
Abstract
In the oral cavity, the tongue is the anatomic subsite most commonly involved by invasive squamous cell carcinoma. Current treatment protocols often require significant tissue resection to achieve adequate negative margins and optimal local tumor control. Reconstruction of the tongue while preserving and/or restoring its critical vocal, chewing, and swallowing functions remains one of the major challenges in head and neck oncologic surgery. We investigated the in vitro feasibility of fabricating a novel combinatorial construct using porcine small intestinal submucosa extracellular matrix (SIS-ECM) and human gingiva-derived mesenchymal stem cells (GMSCs) as a GMSC/SIS-ECM tissue graft for the tongue reconstruction. We developed a rat model of critical-sized myomucosal defect of the tongue that allowed the testing of therapeutic effects of an acellular SIS-ECM construct versus a GMSC/SIS-ECM construct on repair and regeneration of the tongue defect. We showed that the GMSC/SIS-ECM construct engrafted at the host recipient site, promoted soft tissue healing, and regenerated the muscular layer, compared to the SIS-ECM alone or nontreated defect controls. Furthermore, our results revealed that transplantation of the GMSC/SIS-ECM construct significantly increased the expression of several myogenic transcriptional factors and simultaneously suppressed the expression of type I collagen at the wounded area of the tongue. These compelling findings suggest that, unlike the tongue contracture and fibrosis of the nontreated defect group, transplantation of the combinatorial GMSC/SIS-ECM constructs accelerates wound healing and muscle regeneration and maintains the overall tongue shape, possibly by both enhancing the function of endogenous skeletal progenitor cells and suppressing fibrosis. Together, our findings indicate that GMSC/SIS-ECM potentially served as a myomucosal graft for tongue reconstruction postsurgery of head and neck cancer.
Introduction
W
Techniques that are available today for tongue reconstruction range from primary closure, healing by secondary intention, biologic skin substitutes, skin grafts, local and regional flaps to more sophisticated microvascular-free tissue transfer flaps. 6 The ultimate goal of tongue reconstruction irrespective of etiology is to restore the integrity of the tongue while preserving its critical functions (i.e., articulation, mastication, deglutition) and minimize the morbidity profile of a selected reconstructive technique. 7
Through decades of evolution in reconstructive principles and techniques, microvascular-free tissue transfer has evolved as the reconstructive technique of choice following extirpation of malignant neoplasms. 8 Soft tissue-free flaps, such as the radial forearm-free flap and the anterolateral thigh-free flap, have opened up new avenues for improving tongue reconstruction outcomes based on their tissue bulk and versatility of flap inset that limit tethering of the tongue and, if necessary, allowing for composite tissue replacement.8,9 However, these flaps, made up of skin, subcutaneous adipose tissue, and fascia, do not allow for the restoration of muscular-like tissue. Furthermore, harvesting these flaps will always result in donor site morbidity that will cause some degrees of local pain, edema, limb weakness, and scar formation.
Implant transplantation has been explored as another reconstructive option. Of particular interest is the ability to implant biological materials that promote tongue tissue regeneration with resultant biological tissues representing normal tongue anatomy that is devoid of fibrosis. Even though various combinations of implants have been used, treatment outcomes are still suboptimal.10,11 A candidate implant is the porcine small intestinal submucosa extracellular matrix (SIS-ECM), which has been shown to promote tissue-specific growth and differentiation across various applications. 12
Multiple studies have demonstrated that SIS-ECM contains key ECM components and growth factors necessary for normal tissue regeneration, such as collagen, proteoglycan glycosaminoglycan, glycoprotein, vascular endothelial growth factor (VEGF), 13 transforming growth factor-beta (TGF-β), basic fibroblast growth factor (bFGF), and epidermal growth factor (EGF). 14 SIS has been tested in animals to successfully repair urinary bladder, 15 abdominal body wall defects, 16 and esophageal, 17 tracheal, 18 cardiovascular, 19 partial- and full-thickness skin defects. 20 More importantly, as a product approved by the U.S. Food and Drug Administration (FDA), this biomaterial has been applied to over 1 million patients for the repair of a variety of tissue defects.21–29 These studies have demonstrated the compatibility of SIS-ECM with host tissues by not only providing structural support but also promoting the regenerative responses of the host during the tissue repairing process.
