
Abstract
Advanced biomaterials that are capable of guiding robust bone regeneration are highly demanded for translational therapy of bone defects or bone augmentation in clinics. One of the strategic approaches is to produce tissue engineering (TE) constructs that mediate bone regeneration by recapitulating the natural bone formation or healing process. In this study, we aimed at producing devitalized mineralized carriers with augmented bone forming capacity via a modified culture protocol (i.e., culture conditions with high calcium and/or phosphate concentrations) that first promotes cell growth and, subsequently, mineralized extracellular matrix (ECM) deposition by human periosteum-derived osteoprogenitor cells (hPDCs) on additive manufactured three-dimensional (3D) porous titanium (Ti)-based scaffolds. Qualitative and quantitative analysis was performed to characterize the physicochemical properties of the produced devitalized mineralized carriers, as well as their effects as carriers on in vitro cell growth and osteochondrogenic differentiation of hPDCs under a perfusion bioreactor culture set-up. The results showed that the modified culture protocol was useful to produce devitalized mineralized carriers with different amount, distribution, composition, and morphology of mineralized matrix that resembled hydroxyapatite, and exhibited different Ca2+ release kinetics, distinct human bone morphogenetic protein (hBMP)-2, human vascular endothelial growth factor (hVEGF) proteins, and collagen contents. The produced devitalized mineralized carriers supported 3D growth of hPDCs, with minor osteochondrogenic differentiation effects under the perfusion bioreactor culture condition. Subcutaneous implantation of hPDC-seeded devitalized mineralized carriers in athymic nude rats showed nearly five-fold augmentation in the ectopic bone-forming capacity, with no bone induction obtained for unseeded, devitalized mineralized carriers and plain Ti scaffolds. Implantation of devitalized mineralized carriers in critical-sized calvarial defects resulted in encouraging defect bridging as compared with limited defect bridging by plain Ti scaffolds or in empty defects. This defect bridging was not enhanced by implanting hPDC-seeded devitalized mineralized carriers. In conclusion, the investigated modified culture protocol was useful to produce devitalized mineralized carriers with augmented bone-forming capacity, which potentially could aid bone repair or augmentation in clinics.
Introduction
P
Indeed, in vitro cell culture-derived ECM offers attractive advantages over synthetic or naturally derived bone substitutes. 10 In particular, it consists of cell-secreted molecules that are readily bioactive and has presumably been assembled within the correct biological context such as the matrix architecture and composition. The ECM may also contain essential ECM-bound bone-inducing growth factors such as bone morphogenetic proteins (BMPs) or vascular endothelial growth factor (VEGF), depending on the cell type used. Moreover, native ECM is known to play a fundamental role in coordinating growth factor activity in vivo. Therefore, it can serve as an ideal controlled delivery system for growth factors to promote bone regeneration. 11
Hence, ECM-based TE constructs may possess higher regenerative potency (e.g., as compared with synthetic constructs), especially when confronting challenging clinical scenarios such as atrophic nonunions, large bone defects, and an illness-associated compromised defect environment. It also offers feasibility to prefabricate TE constructs for spontaneous clinical demands and to customize for patient-specific requirements (e.g., based on the defect geometry, disease background, and the age- and defect location-dependent ECM matched). Nevertheless, the current lack of a robust methodology to produce such ECM-based TE constructs with a high bone-inducing capacity has limited their clinical applicability. Therefore, substantial research efforts are still required in this field, especially in identifying the critical bone regeneration determinants and, subsequently, their translation into in vitro methodology that produces ECM-based bone-repairing constructs with excellent clinically relevant attributes. 12
It is known that periosteal cells play a crucial role in bone fracture healing via callus formation due to their remarkable regenerative capacity and bipotency in osteogenic and chondrogenic differentiation.13,14 By harnessing the body's own healing potential, periosteum-based bone substitutes can be tuned for diverse clinical scenarios and regenerative medicine approaches. 15 Therefore, osteochondroprogenitors derived from human periosteal (defined as human periosteum-derived cells, hPDCs) represent a promising stem cell source 16 and are often used to promote bone regeneration by seeding on mineralized or calcium phosphate-based biomaterials.17,18 Interestingly, removal of the mineralized component from the biomaterials by decalcification abrogated ectopic bone formation by hPDCs.19,20 This indicated that the ectopic bone-forming capacity of hPDCs is dependent on the presence of a mineralized component within the cell-biomaterial configuration.
One of our strategic bone regeneration approaches is to establish research protocols that activate, expand, and differentiate hPDCs to build a mineralized ECM-based 3D biotemplate that guides bone regeneration. For this, we developed a novel direct mineralizing culture protocol to produce devitalized mineralized carriers by surface functionalization of a 3D porous titanium-based (Ti) scaffold with hPDC-deposited mineralized ECM. We recently reported the proof of principle of ectopic bone induction by these devitalized mineralized carriers (in combination with hPDCs). 21 This direct mineralizing culture protocol was based on simultaneous calcium (Ca) and phosphate (P) supplementation in culture medium to directly provoke active culture mineralization. However, the percentage of bone induced was far from trivial for clinical applications (<1% based on the calculated bone volume per total scaffold void volume of 64.8 mm3), an observation that we believe was attributed to a low amount of deposited mineralized ECM due to direct induction of culture mineralization that limited further cell growth and ECM deposition.
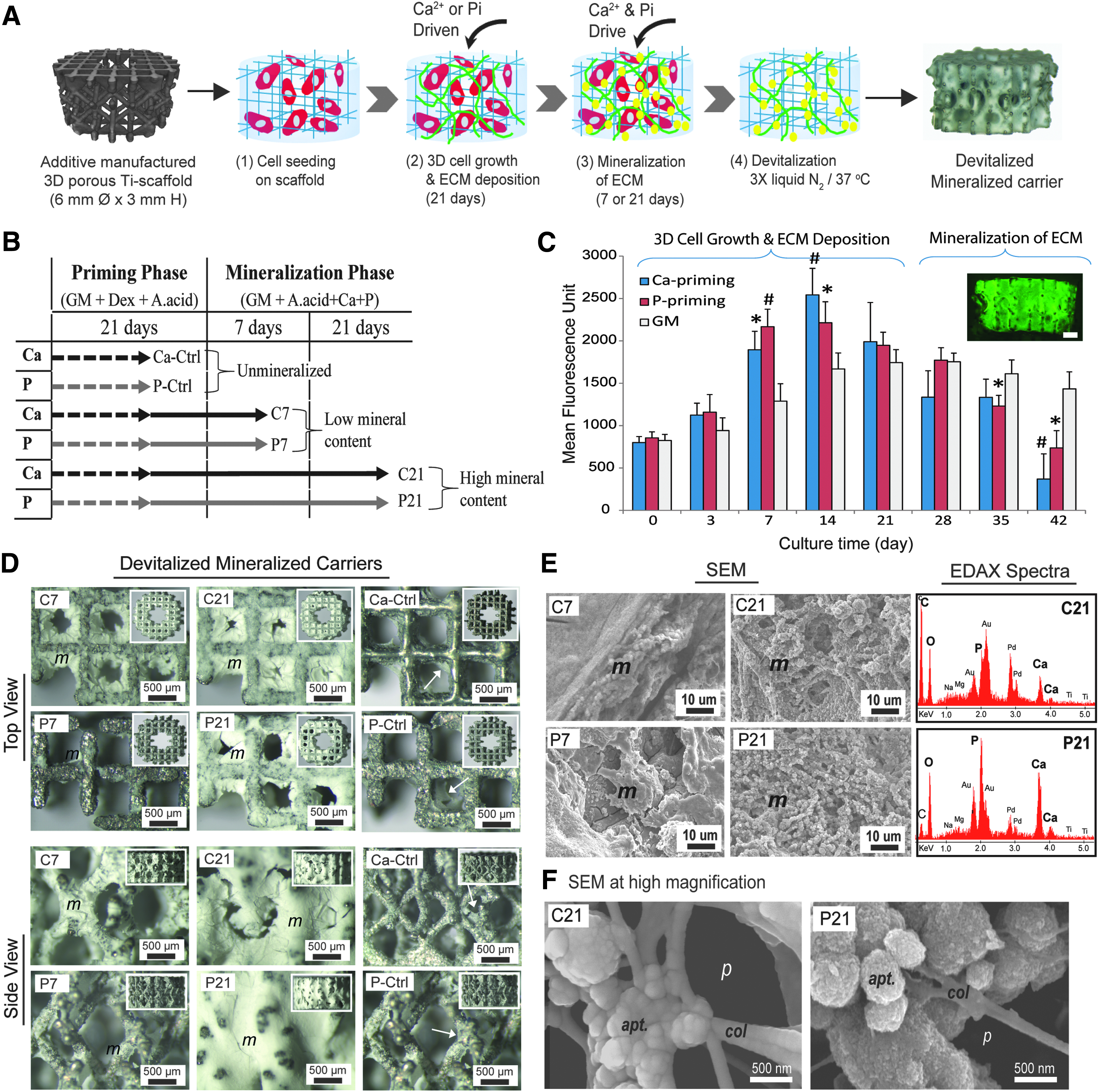
In this study, we aimed at augmenting the bone-forming capacity of these mineralized carriers by subjecting them to a modified culture protocol that combined the direct mineralizing culture protocol with a previously reported priming culture condition. This priming culture condition was based on single-ion (either Ca or P ion) supplementation in culture medium to boost high cell proliferation and osteoid matrix formation before initiating active mineralization 22 (Fig. 1A). Our hypothesis was that promoting a higher amount of cell-made mineralized ECM deposition on prefabricated porous Ti scaffolds would produce 3D porous devitalized mineralized carriers that are capable of inducing clinically relevant bone formation. This hypothesis was assessed through the production of carriers with relatively low and high mineral contents by varying the mineralization culture duration (7 or 21 days) with regard to the initial Ca- or P-priming condition.
