
Abstract
This report describes activity in Europe for the years 2016 and 2017 in the area of cellular and tissue-engineered therapies, excluding hematopoietic stem cell treatments for the reconstitution of hematopoiesis. It is the eighth of its kind and is supported by five established scientific organizations. In 2016 and 2017, a combined 234 teams from 29 countries responded to the cellular and engineered tissue therapy survey; 227 teams reported treating 8236 patients in these 2 years. Indications were categorized in hematology/oncology (40%; predominantly prevention or treatment of graft vs. host disease and hematopoietic graft enhancement), musculoskeletal/rheumatological disorders (29%), cardiovascular disorders (6%), neurological disorders (4%), gastrointestinal disorders (<1%), as well as miscellaneous disorders (20%), which were not assigned to the previous indications. The predominantly used cells were autologous (61%). The majority of autologous cells were used to treat musculoskeletal/rheumatological (44%) disorders, whereas allogeneic cells were mainly used for hematology/oncology (78%). The reported cell types were mesenchymal stem/stromal cells (MSCs) (56%), hematopoietic cells (21%), keratinocytes (7%), chondrocytes (6%) dermal fibroblasts (4%), dendritic cells (2%), and other cell types (4%). Cells were expanded in vitro in 62% of the treatments, sorted in 11% of the cases, and rarely transduced (2%). The processing of cells was outsourced to external facilities in 30% of the cases. Cells were delivered predominantly intravenously or intra-arterially [47%], as suspension [36%], or using a membrane/scaffold (16%). The data are compared with those from previous years to identify trends in a rapidly evolving field. In this edition, the report includes a critical discussion of data collected in the space of orthopedics and the use of MSCs.
Impact statement
The surveying of cell and tissue-engineered therapies is a relevant instrument to capture developing trends and monitor advances in the field, based on effective treatments performed.
Introduction
Delivery of cell and tissue-engineered therapies continues to increase steadily, both in terms of the number of patients receiving transplants and the range of diseases treated. The methodology used in these therapies is also progressively becoming more varied and complex, with a growing number of possible tissue sources, methods of cell preparation and expansion, and transplant delivery procedures. Several aspects of the current therapeutic environment for transplant therapy warrant real-world documentation of the interventions being performed in transplant centers.
First, a large proportion of cell and tissue-engineering treatments is currently administered outside the clinical trial or peer-reviewed study setting. In some cases, these interventions have not yet been approved for the particular indication by corresponding regulatory bodies. The published literature, therefore, does not provide an accurate representation of the current trends associated with cell and tissue-engineered therapies. Furthermore, analysis of peer-reviewed studies indicates that patients treated with cells (stem or otherwise) from the same tissue source may not be receiving the same treatment across centers. This is due to center-specific differences in cell product definition criteria, as well as wide variability in cell/tissue production techniques.
Given this present therapeutic landscape, it is imperative to provide transparent reporting of a representative cross-section of all procedures performed across transplant centers to document treatment patterns and the methodological details of delivered interventions. These data will not only provide documentation of the prevalence of specific procedures relative to supporting data and approval from regulatory bodies but also will help direct and prioritize future research.
Since its first appearance in 2008, the aim of this survey has been to report an unbiased update on the voluntarily provided number of patients treated using cellular and tissue-engineered therapies in Europe and Eurasian countries associated with the European Group for Blood and Marrow Transplantation (EBMT).1–7 The International Society for Cellular Therapy (ISCT), of the European Chapter of the Tissue Engineering and Regenerative Medicine International Society (TERMIS-EU), of the International Federation for Adipose Therapeutics (IFATS), of the International Cartilage Repair Society (ICRS), and the EBMT have made this possible by their continued support.
The survey comprises data of treated patients sorted by specific therapeutic indications, cell/tissue donor types, together with the processing and delivery modes, without reference to the clinical outcome and thus avoiding any infringement of the publication rights for the clinical teams themselves.
Data generated in the surveys of previous years have already been published, along with assessments on the development of treatment numbers and modalities of cell delivery for the target indications.1–7 The combined treatments for 2016 and 2017, as well as distinguished recent trends, are reported in this article as determined by the data provided from the 9th and 10th activity survey, with a description of some recent trends. In addition to presentation of the collected data, the report includes an in-depth analysis of cell therapy development for musculoskeletal/rheumatological indications and discusses the importance of transparency in the processing of cells as well as their clinical use.
