosteum and perichondrium as demonstrated here
In group V, by contrast, transverse sections demonstrated a spot of osteoid tissues; the fibrous tissues grew into the partially degraded scaffold at 1.5 months postoperatively. At 3 months, the DBM scaffold further degraded, no bone or cartilage tissues were observed. Later at 6 months, there were still bits of residual scaffolds, which completely degraded by 12 months (Fig. 4C).
Fluorescent labeling analyses
Groups I–IV showed similar labeling characteristics, and here we take group IV as an example. At 1.5 months, large areas of fluorescent labeling indicate high activity of osteogenesis (Fig. 5A–D). Later at 3 months, fluorescent labeling showed overlapping osteogenesis areas (Fig. 5E–H). This further confirmed the shaping and reconstruction activity in the newly formed bone. At 6 (Fig. 5I–L) and 12 (Fig. 5M–P) months postoperatively, the fluorescent labeling showed no significant difference to normal bone (Fig. 5Q–T). In contrast, no fluorescent labeling was detected in group V indicating the absence of osteogenesis in group V.
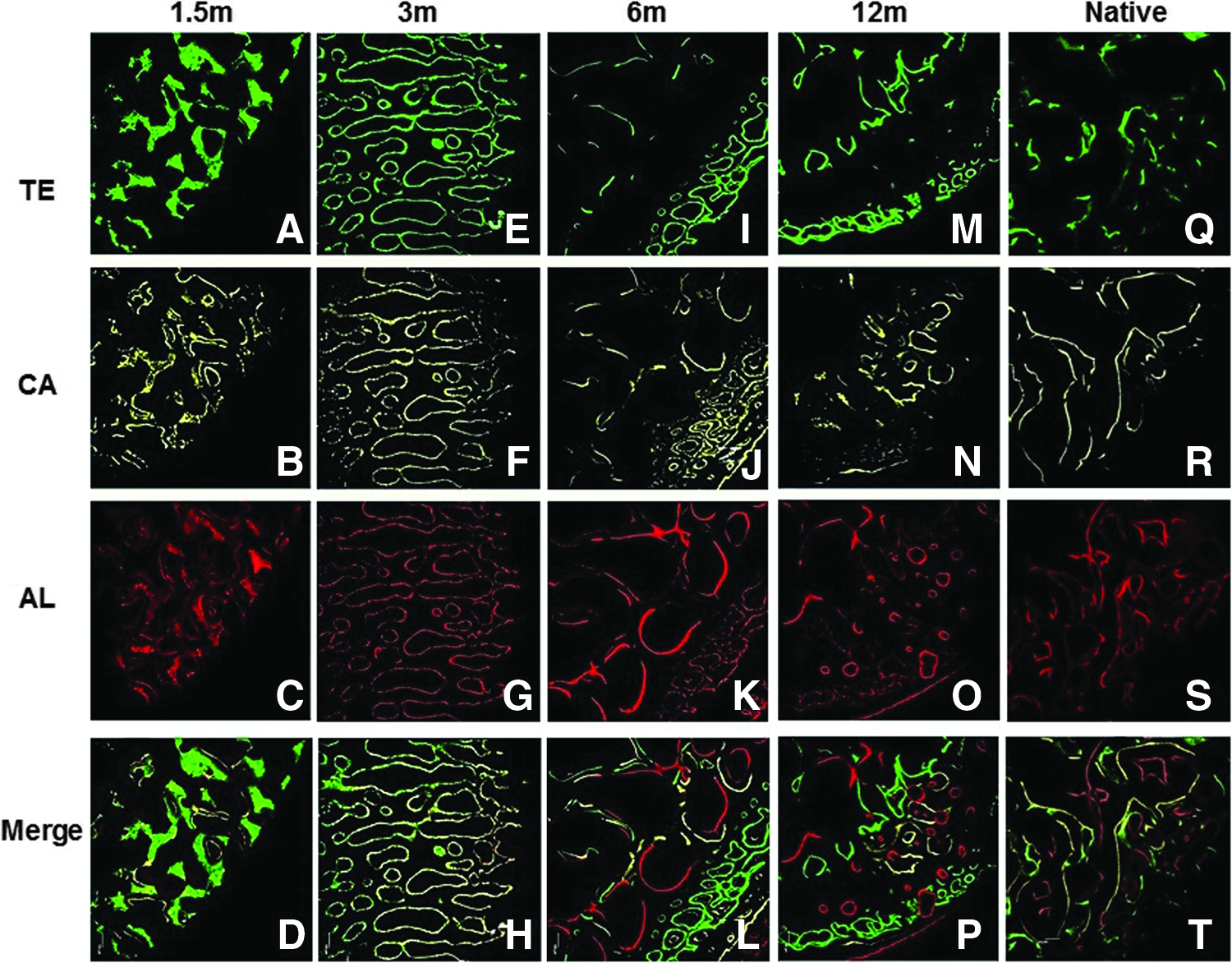
Fluorescent labeling of osteogenesis shown exemplarily in group IV.
