
Abstract
Tendons are subjected to high strength dynamic mechanical forces in vivo. Mechanical strength is an essential requirement for tendon scaffold materials. A composite scaffold was used in this study to provide mechanical strength, which was composed of an inter part of nonwoven polyglycolic acid (PGA) fibers and an outer part of the net knitted with PGA and polylactic acid (PLA) fibers in a ratio of 4:2. This study compared three different approaches for in vivo tendon engineering, that is, cell-free scaffold and allogeneic and autologous cell seeded scaffolds, using a rabbit Achilles tendon repair model. Dermal fibroblasts were, respectively, isolated from the dermis of regular rabbits or green fluorescence protein transgenic rabbits as the autologous and the allogeneic cell sources, respectively. The cell scaffolds and cell-free scaffolds were implanted to bridge a partial segmental defect of rabbit Achilles tendon. The engineered tendons were harvested at 7 and 13 months postsurgery for various examinations. The results showed that all three groups could achieve in vivo tendon regeneration similarly with slightly better tissue formation in autologous group than in other two groups, including better scaffold degradation and relatively thicker collagen fibrils. There were no statistically significant differences in mechanical parameters among three groups. This work demonstrated that allogeneic fibroblasts and scaffold alone are likely to be used for tendon tissue engineering.
Introduction
I
In recent years, in situ tissue regeneration with implanted scaffold only without seed cells also became an important strategy. It uses tissue inductive materials to regenerate tissue through recruiting host endogenous cells. 4 Such an approach has been demonstrated effectively in regenerating bone, cartilage, skin, blood vessel, peripheral nerve, and tendon.4–9 The apparent difference between cell-free inductive materials and traditional cell based scaffold approaches is likely due to the design of inductive scaffold materials and tissue regenerative environment. Previously, it was shown that the use of natural extracellular matrices as one of the components of scaffold favors cell-free approach of tissue regeneration. For example, Meimandi-Parizi et al. reported that collagen implant with or without polydioxanone sheath can improve tendon regeneration with better clinical scoring. 8 It was also demonstrated that better vascularized regions tended to regenerate tissue in situ through better access of endogenous cells to the implanted scaffold. 10
Allogeneic approach has also been tried in engineered tissue repair, such as bone, skin, and cartilage. 11 Han et al. reported that the use of human allogeneic fibroblast cells seeded on allogeneic skin substitutes was found to be a safe and effective treatment for diabetic foot ulcers. 12 Almqvist et al. demonstrated that alginate beads containing human mature allogenic chondrocytes could repair symptomatic cartilage defects in the knee without adverse reactions. 13 Whether allogeneic cell based tissue engineering is a generally feasible approach remains controversial depending on the size, anatomical locations, and tissue types to be replaced.
Tendons play crucial roles in force transmission and joint stability under high strength mechanical loading. Mechanical property, particularly tensile strength, is an essential requirement of tendon scaffold materials. 14 For example, tensile strength of human tendon could reach 50–150 MPa. 15 Thus, this study used a composite scaffold composed of an inter part of nonwoven polyglycolic acid (PGA) fibers and an outer part of the net knitted with PGA and polylactic acid (PLA) fibers in a ratio of 4:2 as previously reported, which was able to bear high strength mechanical loading with tensile strength above 50 MPa. 16
Tendon is a type of connective tissue that has a simple tissue structure composed of tenocytes, collagens and proteoglycan based extracellular matrices. 17 It is relatively avascular with densely deposited extracellular matrix. In the literature, autologous cell based tendon engineering is the most often reported approach, whereas allogeneic cell based and cell-free scaffold based approaches have been reported as well.18–20 These reported studies vary in their animal models, cell types, defect size, and anatomic locations, and their outcomes are difficult to be compared to conclude the difference in their efficacy and feasibility based on long-term results.
Rabbit Achilles tendon repair is a common model that was used in many tendon engineering studies.16,21 Previously, we have used dermal fibroblasts as the cell source for in vitro 22 and in vivo 23 tendon engineering. In this study, we used rabbit Achilles tendon repair as the animal model 16 and dermal fibroblasts as the cell source to evaluate the efficacy and feasibility of autologous, allogeneic, and cell-free scaffold approaches for engineered tendon repair with a side-by-side design.
Materials and Methods
Experimental design
This study involved three groups. (1) Autologous cell group: before in vivo implantation, autologous dermal fibroblasts were seeded on a composite tendon scaffold composed with PGA nonwoven fibers and a net knitted with PGA and PLA fibers as previously reported. 16 (2) Allogeneic group: allogeneic dermal fibroblasts were seeded on the composite scaffold before in vivo implantation. (3) Cell-free scaffold group: the composite scaffold was in vivo implanted without cell seeding. After cell seeding, cell-seeded constructs were kept in an incubator for 2 h before their in vivo implantation for Achilles tendon repair in a rabbit model.
Animal studies
Six-week-old mature New Zealand White rabbits were purchased from Shanghai Chuansha Breeding Factory (Shanghai, China). All animal experimental protocols were approved by Animal Care and Experiment Committee of Shanghai Jiao Tong University School of Medicine. Total 42 rabbits with weight ranging from 1.7 to 2.5 kg, either male or female, were randomly assigned to three groups (n = 14 for each group). During the experimental procedure, 10 rabbits were eventually excluded from the study due to unexpected death. As shown in Table 1, 5 animals were dropped from autologous group (5 of 14, 35.7%), 4 (4 of 14, 28.6%) were dropped from allogeneic group, and 1 (1 of 14, 7.1%) was dropped from the cell-free group. Animals were sacrificed, respectively, at the time points of 7 months (n = 4 for autologous; n = 5 for allogeneic; and n = 6 for cell-free group) and 13 months (n = 5 for autologous; n = 5 for allogeneic; and n = 7 for cell-free group) postsurgery for biomechanical, histological evaluation and transmission electron microscopic (TEM) evaluation. Normal tendon was harvested as a control.
Skin harvesting procedure
Anesthesia was performed with an intramuscular injection of ketamine (10 mg/kg) and Lumianxin (5 mg/kg), which provided ∼40 min of adequate sedation. Nuchal skin tissue was harvested from the rabbits in sterile conditions and placed into a 50 mL centrifuge tube with Dulbecco's modified Eagle's medium (DMEM; Hyclone, Logan City, UT) containing 10% fetal bovine serum (FBS, Hyclone) and Antibiotic-Antimycotic solution (100 ×; Gibco). The tissue samples were prepared for cell isolation within 2 h postharvest. The wound was closed, and all rabbits were returned to their cages.