Patients and Methods
Definitions
For the purpose of this survey, cellular and tissue-engineered therapy is any clinical treatment based on living cells, excluding donor lymphocyte infusions (DLIs) and nonmanipulated hematopoietic cells, for hematological reconstitution. Data regarding DLIs and nonmanipulated hematopoietic cells for hematological reconstitution are collected and reported independently by the EBMT.8,9
Data collection and validation
Participating teams were, as in previous years, requested to report their data for 2016 and 2017 by indication, cell type and source, donor type, processing method, and delivery mode. In addition, for these two years, the survey was extended to include the type of clinical procedure and the site of processing. The survey followed the traditional principles of the EBMT transplant activity survey, which concentrates on numbers of patients with a first cellular therapy.
For the 2016 and 2017 survey, >500 teams known to be actively transplanting in 49 countries (39 European and 10 EBMT-affiliated countries) were contacted. The non-European countries affiliated with the EBMT activity survey are Algeria, Azerbaijan, Iran, Israel, Jordan, Lebanon, Nigeria, Saudi Arabia, South Africa, and Tunisia.
Aside from past contributors to the survey, newly identified teams were contacted and invited to report their data. These teams were identified either through their contribution to published clinical trials or their reports on the platform https://clinicaltrials.gov (using the search terms “Tissue-engineer” and “Cell” associated with either “Transplant” or “Treatment” in the relevant countries). In addition, the supporting societies distributed the survey directly to their members in Europe by email and/or published the survey and documents on their websites. Extended questionnaires (Supplementary Table S1), were received electronically.
Treatment rates
Treatment rates, defined as the reported numbers of patients receiving cellular or tissue-engineered therapies and the number of teams reporting treatments per 10 million inhabitants, were computed for each country, without adjustments for patients who crossed borders or received treatment in a foreign country. Population numbers were obtained from the 2016 and 2017 Eurostat database (ec.europa.eu/eurostat) and then averaged for the 2 years.
Results
This report discloses the data of the surveys for the years 2016 and 2017 as a sum of both years, unless otherwise specified. For the purpose of comparison, previous data are also displayed in graphs as the sum for two adjacent years (2010/2011, 2012/2013, and 2014/2015).1–5
Participating teams and transplant rates
A total of 234 teams from 25 European countries and 4 EBMT-affiliated countries (i.e., Azerbaijan, Iran, Israel, and Saudia Arabia) responded to either or both the 2016 and 2017 survey editions. A total of 227 teams from these countries reported patient treatments by cellular or tissue-engineered therapies. Details of the indication, source and type of cells used, donor origin, processing, and delivery mode were provided by all the teams. No activity was reported by seven teams in either year. The Appendix A1 lists in alphabetical order of country, all the teams who reported their activity, in addition to the total number of treatments and the split between allogeneic and autologous donors. Group information about EBMT members was anonymized without the groups' consent for disclosure; otherwise, consenting EBMT groups are marked with EBMT CIC code.
The reported number of treated patients was higher in the 2016 and 2017 survey editions compared to previous years. Also, the number of reporting teams was increased in 2016/2017, after the previous decrease in 2014/2015. Over the last 8 years, the number of reporting teams thus increased by 30.4% (from 174 in 2010/2011), and the number of treated patients increased by 171.9% (from 3029 in 2010/2011) (Fig. 1A).

Figure 1B displays the average of transplants reported for 2016 and 2017 per 10 million inhabitants in the investigated countries. The highest transplant rates (i.e., >40 per 10 million population) were reported in (in decreasing order) Slovenia, Denmark, Spain, Turkey, Belgium, France, Iran, Italy, Lithuania, the Netherlands, Switzerland, Belarus, Israel, Germany, United Kingdom, and Ukraine.
Figure 1C displays the number of reporting teams in the investigated countries, normalized to the inhabitant numbers (Fig. 1C). The number of reporting teams per 10 million inhabitants, which was higher than 4 (in decreasing order), were in Slovenia, Switzerland, Denmark, Spain, Belgium, and the Netherlands. Data reported by the top 10 countries accounted for 88% of all treated patients.
Number of cellular or tissue-engineered therapies, disease indications, and donor type
Eight thousand two hundred thirty-six patients were reported to have been treated with cellular or tissue-engineered therapies in 2016 (4501) and 2017 (3735). Of these patients, 5033 (61%) were treated with autologous and 3203 (39%) with allogeneic cells (Table 1). Out of all treatments, musculoskeletal/rheumatological disorders (44%) were the most representative indications using autologous cells, followed by miscellaneous (26%) and hematology/oncology (20%) indications. Therapies within hematology/oncology predominantly used allogeneic cells (78%) (Fig. 2A).