Several key properties of the mineralized ECM that have been reported to be the crucial key factors for the bone induction property of calcium phosphate-based biomaterials23,24 were characterized and analyzed for their effects on the bone-forming capacity by using subcutaneous and critical-sized calvarial defect models in athymic nude rats. The need for future onsite delivery of autologous or allogeneic progenitor cells to patients when using these carriers was addressed by implanting carriers that were seeded either with or without hPDCs.
Materials and Methods
Production of devitalized mineralized carriers using the modified culture protocols
Three-dimensional porous, cylindrical Ti scaffolds (6 mm diameter × 3 mm height; with 2 mm center hollow channel) were fabricated by additive manufacturing (i.e., selective laser melting, SLM), then cleaned, and finally oxidized before subsequent experiments as previously described. 25 These Ti scaffolds were reported to have an average strut thickness of 256.1 ± 7.4 μm, a pore size of 821.8 ± 6.4 μm, porosity of 80.6%, total strut surface area of 2.4 ± 0.09 cm2, and a total void volume of 64.8 ± 2.0 mm3. 22 Human periosteum-derived cells (hPDCs) were isolated from periosteum biopsies that were obtained from patients undergoing total knee replacement surgery or distraction osteogenesis with informed consent and approval by the ethics committee for Human Medical Research of the KU Leuven, as previously described. 26
The cells were expanded in T-175 flasks in growth medium (GM) comprising DMEMGlutaMax−1 (Gibco) + 10% fetal bovine serum (FBS; Gibco) + 1% antibiotics/antimycotics + 1% sodium pyruvate. Expanded cells at different passages were stored in liquid nitrogen. In this study, hPDCs of passage 5 were thawed from liquid nitrogen and expanded in GM. Before cell seeding, sterilized Ti scaffolds were incubated in GM for 1 h and then dried in laminar flow overnight under sterile condition. After reaching confluence, the cells were harvested, and 40 μL of a cell suspension containing 200,000 hPDCs was drop seeded onto each scaffold. They were then incubated for 1 h in a cell culture incubator before they were transferred onto a Mini LabRoller rotator (Labnet Int., Inc.) to perform dynamic rotational seeding overnight as described in a previous study. 22
Subsequently, the samples were transferred to 24-well plates and cultured in GM for 24 h by using a 3D platform rotator (30 rpm; Grant-Bio). Then, the cell cultures were treated with the priming culture condition, that is, GM supplemented with Ascorbic Acid (50 μg mL−1), Dexamethasone (100 nM), and either 6 mM of Ca (the Ca-priming) or 4 mM of PO43− (the P-priming) to promote cell proliferation and osteogenic ECM formation over a duration of 21 days. This was followed by the treatment in direct mineralizing culture conditions: in GM supplemented with Ascorbic Acid (50 μg mL−1), and 6 mM of Ca and 4 mM of P to initiate active mineralization of the ECM for either 7 or 21 days, respectively. For both treatment stages, the media were refreshed twice a week. Cell growth during the entire treatment regime was monitored by measuring the metabolic activity of each sample (n = 16 per group; duplicate measurements) by using the PrestoBlue® Cell Viability Reagent (Life Technologies) at defined time points according to the manufacturer's instructions. Samples that were cultured in GM were used as negative controls.
In addition, cell viability on the scaffold was assessed by using a Live/Dead® cell viability kit (Invitrogen). After 28 or 42 days of treatment, the samples were rinsed with PBS twice and transferred to Eppendorf tubes containing 1 mL of sterile demineralized water for storage at −80°C to preserve the deposited biological integrity. Before subsequent experiments, the samples were subjected to three freeze-thaw cycles between liquid nitrogen and 37°C in a water bath under sterile condition and then dried under laminar flow overnight to produce the devitalized, mineralized carriers with relatively low (designated as C7 or P7) or high (designated as C21 and P21) mineral contents. Plain Ti scaffolds and/or devitalized unmineralized carriers (i.e., after 21 days of Ca- or P-priming and without being subjected to active mineralization phase; designated as Ca-Ctrl or P-Ctrl) were used as controls (Fig. 1B).
Physicochemical characterization of the mineralized ECM on the carriers
The physicochemical properties of the apatite component within a calcium phosphate-based biomaterial have been reported to be the key determinants for osteoinductivity.23,24 Therefore, the microstructure and the apatite composition of the produced devitalized mineralized carriers were characterized. Briefly, the devitalized mineralized carriers were sputter coated with gold, and the microstructure and composition of the mineralized ECM were examined by using a scanning electron microscope coupled with energy-dispersive X-ray analysis (SEM-EDAX; FEI XL30-FEG) at an accelerating voltage of 10 kV and 10 mm of working distance. Devitalized unmineralized carriers (i.e., Ca-Ctrl & P-Ctrl) were used as negative controls. In addition, the mass percentages of calcium and phosphorus were quantitatively analyzed with a spatial resolution of 1 μm at four locations across the deposited mineralized ECM layer by electron probe microanalysis (EPMA; JEOL Hyperprobe JXA-8530F), allowing calculation of the local calcium:phosphorus ratio. The crystalline structure of the deposited minerals was assessed by using an X-ray diffractometer (Seifert XRD 3003 TT) with a Cu K-source in the 20o–50o 2θ range (step size = 0.02o; scan time = 3 s; slit size = 0.1 mm; measurement temperature = 25°C), and the scans were analyzed by using X'Pert HighScore Plus software and compared with that of the devitalized unmineralized carriers (i.e., Ca-Ctrl & P-Ctrl) (PANalytical B.V.).
Characterization and quantification of the mineralized ECM by constrast-enhanced nanofocus X-Ray computed tomography
The efficiency of the treatment regimes in promoting mineralized ECM deposition onto 3D porous Ti scaffolds was assessed via quantification of the deposited mineralized ECM by means of contrast-enhanced nanofocus X-Ray computed tomography (CE-nanoCT) by using phosphotungstic acid (PTA) as a contrast-enhancing agent that is known to bind collagen matrix (n = 3 per group). 27 Briefly, the devitalized mineralized carriers were stained with PTA solution (6% in PBS) for 20 min, blotted dry, and analyzed by nanoCT scanning (Phoenix Nanotom S system; GE Measurement & Control Solutions) by using a tungsten target with the following parameters: voxel size = (3.125 μm) 3 ; filter = 1 mm Aluminium & 0.3 mm Copper; voltage = 90 kV; current = 146 mA; exposure time = 500 ms; frame averaging = 1; and scanning time = 20 min.
A total of 2400 X-ray images per sample (n = 3 per group) was generated, reconstructed, and the volume and distribution of the deposited ECM were analyzed by using the CTAn software (Bruker microCT). An in-house algorithm involving dilatation of the scaffold volume was applied to include the volume due to beam hardening near the titanium surface so that these scaffold and beam-hardening volumes could be segmented out from the quantification of mineralized ECM. 28 Nondevitalized mineralized carriers were also analyzed (n = 3 per group) by using similar CE-nanoCT scanning and analysis protocols to assess the effect of devitalization procedure on the retention of the mineralized ECM.