Dermal fibroblast cell isolation and culture
Harvested skin tissues were transferred to our laboratory in a 50 mL centrifuge tube followed by antibacterial treatment with 2.5% chloramphenicol solution for 10 min and three washes with phosphate-buffered saline (PBS) before use. Afterward, these samples were cut into 2 × 4 mm2 pieces by sterile scissors. The tissue fragments were placed into a 50 mL centrifuge tube containing 0.2% dispase (Roche Diagnostics, Indianapolis, IN) that was dissolved in DMEM supplemented with 10% FBS and incubated at 4°C overnight. Skin dermis and epidermis were mechanically separated with a forceps and then the dermis was cut into small pieces followed by the digestion in 0.2% collagenase (Collagenase NB 4 Standard grade, SERVA, GER) dissolved in DMEM containing 10% FBS for 2 h at 37°C on a rotator. Then, the obtained cell suspension was centrifuged at 524 g for 5 min, and the cell pellet was resuspended in high-glucose DMEM culture medium and transferred onto 10 cm culture dish (BD Falcon) in regular density (1.5 × 106 per dish) for culture at 37°C in humidified incubator supplied with 5% CO2. After confluence of the cultured cells, they were detached with 0.25% trypsin-EDTA (Gibco, Grand Island, NY) and subcultured at the same density. The subcultured cells in the fifth passage were used in this study.
In addition, skin tissues were also harvested from a green fluorescence protein (GFP) transgenic rabbits (also New Zealand White strain, a kind gift from Prof. Xuejing Chen, Experimental Animal Center, Shanghai Jiao Tong University School of Medicine). The dermal fibroblasts were extracted as the allogeneic cell source using the same procedure as above described.
Preparation of scaffold material
As previously reported, 16 a composite scaffold was used in this study, which consisted of an inner part of PGA nonwoven fibers and an outer part of net scaffold knitted with PGA and PLA fibers in a ratio of 4:2. Each construct was disinfected with ethylene oxide followed by soaking in 75% ethanol and washing in PBS. The scaffold was then preincubated in DMEM supplemented with 10% FBS at 37°C overnight in an incubator before cell seeding or before in vivo implantation.
Cell seeding on scaffold
The autologous or allogeneic fibroblasts at the fifth passage were collected and seeded evenly onto the composite scaffold with 1 mL of cell suspension at a density of 5 × 107 cell/mL to form cell-scaffold constructs and then kept in an incubator for 2 h. Afterwards, both cell-seeded and cell-free scaffolds were coated with 2% (20 mg/mL) cross-linked sodium hyaluronate gel.
Surgical procedure
The rabbits were anesthetized with intramuscular injection of ketamine (10 mg/kg) and Lumianxin (5 mg/kg) and laid prone; then the right posterior parts of their legs above the ankle joint were shaved and sterilized with 0.1% benzalkonium bromide tincture. A midline skin incision was made, and subcutaneous tissues were divided followed by segmental resection of 1.5-cm-long tendon fragment to create a partial tendon defect of Achilles tendon as previously described. 16 Afterwards, both ends of the severed tendon were allowed to retreat by themselves and resulted in a defect about 3 cm in length. The defect was bridged with a 3-cm long cell-seeded construct or cell-free scaffold using 5–0 nonabsorbable suture material in a Kessler core pattern to connect the ends of severed tendons and the construct. This method was applied to all three groups (Fig. 1). The skin over the lesion was closed using 3-0 silk suture in a simple interrupted suture pattern. The rabbits were returned to the cages for their free activities after surgical procedure.
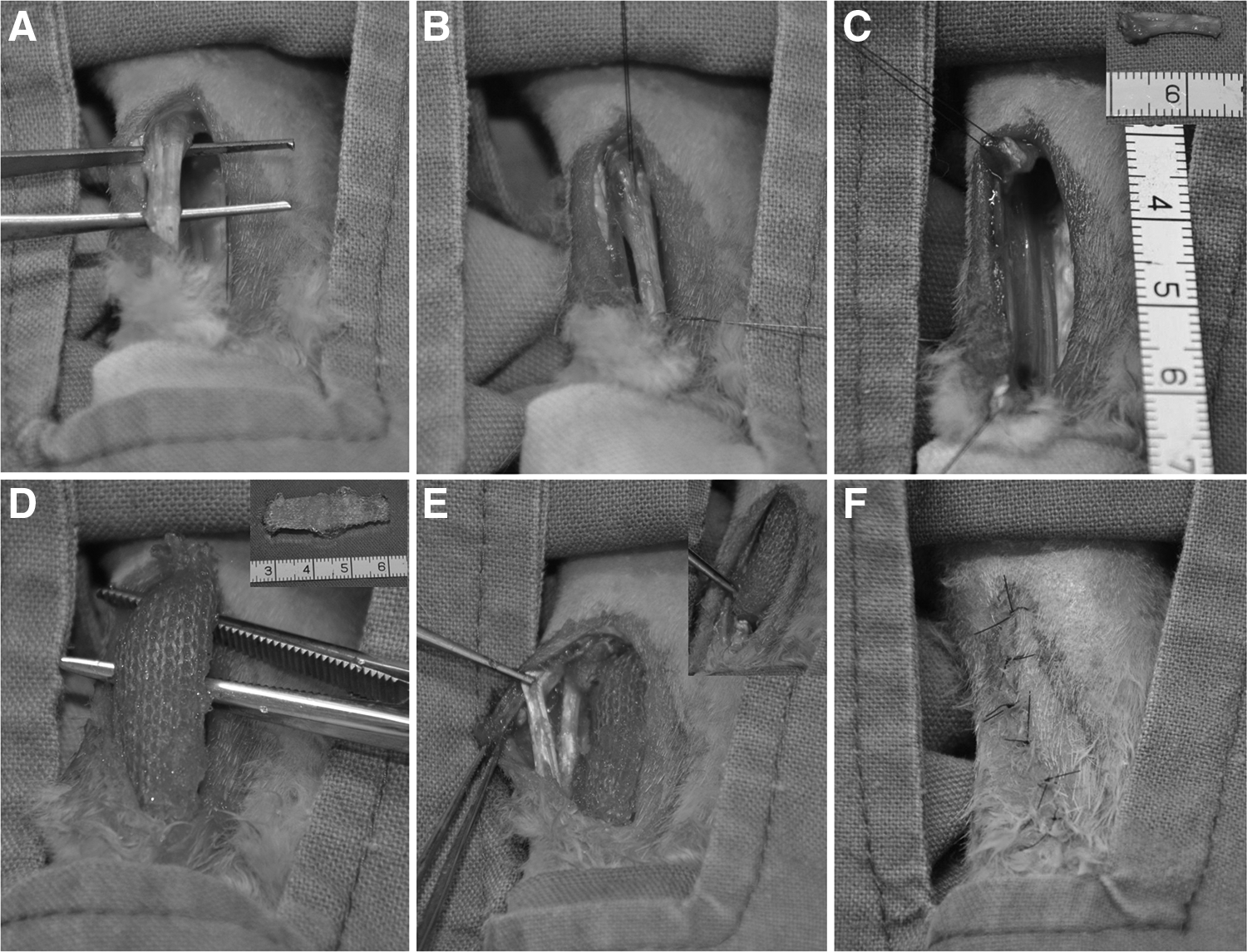
Surgical procedure of repairing Achilles tendon defect in a rabbit model.
