
Abstract
Bone morphogenetic protein 2 (BMP-2) is widely used in spinal fusion but it can cause adverse effects such as ectopic bone and adipose tissue in vivo. Neural epidermal growth factor like-like molecule-1 (NELL-1) has been shown to suppress BMP-2-induced adverse effects. However, no optimum carriers that control both NELL-1 and BMP-2 releases to elicit long-term bioactivity have been developed. In this study, we employed polyelectrolyte complex (PEC) as a control release carrier for NELL-1 and BMP-2. An ultra-low dose of BMP-2 synergistically functioned with NELL-1 on bone marrow mesenchymal stem cells osteogenic differentiation with greater mineralization in vitro. The osteoinductive ability of NELL-1 and an ultra-low dose of BMP-2 in PEC was investigated in rat posterolateral spinal fusion. Our results showed increased fusion rate, bone architecture, and improved bone stiffness at 8 weeks after surgery in the combination groups compared with NELL-1 or BMP-2 alone. Moreover, the formation of ectopic bone and adipose tissue was negligible in all the PEC groups. In summary, dual delivery of NELL-1 and an ultra-low dose of BMP-2 in the PEC control release carrier has greater fusion efficiency compared with BMP-2 alone and could potentially be a better alternative to the currently used BMP-2 treatments for spinal fusion.
Impact Statement
In this study, polyelectrolyte complex was used to absorb neural epidermal growth factor like-like molecule-1 (NELL-1) and bone morphogenetic protein 2 (BMP-2) to achieve controlled dual release. The addition of NELL-1 significantly reduced the effective dose of BMP-2 to 2.5% of its conventional dose in absorbable collagen sponge, to produce solid spinal fusion without significant adverse effects. This study was the first to identify the efficacy of combination NELL-1 and BMP-2 in a control release carrier in spinal fusion, which could be potentially used clinically to increase fusion rate and avoid the adverse effects commonly associated with conventional BMP-2.
Introduction
Spinal fusion is a surgical procedure that unites two or more vertebrae to achieve segmental stability and relieve pain, which involves the physiological process of bone regeneration. It is performed to treat spine fracture, isthmic spondylolisthesis, stenosis, herniation, tumor, and other degenerative diseases. 1 In the United States, the annual volume of elective spinal fusion increased by 62.3%, and health care burden associated with spinal fusion surgery increased by 152% from 2004 to 2015. 2 To date, autologous bone graft has been regarded as the “gold standard” for spinal fusion. However, the autologous bone harvest is associated with donor site morbidity, increased surgical time, and hospital stay. Further, the usage is limited by the quality of the donor's bone, as well as the available volume that can be harvested.
Alternatively, various growth factor therapies have shown great osteogenesis potentials. Bone morphogenetic protein-2 (BMP-2) is one of the most potent osteoinductive growth factors in promoting bone regeneration. Infuse™ Bone Graft, a product (Medtronic, Minneapolis, MN) sold as an autograft substitute consisting of recombinant human BMP-2 (rhBMP-2), absorbable collagen sponge (ACS), and a fusion cage device, was approved by the FDA for anterior lumbar interbody fusion at a single level in 2002 and oblique lateral interbody fusion in 2015. 3
BMP-2 has been proven to be effective to promote fusion, decrease pain, and improve patient satisfaction in the FDA-recommended applications.4–6 In 2006, BMP-2 was introduced in 25% of all spinal fusions. 7 As off-label use of BMP-2 becomes the predominant treatment, adverse events, including inflammation complications, 8 ectopic bone formation,9–11 dysphagia, 12 radiculopathy, 13 osteolysis, bone cyst formation, 14 retrograde ejaculation, seroma, 15 and hematoma, 11 have been reported, raising safety concerns.
The side effects are dose related. 16 Supraphysiological concentration of BMP-2 was believed to trigger unwanted adverse events. 17 One of the solutions to address the side effects problem is to reduce the dose of BMP-2 with control release carriers. We developed a heparin-incorporated polyelectrolyte complex (PEC) as a control release carrier of BMP-2.18–21 The required dose of BMP-2 for spinal fusion was significantly reduced, with side effects suppressed when delivered in PEC.
Attempts have also been made to identify alternative growth factors to BMP-2 for bone regeneration. Recently, a novel osteoinductive growth factor, neural epidermal growth factor like-like molecule-1 (NELL-1) has attracted researchers' attention. NELL-1 was first identified to be overexpressed in human craniosynostosis, a cognitive disease due to cranial sutures overgrowth. 22 A similar phenotype was observed in transgenic mice overexpressing NELL-1, 23 whereas NELL-1-deficient mice exhibited reduced thickness and density in calvarial bone. 24 These results suggest that NELL-1 is of significance during bone development and potentially elicits osteoinductive effect for bone regeneration applications.
NELL-1 has been shown to facilitate bone regeneration. Lyophilized NELL-1 on demineralized bone matrix (DBM) resulted in comparable fusion to BMP-2 with ACS in a rat spinal fusion model. 25 Moreover, NELL-1 did not cause the formation of ectopic bone and cyst-like bone voids as observed with BMP-2. Apart from DBM, human cancellous bone chips were also used as a scaffold for NELL-1 application. 26
Some studies showed that NELL-1 delivered by a non-DBM carrier, hydroxyapatite-coated poly (lactic-co-glycolic acid) (PLGA), resulted in rather limited bone regeneration and failure in critical defect fusion.27,28 However, NELL-1 with collagen/PLGA scaffold was reported to stimulate calvarial defect healing, showing nearly 90% bone density of uninjured bone and equivalent mineralization as compared with BMP-2. 29 Whether the efficacy of NELL-1 is independent on DBM or its counterpart remains controversial.
A few studies have combined NELL-1 with BMP-2 for bone regeneration. Adenovirus-mediated delivery of NELL-1 and BMP-2 significantly enhanced osteoblastic differentiation of myoblasts, as detected by elevated expression of alkaline phosphatase (ALP) and osteopontin. 30 In vivo implantation to nude mice showed that a larger bone mass was induced by dual delivery of NELL-1 and BMP-2 than the delivery of either NELL-1 or BMP-2. 30 Greater bone formation of NELL-1 + BMP-2 was also reported in femoral defect, 28 rapid distraction, 31 and calvarial defect. 32
However, NELL-1 and BMP delivered in either phosphate saturated buffer, collagen or hydroxyapatite, suffered from burst release and short half-life.33,34 A lack of control release carrier compromises the efficiency of NELL-1 and BMP-2 combination and, consequently, requires high doses of growth factors to elicit their osteoinductive activity.
