
Abstract
Ever since the introduction of the concept of tissue engineering (TE), the field has developed and matured from a hype to a proper scientific discipline. Recently, the field is witnessing a reversal of the innovation drivers as it has started to move from a technology-driven science-focused field toward a patient-driven, manufacturing-focused one. This evolution is made possible through innovations at the interface between biology and technology, including robust biological building blocks, precise biomanufacturing technologies, in-depth characterization methods, and in silico models. Combining this with novel insights on TE-related regulatory sciences and business strategies, the field is ready to meet the grand challenge of designing, developing, and delivering living implants with the accuracy and robustness expected from inanimate implants, leading to sustainable, predictable, and vastly superior biological and clinical results.
Impact Statement
From this perspective, we discuss the different stages of development the tissue engineering (TE) field has gone through in its relatively young history. We discuss how TE is evolving from a technology-driven, science-focused field toward a patient-driven, manufacturing-focused one where patients' needs are translated into production process requirements, and subsequently into technological and biological innovations needed to meet the regulatory and clinical demands.
Introduction
Undoubtedly, the interdisciplinary field of TE has made vast progress since it was coined in the mid-80s, undergoing a dramatic technological but also conceptual evolution. However, to date there is still a lack of a widespread implementation of TE therapeutics in clinics with only four TE products having obtained to date official marketing authorization in the EU. These are Spherox (CO.DON), Holoclar (Chiesi Farmaceutici), MACI (Vericel), and Chondrocelect (TiGenix); however, the last two products are no longer authorized or have been suspended. 1 This demonstrates that there is still considerable progress to be made before a systematic and consistent pipeline of TE products to the clinic can be established.
A Historic Perspective
In the relatively young history of TE, roughly three periods can be distinguished (Fig. 1):

The three eras of TE. The years indicated in the figure are rough indications, not related to any particular event. TE, tissue engineering.
The first era of TE (∼1985–2000) is a perfect example of the brazenness that is typical for young and highly innovative fields. As any new technology or field going through the Gartner hype cycle, the first phase was characterized by bold claims and inflated expectations. Large investments were made in start-ups with the aim of making it to the clinics by the turn of the century. However, these promises were too high, and the suggested clinical introduction was not realistic. Furthermore, the challenge of creating living implants was ill defined at the time, and the teams approaching the challenge were still deeply embedded in their respective disciplines, be it on the technology or the biology side. The main innovation drivers were technological (mostly related to biomaterials) or biological (mostly related to stem cells) innovations from the respective disciplines. Around the 2000s, many of these start-ups had failed or folded, and the field was going through the “trough of disillusionment” (cf. Gartner hype cycle). 2 However, in academia, the TE field continued its evolution into a distinct scientific field with its own community and jargon.
The second era of TE (∼2000–2015) can be described as the coming of age of TE as a scientific discipline, finally overcoming some of the major challenges related to its interdisciplinarity. A new generation of researchers appeared, which could be described as the first real tissue engineers, able to cross the lines between the different disciplines. Paradigms were questioned and alternatives such as developmental engineering (DE)3,4 were proposed, while major breakthroughs in technologies such as the development of the induced pluripotent stem cell (iPS) technology, 5 gene editing, 6 and bioprinting7,8 provided, from different angles, unprecedented possibilities. However, this increased quality was not yet translating into a tangible impact on patients' lives.
This growing realization meant that TE started entering a new phase, one that sees the reversal of the innovation drivers. The innovation drivers are no longer the developments in individual disciplines but rather the needs of the patient (Fig. 2). To reach the patient, products need to possess a set of quality attributes that ensure product potency while they should be engineered in a robust manufacturing process guaranteeing the quality of the resulting product. For this to happen, innovations are needed in terms of developing robust biological building blocks—tissue structures, precise manufacturing technologies, and high-throughput quality control (QC) tools. Recent developments in these areas, discussed in more detail in the following sections, contribute to an increase in the capacity of the entire field to produce potent and clinically relevant health care solutions.