Macrographic examination of in vivo engineered tendon
At 7 and 13 months postsurgery, animals were sacrificed with overdose of drug injection and each of engineered tendons harvested from three groups was carefully examined for the levels of hyperemia, peritendinous adhesions, general appearance, nearby muscle atrophy, and interface healing between engineered and host tendons.
Hematoxylin and eosin staining
The harvested tissue examples of in vivo engineered tendons were fixed in 4% paraformaldehyde overnight, washed in PBS, and dehydrated through graded alcohols and paraffin embedding. The samples were then sectioned parallel to the longitudinal axis of the engineered tendons with a thickness of 5 μm using a microtome. These sections were stained with hematoxylin and eosin (H&E) staining for visualizing PGA degradation, cellular density, collagen production and alignment, and the interface healing between engineered and host tendons under light microscopy. The sample size for the procedure was n = 5 for 7 months and n = 7 for 13 months in cell-free group; n = 3 for 7 months and n = 5 for 13 months in autologous group; and n = 4 for both 7 and 13 months in allogenic group.
Histological scoring and semiquantitative analysis
As reported in previous studies,24–27 general histological scoring and semiquantitative analysis were performed based on H&E staining. Eight parameters (fiber structure, fiber arrangement, roundness of nuclei, inflammation, vascularity, density of cells, biodegradation, and interface) were assessed based on H&E staining results. These eight parameters were semiquantitatively graded into four-point scoring system (0 normal, 1 slightly abnormal, 2 moderately abnormal, and 3 markedly abnormal). Animals were sacrificed, respectively, at the time points of 7 months for the analysis after H&E staining (n = 3 for autologous; n = 4 for allogeneic; and n = 5 for cell-free group) and 13 months for the analysis (n = 5 for autologous; n = 4 for allogeneic; and n = 7 for cell-free group) postsurgery for histological evaluation. The evaluation was performed by two observers blindly. All these data are presented as mean ± standard deviation.
TEM examination
To reflect collagen formation and superstructure of tissue specimens at months 7 and 13 postrepair, a transmission electron microscope (Quanta 200 FEI) was used to examine the distribution and diameter of collagen fibrils in the engineered and native tendons. Briefly, middle part of the samples was first fixed in cold 2% glutaraldehyde, dehydrated in graded ethanol, and then embedded in EPON resin. Transverse and vertical ultrathin sections (n = 3 for each group) were prepared. In addition, the diameter of the collagen fibrils at different fields of the same magnification ( × 65,000) for each tissue cross-section was measured and calculated by KS400 Image analysis software (version 3.0; Zeiss), and about 50 collagen fibrils were randomly selected from each one of two images of each tissue sample to measure and obtain an averaged diameter of the collagen fibrils. All these data are presented as mean ± standard deviation.
Biomechanical analysis
After the animals were sacrificed either at 7 or 13 months postsurgery, the freshly harvested tissue samples were immediately subjected to mechanical property analysis using a biomechanical analyzer (Instron 4411, Canton, MA) as previously reported.16,28 The tested tissue with a length of 1.5 cm was fixed between two gripper of both ends, and the tissues were stretched at a speed of 25 mm/min, and then the maximal load (N) was measured by the load-deformation curve until tissue rupture. Tensile strength (MPa) was derived from the dividing of the maximal load with the cross-sectional area of the tissue, whereas Young's modulus (MPa) was calculated from the linear slope of a stress–strain curve as previously described. 28 All these data are presented as mean ± standard deviation. The sample sizes for this analysis were autologous group (n = 4 for 7 months and n = 3 for 13 months), allogeneic group (n = 5 for 7 months and n = 3 for 13 months), and cell-free group (n = 6 for both 7 and 13 months).
Statistical analyses
All data were presented as mean ± standard deviation. After confirming the normal distribution of the data, the significant differences in the measured values among different groups at a particular time point were statistically analyzed with one-way ANOVA. In addition, least significant difference of Post hoc test was applied to analyze the difference in the data between two time points of the same group. Due to the heterogeneity of variance of average diameters of collagen fibers at 7 months postsurgery and the Young's modulus data at 13 months postsurgery among different groups, nonparametric test (Kruskal–Wallis H test) analyses were used to detect the statistical difference among three groups, and Dunn test was applied to analyze the difference between two groups. All statistical analyses were performed using statistical software SPSS (version 19.0; SPSS, Inc., Chicago, IL). A p-value less than 0.05 (p < 0.05) was considered statistically significant.
Results
Dermal fibroblast culture
During in vitro cell culture, the primary fibroblasts appeared in heterogeneous cell shapes and exhibited apparent refraction. These cells spread gradually with reduced refractivity after 24 h. After subculture, passaged cells usually grew much faster and could reach confluence in 3 days. As shown, during cell passages, these cells exhibited a spindle shape (Fig. 2A, B, E, F). Dermal fibroblasts derived from GFP rabbits also revealed similar cell morphology with apparent green color of GFP under fluorescence light (Fig. 2C, D, G, H).

Cell morphology observation. The morphology of rabbit fibroblasts was observed under inverted phase-contrast microscopy for regular fibroblasts
Gross view of in vivo repaired tendon
At 7 months postrepair, an immature tendon-like tissue was found in two harvested tissue samples of cell-free group, in which no obvious material residues were observed (Fig. 3A and Table 1). However, in other four animals of the same group, scaffold materials of knitted PLA/PGA nets remained largely observable along with formed connective tissue at the implantation site (Fig. 3D and Table 1). In allogeneic group, relatively more matured tendon-like tissues were formed in two harvested samples with less adhesion to surrounding tissue and no obvious residues of scaffold materials (Fig. 3B and Table 1). However, knitted net materials remained largely observable in the harvested tissue samples of other three rabbits of the same group (Fig. 3E, Table 1). Similarly, in autologous group, relatively more mature tendon-like tissue was formed in one rabbit with moderate adhesion to surrounding tissue and no obvious scaffold materials left (Fig. 3C and Table 1). In other three rabbits of the same group, undegraded PLA/PGA knitted net materials along with formed connective tissues remained observable (Fig. 3F and Table 1). There seemed no obvious difference among three groups in gross view at this time point.
