
Abstract
In dental clinical practice, systemic steroids are often applied at the end of implant surgeries to reduce postsurgical inflammation (tissue swelling, etc.) and to reduce patient discomfort. However, the use of systemic steroids is associated with generalized catabolic effects and with a temporarily reduced immunological competence. We hypothesize that by applying locally anticytokine antibodies (antitumor necrosis factor alpha and anti-interleukin-1 beta) together with a bioactive osteogenic implant at the time of the surgical intervention for the placement of a construct, we will be able to achieve the same beneficial effects as those using systemic steroids but are able to avoid the generalized antianabolic effects and the reduced immunocompetence effects, associated with the systemic use of steroids. In an adult rat model, a collagen sponge, soaked with the osteogenic agent bone morphogenetic protein-2, was used as an example for a bioactive implant material and was surgically placed subcutaneously. In the acute inflammatory phase after implantation (2 days after surgery) we investigated the local inflammatory tissue response, and 18 days postsurgically the efficiency of local osteogenesis (to assess possible antianabolic effects). We found that the negative control groups, treated postsurgically with systemic steroids, showed a significant suppression of both the inflammatory response and the osteogenetic activity, that is, they were associated with significant general antianabolic effects, even when steroids were used only at a low dose level. The local anticytokine treatment, however, was able to significantly enhance new bone formation activity, that is, the anabolic activity, over positive control values with BMP-2 only. However, the anticytokine treatment was unable to reduce the local inflammatory and swelling responses.
Impact statement
In clinical practice of oral surgery after implantation of tissue-engineered devices and other constructs for surgically driven bone tissue engineering purposes (lateral and vertical bone augmentation, sinus lift, barrier membranes, etc.) local tissue inflammation and swelling processes are unavoidable. This study illustrates that the local use of specific anticytokine antibodies as an alternative to the generally used systemic steroids is able to enhance the desired osteogenesis activity significantly, and thus is able to avoid the general antianabolic and anti-immunological effects associated with the use of steroids. However, anticytokine therapy was unable to reduce local tissue swelling and inflammation.
Introduction
Oral surgeries are nowadays very frequent interventions in daily dental practice. A major area relating to this topic is dental implantology during which implants are placed, bone augmentation surgeries performed, and a number of different biomaterials used (barrier membranes, carrier materials, etc.).1,2 Such interventions are associated, as it is generally the case for surgical interventions, with postoperative tissue reactions at the surgically induced trauma site; in particular, postoperative acute local inflammation processes develop, combined with tissue reactions to local bleeding, 3 tissue swelling, etc.
And these tissue responses are often associated with unpleasant symptoms in the patients such as postoperative discomfort, local pain, tissue swelling, and local hyperthermia.4–6 To relieve the patients from these types of local symptoms (predominantly from local discomfort, from neurosensory disturbances, and from associated pain), and to reduce tissue reactivity and swelling, many surgeons use postoperatively in their patients systemic steroids as a one-time shot, in particular, if more extensive surgical interventions were performed.7–9
This therapeutic measure represents, however, quite a drastic treatment step, associated with a number of unwanted effects. Steroids are indeed well known to reduce tissue reactivity, acute inflammation, and also chronic inflammation, tissue swelling, but they are also associated with a reduction in anabolic activities and thus may impair desired postoperative osteogenic activities by promoting actively catabolic pathways. 10 Moreover, such effects are systemic indeed and expose the patients to higher risks of infection, impaired wound healing, and unwanted endocrine side effects, beside a possible unwanted effect of reduction of osteogenesis, in particular, if dental implants are placed or if bone augmentation measures were established such as ridge augmentation, lateral or vertical bone augmentation, or sinus lift procedures.11,12
The immuno-osteological mechanisms associated with such implant surgeries are mainly based on the acute (sterile) inflammatory response governed by different types of macrophages, which actively provoke and regulate these processes by a number of cytokines that are secreted by them.13–15 A large number of cytokines have been described in the literature to be involved in these postoperative acute inflammatory responses to implants and surgical trauma in the bony environment, and the major ones that were described repeatedly are tumor necrosis factor alpha (TNF-α) and interleukin-1 beta (IL-1β).16–18 We hypothesize that by applying locally at the end of surgery, instead of systemic steroids, local anticytokine antibodies to inhibit TNF-α and IL-1β biological effects, that we will be able to obtain the same desired therapeutic effects as generated with systemic steroids, but are able to avoid the unwanted antianabolic and the undesired systemic effects of steroids. We chose TNF-α and IL-1β as representative cytokines for this study since these two compounds are practically always involved in proinflammatory processes, are very well characterized, are therapeutically dealt with in human clinical medicine, and their pleomorphic nature is also well known.19–22
To test this hypothesis we applied during the surgical intervention in which we subcutaneously deposited in adult rats as experimental animal model a bioactive osteogenic implant, that is, a biological carrier (bone morphogenetic protein-2 [BMP-2] soaked collagen) a local one-time depot of anti-TNF-α-antibodies (aTNF-α) and anti-IL-1β-antibodies (aIL-1β). We then investigated in the acute postoperative phase (2 days after surgery) the extent of the expected anti-inflammatory response and checked 18 days after surgery if there was a beneficial effect on osteogenesis relating to this local anticytokine treatment protocol. Comparisons with systemic steroid applications as controls and as comparison to clinically used standard therapies nowadays were also performed, and appropriate negative and positive control groups established.