An optimal carrier that controls the growth factor releases to elicit long-term bioactivity would improve the osteoinductive efficiency of NELL-1 and BMP-2 combination. Heparin PEC has been used to reduce the dose of BMP-2 to a low level (5% of its conventional dose in ACS) in rat posterolateral spinal fusion. 19 In this study, we hypothesize that PEC will control the release of both NELL-1 and BMP-2 and improve their osteoinductive efficiency for spinal fusion. The objectives are to validate an optimal control release carrier for the dual delivery and to further reduce the dose of BMP-2 with the addition of NELL-1 for solid spinal fusion.
Materials and Methods
Cell culture
Porcine bone marrow mesenchymal stem cells (BMSCs) were isolated from the iliac crest of pigs. Bone marrow aspirate was cultured in growth medium consisting of α-MEM (Gibco, Waltham, MA), 10% mesenchymal stem cell-qualified fetal bovine serum (FBS; Thermofisher, Waltham, MA), and 1% penicillin-streptomycin (P/S; Thermofisher) at a 37°C. After 7 days, nonadherent cells were washed away. Adherent cells were expanded until they reached 90% confluence. Cells of passage 1–3 were used in all the experiments.
Osteogenic differentiation in vitro
Osteogenic differentiation was induced in osteogenic differentiation medium (ODM) consisting of α-MEM, 10% FBS, 1% P/S, 50 μM
Alizarin red S staining quantification
On day 14, cells were fixed with 10% formalin for 15 min, and they were stained with 40 mM alizarin red S (Sigma-Aldrich). Dye solution was removed after 20 min, and cells were washed twice with distilled water. Images were taken by a TissueFAXS slide scanner (TissueGnostics GmbH, Australia). One hundred microliters of 10% acetic acid was added to each well to extract the dye. Cells were scraped to a centrifuge tube and heated at 85°C for 5 min. The slurry was centrifuged at 20,000 g for 15 min, and the supernatant was collected. The supernatant was then neutralized with 10% ammonium hydroxide. The samples and alizarin red S standards were transferred to a 96-well plate, and the absorbance at 405 nm was measured by a plate reader. The result was expressed as the fold change of alizarin red S relative to the ODM group. All experiments were done in triplicate.
ALP bioactivity
ALP bioactivity of BMSC treated with NELL-1 and/or BMP-2 was performed on day 6. Cells were washed with phosphate buffered solution (PBS) twice and then lysed with the lysis buffer provided by an ALP assay kit (SensoLyte Alkaline Phosphatase Assay Kit; Anaspec, Fremont, CA). The cell lysate was centrifuged at 2500 g for 10 min at 4°C. The supernatant was collected and mixed with an equal volume of p-nitrophenyl phosphate substrate. The absorbance at 405 nm was measured by a plate reader (Infinite M200; Tecan, Switzerland). ALP was calculated according to a standard curve. The amount of total protein in the supernatant was measured by using a microBCA kit (Thermofisher). ALP bioactivity normalized to total protein was expressed as the fold change relative to the ODM group. All experiments were done in triplicate.
Quantitative polymerase chain reaction
The expression of osteoblastic markers, including runt-related transcription factor 2 (RUNX2), ALP, osteopontin (OPN), osteocalcin (OCN) and collagen type I alpha 1 chain (COL1A1), was examined on day 6 by quantitative polymerase chain reaction (PCR). The primer sequences are listed in Table 1. Specificity of the primes was confirmed by melting curve analysis. Total RNA from BMSC was extracted according to the manufacturer's protocol (Qiagen). The concentration and purity of RNA were measured by using Nanodrop (Thermofisher). cDNA was synthesized from 500 ng RNA by using iScript cDNA Synthesis Kit (Bio-Rad).
Primer Sequences
ALP, alkaline phosphatase; COL1A1, collagen type I alpha 1 chain; GAPDH, glyceraldehyde 3-phosphate dehydrogenase; OCN, osteocalcin; OPN, osteopontin; RUNX2, runt-related transcription factor 2.
Quantitative PCR reactions were performed by using the condition: 95°C 10 min, 40 cycles of 95°C × 15 s, 60°C × 30 s, and 72°C × 30 s in Step-one Real-time System (Applied Biosystems). Relative expression of osteoblastic markers was calculated by using the 2−ΔΔCt method where day 0 BMSC and glyceraldehyde 3-phosphate dehydrogenase (GAPDH) served as reference sample and reference gene, respectively. All experiments were done in quadruplicate.
PEC preparation
Gamma-irradiated sodium alginate (NovaMatrix, Sandvika, Norway) was dissolved in distilled water to obtain 4% solution. The solution was dripped into 0.2 M SrCl2. Microbeads were generated by an electrostatic bead encapsulator (Nisco Engineering AG, Switzerland). For polyelectrolyte surface modification, microbeads were incubated in 0.2% (w/v) protamine (Sigma-Aldrich) solution for 15 min (protamine PEC) followed by twice washing of distilled water. Subsequently, protamine PEC was impregnated in 0.05% (w/v) heparin (Sigma-Aldrich) solution for 15 min (hereafter referred to as heparin PEC) followed by twice washing of distilled water.
To examine whether growth factors can bind to the surface of PEC, fluorescence-labeled growth factors were incubated with PEC beads for 1 h and observed with an Olympus FV1000 TIRF confocal microscope (Japan). Fibrinogen (Sigma-Aldrich) was ligated with fluorescein isothiocyanate (FITC). BMP-2 was dialyzed against distilled water and lyophilized to remove the stabilizers present in the commercial BMP-2 solution that may interfere with the fluorescence labeling reaction. Lyophilized BMP-2 was reconstituted in PBS and conjugated with HiLyte Fluor™ 555 according to the manufacturer's protocol (Anaspec).
