
Abstract
Conventional root canal treatment in immature permanent teeth can lead to early tooth loss in children because root formation is discontinued. We investigated whether the stem cell factor (SCF) could facilitate cell homing in the pulpless immature root canal and promote regeneration of a functional pulp. In vitro, human mesenchymal stem cells (hMSCs) were exposed to SCF at various concentrations for assessing cell migration, proliferation, and differentiation toward odonto/osteoblasts by 3D-chemotaxis slides, WST-1 assay, and alkaline phosphatase activity, respectively. Fibrin gels were used to deliver 15 μg/mL SCF for in vivo experiments. The release kinetic of SCF was assessed in vitro. Two corresponding human immature premolars, with or without SCF, were placed at rat calvariae for 6 and 12 weeks. All tooth specimens were either analyzed histologically and the percentage of tissue ingrowth determined or the cells were extracted from the pulp space, and the mRNA level of DMP1, DSPP, Col1, NGF, and VEGF were assessed by quantitative polymerase chain reaction. In the presence of SCF, we saw an increase in hMSCs directional migration, proliferation, and odonto/osteogenic differentiation. SCF also increased the extent of tissue ingrowth at 6 weeks but not at 12 weeks. However, at this time point, the formed tissue appeared more mature in samples with SCF. In terms of gene transcription, DMP1, Col1, and VEGF were the significantly upregulated genes, while DSPP and NGF were not affected. Our results suggest that SCF can accelerate cell homing and the maturation of the pulp–dentin complex in human immature teeth.
Introduction
A
With the uncertainty of the treatment outcome and the need for a viable pulp for continued root growth, the idea to regenerate a new functional pulp has been suggested. 2 Revascularization of a pulpless immature permanent tooth is a recent technique in a newly evolving field termed regenerative endodontics, which has been discussed in previous years.3,4 The revascularization procedure starts with provoked bleeding from periapical tissues, which can lead to the recruitment of stem cells, most likely from the periapical papilla. 5 The formation of a blood clot acts like a scaffold for those cells. Although this treatment has been performed and reported with successful clinical outcomes such as radiographic signs of tooth maturation and symptom reduction, there are still significant drawbacks and undesirable outcomes, including tooth discoloration, cervical fracture, and especially ectopic hard tissue formation. 6
In regenerative endodontics, cell homing appears to be a more promising strategy than intentional bleeding in the near future.7,8 The concept depends on a scaffold, normally a cellular matrix, and growth factors or cytokines to promote host cell migration into the pulp space and finally regeneration of resident tissues by the host cells. 7 Various scaffold materials, such as collagen, synthetic-polypeptide hydrogels, and fibrin gels, are able to promote odontoblast-like cell formation and/or dental pulp-like tissue production.9–11 Growth factors such as bone morphogenetic protein (BMP), nerve growth factor (NGF), and granulocyte colony-stimulating factor have also shown to facilitate tissue growth from the apical all the way to the coronal aspects of the root canal.8,12 Without these growth factors, the intrinsic signals embedded in dentin and liberated by root canal irrigants such as ethylenediaminetetraacetic acid (EDTA) can also produce an apparently functional pulp.10,13 As a result, the application of the cell homing concept appears efficient to induce repair/regenerative processes within the pulp space and can therefore circumvent some disadvantages of a natural blood clot.
The first step in a cell homing approach is the attraction of cells to the diseased site. To this end, stem cell factor (SCF) has recently been shown to be a powerful chemokine. It is the polypeptide ligand that binds to c-kit receptor (or CD 117) and has chemotactic properties to recruit progenitor cells. 14 At the site of injury, SCF is also found abundantly before the repair processes. 15 In tissue engineering, SCF applications initiated the repair of diverse tissues such as heart,16,17 liver, 18 and nerves. 19 Furthermore, SCF was shown to regulate protein secretion needed during proliferation, chondrogenesis, and extracellular matrix formation of MSCs. 20 SCF and its receptor were also found in differentiating dental pulp cells and in the subodontoblastic layer of Höhl. 21 In pulp tissue engineering, a previous application of SCF on a collagen sponge either with or without pulp cells showed an increased expression of genes required for collagen remodeling, cell migration, and cell proliferation. 21 However, the application of SCF in a cell homing approach to form a fully functional pulp has not been investigated yet.
The present study, therefore, used SCF to accelerate cell homing and improve the regenerative process toward a functional dental pulp. In vitro experiments were set up to test the effect of SCF on human mesenchymal stem cells (hMSCs), and in vivo experiments were performed using a cell homing model in rats 10 to reveal the effect of SCF on tissue ingrowth and odontoblast maturation.