Materials and Methods
Materials
Collagen sponge (absorbable collagen sponge [ACS]; Inductos®) was obtained from Medtronic (Minneapolis, MN, USA), as well as human recombinant BMP-2 (Inductos). BMP-2 was used at a concentration of 1 μg/μL in sterile aqueous BMP-2 solvent, provided by the manufacturer (Medtronic). TNF-α monoclonal antibodies (rat-derived; R&D Systems, Minneapolis, USA) were used at a concentration of 1 μg/μL, and IL-1β monoclonal antibodies (rat-derived; R&D Systems) also at 1 μg/μL. Both antibodies were dissolved in sterile PBS (standard phosphate-buffered saline); dexamethasone (Dex) was purchased from Guangzhou Baiyunshan Tianxin Pharmaceuticals, Guangzhou, China; low concentration of Dex (l-Dex) was chosen as 1.2 mL of 0.1 mg Dex/mL; a medium concentration (m-Dex) at 2.4 mL of 0.1 mg Dex/mL; and a high concentration of Dex (h-Dex) at 3.6 mL of 0.1 mg Dex/mL. Dilution of Dex was performed with medical-grade physiological saline (Chen Xin®; Chen Xin Pharmaceutical Co., Ltd., Jining, China).
Experimental design
Eight-week-old male Sprague Dawley (SD) rats (mean body weight: 230 g, ranging from 190 to 250 g) were used in this study and divided into seven experimental groups (Tables 1 and 2); each group consisting of n = 6 animals. This resulted in the use of a total of 72 rats by placing one implant (ACS sponge) per animal and by investigating results at two different time points (i.e., at 2 days [all groups, n = 42] and at 18 days [groups with BMP-2, n = 30]) postoperatively. ACS-sponges were cut into identically sized circular samples (8 mm diameter). The experimental groups were defined as follows (Table 1): collagen sponge (ACS) with both anticytokine antibodies (5 μL of anti-TNF-α + 5 μL of anti-IL-1β antibodies +20 μL 1 μg/μL BMP-2, all of these compounds added directly to the ACS-collagen carrier); BMP-2 dosage for effective osteoinduction within 3 weeks in the rat model had been determined previously (see Ref. 23 for details). Then three groups with low, medium, and high concentrations of Dex (ACS +20 μL BMP-2 + low(l)-Dex (applied 12 h after operation by an intravenous route; dorsal tail vein); ACS +20 μL BMP-2+ medium (m)-Dex; ACS +20 μL BMP-2+ high (h)-Dex). Dosages chosen for steroids were based on previous reports performed in rodents, in which the dosages used relate to human dose equivalents 24 ; the anticytokine antibody dosages employed were based on studies performed on anticytokine receptor drug activities.25,26
Experimental Groups
BMP-2, bone morphogenetic protein-2; DEX, dexamethasone; IL-1β, interleukin-1 beta; TNF-α, tumor necrosis factor alpha.
Antibody Treatments
One experimental group received BMP-2 only with ACS (positive control group, the BMP-2 again being added directly to the ACS sponge). We also established two negative control groups receiving the anticytokine antibodies only (ACS +5 μL anti-TNF-α antibody solution and ACS with 5 μL anti-IL-1β antibody solution, these again being added directly to the ACS sponge; cf. Table 2). The prepared ACS samples were stored under aseptic conditions overnight before use. Half of the animals were sacrificed 2 days after surgery (peak time of the acute inflammatory response) for analysis and quantification of the degree of inflammation (see section Microscopy and histomorphometry), and the other half at 18 days postoperatively for the quantification of the newly formed bone tissue.
Surgery
All SD rats received a general anesthesia by intraperitoneal injection of 3% pentobarbital (Devon Biological Co., Ltd., Hangzhou, China). Aseptic techniques were used during the surgical procedures. The iliac crest was used as the landmark to determine the location of the skin incision; a 25 mm posterior longitudinal incision was made unilaterally on the back of the animals, 5–10 mm laterally from the midline. ACS carrier materials were then implanted in the subcutaneous space at the lumbar level of the back together with the test substances, as described in Table 1. The implantation site was thereafter closed, and the skin sutured with standard nonabsorbable suture materials (Hangzhou Huawei Medical Supplies Co., Ltd., Hangzhou, China) and disinfection performed with 10% povidone iodine (Minsheng®; Hangzhou Minsheng Pharmaceutical Co., Ltd, Hangzhou, China). The Dex-experimental groups received a one-time low, medium, or high dosage of Dex 12 h after surgery intravenously (see section Experimental design).
The permission for the animal experiments was obtained from the Zhejiang province, China. Moreover, the animal experiment was approved by the Ethical Committee of the School of Stomatology, Zhejiang Chinese Medical University (animal ethical committee approval number: SYXK (浙) 2018-0012). All animal experiments were carried out according to the ethical laws and regulations of China and the guidelines of animal care established by the Zhejiang Chinese Medical University, as well as the EU Directive 2010/63/EU for animal experiments.