Growth factor release in vitro
Five micrograms of BMP-2 or fibrinogen was loaded to heparin PEC or protamine PEC. After 1 h of incubation, 1 mL of PBS was added. The supernatant was immediately collected to measure the amount of unbound growth factors. One milliliter of fresh PBS was replenished and collected at predetermined time points at 4°C in darkness under constant shaking. The amount of BMP-2 was measured by an enzyme-linked immunosorbent assay according to the manufacturer's protocol (Invitrogen, Carlsbad, CA). The amount of fibrinogen was measured by a fluorometric method. Uptake percentage and cumulative release are calculated as the formulas in Table 2.
Formulas of Uptake Percentage and Cumulative Release
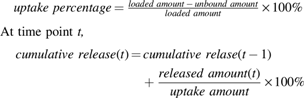
Where cumulative release (t-1) refers to cumulative release at the previous time point, release amount(t) refers to the amount in the collected sample at time point t; uptake amount refers to loaded amount − unbound amount.
Implants preparation
PEC beads coated with different doses of NELL-1 and/or BMP-2 were prepared 1 day before rat surgery. Coated beads were then stuffed into mPCL-TCP scaffolds (Osteopore, Singapore) and placed on ice until implantation. A 20 μL of solution containing 10 μg BMP-2 was dipped onto ACS (Medtronic), serving as a positive control.
Rat posterolateral spinal fusion surgery
All animal-related procedures were approved by our Institutional Animal Care and Use Committee (IACUC, protocol: R14-0038, R18-0281). The Sprague-Dawley rats (InVivos, Singapore) weighed between 500 and 650 g. Twenty-eight rats underwent L4–L5 posterolateral spinal fusion. Implantation was divided into six groups. Group I: PEC blank (PEC: BLK, n = 4); Group II: PEC +20 μg NELL-1 (PEC: N(H), n = 4); Group III: PEC +0.25 μg BMP-2 (PEC: B, n = 6); Group IV: PEC +3.5 μg NELL-1 + 0.25 μg BMP-2 (PEC: N(L)+B, n = 3); Group V: PEC +20 μg NELL-1 + 0.25 μg BMP-2 (PEC: N(H)+B, n = 7); and Group VI: ACS +10 μg BMP-2 (ACS: B, n = 4).
Rats were anesthetized with isoflurane (5% for induction, 2% for maintenance). A posterior middle skin incision was made. Two separate paramedian incisions were made followed by subperiosteal dissection of muscles from the transverse processes of L4 and L5 vertebrae. The transverse processes were decorticated with a scalpel meticulously. The implants were placed above the decorticated transverse processes and secured by 4-0 Tricon sutures (Medtronic). The muscle and skin incision were closed with 3-0 biodegradable sutures. Buprenorphine and enrofloxacin were given for 3 days postoperation. All the rats were fed ad libitum and allowed to move inside the cage without restriction. Rats were euthanized by CO2 inhalation at 8 weeks postoperation. The spines were harvested and stored at −80°C for further analysis.
Manual palpation
Fusion of the harvested spines was evaluated by two blinded observers as previously described. 35 If there were no motion present in all six directions (flexion, extension, left and right lateral bending, and axial rotation), the segment would be graded as fused. Otherwise, it would be graded as not fused.
Micro-computed tomography analysis
Live micro-computed tomography (μ-CT) was performed at 4 weeks postoperation at a resolution of 118 μm voxel (Quantum Fx μ-CT system; PerkinElmer). Harvested spines at 8 weeks postoperation were scanned at a resolution of 59 μm voxel by using the same μ-CT system. Isotropic slice data obtained from this system were used for image reconstruction by using VG Studio Max 1.2 (Volume Graphics GmBH, Germany).
The total volume of interest was defined as all the space inside the scaffold. An optimized density threshold was applied to all images to isolate mineralized bone for bone histomorphometric parameters calculation. The following three-dimensional microstructural parameters of bone tissue were calculated by CTAn (SKYSCAN, Kontich, Belgium), including bone volume fraction (bone volume/total volume [BV/TV], %), bone surface to total volume (bone surface/total volume [BS/TV], 1/mm), trabecular thickness (Tb. Th, μm), trabecular number (Tb. N, 1/mm), trabecular separation (Tb. Sp, μm), 36 and ectopic bone outside the scaffold (mm3). Fusion score was based on μ-CT images on a 2-point scale: 0, no fusion; 1, unilateral along the transverse process; fusion; 2, bilateral fusion along the transverse processes.
Histology
Frozen spines were thawed at room temperature, and then fixed in 10% buffered formalin for 2 weeks. Tissue was decalcified in 30% formic acid, dehydrated, and embedded in paraffin. A series of 7-μm thickness sections were made by a microtome (HistoCore BIOCUT, Leica, Germany). The sections were stained with hematoxylin and eosin, and Masson-Goldner trichrome (Merck Millipore). Stained sections were scanned by Nikon Eclipse Ci attached with a DS-Fi2 camera. Microscopic images were taken by using an optical microscope (Olympus IX71, Japan).
Biomechanical test
The stiffness of bone was determined by measuring displacement distance in a cantilever system using an Instron 5543 according to methods previously described with slight modification. 37 After thawing the frozen rat spines to room temperature, the remaining muscular tissue was removed, leaving the surrounding ligaments intact. The vertebral bodies were drilled with small screws. The specimens were checked under x-ray to prevent the screw from entering the disk. The exposed ends of screws were embedded firmly in the dental cement, polymethylmethacrylate (PMMA).
The moment was fixed at 20 Nmm, and the moment arm was fixed at 22 mm. A force of 0.91 N was applied to the cement attached to the L4 vertebral body. The samples were tested in flexion, extension, and lateral bending at a constant loading rate of 0.05 mm/s. Between two loadings, a relaxation time of 30 s was adopted. Three consecutive cycles were tested, and only the last one was used for calculation of stiffness. Normal intact spine from L4 to L5 without fusion was tested as a negative control. Stiffness was expressed as Nmm/degree.
Methods of analysis
Data were presented as mean ± standard deviation. Two-samples t-test was used when two groups were compared. One-way analysis of variance followed by Tukey post hoc was used when more than two groups were compared. p < 0.05 was considered statistically significant. The statistics were performed by using GraphPad prism software (v 8.0; GraphPad Software, Inc.).
