
Abstract
The non-union rate after lumbar spinal fusion is potentially as high as 48%. To support efficient bone regeneration, recombinant human bone morphogenetic protein-2 (rhBMP-2) is commonly used as it is regarded as the most potent bone-inducing molecule. However, recently, there have been increasing concerns on the use of rhBMP-2 such as serious complications, including seroma and heterotopic ossification, and the low quality of bone at the center of fusion mass. Thus, many studies were conducted to find and to develop a potential alternative to rhBMP-2. In this study, we investigated the osteogenic potential of tauroursodeoxycholic acid (TUDCA) in the mouse fusion model and compared its effects with rhBMP-2. Twenty-four mice underwent bilateral posterolateral lumbar spinal fusion bone formation at L4-L5. Collagen sponge infused with saline, TUDCA, or rhBMP-2 was implanted at the fusion area. Two and 4 weeks postimplantation, bone formation and tissue regeneration were evaluated via micro-computed tomography and histological analysis. Compared with the TUDCA-treated group, the rhBMP-2 treatment produced a higher amount of bone fusion formation after 2 weeks but also showed higher resorption of the centralized bone after 4 weeks. Interestingly, the TUDCA-treated group developed higher trabecular thickness compared with rhBMP-2 after 4 weeks. Moreover, TUDCA treatment showed distinct angiogenic activity in human umbilical vein endothelial cells as confirmed by an in vitro tube formation assay. Our findings suggest that TUDCA is comparable to rhBMP-2 in supporting bone regeneration and spinal bone formation fusion by increasing trabecular thickness and promoting angiogenesis. Finally, our results indicate that TUDCA can be utilized as a potential alternative to rhBMP-2.
Introduction
S
To prevent non-fusion and support tissue regeneration, several strategies have been conducted, including the augmentation with autologous iliac crest bone grafts (ICBG), and supplementation with bone-inducing growth factors. Although ICBG is the gold standard technique in enhancing bone fusion, it poses several complications, including damage to blood vessels and nerves, joint disruption, fracture, herniation of abdominal contents, and delayed iliac abscess. 8 Moreover, multi-level spinal fusions often require bone grafts that are even larger than what is available in the iliac crest.9–12
Due to these problems, biological augmentation using bone-inducing growth factors have, therefore, received great deal of attention such as the use of recombinant human bone morphogenetic protein-2 (rhBMP-2). In fact, in 2002, the first human trial of rhBMP-2 as spinal fusion adjunct demonstrated a 100% lumbar fusion without the additional internal fixation.13,14 More recently, however, there have been growing concerns about the use of rhBMP-2 because of the low quality of the bone fusion mass and complications such as anterior neck swelling, dysphagia, airway compromise, osteolysis, graft resorption, heterotopic ossification, retrograde ejaculation, radiculitis, pseudoarthrosis, and new onset of cancer.15–28 These problems have encouraged researchers to find and develop better and safer fusion adjuncts that can be used as an alternative to rhBMP-2.
Tauroursodeoxycholic acid (TUDCA), a chemical chaperone, is a commercially available bile acid derivative that has been widely used in treating cholelithiasis and cholestatic liver disease. 29 TUDCA promotes angiogenesis 30 and suppresses adipogenesis 31 when applied to human mesenchymal stem cells (MSCs) both in vitro and in vivo. Studies have shown that bone formation is highly associated with the induction of angiogenesis (enhanced blood, nutrient, and oxygen supply) and suppression of adipogenesis (inversely proportional to osteogenesis).31–33 Also, it has been reported that TUDCA could play crucial roles in preventing cell death as a potent anti-apoptotic and antioxidant agent via modulation of the mitochondrial pathway, the phosphatidylinositol 3-kinase pathway, and nuclear steroid receptors and that TUDCA treatment could improve several disorders, including systemic insulin resistance, hepatic steatosis, spinal cord injury, stroke, and Huntington's disease in preclinical studies.34–37
Clinically, TUDCA is frequently prescribed to patients with cholestatic diseases and usually two capsules (one capsule: 250 mg) are taken per day. From a clinical perspective, TUDCA has many advantages because it is already approved by the Food and Drug Administration (FDA), relatively stable, and inexpensive (about $ 50 for 60 capsules). Therefore, if TUDCA demonstrates effectiveness for spinal bone formation and regeneration, it will be a powerful and promising alternative to rhBMP-2 for bone tissue regeneration and formation. However, the role and underlying mechanism of TUDCA in bone formation, especially spinal bone regeneration, have not been studied. Therefore, we propose that TUDCA can potentially be a safe and effective alternative to rhBMP-2 in promoting bone formation followed by enhancement of spinal bone regeneration. In this study, we investigated the osteogenic potential of TUDCA in a mouse lumbar spinal fusion model and compared it with rhBMP-2.