Materials and Methods
Cell migration
Non-coated μ-Slide Chemotaxis 3D assays (Ibidi, Munich, Germany) were used to study the effect of SCF on the directionality of hMSC migration. The fully characterized hMSCs were obtained from Dr. Martin Ehrbar (Department of Obstetrics, University Hospital Zurich). The cells showed multidifferentiation potential, as was tested and confirmed before the main experiments. hMSCs were plated in plastic tissue culture dishes and grown in minimal essential medium (α-MEM; Thermo Fisher Scientific, Steinhausen, Switzerland) supplemented with 10% fetal bovine serum (FBS; Thermo Fisher scientific), 1% penicillin/streptomycin (P/S; Thermo Fisher scientific), and 5 ng/mL FGF (ImmunoTools, Friesoythe, Germany). To passage hMSCs, trypsin/EDTA (Thermo Fisher Scientific) was used each time as previously described. 22 hMSCs were used from passage 4 to 6. 1 × 106 cells per mL were loaded into a middle chamber of the μ-slide according to the instructions of the manufacturer. Pure α-MEM was used to wash away non-adherent cells after 4 h and to starve the cells 4 h prior to the beginning of the assay. One reservoir of the cell chamber was filled with control medium (α-MEM), and the other was filled with the same medium supplemented with different concentrations of stem cell factor (SCF) (ImmunoTools). To observe cell migration, μ-slide was mounted on the stage of an inverted microscope at 37°C in 5% CO2 atmosphere. Video microscopy for the time-lapse experiment was set up to use a 5 × objective lens with phase-contrast mode, and each frame was recoded every 10 min for 24 h. Thirty cells randomly selected were tracked manually using MTrackJ 23 in combination with the ImageJ plug-in. Cell-migration plots and the Rayleigh test were generated by ImageJ plug-in. 24
Cell proliferation
Equal numbers (1 × 104 cells per mL) of the hMSCs from passage 4 to 6 were seeded in 96-well plates 24 h before changing the medium. The growth medium was prepared with complete α-MEM supplemented with 10% FBS and 1% P/S as a reference medium. The complete α-MEM alone was used as a negative control, while double-cell concentration in the reference medium was used as a positive control. Growth media were supplemented with different concentrations of SCF. Measurements were done in triplicate. After 48 h, 10% WST-1 reagent (Roche, Basel, Switzerland) was added to each well for monitoring cell proliferation spectrophotometrically at 630 nm. Absorbance values of the samples and controls were related to the absorbance value of the reference medium.
Odonto/osteogenic differentiation
To test the effect of SCF on odonto/osteogenic differentiation of hMSCs, cells of passage 4–6 were seeded in 96-well plates containing the growth medium described above. Three days after the cells reached 70% confluence, an osteogenic differentiation medium was supplied as previously reported. 22 All measurements were performed in triplicate. The growth medium and the standard differentiation medium were used as a negative and positive control, respectively. Alkaline phosphatase (ALP) activity was assessed quantitatively with a modified assay as described earlier 25 and normalized to total cellular protein concentrations using Coomassie Brilliant Blue staining (Sigma-Aldrich). Furthermore, cells were stained with ALP staining solution, including a mixture of 0.1 mg/mL naphthol AS-MX phosphate and 0.6 mg/mL Fast Blue BB salt (Sigma-Aldrich) and 0.5% N,N-dimethylformamide, 2 mM MgC12 in 0.1 M Tris-HCl at pH 8.5.
Specimen preparation
Ten pairs of bilateral immature premolars with open root apices were supplied by the Orthodontic Department of the Center of Dental Medicine, University of Zurich and originated from patients aged between 9 and 15 years. All teeth used in the present study were extracted for reasons unrelated to this project. Written informed consent for secondary use of the extracted teeth was obtained by all donors (and their legal guardians) before extraction according to the directives set by the National Federal Council (Human Research Ordinance [810.301], Art. 30). Irreversible anonymization of the teeth was performed in accordance with State and Federal Law (Human Research Act [810.30], Art. 2 and 32, Human Research Ordinance [810.301], Art. 25). All these teeth were stored in pairs at −20°C. Teeth were cleaned and processed as reported earlier. 10 Briefly, they were disinfected with 5% NaOCl and accessed from the crown prior to irrigating in the root canal using 5% NaOCl, followed by 17% EDTA (Kantonsapotheke, Zurich, Switzerland). Finally, 0.9% normal saline solution was used to free the teeth from the remaining EDTA. The coronal access was subsequently closed with a glass ionomer cement (Ketac Molar, 3M-ESPE, Seefeld, Germany), and all tooth specimens were kept sterile in 70% ethanol.