Mesenchymal stem cells (MSCs) represent a subpopulation of multipotent stromal cells that reside in almost all adult tissues and are capable of differentiating into several different cell lineages, escaping allogeneic immune responses, and also possess potent immunomodulatory and anti-inflammatory functions.30,31 Accumulating evidence suggests that both endogenous and exogenous MSCs are capable of sensing their microenvironment and migrating to injured sites where they interact with other types of structural and immune cells to orchestrate the complex site-specific tissue repair process.30,32 These unique properties make MSCs a unique candidate cell source for stem cell-based therapy in a wide range of clinical scenarios, including the tissue engineering/regeneration of various types of tissues and organs.30,32,33
Recent studies have shown that SIS-ECM could be an ideal scaffold for effective delivery of MSCs, whereby combinatorial use of SIS-ECM and MSCs exhibited improved regenerative outcome in skin wound healing and a variety of tissue defects, including cardiovascular, 19 urinary bladder, vocal fold, 34 tracheal, 18 muscle, and bone tissues.18,19,20,34–37 However, little is known about the potential application of SIS-ECM alone or in combination with MSCs in repair/regeneration of critical-sized tongue defects.
Our group has isolated and characterized a unique population of gingiva-derived MSCs (GMSCs), which showed a high proliferation rate, multipotent differentiation potential, and potent immunomodulatory/anti-inflammatory functions.38,39 We have also shown that the systemic administration of GMSCs could promote skin wound healing and mitigate chemotherapy-induced oral mucositis.40,41 In this study, we developed a rat model of critical-sized myomucosal defect of the tongue, which allows us to test the therapeutic effects of the combinatorial GMSC/SIS-ECM constructs on repair and regeneration of the tongue.
Materials and Methods
Animals
Female Sprague-Dawley rats weighing 200–250 g (6–7 weeks old) (Charles River Laboratories, Wilmington, MA) were used in this study. All animal procedures were handled according to the guidelines of the Institutional Animal Care and Use Committee (IACUC) of the University of Pennsylvania. We adopted a randomized, prospective, and controlled animal model design according to all the recommendations of the ARRIVE (Animal Research: Reporting In Vivo Experiments) guidelines. Rats were group-housed in polycarbonate cages (three animals per cage) in the animal facilities with controlled temperature (23°C ± 2°C), 40–65% of humidity, and a 12-h light/12-h dark cycle. Rats were acclimatized for at least 1 week before the study, fed with a standard laboratory diet, and allowed ad libitum access to drinking water.
Cell cultures
Gingival tissues were obtained as remnants of discarded tissues from healthy human subjects who underwent routine dental procedures under the approved Institutional Review Board (IRB) protocol at the University of Pennsylvania. The gingiva-derived mesenchymal stem cells (GMSCs) were isolated and cultured according to methods as we previously described.
38
Primary cells were cultured and ex vivo expanded in complete growth medium consisting of alpha-MEM supplemented with 1%
SIS-ECM construct preparation
A novel combined construct was generated using an FDA-approved decellularized porcine small intestinal submucosa extracellular matrix (SIS-ECM 2.0) (Cook Biotech, Inc., West Lafayette, IN) 42 seeded with human gingiva-derived mesenchymal stem cells (GMSCs). Prelabeling of GMSCs with PKH26 fluorescein dye (Sigma-Aldrich, St. Louis, MO) was performed according to the manufacturer's instructions. Then, 5 × 4 mm strips of SIS-ECM membranes were soaked in serum-free medium for 24 h, and GMSCs (3.5 × 105 cells/cm2) prelabeled with PKH26 were seeded onto the mucosal side of the SIS-ECM and cultured for 48 h at 37°C with 5% CO2 before being transplanted into the defected tongues of rats. SIS-ECM membranes soaked in serum-free medium for 24 h without seeded GMSCs were used as controls.
Animal surgery
Animals were anesthetized with intraperitoneal injection of ketamine/xylazine (100/10 mg/kg) followed by injection of 0.1 mL of 1% lidocaine with 1:100,000 epinephrine into the left hemitongue for local vasoconstriction. All rats underwent a left-sided anterior defect by way of a lateral approach. A tongue wound was created using a 6-mm biopsy punch (Miltex, Inc., York, PA) in the left side of anterior dorsal tongue surface at the depth (3 mm) of the muscle layers to damage both the epithelium and the stroma.
Animals were randomly divided into the following groups (n = 6/group): (1) Tongue defect; (2) Tongue defect transplanted with SIS-ECM; (3) Tongue defects transplanted with SIS-ECM seeded with GMSCs prelabeled with PKH26 (GMSC/SIS-ECM). The SIS-ECM constructs were patched over the wound, with the cell-seeded side oriented toward the wounded muscle layers. Then, 8–0 Ethilon (Ethicon, Inc., Somerville, NJ) interrupted sutures were applied to secure the construct. The entire procedure was performed under a surgical microscope (Global Surgical Corporation, St. Louis, MO).