Assessment of calcium release kinetic by inductively coupled plasma-optical emission spectroscopy
The release kinetic of the calcium ion (Ca) is another crucial factor in governing the bone-forming capacity of a calcium phosphate-based biomaterial.17,24 In this study, the dissolution behavior of the Ca2+ from the mineralized ECM was measured by inductively coupled plasma-optical emission spectroscopy (ICP-OES) (Varian 720 ES) over 21 days of incubation in phosphate-buffered saline (PBS) under a dynamic condition. Briefly, the initial weight of the individual devitalized mineralized carriers was first recorded by using a micro-analytical balance. Then, the carriers were individually incubated in 16 mL of PBS on a rotator (10 rpm) at 37°C. At 6 h, 1, 7, 14, and 21 days of incubation, 3 mL of PBS from each sample was collected (n = 3) and stored at 4°C until ICP-OES analysis, and the remaining PBS was completely refreshed after each sample collection.
For ICP-OES analysis, 240 μL of nitric acid solution was added into the samples to avoid mineral re-precipitation, and the Ca intensity was measured at 393.366 nm wavelength (n = 3 per group; triplicate measurements). Then, the concentration of Ca was calculated based on a standard curve plotted with known concentrations diluted from a standard Ca solution (1000 ppm; GFS Chemicals, Inc.). After PBS sample collection at 21 days of incubation, the carriers were retrieved and the dried weight of each carrier was recorded for the calculation of the percentage of total weight loss. Subsequently, the Ca2+ release profiles of the carriers were evaluated by comparing them with the Ca2+ release profiles of five commercial calcium phosphate bone fillers (i.e., Collagraft™, Bio-Oss® and NuOss™, Vitoss® and CopiOs™) that are known for their ectopic bone-forming capacities from our previous study. 17
Quantification of hBMP-2, hVEGF, and collagen contents on the produced devitalized mineralized carriers
Production of devitalized mineralized carriers containing cell-secreted matrix-bound growth factors represents a unique benefit to augment the bone-forming capacity of a biomaterial. Within the context of this study, the contents of hBMP-2 and hVEGF were quantified by ELISA. Briefly, the devitalized mineralized ECM was extracted from the carriers by using a cell extraction buffer (Invitrogen™) containing 0.05% protease inhibitor cocktail (Sigma), 0.3 M Phenylmethylsulfonyl fluoride (PMSF), and supplemented with 10 mM Ethylenediaminetetraacetic acid (EDTA) to facilitate dissociation of proteins from the minerals. Extracted lysates were analyzed for hBMP-2 and hVEGF proteins by using Standard TMB ELISA Development Kits from the manufacturer (PeproTech) according to the supplied protocols (n = 3 per group; duplicate measurements). However, the total collagen content in the lysates was quantified colorimetrically by using the Sircol INSOLUBLE Collagen Assay kit (Tebu-Bio) according to the manufacturer's instructions (n = 3 per group; duplicate measurements). Devitalized unmineralized carriers (i.e., Ca-Ctrl & P-Ctrl) were used as negative controls.
Analysis of 3D growth and osteochondrogenic differentiation of hPDCs on devitalized mineralized carriers in a perfusion bioreactor
The cell-biomaterial interactions (including cell attachment, migration, proliferation, and differentiation) within a 3D culture set-up can provide important information on the bioactivity of the produced carriers, as well as the feasibility for an up-scaled production of clinically relevant advanced therapy medicinal products (ATMPs). In addition, culturing 3D cell-seeded constructs in a perfusion bioreactor could ensure viability of cells inside the scaffold due to an improved nutrient-waste exchange by the perfused medium. In this study, we investigated the effects of the devitalized mineralized carriers on the growth and osteochondrogenic differentiation of the seeded hPDCs (300,000 cells per carrier) by culturing the cell-seeded constructs in GM by using a perfusion bioreactor system (medium flow rate = 0.1 mL min
The osteochondrogenic differentiation effects were assessed by quantifying the expression of osteochondrogenic-related gene markers after 21 days of culture by using a quantitative polymerase chain reaction (qPCR) (n = 3 per group; duplicate measurements). Briefly, the samples were harvested in RA1 cell lysis buffer and, subsequently, sonicated gently in ice-cold condition to facilitate lysis of cells inside the scaffolds. 30 Then, the total RNA was extracted from each sample by using the RNeasy mini kit (Qiagen), and 800 ng of the extracted RNA from each sample was converted to cDNA (RevertAid First Strand cDNA synthesis kit, Life Technologies) for Sybr Green qPCR analysis by using a Rotor-Gene sequence detector (Corbett Life Science): 95°C for 3 min, 40 cycles of 95°C for 3 s, and 60°C for 60 s (Table 1 for primers' sequences). Relative differences in expression were calculated by using the 2−ΔCT method by normalizing to the expression level of the housekeeping gene β-Actin, which was verified based on its similar expression level in all tested groups. cDNA samples obtained from the devitalized unmineralized carriers (i.e., Ca-Ctrl & P-Ctrl) were used as negative controls.
Assessment of ectopic bone induction and critical-sized calvarial defect bridging in immunocompromised athymic nude rats
In this study, we assessed the ectopic bone induction and critical-sized calvarial defect bridging capacities of the produced devitalized mineralized carriers by using an immunocompromised large rodent model, that is, athymic nude rats (as compared with only ectopic implantation in nude mice in our previous study 21 ). This model was beneficial to avoid immunorejection of the hPDC-seeded carriers due to untoward immune responses on the transplanted human cells. In addition, these studies aimed at re-confirming the proof of principle as well as at establishing solid evidences before entering into larger animal models (e.g., rabbits or sheep) and for clinical translation. The produced devitalized mineralized carriers were evaluated by implanting hPDC-seeded (3.6 million cells per carrier) and unseeded devitalized mineralized carriers in a subcutaneous pocket at the back region and in critical-sized calvarial defects (6 mm in diameter) of athymic nude rats (11 weeks; Foxn1nu, Harlan Laboratories).
Briefly, the rats were anesthetized in the prone position with isoflurane in oxygen (Induction = 5%; during surgery = 2%; gas pressure = 4 barr) by using an anesthesia system (Vet-Tech), and a dose of Buprenorphine (Tamgesics: 0.03 mg/kg) was given subcutaneously for perioperative analgesia. A midline incision was made over the scalp along the sagittal crest, and the calvarium was exposed by carefully separating the underlying tissues and periosteum with a self-retaining retractor and a periosteum elevator. Then, the calvarium was scored gently with a trephine burr operating at 1500 rpm while it was irrigated with sterile saline dropwise to prevent thermal injury of the tissue at the defect margins. Then, a bone elevator was used to lift the scored calvarium without damaging the dura membrane to create a complete defect that was 6 mm diameter in each parietal bone. The defects were washed copiously with sterile saline to remove any debris or bone chips before placing the carriers (n = 3 per group), and the periosteum was closed over the carriers followed by closing the skin with wound clips.
For ectopic implantation, the carriers were implanted in subcutaneous pockets on the back region of the rat (one on each lateral side), and the incision was closed with wound clips. Postoperative analgesics (Tamgesics: 0.03 mg kg
Quantification of ectopic bone induction or defect bridging by nanoCT imaging analysis and histology
The volume and distribution of the newly formed bone in the ectopic and orthotopic explants were assessed by nanoCT imaging analysis as aforementioned without contrast agent.31,32 The generated nanoCT images were then analyzed by using CTAn software and by applying the 4-level Otsu segmentation algorithm on the individual 2D slices, whereby the newly formed bone tissues were segmented from the nonosseous tissues, Ti scaffolds, and the background. The segmented images were binarized, and the newly formed bone tissues were quantified. The quantified bone volumes were then normalized to the total scaffold void volume (n = 3 per group). Calvarial bone defect bridging was represented by the quantified bone volume within the defect, and the quantified bone volumes in defects implanted with hPDC-seeded plain Ti scaffolds were used as baseline for comparison purposes. For histological analysis, the explants were embedded in polymethylmethacrylate resin (Technovit 9100 NEW, Heraeus Kulzer) and sectioned by using a diamond saw (Leica) before being ground to about 70 μm thickness. In the tissue sections, the newly formed bone was then stained with Stevenel's Blue & Van Gieson's Picrofuchsin solution at 60°C.