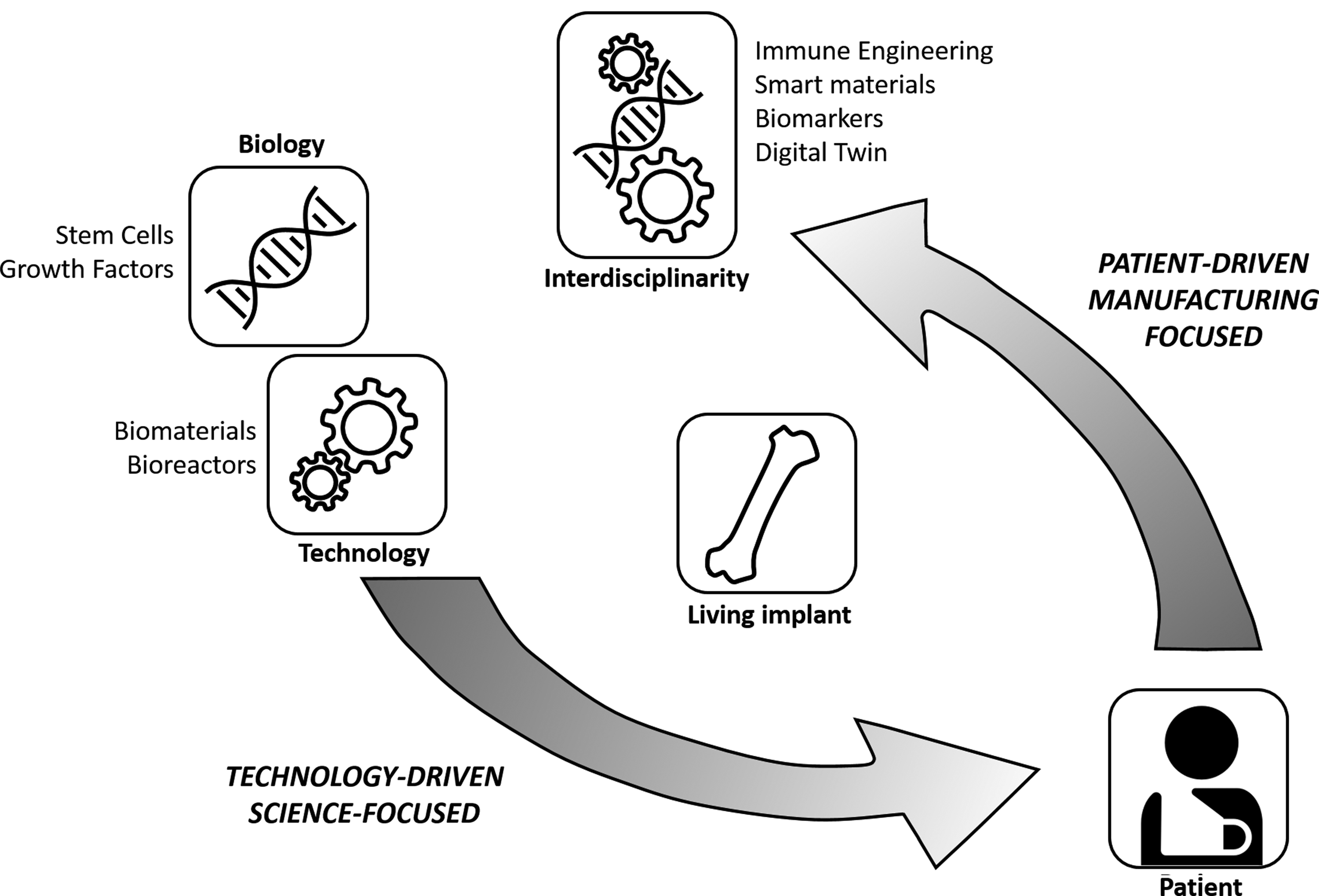
Reversing the innovation drivers. Originally being technology driven and science focused, the TE field is (or should be) increasingly becoming patient driven and manufacturing focused.
Starting from a clear identification of the patients' needs, bearing in mind the manufacturing requirements, means the grand challenge for the third era of TE is to design, develop, and deliver living implants with the accuracy and robustness we expect from inanimate implants, leading to predictable and vastly superior biological and clinical results. To tackle this grand challenge, technological and biological advances are required. In the second part of this perspective we highlight a number of these advances and discuss their role in the global picture of TE.
From Technological and Biological Advances…
Developmental engineering
DE refers to the use of developmental processes as blueprint for the design of TE products. Developmental cascades show a tight regulation and robustness. In mimicking these processes, the aspiration is to overcome the current lack of quantitative metrics able to capture the degree of phenotypic progression that could forecast final TE product potency. Hence, concepts such as “developmental engineering,”3,4 “engineered tissues as organ germs,” 9 and “reverse engineering development” 10 are gaining ground. This allows for a gradual transition from the top-down question of “what is a biomimetic combination of cells-material-growth factor closely mimicking a target tissue” to a bottom-up question of “how can key developmental niches be accurately dissected, designed and precisely biomanufactured at the correct length scales into efficacious TE products.”
