
Abstract
Produced through electrospinning, poly(
Introduction
W
An ideal wound dressing should not only act as a barrier to microorganisms but also be made from biocompatible, nontoxic, and nonallergenic materials, and it should maintain a moist environment at the wound interface, allowing gaseous exchange and the removal of excess exudates. Current research strategies are focused on the acceleration of wound repair using systematically designed dressing materials that add a variety of functionality to the basic wound healing requirements. Many researchers have described antimicrobial dressings that use silver nanoparticles,3–6 but there has also been research into wound dressings that use chitin and its derivative chitosan, which are biocompatible, biodegradable, nontoxic, antimicrobial, and hydrating agents.7–10 Several studies have investigated growth factors such as vascular endothelial growth factor (VEGF) to promote angiogenesis near the wound dressing. Angiogenesis, which is the physiological process of new blood vessel formation from preexisting vessels, occurs during the proliferation phase of the wound healing process.11–13 Angiogenesis is usually a minor problem in the case of small wounds, but severe wounds such as ischemic chronic wounds and diabetic wounds with delayed wound healing can result in scarring because absent or insufficient angiogenesis prevents movement of fresh nutrients and oxygen to the wound site.14–16 Although angiogenesis has an important role in wound healing, there is a lack of research on wound dressings and their effect on angiogenesis. In this regard, our study focused on the development of a wound dressing with pro-angiogenic characteristics.
Electrospinning is a fiber production method that uses an electric force to draw charged threads from polymer solutions or polymer melts. Thread diameters are in the order of some tens of nanometers.
17
This technique can be used to create porous, high surface area structures by regulating fiber diameter with the fiber diameter controlled by electrospinning voltage and polymer solution concentration. Such structures are effective in the inhibition of exogenous microorganism invasion, maintenance of moist environment, gaseous exchange, and removal of excessive exudates, which are the basic requirements for an effective wound dressing.
18
Poly(
Figure 1 shows a schematic diagram of the overall study. We fabricated a nanofibrous electrospun hdECM-based hybrid scaffold (NEhdHS) through electrospinning of a rat hdECM hydrogel mixed with PLCL dissolved in 1,1,1,3,3,3-hexafluoroisopropanol (HFIP). Human dermal fibroblasts (HDFs) were seeded on the front side of the NehdHS, and human umbilical vein endothelial cells (HUVECs) were seeded on the back side of the scaffold. Subsequently, the HDFs-HUVEC-seeded NEhdHS was folded over and over again and then cultured in an incubator before being used to investigate the angiogenic activity of the NEhdHS in vitro. To confirm the effect of NEhdHS as a pro-angiogenic, scar-reducing wound dressing in vivo, full-thickness skin wounds (10 mm diameter) were made aseptically on rat dorsa using a biopsy punch. The NEhdHS was then treated to the wounds along with either a PLCL scaffold or a gelatin-containing PLCL scaffold.
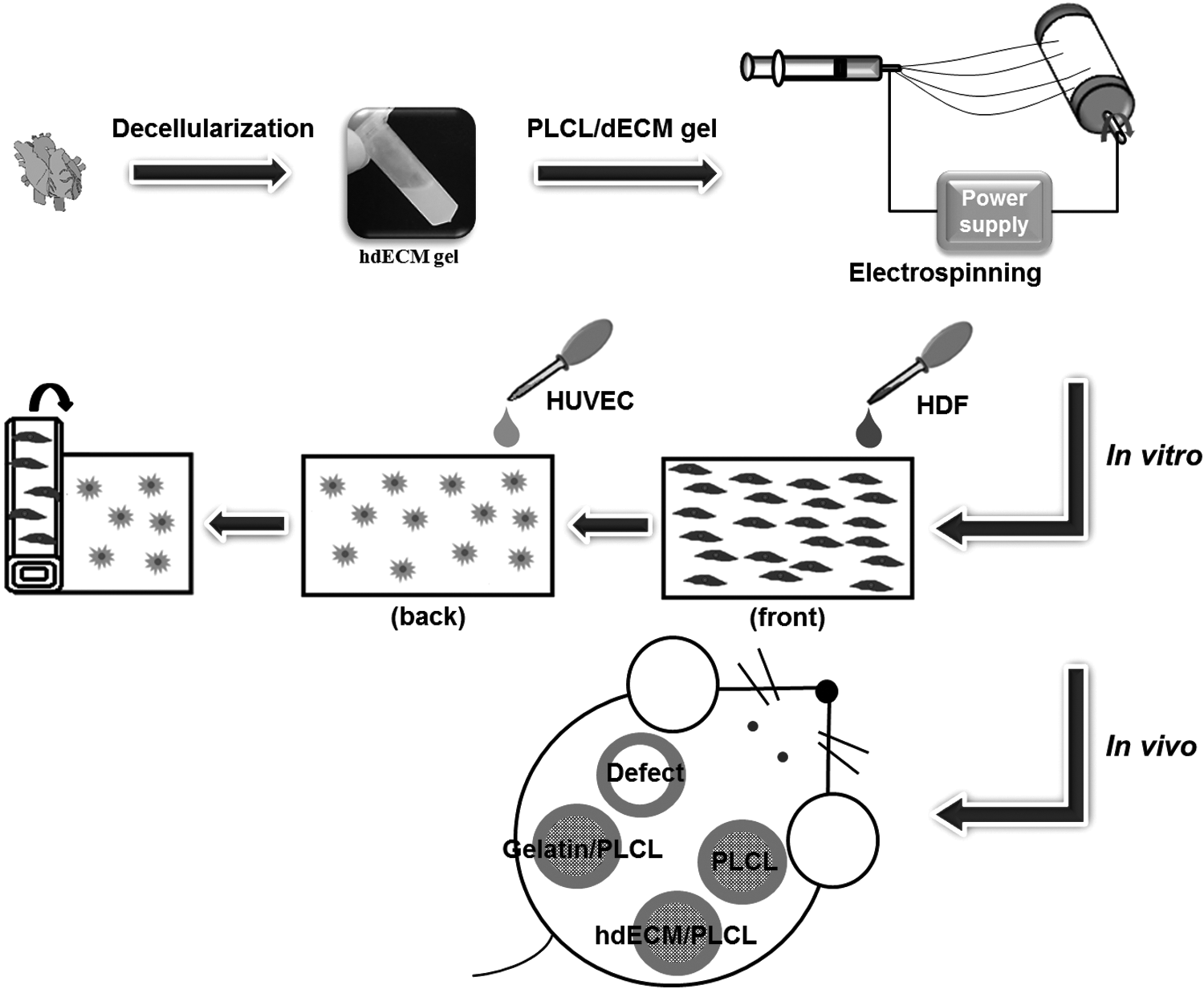
Schematic diagram outlining the investigation of a NEhdHS developed for effective wound healing as a pro-angiogenic therapy. The NEhdHS was fabricated using hdECM gel mixed with a biocompatible and biodegradable polymer, PLCL, by applying an electrospinning technique. The NEhdHS on which HDFs were seeded on the front side and HUVECs on the back side was first folded to create multiple folds and then cultured in an incubator to determine pro-angiogenic ability in vitro. The NEhdHS was treated on wounds of an excisional wound rat model, along with PLCL only and gelatin-containing PLCL scaffolds, to elucidate the features of NEhdHS as a pro-angiogenic and scarless wound dressing in vivo. hdECM, heart decellularized extracellular matrix; HDFs, human dermal fibroblasts; HUVECs, human umbilical vein endothelial cells; NEhdHS, nanofibrous electrospun hdECM-based hybrid scaffold; PLCL, poly(
Materials and Methods
Materials
Decellularization of tissues
All animals were treated in accordance with standard operating protocols of the Institutional Animal Care and Use Committee at our Biomedical Research Institute. All protocols for Animal Experiments were approved by the Institutional Review Board of Animal Experiments at our institute.
To manufacture the electrospun nanofibrous PLCL/hdECM scaffold, heart tissue of outbred Sprague-Dawley rats (SD rats; Narabio, Seoul, Korea) was used. We euthanized male 8-week-old outbred SD rat with 400 mg/kg avertin (2, 2, 2-Tribromoethanol; Sigma) injected intraperitoneally and then removed the heart. Heart tissue decellularization was conducted by following a protocol published elsewhere, but with slight modification. 31 Heart tissues were chopped into pieces ∼1 mm thick. The chopped heart tissue was stirred in 1% sodium dodecyl sulfate (SDS; Invitrogen, Waltham, MA) in deionized water (DW) for 12 h followed by treatment with 1% Triton X-100 (Biosesang, Sungnam, Korea) solution in DW for 30 min. The decellularized heart tissue was washed using antibiotic-containing (5% penicillin-streptomycin solution, 100 × ; Corning, Corning, NY) phosphate-buffered saline (PBS; Welgene) for 3 days.
To investigate angiogenic cytokines in various decellularized organ tissues, we used male 8-week-old Imprinting Control Region (ICR) mice (Narabio). For that investigation, heart tissue was obtained and decellularized using the same procedure as that used for rat heart tissue.
Mouse liver tissue was decellularized by following a protocol published elsewhere, but with some modification 32 Briefly, minced liver was stirred in 0.01% SDS for 24 h and then stirred with 0.1% SDS for 24 h, with 1% SDS for 24 h, and then treated with 1% Triton X-100 for 30 min to remove residual SDS. Decellularized liver tissues were washed with antibiotic-containing PBS for 1 h.