Fibrin gels and SCF
0.4% fibrin gels were prepared by mixing 1:1 a 8 mg/mL fibrinogen solution with a solution of 2.5 mmol/L Ca++ and 2 National Institutes of Health Units/mL thrombin (Baxter, Zurich, Switzerland), all prepared in a 100 mM Tris HCl pH 7.6, 150 mM NaCl. SCF at concentration of 15 μg/mL (ImmunoTools; Friesoythe, Germany) was added into thrombin solution prior to the mixing step.
In vitro release
Fifty microliters fibrin gel precursor 1:1 mixture doped with 15 μg/mL SCF was injected into 18 single-opening silicone tubes of 2 mm diameter and 6 mm length and allowed to cure. Next, the silicone tubes were immersed in phosphate-buffered saline (PBS) at 37°C, and the release kinetics of SCF was observed up to 28 days using an enzyme-linked immunosorbent assay (R&D Systems). SCF without a fibrin hydrogel was used as control to monitor its degradation over time.
In vivo embedding
All experimental procedures with animals were approved by the local authorities (Veterinary Office of Canton Zurich No. 108/2012). Adult female Sprague Dawley rats weighing 200–250 g were used for these experiments. The prepared teeth filled with fibrin hydrogels with or without SCF were placed on top of the calvaria of rats as previously described. 10 The paired teeth were horizontally placed in the same animal for 6 or 12 weeks and their opened apexes turned in opposing directions (left and right).
Histological evaluation
Tooth specimens were collected following carbon dioxide euthanasia of the rats and were immediately fixed in 4% paraformaldehyde followed by a serial dehydration in ethanol. In this study, we used Technovit 9100 New (Heraeus Kulzer, Wehrheim, Germany) to embed all specimens according to the manufacturer's instructions. The resin blocks were longitudinally cut at the middle of the root canal in the mesiodistal plane before sectioning 0.5-μm-thick slides with a microtome (Leica Microsystems, Heerbrugg, Switzerland).
Histomorphometric assessment
Histological images were prepared as previously described. 10 Three subsequent sections were made from the center of each specimen and used for histological analysis. The slides were stained with Goldner's Trichrome, and the images of them were taken using a Mirax slide scanner (Zeiss, Feldbach, Switzerland). Quantitative analysis was performed using a measurement module from Pannoramic Viewer (3DHISTECH, Budapest, Hungary). The areas of ingrown tissue were normalized to the total pulp space area and three sections per specimen averaged. Mean values per specimens were used for the statistical comparison between groups. For the evaluation of the cytoplasmic process, three representative areas from each tooth were randomly selected, and the extent of the process of 10 odontoblast-like cells from the pulp–dentin interface was measured.
Gene expression
Cells within the bulk ingrowth and cells attached to the dentinal wall were collected from teeth that had been embedded in the rat for 12 weeks. RNA was extracted using TRIzol® (Life Technology, Luzern, Switzerland) from specimens preserved in RNAlater (Qiagen, Hilden, Germany). Total RNA was measured following the clean-up protocol using a silica membrane column (Qiagen). Complementary DNA (cDNA) was transcribed from 200 ng RNA using a cDNA Synthesis Kit (Roche, Basel, Switzerland). For the quantitative expression, real-time reverse transcription polymerase chain reaction was performed using the LightCycler® 480 DNA SYBR Green I master (Roche) and 25 μL of master mix consisting of 2 μL of cDNA, 12.5 μL of SYBR Green, 0.3 μM of primer, and RNase-free water. The rat-specific forward (F) and reverse (R) primers, including DSPP, VEGF, NGF, and COL type I, were used in this experiment, and GAPDH was the housekeeping gene for internal gene normalization (Table 1). Quantitative polymerase chain reaction was done in the following three steps: 2 min at 50°C, 15 min at 95°C, followed by 55 cycles of 15 s at 94°C, 30 s at 55°C, and 30 s at 72°C. Normalized gene expression was analyzed using the 2−ΔΔCt method and was compared statistically between groups.
Statistical analysis
Following a normal distribution evaluation, in vitro results were statistically compared by one-way analysis of variance followed by Fisher's Least Significant Difference for pairwise tests. For the in vivo data, the difference between two data sets was assessed using the Mann–Whitney U test. All statistical tests were performed using SPSS 22.0. A difference was considered significant at the 5% level. For the cell migration assay, the data were analyzed with Rayleigh test, which determined uniformity in circular distribution of cell end points. A p-value below 0.05 implied an unequaled movement of cells.