Materials and Methods
Materials
For the delivery of rhBMP-2 (ProSpec-Tany TechnoGene, Rehovot, Israel) and TUDCA (Calbiochem, San Diego, CA), collagen sponge (CollaCote®; Zimmer Dental Inc., Carlsbad, CA) was utilized as an absorbable matrix scaffold. The collagen sponge (2 mm [W] × 7 mm [L] × 2 mm [H]) impregnated with rhBMP-2 (3 μg/30 μL) or TUDCA (300 μg/30 μL) solution was applied bilaterally to decorticated sites.
Surgical procedure
All animal procedures were performed in accordance with the protocol approved by the Institutional Animal Care and Use Committee (IACUC) of CHA University (IACUC150003). A total of 27 female ICR mice (10-week-old and 22–24 g) were purchased from Orient Bio, Inc. (Seongnam, Korea) and were raised at 55–65% humidity and a controlled temperature of 24°C ± 3°C with a light/dark cycle of 12 h. Mice had free access to food and tap water ad libitum. All mice underwent posterolateral lumbar spinal fusion with implantation of saline, rhBMP-2, or TUDCA-impregnated collagen sponges. Namely, the animals were randomly divided into four experimental groups: Group 1 received decortication only (n = 6), Group 2 received 30 μL saline-soaked collagen sponges bilaterally (n = 7), Group 3 received 3 μg/30 μL rhBMP-2-impregnated collagen sponges bilaterally (n = 7), and Group 4 received 300 μg/30 μL TUDCA-impregnated collagen sponges bilaterally (n = 7).
Surgery was performed by one experienced surgeon (B.J.K.) in a single sitting. The animals were anesthetized with Zoletil® (50 mg/kg; Virbac Laboratories, France)/Rompun® (10 mg/kg; Bayer, Korea) solution administered intramuscularly. Hair overlying the surgical site was shaved once mice were anesthetized, and the surgical site was prepped with povidone-iodine and 70% ethanol. Animals were positioned prone with folded gauze beneath the abdomen, increasing the excursion of the lumbar spine to facilitate access to and visibility of the surgical field. Aseptic technique was utilized for all surgical procedures. Posterolateral inter-transverse lumbar fusion at L4-L5 was performed as described in a prior study. 38 Briefly, the L5-L6 interspace was identified by using the iliac crest as a landmark. A 15 mm midline longitudinal incision was made through the skin and subcutaneous tissue over L4-L5 down to the lumbodorsal fascia. A second 15 mm incision, through the dorsolumbar fascia, was made in the midline, along the spinous processes.
The lumbar paravertebral muscles overlying the articular processes of L4-L5 were separated from the spinous processes in a single motion by scraping a #10 blade down the lateral border of the spinous process and pulling the muscle laterally. This was performed by bilaterally exposing the articular processes, and a pneumatic 1 mm diamond burr was used to decorticate the articular processes until punctate bleeding was observed (Fig. 1). The surgical site was irrigated with sterile saline, and then 30 μL sterile saline, 3 μg/30 μL rhBMP-2, or 300 μg/30 μL TUDCA was impregnated into a piece of collagen matrix (2 mm [W] × 7 mm [L] × 2 mm [H]), and subsequently placed over the bilateral decorticated transverse processes on each site. Sutures were used to enhance the internal fixation stability. After surgeries, all animals were housed individually and were monitored closely. All animals were euthanized by using carbon monoxide inhalation 4 weeks after implantation, and their spines were excised for evaluations.

Mouse model of posterolateral inter-transverse lumbar fusion.