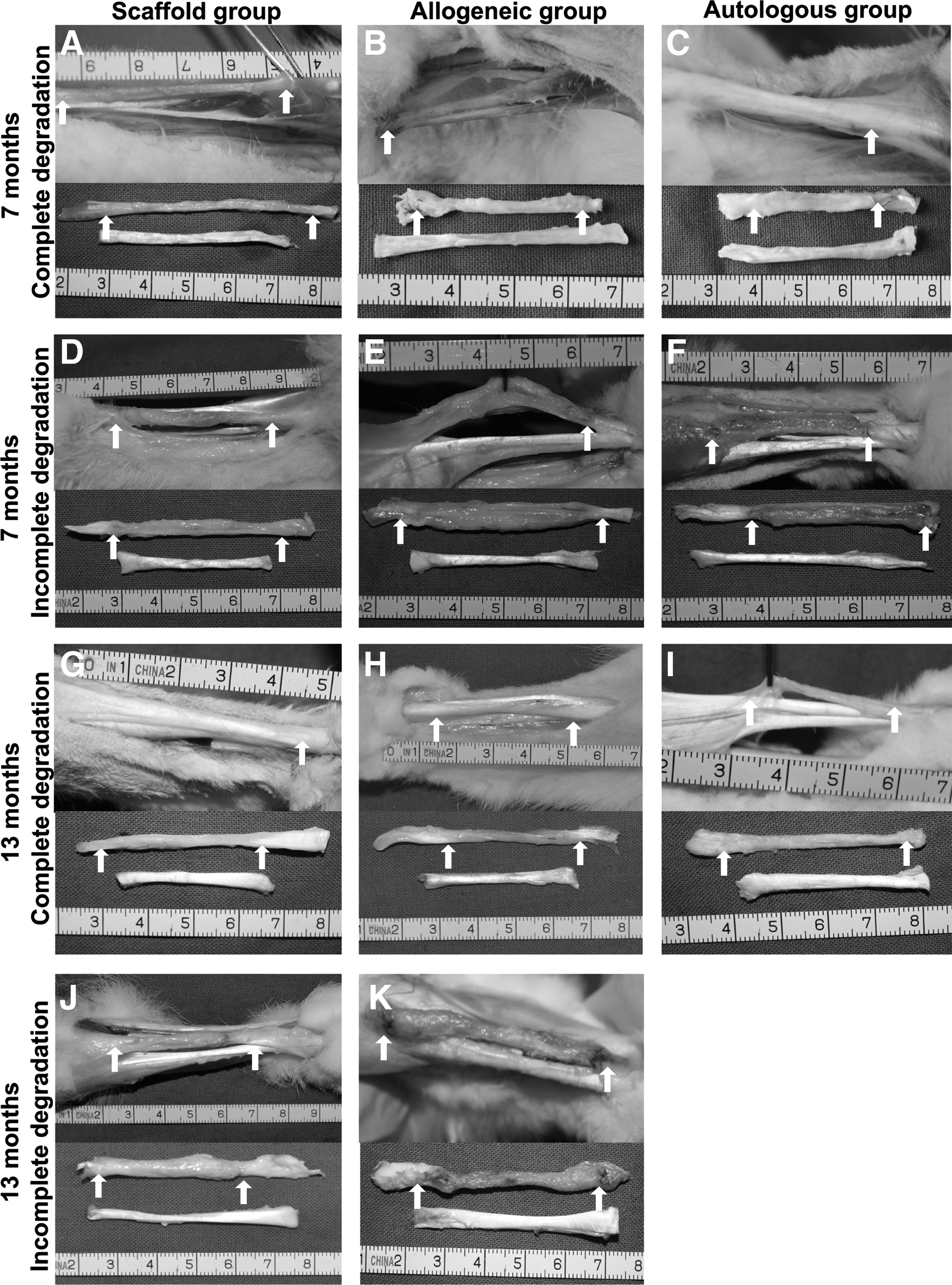
Gross view of the engineered tendons at 7 months
At 13 months postrepair, two samples of the cell-free group formed more mature tendon-like tissues without obvious material residue and less adhesive to surrounding tissue (Fig. 3G and Table 1) compared with the same group tissues of 7 months (Fig. 3A). Still, other five samples of cell-free group formed irregular connective tissue with obvious undegraded net materials encapsulated inside formed fibrotic tissue (Fig. 3J and Table 1). In allogenic group, four out of five harvested samples formed relatively mature tendon-like tissues with less fibrotic adhesion to the surrounding tissues and no apparent net materials left (Fig. 3H and Table 1), whereas only one sample exhibited undegraded scaffold material and apparent fibrotic adhesion to surrounding tissue (Fig. 3K and Table 1). By contrast, at 13 month time points, all of five harvested samples of autologous group formed engineered tendons which exhibited a relatively shiny white and cord-like shape with a relatively smooth surface and no scaffold left. The engineered tendons became relatively more comparable to the normal tendon and were easily separable from nearby host tissue (Fig. 3I and Table 1).
Biomechanical analysis
In this study, maximal load, tensile strength, and Young's modulus serve as the parameters for mechanical property analyses. As shown in Figure 4A, the maximal load at 7 months postsurgery for cell-free scaffold, allogeneic, and autologous groups were, respectively, 12.91 ± 2.84 N, 13.50 ± 5.06 N, and 16.69 ± 3.12 N. Statistical analysis showed no significant difference in the maximal load among three groups (p > 0.05) and no significant difference in any of the paired comparison of three groups (p > 0.05). The maximal load at 13 months postsurgery for cell-free scaffold, allogeneic, and autologous groups was, respectively, 12.09 ± 4.02 N, 12.64 ± 4.70 N, and 15.41 ± 4.13 N. No significant difference was found as well among three groups as revealed by statistical analysis (p > 0.05). Similarly, no significant difference was found in any of the paired comparison among three groups (p > 0.05). In addition, the maximal load for native tendon was 19.12 ± 1.33 N, which was significantly higher than those of cell-free and allogeneic groups at 7 and 13 months postsurgery (p < 0.05), but was not significantly different from that of autologous group of both time points (p > 0.05). In the same group, no significant difference in the maximal load could be found between two time points (p > 0.05).