At days 0, 1, 3, 5, 7 following surgery, the wounds were photographed using a Nikon D90 digital camera with an AF Micro NIKKOR 60 mm lens. The images were uploaded to a computer and opened with Olympus cellSens™ imaging software (Olympus America, Inc., Center Valley, PA). For each photographic image, measurements were calibrated using a ruler at the base of the image included in the photographic frame. The wound margins were defined and traced from the photographic images, and the wound areas were calculated as a percent area of the original wound at day 0.43,44 On day 14 and 28 postsurgery, rats from each group were sacrificed and the tongues were harvested by transection at the circumvallate papillae and subsequently prepared for histological and immunohistochemical analysis.
Histological and immunofluorescence studies
The tongue samples were fixed in 10% neutralized formalin for 48 h and 5-μm-thick paraffin sections and 8-μm-thick cryosections were cut, respectively. Hematoxylin and eosin staining was performed according to the standard procedures, while Trichrome staining of collagens was performed using a Trichrome Stain Kit for connective tissue stain according to the manufacturer's procedures (Abcam, Cambridge, MA).
For immunofluorescence studies, the cryosections were permeabilized and blocked in PBS with 3% bovine serum albumin and 0.5%Triton X-100 at room temperature for 1 h. Then, the sections were incubated with primary antibodies for MyoD, Myf5 (Santa Cruz Biotechnology, Inc., Santa Cruz, CA), or PAX7 (R&D Systems, Inc., Minneapolis, MN) (1:250) overnight at 4°C, followed by incubation with FITC-conjugated secondary antibodies for 1 h at room temperature. Isotype-matched control antibodies (BioLegend, Inc., San Diego, CA) were used as negative controls. Nuclei were counterstained with 4′,6′-diamidino-2-phenylindole (DAPI) (Life Technologies), and slides were observed under a fluorescence microscope (Olympus IX-73). The integrated immunofluorescence density of a region of interest (ROI) was quantified using Olympus cellSens imaging software.
Western blotting
Equal amount of protein samples (30 μg) from the injured areas of the tongue was separated on 10% sodium dodecyl sulfate–polyacrylamide gel electrophoresis (SDS-PAGE) and electroblotted onto nitrocellulose membrane (Bio-Rad, Hercules, CA). After blocking with TBS/5% nonfat dry milk, the membrane was incubated with antibodies against MYOD, PAX7, and MYF5 (1:1000) followed by incubation with a horseradish peroxidase (HRP)-conjugated secondary antibody, and the signals were visualized by enhanced chemiluminescence detection (Thermo Scientific). The blots were also reprobed with a specific antibody against β-actin (Sigma) as internal controls.
Statistical analyses