Micro-computed tomography analysis
The microstructural morphology of the lumbar spines was evaluated by using a Skyscan 1076 micro-computed tomography (micro-CT) device (Skyscan, Kontich, Belgium) at 2 and 4 weeks after implantation. The X-ray source was set to a voxel size of 18 μm at 40 keV and 250 μA. Exposure time was 520 ms with a frame average of 3. X-ray beam filtration made of 1 mm aluminum was used. 39 Data were recorded at every 0.4° of the rotation step until 180°. Image slices were reconstructed by using the NRecon software (Skyscan) based on the Fledkamp algorithm, and by applying correction for the beam. For the purposes of bone volume (BV) and density calculation, the new bone mass was isolated from native bone by means of a manually drawn region of interest (ROI). The outline of ROIs was manually drawn by using CT-Analyser 3D data analysis software (Skyscan); care was taken not to select outgrowing mineralized osteophytes. Spinal fusion was defined as the presence of bridging bone between the L4 and L5 transverse processes. The reconstructed three-dimensional (3D) images were judged as fused or not fused by two experienced independent observers. To quantify the density of bone formed within each new mass, the tissue volume (TV) of the mass, trabecular BV within the mass, and percent BV (BV/TV, %) were calculated. In addition, trabecular thickness (Tb.Th mm), trabecular number (Tb. N 1/mm), and trabecular separation (Tb.Sp mm) were calculated.
Histological analysis
After micro-CT scanning, lumbar spines were decalcified by using decalcification solution (National Diagnostics, Atlanta, GA), the tissues were placed in a dehydrated graded series of ethanol and xylene and embedded in paraffin, and axial sections (4 μm thickness) were obtained. The sections were stained with hematoxylin and eosin (H&E) stain and Masson's trichrome stain to demonstrate new bone formation. For immunohistochemistry, the axial sections were incubated for 10 min at room temperature (Golden Bridge International, Inc., Mukilteo, WA). Endogenous peroxidase blocking was done with 1% H2O2 for 20 min at room temperature. The samples were incubated with blocking solution (Vector Laboratories, Burlingame, CA) for 30 min at room temperature. Primary antibody to osteocalcin (Santa Cruz Biotechnology, CA) was used at 1:100, and biotin-conjugated anti-IgG secondary antibody was used at 1:200. The peroxidase-conjugated avidin system was used according to the manufacturer's instructions (Vector Laboratories). The immunostained samples were counterstained with Mayer hematoxylin (Sigma, MO).
Biomechanical testing
Biomechanical force of the transplanted L4-L5 segment was evaluated by applying a downward force perpendicular to the longitudinal axis of the mouse spine. To do this, the L3–L6 segments of each specimen were analyzed via a three-point bending test by using an Instron testing machine (H50KT; Instron, MA) to compare the bending stiffness among these three groups: (1) Sham group, (2) TUDCA treatment group, and (3) rhBMP-2 treatment group. Both ends of the L3–L6 segment were placed with their ventral sides positioned down onto two fulcrums. A compressive force was then applied to the dorsal surface of the longitudinal spine via a rod steel of load cell. Three-point bending tests were performed with a 19-mm inter-support distance and a 50-mm/min head speed. The load-deflection curves of each specimen were obtained in each group, and the compressive forces of each displacement were statistically compared.
Tube formation assay
Forty-eight-well tissue culture plates were coated with 100 μL of Matrigel (BD Biosciences). The 4 × 104 of human umbilical vein endothelial cells (HUVEC) were seeded on the culture plate and 150 μL of endothelial basal medium-2 supplemented with 1% fetal bovine serum and vascular endothelial growth factor was the only growth factor. Cells were then treated with vehicle control, rhBMP-2 (1 or 3 μg), or TUDCA (1 or 3 μg) for 24 h at 37°C. Each condition was repeated at least two times in triplicate.
Statistical analysis
Experimental results are reported as means ± standard deviations. Statistical analysis was performed by using the SPSS program (version 12.0; IBM, NY). Student's t-test was used to evaluate differences between experimental groups. One-way analysis of variance (ANOVA) with the Tukey's post hoc test was used for analysis of micro-CT data. p-Values less than 0.05 were regarded as statistically significant.
Results
rhBMP-2 or TUDCA solution was impregnated into scaffolds and successfully administrated without loss of solution. The scaffolds were stuck to the injury site without any technical problems (Fig. 1). After surgery, there was no intra- or postoperative morbidity or mortality and no animals were excluded from the experiments conducted in this study.