Histological findings
Osteogenesis
Histological VG (Fig. 6) and immunohistochemical OC (Fig. 7R) staining at 1.5 months after implantation showed typical bone tissue structure, including osteoblasts, trabecula, bone marrow cavity, and cortical and cancellous bone. As to histomorphometrical results, trabecular areas were initially reduced in groups III and IV compared with native rib, but were significantly increased at 3 months postoperatively. In detail, trabecular areas of groups I and II were larger than groups III and IV (p < 0.05), but there is no statistically significant difference between the native bone and groups I and II (p > 0.05). After 3 months the trabecular areas of groups II–IV were found to be increased compared with native controls, but only group IV showed a statistically significant difference (p < 0.05). In group I, trabecular areas were similar to native ribs, but significantly reduced compared with groups II and IV (p < 0.05). Then, no statistically significant difference was found between the groups and native bone after 6 months. There was no typical trabecular structure in group V, so it was not analyzed at the same time (Fig. 6Q, R).
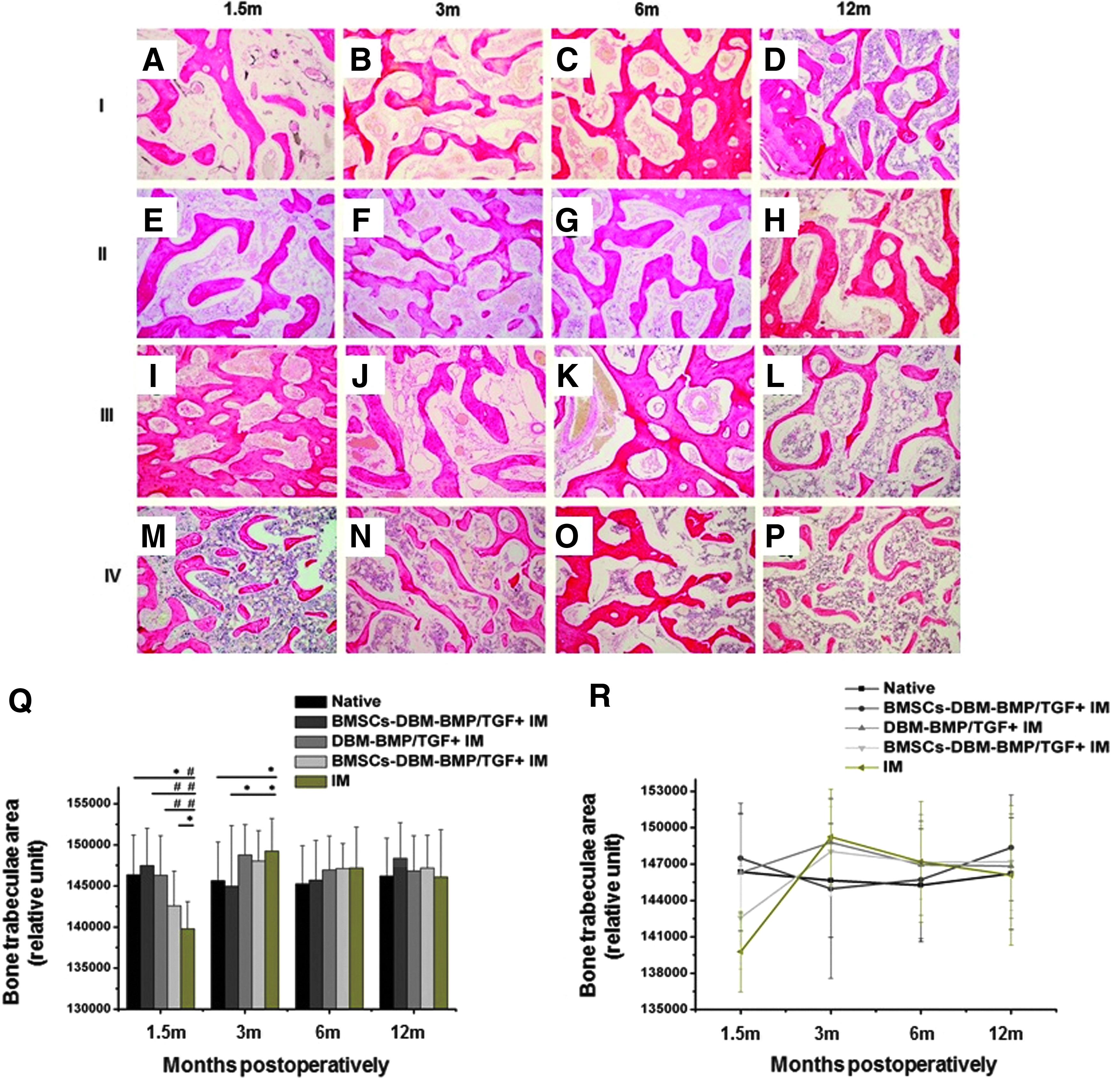
Histological analysis of the neobone using VG staining.
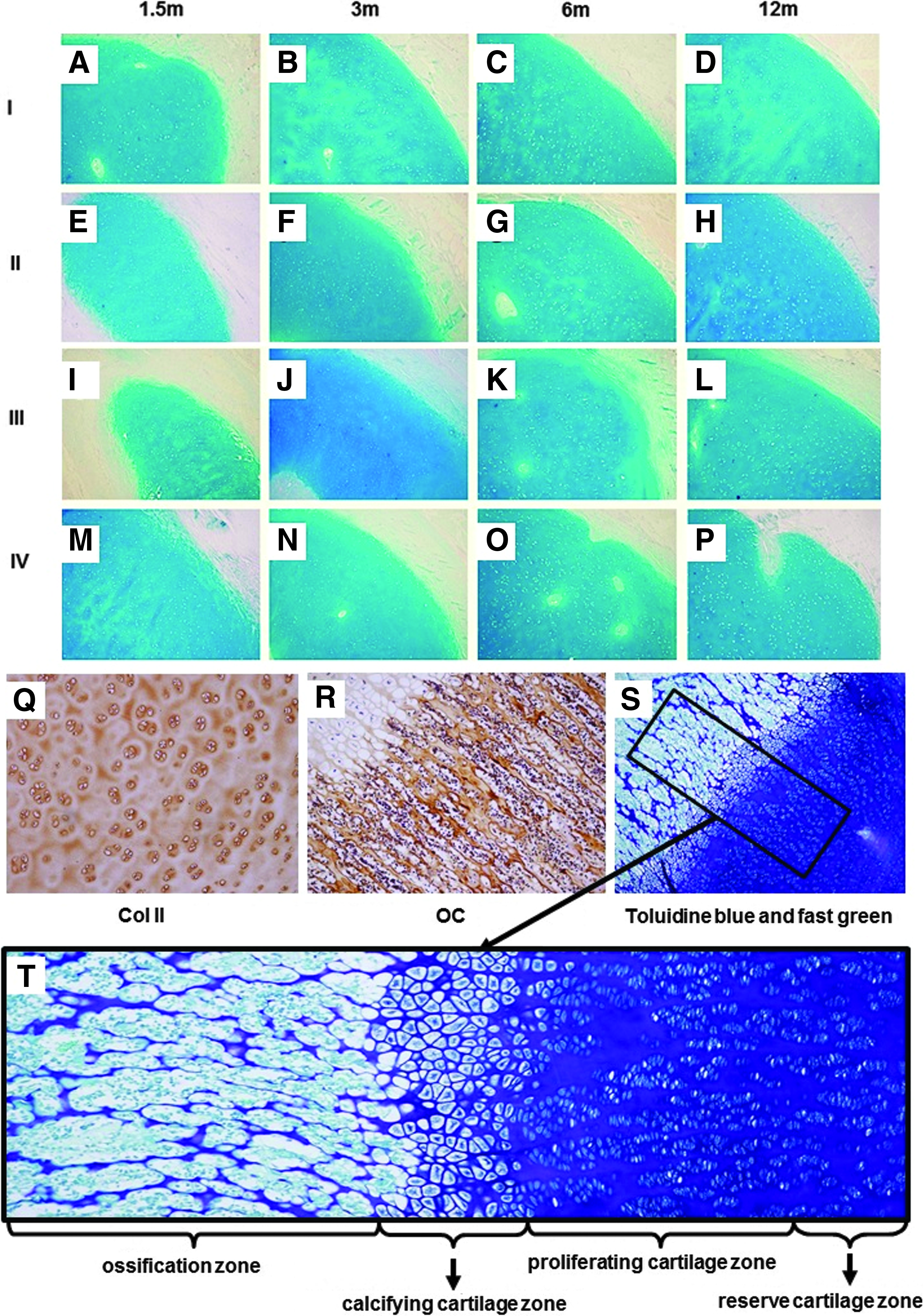
Histological analysis of neocartilage.
Chondrogenesis
The hyaline cartilage tissue staining using Alcian Blue (Fig. 7A–P) and immunohistochemical staining against Col II (Fig. 7Q) clearly showed typical hyaline chondrocytes, cartilage lacuna, and matrix in groups I–IV. Although chondrocytes were histologically larger than the normal cells at 1.5 months after harvest, no significant difference was found 3 months postoperatively. For group V, by contrast, no new cartilage formation was observed at any time.
Bone and cartilage transition zone
The typical four zones of the newly formed bone and cartilage transition were clearly shown by OC (Fig. 7R) as well as Toluidine Blue and Fast Green staining (Fig. 7S): zone of reserve cartilage, zone of proliferating cartilage, zone of calcifying cartilage, and zone of ossification (Fig. 7T).
Angiogenesis in the newly formed bone
Increased angiogenesis was found in groups I–IV as seen in VG, Azan–Mallory staining, and immunohistochemical staining against vWF (Figs. 6 and 8). From 1.5 to 3 months, groups I–IV showed a continuous increase in newly formed blood vessels. Groups I and III exhibited increased vascularization compared with groups II and IV, whereas the bone marrow cavity of the latter two showed excessive accumulation of red blood cells (Figs. 6 and 8). At 3 months, the vascularization of groups I and III further increased with no statistically significant difference compared with native rib (p > 0.05). After 6 months, there was no statistically significant difference between groups I–IV and native bone in terms of vascularization (p > 0.05). Perfusion patterns of blood vessels with Indian ink were consistent with the histological staining (Fig. 8).