Results
NELL-1 and ultra-low doses of BMP-2 synergistically enhance BMSC osteogenic differentiation
The osteoinductive effects of NELL-1 and ultra-low doses of BMP-2 applied alone or in combination were examined by alizarin red staining of the differentiated cells. The positive effect of NELL-1 alone (10 μg/mL, alizarin red S relative to ODM increased by 8.9-fold) on BMSC mineralization was confirmed by alizarin red staining (Fig. 1A). Ultra-low doses of BMP-2 (5 and 10 ng/mL) increased calcium deposits by approximate five-fold (Fig. 1B). A combination of NELL-1 and ultra-low doses of BMP-2 showed significantly enhanced mineralization compared with the ODM group or either NELL-1 or BMP-2 alone.

BMSC osteogenic differentiation with NELL-1 and/or BMP-2. NELL-1 (5 and 10 μg/mL) and/or BMP-2 (5 and 10 ng/mL) were supplemented to ODM.
When 5 μg/mL of NELL-1 was combined with BMP-2, it induced the most calcium deposits (10.91-fold with 5 ng/mL BMP-2, and 12.11-fold with 10 ng/mL BMP-2, respectively). Calcium formation induced by NELL-1 reached a plateau at 10 μg/mL and it did not further increase with addition of BMP-2. Thus, the result suggests a synergistic effect between 5 μg/mL NELL-1 and 5–10 ng/mL of BMP-2 on BMSC mineralization.
We chose the combination of 5 μg/mL NELL-1 and 10 ng/mL BMP-2 that resulted in the highest calcium deposits for the following ALP bioactivity and gene expression assay. BMP-2 alone increased ALP by 2.0-fold compared with ODM, whereas NELL-1 at the concentration of 5 μg/mL barely affected ALP (Fig. 1C). Similar to the alizarin red S staining result, the combination of NELL-1 and BMP-2 (B+N) induced significantly higher ALP bioactivity than either NELL-1 or BMP-2 alone.
The expression of osteoblastic markers on day 6 was examined by quantitative PCR. The combination of NELL-1 and BMP-2 (B+N) significantly increased expression of ALP and OPN, the intermediate marker, relative to BMP-2 or NELL-1 alone (Supplementary Fig. S1). However, the synergistic effect was not observed in the expression of the early marker (RUNX2) and the late markers (OCN and COL1A1), although both BMP-2 alone and BMP-2 + NELL-1 increased their expression compared with ODM. Day 6 might not be the optimal time point to detect expression changes of the early and late makers.
PEC absorbs fibrinogen and BMP-2 and releases them in a controlled manner