Three-dimensional micro-CT analysis
According to 3D micro-CT evaluation of complete reconstructions and axial sectional cuts (Fig. 2), new bone formation was not found in the decortications-only procedure (Group 1, sham) at 2 and 4 weeks after implantation. In addition, the collagen sponge with saline treatment did not show new bone formation (Group 2), demonstrating that the collagen sponge is hardly able to induce bone formation without other osteogenic factors. On the other hand, a large volume of new bone was observed in both collagen sponges with rhBMP-2 treatment (Group 3) and TUDCA treatment (Group 4). This was also supported by 3D architecture of micro-CT images in all of the ROIs (Fig. 3). Interestingly, however, at 4 weeks after implantation, both rhBMP-2 and TUDCA treatment showed a decrease in the size of the newly formed bone at the center of the mass, presumably due to bone resorption. Compared with rhBMP-2 treatment (Group 3), TUDCA treatment (Group 4) exhibited a lower level of new bone formation (Figs. 2 and 3).

Three-dimensional reconstructed image and cross-section image of micro-CT at 2 and 4 weeks. The mice are divided into four groups (sham, collagen sponge+sterile saline, collagen sponge+rhBMP-2, collagen sponge+TUDCA). White dotted line, on the other hand indicates the location where the spine was crossed sectioned. The cross-sectioned images of the ROI (framed white circle) were analyzed by bone histomorphometry. White triangles show grafted collagen sponge+rhBMP-2 and collagen sponge+TUDCA. CT, computed tomography; ROI, region of interest.
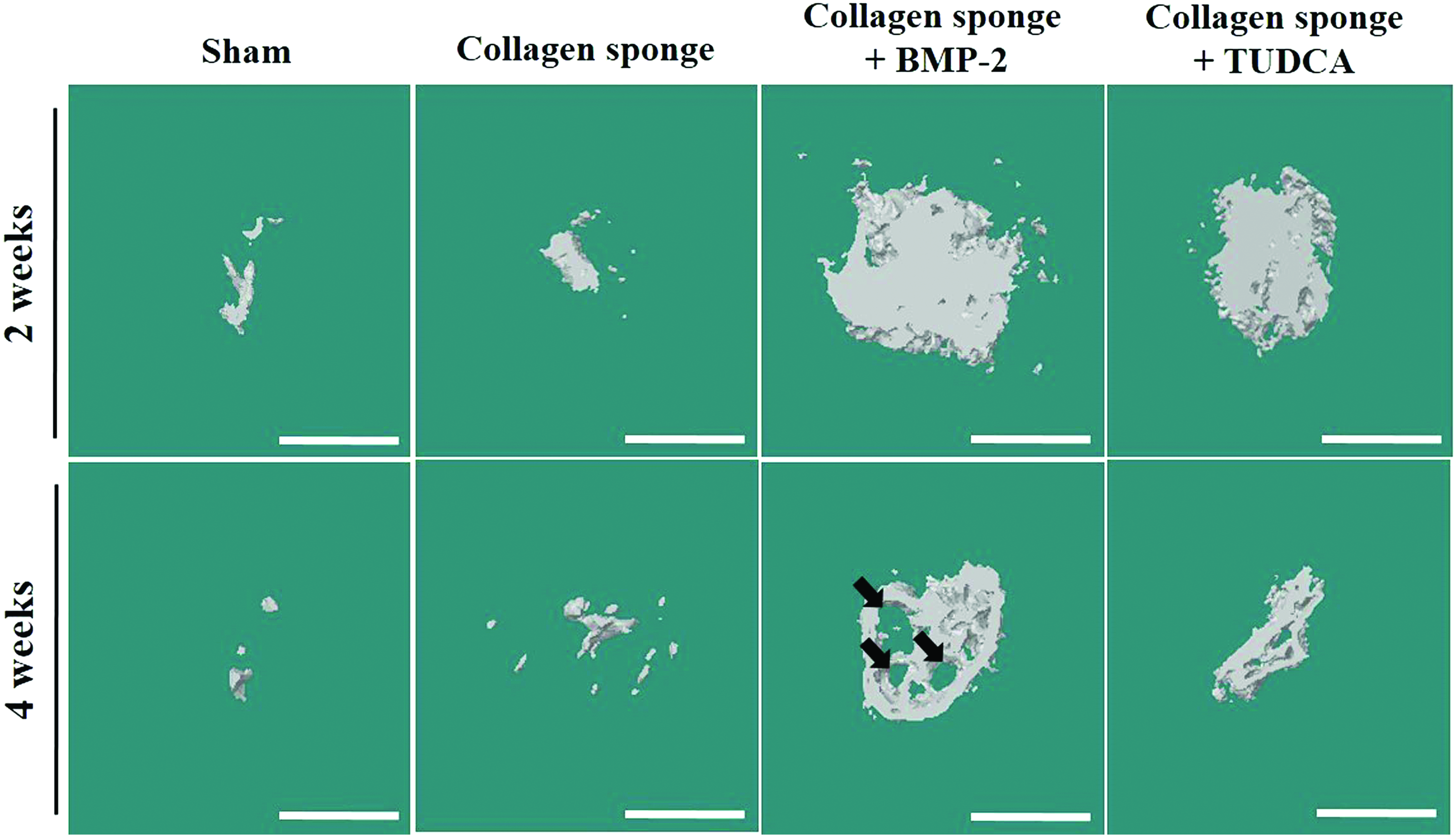