Results
In vitro effects of SCF on hMSCs
To examine whether SCF can direct hMSC migration, we performed experiments in chemotaxis microslide chambers. Tracking the movement of cells exposed on one side to 2.5 and 12.5 μg/mL of SCF, the hMSCs preferentially moved toward the SCF containing reservoirs (Fig. 1A). Therefore, a gradient formed by SCF from a peak concentration of 2.5 μg/mL was sufficient to direct hMSCs toward the source of SCF.
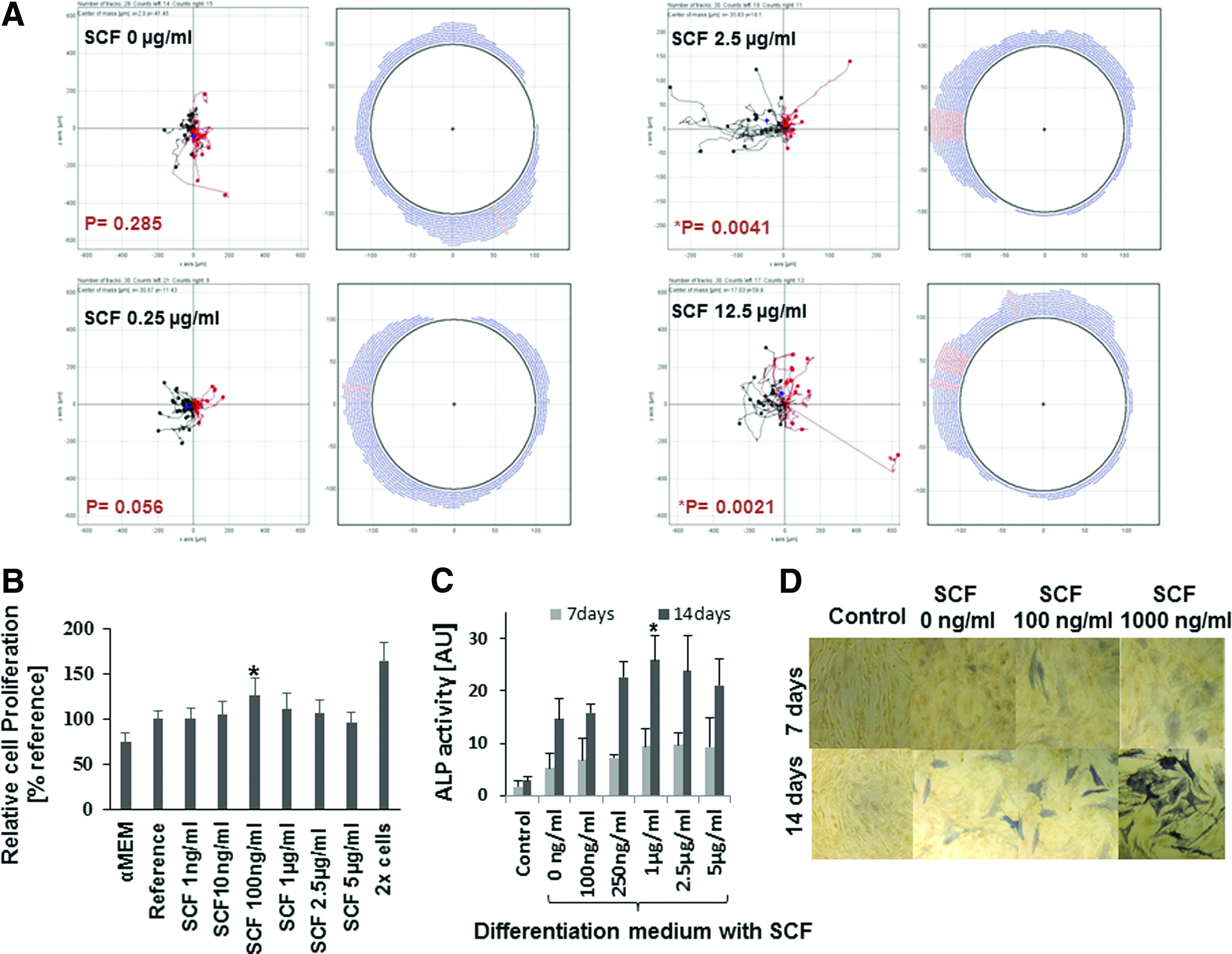
In vitro effects of SCF on the migration, proliferation, and odonto/osteogenic differentiation of human mesenchymal stem cells (hMSCs).