Statistical analysis
All data are expressed as mean ± standard deviation (SD) or otherwise as stated in the figure captions. Statistical significance was established by analyzing the data by using an unpaired student t-test (two-tailed) or a one-way analysis of variance (ANOVA) followed by multiple-comparison post hoc Tukey's test using SPSS (PASW statistics) as indicated in the figure captions: *p < 0.05, **p < 0.01, and ***p < 0.001.
Results
Three-dimensional hPDCs growth and mineralized ECM deposition on Ti scaffolds
As shown in Figure 1C, Ca- or P-priming resulted in significantly higher cell proliferation, as indicated by the higher metabolic activity measured at 7 and 14 days of the priming stage as compared with carriers cultured in GM. No significant difference between the effects of Ca- and P-priming on cell proliferation was observed. During the active ECM mineralization stage, a gradual decrease in the metabolic activity was observed, which became significantly lower than that of the GM condition after 42 days of culture. However, live-dead staining showed abundant green fluorescence-labeled cells on the mineralized carriers, which indicated relatively high cell viability despite a gradual decrease in metabolic activity (see representative image as inset). Through devitalization, mineralized carriers with low (designated as C7 or P7) or high (designated as C21 or P21) mineralized ECM content (m) were obtained after they were cultured in the mineralization stage for 7 or 21 days respectively, as shown by the representative bright-field images (Fig. 1D). In contrast, no mineralized ECM was formed on the scaffolds that had not been cultured under mineralizing conditions (i.e., Ca-Ctrl & P-Ctrl).
These observations were supported by SEM analysis, which showed higher mineralized ECM content by prolonging the mineralizing condition from 7 to 21 days (Fig. 1E). At high magnification, SEM revealed different morphologies of the mineralized ECM between Ca- and P-primed carriers, in which the mineralized ECM consisted of collagen fibers (col; identifiable with visible periodic banding pattern) that were integrated with unique sub-micron apatite agglomerates (for Ca-priming) or apatite spherulites (for P-priming) (labeled as “apt.” in Fig. 1F). Sub-micron porosity (p) was also clearly visible within the mineralized ECM. EDAX element analysis suggested the formation of apatite minerals within the organic compartment of the ECM based on the measured spectra of calcium (Ca), phosphorus (P), oxygen (O), and carbon (C) peaks (Fig. 1E).
Crystallinity, Ca & P composition, and Ca release kinetics of the produced devitalized mineralized carriers
Via XRD analysis, all devitalized mineralized carriers contained semi-crystalline minerals that closely resembled the diffraction patterns of hydroxyapatite (XRD peaks at 2θ = 26o, 32o, and 48o; Fig. 2A). Only XRD peaks associated with the titanium scaffold (at 2θ = 35o, 38o, and 40o) were detected in the unmineralized controls (i.e., Ca-Ctrl & P-Ctrl). Through semi-quantitative EPMA analysis at four locations, the results showed that Ca-primed carriers contained mineralized ECM with a high Ca:P ratio across the thickness, whereas P-primed carriers contained mineralized ECM with a higher P content (Fig. 2B). These results indicated possible different mechanisms of ECM mineralization between Ca- and P-primed ECM.
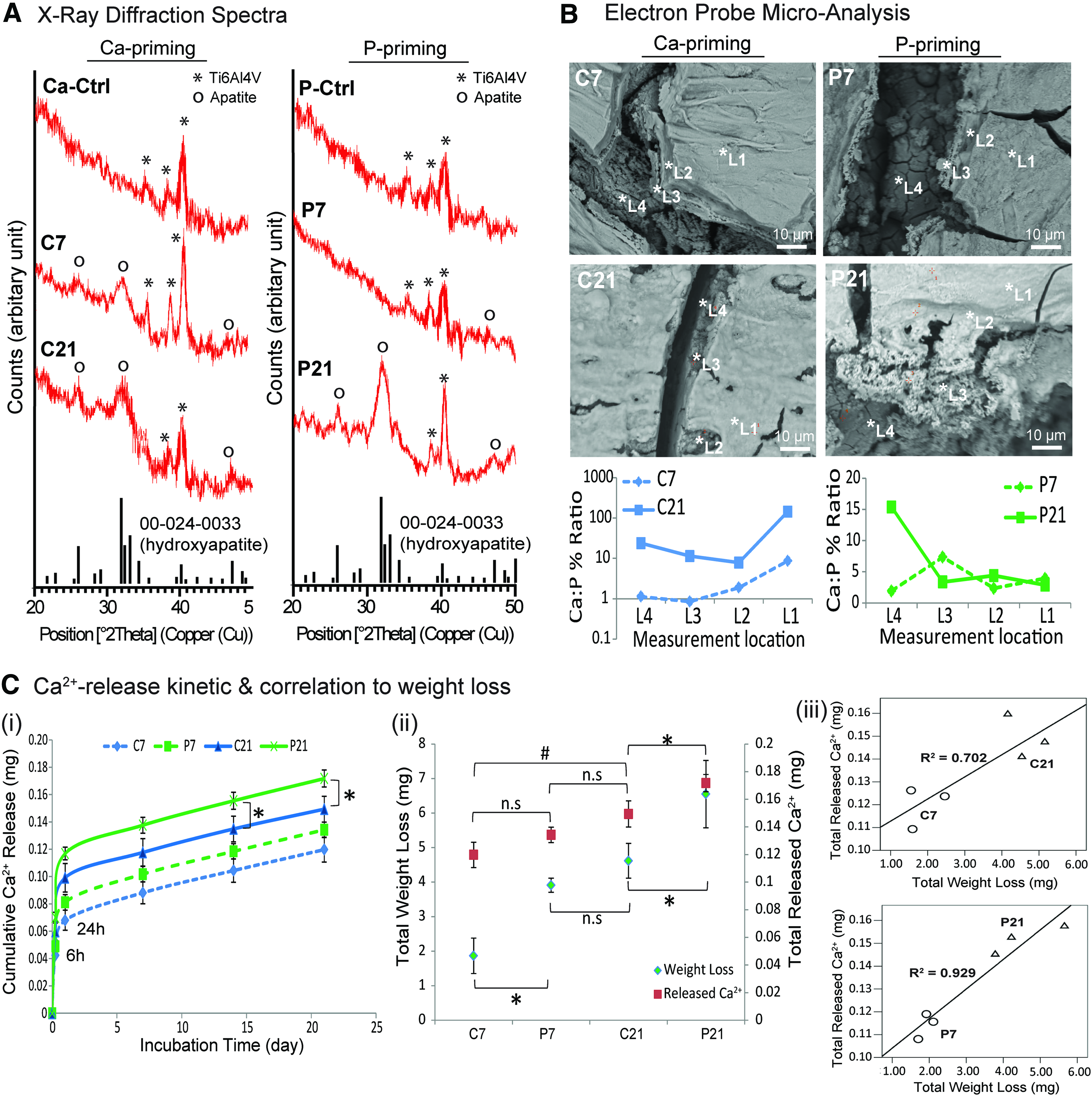
Through ICP-OES analysis, the Ca2+ release kinetic was found to be dependent on the culture conditions, which demonstrated a burst release at 6 and 24 h by all carriers (Fig. 2C i). In general, P-primed carriers showed higher Ca2+ release than Ca-primed carriers during the 21 days of dissolution testing, and the Ca2+ release was higher for carriers with a higher mineralized ECM content. In particular, the Ca2+ release of P21 at 14 and 21 days was significantly higher than that of C21. Measurement of the total released Ca2+ after 21 days of dissolution showed that P21 gave rise to the highest released Ca2+; meanwhile, the total released Ca2+ of C21 was significantly higher than that of C7.
These data were supported by the measurement of total weight loss after the dissolution tests, whereby P21 accounted for the highest weight loss (8.62%), followed by C21 (6.51%), P7 (6.18%), and the lowest by C7 (3.04%) (Fig. 2C ii). Correlation plots indicated that the total released Ca2+ was highly correlated to the total weight loss for P-primed carriers (R2 = 0.929); meanwhile, the correlation was lower for Ca-primed carriers (R2 = 0.702) (Fig. 2C iii). When compared with the Ca2+ release profiles of the five commercial calcium phosphate bone fillers that are known for their ectopic bone-forming capacities (when seeded with hPDCs) from our previous study, 17 encouragingly, all carriers demonstrated dissolution profiles that were in the range that was closer to high bone formers (i.e., Collagraft, Bio-Oss, and NuOss) but not the low and no bone formers (i.e., Vitoss and CopiOs) (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/tea).