Number of Reported Cell and Tissue-Engineered Therapy Treatments in Europe in 2017 and [2016] Sorted by Indication, Cell Source, and Donor Type
HPC, hematopoietic progenitor cells; MSC, mesenchymal stromal/stem cells.
Reported indications were hematology/oncology (predominantly prevention or treatment of Graft vs. Host Disease [GvHD], and hematopoietic graft enhancement) (40% of all reported patients; 25% of these treatments were based on autologous cells), musculoskeletal/rheumatological disorders (29%; 92% autologous), cardiovascular disorders (6%; 58% autologous), neurological disorders (4%; 56% autologous), gastrointestinal disorders (<1%; 71% autologous), and miscellaneous indications (20%; 90% autologous) (Fig. 2B). Subtype indications classified as “other” with corresponding patient numbers can be found in Supplementary Table S2.
The use of allogeneic cells clearly increased for the treatment of cardiovascular and neurological indications, compared to the previous double years. Instead, a larger number of patients were treated with autologous cells for the miscellaneous indications, as well as gastrointestinal indications, despite a strong deviation for the years 2014/2015. For musculoskeletal/rheumatological and hematology/oncology indications, the percentages were relatively stable over the years (Fig. 2B).
Cell type and source
In descending order of frequency, used cell types were mesenchymal stem/stromal cells (MSC) (56%), hematopoietic stem and progenitors (HPC) (21%), keratinocytes (7%), chondrocytes (6%), dermal fibroblasts (4%), dendritic cells (2%), and others (4%) (Table 1). Source of MSCs was bone marrow (55%), fat tissue (20%), placenta/amniotic membrane (12%), cord blood (10%), and others (3%), which included Wharton's jelly and endometrium (Supplementary Fig. S1A). Furthermore, 68% of autologous MSCs were used for musculoskeletal/rheumatological indications and 73% of allogenic MSCs for hematological/oncological malignancies. The source of HPC was mainly confined to peripheral blood (82%), followed by bone marrow (13%), cord blood (< 1%), and other sources (5%), which were not explicitly declared (Supplementary Fig. S1B).
The types of “other” cells in the received forms are reported as cardiac stem cells, cardiovascular progenitors, endothelial cells, gingival fibroblasts, limbal epithelial stem cells, melanocytes, muscle cells, neural crest stem/progenitor cells, embryonic neural stem cells, and pancreatic islet-derived cells. Indications and patient numbers treated with the “other” cells can be found in “A” in Supplementary Table S3. Future surveys will be adapted accordingly if specific “other” cell sources are regularly reported over the years.
In some instances, patients were treated with more than one cell source. These patients were categorized in the survey under the provided primary cell source. Combined cell types were MSCs with chondrocytes, muscle cells, or osteoprogenitor and endothelial cells. In other instances, melanocytes, fibroblasts (autologous as well as allogenic), or limbal epithelial stem cells were additional cell sources in combination with keratinocytes (“B” in Supplementary Table S3).