For decellularization of mouse lung tissue, chopped lung tissue was stirred in 0.1% SDS for 120 min, followed by stirring for 10 min with 1% Triton X-100. Antibiotic-containing PBS was used to wash the lung tissue for 3 days.
To decellularize mouse kidney tissue, we chopped the kidney tissue into pieces less than 1 mm thick and stirred them in 1% SDS for 12 h followed by stirring in 1% Triton X-100 for 30 min. After decellularization, we washed the kidney tissue with antibiotic-containing PBS for 3 days.
Mouse skin was procured by euthanizing BALB/c nude mice. The skin was decellularized by following a protocol published elsewhere, but with some modification. 33 Blood and tissue debris was removed by washing the skin in PBS solution. After chopping the skin into small pieces, the pieces were stirred in hypertonic solution (605 mg tris base, Sigma; 4 g sodium chloride, Sigma; and 202.5 mg EDTA, Sigma, all in 100 mL PBS) for 8 h for de-epithelialization; next, the dermis was decellularized using 1% sodium deoxycholate (Sigma) for 48 h.
Analysis of dECM angiogenic cytokines
To confirm the presence of residual angiogenic cytokines in various dECM tissues (heart, lung, liver, kidney, and skin), analysis of angiogenic cytokines was performed by dot-blotting using a Mouse Angiogenesis Array Kit (R&D Systems, Minneapolis, MN). The pixel densities of the dots were calculated using ImageJ software (NIH, Bethesda, MD).
Biochemical characterization of hdECM
To verify the extent of decellularization, histological sections were analyzed following hematoxylin and eosin (H&E), Masson's trichrome (MT), and immunofluorescent staining. The residual DNA and ECM components, such as collagen and glycosaminoglycans (GAGs), in the decellularized tissue were also assessed. For histological evaluation, both native and decellularized tissues were fixed in 4% paraformaldehyde (3M, Maplewood, MN), embedded in paraffin, and sectioned at a thickness of 6 μm using a microtome (RM2255; Leica, Wetzlar, Germany). Sections were deparaffinized and stained with MT to stain the collagen and sulfated GAGs, as well as with H&E to stain the nucleus and cytoplasm. For the immunofluorescent staining, antibodies against collagen I (anti-collagen I at 1:1000; Abcam, Cambridge, MA), collagen IV (anti-collagen IV at 1:500; Abcam), laminin (anti-laminin at 1:200; Abcam), and fibronectin (anti-fibronectin at 1:400; Acris, Herford, Germany) were used to identify ECM components present after decellularization.
For DNA quantification, DNA was extracted from normal and decellularized heart tissue using a commercially available kit (DNeasy Blood & Tissue Kit; Qiagen, Venlo, Netherlands). Extracted DNA was quantified at 260 nm wavelength using a NanoDrop (ND-1000; Daemyung Science, Seoul, Korea).
The GAG content was estimated through quantifying the amount of sulfated GAGs using 1,9-dimethylmethylene blue solution. The absorbance was measured with a microplate reader at a wavelength of 530 nm. A standard curve was created in advance using chondroitin sulfate and was used for estimating the amount of sulfated GAGs in samples. The amount of soluble collagen was measured using a Sircol Assay Kit (Biocolor, Carrickfergus, United Kingdom). Soluble collagen was extracted by applying an acid-pepsin extraction procedure as per the instruction manual provided with the assay kit and precipitated out by adding the acid-neutralizing reagent followed by isolation and addition of the concentration reagent. The precipitate was incubated with collagen dye reagent; the complex was further recovered by addition of alkali reagent and was measured at 555 nm. All reagents used were provided with the assay kit. The total collagen content was determined through a conventional hydroxyproline assay. The absorbance of the sample was measured at 550 nm and quantified by referring to the standard curve created in advance with hydroxyproline. 34
Scaffold fabrication
The synthesis of PLCL was described in detail elsewhere. 19 Briefly, LA (100 mmol) and CL (100 mmol) were polymerized at 150°C for 24 h in a 50 mL glass ampule containing 1,6-hexanediol (0.5 mmol) and stannous octoate (1 mmol). After that reaction, the product was dissolved in chloroform, precipitated in methanol, filtered, and dried under a vacuum.
For fabrication of the NEhdHS, a hdECM solution was prepared by following a protocol published elsewhere, but with slight modification. 27 Lyophilized dECM was crushed into a powder using a freezer mill (6775 Freezer/Mill; SPEX SamplePrep, Metuchen, NJ). The 3 w/v% hdECM powders were digested in a solution of 0.5 M acetic acid with pepsin (1% w/w with respect to hdECM; Sigma) for 48 h. After complete solubilization of hdECM, the solution was mixed in a PLCL solution prepared by dissolving PLCL in HFIP (Tokyo Chemical Industry, Tokyo, Japan) at a concentration of 9 w/w%. With respect to PLCL/hdECM solutions, three different hdECM contents were used (5, 10, and 12.5 w/w%). The PLCL/hdECM solutions were poured into a syringe to be electrospun through a blunt tip metallic needle (18G) onto a metallic target under the following conditions: 12 kV applied voltage (Nano NC, Seoul, Korea), 0.4 mL/h feed rate (KD Scientific, Holliston, MA), and 10 cm needle-to-target distance. All samples were vacuum dried for 48 h and stored in a desiccator.
Scanning electron microscopy
For scanning electron microscopy (SEM) analysis, the electrospun fibers of the NEhdHS were sputter coated with gold (SPI-module sputter coater; SPI supplies, West Chester, PA) and observed with a SEM (Nova NanoSEM; FEI, Hillsboro, OR) at an acceleration voltage of 15 kV. The mean fiber diameter was estimated using ImageJ software and was calculated after selecting 20 single fibers randomly observed on SEM images.
Cell adhesion and proliferation
For the in vitro cell adhesion and proliferation study, cell suspensions (1 × 104 HDFs/200 mL) were seeded onto NEhdHS. Cell proliferation was measured at days 1, 3, 7, and 10 by applying the water-soluble tetrazolium salt-1 (WST-1) assay (Dojindo Molecular Technologies, Rockville, MD), which is based on the ability of living cells to reduce a tetrazolium salt into a soluble, colored formazan product.
Tensile properties
Samples (5 × 10 mm) cut from the NEhdHS, as well as from the gelatin-containing PLCL and PLCL scaffolds, were tested for tensile properties. The mechanical properties of the scaffolds were measured by performing universal testing machine (UTM) with an Instron 5966 tester (Instron, Norwood, MA) at a 10 N load cell number and a cross-head speed of 10 mm/min (n = 4). Young's modulus, tensile strength, and elongation at break were obtained from the stress–strain curves.
Mercury intrusion porosimetry
A mercury intrusion porosimeter (MIP; Micromeritics AutoPore IV 9500, Oak Ridge, TN) was used to determine the average pore diameter and porosity of the scaffolds. Briefly, the dried scaffold samples were subjected to a pressure cycle starting at ∼0.2 psia and then increasing to 1000 psia. The analysis was performed using AutoPore IV 9500 v1.07 software and was based on the amount of mercury intrusion into the samples through their internal pore structures. A total of 0.1–0.3 g of each sample was used to obtain measurements.
Cell seeding and in vitro study
HDFs at passage 8 were seeded on one side of the NEhdHS for 1 day in order for attachment to occur. Subsequently, HUVECs at passage 7 were seeded on the other side of the scaffold. The density of cell seeding was 5000 cells per 1 cm2 of scaffold. After the seeding process, the two-dimensional shaped scaffold was folded to ∼1 cm width and then cultured for 3, 7, 14, or 21 days.
To evaluate angiogenesis and tubule formation by HUVECs and HDF in the folded NEhdHS, immunofluorescence staining was performed at each culture time. Cell complexes were fixed onto the NEhdHS using 4% paraformaldehyde (3 M) for 24 h at 4°C, after which the folded NEhdHS was cut to a length of 1 cm. The samples were then permeabilized in a blocking solution consisting of 0.01 g/mL bovine serum albumin (Sigma) dissolved in PBS for 2 h. The cell complexes in the scaffold were then stained using rabbit polyclonal anti-von Willebrand factor antibodies (vWF at 1:400; Abcam). Alexa Fluor secondary antibody (Abcam) was used to provide color fluorescence. Cell nuclei were stained with 4′,6-diamidino-2-phenylindole (DAPI at 1:1000; Molecular Probes).
For quantifying angiogenesis and tubule formation on the scaffold, vWF-positive regions in five random fields were evaluated. The percentage of vWF-positive area, the length of vascular constituent elements of angiogenesis, and the area of capillary-like tubular structures were quantified using ImageJ software (n = 5 in each group). 35
Excisional wound model and estimation of wound closure
For the excisional wound model, 8-week-old SD rats (SAMTAKO, Osan, Korea; four per group) were anesthetized with an intraperitoneal injection of 2% avertin (2,2,2-tribromoethyl alcohol, Sigma-Aldrich; tert-amyl alcohol, Sigma-Aldrich) at a dosage level of 20 μL of avertin per gram of body weight. Subsequently, rat dorsa were shaved and cleaned with 70% ethanol. Full-thickness skin wounds (10 mm diameter) were made aseptically using a biopsy punch (Kai Industries, Tokyo, Japan). Scaffold treatments involve placing them in direct contact with the wound and fixing with medical tape to prevent separation (Fig. 1). Treatment groups are as follows: (1) without scaffold material placement (defect group), (2) NEhdHS treated (dECM group), (3) PLCL/gelatin scaffold treated (gelatin group), and (4) PLCL scaffold treated (PLCL group).