Qualitative examples of the DE approach have been successfully provided, for instance in bone TE, where cartilage intermediate templates have been shown to give rise to bone ossicles through endochondral ossification. The DE approach was also applied successfully using both adult11,12 and embryonic13,14 stem cell sources and both scaffold-free and scaffold-based approaches,15,16 demonstrating the robustness of this paradigm. However, to date, it has not yet been demonstrated that TE implants can guide regeneration in vivo, leading to an outcome where contaminating tissue structures are absent (contaminating tissues are tissues unrelated to the regenerative context and not contributing to TE product potency). In addition, engineered TE products possessing a hierarchically complex structure able to perform dual (or more) regenerative tasks upon implantation remain elusive. Scalable production of tissue modules that can guide regenerative events upon implantation is thus an important hallmark for the next generation of TE products.
In-depth characterization technologies—single cell analysis and molecular characterization
“You are as good an engineer as quality controls allow you to be.” One of the most important ongoing activities is the development of the analytics toolbox of the field. At the top of this, single cell genomics revolutionized the way we view cell populations. It provides a window into developmental cascades and tissue composition at the cell scale. The quantification of the kinetics of cell population transition from one cell type to another along developmental cascades will provide an unprecedented compass for the design of TE products. However, TE is more than single cells, and hence technologies that can provide insight into the molecular composition and architecture of extracellular matrices are equally needed.
Quantitative Raman imaging represents a novel label-free method that enables visualization of 3D cell morphology and volumetric quantification of biomolecular structures with submicron-size detail. 17 This provides, among others, an excellent tool for deciphering extracellular matrix (ECM) in terms of its molecular properties. For example, for native and engineered cartilage tissue Quantitative Raman imaging allowed a quantitative analysis of the distribution and organization of ECM constituents. 18 In addition, advances in nano-CT imaging allow for the 3D representation of the structural organization of complex tissues. For example, recently mineralized bone, bone marrow vasculature, and adipose tissue can be detected simultaneously in 3D, providing insight into the design principles that complex bone TE constructs should possess to capture interactions between these three tissues. 19
Contrast enhanced nano-CT has furthermore produced insights at the nanoscale, providing architectural information on tissue complexity. 20 Taken together, the TE field possesses a toolbox that captures ever more accurately the native tissue composition, structure, complexity, and organization. These technologies allow deciphering in situ regenerative events and developmental cascades, providing a high-resolution picture of the properties that TE products should possess to exhibit regenerative properties. These technologies could therefore lead to precise characterization of the mechanisms of action of future TE products and their corresponding critical quality profile, essential for manufacturing processes described in the following section.
High-precision, scalable biomanufacturing
Biofabrication technologies able to operate with ever-increasing resolution and precision provide an unprecedented opportunity for building tissues of increased complexity with a single molecule, cell, niche resolution comparable with that encountered in native tissues.21,22 Examples of this enhancement in biomanufacturing capacity are the development of melt electrowriting, 23 stereolithography, 24 and laser-assisted technologies, 25 all operating <100 μm resolution. In addition, robotic devices have been shown to possess the capacity to manipulate tissue modules such as single spheroids and positioning them in preordered grids allowing them to fuse 26 or deposit them in printed scaffolds. 27
The ability to reproduce accurately computer aided design (CAD)-based designs allows the incorporation of automation principles during production, although to date there are limited online QC methodologies that could validate the comparability between “as-designed” and “as-produced” products. In addition, technical bottlenecks such as the production of vascularized, multicentimeter-sized implants will require the combined use of the aforementioned technologies now that successful proof of concept has been generated for endochondral bone repair.28,29 The potential to build larger tissue structures based on robust modules, that is, following a robust biological paradigm, produced through robust manufacturing processes and possessing a defined set of quality attributes, allows the implementation of Quality by Design in TE manufacturing 30 using the quality characterization methodologies described earlier.
In silico toolbox—digital twins of intracellular gene regulation to bioreactor biology
As described above, the TE field is evolving into adopting solid biological paradigms that provide robust biological building blocks, high-precision biofabrication technologies that can use these building blocks to construct TE products, and unprecedented quality characterization technologies that allow us to assess the quality during and after production. Another enabling technology that could play an important role in establishing the systematic pipeline of TE products to the clinics is in silico modeling. In silico is a term that was coined in analogy to the terms in vitro and in vivo; it is derived from the word silicium being the main component of computer chips, and refers to computer modeling and simulation.