Effect of culture treatment and devitalization procedure on the volume and distribution of mineralized ECM and the porosity of the carriers
Through the use of PTA as a contrast agent to selectively bind collagen matrix, the deposited mineralized ECM on the carriers could be visualized and quantified via nanoCT image analysis, as shown by the binarized cross-sectional images in Figure 3A. Homogeneous mineralized ECM distribution surrounding each of the scaffold struts was observed on the carriers. Quantitatively, Ca-primed carriers contained 1.77- to 2.4-fold higher mineralized ECM content but lower porosity than P-primed carriers (63–66% porosity for C21 & C7 as compared with 71–73% porosity for P21 and P7, respectively; Fig. 3B). The 3D reconstructed images (excluding the volume of Ti scaffolds) showed that the mineralized ECM followed the scaffold geometry and displayed macro-porosity. On the other hand, the devitalization procedure has resulted in a significant loss of mineralized ECM content (48.1–55.6%) on Ca-primed carriers, and greater losses (54.5–68%) on P-primed carriers (Fig. 3C). Of note, the volume percentage of the Ti scaffolds was calculated to be 21–24%, which indicated no scaffold loss due to the culture treatments and the consistency of our scaffold production process via SLM. Devitalization also resulted in a significant reduction of the matrix:scaffold surface ratios of the carriers, giving rise to comparable matrix:scaffold surface ratios for all produced devitalized mineralized carriers (Fig. 3D).
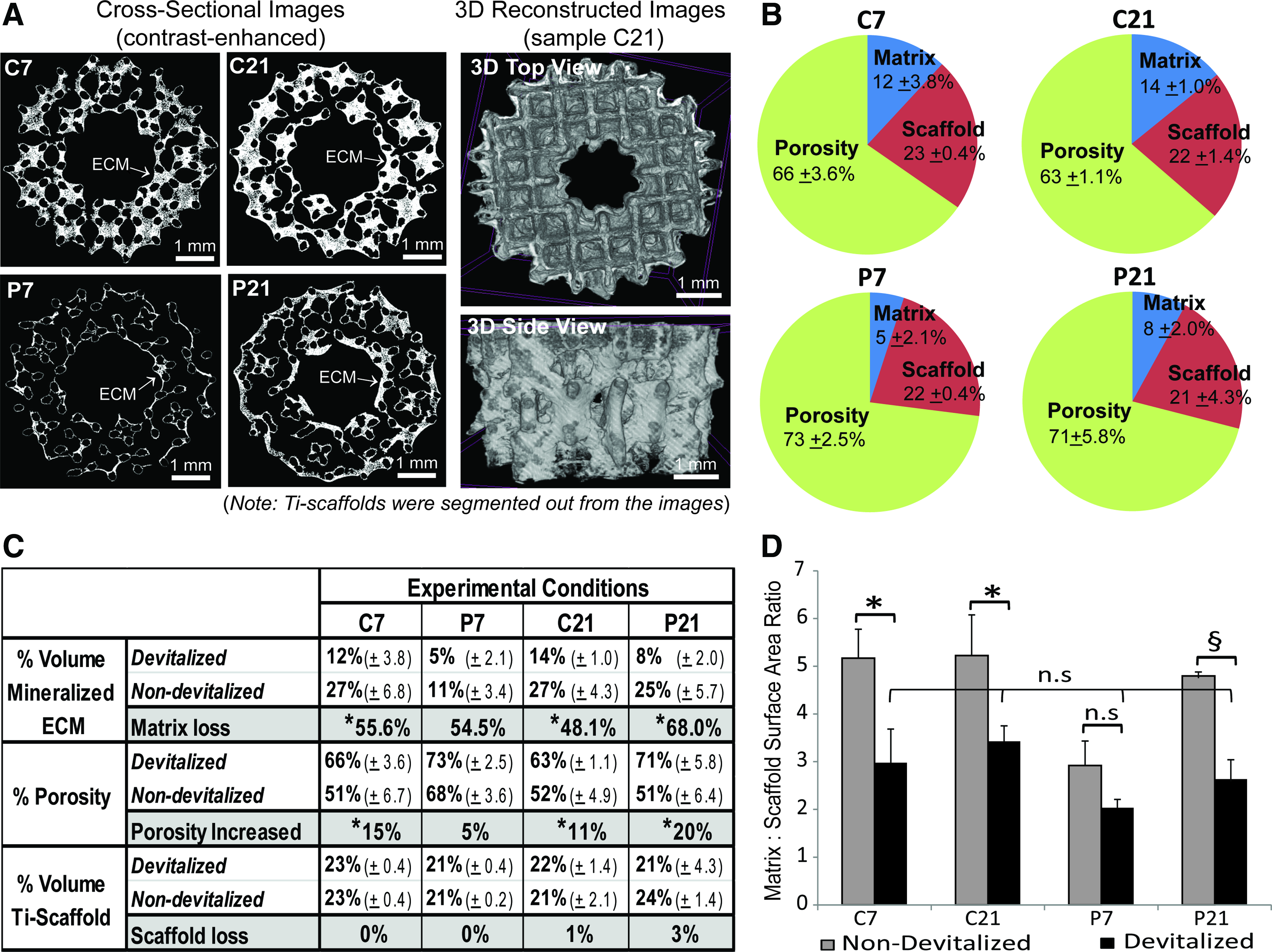
Contrast-enhanced nanofocus X-Ray computed tomography characterization and quantification of the volume and distribution of mineralized ECM, and the porosity of the carriers both before and after the devitalization procedure (contrast agent = phosphotungstic acid [PTA]).
hBMP-2, hVEGF, and collagen contents of the produced devitalized mineralized carriers
The contents of two major ECM-bound human osteogenic growth factors (i.e., hBMP-2 and hVEGF) were quantified by ELISA assays. The results showed that both the Ca- and P-primed devitalized mineralized carriers contained lower hBMP-2 protein content than the unmineralized counterparts, in particular for C21 and P21, whereby the protein content was significantly lower than the controls (Fig. 4A i). In contrast, both the Ca- and P-primed devitalized mineralized carriers contained higher hVEGF protein content than the unmineralized counterparts, in particular for Ca-primed carriers, where the hVEGF protein content was significantly higher than the controls (Fig. 4A ii). Nevertheless, the level of hVEGF protein in the P-primed carriers was not statistically different from that of the unmineralized controls. This result suggested a positive effect of the mineralizing condition on hVEGF expression.