Differences between experimental and control groups were analyzed by the paired Student's t-test. One-way analysis of variance was used to test the statistical significance of multiple group differences, unless otherwise indicated. Post hoc pairwise comparison between individual groups was made using the Tukey test. p-Values <0.05 were considered statistically significant. SPSS software was used for all the analyses. All data are expressed as mean ± standard deviation (S.D.).
Results
Generation of combinatorial constructs of GMSC/SIS-ECM
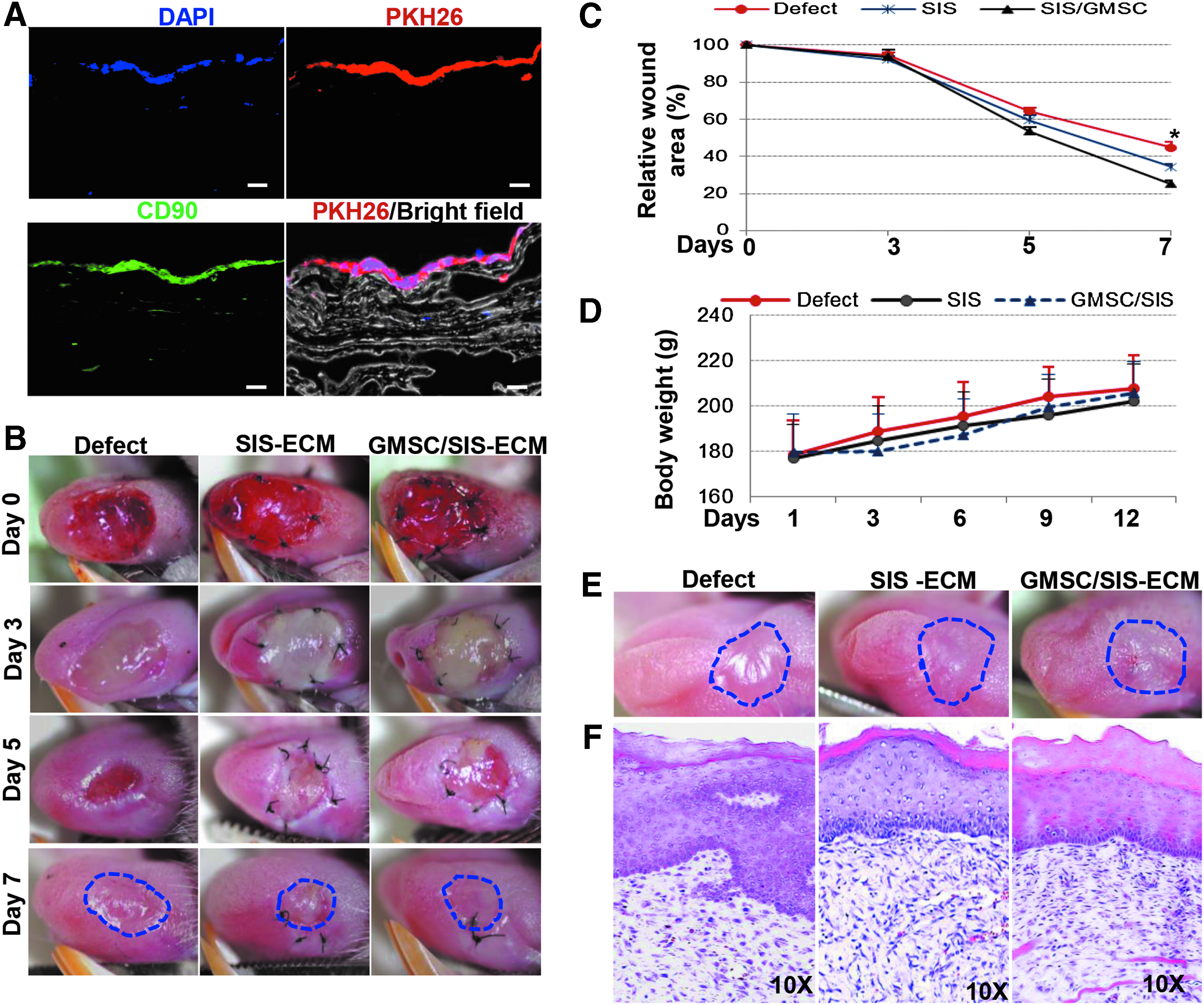
Human gingiva-derived mesenchymal stem cells (GMSCs) used in this study were isolated and characterized according to the expression of a panel of cell surface markers (CD29, CD44, CD73, CD90) but negative for hematopoietic and endothelial cell surface markers and their multipotent differentiation capabilities as previously described. 38 To fabricate the combinatorial construct, GMSCs prelabeled with PKH26 were seeded onto the mucosal side of the decellularized SIS-ECM scaffold at a cell density of 3.5 × 105 cells/cm2 according to a previous report. 19 After culture for 48 h, the constructs were harvested and immunofluorescence staining showed that a confluent monolayer of GMSCs adhered on SIS-ECM scaffold and positively expressed CD90 (Fig. 1A).
Integration of GMSC/SIS-ECM constructs with host tissues and promotes tongue wound healing.
Integration of GMSC/SIS-ECM constructs with host tissues promotes tongue wound healing
We then transplanted the SIS-ECM scaffold seeded with (GMSC/SIS-ECM) or without GMSCs onto the critical-sized tongue defects and observed the wound healing process at different time points. All rats were able to survive after the surgical insult and tolerate the defect while maintaining appropriate body weight (Fig. 1D).
Our results indicated that the transplanted SIS-ECM scaffold was completely resorbed by day 7 after transplantation (Fig. 1B). The wound healing rate is defined as the gross epithelialization of the wound defect area. 45 Until day 5 postsurgery, no obvious differences in the wound healing rate were observed among different groups (Fig. 1B). However, by day 7 postsurgery, the tongue wound areas for both SIS-ECM and GMSC/SIS-ECM groups were smaller than the defect control group; whereby, the GMSC/SIS-ECM group had a faster wound healing rate than SIS-ECM group (p < 0.05) (Fig. 1C).
By day 14 postsurgery, clinical morphology of tongue indicated that both SIS-ECM and GMSC/SIS-ECM groups showed less scarring and wound contracture and maintained the overall tongue shape without deformity compared to the defect control, whereas GMSC/SIS-ECM group displayed better tissue restoration than transplantation of SIS-ECM scaffold alone (Fig. 1E). Histological analysis showed complete reepithelialization throughout all groups, but GMSC/SIS-ECM group showed apparent muscle regeneration compared with SIS-ECM alone and defect control groups (Fig. 1F). These findings suggest that the combinatorial GMSC/SIS-ECM constructs are capable to regenerate, in some extent, some specialized tissue components, specifically the muscle layer, compared to SIS-ECM scaffold alone or nontreated defect control.