Although NELL-1 comprises a heparin binding domain, 38 the affinity to heparin is considered moderate as the dissociation constant value was estimated to be 409 nM whereas that of BMP-2 was measured as around 45 nM. 39 Protamine PEC with a layer of positively charged protamine was used to electrostatically bind to the negatively charged NELL-1. Fibrinogen was used as an NELL-1 mimetic as it possesses similar charge and molecular weight as NELL-1 (isoelectric point of NELL-1 and fibrinogen = 5.66 and 5.5, the molecular weight of NELL-1 and fibrinogen is around 400 and 340 kDa).40,41 Confocal microscopy with FITC-labeled fibrinogen confirmed uniform uptake and distribution of fibrinogen on the circumference of beads (Fig. 2A). Protamine PEC absorbed 94.24% ± 2.06% of fibrinogen (Fig. 2C).
Uptake and release profile of growth factors on PEC beads.
Heparin PEC has been shown to control BMP-2 release. 18 Confocal microscopy with Hilyte555-labeled BMP-2 (Fig. 2B) confirmed a similar uniform uptake of BMP-2 on the circumference of beads. Heparin PEC absorbed 89.90% ± 1.72% of BMP-2 (Fig. 2C).
Both carriers showed an initial burst release of the bound proteins within the first 24 h followed by a similar control release pattern (Fig. 2D). Cumulative release of fibrinogen and BMP-2 over 336 h was 26.05% ± 5.74% and 18.76% ± 6.48%, respectively.
NELL-1 enhances an ultra-low dose of BMP-2-induced spinal fusion
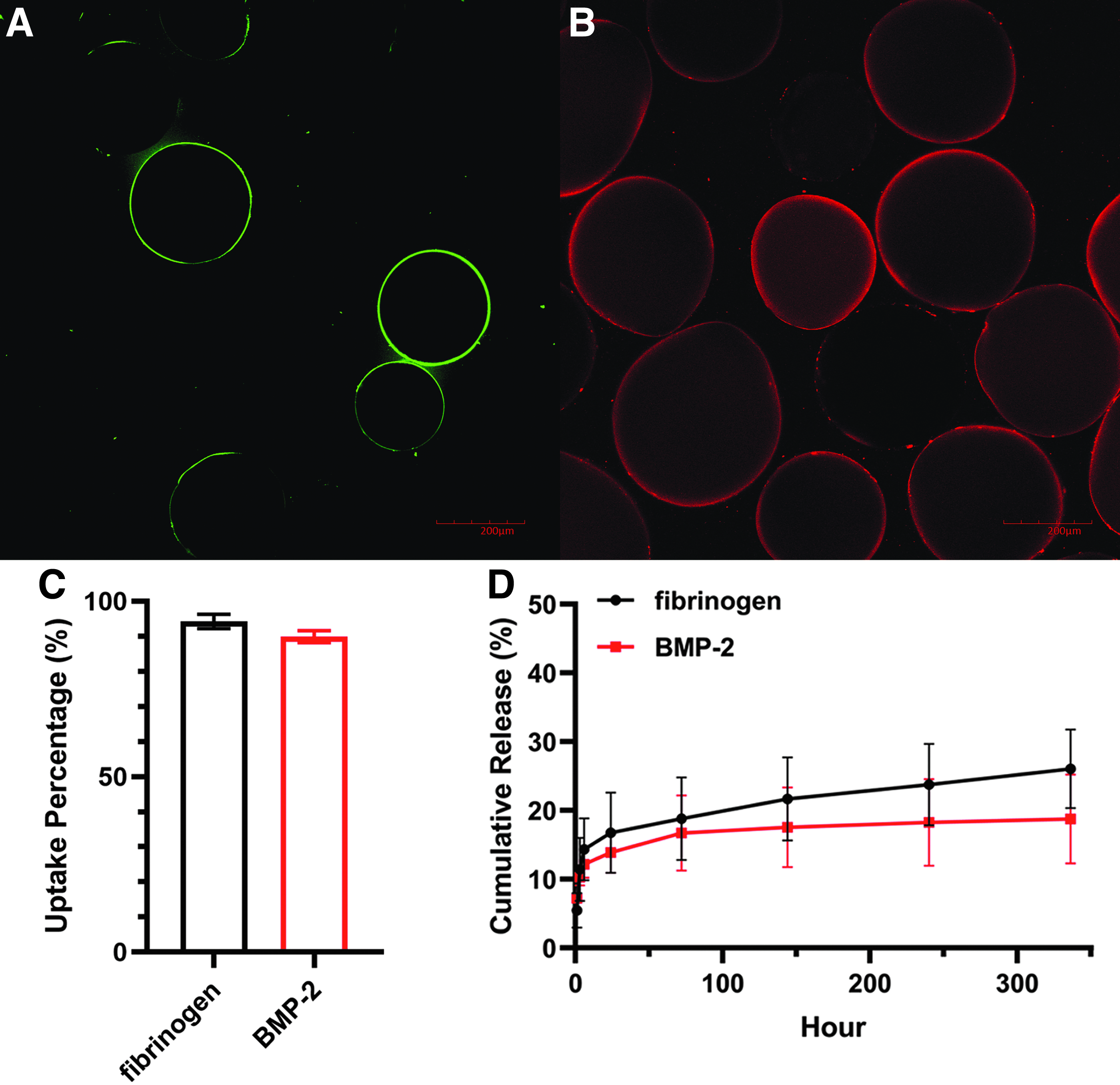
Bone formation at the L4-L5 posterolateral side was evaluated by μ-CT at 4 weeks and 8 weeks postoperation. Three-dimensional reconstructs revealed the extent of bone formation between L4 and L5 transverse processes (Fig. 3). Fusion rate was assessed by manual palpation at week 8 after tissue harvest (Table 3).
Reconstructed micro-computed tomography images of bone formation in the rat posterolateral spinal fusion model. PEC: BLK (blank beads, no growth factor), PEC: N(H) (20 μg NELL-1), PEC: B (0.25 μg BMP-2), PEC: N(L)+B (3.5 μg NELL-1 + 0.25 μg BMP-2), PEC: N(H)+B (20 μg NELL-1 + 0.25 μg BMP-2), ACS: B (10 μg BMP-2). Clear gaps between transverse processes are indicated by white arrows. Successful bony bridges are indicated by closed triangles. More ectopic bone (dotted arrows) is found in ACS: B compared with the other groups. ACS, absorbable collagen sponge.
Fusion Score and Fusion Rate
Fusion score was determined by micro-computed tomography based on a 2-point scale: 0, no fusion; 1, unilateral fusion along the transverse processes; and 2, bilateral fusion along the transverse processes. Fusion rate was determined by manual palpation.
ACS, absorbable collagen sponge; BLK, blank; BMP-2, bone morphogenetic protein 2; NELL-1, neural epidermal growth factor like-like molecule-1; PEC, polyelectrolyte complex.