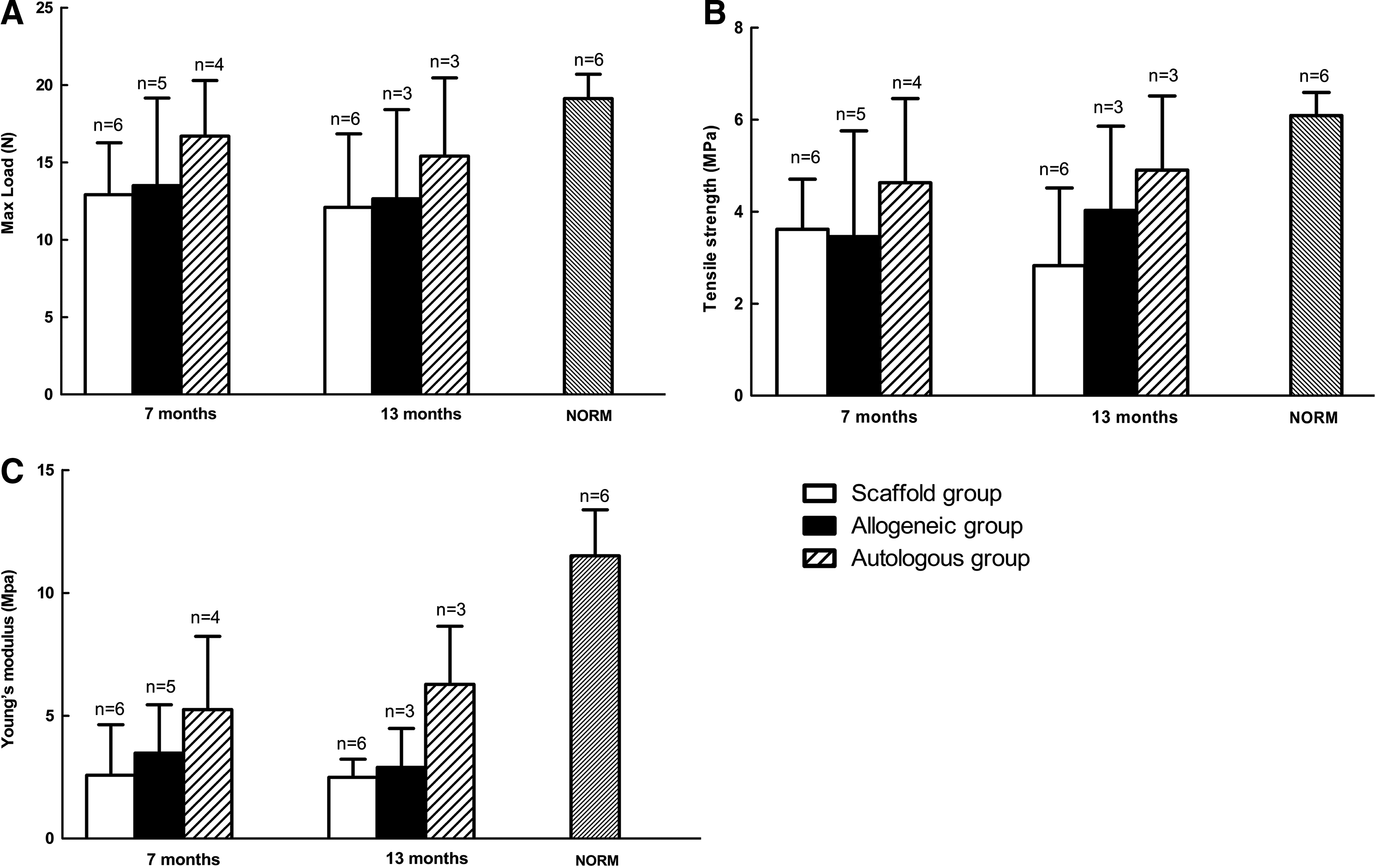
Mechanical property analysis of engineered tendons. Quantitative analyses of maximal load
As shown in Figure 4B, the tensile strength at 7 months postsurgery for cell-free scaffold, allogeneic, and autologous groups was, respectively, 3.62 ± 0.99 MPa, 3.46 ± 2.06 MPa, and 4.63 ± 1.58 MPa. Statistical analysis showed no significant difference among three groups (p > 0.05) and no significant difference in any of paired comparisons of three groups (p > 0.05). The tensile strength at 13 months postsurgery for cell-free scaffold, allogeneic, and autologous groups was, respectively, 2.83 ± 1.54 MPa, 4.03 ± 1.50 MPa, and 4.91 ± 1.31 MPa. No significant difference could be found among three groups (p > 0.05) and no significant difference in any of paired comparisons (p > 0.05). However, the tensile strength of native tendon (6.09 ± 0.46 MPa) was significantly higher than those of cell-free group and allogeneic groups at both time points (p < 0.05), but not significantly different from those of autologous group at both time points (p > 0.05). In the same group, no significant difference in the tensile strength could be found between two time points (p > 0.05).
As revealed in Figure 4C, the Young's modulus at 7 months postsurgery for cell-free scaffold, allogeneic, and autologous groups was, respectively, 2.58 ± 1.87 MPa, 3.48 ± 1.76 MPa, and 5.25 ± 2.58 MPa. There was no significant difference in the Young's modulus among three groups (p > 0.05) and no significant difference in any of the paired comparisons among three groups (p > 0.05). At 13 months postsurgery, the Young's modulus for cell-free, allogeneic, and autologous groups was, respectively, 2.49 ± 0.67 MPa, 3.36 ± 1.29 MPa, and 6.28 ± 1.93 MPa and statistical analysis showed no significant difference in the Young's modulus among three groups (p > 0.05). In addition, the Young's modulus of native tendon (11.51 ± 1.68 MPa) was also significantly higher than that of cell-free group (p < 0.05), allogeneic group (p < 0.05), and autologous group (p < 0.05) at both time points of 7 and 13 months. In the same group, no significant difference in the Young's modulus could be found between two time points (p > 0.05).
Histological analysis
At the time point of 7 months postrepair, the scaffold materials had completely degraded in some of harvested tissue samples (Fig. 5A–F), while they remained partially undegraded in other tissue samples (Fig. 5G–L). Among three groups, good interface healing was observed between implanted construct and the host tissue in those of harvested tissue samples, where the scaffold materials were completely degraded (Fig. 5A–C). In general, it seemed that the formed tendon tissues in cell seeded groups were comparatively more organized than in cell-free group in terms of collagen fiber arrangement, cell density, interface healing, and degradation of scaffold materials. As shown in Figure 5D–F (middle part of the grafts), similar cell density was observed among three groups. Collagen and cell alignment were relatively better organized in cell-seeded groups than in cell-free group. For the harvested tissue samples that contained part of undegraded materials (arrowed), interface healing and tissue maturation were relatively poorer (Fig. 5G–I) compared to those with completed degradation of scaffold materials (Fig. 5A–C). In addition, both fibroblasts and inflammatory cells were observed. There were no GFP-labeled cells that could be detected under fluorescence microscope from the tissues of both time points of 7 and 13 months postsurgery.