Animal husbandry
The rats were kept at the animal experiment center of Zhejiang Chinese Medical University Laboratory Animal Research Center, Hangzhou, China. Room temperature was kept at 18–23°C, day/night light cycle times were defined as 14/10 (h/h) cycles, and the humidity was monitored and adjusted to 60–80%. The animals received sterile complete rat food (Anlimo, Nanjing, China), and their drinking water was filtered; they had free unlimited access to water.
Tissue processing and sampling
The SD rats were sacrificed by overdoses of CO2 gas on postoperative days 2 or 18, respectively, at which point in time the implants were retrieved together with ample surrounding tissue masses. Chemical fixation of the retrieved tissue blocks was performed in buffered 10% formaldehyde solution (for details see Ref. 27 ) for 1 day at room temperature. Then they were rinsed in tap water, dehydrated in ethanol, and embedded in methylmethacrylate, as previously described in Ref. 28
According to a systematic random-sampling protocol, 29 the tissue blocks were then cut into 5–7 slices of 1-mm thickness by using a Leco diamond saw (Leco VC-50; St. Joseph, MO, USA). 28 All slices were glued to plastic specimen holders and ground down to a final thickness of 80–100 μm. They were then surface polished and surface stained with McNeal's Tetrachrome, Toluidin blue O, and basic Fuchsin. 27
Microscopy and histomorphometry
Volume of inflammation
The histological sections were photographed at a final magnification of × 40 in a Nikon light microscope (Eclipse 50i Microscope, Tokyo, Japan), and photographic subsampling performed according to a systematic random-sampling protocol. 29 Using the photographic prints, the total areas of inflammation around implants (correlated with each sample) were measured, using stereological principles, by point counting methods. 30 The final total tissue volumes were then estimated using Cavalieri's principle. 31
Numerical estimators
The total number of cells in the inflamed areas (number of cells per unit tissue area) was counted (at 100 × magnification); these included macrophages, connective tissue cells, endothelial cells, etc. to obtain the numerical area densities of all cells (NA) (at 400 × magnification); macrophages were counted separately for a more detailed analysis of their involvement in the inflammatory process. We also determined the blood vessel area density (at 100 × magnification), as previously described. 32
Volume of newly formed bone
