
Abstract
Peripheral arterial disease causes blood vessel dysfunction that requires surgical intervention. Current surgical interventions employ synthetic or allogeneic vascular grafts, which offer biocompatible material solutions that are not able to regenerate or grow with the patient. Decellularized scaffolds have gained significant momentum in the past few years, since they have the potential to regenerate in the patient. The aim of this study was to investigate the effects of modified decellularization protocol on the biocompatibility and immunogenicity of allogeneic rat abdominal aorta in an orthotopic rat model. Native syngeneic Wistar (W) and allogeneic Dark Agouti (DA) aortas, together with decellularized allogeneic DA aortas, were assessed histologically, immunohistochemically, and biomechanically. The immunogenicity of the untreated and decellularized syngeneic and allogeneic grafts was assessed in W rats, implanted orthotopically. Following implantation for 6 weeks, the grafts were explanted and assessed for the presence of T cells and macrophages by immunohistochemistry, and for their biomechanical integrity and histoarchitecture. No obvious histoarchitectural differences were observed between the native W and DA aortas, with both presenting similar three-layered structures. Histological analysis of decellularized DA aortas did not reveal any remaining cells. Explanted native DA allografts showed media necrosis, partial elastic fiber degradation, and adventitia thickening, as well as infiltration by lymphocytes (CD3+, CD4+) and macrophages (CD68+) in the adventitia. The explanted decellularized DA allografts indicated reduced immune injury compared to the explanted native DA allografts. The explanted native W syngeneic grafts showed a mild immune response, with an intact media and no lymphocyte infiltration. The explanted native DA allografts showed significantly lower collagen phase slope than the decellularized DA allografts before implantation, and significantly higher thickness than the explanted decellularized DA allografts. The results indicated that the modified decellularization protocol did not affect significantly the mechanical and histological properties of the native DA rat aorta. Overall, the immune response was improved by decellularization. Native DA allografts induced an adverse immune response in W rats, whereas syngeneic W grafts showed good tissue integration
Impact Statement
The generation of a small-caliber arterial graft, utilizing a large vessel of a small animal, such as the aorta of the rat or rabbit, for clinical use in the peripheral arterial tree, can widen the options for arterial prostheses. This in vivo study demonstrated the ability of the decellularization protocol that was used to produce a noncytotoxic acellular small-caliber arterial graft, with sufficient biomechanical and biological integrity to withstand the demanding flow and pressure environment of the rat aorta. This work also demonstrated the superiority of the decellularized homograft over its intact counterpart, in terms of lower immunogenicity.
Introduction
Peripheral arterial disease is a highly prevalent and debilitating condition that affects more than 25 million patients in Europe and North America alone.1,2 Peripheral arterial disease leads to the damage of blood vessels, which can be replaced by synthetic, autologous, or allogeneic vascular grafts. Current replacement approaches employ biocompatible material solutions that are not able to regenerate or grow with the patient. The gold standard for vascular grafting is autologous tissue, such as reversed saphenous vein graft. 3 Despite its low cost and nonimmunogenicity, autologous tissue does not represent the ideal solution due to its limited availability and size mismatch. 4 Synthetic grafts, made of expanded-polytetrafluoroethylene (ePTFE) or Dacron, have been reported to give successful outcomes in large-diameter arterial reconstructions (>8 mm), but not for small-diameter arterial reconstructions (<5 mm), due to thrombosis and limited reendothelialization.5,6 In addition, cryopreserved arterial allogeneic grafts have a limited availability and durability, due to calcification, immunogenicity, and thrombogenicity. 7
The shortcomings of the conventional grafts have prompted the investigation of new approaches for peripheral artery reconstructions, such as the fabrication of tissue-engineered small-diameter vessels. Several studies have reported on the development of small-diameter vascular graft using naturally-derived proteins, such as collagen, fibrin,8–11 and synthetic polymers. 12 However, the inadequate mechanical properties of these grafts13–15 have prompted workers in the field to adopt alternative approaches, such as the use of decellularized tissue, which has been successfully used for tissue reconstructions, such as heart valves, bladder, tendons, and meniscus.16–22
Decellularization represents a promising approach for overcoming the limited availability of autologous small-diameter vascular conduits, as well as the limited availability of histocompatible allogeneic grafts since decellularization has the potential to remove the major antigenic determinants of allogeneic grafts. The latter has been effectively demonstrated by the successful translation of decellularized aortic and pulmonary allogeneic heart valves in the clinical setting,20,22 whereas a number of studies have reported promising results with decellularized small-diameter vascular grafts.23–26
This study was part of an overarching project that was aimed at creating a small-caliber arterial graft for clinical use, utilizing the decellularized rat aorta. This approach was chosen due to the arterial properties of the rodent graft and its suitable size for small-caliber arterial reconstructions in humans. To the best of the authors' knowledge, such an approach has not been reported in the literature. Dark Agouti (DA) rat abdominal aortas were decellularized using the widely employed detergent sodium dodecyl sulfate (SDS)27–30 in 3-[(3-cholamidopropyl) dimethylammonio]-1-propanesulfonate (CHAPS) buffer.23,25,26 Previously, we have reported on the effect of this modified decellularization protocol on the mechanical and histological integrity of DA rat aortas in vitro. 31 This study was focused on assessing the performance of the decellularized graft under orthotopic allogeneic transplantation in inbred Wistar (W) rats without immunosuppression, before proceeding to heterotopic xenotransplantation. This specific animal model was chosen since the inbred W and inbred DA rats differed in both their major and minor histocompatibility loci (MHC I and II). Moreover, the orthotopic transplantation was chosen to assess the decellularized graft in the more demanding, higher pressure environment of the aorta. The elicited immune response was evaluated in terms of inflammatory cell infiltration into the implanted grafts, as well as in terms of the histoarchitectural and biomechanical changes in the implanted grafts, after 6 weeks of implantation.
Materials and Methods
Experimental animals
The study was conducted using 40 male inbred W and 20 male inbred DA rats, which were maintained in accordance with the European Directive 2010/63 for the protection of animals used for scientific purposes and the “Guide for the Care and Use of Laboratory Animals.” 32 All procedures were carried out in the animal facility of the Biomedical Research Foundation of the Academy of Athens (EL25BIO003). The experimental protocol was approved by the competent veterinary authority of the Biomedical Research Foundation of the Academy of Athens (7047/27-11-2012), in accordance with the Greek legislation on the protection of experimental animals and the European Directive 2010/63.
Specimen procurement and dissection
The abdominal aorta was approached through a midline laparotomy incision under isoflurane anesthesia (IsoFlo; Abbott; 2.5%, 0.5 L/min O2), as described by Onuta et al. 33 and Hwang et al., 25 and the side branches were carefully cauterized (HTC; FLAB). The aorta was then mobilized and transected between a point distally to the left renal artery and proximally to the iliac bifurcation. The harvested conduit was flushed with normal saline. 33 Twenty native aortas from 10 DA (DA-W group; allogeneic control) and 10 W (W-W group; syngeneic control) rats were orthotopically implanted untreated in W rats. Moreover, 10 DA aortas were decellularized using a modified protocol 31 and implanted orthotopically in W rats (n = 10; decell DA-W group). The implanted aortas were explanted after 6 weeks and tested histologically (n = 2 from each group), immunohistochemically (n = 2 from each group), and biomechanically (n = 6 from each group).