Engraftment of transplanted GMSCs at the wound site
We next determined whether PKH26 prelabeled GMSCs transplanted with SIS-ECM scaffold engrafted at the wound defect sites following transplantation. At day 14 post-transplantation of the PKH26-labeled GMSC/SIS-ECM construct, frozen sections were harvested and immunostained with antibodies for MyoD, Myf5, and PAX7, three myogenic transcription factors.46,47 Using immunofluorescent studies, we showed that PKH26 labeled GMSCs transplanted with SIS-ECM scaffold engrafted at the deep muscle layer of the tongue defect (Fig. 2A); ∼10% engrafted PKH26 labeled GMSCs harbored overlapping green signals that represent the positive expression of MyoD, Myf5, or PAX7 (Fig. 2B–D). These findings suggest that a small proportion of transplanted GMSCs engrafted at the deep muscle layer of the critical tongue defect and were able to differentiate into myoblast progenitor-like cells.

Engraftment of Transplanted GMSCs at the Wound Site and Expression of Myogenic Transcriptional Factors.
Transplantation of GMSC/SIS-ECM constructs increased the expression of myogenic transcriptional factors
We next determined the effect of transplantation of GMSC/SIS-ECM constructs on the expression of myogenic transcriptional factors, MyoD, Myf5, and PAX7, in the wounded defect area of the tongue on day 14 postsurgery.
Our results showed that transplantation of both SIS-ECM alone and GMSC/SIS-ECM significantly increased the expression of MyoD and PAX7, but the effect conferred by the combinatorial GMSC/SIS-ECM constructs was more pronounced than the SIS-ECM scaffold alone (Fig. 3A, B, D, E). In addition, we found that transplantation of the combinatorial GMSC/SIS-ECM constructs, but not the SIS-ECM scaffold alone, led to a robust increase in the expression of Myf5 (Fig. 4A, B). The increased expression of these myogenic transcriptional factors induced by transplantation of the combinatorial GMSC/SIS-ECM constructs was further confirmed by Western blot analysis (Figs. 3C, F and 4C).
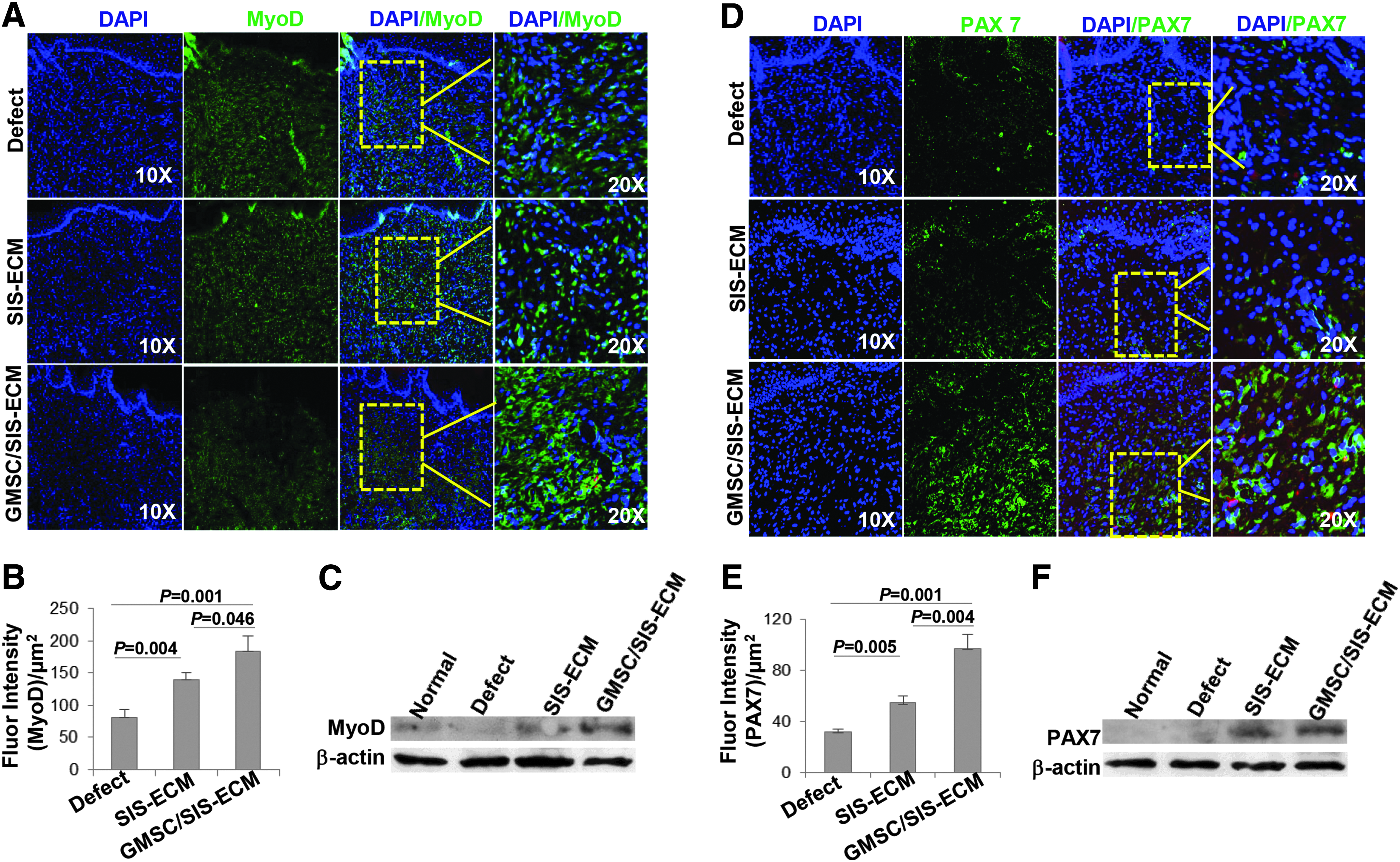
Increased expression of MyoD and PAX7 in both wounded tongue areas with transplantation of GMSC/SIS-ECM and SIS-ECM in comparison with defect control. Expression of MyoD (green)

Increased expression of Myf5 in wounded tongue areas with transplantation of GMSC/SIS-ECM in comparison with SIS-ECM alone and defect control.