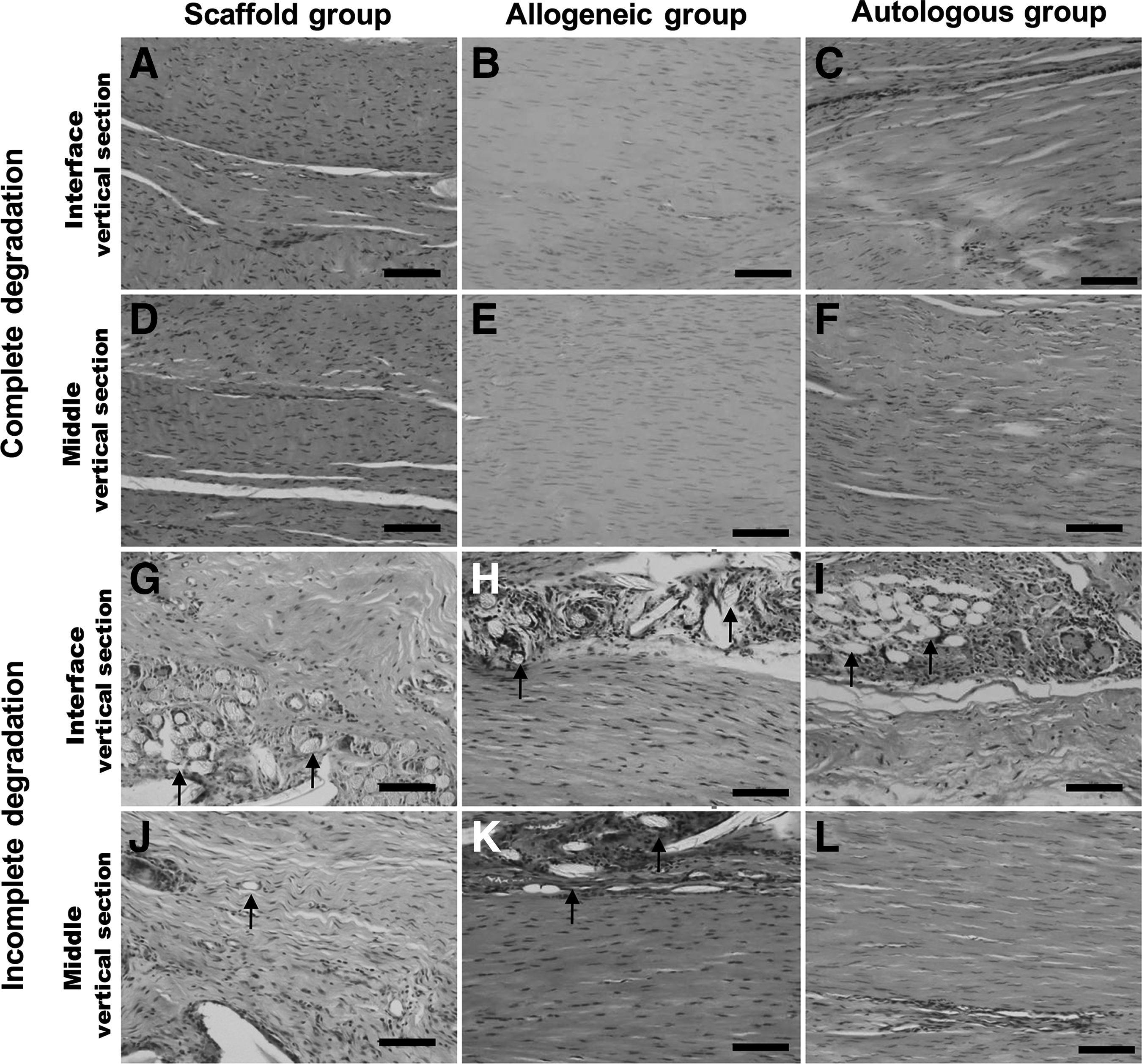
Histological evaluations (H&E) of regenerated tendon at 7 months postimplantation for engineered tendons with complete scaffold degradation
After H&E staining, the stained tissue samples were subjected to tissue quality evaluation. As shown in Figure 7, there was no significant difference in tissue score among all three groups (p > 0.05) at the time point of 7 months postsurgery.
At the time point of 13 months postsurgery, better interface healing could be observed in the harvested tissues with scaffold completely degraded (Fig. 6A–C) compared with those of 7 months (Fig. 5A–C). In the middle part, tendon tissues were much better developed with more organized tissue structure compared with 7 month histology. Collagen and the cells were aligned in parallel and cell density was relatively lower (Fig. 6D–F) than those of 7 months (Fig. 5D–F), indicating that tissue remodeling under mechanical loading in vivo further enhanced tissue maturation. At this time point, it seemed that there was no significant difference in tissue structures of all three groups.
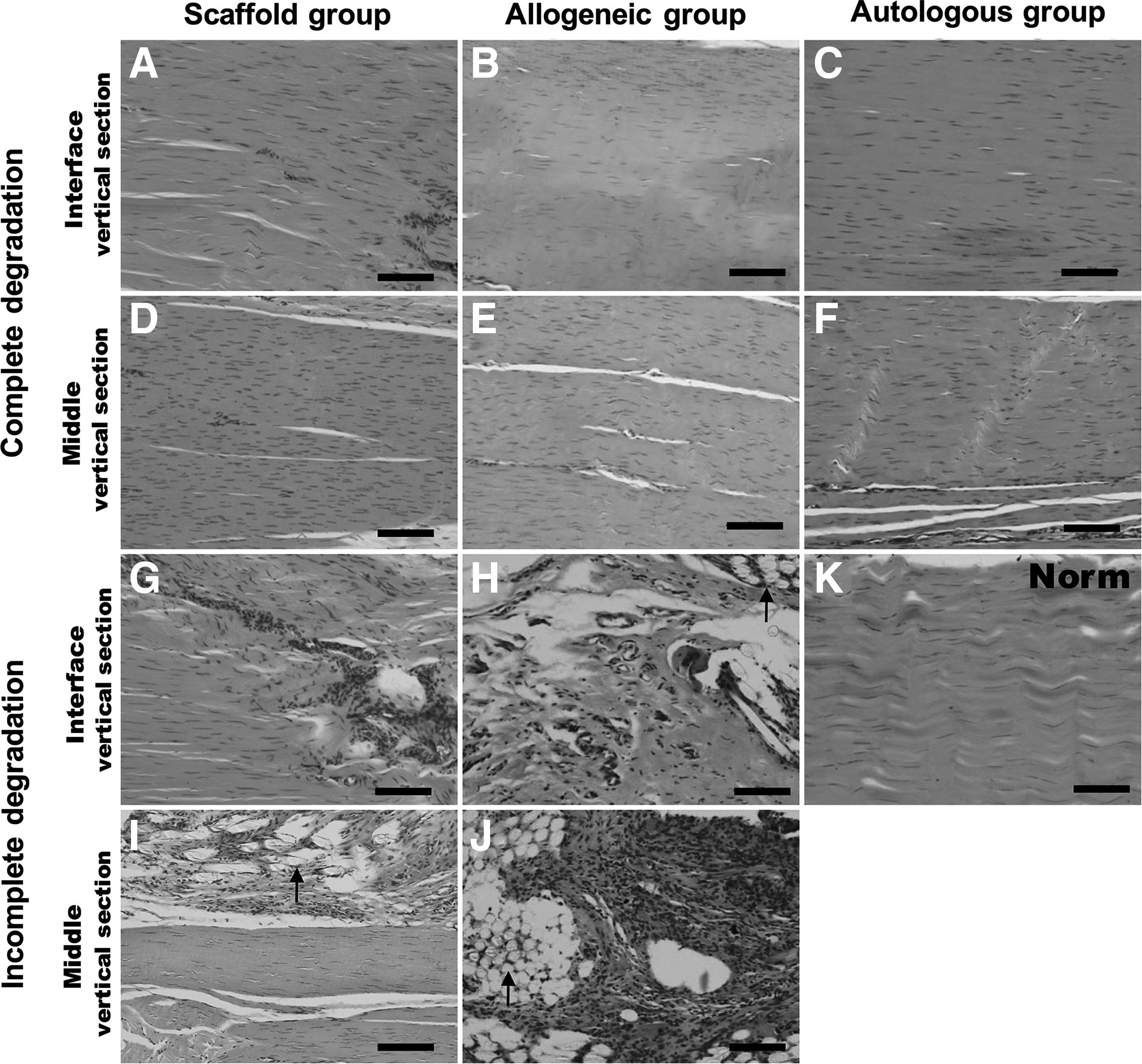
Histological evaluations (H&E) of regenerated tendon at 13 months postimplantation for engineered tendons with complete scaffold degradation
In agreement with the gross view, undegraded scaffold materials remained observable, in part, of harvested tissues of both cell-free and allogeneic groups; their interface healing and tissue maturation were much poorer (Fig. 6G, H, I, J) than those with scaffold completely degraded (Fig. 6A, B, D, E). Likewise, histological score analysis of all tissue samples harvested at 13 months postsurgery reveals no significant difference among three groups (p > 0.05, Fig. 7).