To further examine the effect of SCF on hMSCs, we followed proliferation and odonto/osteogenic differentiation. At a concentration of 100 ng/mL SCF, hMSC proliferation was significantly faster than in the reference group, that is, the same medium lacking SCF and the cell number increased by an average of 30% (Fig. 1B). The negative control containing only the complete α-MEM showed lower cell growth compared to the reference with additional 10% FBS. Meanwhile, the positive control with the double-cell load revealed almost twice the cell proliferation compared to the reference group. Below 100 ng/mL SCF, no significant increase in proliferation could be observed. In terms of differentiation, 1000 ng/mL SCF increased ALP activity (26 ± 5 U) significantly in an osteogenic medium (Fig. 1C). The SCF at high concentrations (2500 and 5000 ng/mL), however, showed a very low level of response. The increase in ALP for 1000 ng/mL was confirmed by ALP staining (Fig. 1D). In essence, concentrations of SCF from 100 ng/mL increased proliferation of hMSCs, but differentiation was only affected at very high concentrations of 1000 ng/mL SCF.
Release kinetics of SCF
In vitro results suggested that SCF can be freed from the current fibrin gel formulation. The release of SCF was observed over the course of 4 weeks. Release was low during the first 3 days and completed after 7 days (Fig. 2A). The decrease in SCF from day 7 until day 28 reflects instability of human SCF in PBS (Fig. 2B).

In vitro release of SCF from fibrin matrix over the period of 28 days.
Cell homing by SCF
To assess the effect of SCF on tissue ingrowth into immature teeth placed on top of the calvarial bone, we analyzed teeth implanted for 6 and 12 weeks histologically. At 6 weeks for teeth filled with fibrin gel plus 15 μg/mL SCF, the percentage of tissue ingrowth at 21% ± 5% was higher compared to the 6% ± 2% observed with fibrin gel alone (Fig. 3). At 12 weeks, both numbers increased. In the presence of SCF, tissue ingrowth was 47% ± 15%. In the teeth without SCF, soft tissue was present in 38% ± 13% of the pulp space.

The effect of SCF on tissue ingrowth. Bilateral human premolars filled with fibrin gel alone (FG) or in combination with 15 μg/mL SCF (FG+SCF) were implanted on top of the rat calvaria for 6 and 12 weeks. The percentage of the pulp space where tissue had grown in was determined based on the middle sections from the histological sections. The average value of each group is indicated by a horizontal bar. Both intervals showed a tendency toward greater tissue formation with the SCF-loaded fibrin gel compared to the pure fibrin gel. The mean values, however, differed statistically significantly (*p < 0.001) only at 6 weeks, but not at 12 weeks.
Histology of bilateral human premolars harvested after 6 weeks revealed that tissue ingrowth was accelerated by the application of SCF, and the morphology of this tissue was also affected (Fig. 4). In the absence of SCF, ingrown tissue was found at the apical third of the root canal only and appeared to be at an early stage of development, since areas of accumulated red blood cells were still visible. Immature mineral matrix was also below half of the old predentin thickness. Newly formed hard tissue could not be detected at the dentinal wall or the apical opening, regardless of whether SCF was applied or not. The stage of tissue maturation, however, progressed in the presence of SCF-doped fibrin gels. First, the area of tissue ingrowth reached up to the middle third of the root canal and second, early blood vessel formation together with red blood cells could be appreciated. Third, the immature mineral matrix reached along the entire predentin layer.

Histological observations at 6 weeks. The bilateral teeth were filled with fibrin gel that was either doped with SCF or not and were transplanted in the same rat
At 12 weeks, the effect of SCF on overall tissue ingrowth was not significant anymore (Figs. 3 and 5), but the formed tissue in specimens containing SCF was more mature. Without SCF, the ingrown tissue extended to the middle third of the root canal. It contained highly developed blood vessels together with odontoblast-like cells at the dentinal wall, whereas only connective tissue developed to close the opened apex. A similar pattern could be seen in the presence of SCF. However, the tissue appeared more diversified. First, hard tissue had developed at the apical opening; second, revascularization appeared to be improved; and third, the odontoblast-like cells extended their processes further down the dentinal tubules.