Decellularization
The decellularization of the rodent abdominal aortas was carried out as described previously 23 with modifications. 31 Briefly, 20 aortas of ∼15 mm in length were incubated with CHAPS solution (8 mmol/L CHAPS [AppliChem], 1 mol/L NaCl, and 25 mmol/L EDTA in phosphate-buffered saline [PBS; Sigma]) at pH 8 for 22 h, followed by brief washes in PBS. The aortas were further incubated with SDS solution (1.8 mmol/L SDS [Sigma], 1 mol/L NaCl, and 25 mmol/L EDTA in PBS) at pH 7.5 for 24 h, followed by three washes, 5 min each, in PBS to completely remove the detergent. Finally, and modifying the previously described protocol, 24 the aortas were incubated at 37°C for 48 h in alpha minimal essential medium (a-MEM; Gibco Life Technology), containing 40% (v/v) fetal bovine serum (FBS; Gibco Life Technology) and 1000 U/mL penicillin-streptomycin (Gibco Life Technology). FBS was added for removal of residual DNA from the scaffolds (Gui et al. 24 ), since it contains DNAses and RNAses activated at 37°C in an incubator. In addition, FBS can be stored for a minimum 10 days at 4°C without altering its properties, while it has been approved by FDA for several cellular and tissue engineered products. On the other hand, protocols that use external DNAses and RNAses or EGM-2 are of a higher cost due to the fact that a nuclease solution must be used immediately and is stable only for 3–5 h, creating storage issues.18,23 Moreover, this step does not alter the mechanical properties of the scaffold, as assessed by our group. 31 All decellularization steps were carried out under agitation and sterile conditions.
Implantation procedure
Anesthesia and aortic mobilization were performed as in the case of donor preparation, while heparin was added in a dose of 10 IU/100 g body weight intravenously. The aorta was transplanted just distally to the renal artery and proximally to the iliac bifurcation in an end-to-end continuous manner with 8-0 polypropylene suture (Prolene; Ethicon,). No additional anticoagulation was administered postoperatively. Postoperatively, 5 mg/kg SC carprofen (Rimadyl; Pfizer) daily and 150 mg/kg SC amoxicillin (Amoxil; GlaxoSmithKline) twice a day were administered for 3 days, for pain and antibioprophylaxis, respectively. The recipient W rats were euthanized 6 weeks postoperatively, and the grafts, with ∼2 cm surrounding tissue, were removed from the recipients.
Histology
The tissue morphology and cellular content of the native, decellularized, and explanted grafts were assessed by histology. Whole aorta segments measuring 10 mm in length were isolated and fixed in 10% (v/v) neutral buffered formalin (Sigma-Aldrich) overnight at 4°C. The samples were then dehydrated by sequential immersion in graded concentrations of ethanol (70% v/v, 90% v/v, and 100% v/v), in distilled water for 1 h each, before they were immersed thrice in xylene for 1 h each time. The samples were then placed into metal molds that were partially filled with paraffin. The molds were transferred onto a cold plate, to initiate wax solidification and secure sample orientation, and then were filled with paraffin. The molds were placed onto the cold plate again, until the wax was completely solid. Subsequently, the paraffin blocks were removed from the molds and sectioned using a microtome at a thickness of 6 μm. Circumferential sections were cut from the central region of the grafts, to avoid the suture lines. Subsequently, the sections were transferred into a water bath at 50°C and onto microscope slides. The slides with the tissue sections were dried on a 60°C hotplate. Before staining, the sections were dewaxed by sequential immersion in two individual pots with xylene for 10 min each, and were then sequentially rehydrated by immersion in graded concentrations of ethanol (2 × 5 min 100% v/v, 1 × 2 min 95% v/v, and 1 × 2 min 70% v/v) in distilled water.
The general histoarchitecture of the grafts was evaluated using standard hematoxylin and eosin (H&E; Merck) staining. Sections were immersed into Mayer's hematoxylin for 1 min, rinsed under tap water for 5 min, and then immersed into eosin for 3 min. Masson's trichrome was used to visualize collagen fiber alignment and cell nuclei according to the method described by the manufacturer (Sigma-Aldrich). Briefly, sections were treated with Weigert's iron hematoxylin for 5 min, and then in Biebrich scarlet-acid fuchsin and aniline blue for 6 and 5 min, respectively. Elastica Van Gieson was used to visualize elastic fibers and cell nuclei according to the manufacturer's instructions (Sigma-Aldrich). Briefly, sections were immersed in Weigert's resorcin fuchsin solution for 11 min, followed by Weigert's iron hematoxylin and picrofuchsin solution for 5 and 2 min, respectively. All stained sections were dehydrated again in graded concentrations of ethanol (70% v/v, 90% v/v, and 100% v/v) in distilled water, cleared with xylene, and mounted with Corbit Balsam mountant. Images were captured using a Nikon TE300 Eclipse light microscope, incorporating a Nikon Digital Sight DS-U3 camera controller, and processed through the NIS-Elements D Microscope Imaging Software (Nikon Instruments).
Immunohistochemistry
The elicited immune response was evaluated in terms of inflammatory cell (T cells, monocytes, and macrophages) infiltration by immunohistochemical staining. The presence of smooth muscle cells (SMCs)/fibroblasts and endothelial cells (ECs) in the native and explanted grafts was also investigated by immunohistochemical staining. Whole aorta samples measuring 10 mm in length were isolated and fixed in zinc fixative at 4°C, dehydrated, and embedded in paraffin wax, as described above. Circumferential sections (6 μm) were cut close to the central region of the samples, dewaxed, and stained. Monoclonal antibodies against CD31 [ECs; PECAM-1(M-20)-R; Santa Cruz Biotech], calponin (SMCs/myofibroblasts; 46794; Abcam), CD68 (monocytes and circulating and tissue macrophages; MCA341GA; AbD Serotec), CCR7 (M1 macrophage subtype; rabbit monoclonal Anti-CCR7 antibody [Y59], ab32527; Abcam), and CD206 (M2 macrophage subtype; rabbit polyclonal to Mannose Receptor, ab64693; Abcam) were used to stain sections of native and explanted aortas.34,35 Explanted aortas were also stained with anti-CD3 (T cells at all stages of development; ab5690; Abcam) and anti-CD4 (T-regulatory and T-helper cells; ab125711; Abcam) antibodies. Fresh porcine mitral valve posterior leaflet was used as positive control for calponin staining, whereas spleen was used as positive control for T cell staining. Isotype control antibodies (normal rabbit IgG for CD31, calponin, and CD3; Calbiochem; mouse IgG1 for CD4 and CD68; Dako) and omission of the primary antibody (secondary antibody control) served as negative controls. Immunolabeling of anti-CD31, anti-CD68, anti-CD3, and anti-CD4 was carried out using the EnVision®+ Dual Link System-HRP (DAB+; K4065; Dako). Hydrogen peroxide (Sigma) was used to block endogenous peroxidase. Images were captured under light microscopy, as described above.