These findings further support the notion that transplantation of the combinatorial GMSC/SIS-ECM constructs not only accelerates tongue wound healing but also induces muscle regeneration, possibly by enhancing the function of endogenous skeletal progenitor cells.
Transplantation of GMSC/SIS-ECM constructs decreased the expression of type I collagen
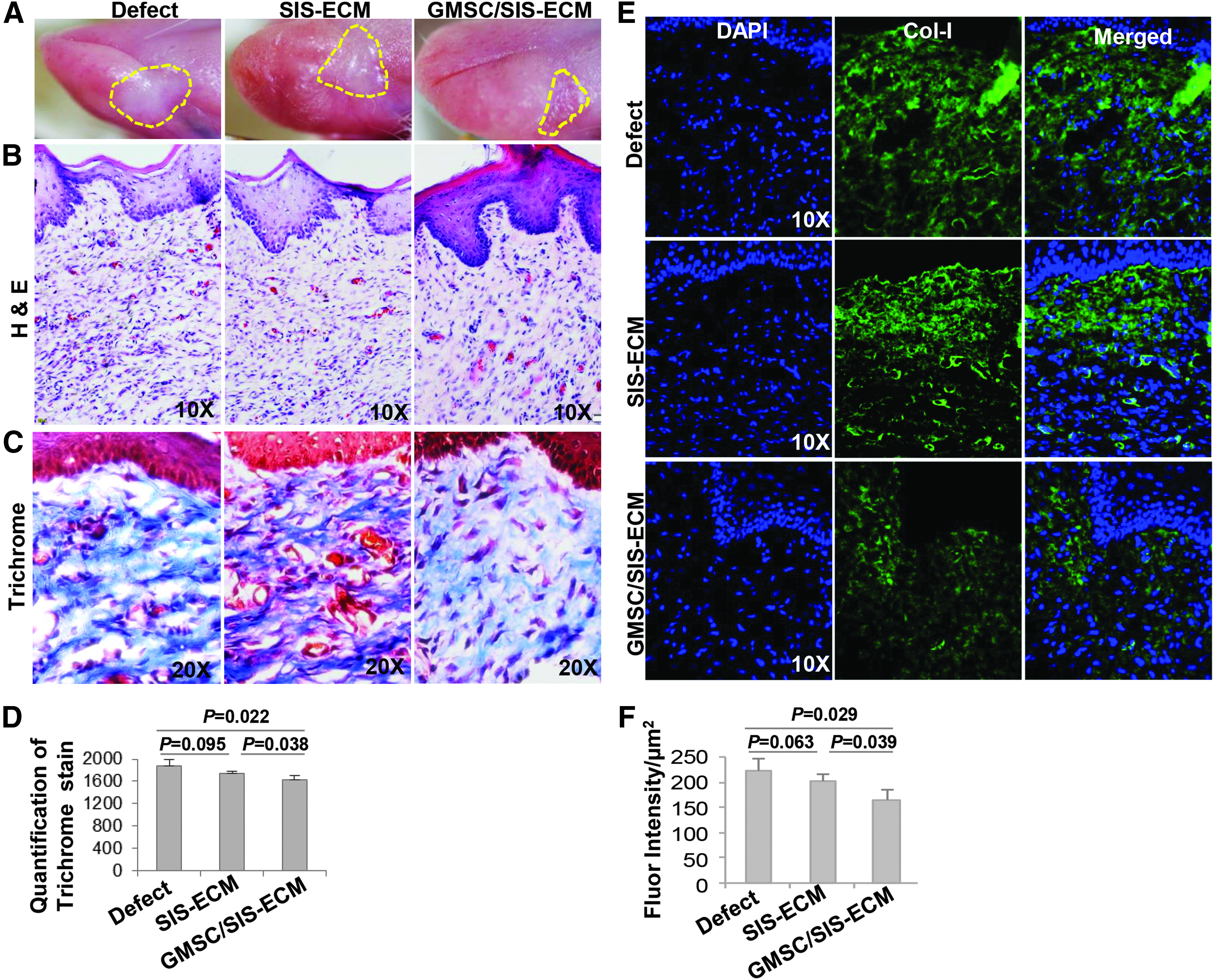
Previous studies have shown that MSCs promote skeletal muscle regeneration and functional recovery by inhibiting fibrosis and remodeling scar tissues.33,48 We then examined the expression of type I collagen in the wounded defect areas of tongue at day 14 following transplantation. The results showed that transplantation of the combinatorial GMSC/SIS-ECM constructs, but not SIS-ECM scaffold alone, significantly suppressed the expression of type I collagen at the wound defect areas (Fig. 5A, B). Trichrome staining of collagens showed similar findings (Fig. 5C, D). These findings were in accordance with the clinical observation showing decreased wound contracture and scar fibrosis at the tongue defect site grafted with the GMSC/SIS-ECM construct (Fig. 1D).

Decreased expression of collagen I in defected tongue areas with transplantation of GMSC/SIS-ECM in comparison with SIS-ECM alone and defect control. Expression of Col-I (green) at local defect area 2 weeks after surgery in control, SIS-ECM only, and GMSC/SIS-ECM construct groups was determined by immunostaining and observed under a fluorescence microscope. The nuclei were counterstained with DAPI
To further determine the anti-fibrotic effects conferred by transplantation of GMSC/SIS, we prolonged our observation up to 4 weeks postsurgery. Clinical morphology of tongue indicated that GMSC/SIS-ECM groups showed much less scarring and wound contracture and maintained the overall tongue shape without deformity compared to the defect control and SIS-ECM scaffold alone groups (Fig. 6A). Histological analysis indicated that GMSC/SIS-ECM group showed apparent muscle regeneration compared with SIS-ECM alone and defect control groups (Fig. 6B). Both trichrome staining (Fig. 6C, D) and immunofluorescence studies (Fig. 6E, F) indicated that GMSC/SIS-ECM group had less collagen deposition and type I collagen expression in defected areas of tongue in comparison to the defect control and SIS-ECM scaffold alone groups.
Decreased expression of collagen I in defected tongue areas with transplantation of GMSC/SIS-ECM in comparison with SIS-ECM alone and defect control.