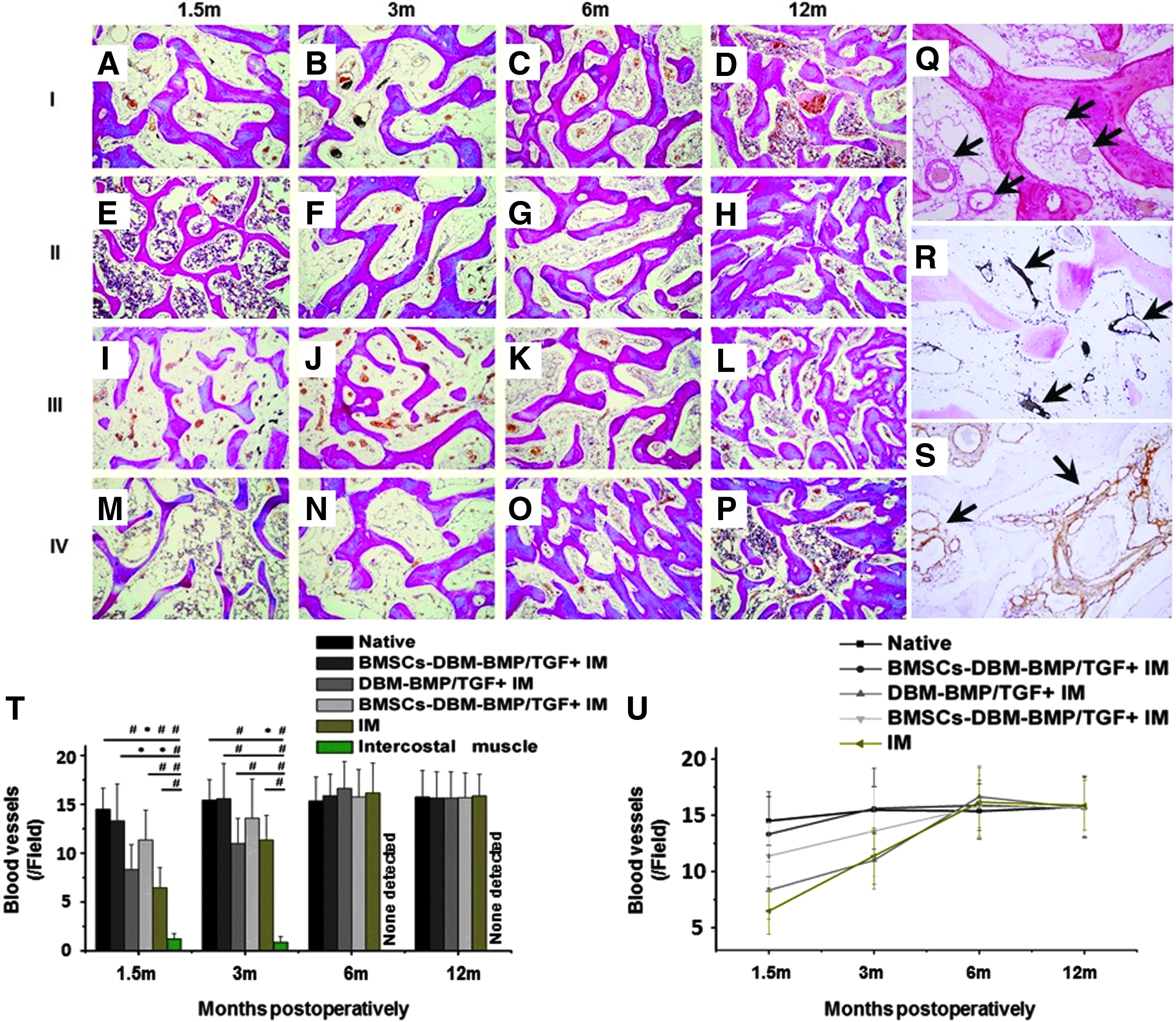
Histological analysis of the newly formed blood vessels.
Biomechanical and bone mineral density analyses
At 1.5 months after surgery, groups I and II exhibited similar values of bending load strength to native rib cartilage (p > 0.05), whereas the strength was significantly decreased in groups III and IV (p < 0.05). After 3 months, group I showed increased strength compared with regular rib (p < 0.05). In contrast, bending load strength values of groups II–IV were not significantly different from native cartilage (p > 0.05). At 6 and 12 months, no significant difference was found between groups I–IV and native cartilage. However, bending load strength of group V was significantly reduced in comparison to native control (p < 0.01) (Fig. 9).