Immunofluorescence staining was conducted for the immunolabeling of anti-calponin, anti-CCR7, and anti-CD206. Briefly, samples were incubated in blocking medium (1% w/v bovine serum albumin in PBS) for 60 min at room temperature (R)T, before they were washed once in TBS/Tween and twice in TBS, for 5 min each time. Incubation in primary antibody was carried out for 1 h at RT. All samples were then washed twice in TBS/Tween and twice in TBS for 5 min each, and incubated with the secondary antibody (Alexa Fluor 488, donkey anti-rabbit, IgG; Jackson) for 30 min in the dark at RT. The samples were then washed shortly in TBS/Tween and TBS and incubated in Roti®-Mount FluorCare DAPI, or in 1 μM DAPI solution (Life Technologies) for 15 min at RT, followed by mounting. Images were captured using B-2A and UV-2A Nikon filters, with the microscope described above.
Biomechanical characterization
The mechanical integrity of the explanted grafts was assessed under uniaxial tension. Longitudinal samples (n = 6 for each group) measuring 5 mm in length by 2.5 mm in width were isolated from the aortas and subjected to low strain-rate uniaxial tensile loading to failure, according to the method reported previously, 36 with minor modifications. The testing was conducted in a Zwick/Roell tensile tester (model Z 0.5) equipped with a 200 N load cell. Before testing, the thickness of the samples was measured using a Sylvac position sensor equipped with a Kalibriert force sensor (model: μS246). The test sample was positioned between the position sensor and a bottom plate, and the position sensor was lowered in a gradual and controllable manner, till it touched the sample and a force was registered. The distance between the position sensor and bottom plate was recorded as the sample thickness. The thickness of the samples was measured at three different points along their length, and averaged. Subsequently, the samples were clamped at their ends, using sandpaper and a small amount of superglue to prevent slippage, under zero strain on the tensile tester, which was set to produce a specimen preloading of 0.005 N before the operating program started to acquire any data. During testing, the specimens were preconditioned for 10 cycles at a rate of 10 mm/min, before they were sequentially stretched to failure at the same rate.
Failure was assumed when the first decrease in load was detected during specimen extension, whereas the mode of failure observed was near middle-section necking and rupture for all the samples tested. The sample extension (Δl, in mm) and corresponding generated load (F, in Newtons), which were recorded during the final loading to failure phase of the test, were converted to engineering strain (ɛ) and engineering stress (σ, in MPa), respectively. 36 The stress-strain behavior of each sample was analyzed by means of six parameters, 36 including the elastin (El-E) and collagen (Col-E) phase slopes, transition stress (σTrans) and strain (ɛTrans), ultimate tensile strength (σUTS), and failure strain (ɛUTS). The biomechanical parameters for each sample were calculated and averaged over the number of samples in each group.
Data analysis
The biomechanical testing results were presented as means together with their 95% confidence intervals. The data were analyzed by one-way analysis of variance, followed by calculation of the minimum significance difference (MSD). Statistical significance was determined at the 0.05 confidence level. 37
Results
Histological analysis
The histological results of the native, decellularized, and explanted syngeneic and allogeneic grafts are illustrated in Figure 1 and at higher magnification in Figure 2. The results indicated that there were no apparent differences between the histoarchitectures of native W and DA rats, with the aorta of both strains demonstrating a three-layered structure, comprising the tunica intima (outer layer of cells facing the lumen), tunica media, consisting of SMCs, collagen fibers and elastic fibers organized in a concentric manner, and adventitia, mainly consisting of collagen fibers, fibroblasts, and loosely-aligned elastic lamellae.31,38,39 The decellularized DA rat aorta was shown to be completely void of any observable cells and cellular debris, while it maintained the general native trilaminar histoarchitecture with preserved collagen and elastic fibers. However, it also appeared swollen with obvious gaps in the extracellular matrix (ECM), especially at the sites in the adventitial layer that were heavily populated with cells.

Histological characterization of whole cross-sections of native, decellularized and explanted aortas, stained with H&E, Masson's Trichrome or Elastica Van Gieson. W, W rat native aorta; DA, DA rat native aorta; decell DA, decellularized DA rat aorta; W-W, W rat aorta implanted in W rat (syngeneic model); DA-W, DA rat aorta implanted in W rat (allogeneic model); decell DA-W, decellularized DA rat aorta implanted in W rat (allogeneic model). Scale bars indicate 500 μm. H&E: cell nuclei and connective tissue were blue/black and pink stained, respectively; Masson's Trichrome: cell nuclei, collagen fibers, and cytoplasm/muscle fibers were stained blue/black, blue and red, respectively; Elastica Van Gieson: cell nuclei, elastic fibers, and collagen fibers were stained black-brown, black, and red, respectively. H&E, hematoxylin and eosin. Color images are available online.
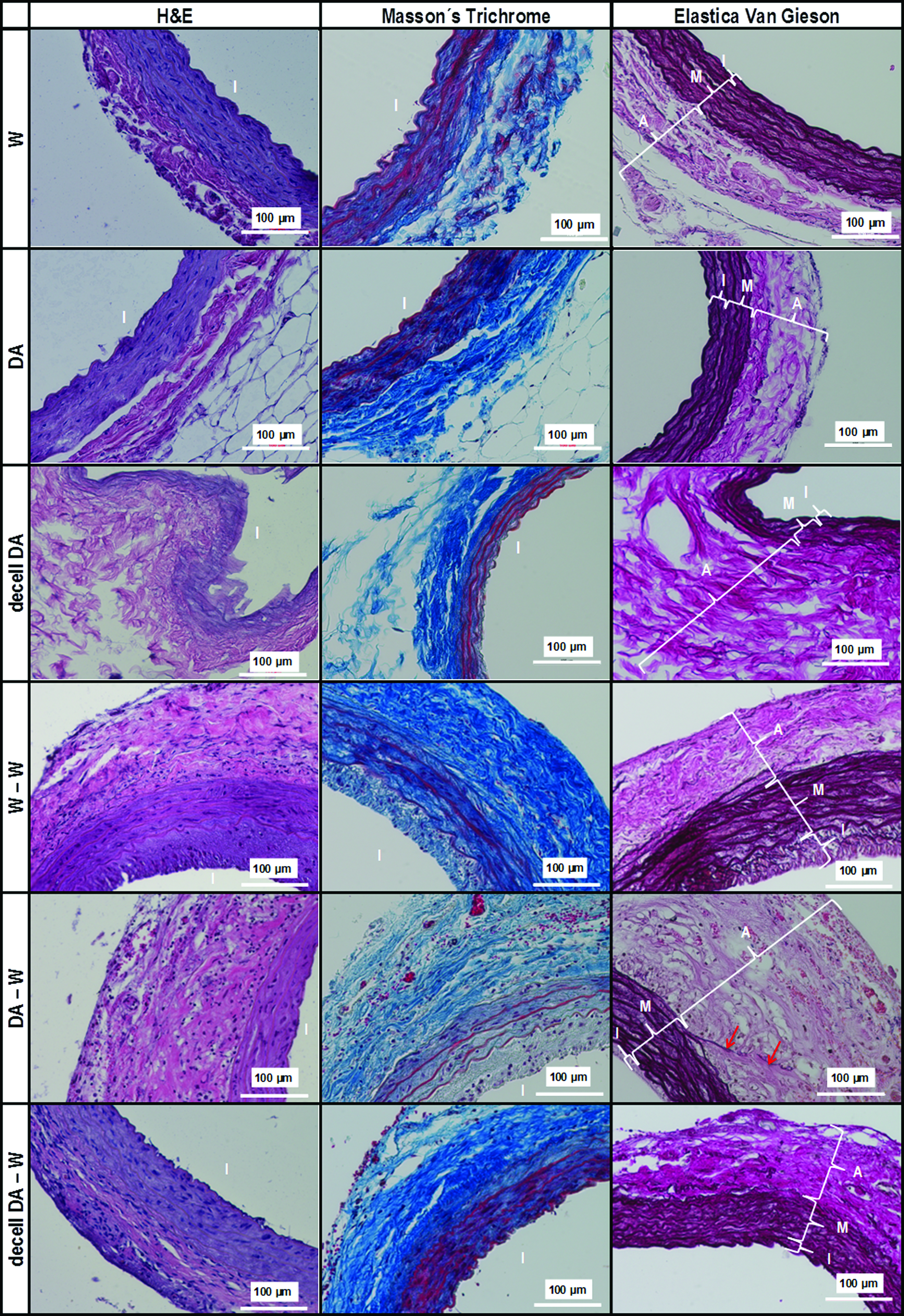
Histological characterization of native, decellularized and explanted aortas, stained with H&E, Masson's Trichrome or Elastica Van Gieson. W, W rat native aorta; DA, DA rat native aorta; decell DA, decellularized DA rat aorta; W-W, W rat aorta implanted in W rat (syngeneic model); DA-W, DA rat aorta implanted in W rat (allogeneic model); decell DA-W, decellularized DA rat aorta implanted in W rat (allogeneic model). I, tunica intima; M, tunica media; A, adventitia. Red arrows indicate elastic fiber degradation. Scale bars indicate 100 μm. H&E, cell nuclei and connective tissue were blue/black and pink stained, respectively; Masson's Trichrome: cell nuclei, collagen fibers, and cytoplasm/muscle fibers were stained blue/black, blue, and red, respectively; Elastica Van Gieson: cell nuclei, elastic fibers and collagen fibers were stained black-brown, black, and red, respectively. Color images are available online.