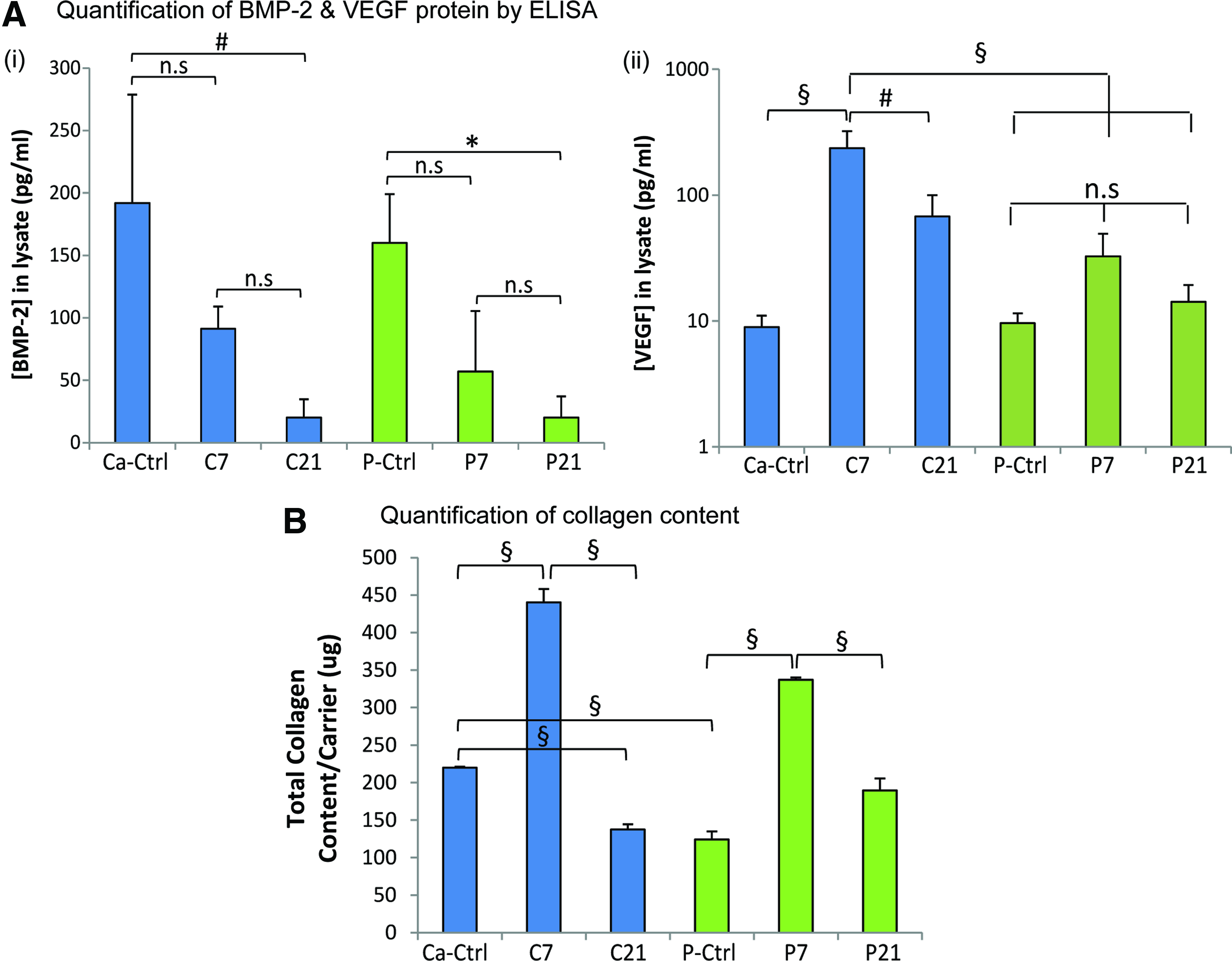
These observations indicated that the current culture treatment had a significant impact on the secretion of hBMP-2 and hVEGF by hPDCs, which can potentially influence the bone-forming capacity of the devitalized mineralized carriers. The collagen content of the produced carriers was also quantified to reveal the composition of the deposited mineralized ECM (Fig. 4B). The results showed that the highest collagen content was quantified in C7 and P7, which were significantly higher than that of the unmineralized conditions. Interestingly, C21 had significantly lower collagen content than the control, whereas the collagen content of P21 was comparable to the control despite a higher amount being quantified.
Three-dimensional growth and osteochondrogenic differentiation of hPDCs on devitalized mineralized carriers under perfusion bioreactor culture
The effects of the produced mineralized carriers on supporting 3D cell expansion and osteochondrogenic differentiation of hPDCs were assessed by culturing hPDC-seeded carriers in a perfusion bioreactor for 21 days by using GM. Metabolic activity measurements showed that carriers produced via both priming conditions trended to support higher cell expansion after 21 days of culture, except for C21, which was comparable to the unmineralized controls (Fig. 5A, B). Gene expression analysis showed that all carriers had no significant effects on osteochondrogenic differentiation of hPDCs after 21 days of culturing in the perfusion bioreactor, as most of the related osteogenesis-related gene markers were not differentially regulated as compared with the unmineralized controls (Fig. 5C). Nevertheless, BMP-2 expression was upregulated by the devitalized mineralized carriers, in particular for P21, which was significantly higher than P7 and the unmineralized controls (Fig. 5D). In contrast, the ALP expression was downregulated by hPDCs when they were seeded on the devitalized mineralized carriers as compared with the unmineralized controls, in which C21 and P21 resulted in the lowest ALP expression (Fig. 5E).

Three-dimensional cell growth and osteochondrogenic differentiation of hPDCs seeded on the devitalized mineralized carriers during 21 days of culture in a perfusion bioreactor.
Ectopic bone induction by hPDC-seeded devitalized mineralized carriers
The CSE of the devitalized mineralized carriers was evaluated before implantation. The results showed that all carriers allowed high CSE (>90% as compared with 60% CSE on plain Ti scaffolds reported in our previous study 22 ), and the CSE was not significantly different between carrier types (Supplementary Fig. S2). After 8 weeks of subcutaneous implantation of hPDC-seeded carriers in nude rats, histological analysis showed that all carriers induced ectopic bone formation (as visualized by Stevenel's Blue and Van Gieson's Picrofuchsin staining; Fig. 6A). Newly formed bone (B; stained bright red) was found in close proximity and/or in direct contact with the scaffolds (Ti). At high magnification, osteocytes (indicated by white arrow heads) could be clearly seen within the newly formed bone surrounded by soft tissues (s.t.). No ectopic bone formation was induced by the unseeded, devitalized mineralized carriers and hPDC-seeded plain Ti scaffolds.
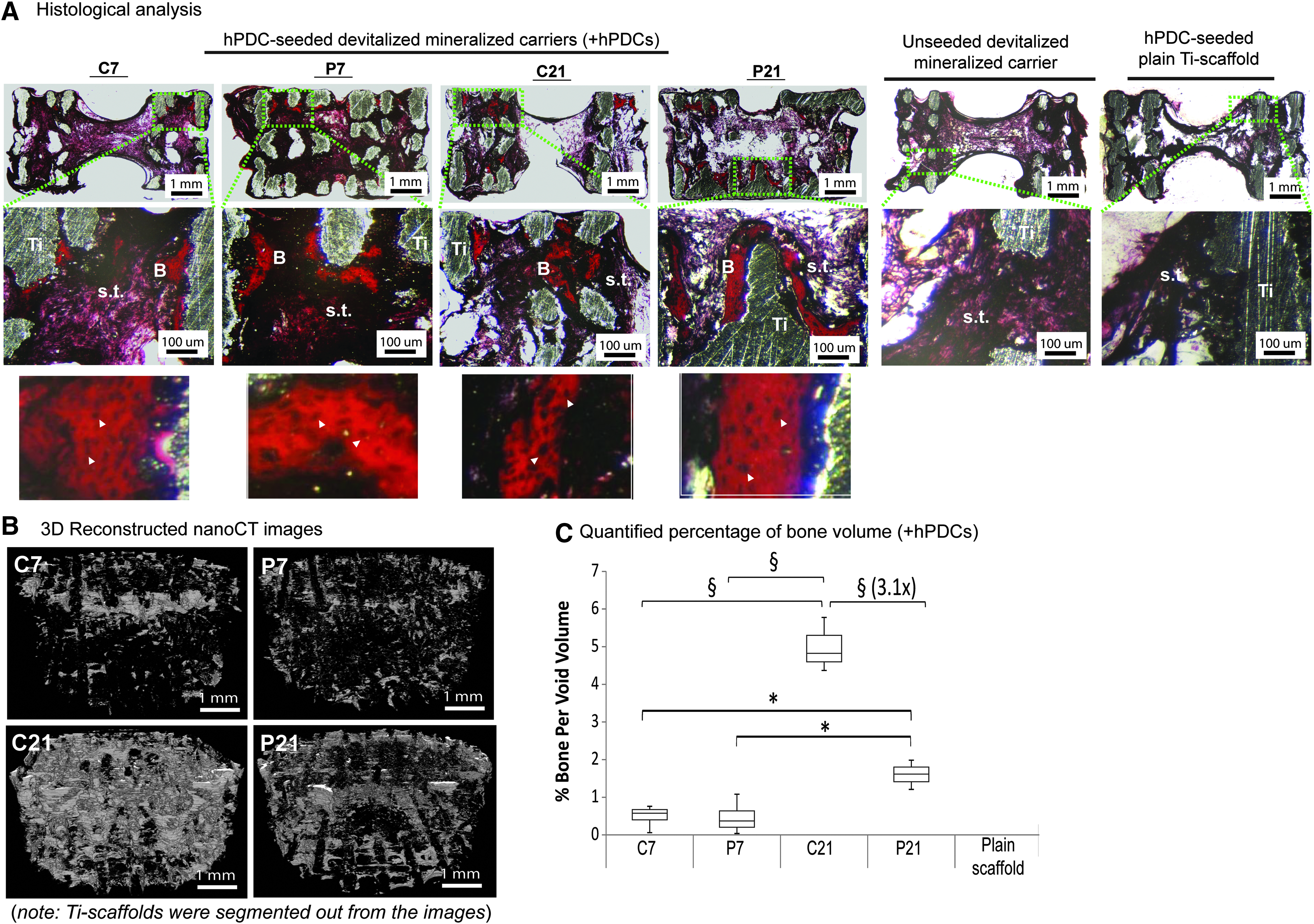
Ectopic bone induction by hPDC-seeded devitalized mineralized carriers after 8 weeks of subcutaneous implantation in nude rats.