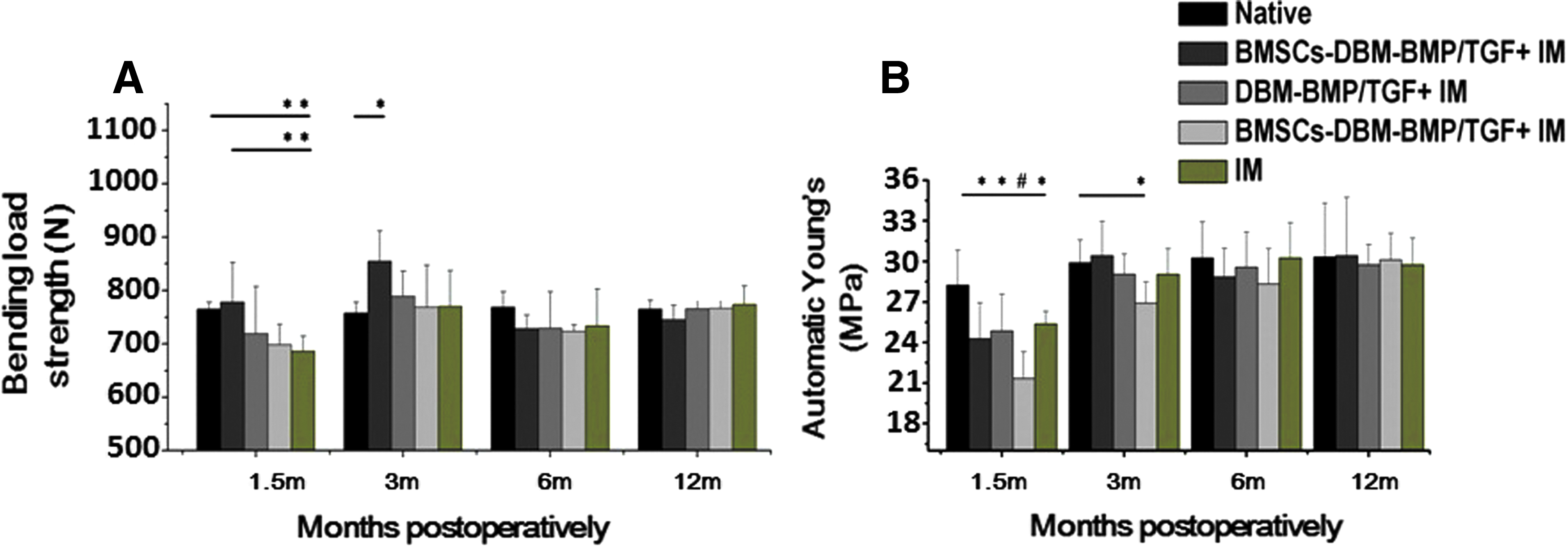
Biomechanical analysis of neobone and neocartilage compared with native rib and costal cartilage.
Young's modulus for the neocartilage was lowest in group III after 1.5 months (p < 0.01). Groups I, II, IV, and V, as well as regular cartilage showed significant differences (p < 0.05). After 6 months, the neocartilage in all study groups showed no significant differences compared with native control (p < 0.05).
Discussion
In this study, we conclusively demonstrated the role of the IM in tissue regeneration. Based on a piece of periosteum and perichondrium from rib and costal cartilage, respectively, as well as their neurovascular bundle, we were able to generate osteochondral composite tissues in vivo. Importantly, this was achieved without the use of common components of tissue engineering, thus qualifying the role of cell seeding, bioscaffolds, and growth factors. The guided self-generated osteochondral composite tissues not only exhibited promising biomorphological features, but also promising biomechanical properties. Moreover, the generation process was safe with an excellent outcome in terms of in vivo functionality. Notably, after undergoing a process of excessive proliferation, structure and function of self-generated tissues were similar to normal tissue and showed stable long-term results without any signs of degeneration. To study the biofunctionality of the regenerated tissue, we chose swine as a large animal model due to its similar structure compared with human. Therefore, the present study paves the way for clinical application.