The explanted syngeneic grafts (W-W; Figs. 1 and 2) demonstrated an intact media with intact collagen and elastic fibers, while their adventitia appeared more compact compared to their nonimplanted control (W), suggesting the production of ECM. The syngeneic grafts also presented a noticeable intimal thickening and cellular content throughout their thickness. The explanted decellularized allografts (decell DA-W; Figs. 1 and 2) showed a similar response to syngrafts, with preserved elastin and collagen fibers in the media and a more compact adventitia compared to their nonimplanted control (decell DA). Moreover, they did not show any thickening of their intima, while they demonstrated a significant cell repopulation throughout their thickness, as evidenced by the H&E staining. The latter observation highlighted the noncytotoxic nature of the decellularized grafts, which resulted in cell colonization and subsequent ECM remodeling.
On the other hand, the explanted allografts (DA-W; Figs. 1 and 2) demonstrated disruption of the elastin and collagen network, as well as cellular loss in the media, as evidenced by H&E and the distinct gaps in the sites that were previously occupied by cells. Moreover, the DA-W allografts experienced cellular infiltration in the adventitia and adventitial fibrosis that resulted in significant thickening of their adventitia, as well as neointimal formation.
Immunohistochemical analysis
The immunohistochemical results of the native and explanted syngeneic and allogeneic grafts are illustrated in Figure 3 (CD31), Figure 4 (CD68), Figure 5 (CD3 and CD4), Figure 6 (calponin), Figure 7 (CCR7), and Figure 8 (CD206). ECs (CD31+) were observed in the lumen and vasa vasorum of the native DA and W aortas, and explanted syngrafts (W-W) and untreated allografts (DA-W) (Fig. 3). In contrast, no CD31+ cells were visible on the explanted decellularized allografts (decell DA-W; Fig. 3). Putative SMCs or myofibroblasts (calponin+) were observed in the tunica media of the native DA and W aortas, and the explanted syngrafts (W-W), but not in the tunica media of the explanted untreated (DA-W) allografts (Fig. 6). Instead, the untreated (DA-W) allografts demonstrated calponin+ cells only in their intima. No calponin+ cells were observed in the decellularized (decell DA-W) allografts (Fig. 6). The native DA and W aortas were stained negative for CD68 (circulating and tissue macrophages and monocytes) (Fig. 4), whereas some CD68+ infiltrates were observed in the adventitia and intima of the explanted syngrafts (W-W; Fig. 4). Extensive infiltration of CD68+ cells was observed in the case of the untreated allografts (DA-W), which was spread uniformly throughout the thickness of these grafts (Fig. 4). CD68+ cells were also observed in the subendothelial region of the intima, as well as the adventitia, of the explanted decellularized allografts (decell DA-W; Fig. 4). However, the infiltration of CD68+ cells in the explanted decellularized allografts was only regional, and not spread throughout the graft, as in case of the explanted untreated allografts. Despite the lack for CD68+ staining in the native DA and W aortas, CCR7+ cells (M1 macrophage subtype) were detected in these tissues (Fig. 7). CCR7+ cells were also detected in the intima and media of the explanted syngrafts (W-W; Fig. 7). Similar observations were apparent in the case of the explanted allografts (DA-W; Fig. 7), in which CCR7+ infiltrates were observed in their intima and adventitia. On the other hand, the explanted decellularized allografts (decell DA-W; Fig. 7) demonstrated a milder infiltration of CCR7+ cells, compared to the W-W and DA-W grafts, which was limited in their adventitia layer. No CD206+ cell infiltration was detected in any of the native tissues (DA and W), or syngraft (W-W), untreated allograft (DA-W) or decellularized allograft (decell DA-W) explants (Fig. 8).