The distribution and amount of newly formed bone were visualized via 3D reconstruction of the nanoCT images after segmenting out the Ti-scaffold volume (Fig. 6B). Notably, the highest bone formation was quantified in C21 (4.99% ± 0.72%), which was significantly higher than that of P21, C7, and P7 (Fig. 6C). Although P21 induced significantly higher ectopic bone formation (1.60% ± 0.39%) than C7 (0.49% ± 0.31%) and P7 (0.47% ± 0.45%), its value was 3.1-fold lower than C21. These data suggested that the current culture treatment produced devitalized mineralized carriers with a higher ectopic bone-forming capacity (nearly five-folds higher) than that previously reported in our proof-of-principle study. 21
Augmentation of critical-sized calvarial defect bridging by devitalized mineralized carriers
Devitalized nineralized carriers (6 mm diameter × 3 mm height) with or without seeded hPDCs (indicated as “+hPDCs” or “−hPDCs”) were implanted into critical-sized calvarial defects (6 mm diameter; ∼1 mm thickness) of nude rats to assess their orthotopic bone defect bridging capacity. After 8 weeks of implantation, qualitatively all carriers were integrated into the defects with no sign of inflammation or tissue necrosis. The 2 mm hollow centers were also infiltrated mostly with hard tissues by palpation. By 3D reconstruction of the nanoCT images, various degrees of bone defect bridging (n.b.; delineated by green dotted lines) were achieved within the defects that were implanted with carriers seeded with or without hPDCs (Fig. 7A). NanoCT quantification showed that devitalized mineralized carriers with a relatively lower mineralized ECM content (i.e., C7 and P7) induced on average ∼10% bone formation (per total scaffold void volume) in the calvarial defects, whereas the counterparts with a higher mineralized ECM content (i.e., C21 & P21) gave rise to ∼4–8% bone formation (per total scaffold void volume) (Fig. 7B i).
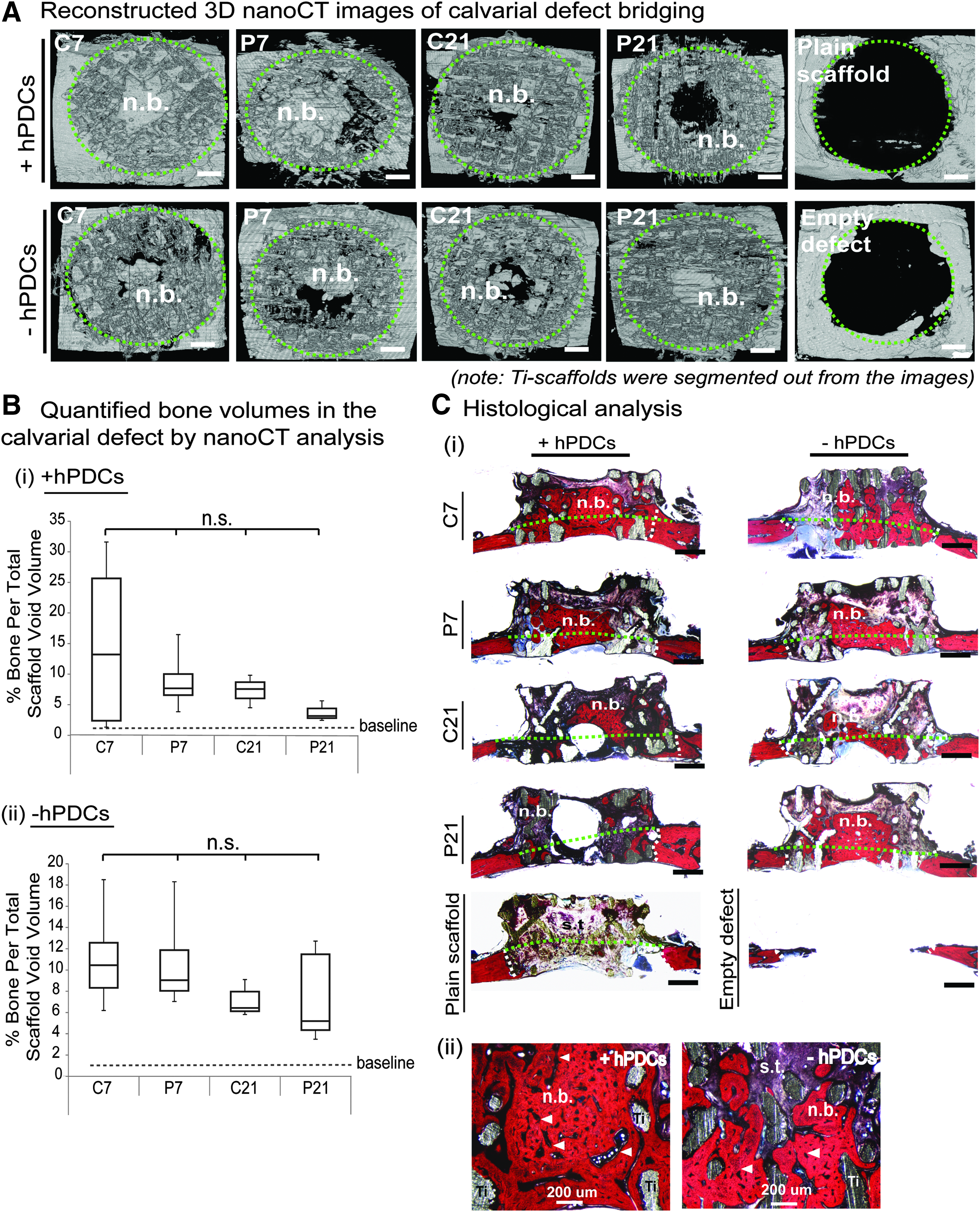
Bone defect bridging capacity of the devitalized mineralized carriers (seeded with or without hPDCs; +/− hPDCs) after 8 weeks of implantation in critical-sized nude rat calvarial defects.
In addition, seeding hPDCs onto the carriers has no added value to improve the bone defect bridging property of the devitalized mineralized carriers in all conditions (Fig. 7B ii). Limited bone defect bridging was observed in defects that were implanted with hPDC-seeded plain Ti scaffolds (indicated by the baseline) or in empty defects. These results were corroborated by the histological analysis that showed that the carriers with lower mineralized ECM contents (i.e., C7 and P7) induced more bone defect bridging than those with higher mineralized ECM contents (i.e., C21 and P21) (Fig. 7C i). Noticeably, native bone tissue ingrowth (indicating osteoconduction) and extraosseous bone tissue formation (indicating osteoinduction) were observed in the bone defects and within the scaffolds outside of the defects (delineated by the green dotted lines). At high magnification, direct contact was observed at the interfaces of scaffolds (Ti) and the newly formed bones (n.b.), indicating high osseointegration of the carriers with the regenerating bones containing osteocytes residing in the lacunae and bone marrow compartments (white arrow heads) (Fig. 7C ii). Limited bone regeneration or defect bridging was observed in defects that were implanted with plain scaffold or empty defects.
Discussion
Functionalization of 3D porous scaffolds with cell-secreted mineralized ECM represents a promising bio-inspired approach to produce TE constructs that may effectively mediate bone regeneration.7,9 It is based on an appreciation of developmental biology and the postnatal healing process to semi-autonomously “kick-start” and guide the bone regeneration cascade. This concept of bone induction by mineralized ECM-based TE constructs is also strongly supported by a natural pathological phenomenon of heterotopic ossification of traumatized soft tissues or burn wounds due to undesirable tissue mineralization.33,34 In fact, our previous study has provided a “proof-of-principle” that 3D porous scaffolds bearing cell-secreted mineralized ECM were readily recognized by the host environment as an “osteogenic biotemplate” and triggered bone formation. 21
The limited bone formation on the carriers (<1% per total scaffold void volume of 64.8 mm3) served as our motivation to further optimize the mineralizing culture condition in this study. As a result, we showed that the current modified culture protocol (i.e., combining the priming followed by a direct mineralization phase) augmented nearly five-fold ectopic bone formation on the carriers as compared with the previously reported direct culture mineralization method. The 5% of bone volume induction is highly comparable and even out-performed some of the commercial bone fillers under the same cell seeding density [Bio-Oss (∼5%), Collagraft (∼1.8%), Vitoss (∼3%), and CopiOs (0%)], as previously reported. 17 Despite current culture priming protocols requiring relatively longer times to produce devitalized mineralized carriers, the effects on enhancing mineralized ECM deposition and augmenting the bone-inducing capacity of the carriers were highly appreciable.