Pseudarthrosis and unilateral fusion was observed from the coronal and sagittal view in some animals with PEC delivery of the ultra-low BMP-2 alone (Group III, PEC: B) group, achieving a fusion score of 0.67 and 1.33 at 4 and 8 weeks, respectively; and a fusion rate of 66.7% at 8 weeks. Both NELL-1 alone (Group II, PEC: N(H)) and blank control (Group I, PEC: BLK) induced minimal bone formation, as evident from the gaps (white arrows) between the adjacent transverse processes and the lower fusion score compared with PEC: B (Table 3). Combined delivery of NELL-1 and BMP-2, either low NELL-1 (Group IV, PEC: N(L)+B) or high NELL-1 (Group V, PEC: N(H)+B), resulted in complete bony bridges (closed triangles) or successful bilateral fusion with a fusion rate of 100% and 85.7% at 8 weeks. All the six implants of PEC: N(L)+B in three animals achieved successful fusion (Supplementary Fig. S2).
Bilateral fusion was achieved in Group VI, in which 10 μg of BMP-2 was delivered by ACS (ACS: B) at as early as 4 weeks, achieving a perfect fusion score and 100% fusion rate at 8 weeks (Table 3). However, a large amount of ectopic bone formation (dotted arrows) was detected in the ACS: B samples, in which a shell of bone was formed outside the scaffold; whereas the inner region of the scaffold remained void. The phenomena of a large amount of heterotopic bone and inner radiolucency from BMP-2 are consistent with other animal studies.16,25
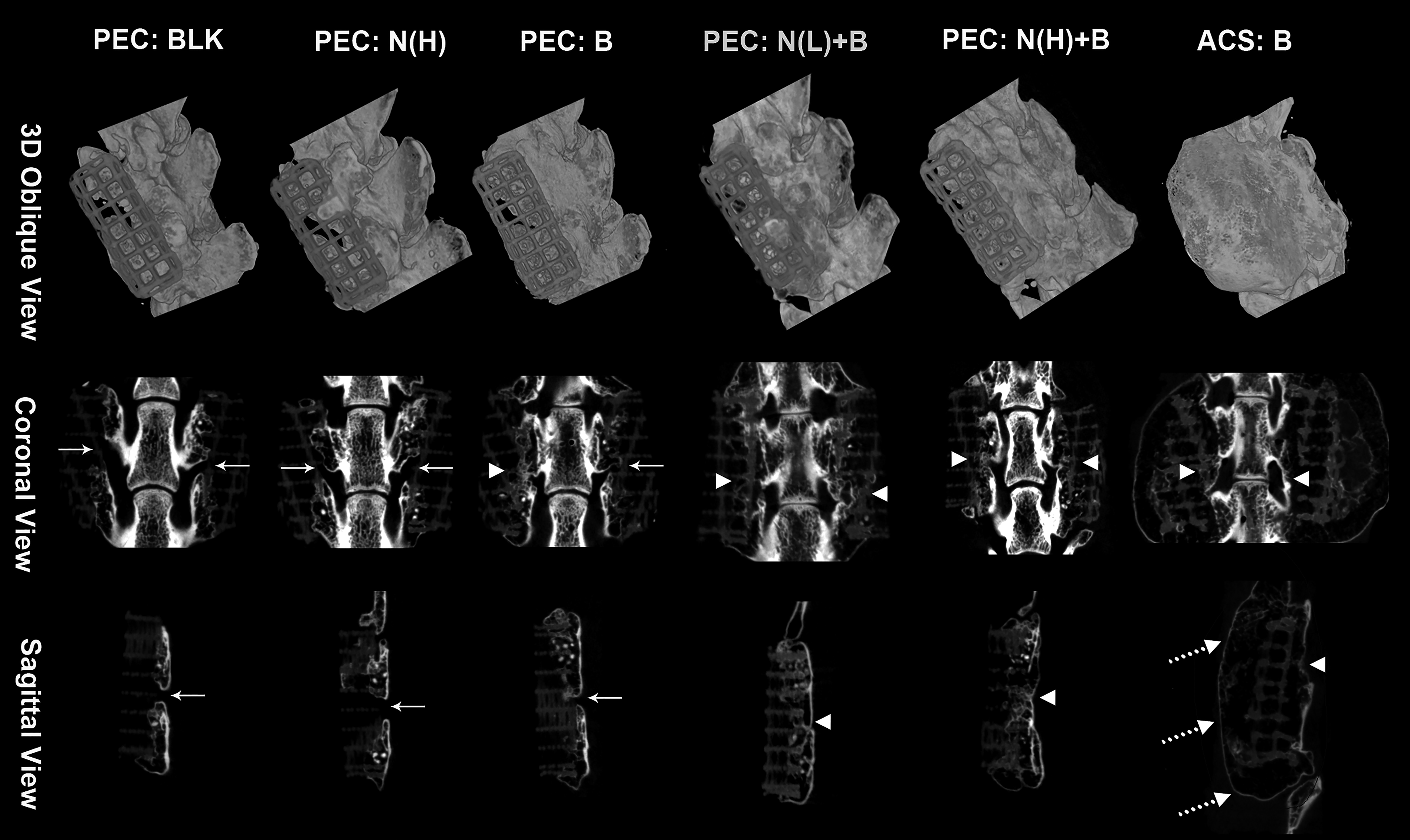
To quantify μ-CT results, bone histomorphometry parameters were analyzed (Fig. 4). PEC: N(L)+B and PEC: N(H)+B showed a similarly superior bone architecture, including higher bone volume fraction (BV/TV), Tb. Th, bone surface density (BS/TV), and Tb. N, and lower specific bone surface (BS/BV) and Tb. Sp. ACS: B induced a significant amount of ectopic bone (23.09 ± 12.77 mm3) than the other groups (<4 mm3), whereas no significant ectopic bone formation was detected in other tested groups compared with the PEC: BLK (Fig. 5).
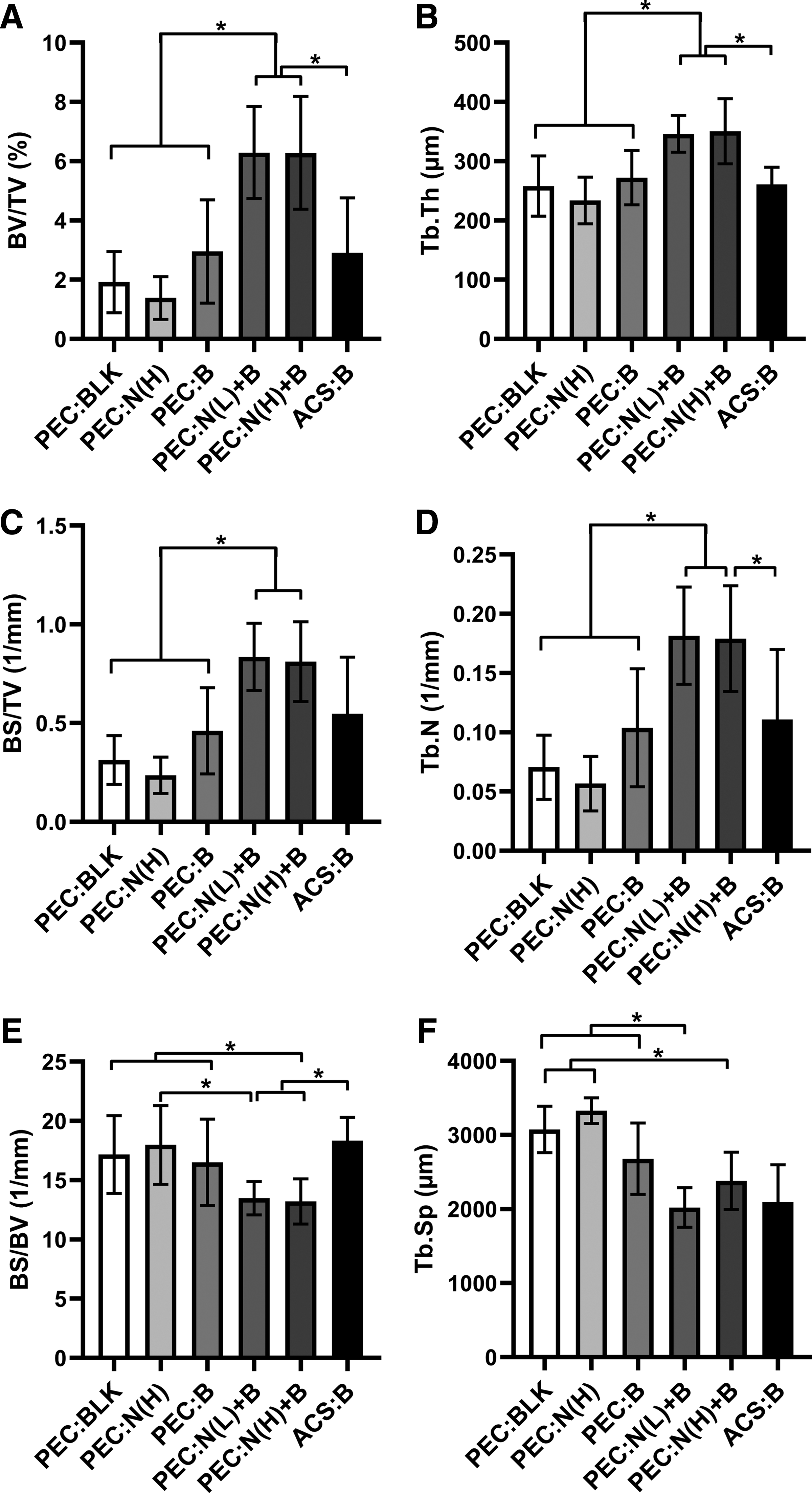
Bone histomorphometry parameters of the fusion mass inside the scaffolds, presented as

Analysis of ectopic bone volume of newly formed bone outside the scaffold. Results were presented as mean ± standard deviation (for PEC: N(L)+B, n = 6; for PEC: BLK, PEC: N(H), and ACS: B, n = 8; for PEC: B, n = 12; for PEC: N(H)+B, n = 14). Statistical analysis was performed by using one-way ANOVA followed by Tukey post hoc test. *p < 0.05. PEC: BLK (blank beads, no growth factor), PEC: N(H) (20 μg NELL-1), PEC: B (0.25 μg BMP-2), PEC: N(L)+B (3.5 μg NELL-1 + 0.25 μg BMP-2), PEC: N(H)+B (20 μg NELL-1 + 0.25 μg BMP-2), ACS: B (10 μg BMP-2).