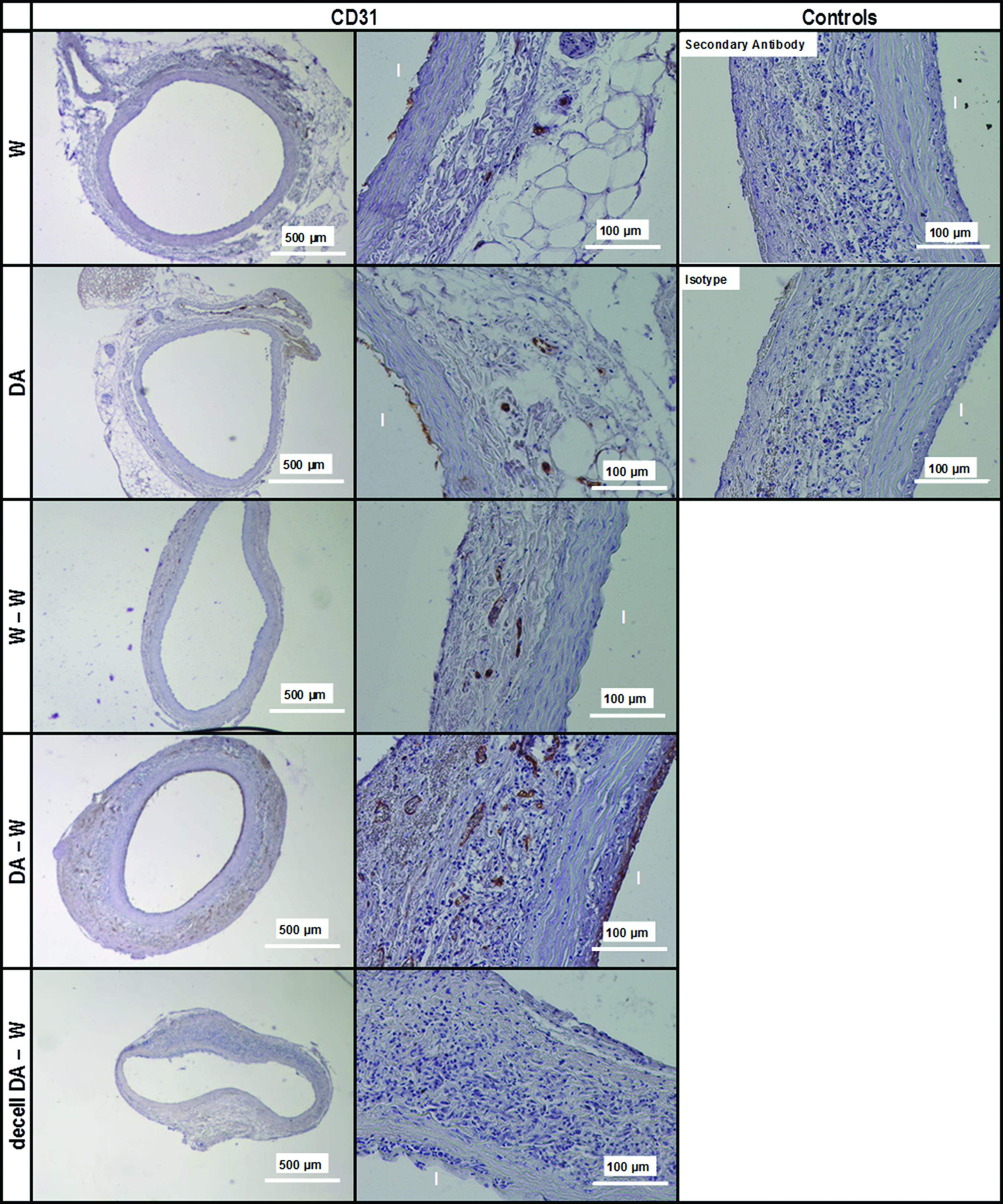
Immunohistochemistry of native and explanted aortas stained against CD31 (ECs). W, W rat native aorta; DA, DA rat native aorta; W-W, W rat aorta implanted in W rat (syngeneic model); DA-W, DA rat aorta implanted in W rat (allogeneic model); decell DA-W, decellularized DA rat aorta implanted in W rat (allogeneic model); I, tunica intima. Scale bars indicate 100 μm (high magnification sections) or 500 μm (whole vessel cross-section). Tissue positive for CD31 was stained brown, cell nuclei were stained blue/black. ECs, endothelial cells. Color images are available online.

Immunohistochemistry of native and explanted aortas stained against CD68 (pan-macrophage marker). W, W rat native aorta; DA, DA rat native aorta; W-W, W rat aorta implanted in W rat (syngeneic model); DA-W, DA rat aorta implanted in W rat (homogeneic model); decell DA-W, decellularized DA rat aorta implanted in W rat (allogeneic model); I, tunica intima. Scale bars indicate 100 μm (high magnification sections) or 500 μm (whole vessel cross-section). Tissue positive for CD68 was stained brown, cell nuclei were stained blue/black. The red arrows and red ovals indicate sites of CD68+ cell infiltration. Color images are available online.

Immunohistochemistry of explanted aortas stained against CD3 and CD4 (lymphocytes). W-W, W rat aorta implanted in W rat (syngeneic model); DA-W, DA rat aorta implanted in W rat (allogeneic model); decell DA-W, decellularized DA rat aorta implanted in W rat (allogeneic model); I, tunica intima. Scale bars indicate 100 μm (high magnification sections) or 500 μm (whole vessel cross-section). Tissue positive for CD3 or CD4 was stained brown, cell nuclei were stained blue/black. The red arrows and red ovals indicate sites of CD3+ and CD4+ cell infiltration. Color images are available online.

Immunofluorescence staining of native and explanted aortas stained against calponin (SMCs and myofibroblasts). W, W rat native aorta; DA, DA rat native aorta; W-W, W rat aorta implanted in W rat (syngeneic model); DA-W, DA rat aorta implanted in W rat (homogeneic model); decell DA-W, decellularized DA rat aorta implanted in W rat (homogeneic model); I, tunica intima; M, tunica media; A, adventitia. Scale bars indicate 100 μm (high magnification sections) or 500 μm (whole vessel cross-section). Tissue positive for calponin was stained green, cell nuclei were stained blue. SMCs, smooth muscle cells. Color images are available online.
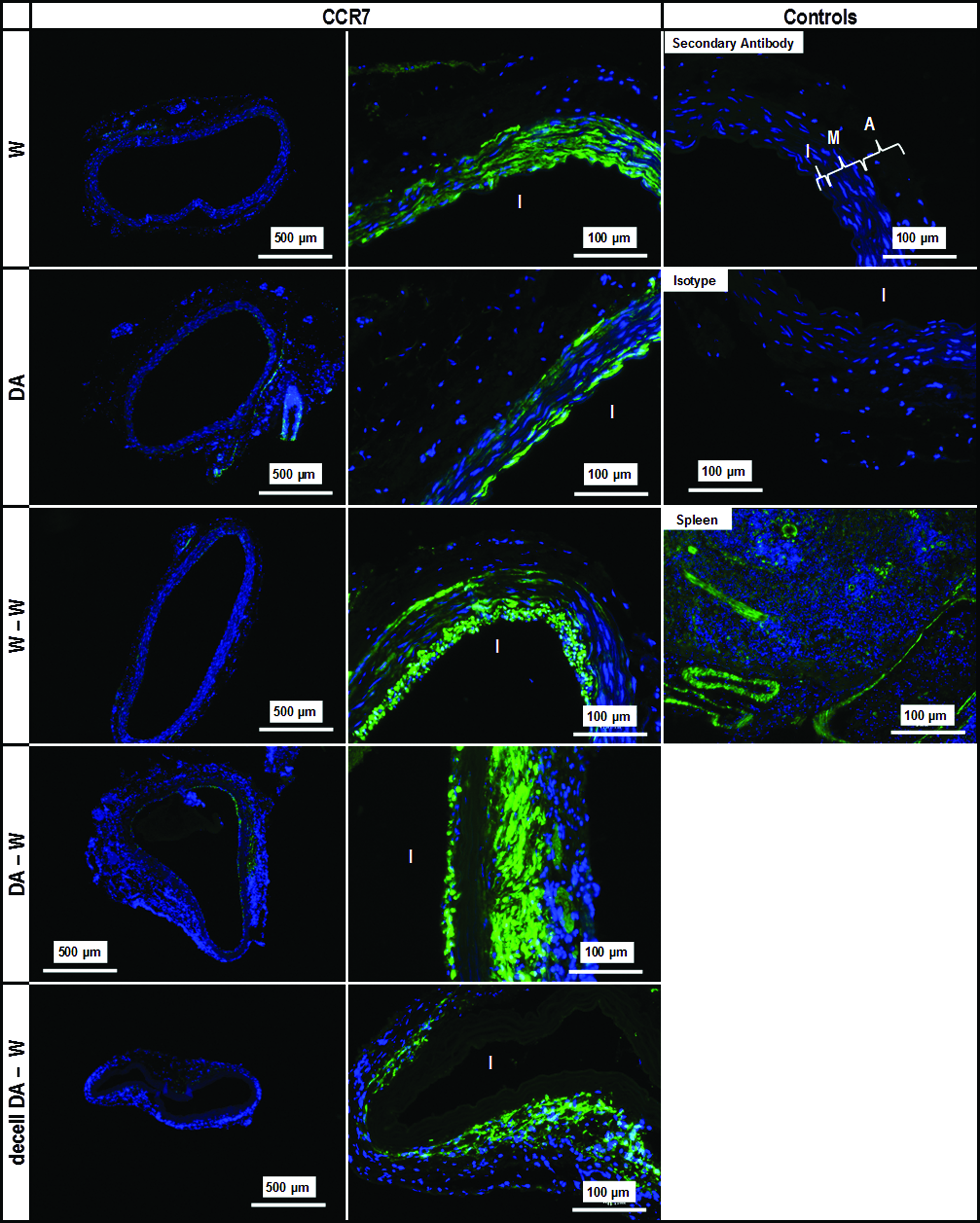
Immunofluorescence of native and explanted aortas stained against CCR7 (M1 macrophage subphenotype). W, W rat native aorta; DA, DA rat native aorta; W-W, W rat aorta implanted in W rat (syngeneic model); DA-W, DA rat aorta implanted in W rat (homogeneic model); decell DA-W, decellularized DA rat aorta implanted in W rat (homogeneic model); I, tunica intima; M, tunica media; A, adventitia. Scale bars indicate 100 μm (high magnification sections) or 500 μm (whole vessel cross-section). Tissue positive for CCR7 was stained green, cell nuclei were stained blue. Color images are available online.