Of note, this modified mineralizing culture protocol was not supplemented with exogenous growth factors; meanwhile, the deposition of mineralized ECM on 3D porous Ti scaffolds was purely driven by calcium and/or phosphate ions, in addition to the supplemented general culture chemicals (i.e., dexamethasone and ascorbic acid). Undoubtedly, these have a significant beneficial impact from economic and safety aspects. We believe that further optimization of this mineralizing culture protocol using serum-free culture medium in future will certainly enhance the feasibility of these carriers for clinical repair of bone defects.
Despite the underlying mechanism to explain the proliferative effect by Ca- or P-priming not being investigated in this study, it has been reported that Ca2+ acts on the calmodulin-dependent protein kinase II (CaMKII) pathway to regulate cell proliferation 35 ; meanwhile, P regulates proliferation and osteogenesis via adenosine signaling. 36 Similarly, the mechanism of ECM mineralization could be linked to two well-described mechanisms in the literature: (i) calcification of collagen fibers by cell-secreted matrix vesicles formed via uptake of free Ca2+ and P from the extracellular compartment37–40 ; (ii) direct binding of free Ca2+ or P to both the gap and overlap regions of nucleation sites on the collagen fibers (via noncollagenous proteins), thus promoting apatite crystal growth and propagation along the collagen fibers.41,42
As observed in this study, the priming conditions may have initiated different apatite crystal growth and propagation mechanisms and, thus, resulted in different crystal structures (i.e., agglomerates for Ca-priming and spherulites for P-priming). The priming conditions also resulted in different mineral composition, different efficacy in promoting mineralized ECM deposition, and different retention of mineralized ECM on the devitalization process. Optimization of the devitalization protocol is apparently an added value to improve the existing culture protocol, besides having the need to characterize and quantify the genetic remnants from the cells to fulfill the regulatory requirements from a safety perspective.
It is widely accepted that the Ca2+ release kinetics of a biomaterial is one of the key determinants of osteoinductivity,23,43 and, therefore, the in vitro Ca2+ release profile is often used as a predictive marker to assess the bone-forming capacity. 44 In this study, we found that the priming conditions influenced physicochemical properties of the produced devitalized mineralized carriers, and they also resulted in different Ca2+ release kinetics that positively correlated to higher bone formation. However, it was not the only key factor, as P-primed carriers (i.e., P21, which had the highest Ca2+ release kinetics) induced significantly lower (3.1-fold) bone formation than Ca-primed carriers (i.e., C21), despite comparable CSE being measured on both carrier types. Nevertheless, our findings suggested the technological feasibility of the current modified culture method to fine-tune material properties of the carriers to optimally elicit bone regeneration. In addition, by comparing the Ca2+ release profiles of devitalized mineralized carriers with those of five clinically used bone fillers, we believe that the produced devitalized mineralized carriers possess Ca2+ release kinetics that are of clinical relevance for bone defect repair.
In addition, we assessed the effects of the carriers on the growth and differentiation of hPDCs over 21 days of culture in a perfusion bioreactor set-up. For this, a much lower cell seeding density (300,000 cells per carrier) was used to prevent immediate inhibition of cell growth due to space limitation on the scaffold when a high density of cells would be seeded. Moreover, the gene expression analysis was conducted in the GM condition, so to ascertain that any of the osteochondrogenic differentiation effects was purely due to devitalized mineralized carriers but not caused by the culture medium. Here, gene expression data obtained from devitalized unmineralized carriers were used for comparison purposes. The results showed that the in vitro growth of hPDCs was supported by the devitalized mineralized carriers indicating biocompatibility, and a minor osteochondrogenic differentiation effect suggesting that the produced devitalized mineralized carriers might resemble the native bony microenvironment niche and, thus, be conducive for in vitro expansion of hPDCs. This phenomenon is beneficial to prevent terminal differentiation of hPDCs when aiming at delivering stem cells with competent in vivo self-renewal and differentiation capacity to initiate repeated “waves” of bone tissue regeneration.21,45,46
Importantly, the devitalized mineralized carriers induced upregulation of BMP-2 gene expression, which may be associated with an effect induced by the mineralized ECM due to the release of Ca2+ and P ions. 43 On the other hand, the downregulation of ALP gene expression can be associated with a negative feedback loop of hPDCs in regulating culture mineralization in response to the release of supraphysiological free Ca2+ and P ions from the carriers. 22 Despite the detection of hBMP-2 and hVEGF proteins on the carriers, the protein content was either low or was found to be not correlated to the ectopic bone-forming capacity. We are aware of the fact that cell density alters cellular gene expression and differentiation potential. The in vitro cell seeding density used was much lower than that of the in vivo bone formation assays. The in vitro gene expression data were obtained when the cultured cells reached a relatively high cell density for an in vitro set-up (as indicated by a more than three-fold increase in metabolic activity after 21 days of culture). Therefore, the data provided valuable information on the osteogenicity of the carriers, which was helpful for the interpretation of the in vivo bone formation results. Furthermore, these data provided an essential basis for establishing an in vitro cell expansion platform toward the manufacturing of cell-based ATMPs.
As the ultimate goal of this study is to produce devitalized mineralized carriers for stem cell delivery and bone regeneration, the geometry and macro-porosity of the carrier will significantly influence the biological outcomes. In this study, we showed that the produced carriers preserved the predesigned morphology and the macro-porosity (63–73%) of Ti scaffolds that were optimized to facilitate cell seeding, nutrient-waste diffusion, and bone tissue growth/in-growth. 47 The carriers allowed seeding a high amount of hPDCs (3.6 million cells per carrier of 6 mm diameter × 3 mm height) with high CSE (>90%), an important parameter that is required to ensure effective bone tissue induction toward clinical applicability. Once again, our current findings showed that the bone induction capacity of the produced carriers was dependent on the presence of hPDCs to initiate ectopic bone formation.
Nonetheless, this finding did not hold for healing the calvarial defect, as statistically comparable bone bridging was quantified for all carrier types regardless of whether they were seeded with or without hPDCs. It is noteworthy that although the sample size (n = 3) used for most of the experiments performed within this study was relatively low, a power analysis we performed (based on findings of similar studies reported in four recent publications from our group24,48–50) gave a minimum sample size ranging between 2 and 4 (with a power value = 0.8 and type I error rate = 0.5%). Nevertheless, a correct amount of mineralized ECM needs to be determined in future studies to ensure sufficient porosity to facilitate native bone ingrowth into complete defect regeneration. This represents a crucial consideration when designing future novel bone regeneration strategies for the healing of large bone defects where osteoconduction is required to ensure high osteointegration at the defect margin and osteoinduction is necessary to induce bone formation at a remote area (typically the center area) of the defect.
Conclusions
In this study, we showed that the current modified culture protocol appears to be a useful functionalization strategy to modify 3D porous scaffolds with augmented bone-forming capacity by harnessing the osteogenicity of cell-derived mineralized ECM. In addition, we provided further understanding on several carrier variables and their effects on in vivo bone-forming capacity, which could represent critical parameters that need to be taken into account when designing advanced TE constructs for effective bone regeneration.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Marina Marechal for the guidance on the critical-sized calvarial defect implantation and Roel Kroes for the assistance with the histological analysis. This research is funded by the Research Foundation-Flanders (FWO: 1.5.172.13 N-Interdisc.), the Government Agency for Innovation by Science and Technology (IWT-111545), and ENDEAVOUR project G.0982.11 N of FWO, and it is a part of Prometheus, the Leuven Research & Development Division of Skeletal Tissue Engineering of the KU Leuven. The nanoCT images have been generated on the X-ray computed tomography facilities of the Department of Materials Engineering of the KU Leuven, financed by the Hercules Foundation (project AKUL 09/001: Micro- and nanoCT for the hierarchical analysis of materials).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.