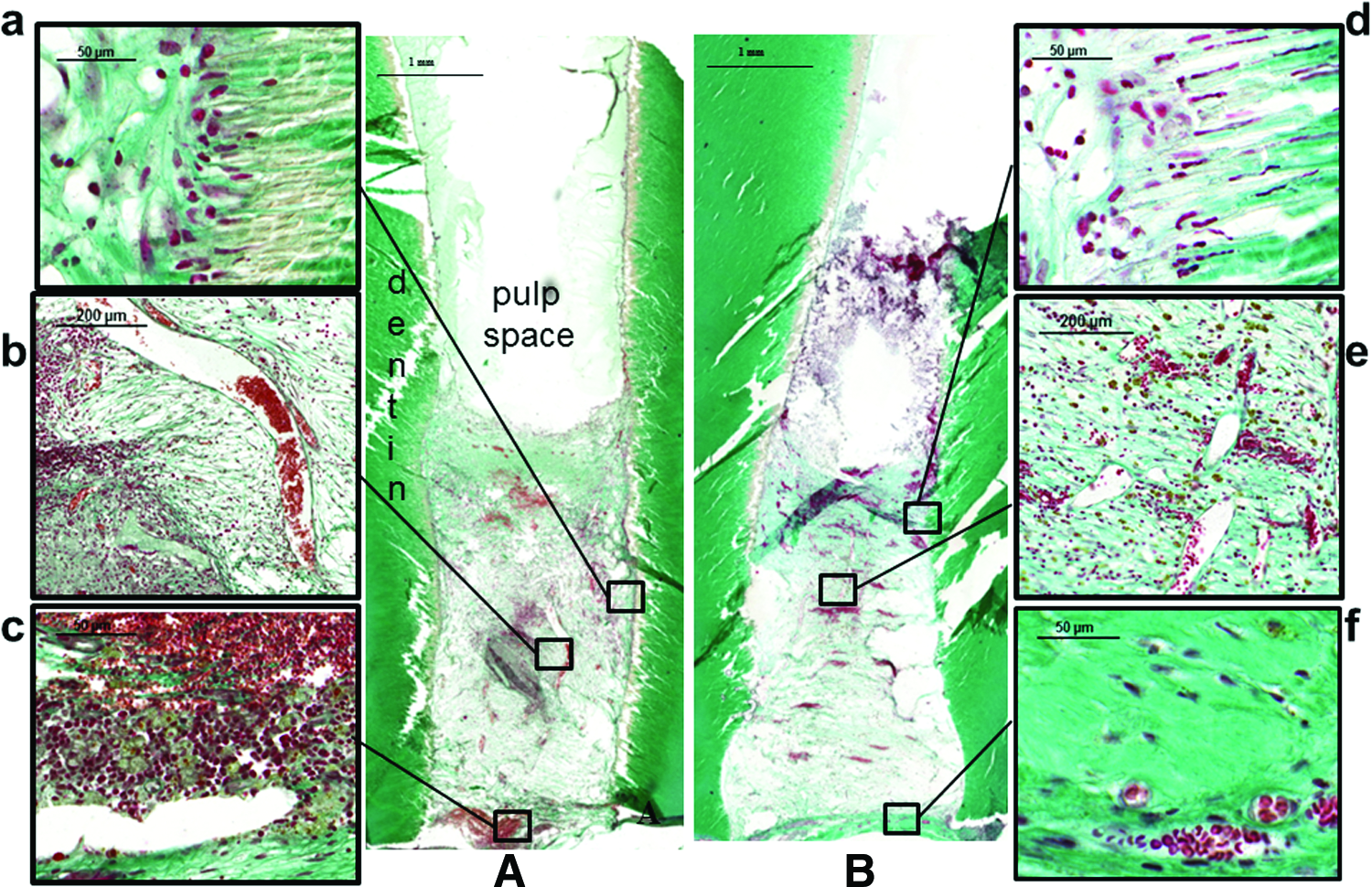
Histological observations at 12 weeks. Root canals filled with the SCF-combined fibrin gel were placed on top of rat calvaria together with a paired tooth filled with mere fibrin gel as a control
As shown in Figure 6 A, in the presence of SCF, odontoblast-like process reached 87 ± 6 μm into the dentin, while in absence of SCF, the corresponding value was 26 ± 3 μm (p < 0.001). On the level of DSPP and NGF expression, no difference was seen between fibrin gel+SCF and nondoped fibrin gel samples. DMP1 and Col1 mRNA content in the SCF-doped fibrin gels was significantly upregulated in cells attached to the dentinal wall (Fig. 6B). In the newly formed tissue in the pulp space, the expression of VEGF was slightly increased.