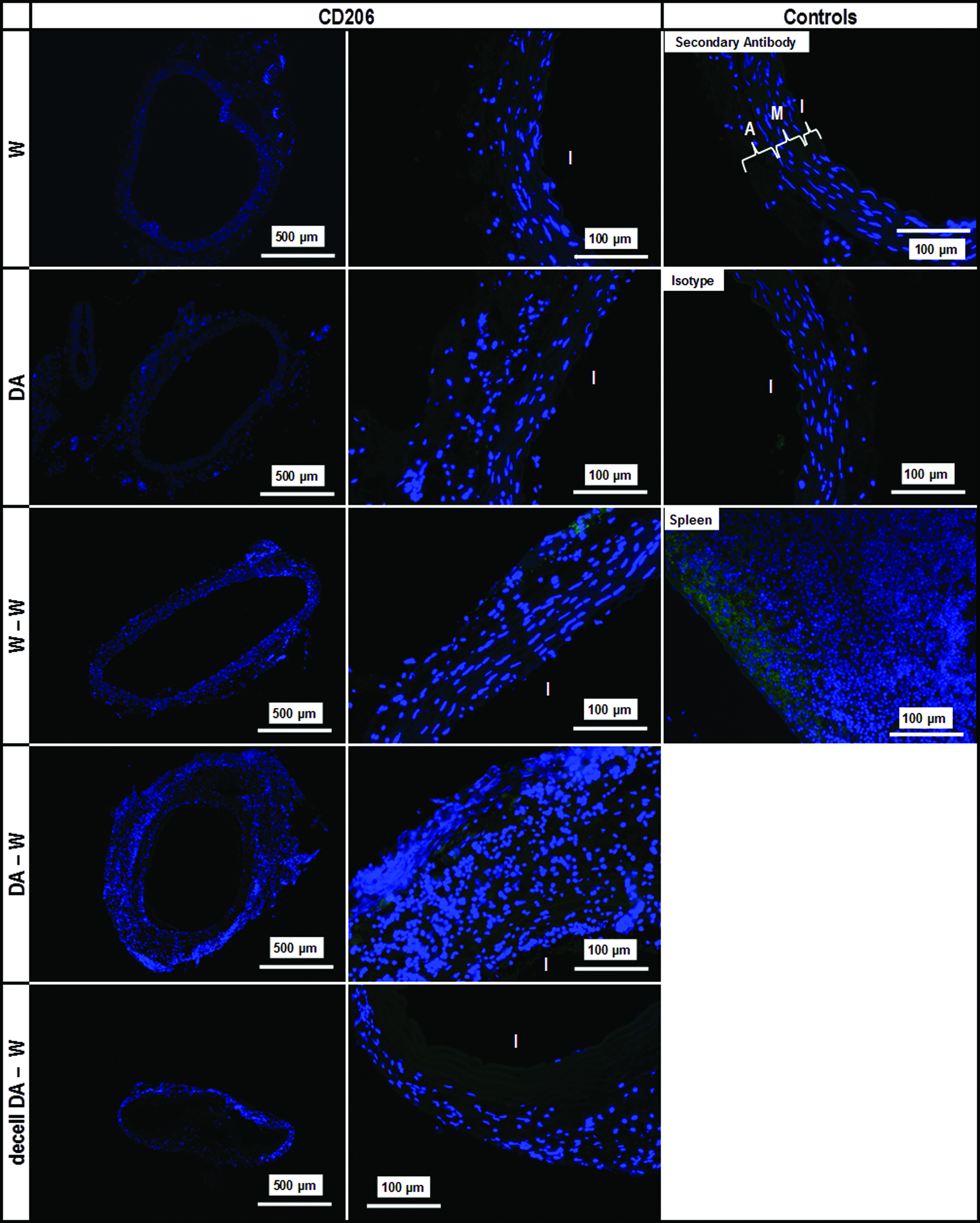
Immunofluorescence of native and explanted aortas stained against CD206 (M2 macrophage subphenotype). W, W rat native aorta; DA, DA rat native aorta; W-W, W rat aorta implanted in W rat (syngeneic model); DA-W, DA rat aorta implanted in W rat (homogeneic model); decell DA-W, decellularized DA rat aorta implanted in W rat (homogeneic model); I, tunica intima; M, tunica media; A, adventitia. Scale bars indicate 100 μm (high magnification sections) or 500 μm (whole vessel cross-section). Tissue positive for CD206 was stained green, cell nuclei were stained blue. Color images are available online.
No T cell infiltration could be observed in the explanted syngrafts (W-W; Fig. 5), whereas a significant infiltration of CD3+ cells could be observed in the adventitia of the explanted untreated allografts (DA-W). Some localized CD3+ cell presence could also be observed in the adventitia of the explanted decellularized allografts (decell DA-W; Fig. 5), but it was considerably reduced compared to the explanted untreated allografts (DA-W). The latter also demonstrated a sporadic infiltration of CD4+ cells in their adventitia, in contrast to the explanted decellularized allografts (decell DA-W), which did not show any evidence of CD4+ cell infiltration (Fig. 5). In general, the explanted untreated allografts (DA-W) demonstrated a prominent infiltration of mononuclear cells, which was significantly reduced in the case of the explanted syngrafts (W-W) and decellularized allografts (decell DA-W) (Figs. 4 and 5). There was no unspecific staining observed for both the secondary antibody and the isotype controls of all the abovementioned antibody stains (Figs. 3–8).