Scaffolds (40 ± 5 μm thick) were cut into circles using a 12 mm diameter biopsy punch (Kai Industries) and sterilized by applying ethylene oxide sterilizer (PERSON-EO35; Person Medical, Gyeonggi, Korea). A NEhdHS, gelatin-containing PLCL, or PLCL scaffold circle was placed in the wound bed and covered with a dressing (15 × 15 mm) containing a 10 mm diameter circular perforation so as not to cover the scaffold.
To estimate wound closure, each wound was digitally photographed at indicated times. Changes in the wound were measured using a digital slide caliper and are expressed as percentages of the initial wound size.
Histological and immunohistological evaluation of wound healing
Healed wounds and their surrounding areas were collected at indicated times. Collected tissue samples were fixed in 4% paraformaldehyde (3 M), embedded in paraffin, and sectioned at a thickness of 6 μm using a microtome (Leica). Sections were then deparaffinized and, using standard protocols, stained with H&E to detect inflammation in healed skin in the various groups or stained with MT to show the distribution and density of collagen in healed skin in the various groups. The fibrosis area of each group was quantified as the ratio of the fibrosis area to the total area of MT staining image wound regions on day 21 using ImageJ software (n = 5 in each group).
For immunofluorescence staining, samples were blocked, incubated initially with a primary antibody, and subsequently with the corresponding secondary antibody. To estimate the immune response by macrophages, the primary antibodies were mouse monoclonal anti-cluster of differentiation 68 (CD 68 at 1: 100 using Abcam) for both M1 and M2 macrophages, as well as goat polyclonal anti CD 206 (Santa Cruz Biotechnology, Dallas, TX) for M2 macrophages. The CD 68- and CD 206-positive areas in five random fields ( × 100 magnification) were quantified using ImageJ software (n = 4 in each group). Primary antibodies to detect angiogenic activity were vWF (Abcam) for staining ECs and mouse monoclonal anti-alpha smooth muscle actin antibody (α-SMA at 1:100; Abcam) for staining vascular smooth muscle cells. The vWF- and α-SMA-positive areas in five random fields ( × 200 magnification) were quantified using ImageJ software (n = 5 in each group). The positive areas are presented as a mean value per unit area (1 mm2). The maturation index was quantified as the ratio of the α-SMA-positive vessel area to the total area of vessels. 36 To detect scar formation, the primary antibodies used were mouse monoclonal anti-collagen antibody (COL-1; Abcam) and rabbit polyclonal anti-collagen III antibody (COL-3; Abcam). The COL-1- and COL-3-positive areas in five random fields ( × 200 magnification) were quantified using ImageJ software (n = 5 in each group). The positive areas were quantified as the ratio of the COL-1- or COL-3-positive area to the total image area.
Statistical analysis
Where applicable, all data are expressed as mean ± standard deviation values. Student's t-test and single-factor analysis of variance were used for parameter estimation and hypothesis testing, with *p < 0.05 and **p < 0.01 considered statistically significant.
Results
Analysis of angiogenic factors in dECMs
The types and amounts of angiogenic factors, including growth factors and cytokines regulating, reducing, or enhancing angiogenesis, in the various dECMs, including those from skin, heart, lung, kidney, and liver, were analyzed by assessing dot blots (Fig. 2A). The amount and type of angiogenic factors involved in hdECM were highest among the tested dECM sources. Notably, hdECM had the greatest numbers by type and amount of pro-angiogenic factors, which included Ang-1, Ang-3, CCN1, FGF-1, FGF-2, leptin, MMP-9, NOV, SDF-1, and VEGF-B, factors that can induce angiogenesis during wound healing (Fig. 2B). The results are similar to those reported previously. 30
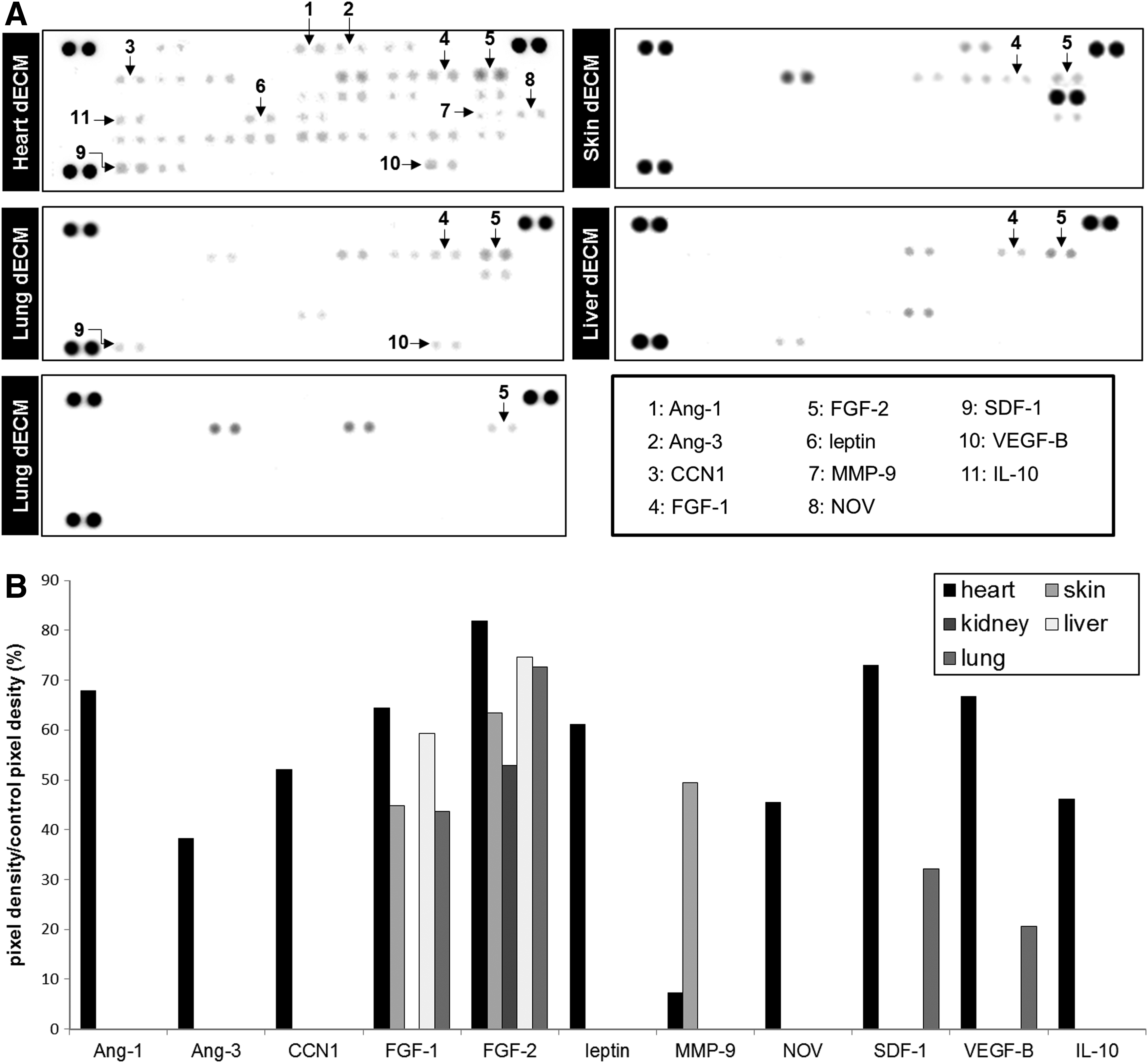
Analysis of pro-angiogenic factors contained in various decellularized tissues.
hdECM characterization
To evaluate the efficiency of the decellularization method, we performed histological evaluation and quantitative estimation of the DNA and ECM components of hdECM. The H&E and MT staining results confirmed that, compared with native tissue, only nuclei, cell debris, and cytoplasm had been removed during decellularization, and only ECM collagen remained in the matrix after decellularization of hdECM (Supplementary Fig. S1A, B; Supplementary Data are available online at www.liebertpub.com/tea). Moreover, immunofluorescence staining confirmed that various ECM components with pro-angiogenic properties, including collagen type I, type IV, laminin, and fibronectin, remained in the decellularized hdECM (Supplementary Fig. S1C).
Supplementary Figure S1D shows the results of the quantitative analysis of the DNA and major ECM components, GAG and collagen, in hdECM. After decellularization, the portion of remaining DNA was <1% of that in native tissue (0.94% ± 0.49% DNA remained in the hdECM; p < 0.01). Of the major ECM components, although GAG level decreased significantly (81.05% ± 0.15% GAG remained in the hdECM; p < 0.01), the collagen level did not decrease significantly after decellularization (95.33% ± 12.47% collagen remained in the hdECM; p > 0.05).
Preparation of NEhdHS
To determine the most effective mixing ratio of hdECM to PLCL, the hdECM content was varied (5, 10, and 12.5 wt%). However, in the 12.5 wt% hdECM, the hdECM hydrogel and the PLCL solution separated without mixing homogeneously; thus, we only compared 5 wt% hdECM/PLCL, 10 wt% hdECM/PLCL, and PLCL-only scaffolds. All scaffolds were spun to a thickness of 40 ± 10 μm, and the fiber diameter was 1.0 ± 0.5 μm in all samples (Supplementary Fig. S2A).