Three-dimensional architecture of rendering obtained from micro-CT image of all the ROIs. Representative 3D architecture in vivo micro-CT analysis of an ROI incorporating 20 lines (360 μm) starting from the L4 to the L5. The cross-sectioned images of the ROI (Fig. 2, framed white circle) were analyzed by bone histomorphometry. Black arrows indicate bone resorption. Scale bar 1 mm. 3D, three-dimensional. Color images available online at www.liebertpub.com/tea
Based on micro-CT images, the new bone formation was evaluated by many parameters such as percent bone volume (BV/TV, %), trabecular thickness (Tb.Th), trabecular number (Tb.N), and trabecular separation (Tb.Sp) (Fig. 4). The percent volume of new bone formation with the rhBMP-2 treatment (Group 3) was 33.1% ± 10.3%, that is, significantly greater than 13.6% ± 1.9% with TUDCA treatment (Group 4) with 2 weeks after implantation (Fig. 4A). With 4 weeks after implantation, new bone formation was also higher with rhBMP-2 treatment (16.1% ± 4.8%) than with TUDCA treatment (6.2% ± 3.2%). This demonstrates that rhBMP-2 is able to induce in vivo bone formation to a higher degree than TUDCA. Surprisingly, trabecular thickness with TUDCA treatment (0.16 ± 0.03 mm) was significantly higher than with rhBMP-2 treatment (0.12 ± 0.04 mm) (Fig. 4B). However, trabecular number (Tb.N, the number of trabeculae in a unit length) was significantly higher with rhBMP-2 treatment (Group 3) than with TUDCA treatment (Group 4) (Fig. 4C). Interestingly, the amount of new bone formation, trabecular number, and trabecular thickness with both rhBMP-2 and TUDCA treatment was decreased at 4 weeks after implantation compared with 2 weeks. These are probably due to bone resorption, which happens with newly formed bone tissue after in vivo implantation. On the other hand, trabecular separation (Tb.Sp) representing the non-bone part of ROI showed no statistically significant difference between rhBMP-2 treatment and TUDCA treatment (Fig. 4D, p > 0.1).