Mechanical testing
The mean biomechanical parameters of the explanted syngeneic and allogeneic grafts are illustrated in Figure 9. Figure 9 also features the corresponding mean biomechanical parameters of native W (W) and DA (DA) rat aortas, as well as of decellularized DA rat aortas (dec DA) that were produced using the same decellularization protocol. These data, which were obtained using the same uniaxial tensile testing protocol as in this study, were adopted from Katsimpoulas et al. 31 and were included in the analysis to better understand the potential changes in the biomechanics of the scaffolds following implantation.
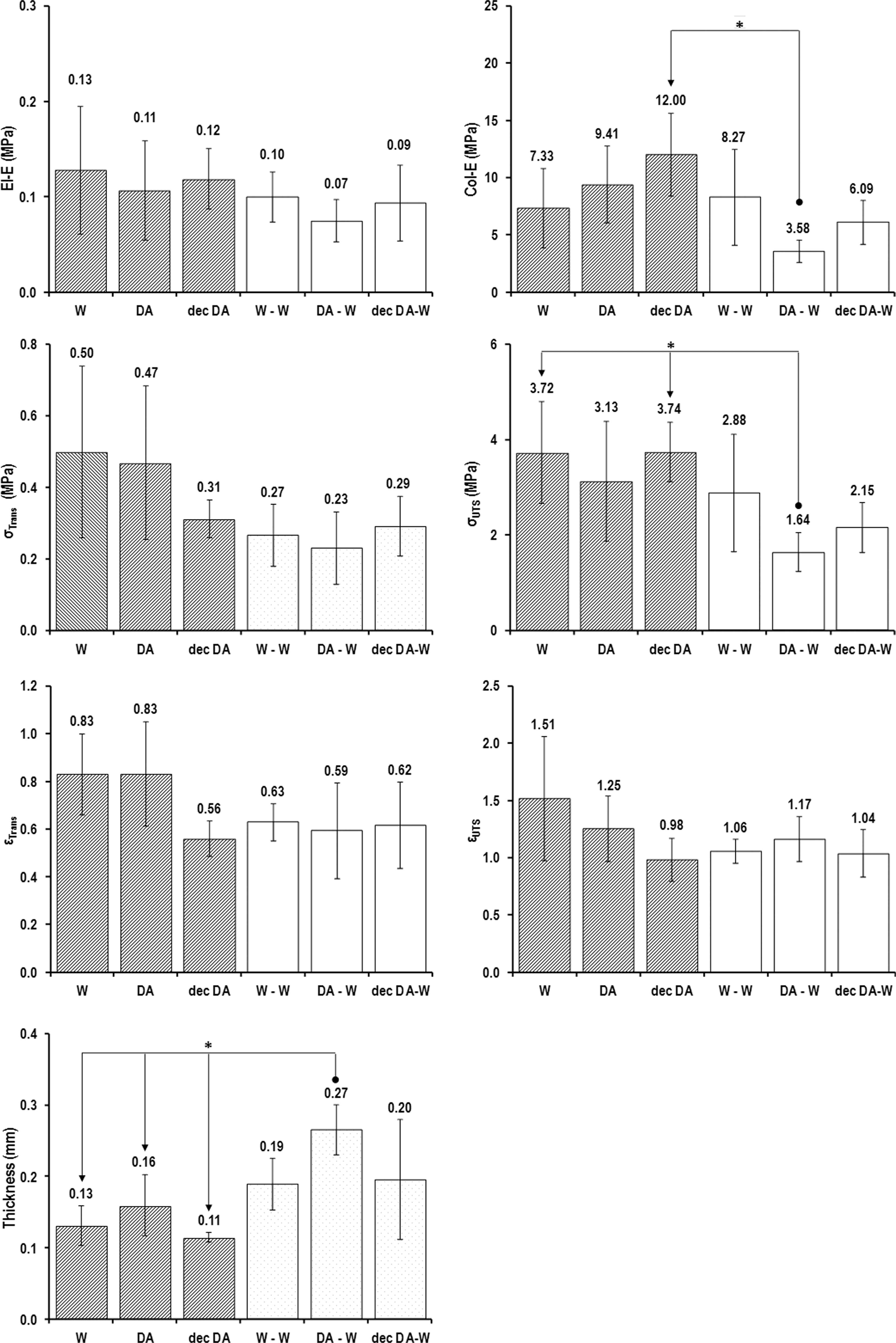
Mean biomechanical parameters of native, decellularized and explant aorta groups. W, W rat native aortas (n = 5) (adopted from Katsimpoulas et al. 31 ); DA, DA rat native aortas (n = 6) (adopted from Katsimpoulas et al. 31 ); dec DA, decellularized DA rat aortas (n = 6) (adopted from Katsimpoulas et al. 31 ); W-W, W rat aortas implanted in W rats (n = 6); DA-W, DA rat aortas implanted in W rats (n = 6); dec DA-W, decellularized DA rat aortas implanted in W rats (n = 6). Error bars indicate 95% CI. The arrow connectors indicate significant difference (*) between originator and end-arrow group. CI, confidence interval.
Statistically significant differences were found only in the collagen phase slope (Coll-E), ultimate tensile strength (σUTS), and thickness (p = 0.025, 0.027, and 0.004, respectively). In all three cases, the statistically significant differences arose from the differences between the explanted untreated allograft (DA-W) group and the other groups tested. Specifically, the DA-W group demonstrated the lowest Coll-E compared to the other groups, with the difference being statistically significant only compared to the decellularized DA (decell DA) group (MSD = 7.22). Similarly, the DA-W group achieved the lowest σUTS, with the difference being statistically significant when compared to the W and decell DA groups (MSD = 2.07). Moreover, the average thickness of the DA-W group was higher than any of the other groups, with the difference being statistically significant when compared to the native W and DA, and decell DA groups (MSD = 0.11). The explanted decellularized allograft (decell DA-W) group showed no significant differences compared to any of the other groups used in the study.
Discussion
This study was a part of an overarching project that aimed at creating a small-caliber arterial graft for clinical use, utilizing the decellularized rat aorta. Along these lines, the work was focused on assessing the performance of the decellularized DA aorta, in terms of its biomechanical integrity and arterial compatibility, and potential immunogenicity, under orthotopic allogeneic transplantation in W rats, before proceeding to heterotopic xenotransplantation in a large animal in a future study. The orthotopic transplantation was chosen to assess the graft in the more demanding pressure environment of the aorta.