Cell viabilities observed for up to 10 days for HDFs cultured on 5 wt% hdECM/PLCL, 10 wt% hdECM/PLCL, and PLCL-only scaffolds are plotted in Supplementary Figure S2B. The number of viable cells after 1 day, which reflects the time when cell adhesion is present, was significantly higher in the 10 wt% hdECM/PLCL scaffold than those in the 5 wt% hdECM/PLCL and PLCL-only scaffolds (Supplementary Fig. S2C). At 10 days of culture, the viability of HDFs on 10 wt% hdECM/PLCL scaffold was highest, followed by that on the 5 wt% hdECM/PLCL and lowest on the PLCL-only scaffolds (Supplementary Fig. S2D). Based on these results, we selected the 10 wt% ratio of hdECM to PLCL for use in fabricating the NEhdHS.
Estimation of NEhdHS
To determine the effects of the NEhdHS, we set up three groups as follows: NEhdHS (dECM), PLCL-only (PLCL), and gelatin-containing PLCL (gelatin). Gelatin, which is a natural biopolymer derived from partial hydrolysis of native collagens, has been used in medicine, including its use as a wound dressing, because it has been shown to induce activation of macrophages and have a high hemostatic effect. 37 Thus, we used the gelatin group as a positive control. The morphology of the structures in the dECM group was analyzed using SEM and was compared to those of the PLCL and gelatin groups. All groups exhibited fine fibers, and the presence of dECM and gelatin components did not significantly modify fiber diameter, scaffold thickness, or morphology (Fig. 3A–C). Figure 3D and E show that pore diameters (8.50 ± 2.61 μm in the dECM group, 7.68 ± 3.32 μm in the gelatin group, and 9.28 ± 3.92 μm in the PLCL group) and porosities (65.40% ± 6.08% in the dECM group, 57.94% ± 14.54% in the gelatin group, and 65.79% ± 20.61% in the PLCL group) were quite similar among the three groups. Taken together, the results indicate that the presence of dECM and gelatin components did not affect the PLCL scaffold structure (e.g., fiber diameter, scaffold thickness, pore size, and porosity remained similar). Thus, scaffolds in all three groups provide good gas permeability and offer protection of wound from infection and dehydration, which are requirements for wound dressings with porosity >50%.
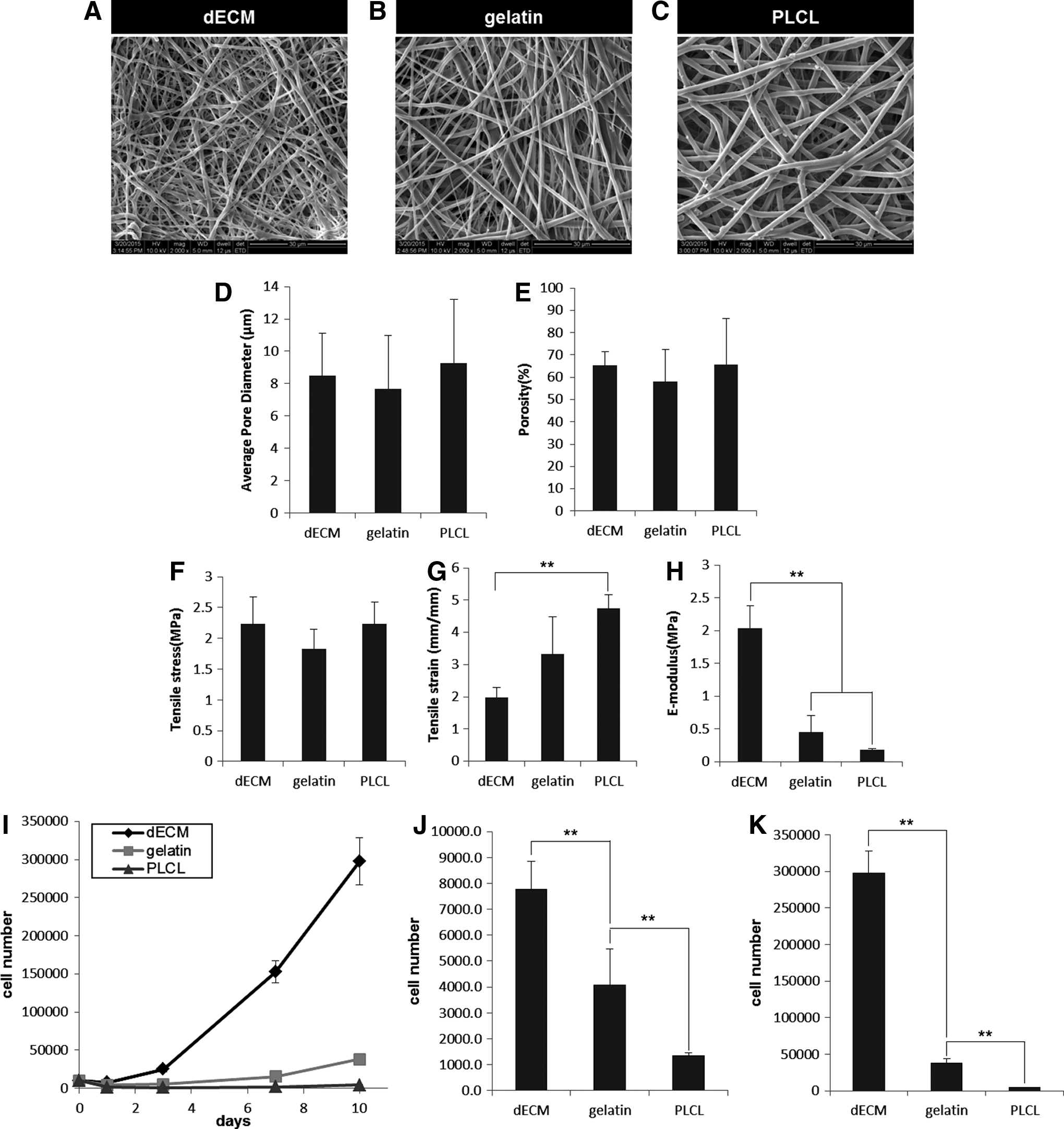
Examination of NEhdHS, gelatin-containing PLCL, and PLCL-only scaffold characteristics. SEM morphology of
Tensile properties
The tensile properties of the dECM group scaffolds were determined using an UTM (Instron), and three values (stress at break, strain at break, and E-modulus) were obtained and compared to those of the PLCL and gelatin groups (Fig. 3F–H). There were no significant differences in tensile stress among the three groups (2.23 ± 0.44 MPa in the dECM group, 1.83 ± 0.31 MPa in the gelatin group, and 2.23 ± 0.36 MPa in the PLCL group). However, tensile strain for the dECM group (1.98 ± 0.31 mm/mm) was significantly lower compared with the PLCL group (4.74 ± 0.42 mm/mm; p < 0.01), whereas the E-modulus for the dECM group (2.04 ± 0.34 MPa) was significantly greater compared with both the gelatin and PLCL groups (0.45 ± 0.25 MPa in the gelatin group, 0.19 ± 0.01 MPa in the PLCL group; p < 0.01).
Taken together, these mechanical property results indicate that the NEhdHS has higher stiffness and lower elasticity than those of PLCL and gelatin-containing PLCL scaffolds.
Cell adhesion and proliferation analysis
To investigate cell adhesion and proliferation in the three scaffold groups, we cultured HDFs on hdECM/PLCL, gelatin-containing PLCL, and PLCL scaffolds for up to 10 days and performed WST-1 tests on each (Fig. 3I–K). At 1 day after HDF seeding, which reflects the time at which cell adhesion has occurred, the dECM group had the greatest number of adhered cells (p < 0.01; Fig. 3J). Moreover, after 10 days of culture, HDFs were most proliferated in the dECM group, followed by that in the gelatin and PLCL groups (Fig. 3K).
Based on these results, the NEhdHS is effective at increasing cell adhesion and proliferation, presumably because the hdECM components contained in the NEhdHS included fibronectin and laminin, which aid in cell attachment and growth.
In vitro angiogenesis analysis
To investigate the effects of the NEhdHS on HUVEC proliferation and angiogenesis, we examined immunofluorescence staining results for vWF (green) and DAPI (blue) in the folded NEhdHS, the gelatin-containing PLCL, and the PLCL scaffolds at indicated times (Fig. 4). At each interval, vWF expression was increased to a greater extent in the dECM group than in the gelatin or PLCL groups (Fig. 4A).

Immunofluorescence analysis of the angiogenic ability of NEhdHS in vitro.
To quantify cellular and angiogenic activity in the dECM, gelatin, and PLCL groups, the vWF-positive regions in five random fields were evaluated, and the vWF-positive expression area (%), the length of vascular constituent elements of angiogenesis (μm), and the area of capillary-like tubular structures (μm2) were quantified in each group and at each time interval using ImageJ software (n = 5 in each group). 35
The HUVEC densities, expressed as the vWF-positive cell expression area, at the indicated times in each of the three groups are presented in Figure 4B. The HUVEC density was greatest in the dECM group, followed by that in the gelatin group and lowest in the PLCL groups at all indicated times. In the dECM and gelatin groups, the HUVEC density increased significantly between days 7 and 14 and remained steadily high until day 21. In the PLCL group, the HUVEC density increased steadily until day 21.