Histological evaluation confirmed the μ-CT findings. The mPCL-TCP scaffolds were dissolved during tissue processing, as indicated by the void spaces on the histological images. A continuous bony bridge was present between two transverse processes in PEC: N(L)+B and PEC: N(H)+B, as shown in the histological images (Fig. 6). Less bone formation and a narrow gap between transverse processes were observed in PEC: B, indicating a failure of fusion. Compared with the newly formed bone in PEC: N(L)+B and PEC: N(H)+B, bone in PEC: B was less mineralized, as suggested by the less red-stained area of new bone in Masson-Goldner trichrome stained images (Fig. 6B, i–k). In contrast, fibrous tissue was mainly found between the transverse processes in PEC: BLK (Fig. 6B, a and g) and PEC: N(H) (Fig. 6B, b and h), with no fusion observed. In ACS: B, a thin layer of bone surrounded the whole scaffold, jointing the transverse processes (Fig. 6B, f and l).

Histological evaluation of bone formation.
Given that PEC: N(L)+B had fewer animals (n = 3), the histological images of all the six implants are provided in Supplementary Figure S3. Continuous bridging between transverse processes was observed in five out of six implants, although all the six implants were assessed as fused from μ-CT (Supplementary Fig. S2).
We further assessed ectopic bone formation beyond the scaffold (Fig. 6C). Fibrous tissue was mainly present at the edge of the scaffold in Group I–V. Newly regenerated bone was well confined within the scaffold area in these groups. On the other hand, a bone shell was found surrounding the scaffold of ACS: B, with massive adipose tissue and scattered bone detected between the scaffold and the bone shell, indicating a larger amount of ectopic bone and adipogenesis (Fig. 6C, f and l).
To evaluate the stiffness of the spine or the quality of the newly formed bone, the spines were potted in the poly (methyl methacrylate) cement and underwent biomechanical testing. Two screws were inserted into the vertebral bodies to extend the testing moment arms. Each specimen was examined by x-ray to confirm that the screw did not go through the disk. PEC: N(L)+B was not included in the biomechanical testing, as all the specimens in this group were processed for histological evaluation.
Figure 7 showed that stiffness in extension, flexion, and lateral bending was significantly improved in all the treatment groups compared with the intact spine without any interventions. PEC: N(H)+B showed improved stiffness in extension (Fig. 7A) and flexion (Fig. 7B) compared with PEC: BLK, PEC: N(H), and PEC: B, although the improvements were not significant. In the lateral bending test, the bone of PEC: N(H)+B was significantly stiffer than that of PEC: B (Fig. 7C). PEC: BLK failed to induce spinal fusion but it improved the stiffness of the spine, suggesting that the implantation of scaffold or formation of the scar tissue after the surgery could increase the biomechanical stiffness of the spine, and it could mitigate the differences caused by different treatments.

Biomechanical stiffness of spines.
Discussion
Combinative application of NELL-1 and BMP-2 has been shown to enhance BMP-2-induced bone regeneration in calvarial defect, 32 tibia rapid distraction osteogenesis model, 31 and femoral defect. 28 Zhu et al. described that dual delivery of NELL-1 (25 μg) and BMP-2 (25 μg) enhanced each growth factor's effect on bone healing in rabbit tibia distraction osteogenesis. 31 No drug delivery carrier was used in this study. Administration of NELL-1 (∼0.6 and 1.2 μg) and BMP-2 (∼0.6 and 1.2 μg) with a collagen/PLGA scaffold increased bone volume of the calvarial defect by 10%, compared with BMP-2 treatment alone. However, the resultant repair was only partial (70% of uninjured bone), 32 suggestive of a need of an appropriate carrier. Hydroxyapatite-coated PLGA scaffold was also used for dual delivery of NELL-1 (45 μg) and BMP-2 (22.5 or 45 μg) in rodent femoral segmental defects, 28 which have resulted in more physiological bone with a thicker cortical structure and much denser trabeculations, compared with the BMP-2-only group.