The histological sections from the 18-day animals were photographed at a final magnification of × 40 in a Nikon light microscope (Eclipse 50i Microscope), and photographic subsampling performed, again according to a systematic random-sampling protocol. 29 The newly formed bone tissue was then quantitated by point counting, 30 and the final bone volumes estimated by applying Cavalieri's principle. 31
Thickness of fibrous capsule
The thickness of the fibrous tissue capsule formed around the implanted materials was estimated by using a set of equally spaced parallel lines placed randomly and perpendicularly to the implanted material surface, and by measuring the line lengths over the fibrous tissue areas (for details see also Ref. 31 ).
Statistical analysis
All data are presented as mean values together with the standard error of the mean. Differences between the experimental groups were analyzed using the one-way ANOVA test. Statistical significance was defined as p < 0.05. All statistical analyses were performed with SPSS® 21.0 software (SPSS, Chicago, IL, USA). The Bonferroni post hoc test was implemented for data comparison purposes.
Results
Morphology
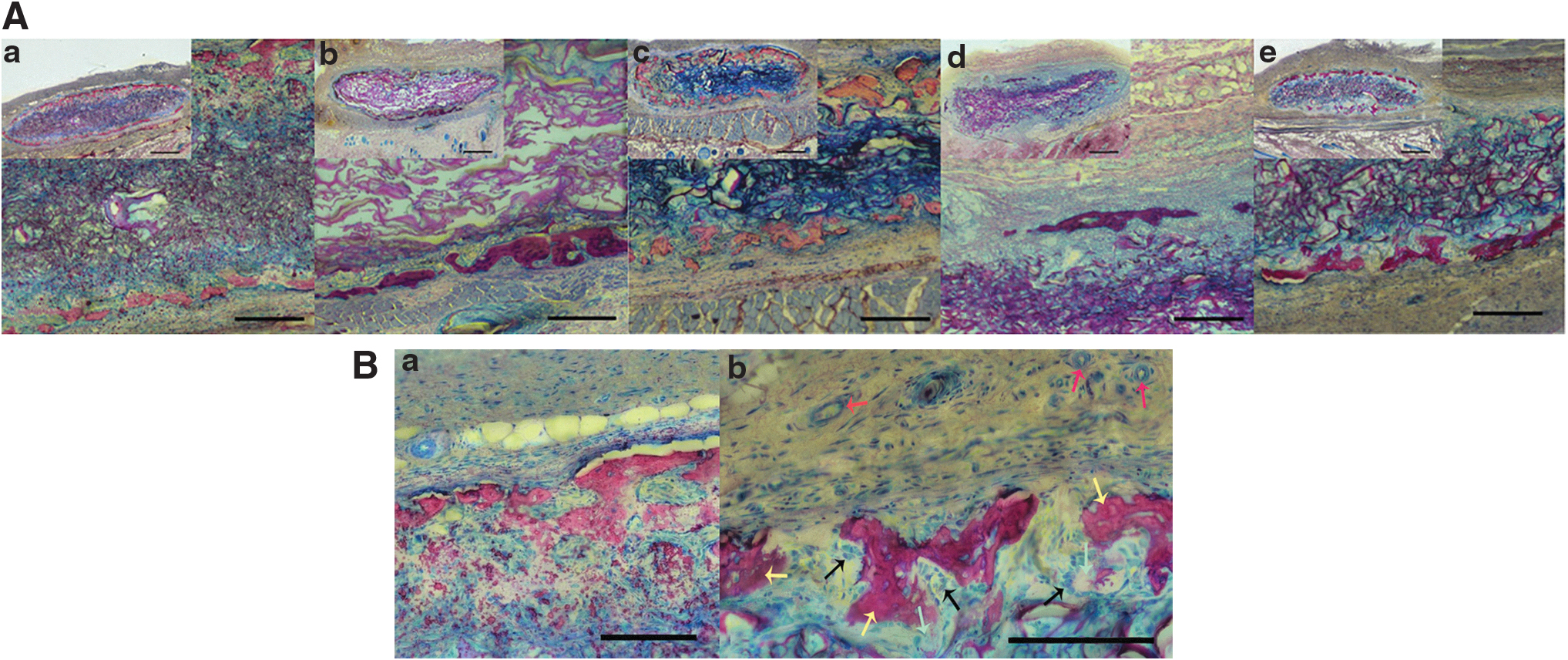
The morphologic analysis of the five experimental groups of specimens from the 2-day postoperative groups (Fig. 1A: a–e) reveals the presence of the collagen sponge materials in each group. For overviews, see inserts in each figure; these also illustrate the inflammation volumes around each implant. The illustrations at higher magnifications reveal the presence of the collagen fibrous materials as a spongy network. Interdispersed between the collagen fibers one can readily recognize not only the presence of numerous free inflammatory cells but also blood vessels and connective tissue cells. The higher magnification images (Fig. 1B: a, b) show the diversity and multitude of inflammatory cells within the collagen sponge and around the sponge. The majority of the inflammatory cells are identified as macrophages with their typical pleomorphic nuclear shapes and the cytoplasm with inclusions of phagosomes. The fiber density of the sponges appears similar among the different groups; that is, a similar degree of swelling seems to occur in these. The inflamed perispongeal spaces, appearing edematous and infiltrated by numerous inflammatory cells, do vary considerably in dimensions and in size between the groups (for quantitative data see section Histomorphometry below). Very similar histological appearances are revealed in the two control groups with aTNF-α and aIL-1β only, but without BMP-2 (Fig. 2). A striking difference to these images is apparent in the 18-day postoperative histological sections (Fig. 3A) where in several groups dark-red-stained masses of newly formed