Figure 4C presents the lengths of the vascular constituent angiogenesis elements in each group (dECM, gelatin, and PLCL) at indicated times (days 3, 7, 14, and 21). The mean length of segments in the dECM group was significantly greater compared with the gelatin and PLCL groups at all times. Moreover, in the dECM group, segment length was increased slightly until day 7, but, at day 14, segment length had increased significantly over that at day 7 (483.97 ± 252.02 μm at day 7, 1026.63 ± 363.15 μm at day 14; p < 0.05). At day 21, the dECM group segment length increased, but not significantly, over that at day 14, but the error range was smaller (1073.00 ± 115.82 μm in the dECM group at day 21; day 7 dECM group vs. day 14 dECM group p < 0.05, day 7 dECM group vs. day 21 dECM group p < 0.01). In contrast to the dECM group, the segments in the gelatin group formed at day 7 and grew until day 14 (2.43 ± 6.43 μm at day 7, 459.78 ± 379.76 μm at day 14; p < 0.01). At day 21, the gelatin group segment length (497.67 ± 223.53 μm) was similar to that at day 14, but the error range was smaller (as observed in the dECM group). In the PLCL group, the segments formed at day 14 and the segment length increased until day 21 (65.84 ± 103.37 μm at day 14, 261.33 ± 100.81 μm at day 21; p < 0.05).
With regard to the formation of branches, the mean length of branches in the dECM group was greater than those in the gelatin and PLCL groups until day 7; however, at day 14, the dECM group's branch length was greater compared with the PLCL group but similar to that of the gelatin group. At day 21, all three groups had similar branch lengths. Interestingly, unlike the other vascular constituent elements, the length of isolated branches was similar among the three groups up to day 7; however, at day 14, the PLCL group had a greater isolated branch length than that in the dECM group. The length of the isolated branches was greatest in the PLCL group at day 21. Furthermore, in the dECM group, the length of isolated branches changed little until day 7, but, at day 14, the isolated branch length decreased significantly (152.61 ± 26.23 μm at day 3, 150 ± 112.96 μm at day 7, 19.16 ± 28.19 μm at day 14; days 3 and 7 vs. day 14 p < 0.01). As observed in the dECM group, the gelatin group also exhibited a gradually decreasing isolated branch length until day 14 (171.20 ± 122.21 μm at day 3, 230 ± 47.62 μm at day 7, 123.64 ± 140.83 μm at day 14, and 73.17 ± 62.72 μm at day 21). In contrast to the other two groups, the PLCL group showed similar isolated branch lengths at all times (223.19 ± 180.54 μm at day 3, 229.25 ± 59.62 μm at day 7, 249.51 ± 202.52 μm at day 14, and 225.57 ± 107.62 μm at day 21).
Figure 4D shows that the area of capillary-like tubular structures was greatest in the dECM group, followed by that in the gelatin group, and lowest in the PLCL group at all of indicated times; similar results to those observed in the HUVEC density data. Moreover, the capillary-like tubular structure area increased significantly between days 7 and 14 and remained steady until day 21 in the dECM group. In the gelatin group, capillary-like tubular structures began to form at day 14, and the tubular structure area only increased slightly after day 14. The PLCL group did not exhibit capillary-like tubular structures until day 21.
Based on these results, we conclude that the NEhdHS produced a marked increase in HUVEC proliferation and angiogenic activity up to day 14. Moreover, vascularization matured after day 14. Thus, the dECM components in the NEhdHS not only promote HUVEC proliferation but also enhance the formation of mature isolated branch segments and capillary-like tubular structures.
Estimation of wound healing
Wound closure
To determine the effect of the NEhdHS on wound healing in rats with excisional wounds, wound closure was observed at the indicated times in the defect, PLCL, gelatin, and dECM groups (Fig. 5). Wound diameters were similar in all four groups until day 7, but, after day 7, wound diameters decreased significantly in all groups. These results indicate that contraction commences approximately a week after wounding, a time when fibroblasts have differentiated into myofibroblasts. 38 At day 14, wound diameter was smallest in the defect group (0.13 ± 0.04 cm) followed by that of the dECM (0.25 ± 0.01 cm), PLCL (0.26 ± 0.02 cm), and gelatin (0.30 ± 0.05 cm) groups (defect group vs. PLCL, gelatin, and dECM groups, p < 0.01). Wound sizes of the dECM and defect groups were similar, and both were smaller than those of the gelatin and PLCL groups at day 21 (0.07 ± 0.01 cm in the dECM group, 0.06 ± 0.02 cm in the defect group, 0.13 ± 0.04 cm in the PLCL group, and 0.17 ± 0.01 cm in the gelatin group).
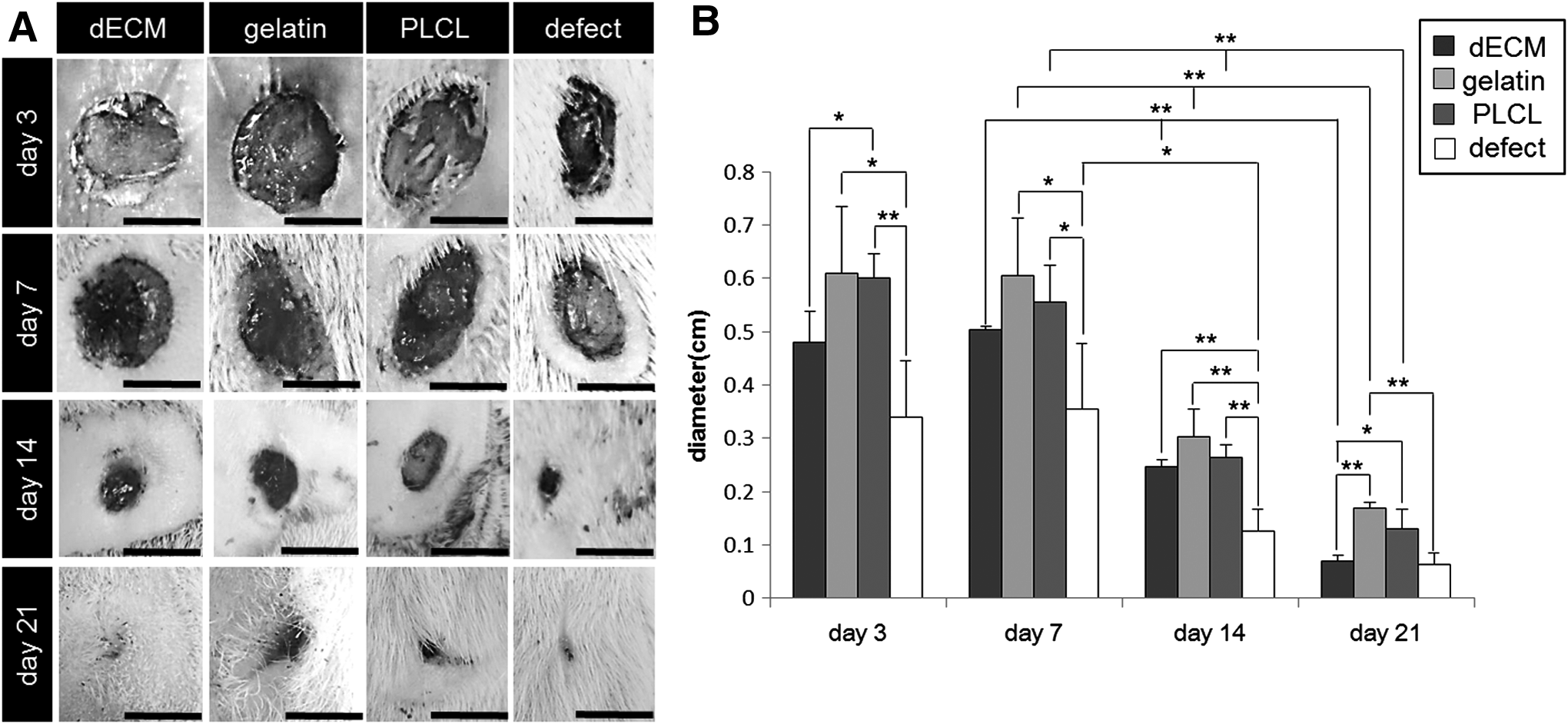
Wound closure analysis for evaluation of NEhdHS wound healing ability.
Histological analysis
For estimation of wound tissue remodeling, skin samples were harvested from healed wounds, and histological assessments were carried out. H&E staining showed that reepithelialization and inflammation occurred at the wound site in all experimental groups (Fig. 6A). When the scaffolds were treated to excisional wound rats after 3 days of treatment, the dECM and gelatin groups showed many acute and chronic inflammatory cells, such as neutrophils, lymphocytes, and macrophage with blood vessels and extravasated red blood cells (Fig. 6A, cross-mark region) compared to native tissue (Fig. 6C left). These initial inflammatory cells promote the migration and proliferation of ECs, which lead to neovascularization and, in turn, aid in reepithelialization of the wounded tissue. 39 Although acute and chronic inflammatory cells were observed in the PLCL and defect groups, the regions of their occurrence in those two groups, especially in the defect group, were smaller than those in the dECM and gelatin groups.

Histological analysis of reepithelialization and collagen remodeling. Representative macroscopic images of
Compared to the PLCL and defect groups at culture days 7 and 14, the dECM and gelatin groups had lower levels of inflammatory cells. Granular tissues with less inflammatory and red blood cells, which facilitate fast wound healing, were observed in the dECM and gelatin groups (Fig. 6A, asterisk region). Moreover, the dECM group had a much larger region of granular tissues than that in the gelatin group, as well as a greater proliferation of fibroblasts, the major producers of collagen, than that in the gelatin group. Moreover, a large area of epithelium had begun to form in the dECM group at day 7 (Fig. 6A, black triangles), whereas the gelatin group showed little epithelium presence at day 7. The PLCL and defect groups only started to form epithelium at day 14.