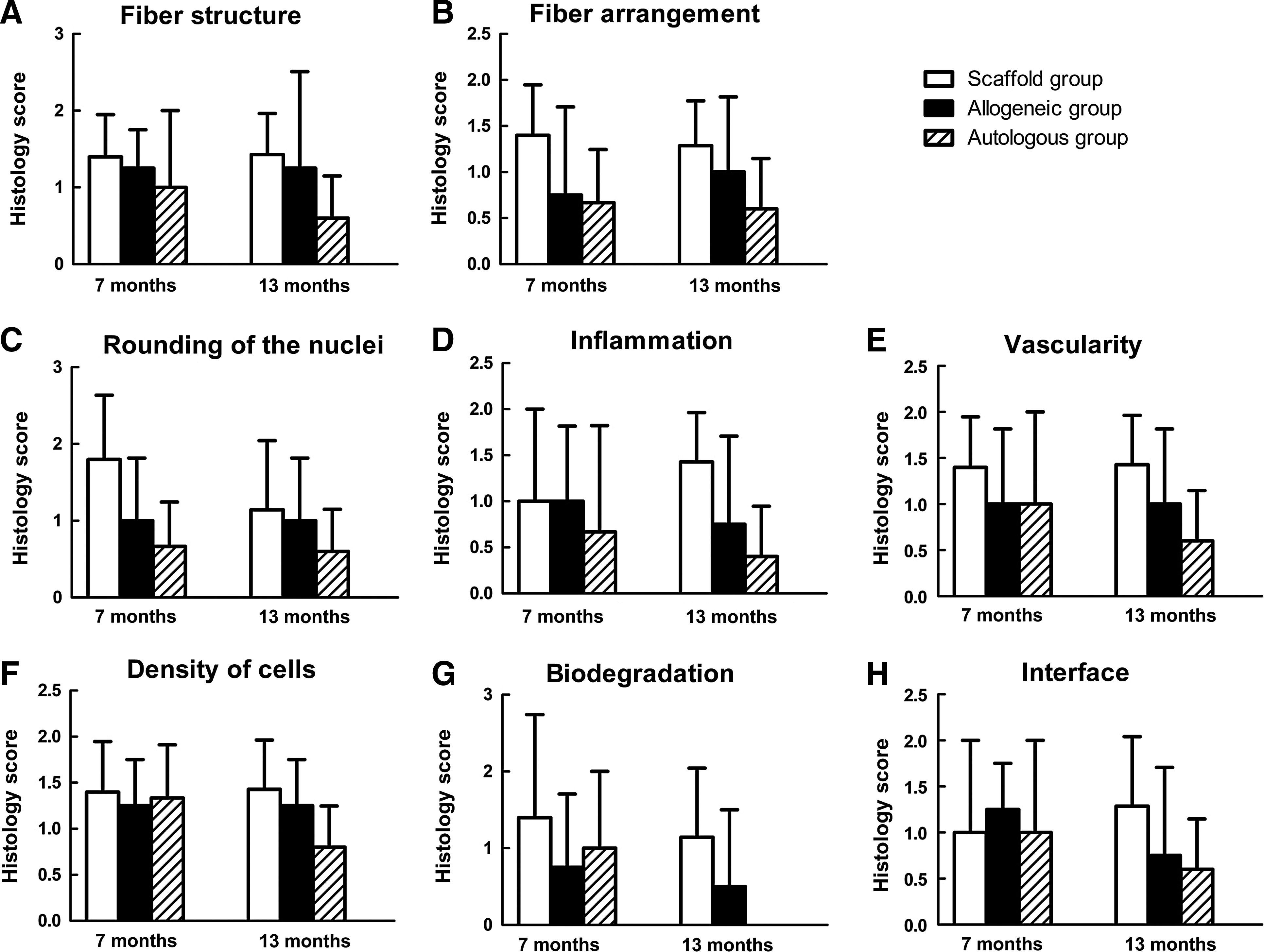
Histological score analysis of engineered tendons of three groups. The included parameters are fiber structure
Distribution and diameter of collagen fibrils
At 7 months postrepair, there was no significant difference in the average diameters of collagen fibrils between cell-free scaffold (66.60 ± 13.73 nm) and allogeneic groups (72.22 ± 7.37 nm) (p > 0.05) (Fig. 8A, B, D, E, O) and between allogeneic and autologous groups (83.72 ± 6.62 nm) (p > 0.05) (Fig. 8B, C, E, F, and O). There is no significant difference among all three groups. The parallel aligned collagen pattern was found in all three groups (Fig. 8D–F).

Collagen superstructure of in vivo regenerated tendons and quantitative analysis. Transmission electronic microscopic images of collagen superstructures for cell-free group
At 13 months postrepair, the collagen fibril diameters of cell-free group were 65.29 ± 6.72 nm, which was significantly smaller compared with autologous group (82.15 ± 7.53 nm, p < 0.001) (Fig. 8G, I, J, L, and O). The diameter of allogeneic group (71.69 ± 3.07 nm) was not significantly different from that of cell-free group (p > 0.05) (Fig. 8G, H, J, K, and O), but was significantly smaller compared with autologous group (p < 0.05) (Fig. 8H, I, K, L, and O). There is significant difference in collagen fibril diameter among three groups (p < 0.05). Engineered tendons became more mature with the development of D-band periodicity structure in all three groups (Fig. 8J, K, and L) compared to those of 7 months (Fig. 8D–8F). Among all three groups, there was no significant difference in fibril diameter between two time points of the same group.