Our findings show that cell seeding (BMSCs), bioscaffold (DBM), and growth factors (BMP/TGF) enhanced osteogenesis, chondrogenesis, and angiogenesis in the early stage compared with IM group alone. Moreover, biological function was shown to be improved regarding osteogenesis and chondrogenesis with the application of cells, bioscaffold, and growth factors. The IM appears to be the determining factor in the differentiation of seeded cells, histological type of neotissues, and degradation rate of the bioscaffold. In the present study, the widely used DBM scaffold was chosen, because DBM is known for its osteoinductive and osteoconductive effects. 13 Intriguingly, the regenerated composite tissues were found to not only exhibit bony tissue characteristics, but also cartilage, as well as a regular chondro-osseous transition on the uniformly structured DBM scaffold indicating the unique role of the microenvironment in cells and tissue differentiation. Similar stimulatory effects were found for seeded BMSCs and growth factors (BMP/TGF) for the regeneration of composition tissues. It is important to note that the IM-only group showed excellent tissue regeneration without cell seeding (BMSCs), bioscaffold (DBM), and growth factors (BMP/TGF). By contrast, the IM of the intercostal muscle (group V) was associated with no significant osteogenesis, chondrogenesis, and angiogenesis at any time point emphasizing the essential role of the IM. In addition, the absorption rate is radically slower in the absence of the IM. The DBM was completely degraded at 1.5 months in the presence of the IM, whereas degradation without IM was much slower and incomplete even after 3 months demonstrating the impact of the IM on the DBM bioscaffold degradation rate. Our observations inspired us to reconsider: Has there been an overreliance on the value of seeding cells, bioscaffolds, and growth factors previously? Have we overestimated in vitro reconstruction of tissues, but ignored the self-regenerative potential of the IM?
In recent years, the application of stem cells, bioscaffolds, growth factors, and gene therapy in the repair and reconstruction of tissues and organs have attracted much attention due to their stimulatory effects for regeneration.14–22 Bioscaffolds have been used as a carrier to transfer cells, provide shape, guide tissue development, even secrete growth factors, and induce cell differentiation. 23 The structure determined by porosity, pore diameter, surface area-to-volume ratio, pore interconnectivity, and surface texture, chemical components, manufacturing (general processing, parameters, coatings), rate of degradation, the ease of implantation, the effect of cell attachment, and the vascularization process have been extensively studied. 23 In the present study, we found that the DBM bioscaffolds promote the osteogenesis, chondrogenesis, and angiogenesis in the early stage, but the determinant element is the in vivo environment. However, the question remains which role the scaffold exactly plays in bone and cartilage tissue regeneration and whether we may focus too much on the application of scaffolds, while ignoring the body's own significant regenerative capability. For a long time, research efforts in tissue engineering were focused on cell culture, a wide variety of scaffold materials, and growth factors. Our findings demonstrate the enormous potential of the IM which has been neglected in the past.
Conclusions
Our findings demonstrate the determining role of the IM for the generation of tissue in vivo. Importantly, the procedure may be independent of any in vitro culturing of cells and other exogenous factors, thus facilitating the transfer to clinical application and extension to other tissue types and organs.
Footnotes
Acknowledgments
The authors thank the staff and members of the Shanghai Key Laboratory of Orthopedic Implant for their support. Funding: This work was supported by National Natural Science Foundation of China (no. 81230042). Authors' contribution—Study design: Q.F.L., C.D., D.H., K.L., J.W.; Figures: T.H., J.W.; Data analysis: J.W., K.L., C.D., J.W.; Writing: Q.F.L., T.H., K.L., M.Y., J.W., C.D., K.L., D.H.
Disclosure Statement
No competing financial interests exist.