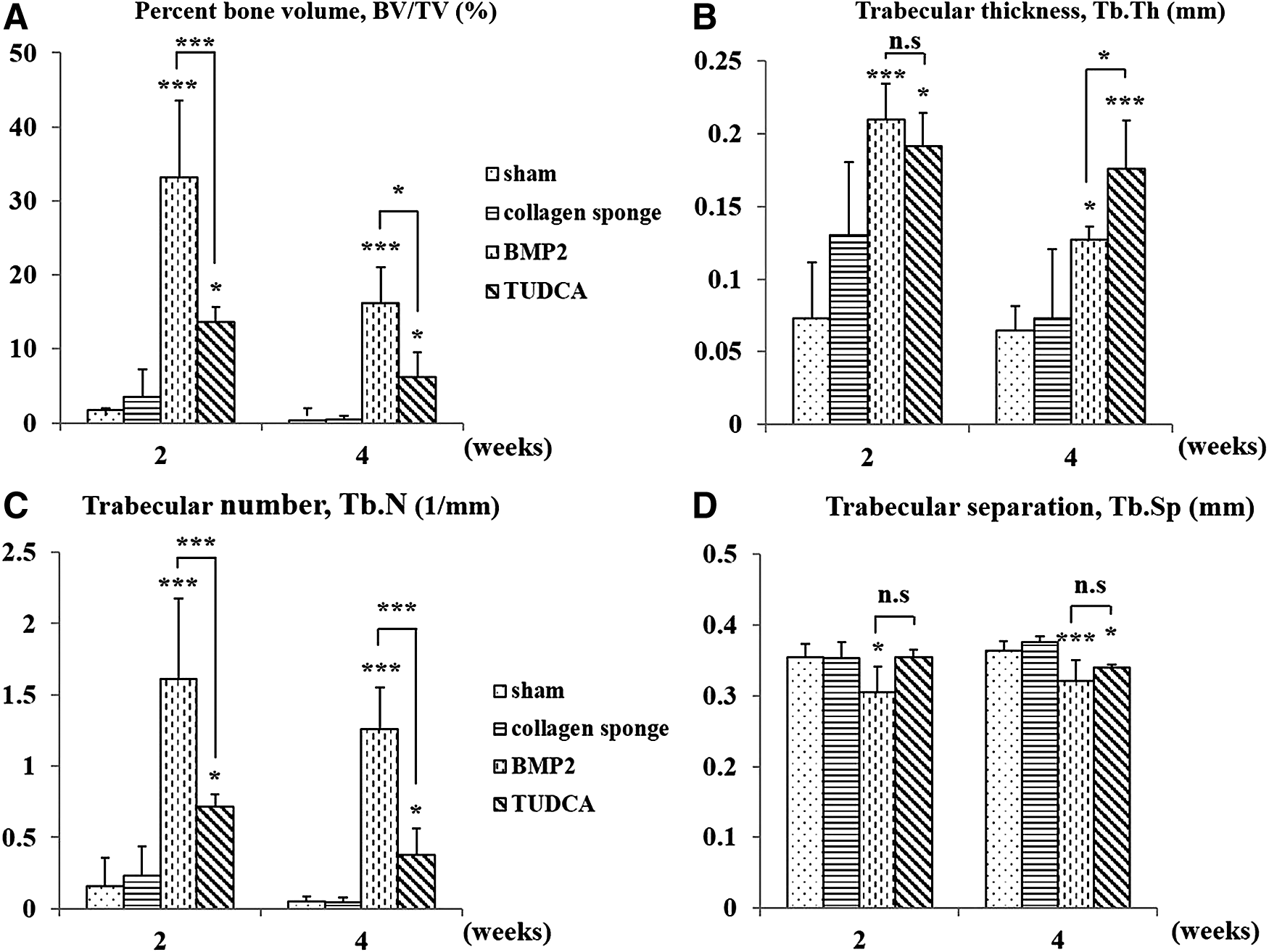
Bone histomorphometry of the 3D bone formation architecture analyzed in an ROI of all groups. Plots of the parameters: percent bone volume (BV/TV, %)
Histological evaluation
Histological analysis revealed a similar trend to the findings with the micro-CT image analysis. H&E staining, Masson trichrome staining, and osteocalcin staining were carried out to evaluate new bone formation at 4 weeks of implantation. As shown in Figure 5, rhBMP-2 treatment (Group 3) and TUDCA treatment (Group 4) distinctly induced new bone formation (large black arrows) and blood vessels (red arrowheads) representing angiogenesis compared with decortications-only (Group 1, sham) and the decortications-only/saline treatment (Group 2). Compared with TUDCA treatment (Group 4), rhBMP-2 treatment (Group 3) produced higher new bone tissue formation. However, rhBMP-2 treatment also induced numerous adipocytes showing lipid droplets (Fig. 5, small yellow arrows) at the center of newly formed bone tissue. According to Masson trichrome staining and osteocalcin staining, interestingly, TUDCA treatment showed mature osteoblasts and bone matrix deposition without adipocyte formation and further enhanced blood vessel formation (Fig. 5, red arrowheads).