The wound site tissue regenerated through tissue remodeling in the dECM group at day 21 had a form similar to that of native tissue. The gelatin and PLCL groups also regenerated tissue in most of the wound site area, but some regions did not regenerate properly (Fig. 6A, black arrow). In the defect group, most of the regenerated wound site tissue formed as fibroses.
Figure 6B shows the results of staining with MT, a stain that allows clear visualization of changes in collagen fibers. In the dECM group, the formation of organized collagen fibers was more prominent at day 14 than that in the other three groups. Moreover, compared to native tissue (Fig. 6C, right), we confirmed that collagen remodeling and degradation occurred simultaneously in the dECM group at day 21 with actions that provide tensile strength and reduce scar formation. In contrast, the gelatin and PLCL group wound samples formed little scar tissue because collagen remodeling and degradation occurred later than in the dECM group (Fig. 6B, black arrow). In the wound sites of the defect group, we observed that the area of collagen continued to increase with time, which indicates that a collagen-only accumulation is occurring with no remodeling or degradation of the formed collagen. For a more precise analysis, we performed the fibrosis quantification of each group in wound regions on day 21 (Fig. 6D, n = 5 in each group). The fibrosis area was the greatest in the defect group and descended in order by PLCL, gelatin group, and dECM group (56.99% ± 4.47% in the defect group, 32.19% ± 5.06% in the PLCL group, 16.11% ± 7.06% in the gelatin group, and 1.71% ± 1.71% in the dECM group). The presence of complete tissue remodeling and faster epithelial formation in the dECM group could significantly accelerate wound healing over that in the other groups.
Estimation of immune response by macrophages
Macrophages, one of the innate immune response cells, play a beneficial role during wound healing with macrophages regulating a wide range of processes. 40 To estimate the immune response by NEhdHS microphages, we performed immunofluorescent staining of each group in wound regions at the indicated time intervals using CD 68 for M1 and M2 macrophages, as well as CD 206 for M2 macrophage primary antibodies (Fig. 7A–D). Results from the quantitative histological assessment, which reflect the quantification of CD 68-positive cells to total cell ratios (%) and the CD 206-positive cells to CD 68-positive cell ratios (%), are summarized in Figure 7E and F, respectively (n = 4 in each group).
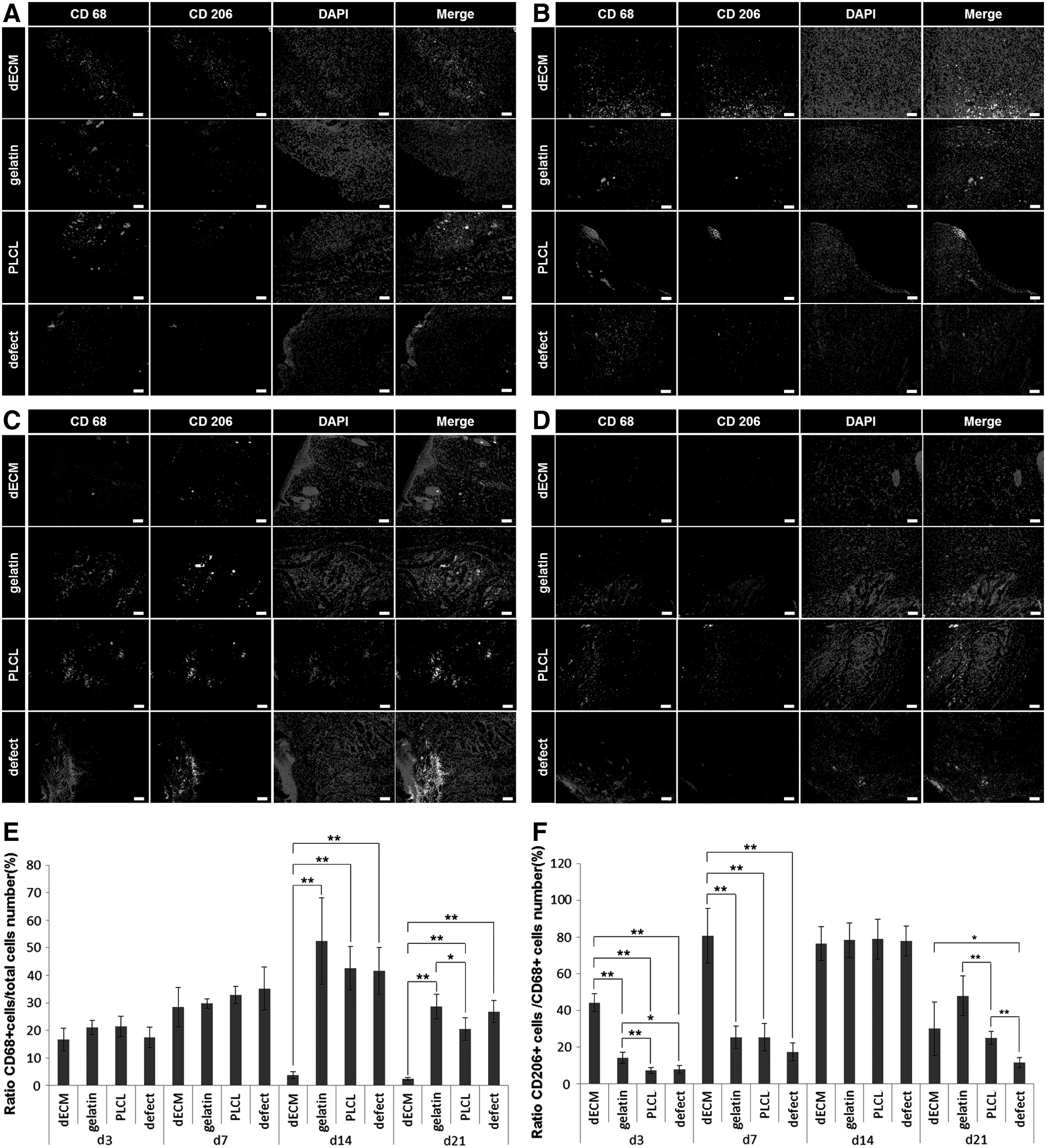
Immunofluorescence analysis to estimate the immune response by macrophages in the NEhdHS. Representative images of immunofluorescence-stained macrophages and M2 macrophages in each group at
The CD 68-positive cells were similarly increased in all groups up to day 7, but CD68-positive cells in the dECM group showed a tendency to decrease rapidly on day 14 (dECM group vs. gelatin, PLCL, and defect groups, p < 0.01), unlike other groups which increased steadily to day 14 and then decreased on day 21 (Fig. 7E).
The CD 206-positive cells to CD 68-positive cell ratios, which are the M2 macrophage ratios to total macrophages, showed a tendency to increase steadily in all groups up to day 14 and then decreased on day 21 (Fig. 7F). Interestingly, the CD 206-positive cells to CD 68-positive cell ratios of the dECM group were 3.12, 6.09, and 5.56 times greater than gelatin, PLCL, and defect groups. The gelatin group was 1.95 and 1.78 times greater than the PLCL and defect groups on day 3, respectively (44.28% ± 4.46% in the dECM group, 14.18% ± 3.00% in the gelatin group, 7.27% ± 1.54% in the PLCL group, and 7.96% ± 2.13% in the defect group). Moreover, the CD 206-positive cells to CD 68-positive cell ratios of the dECM group were significantly higher than the other groups on day 7 (80.79% ± 15.01% in the dECM group, 25.45% ± 6.08% in the gelatin group, 25.41% ± 7.40% in the PLCL group, and 17.48% ± 4.88% in the defect group; dECM group vs. gelatin, PLCL, and defect groups, p < 0.01). It showed similar values as other groups on day 14 (76.41% ± 9.33% in the dECM group, 78.83% ± 10.91% in the gelatin group, 78.83% ± 10.92% in the PLCL group, and 77.84% ± 8.18% in the defect group; p > 0.05). On day 21, the CD 206-positive cells to CD 68-positive cell ratios of the dECM group were significantly higher than the defect group, but not significantly different from the gelatin and PLCL groups (dECM group vs. defect groups, p < 0.05). The CD 206-positive cells to CD 68-positive cell ratios of the gelatin group were 1.91 and 4.09 times higher than the PLCL and defect groups on day 21, respectively. In the dECM group, the M2 macrophages appeared faster during the initial wound healing, and the immune response was completed faster than the other groups.
Angiogenesis evaluation
To evaluate the angiogenic activity of NEhdHS, vWF-positive vessel density (μm2/mm2), α-SMA-positive vessel density (μm2/mm2), and maturation index (%) of each group were determined in wound regions at 21 days after treatment (Fig. 8, n = 6 in each group).

Immunofluorescence analysis to estimate angiogenic ability of NEhdHS in vivo.
The vWF-positive vessel densities of the PLCL, gelatin, and dECM groups were 1.99, 2.25, and 4.33 times greater compared with the defect group (Fig. 8B). There were no significant differences in capillary densities between the PLCL and gelatin groups, whereas capillary density in the dECM group was 2.18 times greater compared with the PLCL group and 1.92 times greater compared with the gelatin group.