In this study, native and decellularized aortas from inbred DA rats were orthotopically implanted into W inbred rats to simulate the allogeneic transplantation model, whereas W rat native aortas were orthotopically implanted into W rats as syngeneic controls. To date, there has been a scarcity of studies on DA rat tissues implanted into W rats; nevertheless, several studies have used tissues from other substrains of W rats for transplantation into DA rats.40,41 These rat strains differ in their major and minor histocompatibility loci, and the immune response in allogeneic models with these strains are mainly driven by the MHC I and II present on donor cells. 42 In this study, lymphocyte presence was investigated using anti-CD3 and anti-CD4 antibodies, since CD3 has been reported to be a pan-T cell marker 43 and CD4 a marker for T-regulatory and T-helper cells. 44 Macrophages were detected by the anti-CD68 antibody, which has been reported as a marker for pan-macrophages, 45 whereas the M1 and M2 macrophage subtypes were detected by anti-CCR7 and anti-CD206 immunofluorescent antibodies, respectively. M1 macrophages are typically activated by IFN-γ or lipopolysaccharides, producing proinflammatory cytokines, and are indicative of an immune response, whereas M2 macrophages are activated by cytokines, such as IL-4, IL-10, or IL-13, and produce either proliferation-inducing polyamines or proline to induce collagen production. M2 macrophages have been associated with wound healing and tissue repair and remodeling.34,35,46–48
Allograft transplantation usually leads to chronic rejection, which mainly consists of inflammation and intimal thickening. 49 In particular, this degenerative process induces a complete loss of SMCs in the media that, in turn, induces media necrosis, elastin degradation, SMC migration toward the intima, and intimal thickening throughout the length of the graft. 41 It has been hypothesized that medial necrosis might be due to a toxic effect of inflammatory cells present in the adventitia, especially lymphocytes, on SMCs in the media. 41 In this study, media necrosis, partial elastic fiber degradation, SMC migration toward the intima and lymphocyte (CD3+ and CD4+), and macrophage (CD68+) infiltration in the adventitia were evidenced in the explanted untreated allografts (DA-W), which also demonstrated a prominent increase in thickness of their adventitia (Figs. 1 and 2). Donor ECs and SMCs were most probably the main antigenic targets of these infiltrates, since the DA-W grafts were stained positively for CD31 in their lumen (Fig. 3) and presented a significant content of calponin+ cells in their intima (Fig. 6). Similar results were described by Mennander et al. 49 for DA rat thoracic aorta transplanted into Wistar Furth rats. The authors reported a peak of inflammatory cells and increase in adventitial thickness after 2 months of implantation.
The syngrafts showed a mild immune response, with an intact media (Fig. 2) and no lymphocyte presence (Fig. 5). Macrophages were observed in all explants, located mainly in the intima, media, and adventitia of the allografts, and in the media and intima of the decellularized allografts and syngrafts (Fig. 4). In all explants, the macrophages were identified as of the M1 subtype (inflammatory; Fig. 7), whereas no M2 macrophages (remodeling/repair) were observed in any of the explants (Fig. 8). In contrast to the DA-W allografts, the explanted decellularized allografts (decell DA-W) induced an immune response similar to the syngrafts (W-W), with a reduced immune injury (Fig. 2), low amount of lymphocyte infiltrates (Fig. 5), and macrophages that were localized mainly in regions of the adventitia (Fig. 7), although some macrophages were also observed in their intima region, as evidenced under CD68 staining (Fig. 4). This regional macrophage presence in the decell DA-W allografts might be due to inconsistencies in the application of the decellularization protocol, and subsequent cellular debris remnants in the grafts. However, these results suggested that the decell DA-W allografts demonstrated a similar performance to their W-W syngraft counterparts, and that the decellularization protocol was generally effective in removing the immunogenic material, such as cellular debris, of the grafts.
The decellularized aortas, both before (decell DA) and after (decell DA-W) transplantation, showed a well-maintained trilaminar structure, typical to abdominal rat aorta, 39 with well-maintained collagen and elastic fibers orientated concentrically along the circumferential direction in the media, and elastin lamellae in the adventitia (Figs. 1 and 2). Elastic fibers and lamellae represent one of the main components of the aortic wall.50,51 Reduction in the number of elastic fibers and elastic lamellae has been reported to cause a reduction of mural elastic resistance, 52 which could contribute to aneurysm formation. 53 The histological analysis of the decellularized aortas before implantation revealed absence of any observable cells or cellular debris throughout the thickness of the arterial wall. The explanted decell DA-W allografts demonstrated extensive cellular population in their media and adventitia, as well as evidence of remodeling of the adventitia, which was rather disrupted by the decellularization process (Fig. 2). However, no ECs could be observed in the lumen of the decell DA-W allografts, as evidenced by the CD31 staining (Fig. 3), or any detectable SMC presence, as evidenced by the calponin staining (Fig. 5). On the other hand, the explanted DA-W allografts showed an overgrowth of their adventitia, probably due to the recruitment of fibroblasts by inflammatory cells, in an attempt to replace the allogeneic tissue, 49 as well as neointima formation (Fig. 2).
The histoarchitectural changes in the explanted DA-W allografts (Figs. 1 and 2) had a direct effect on their mechanical properties. Specifically, the DA-W group demonstrated on average the lowest Coll-E and σUTS, and the highest macroscopic thickness, among the groups tested, indicating a deterioration in the integrity of these grafts (Fig. 9). These changes in the mechanical properties of the DA-W allografts have the potential to induce long-term structural failure. Moreover, the reduced moduli measured for the DA-W explants implied that there was a significant modulus mismatch between these allografts and the native aorta of the recipients. This could have potentially generated significant stress concentrations in the grafts and/or the surrounding aorta of the recipient, generating abnormal biomechanical stimuli to infiltrating cells. In addition, the high stress concentration regions could have potentially generated higher ECM damage, further attracting inflammatory and immune cells, and increasing the immunogenicity of these grafts. On the other hand, and in the absence of a functional vasa vasorum, the increase in the DA-W graft thickness in vivo could have generated progressively increased hypoxic conditions in the media of these grafts, which in turn caused higher migration of immune cells, such as macrophages, macrophages, neutrophils, dendritic cells, lymphocytes, and immune lymphoid cells, whose characteristic ability is to infiltrate in tissues with low nutrients and oxygen levels. 54
In contrast, the explanted decell DA-W allografts showed no significant differences in the mechanical properties compared to the native W rat aorta. Overall, these results suggested that the ECM of explanted decellularized scaffolds was more stable and better maintained after 6 weeks of implantation, in contrast to that of the untreated DA-W allografts, which showed partial disruption of their elastic fibers, adventitia thickening, and deteriorated mechanical properties, caused by the immune response of recipients.
In conclusion, the results from this study demonstrated that the modified decellularization protocol used in this study did not induce significant biomechanical or histological alterations of the DA rat aorta in vivo, whereas the immune response of the recipients was improved by the decellularization treatment compared to the untreated allografts. The latter elicited a significant adverse immune response, which resulted in adventitia fibrosis and thickening, media necrosis, and neointima formation, whereas the syngrafts showed good tissue integration and mild immune response. Future work will assess the presence of nucleic acid and phospholipid remnants in the decellularized scaffolds. Moreover, future work will also assess the performance, remodeling, and adaptation of the decellularized rat aorta graft in a heterotopic peripheral artery porcine model.
Footnotes
Acknowledgments
The authors would like to acknowledge the contribution of Karin Burgwitz at the Lower Saxony Centre for Biomedical Engineering Implant Research and Development for their technical support. This research was supported by the People Programme (Marie Curie Actions) of the EU 7 Framework Programme FP7/2007–2013/under the REA grant agreement number 317512, and the German Research Foundation through the Cluster of Excellence REBIRTH (From Regenerative Biology to Reconstructive Therapy; EXC 62).
Disclosure Statement
No competing financial interests exist for all authors.