Histological analysis of fused murine vertebrae. Histological sections of the area between L4 and L5 were stained with H&E, Masson's trichrome and immunohistochemistry for osteocalcin was performed at 4 weeks after transplantation. Rectangle boxes indicate the implant area. Large black arrows indicate new bone, small yellow arrows indicate adipocytes, and red arrowheads indicate blood vessels. Scale bar = 400 μm. H&E, hematoxylin and eosin. Color images available online at www.liebertpub.com/tea
Biomechanical evaluation
To evaluate the biomechanical property of newly formed bone mass in posterolateral spinal fusion by using rhBMP-2 treatment and TUDCA treatment, L3–L6 specimens were isolated from each mouse 4 weeks postimplantation. Then, a three-point bending test was performed (Fig. 6A). Results shown in Figure 6B demonstrated that there was no difference in the initial slopes among the sham, rhBMP-2, and TUDCA-treated groups. However, when the displacement was increased to more than 6 mm, both the rhBMP-2 and TUDCA treatment groups showed a significant increase in strength compared with the sham (control) group. Interestingly, the biomechanical property of newly formed bone masses in both rhBMP-2 treatment and TUDCA treatment groups did not show any significant difference (Fig. 6B).

Biomechanical test of new bone mass. Spinal bone masses at 4 weeks were evaluated a biomechanical force by a three-point bending test.
Tube formation
To investigate whether rhBMP-2 or TUDCA is able to stimulate tube formation, HUVECs were seeded onto Matrigel-coated plates and then treated with control medium, rhBMP-2, or TUDCA. A low concentration (1 μg/well) of rhBMP-2 and TUDCA treatment exhibited no significant difference compared with the control group (Fig. 7A). However, a high concentration (3 μg/well) of TUDCA exhibited tube formation significantly higher than other groups, demonstrating that a high concentration of TUDCA would be able to stimulate angiogenic activity of HUVEC.

Angiogenic activity of rhBMP-2 and TUDCA. TUDCA stimulates tube formation of endothelial cells.
Discussion
Non-union after spinal fusion surgery is a very important issue. rhBMP-2 is the only identified powerful protein molecule that is capable of strongly inducing bone formation. Its approval by the FDA suggests that rhBMP-2 reliably induces bone formation with few, if any, device-related adverse events. 40 It has been reported that the national rate of BMP application in spinal fusion cases is increasing.41–43 However, it is possible that rhBMP-2 induces a strong inflammatory reaction in surrounding tissue, and it stimulates osteolysis, ectopic bone formation, and bone overgrowth, causing nerve impingement, radiculopathy, and other adverse events.15–28 Recently, another large concern is that rhBMP-2 sometimes induces low-quality bone in the fusion mass because rhBMP-2 treatment can induce the formation of cyst-like bone voids filled with fatty marrow rather than normal trabecular dense bone structures.22,44–46 Thus, rhBMP-2 could promote lower quality bone with an abnormal structure, potentially resulting in inferior mechanical properties. In addition, the low stability and high cost of rhBMP-2 are large concerns for its clinical applications.41,43,45,47,48 The low stability of rhBMP-2 means its activity deteriorates, and the high cost of rhBMP-2 is a burden to patients as well as healthcare providers. 32 Therefore, many attempts have been made to develop an alternative to rhBMP-2 that has stable activity and is inexpensive to enhance the formation of high-quality bone and spinal fusion.