bone tissue can be readily identified. The bony masses are present predominantly in the peripheral parts of the collagen sponges. Higher magnifications of the bone tissue (Fig. 3B) reveal the typical structure of mineralized woven bone with the irregularly enclosed osteocytes in the mineralized bony masses as well as the presence of osteoblasts at selected sites along the bony surfaces. Osteoclasts are also present in these areas but more scarcely (not illustrated).
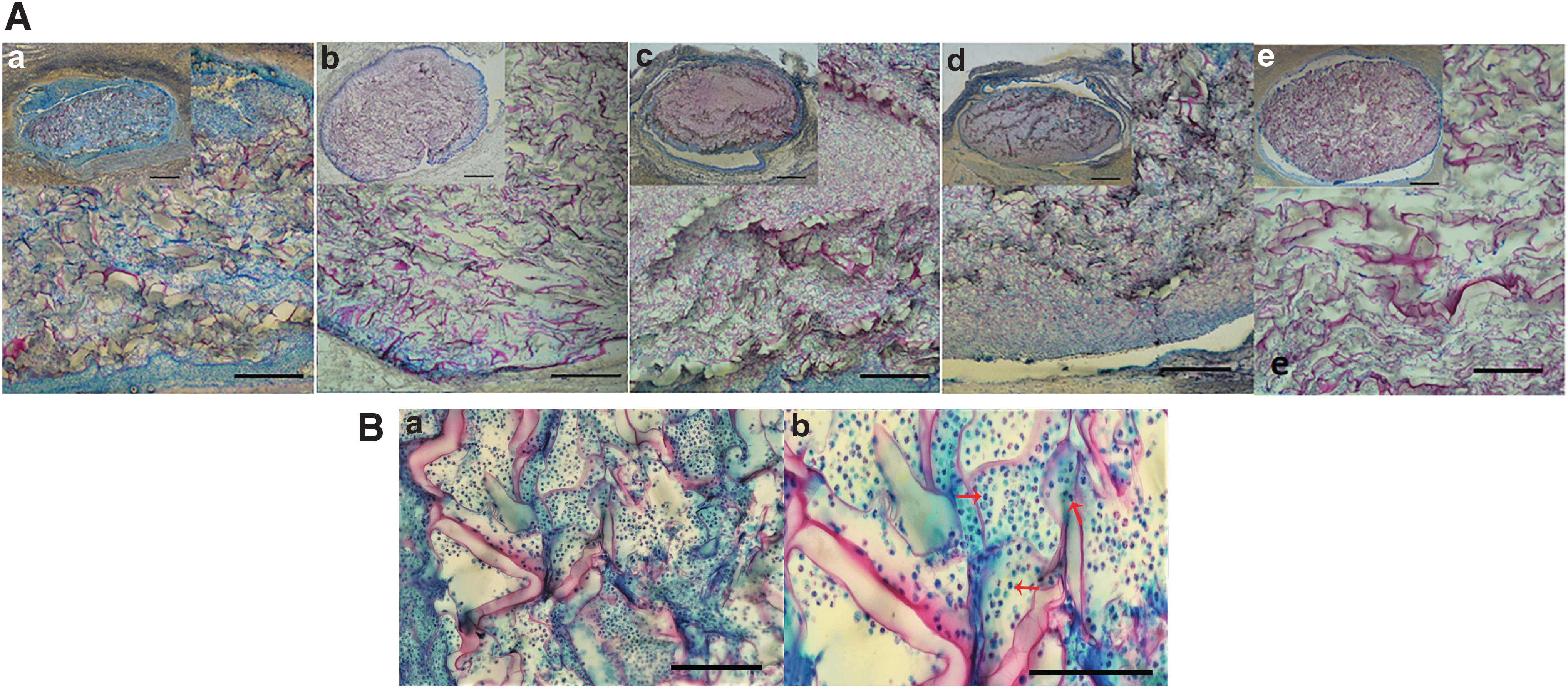
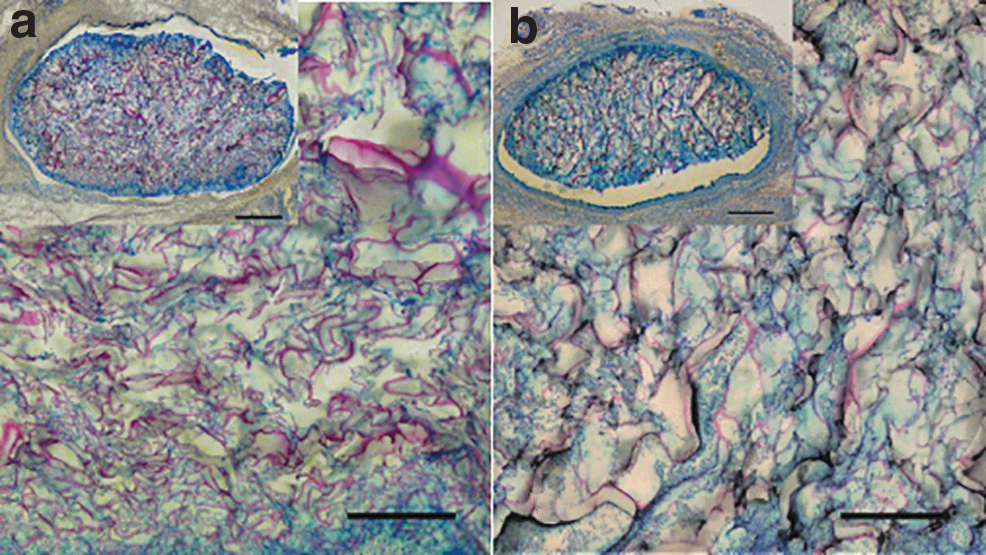
Light micrographs of the subcutaneously implanted ACS-collagen sponge materials of the two control groups in which no BMP-2 was used, 2 days after surgery.
Histomorphometry
Figure 4a illustrates the total inflamed tissue volume 2 days postoperatively around the ACS implants in each experimental group. As expected, when Dex was applied the tissue swelling results were significantly reduced. However, there was no concentration dependency recognizable as an effect of this drug. In fact, the swelling was unexpectedly reduced to a similar degree between the medium and large dose groups of Dex applied, each having been given in a one-time shot. Suppression of tissue swelling was indeed significant compared with the BMP-2 only group (which we take as the reference group here). In the presence of the anti-TNF-α and anti-IL-1β antibodies, the degree of tissue swelling clearly is significantly enhanced over the reference group and characterized by a high degree of variation (CV/coefficient of variation: 31%, compared with a CV of 20% in the control group). Figure 4c reveals further that the cellularity (defined here as number of cells per unit tissue area) in the swollen tissue compartment is clearly highest in the anti-TNF-α/anti-IL-1β groups, at a value significantly higher than the cellularity for the BMP-2 only reference group. Meanwhile, the Dex groups show the lowest cellularities in the swollen area, paralleling the degree of swelling shown in Figure 4a. The same pattern of cellularities was found for the macrophages when these were counted separately and specifically (Fig. 4b), and for the nonmacrophage cells in the swollen areas (Fig. 4d). The analyses of control groups anti-TNF-α antibody (Ab) alone and anti-IL-1β Ab alone (Fig. 5a–d) reveal that the tissue swelling is not reduced by either of the two antibodies; however, the densities of the inflammatory cells were significantly reduced by the anti-TNF-α Ab alone, but not by the anti-IL-1β Ab. In addition, these inflammatory cellularities were not reduced when using these two antibodies in combination (Fig. 4a–d).