The α-SMA-positive vessel density in the dECM group was higher compared with the other groups; 4.33, 3.37, and 2.56 times greater compared with the defect, PLCL, and gelatin groups, respectively (Fig. 8C). In contrast to the vWF-positive vessel density results, the α-SMA-positive vessel density of the gelatin group was 1.32 times greater compared with the PLCL group, a significant difference (p > 0.01), while the α-SMA-positive density in the PLCL group was 2.71 times greater compared with the defect group.
To determine the percentage of mature vessels, maturation indices were calculated based on the double staining results obtained after 21 days of culture. As shown in Figure 8D, maturation was 87.45% ± 6.57% in the dECM group, 66.03% ± 4.70% in the gelatin group, 56.95% ± 8.82% in the PLCL group, and 41.83% ± 5.72% in the defect group. The dECM group maturation index was the highest among all of the groups followed by the gelatin group, the PLCL group, and the defect group (dECM group vs. gelatin, PLCL, and defect groups, p < 0.01). Based on these results, NEhdHS is the most effective scaffold for increasing capillary density and matured vessel density.
Cutaneous scarring evaluation
In the wound healing process, collagen types I and III ratios are major indicators of scar formation. 41 Figure 9A–D presents immunofluorescent staining results for collagen types I and III in each group at the indicated times and indicates group-specific activity related to scar formation. Results from quantitative histological assessments, which reflect quantification of collagen types I- and III-positive expression areas, are summarized in Figure 9E.
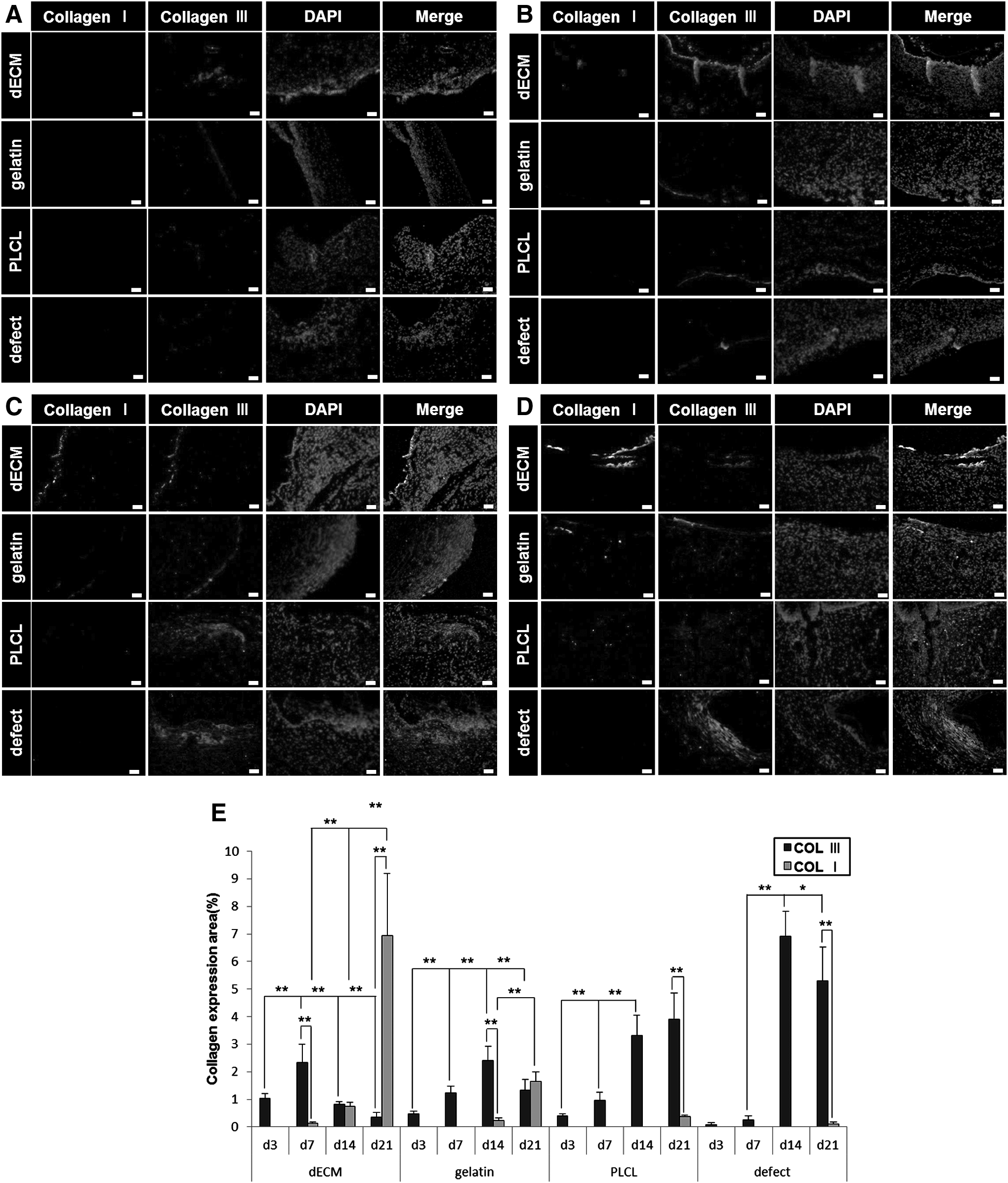
Immunofluorescence analysis to estimate the effect NEhdHS on scar formation. Representative images of immunofluorescence-stained collagen type I and III at
Collagen type III-positive expression levels in the dECM group increased up to day 7 and then decreased steadily. In contrast, collagen type I began to appear at day 7 and increased significantly up to day 21 (p < 0.01). In the gelatin group, the collagen type III-positive expression area increased up to day 14 then decreased significantly to day 21, while the collagen type I began to appear at day 14, later than in the dECM group and then increased significantly up to day 21 (p < 0.01). However, in the PLCL group, the collagen type III-positive expression area increased up to day 14, but thereafter did not decrease, whereas collagen type I only began to appear at day 21. In the defect group, the collagen type III-positive expression area increased up to day 14 and then slightly decreased to day 21, while collagen type I only began to appear at day 21. The defect group had similar trends to those in the PLCL group, but the collagen type III-positive expression area remained larger and collagen type I smaller in the defect group than those in the PLCL group at day 21.
Discussion
To increase the effectiveness of wound healing treatments, studies have been conducted into bioactive wound dressings. Some researchers seek to design an ideal wound dressing that consists of a biocompatible and biodegradable scaffold through which skin cells can interact, migrate, and populate in a natural manner and has features that provide an antibacterial, moist, and soothing environment around the injured tissue. Such scaffolds have included silver nanoparticles, chitin, and chitosan and were prepared through an electrospinning technique.18,42–46 However, although angiogenesis also has an important role in the wound healing process, especially in serious wounds, few studies have investigated pro-angiogenesis features of wound dressings. In this study, we focused on the development of a wound dressing that combines hdECM, which can promote angiogenesis, with a biocompatible polymer and a nanofibrous structure that can create a moist ventilated environment.
Our results showed that hdECM can provide more pro-angiogenic factors than those provided by skin, lung, liver, and kidney dECMs. In particular, angiopoietin-1 (ang-1), which is critical for vessel maturation, adhesion, migration, and survival, and VEGF-B, which has a role in the maintenance of newly formed blood vessels during pathological conditions, were present only in hdECM.47,48 Thus, we fabricated, through an electrospinning technique, a NEhdHS using hdECM mixed with a biocompatible and biodegradable polymer, PLCL, to develop a pro-angiogenic therapeutic application for effective wound healing.
To estimate the effects of the NEhdHS, we assessed three scaffold groups: NEhdHS (dECM), PLCL-only (PLCL), and gelatin-containing PLCL (gelatin). The groups’ scaffolds were fabricated to have similar structural features, including fiber size, scaffold thickness, pore size, and porosity, to clarify the effect of the hdECM components and to minimize the effect of structural differences. Tensile strain was lowest in the dECM group, followed by the gelatin and PLCL groups, while the E-modulus was highest in the dECM group, followed by the gelatin and PLCL groups. Usually, the addition of a natural polymer such as collagen or gelatin to a synthetic polymer such as PLCL increases the E-modulus of the polymer. 49 Zhang et al. showed that the E-modulus of an electrospun poly(CL) fiber was increased by gelatin addition. 50 Based on the current and previous results, the rigid dECM and gelatin particles allow them to act as rigid fillers, thereby increasing the strength and toughness of the scaffold.
We investigated various constituent elements of angiogenesis in NEhdHS, gelatin-containing PLCL, and PLCL scaffolds in vitro and compared the dECM group with the gelatin and PLCL groups to determine the effects of NEhdHS on various angiogenesis parameters. We observed that dECM promoted HUVEC proliferation and capillary-like tubular structure maturation by increasing the vWF-positive expression area, the length of segments, the level of mature vascular constituent elements, and the area of capillary-like tubular structures at all assessed times. However, the length of isolated branches, the initial vascular constituent elements, was shorter in the dECM group than in the other groups. These results indicate that isolated branches form early, grow, and then constitute the segments that become mature vascular structures, which are consistent with the results of our previous angiogenesis study. 35 Thus, the NEhdHS has the capacity to enhance vasculogenesis and maturation of vascular constituent elements. Moreover, in the dECM group, HUVEC density, segment length, and capillary-like tubular structure area increased gradually until day 14; however, there was no difference among the groups at day 21, although the error ranges had decreased. These results indicate that such vessels form in random areas, and, in the dECM group, those regions widened until day 14. By day 21, vessels were evenly formed over all areas of the dECM scaffold. This tendency was also observed in the gelatin and PLCL groups, but the gelatin group started vascular formation and expansion more slowly than that in the dECM group. The PLCL group exhibited the slowest vascular formation among the three groups. Based on these results, application of the NEhdHS would allow rapid angiogenesis and maturation of vessels, thereby enabling rapid wound healing.