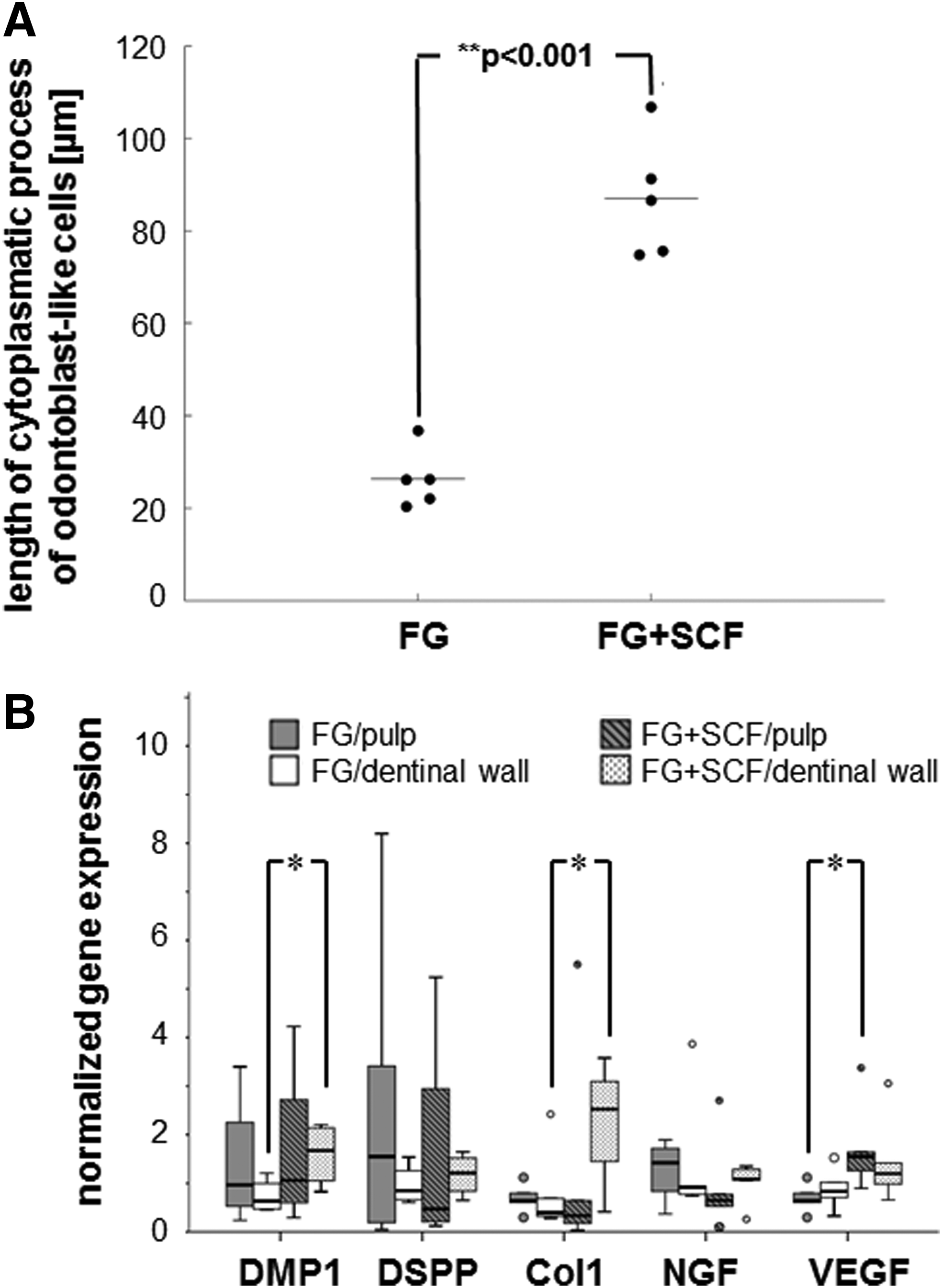
Analysis of the newly formed tissue at 12 weeks.