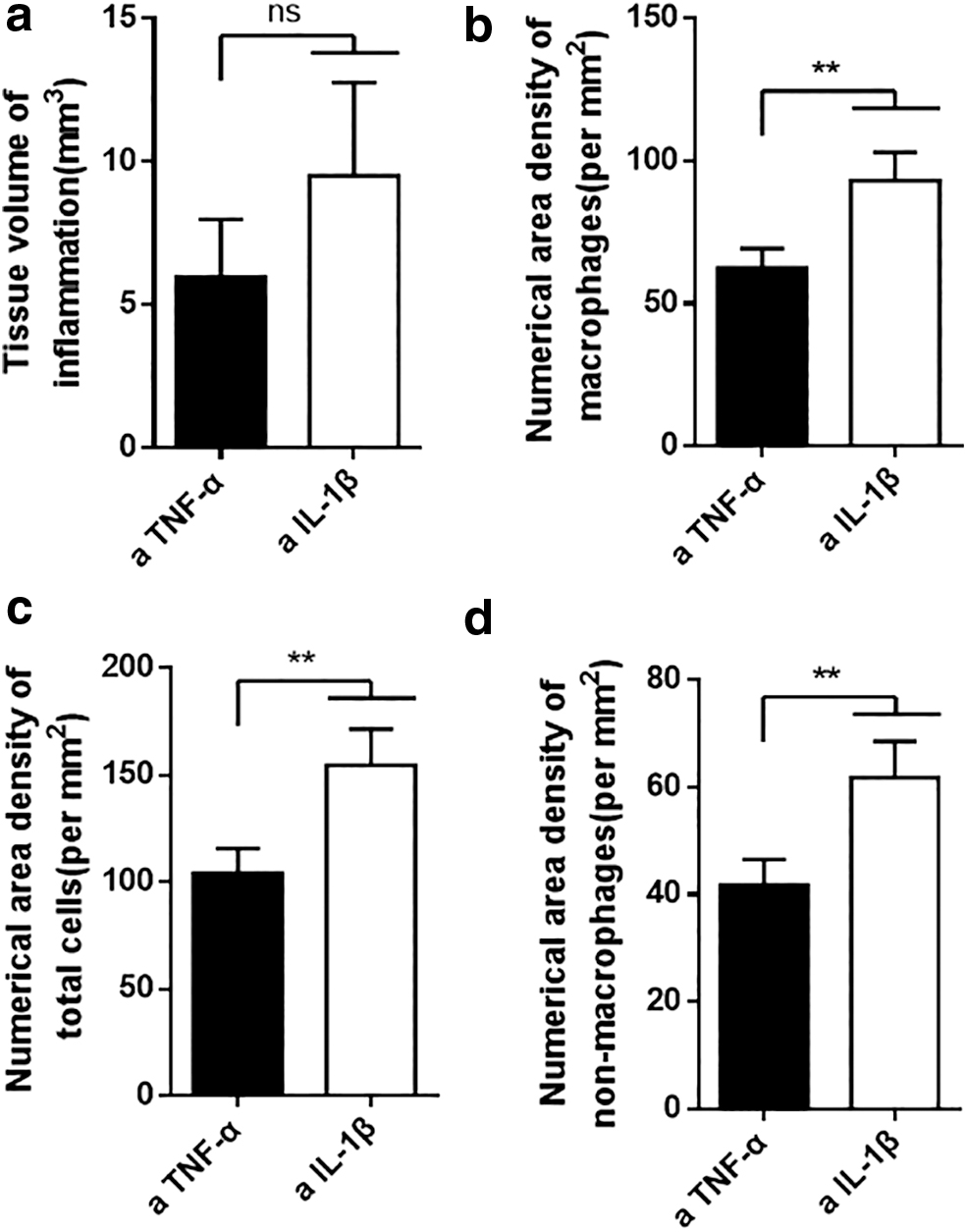
The quantitative results of the two control groups in which local antibody treatment was performed only in the absence of BMP-2. It reveals that the tissue volume of inflammation in the aIL-1β group is practically the same as that in the aTNF-α group, but with a higher degree of variation (see larger SEM bar)
The most interesting result is the finding that the newly formed bone tissue volumes (Fig. 6) are highest when the anti-TNF-α and the anti-IL-1β antibodies were applied together (significant compared with the BMP-2 only group, at 18 days after surgery). As expected in the Dex groups bone formation was reduced significantly in all of them (Fig. 6) when compared with the BMP-2 control group and the anticytokine-Ab-treated groups. The analysis of the thickness of the fibrous tissue capsule (a measure for the fibrotic response) revealed (Fig. 7) that this response was of a similar degree in the BMP-2-only group as in the group to which both the anti-TNF-α and anti-IL-1β Abs were applied. The quantification of the blood vessel area densities (AA of blood vessels) (Fig. 8) as a measure of angiogenesis activity in the peri-implant space shows that these densities are the same as those obtained for the inflamed tissues of all experimental groups (Fig. 8).