However, the collagen fibrils of engineered tendons remained relatively thinner and immature compared to the fibril diameter and superstructure of normal tendon fibrils (Fig. 8M–O), Instead, the native tendon exhibited a bipolar pattern (Fig. 8M) and thick collagen fibrils with diameter of 229.27 ± 47.27 nm (Fig. 8N), which is significantly different from that of engineered tendons (p < 0.05).
Discussion
In traditional tissue engineering approach, autologous cell source is an essential component and, thus, remains to be an individual based therapeutic approach. It has been shown that allogeneic cell based engineered tissue usually serve as biological wound dressing such as engineered skin (Apligraf) 29 or as a biological tissue template which can temporally repair the defected tissue and then be replaced by host cell based tissue remodeling. 30 By contrast, the usage of cell-free inductive biomaterials has become an attractive approach for tissue regeneration because it can be universally applied to all different patients without the concern of immune rejection and, thus, become a truly tissue regenerative product.
Tendon is a dense connective tissue, which plays a functional role in transmitting muscle contraction force into extremity movement. Allogeneic tendon graft has been used for tendon repair with no confirmed therapeutic value possibly due to the risks of disease transmission and immune rejection.31,32 Different from native tendon graft, engineered tendon at initial stage was composed of porous scaffold and seeded cells, which presents as a loose structure that enables the infiltration of host cells into the engineered graft and the replacement of seeded allogeneic cells after its in vivo implantation. It was previously reported that the use of allogeneic MSCs was able to regenerate Achilles tendon in a rabbit model. 20 In addition, cell-free scaffold was also used to regenerate tendon with success.18,19 However, all these studies were performed in different animal models with different experimental settings.
We thus performed a side-by-side comparative study of autologous, allogeneic, and cell-free approaches to evaluate their efficacy and efficiency in tendon regeneration using the same model of rabbit Achilles tendon and the same scaffold materials as previously reported. 16 In general, the results of this study showed that all three approaches were possible to regenerate tendon tissue when eventually evaluated at the time point of 13 months postimplantation with slight differences in scaffold degradation rate, histologic structure, and collagen superstructure of formed tissues.
It was observed that there was apparent variation in the degradation rate of scaffold materials. As shown in both gross view and histology (Figs. 3, 5, and 6), some of harvested samples formed good quality tissue with complete degradation of scaffold materials, whereas other samples formed relatively less organized tissue with undegraded scaffold. This might be caused by varied mechanical loading on cell-free or cell-seeded scaffold materials. As previously described, 16 only part of Achilles tendons (one of three parts) was severed, and thus, the construct was partially subjected to the mechanical loading. Therefore, variation in mechanical loading on individual constructs of different groups was likely to happen.
Indeed, existing evidences indicate that mechanical loading plays an important role in recruiting host cells into the scaffold. It has been shown that mechanical stimulation is important for recruiting cells to regenerate the tissue types that often bear mechanical loading, including bone, cartilage, blood vessel, muscle, and tendon/ligament.5,19,33–35As previously reported, 16 a partial Achilles tendon repair model was used in this study by the section of partial Achilles and its repair; thus unsectioned part of Achilles tendon remained able to partially bear the contraction force and thus avoid the full loading of mechanical force on the implanted scaffold. In the future, repair of full sectioned Achilles tendon with implanted scaffold materials will be the direction of our study to observe the effect of full mechanical loading on tendon regeneration.
Interestingly, seeded cells do seem to play a role in enhancing scaffold degradation. As shown in Table 1, at 13 months postsurgery, all five samples of autologous group exhibited completed degradation of scaffold materials, whereas other two groups remained to have a few samples with retained scaffold materials.
Although not investigated in details for the immunological aspects, it seemed that implanted allogenic cells were eventually replaced with host cells. To trace the fate of implanted allogeneic cells, a GFP transgenic rabbit model was used to extract allogeneic GFP dermal fibroblasts for implantation into regular rabbit tendon defect. As shown in Figure 2, the GFP labeled cells exhibited cell morphology similar to those of dermal fibroblasts derived from regular rabbits. However, after 7–13 months of in vivo implantation, the tissue harvested from allogeneic group revealed no GFP signals (data not shown), indicating that the implanted cells might be replaced by the host autologous cells during the long-term tissue remodeling process. The reasons for failed observation of GFP cells in the early time may also include cell replication, normal turnover, cell death, or loss of the signal.
In situ tissue regeneration using inductive materials has become an important strategy for tissue regeneration. This has apparent advantages over traditional cell-based tissue regeneration strategy, as it overcomes the limitation of individual based therapy and is theoretically possible to treat different individual patients. Recent literature reports also demonstrated that modification of scaffold materials with bioactive molecules such as peptides, extracellular matrices, and growth factors is the proper means to fulfill the goal, because these modifications are able to help recruit host cells into the scaffold for infiltration, adhesion, proliferation, and tissue regeneration.4,10,18,36
Different from our previous studies,16,23 cross-linked hyaluronic acid gel was applied to the scaffold with its coating on the net materials; this may enhance the biocompatibility of the scaffold and tissue regeneration, and this also explains that regenerated tendon formation occurred as well in some of the implanted cell-free scaffolds. In addition to the properties of the implanted scaffold, the local environments of the implantation sites may also contribute to the recruitment of host cells for tissue regeneration such as vascularization status, soluble signals, and host stem cell populations. 4
The shortcoming of this study is the relatively small sample size due to animal death, which may become difficult to achieve statistically significant difference between autologous group and other two groups in some of examined parameters. Even the possibility of better tendon regeneration in autologous group cannot be excluded given a bigger sample size; the fact of formed tendon tissue in both cell-free and allogenic groups indicates the feasibility of engineered tendon regeneration of all three approaches.
Conclusion
In conclusion, this pilot study demonstrates the feasibility of autologous, allogeneic cell based, and cell-free scaffold approaches in tendon regeneration, despite there being differences in histological structure and superstructure of formed tissues and degradation rate of implanted scaffold and the success rate. Although not investigated in detail, immune rejection of implanted allogeneic cells seemed to exist. More importantly, further studies on the effect of local niche environment and modification of tendon scaffolds will be the very important step towards cell-free scaffold approach.
Footnotes
Acknowledgments
This study was supported by the National Natural Science Foundation (31470943, 31170937, 81101359) and National “863” (2012AA020507) and “973” (2005CB522703) Project Foundation.
Disclosure Statement
No competing financial interests exist.