In line with the Industry 4.0 concept, being the current trend of automation and data exchange in manufacturing technologies, digital twins can be created of every step of the TE production process. 31 Digital twins are digital replicas (computer models) of physical entities (e.g., process steps) that exchange information with their physical counterpart through sensors or historic data, and that can be used to unable understanding and optimization of the physical process they represent. Intracellular gene regulatory models32,33 are capable of reducing the in vitro large-scale screening to optimize culture medium composition. A digital twin of the bioprinting process 34 or the subsequent maturation process in the bioreactor35,36 allows for an optimization of these processes with a minimum of trial and error.
Verification, validation, and uncertainty quantification are key principles in building credibility for these models. 37 These digital twins can be connected in silico to form a digital TE pipeline, and identify the crucial process steps and QC checks that guarantee high-quality and predictable products. This provides a unique context for the production of in silico-designed TE products where the appropriate quality attributes necessary for their functionality could be inbuilt. This way, in silico models guide the way from robust biological building blocks to a high-quality production process.
… To Innovation in Regulation and Business
The biological and technological advances discussed in the previous section are by no means an exhaustive summary. Think, for example, about advances in the incorporation of immune engineering requirements into TE products and renewable cell sources such as iPS cells, which have not been included in this perspective but are discussed elsewhere.5,38 What is striking in the discussed examples is the joined involvement of both engineering and biological disciplines. Addressing the TE grand challenge requires true integration of all disciplines involved, transcending the individual disciplines, and establishing TE as a transdisciplinary scientific domain. Simultaneously, it has become quite clear that the innovation is not only needed on the R&D side. TE solutions are inherently more complex and personalized than most pharmaceuticals, and hence require tailor-made regulatory assessment, clinical trial design, and business approaches.
On the regulatory side, it is important to involve regulatory bodies early on in the design and development of TE products. 2 To pass regulatory scrutiny, these TE products should be well-characterized, robust, with consistent efficacy and an acceptable and controlled positive benefit/risk ratio. As argued in the previous section, enabling technologies can play a key role in meeting those demands.
With respect to the design of clinical trials for TE products, the one-size-fits-all, large randomized clinical trials are no longer in line with the current scientific, clinical, and economic reality. Clinical trial failures, especially in phase III, have huge safety and commercial/financial consequences. 2 An evolution has started toward more innovative, efficient, and adaptive trial designs, 39 built around active participation of patients and patient organizations. Adaptive clinical trials, irrespective of the trial phase, use the results accumulated in the trial to modify the trial's course in accordance with prespecified rules. 40 It is furthermore important to derisk the execution of clinical trials, especially in Phase III, by carefully analyzing the risks of the trial execution and by a continuous surveillance of the quality of data being collected. 2
On the business end of the spectrum, innovation is required to cope with the challenging combination of complexity and limited production volumes. 41 Principles such as design to cost 42 will become essential for the manufacturing of high-tech medical products such as TE implants. Design to cost is a management strategy designed to achieve an affordable product by targeting the manufacturing cost as an independent design parameter that must be met during product development. This strategy guarantees that at the end of the R&D process, the developed product can be manufactured at a cost that is not prohibitive to its clinical uptake and penetration in the market. The rigorous quality assessment, scalable manufacturing technologies, and in silico models described in the previous section are elements that are crucial for reaching the design-to-cost objectives.
Conclusion
Starting from a clear identification of the patients' needs and the manufacturing requirements of the corresponding TE solutions, the need for specific biological and technological advances can be identified. The capacity to design and build tissues with predictive performance thanks to these technological and biological advances will result in a high-quality and robust TE production process and resulting product. This will facilitate approval from regulatory bodies while attracting investments by lowering risks associated with market-stage product failure, and hence will contribute to a novel viable medical sector able to revolutionize health care.
Footnotes
Acknowledgments
The authors gratefully acknowledge support from the Research Foundation Flanders (FWO Vlaanderen; I.P: 12O7916N), the Belgian fund for national research (FNRS; T.0256.16), the Regenerative Medicine Crossing Borders initiative (www.regmedxb.com) powered by EWI-Vlaanderen, and the European Research Council under the European Union's Horizon 2020 framework program ERC/CoG 772418 (L.G.). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article. This work is part of Prometheus, the KU Leuven R&D division for skeletal tissue engineering (![]() ).
).
Disclosure Statement
No competing financial interests exist.