Altogether, the data suggest that transplantation of GMSC/SIS-ECM constructs not only promote tongue wound healing but also induce muscle regeneration, at least in part, through suppressing the fibrotic process.
Discussion
Reconstruction of tongue defects after ablative surgery of oral cancer remains a major challenge because of the highly specialized and important functions of the tongue. 49 The current “work-horse” option for tongue reconstruction is vascularized-free flaps of soft tissues, which aim to minimize tethering of the tongue while also providing enough tissue bulk. 50 However, these reconstructive modalities have significant limitations and typically result in some degree of life-altering dysfunction in mastication, speech, swallowing, cosmetic deformities, and psychological effects.50,51 The overall lack of tissue-specific donor sites, severe tissue loss, and wound contracture lead to compromised oral function and a major decrease in the quality of life of patients, which then represents an unmet clinical need in patients with benign and malignant neoplasms of the tongue.
In recent years, novel tissue engineering/regenerative medicine (TE/RM) techniques have received increasing attention for reconstruction of volumetric muscle loss.52–54 The TE/RM approaches that aim to restore or reconstruct damaged tissues typically involve the use of cells, bioactive materials, and biologic or synthetic scaffolds. Among all these biological materials, a variety of naturally occurring decellularized extracellular matrix (ECM) scaffold materials have been widely appreciated for the signals and molecules they provided that can augment many aspects of cell behaviors, thus facilitating skeletal muscle reconstruction/regeneration.52,54
The decellularized gastrointestinal small intestine submucosa (SIS) is among the most commonly used acellular scaffolds that display a comparable level of skeletal muscle regenerative capacity to a skeletal muscle-derived decellularized ECM.28,53–55 The pre- and clinical successful use of SIS-ECM in tissue reconstruction might be due to its special three-dimensional ECM structure, 56 components of inherent bioactive molecules, 57 and the biodegradability that can foster its integration with host tissues. 58 In addition, matrix-derived cell signaling molecules, including certain cytokines and growth factors, may play an important role in modulating fibrosis, 20 inflammation,59,60 angiogenesis,13,56,61,62 and other pathophysiological processes that are critical for tissues to initiate an optimal regenerative response.