This graph illustrates the volumes of the newly formed bone tissue per implant. It reveals that the antiTNF-α/anti-IL-1β group shows the highest volumes of newly formed bone (significantly higher than the BMP-2 only control group). The Dex-treated groups all showed significantly lower bone volumes formed, independent of the Dex dosage used. **Indicates significant differences (p < 0.01) between groups, *p < 0.05.
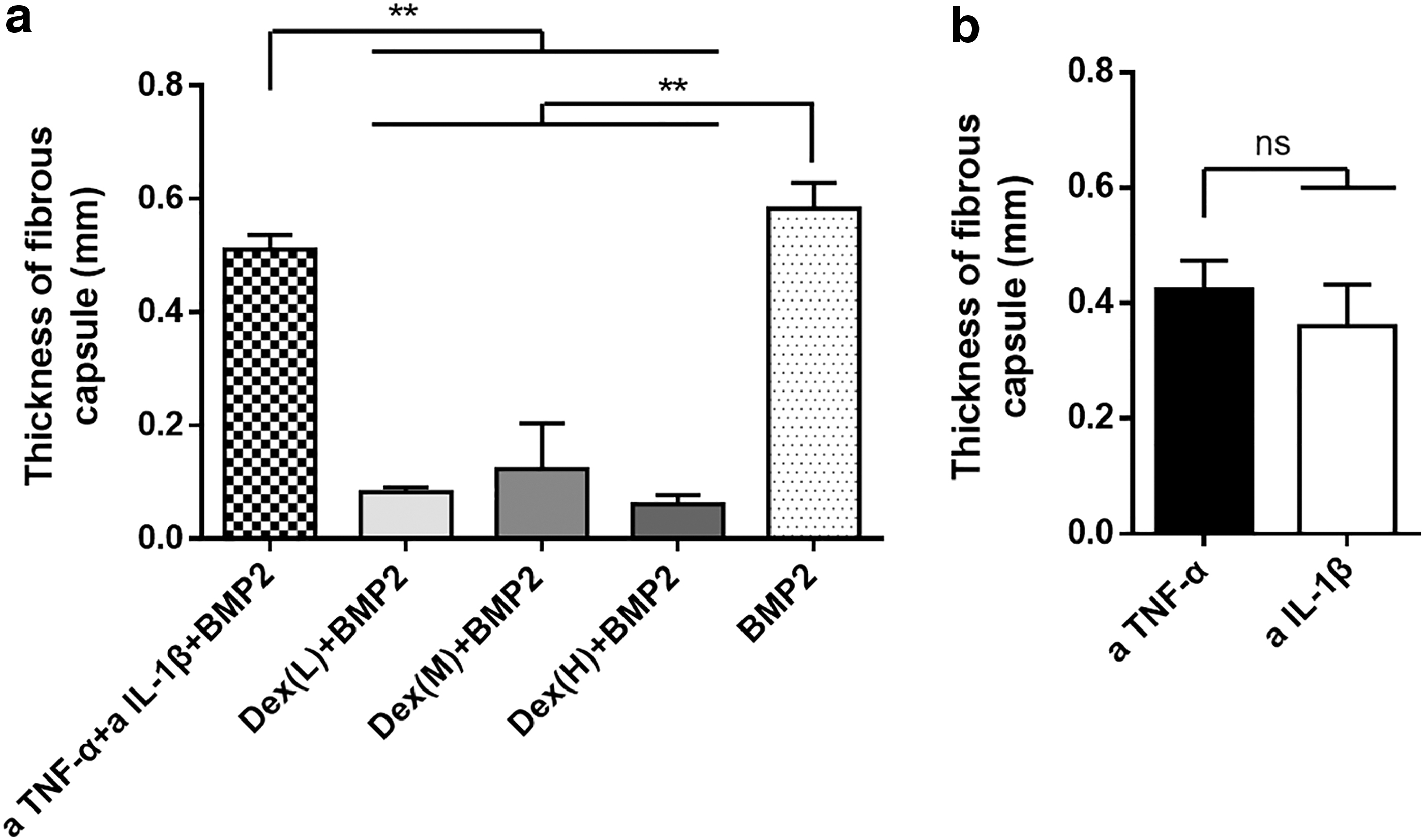
This figure illustrates the thickness of the fibrous capsule present around the implants 2 days postoperatively. It reveals in

This graph illustrates the blood vessel area density for each experimental group. It reveals that these densities are of a similar level in all groups. No significant differences are found, not even between the Dex groups. ns, nonsignificant differences.