In this study, we evaluated whether TUDCA, as an alternative to rhBMP-2, can induce bone tissue formation followed by spinal bone regeneration after in vivo implantation. In a mouse model, new bone tissue formation and spinal bone regeneration were significantly increased by both rhBMP-2 treatment and TUDCA treatment at 2 weeks postimplantation. rhBMP-2 treatment induced a higher amount of new bone formation than TUDCA treatment, demonstrating that rhBMP-2 is more powerful than TUDCA for bone tissue regeneration (Figs. 2 and 3). At 4 weeks postimplantation, histology and micro-CT analysis showed a decrease in bone mass in both groups (Fig. 4). Although the rhBMP-2-treated spine exhibited bony overgrowth at 2 weeks postimplantation, extensive bone resorption of the new bone mass resulted in a decrease in new bone, which was observed at 4 weeks (Fig. 4). It has been reported that BMPs can regulate both bone formation and resorption simultaneously.49–52 Several studies reported that a high dose of rhBMP-2 induces transient bone resorption in vivo.49,53 However, it is unclear which mechanism underlies this bone resorption by BMPs. In this study, bone resorption was more extensive on rhBMP-2 treatment than on TUDCA treatment. On rhBMP-2 treatment, trabecular BV and trabecular thickness were statistically significantly lower at 4 weeks postimplantation than at 2 weeks postimplantation (BV/TV [p* = 0.0439], Tb.Th [p*** = 0.0039]). However, TUDCA-treatment also decreased these parameters, although not statistically significantly (BV/TV [p = 0.1278], Tb.Th [p = 0.2025]). The more extensive centralized bone resorption with rhBMP-2 treatment may be associated with the fact that BMP-2 induces adipogenesis simultaneously during new bone formation. This is coincident with previous studies reporting that rhBMP-2 is a factor that promotes both osteogenesis and adipogenesis.54,55
As shown in Figure 5, rhBMP-2 treatment induced adipose tissue formation with lipid droplets (small yellow arrows) and angiogenesis (red arrowheads) at the center of the new bone mass, whereas TUDCA treatment induced bone tissue formation with angiogenesis but without adipose tissue formation. It was reported that BMP-2 signaling can stimulate adipogenesis not only through activation of adipogenic transcription factors such as peroxisome proliferator-activated receptor gamma (PPARγ), a key regulator of adipocyte commitment, but also through repression of the Wnt signaling pathway, which is known to downregulate adipogenesis.44,56,57 Herein, it was not surprising that trabecular thickness, representing the quality of bone formed, was significantly higher on TUDCA treatment than on rhBMP-2 treatment (Fig. 4B). Taking these results together, it is concluded that TUDCA treatment is more beneficial for the formation of high-quality dense-bone tissue without adipose tissue formation, although it is not as powerful as rhBMP-2 in terms of the volume of bone formed. In addition, it was revealed that bone TUDCA treatment showed higher biomechanical strength of bone formation than sham and that was comparable to rhBMP-2 treatment (Fig. 6).
Our previous study reported that TUDCA can significantly decrease adipogenic differentiation of MSCs both in vitro and in vivo by attenuating the expression of PPARγ through modulation of endoplasmic reticulum stress. 31 In addition, Cho et al. reported that TUDCA could play critical roles in promoting neovascularization by enhancing the mobilization of stem/progenitor cells from bone marrow, their differentiation into endothelial progenitor cells, and their integration with preexisting endothelial cells. 30 As shown in Figure 7, TUDCA treatment increased tube formation of HUVECs, representing angiogenic activity, whereas rhBMP-2 treatment did not. In addition, this angiogenic activity is increased at a higher concentration of TUDCA. Cho et al. reported that TUDCA treatment increased tube formation in a dose-dependent manner. 30 TUDCA can promote angiogenesis and suppress adipogenesis in vitro. Thus, it is highly possible that TUDCA promotes in vivo bone tissue regeneration by enhancing angiogenesis and by suppressing adipogenesis because angiogenesis and inhibition of adipogenesis play pivotal roles in stimulating osteogenesis of stem cells followed by bone tissue formation.
In this study, we sought to investigate whether TUDCA can promote spinal bone formation in a mouse model and compared it with rhBMP-2. At 4 weeks postimplantation, TUDCA treatment stably maintained trabecular thickness with dense bone in comparison to rhBMP-2 treatment (Fig. 4B). Histological evaluation also showed that TUDCA treatment induced the formation of higher quality bone without adipose tissue formation in comparison to rhBMP-2 treatment (Fig. 5). Thus, we believe that TUDCA is a good biological to induce spinal bone regeneration and is superior to rhBMP-2. In conclusion, TUDCA could be widely used as a useful alternative to rhBMP-2 for spinal bone formation and bone tissue regeneration.
Footnotes
Acknowledgments
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant No. HI14C3270, HI16C0106, HI16C1559) and by the National Research Foundation of Korea (NRF) funded by the Korea government (MSIT) (NRF-2016R1D1A1B03931554).
Disclosure Statement
No competing financial interests exist.