Although these studies showed promising outcomes in respect of higher quantity and better quality of bone with NELL-1 + BMP-2 treatment, relatively high levels of BMP-2 were employed. A lack of control release carrier for growth factor delivery could reduce the efficacy of the delivered growth factors and might result in supraphysiologic doses in situ due to burst release, even with the use of a hydroxyapatite-coated carrier. 33
In this study, we demonstrated the synergistic effect of NELL-1 and BMP-2 in vitro for the osteogenic differentiation of BMSC. We further demonstrated the efficacy of dual delivery combining two growth factors for posterolateral spinal fusion in rats by using a PEC system for controlled release of NELL-1 and BMP-2. Two doses of NELL-1 (3.5 and 20 μg) were tested based on previous work on NELL-1.34,42 NELL-1 at the dose of 45 μg delivered with DBM (75 μL) was used to induce bone regeneration, with partial bridging in the femoral segmental defect model, 42 whereas a much lower NELL-1 dose of 5 μg was reported when used with β-TCP/DBM (0.3 mL) to achieve successful spinal fusion. 34 DBM contains beneficial osteoinductive growth factors, mainly BMP-2. Approximately 3.6 μg of BMP-2 was estimated per gram of DBM, 43 indicating that 0.27 and 1.08 μg of BMP-2 was present in the DBM in the two studies.42,43
The ultra-low dose of BMP-2 (0.25 μg) employed in this study was thus at a similar level as the amount present in DBM, in contrast to the high dosage used in others dual delivery studies.28,31,32 Delivery of this ultra-low dose of BMP-2 alone resulted in suboptimal bone fusion, as shown by the lack of significant bone formation in μ-CT bone histomorphometry analysis and histological evaluation. In contrast, the presence of both the low and high dose of NELL-1 together with this ultra-low dose of BMP-2 achieved solid spinal fusion, with significantly enhanced biomechanical stiffness. The control release carrier PEC thus enabled both NELL-1 and BMP-2 to be used at a much lower dose (3.5 μg NELL-1 and 0.25 μg BMP-2) compared with the previous studies, while exerting effective spinal fusion. A high dose of BMP-2 (10 μg) delivered by ACS, although it resulted in satisfactory fusion score, fusion rate, and biomechanical stiffness, did not achieve bone regeneration within the scaffold, with ectopic bone expanding out from the scaffold and forming bone shell. A layer of fat tissue was observed between the scaffold and the bone shell. These phenomena of ectopic bone formation and adipogenesis induced by BMP-2 are in accordance with previous reports.14,16,25,44
Although our in vitro results showed that NELL-1 alone did enhance BMSC osteogenic differentiation, it could not achieve therapeutic efficacy in vivo. Our in vivo results demonstrate that NELL-1, in the absence of DBM carrier, is not able to induce spinal fusion. This is consistent with published reports.27,28 Unlike BMP-2, NELL-1 has a negligible effect on cell proliferation and migration.28,45,46 As a result, it could not elicit cell recruitment and proliferation to initiate bone regeneration in situ. This problem was not encountered in the cell culture assay where the cells were already present.
In addition, the amount of effective NELL-1 present in situ at the spinal defect site would have been lower than the total delivered amount due to the control release system. According to our protein release kinetic analysis, 0.7% of NELL-1 was released per day after the first 24 h. The concentration of NELL-1 from PEC was estimated to be around 0.4 μg/mL after the initial burst release in vivo, far lower than the effective osteoinductive dose of NELL-1 in our in vitro study (10 μg/mL). In vivo, the amount present at the defect site could be even much lower. Despite this, the amount of released NELL-1 was able to synergize with BMP-2 to produce an osteogenic effect.
On investigation of signaling pathways, NELL-1 and BMP-2 function through distinct but complementary signaling pathways. NELL-1 activated the β-catenin-dependent Wnt (canonical Wnt) signaling pathway via integrins, 47 whereas BMP-2 treatment did not affect β-catenin expression. 28 Further, NELL-1 was found to phosphorylate the JNK mitogen-activated protein kinases (MAPK) pathway, which was not affected by BMP-2. 30 A recent study has reported that NELL-1 enhanced osteogenesis via the ERK-MAPK pathway. 48 Thus, NELL-1 may synergize the function of BMP-2 through activating canonical Wnt and MAPK pathways, which are complementary with BMP-2-activated pathways. Increased expression of BMP-2 receptor type I and type II by NELL-1 stimulation may also account for the synergy. 49
There are some limitations in this study. The small and variable sample sizes used in this study could have contributed to the observed high variability in bone histomorphometry analysis. We used a small sample size (n = 4) for the blank control (PEC: BLK), NELL-1 alone control (PEC: N(H)), and the positive control (ACS: B) as studies have their fusion outcomes consistently reported.18,19,27,28 The sample size was initially determined as seven to compare the fusion efficacy of PEC: B and PEC: N(H)+B. 50 One out of seven in PEC: B was euthanized due to paralysis after surgery. The positive results in the combination of BMP-2 and high-dose NELL-1 encouraged us to investigate the effect of a lower dose of NELL-1. Four rats were used in the combination of low-dose NELL-1 and BMP-2 (PEC: N(L)+B) as a pilot trial; however, one in PEC: N(L)+B had to be euthanized due to the paralysis after surgery.
The bone regeneration in this study was not optimum, possibly limited by the pore size of mPCL-TCP scaffold used (1.35 mm), which is larger than the ideal range (100–400 μm) for bone regeneration. The larger pore size could have compromised the trabeculations of newly regenerated bone. In addition, the micro-motion experienced in the rat spine fusion environment (inevitable due to the absence of appropriate internal and external fixation), and the lack of osteoprogenitor cells from surrounding tissue in our model, could have limited the regenerative outcome in our study. Nevertheless, the effective synergistic spinal fusion outcome of our dual delivery of NELL-1 and the ultra-low dose of BMP-2 is of particular significance given the critical size defect (15 × 6 × 4 mm) of our spinal fusion model, compared with the femoral defect (6-mm length and 4-mm diameter) 28 and calvarial defect (5-mm full-thickness) 32 model. Although the fusion efficacy of dual delivery of NELL-1 and BMP-2 is promising in the small animal model, the same needs to be validated in large animals in the future.
Conclusion
In this study, we demonstrated the efficacy of the dual delivery of NELL-1 and BMP-2 by using the PEC control release system in spinal fusion in an animal model. This study is of significance due to the synergistic effect between NELL-1 and an ultra-low dose of BMP-2 in achieving spinal fusion, in the absence of DBM. The adverse effects and high cost related to the supraphysiological dose of BMP-2 used presently in clinical practice can potentially be avoided with the significant reduction of BMP-2 dose.
Footnotes
Acknowledgments
The authors would like to thank Ms. Chan Wai Kam Julee and Mr. Amit K. Ramruttun for their assistance and technical support. L.L. is a PhD student receiving Research Scholarship from the Yong Loo Lin School of Medicine, National University of Singapore.
Disclosure Statement
K.T. is one of the inventors of NELL-1-related patents. He is a founder and board member of Bone Biologics, Inc./Bone Biologic Corp., which sublicenses NELL-1 patents from the UC Regents, which also hold equity in the company.
Funding Information
This study was supported by a grant from the National Medical Research Council (NMRC) (grant number: NMRC/CIRG/1372/2013).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.