Discussion
All experimental groups showed peri-implant tissue spaces with inflammatory responses (Figs. 1–3, 5, and 7). This was an expected finding since the deposition of implant materials into the body is generally associated with an acute inflammatory response. In the majority of body tissue types this response is mediated by foreign body giant (FBG) cells and macrophages. Whereas the FBGs topographically adhere closely to the implant (or carrier) material itself,33–35 the macrophages are dispersed around the implanted materials inside the whole inflamed tissue spaces. They represent the major cell types regulating the peri-implant inflammatory response, and consist of various subtypes with different functions in this process while also playing regulatory roles in bone repair/induction processes.36–39 As expected according to previous publications, in experimental groups treated with steroid hormones the extent of tissue inflammation was greatly reduced.5,8,11 Previous studies had revealed in clinical practice that such a treatment can reduce postsurgical inflammatory symptomatology, helping to reduce the local and general symptoms and patient discomfort.5,12 At the same time, it was an unexpected finding in our study that the tissue volume of inflammation was significantly increased in the anticytokine-treated groups; that is, higher than that in the steroid groups and also higher than that in the untreated control group. Detailed analysis showed that not only did the number of macrophages increase significantly in the peri-implant inflamed spaces in this group (over both control and Dex groups), but that nonmacrophage cell pools had increased significantly in that group. Specific anticytokine treatments are thus not associated with a reduction of local inflammation as in the steroid groups, as could be expected from similar experiments carried out in other fields.9,40–42 It could be speculated that compensatory increases of a number of other cytokines are the basis for such an effect. This may be the case when using the anti-IL-1β antibodies since the negative control group of anti-IL-1β-only revealed an increase in tissue inflammation, even in the absence of the use of BMP-2. The application of anti-TNF-α antibodies alone was not associated with such an increase, and the inflammation volume remained at the same level as that of the BMP-2 control group.
The analysis of the negative control groups with an application of the anticytokine antibodies alone, that is, in the absence of BMP-2, showed that the use of anti-TNF-α antibodies alone indeed is powerful enough by itself to reduce the inflammatory response; however, the anti-IL-1β antibodies were not. This differential response may be related to some subgroups of macrophages (subtypes) that are known to exert quite different effects on the histopathological processes.14,37–39 Since the measurements of the thickness of the peri-implant capsule of the fibrotic response 43 (long-term effects) did not reveal any differential response, the initial differences observed most likely are of a short-term nature only. The anticytokine-Ab groups were not associated either with an enhanced fibrotic response. Only the Dex groups were able to reduce such undesired fibrotic-response effects. A surprising finding in the Dex groups was the result that the lowest dosage group already was associated with a maximum swelling-reduction effect compared with the middle and high dosages, and that a single application mode was sufficient to obtain such effects, illustrating the high degree of efficacy of the steroid application.
Another unexpected finding was that even the lowest Dex dosage (after a one-time application only) was associated with a significant and extensive reduction in bone formation, which was reduced to the same low levels as that of the middle and high dosages of Dex. This illustrates impressively the great disadvantage and risk of steroid use after surgical implant material placement, even when used at a low dose and at a one-time application only. The antianabolic effects of this drug are well known and well documented, but a general awareness of the really high potency and potential risks of postoperative steroid use for the implant healing process is not present in the clinical field.
Another unexpected finding of this study was the result that the local anticytokine treatment protocol was associated with a clear and significant increase of bone tissue formation in the peri-implant tissue spaces. This opposite effect, compared with the steroid therapy, by the anticytokine treatment protocol is difficult to explain. Since we did not find an increased vascularity (Fig. 8) under these conditions (nor any other condition) and thus no increased perivascular cell pool of osteogenic precursor cells was present that could have helped to explain the result. The finding of a similar density in blood vessels in all experimental groups thus points out that the mechanism most likely is associated with other cell populations. The most likely candidate cell pools for explanations are the macrophage populations that became recruited under the different treatment protocols. The anticytokine group may favor, through specific enhancement of an osteogenesis supporting subgroup of macrophages, 44 that more bone tissue is formed. And indeed several, mainly in vitro, studies point to this hypothetical explanation.44–47 This is, however, only one of several possible explanations. Another possible explanation is a locally increased anabolic activity of insulin-like growth factor-1, which was observed to play a role in systemic clinical therapy with anti-TNF-α antibodies in young patients with Crohn's disease,48,49 and elderly patients with osteoporosis combined with Crohn's disease. 50 Since we do not know if the increased local bone masses in our study are due to an increase of osteogenesis activity or are due to a decrease of bone resorption activity (which is another possible mechanistic pathway14,51) we thus may only speculate. An early increase of bone resorption inhibition by a reduced recruitment of osteoclast precursor cells and a reduced formation of osteoclasts, triggered by the influence of specific macrophage subgroups, is another possible mechanistic pathway operating under these conditions.52,53 The experimentally established anticytokine activity may have interfered with the Rank-Ligand-based osteoclast formation mechanism, which is also a possible pathway for an explanation.54,55
What is of a practical importance and of interest to the clinician is the fact that enhanced bone formation activities can be induced by use of a simple, local anticytokine treatment protocol with a simple single local application mode. And if, in spite of an increased local swelling and inflammation that both are observed under such an intervention, the adverse symptoms in the patient become still reduced (or even eliminated, such as discomfort and local pain) then the local anticytokine treatment protocol would still have a potential for future practical use. However, it will be necessary to clarify in clinical practice if the use of such a local, anticytokine treatment protocol is indeed free of unwanted adverse symptomatologies after implant placements, and if it is indeed reduced (or even eliminated), but remains associated with an increased bone formation activity and an increase of the local inflammatory response.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was financially supported by the Foundation of the clinic for Osteoporosis, Inselspital, Bern University Hospital, Bern, Switzerland.