Although SIS-ECM scaffolds have great advantages for tissue reconstruction in mechanical properties and structural integrity, they have a limited ability on their own to regenerate complex tissue structures such as the tongue. The success of the regenerative process depends upon the extent of initial damage and a myriad of other intrinsic and environmental factors. In the last decade, the introduction of stem cells into TE/RM field has resulted in significant strides in the regeneration of various functional tissues, including functional skeletal muscle. 54 A combinatorial or hybrid construct composed of acellular scaffold and stem cells may represent a new generation of biomaterials for skeletal muscle regeneration. 52
Several lines of evidence have shown an improved regenerative efficacy of the combined use of SIS-ECM and MSCs in a variety of animal models of tissue defects.18,19,20,34–37 Due to their potent multipotent differentiation capability and, more importantly, their secretion of a myriad of trophic factors with diverse biological functions, including immunomodulatory/anti-inflammatory, proliferative/antiapoptotic, proangiogenic, and antifibrotic functions, MSCs represent a promising candidate cell source for tissue regeneration.30,63,64
Under several pathological settings, including skin wound,40,65 fibrotic lung disease, 66 liver fibrosis, 67 and muscle injury,34,48 the antifibrotic effects might be one of the most important machineries by which MSCs promote tissue repair/regeneration. Of note, the mechanisms underlying MSC-mediated anti-fibrotic effects are multiple facets, which may involve their secretion of various anti-inflammatory mediators to inhibit the activation of both innate and adaptive immune cells and boost the function of regulatory T cells and polarization of anti-inflammatory M2 macrophages, thus facilitating the resolution of local inflammation and ultimately alleviating fibrosis. On the contrary, MSCs may directly inhibit myofibroblast activation by secreting a panel of antifibrotic factors to curb the profibrotic signaling pathways, such as TGF-β/Smads.65,66
Recently, we have shown that administration of GMSCs could promote skin wound healing by facilitating the polarization of anti-inflammatory M2 macrophages at the wound site. 40 However, the complicated mechanisms by which MSCs attenuate fibrosis under different pathological settings are still not completely understood. 67
To the best of our knowledge, in the current study, we have shown for the first time that transplantation of combinatorial GMSC/SIS-ECM constructs exhibited better effects on accelerating tongue myomucosal regeneration in rats than transplantation of SIS-ECM alone, which was clinically presented as faster wound closure, less scarring, and less wound contraction. Our results also showed that transplanted GMSCs engrafted in the injured deep muscle layers of the tongue, but only a small portion of them (∼10%) exhibited colocalized signals for positive expression of several key myogenic transcriptional factors, MyoD, Myf5, and PAX7. However, transplantation of combinatorial GMSC/SIS-ECM constructs significantly increased MyoD, Myf5, and PAX7 expression in host skeletal progenitor cells while it decreased the expression of type I collagen at the defected area of the tongue.
In summary, our findings suggest that transplanted GMSCs enhance tongue myomucosal regeneration probably by their anti-fibrotic effects as well as through their indirect paracrine effects on the activity and function of endogenous myoblast progenitor cells. 48 However, further studies are warranted to elucidate the cellular and molecular mechanisms by which GMSCs remodel scar/fibrosis and regulate the function of endogenous myoblast progenitor cells to facilitate tongue regeneration.
Footnotes
Acknowledgments
This study was supported by a research grant from National Institute of Health Research Grant (R01DE 019932, A.D.L.), the Oral and Maxillofacial Surgery Foundation Research Support Grant (to Q.X. and L. Carrasco), OsteoScience Foundation (to Q.Z.), and the Schoenleber funding support (to A.D.L.).
Authors' Contributions
Conception and design: A.D.L., Q.X., Q.Z., B.W.O. Jr.; Acquisition of data: Q.X., Q.Z.; Analysis and interpretation of data: Q.X., R.M.S., Q.Z.; Writing, review, and/or revision of the article: Q.X., R.M.S., Q.Z., S.B.C., B.W.O. Jr., A.D.L.; Study Supervision: A.D.L.
Disclosure Statement
No competing financial interests exist.