Discussion
SCF is a chemokine shown to promote migration, neovascularization, and collagen remodeling of dental pulp progenitor cells. 21 To address its potential to improve current cell homing strategies in dental pulp tissue engineering, we tested the effect of SCF on the directionality of hMSC migration in vitro and tested its in vivo impact by delivering it with a fibrin gel in a cell homing model. 10
Our results showed that SCF directs migration of mesenchymal stem cells, but has a minor effect on their proliferation and differentiation. The concentration of SCF needed to direct the migration of hMSCs was higher than previously reported. 26 This might be due to the methodology used to evaluate cell migration and/or the source of the SCF. The advantage of the current methodology is that chemotaxis slides allow observing the migration in linear and stable concentration profiles and distinguish between random migration from primed and directed migration. 24 As the time frame for proliferation was longer than the time frame for migration, prolonged exposure of a high SCF concentration directly on hMSCs appeared to cause cell distress 20 and not an increased hMSC proliferation. In fact, our finding showed that a responsive dose of SCF promotes cell proliferation similar to the effective dose of recent studies,21,27 although their observations occurred after a longer time period and in different growth media. Beyond proliferation, high SCF concentrations affected the osteogenic differentiation, since ALP activity was also increased, which is in line with previous studies.20,21 SCF was found to increase the expression of Collagen type I and III, basic fibroblast growth factor, BMP-6, and tissue inhibitor of metalloproteinase 1 and 4 in MSCs. All these proteins are involved in proliferation, chondrogenesis, and extracellular matrix protein regulation. 20
The release of SCF appeared to be completed after day 7. Despite this short time window, the positive effect of SCF on tissue ingrowth into the pulp space was evident until week 6, but did not last until week 12. Therefore, the development of a sustained release system for SCF could further improve tissue ingrowth and maturation. 28 On the molecular level, SCF can stimulate the signaling cascades of PI3K/Akt and MEK/ERK, thereby rapidly increasing ERK and AKT phosphorylation within the cells. 21 Such very early effects can be the reason why at 6 weeks we saw an increase in tissue ingrowth in fibrin gels with SCF compared to fibrin gels alone. For both time points, the amount of regenerated tissue was similar to an earlier study in which tissue regeneration was achieved by stem cell delivery in immature dog teeth at 14 and 28 days.29,30 This would imply that the use of SCF for cell homing accelerated tissue ingrowth, yet a further acceleration can only be achieved by the application of stem cells. Compared to the application of the revascularization technique in rat teeth over the same period, 31 fibrin gels with SCF apparently resulted in more and earlier tissue ingrowth. However, these results were obtained in different models and can thus not be compared conclusively.
At 12 weeks, the addition of SCF did not result in a significant improvement of tissue ingrowth. The average of percent tissue ingrowth of 12-week implantation in this study was at around 40–50% for the mere fibrin gel, as well as the SCF combined fibrin gel. Although the result did not show a significant difference between both groups, it showed a similar percent tissue ingrowth with our previous publication. 10 This consistence suggested that the preparation method and animal model are quite stable and reliable to be used for testing cell homing during pulp regeneration. The tissue morphology at 12 weeks with SCF also resembled the outcome observed with fibrin only. 10 Nevertheless, more calcified tissue could be found at the apical opening and odontoblastic-like processes extended further into the dentinal tubules in teeth with SCF. Together, these results suggest that under the influence of SCF, odontoblast-like cells formed earlier, covered more of the pulp–dentin interface, and extended further into dentine. 32 Therefore, under the current conditions, SCF secondarily accelerated the maturation of the newly formed pulp tissue and hence the overall regeneration process.
Involvement in tissue maturation by SCF is also evident in the gene expression analysis. As a result of SCF application, Col1 and DMP1 were upregulated in cells adhering to dentin, where the migrated cells should be transformed to odontoblasts and hence produce minerals. The role of SCF to stimulate collagen organization of mineral matrix through the upregulation of Col I and III has already been reported, 21 whereas the effect on DMP1 expression reported in this study has not yet been described and, therefore, suggests additional roles of SCF during dentinogenesis. Since DMP1 regulates DSPP transcription during early odontoblast maturation and function, 33 in our tissue, the odontoblast-like cells may have been in different maturation stages, where DSPP gene expression had not increased yet. Nevertheless, the impact of SCF on genes regulating odontoblast maturation and function supports our in vitro result. Therefore, SCF also showed to establish a pro-angiogenic milieu by increasing VEGF expression in the recruited cells of the ingrown tissue (Fig. 6), resulting in abundant blood vessels (Fig. 4), similar to what was reported earlier for triggering revascularization in infarcted tissue.33,34 However, NGF expression did not differ, which is in line with the histology where we did not see a clear reinnervation.
Conclusion
Under the current conditions, SCF influenced stem cell migration, localization, proliferation, and differentiation. It also increased tissue ingrowth at 6 weeks and caused the formation of a better developed pulp-like tissue at 12 weeks. Thus, under the conditions of the current study, SCF shows the ability to recruit cells into immature human teeth. It does show promise to be implemented in the cell homing approach in the field of regenerative endodontics.
Footnotes
Acknowledgments
The authors thank Yvonne Bloemhard, Ana Perez, and Alexander Tchouboukov for excellent technical assistance. This research was partly supported by a Swiss Government Scholarship and the Dental Association of Switzerland (270-13). The hMSCs used in the current study were kindly provided by Dr. Martin Ehrbar University Hospital Zurich.
Disclosure Statement
No competing financial interests exist.