To evaluate the effect of NEhdHS on wound healing, we observed the wound closure, immune response by macrophage, angiogenic activity, and scar formation processes in excisional wounded rats in the defect, PLCL, gelatin, and dECM groups.
When an injury occurs, monocytes begin migrating into the wound and en route they differentiate multiple phenotypes into wound associated macrophages in a process driven by factors in the extracellular milieu. 51 The differentiated macrophages can be broadly classified as M1 and M2 phenotypes. 52 The M1 macrophages produced by exposure to interferon-γ and tumor necrosis factor-α are pro-inflammatory macrophage phenotype and phagocytized neutrophils that have apoptosed and remove any pathogens or debris in the wound. 53 The M2 macrophages produced by IL-4, IL-10, IL-13, or tumor necrosis factor-β are anti-inflammatory macrophage phenotype and function in wound repair through ECM deposition revascularization and wound reepithelialization. 54 Therefore, we analyzed the changes in total macrophage numbers and M2 macrophage numbers with time and groups by quantifying the CD 68-positive cells to total cell ratios and the CD 206-positive cells to CD 68-positive cell ratios in each group and at each time interval to estimate the immune response in the NEhdHS.
The CD 68-positive cells to total cell ratios showed a tendency to increase steadily in all groups at the initial wound healing stage before decreasing in the final wound healing stage, which is similar to Rodero et al. 55 One of the interesting results is that the CD 68-positive cells to total cell ratios were the lowest in the dECM group. In addition, CD 68-positive cells to total cell ratios decreased after day 7 in the dECM group, which is faster than gelatin, PLCL, and defect groups after day 14. These results mean that the immune response by macrophages occurs less in the dECM group and faster than other groups. This is probably because IL10, the anti-inflammatory cytokine included in hdECM, affects macrophages. 54
The CD 206-positive cells to CD 68-positive cell ratios mean that M2 macrophage numbers were maintained at a low level of about 20% in the gelatin, PLCL, and defect groups at the early stages of wound healing, which are days 3 and 7. They then increased to about 80% at day before decreasing. The tendency of CD 206-positive cells to CD 68-positive cell ratios closely parallels the M1 macrophages that prevail during the early stages of inflammation, whereas M2 macrophages predominate during postinjury in the wound healing process. 56 However, in the dECM group, the CD 206-positive cells to CD 68-positive cell ratios was ∼40% from day 3, which was higher than the other groups and increased to 80% on day 7. These results suggest that IL10 contained in hdECM may not only act as an anti-inflammation but also help differentiation into M2 macrophages. Thus, the inflammation reaction is reduced by M1 macrophages.54,57
The angiogenic activity of the NEhdHS was examined by comparing vWF-positive vessel density, α-SMA-positive vessel density, and maturation index values among dECM, gelatin, PLCL, and defect groups. The vWF-positive vessel and α-SMA-positive vessel densities were greater in the dECM group than those in the other three groups. This is due to the increased adhesion, migration, survival, and maturation of blood vessels induced by the ang-1 present in hdECM, as well as increased M2 macrophages differentiated by IL 10 included in hdECM.54,58 Remarkably, this was the only group in which increased vascular density was maintained at 21 days. In addition, there was a high maturation index (close to 90%) in the hdECM group due to the high level of maintenance of newly formed blood vessels by the VEGF-B component in hdECM. The NEhdHS developed in this study induces angiogenesis, as shown by the high vWF-positive vessel density, and promotes the maturation of previously formed vessels, as shown by the high α-SMA-positive vessel density, thereby enabling effective wound healing through enhancement of stable blood vessel development at the wound site.
The ECM has many functions in the skin, such as providing structure, organization, and orientation to cells and tissues. 59 Moreover, the ECM plays an important role in the wound healing process and is closely related to scar formation. When injury occurs, the wound healing process begins and the formation of a provisional ECM containing fibrin, fibrinogen, and fibronectin stops the bleeding and provides a scaffold for the attachment and proliferation of the cells. Afterward, fibroblasts induced by cytokines of neutrophils and macrophages form granulation tissue composed of procollagen, elastin, proteoglycans, and hyaluronic acid (HA). The granulation allows not only ingrowth of new blood vessels that provide nutrition and oxygen to the growing tissue but also leukocytes to enter the wound site. 60 After that, this highly hydrated ECM that allows cellular invasion and repair is gradually replaced by denser ECM composed mainly of collagen. 61 Scars can be formed as a result of these wound healing processes and are composed of the same ECM molecules as the tissue they replace. The ratios, such as collagen type I/III ratios, in scar tissue are different from normal tissue. 62 Thus, we analyzed the collagen type I and III contents in the dECM, gelatin, PLCL, and defect groups to estimate scar formation.
We confirmed that collagen type III was replaced by collagen type I most rapidly in the dECM group, followed by that in the gelatin, PLCL, and defect groups. Collagen type I and type III fibers coexist with individual fibrils and their relative ratios supposedly play an important role in the regulation of fibrillogenesis and in the determination of the final diameter and the bundle architecture. 63 Physiologically, there is an initial increase of thin collagen type III produced by fibroblast in granulation tissue that is later replaced by thicker, highly cross-linked collagen type I produced by mature wound fibroblast, which appears in later phases.64,65 Then, the matrix metalloproteinases (MMPs) secreted by fibroblast and keratinocytes such as MMP-1 and 13 degrade collagens to control the ratio of collagen type I and III. 60 In this phase, the degradation process of collagen III is facilitated by its low degree of cross-linkage and its smaller diameter for the enzymes of the ECM. An overabundance of collagen type III may lead to an increase in nonpolymeric collagen levels by inhibiting the associative properties of collagen type I. This might considerably contribute to the development of weak scar tissue. 65 Based on the current results and those reported previously, we suggest that the NEhdHS minimizes scar formation by enhancing the replacement of collagen type III with collagen type I.
The wound closure is related to wound contraction, while wound contraction is related to scarring. When the wound is closed before tissue regeneration with fast wound contraction, the immature scar can move on to the final remodeling phase, resulting in scarring as the ECM molecules laid down during the proliferative phase in a disorganized manner are realigned and cross-linked. 60 In skin wounds, scaffolds in the wound site are known to disturb wound contraction, 66 which is why wound closure rates in the dECM, gelatin, and PLCL scaffold groups were slightly better than that in the defect group. Interestingly, although the wound closure rate in the dECM group was slower than the defect group up to day 14 as with the gelatin and PLCL groups, the wound size of the dECM group was similar to the defect group at day 21. However, we confirmed that histomorphology was similar to native tissue, and minor scar formation occurred in the dECM group on day 21. These results suggest that the wound size of the dECM group decreased more than the defect group on day 21 due to fast tissue regeneration not by wound contraction. The rapid tissue regeneration of the dECM group would be due to the fact that IL10 contained in hdECM increased differentiation of M2 macrophages from the initial wound healing step. Fibroblast regeneration and angiogenesis were enhanced so that ECM deposition and remodeling occurred faster than in other groups. 54 Moreover, M2 macrophages induced reepithelialization, and angiogenic factors such as ang-1 and VEGF-B included in hdECM further enhanced angiogenesis, which may also help to rapidly regenerate tissue in the dECM group.48,54,58
The present study developed a NEhdHS for use as a wound dressing that can minimize inflammation, enhance angiogenesis, and promote collagen replacement. It also provides a moist ventilated environment, which helps in tissue remodeling, scarring minimization, and effective wound healing. The scaffolding technique used in the present study could potentially be applied to the treatment of serious wounds that require pro-angiogenic therapy. Future studies will focus on the application of artificial skin to promote effective skin regeneration through the promotion of angiogenesis.
Conclusion
We investigated the effect of including hdECM, which contains a rich supply of pro-angiogenic factors compared to that in skin dECM, in a wound dressing to determine whether it can be used as a pro-angiogenic therapy for effective skin wound healing. The NEhdHS was developed using an elastic, biocompatible, and biodegradable polymer, PLCL, and applying electrospinning technology to develop a scaffold that provides a moist ventilated environment. Such features are considered basic requirements for an effective wound dressing. The NEhdHS had greater rigidity than, and similar pore size and porosity to, the PLCL and gelatin-containing PLCL scaffolds. Moreover, it had the best cell adhesion and proliferation properties. The results of this study show that the NEhdHS can form a humid well-ventilated environment and enhance granulation tissue formation and epithelialization. Moreover, the NEhdHS not only regenerates tissue rapidly to minimize inflammation by increasing initial M2 macrophages and promoting angiogenesis—including the proliferation of ECs and the formation of matured vascular structures—but also it reduced scarring by rapidly replacing collagen type III with the stronger collagen type I. Therefore, the NEhdHS is considered to have potential as a pro-angiogenic therapeutic for enhancement of wound contraction and collagen remodeling, resulting in scarless wound healing. Furthermore, the developed NEhdHS has potential for use in wound healing of organs other than skin, such as wounds related to heart infarcts.
Footnotes
Acknowledgments
This study was supported by the KIST Institutional Program (project 2E26900), the KU-KIST Graduate School of Converging Science and Technology Program, and a grant of the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (2016R1A2B2009550), Republic of Korea.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.