Cell processing
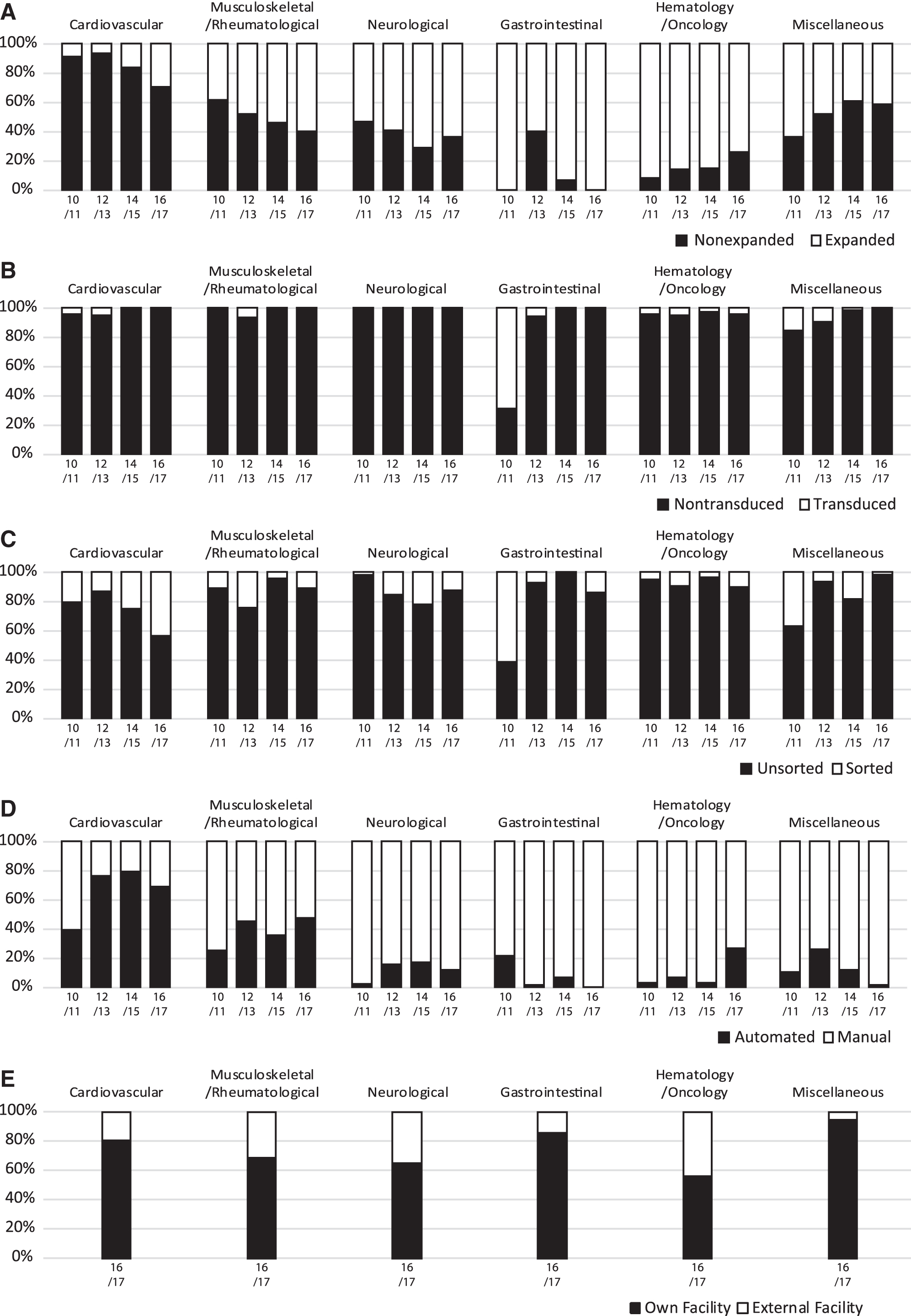
Cells were expanded in 62% of the overall reported treatments (Supplementary Table S4). When comparing with previous years, cells were more frequently expanded for the treatment of cardiovascular, musculoskeletal/rheumatological, and gastrointestinal indications. Conversely, the usage of expanded cells decreased for hematology/oncology and miscellaneous indications (Fig. 3A).
Comparative analysis of indications for cell and tissue-engineered therapies in Europe for the combined years of 2016 and 2017, sorted by mode of processing
Most treatments were based on nontransduced (98%) and unsorted (89%) cells (Supplementary Table S4). Although transduced cells were employed for various indications between 2010–2013, they have been reduced to only being used for hematology/oncology indications in following years (Fig. 3B). On the other hand, the sorting of cells has been a part of cell processing in a subset of all indication categories. Cell sorting for cardiovascular indications appears to be establishing itself as it has steadily increased over the last 6 years. However, no other apparent trend could be determined, as the percentage of patients treated with sorted cells fluctuated over the years in the other indication groups (Fig. 3C).
Cells were manually processed for 89% of the treatments. The majority of therapies with automated cell processing are found for cardiovascular (373 patients), musculoskeletal/rheumatological (1143 patients), and hematology/oncology (928 patients) indications (Supplementary Table S4). In the instance of cardiovascular and musculoskeletal indications, the percentages of the patients who were treated with automated processed cells in the last 6 years were higher than 60% and 35%, respectively. Otherwise, <30% of the remaining indications were treated with manually processed cells (Fig. 3D).
As the sector of cellular and tissue-engineered therapies evolves and prospers, it is also becoming commercialized. There are >230 companies providing services for regenerative medicine and advanced therapies in Europe and Israel. 10 As we consider this outsourcing of cell processing an important development in the field, we have expanded the survey to include whether cells were processed in the team's own facility or an external facility. External facilities performed 30% of the cell processing for the combined years 2016/2017 (Supplementary Table S4). The processing of cells for musculoskeletal/rheumatological and hematology/oncology indications were the primary contributors, as they not only have the most patients (2402 and 2509, respectively) but also have the highest percentage of external facility processing (31%, and 43%, respectively) (Fig. 3E). As this is the first time that we have followed up on the production facility, neither trends nor predictions could be determined.
Delivery mode
In 2016/2017, 47% of the treatments were based on intravenous (i.v.) or intra-arterial (i.a.) delivery. The remainder 53%, delivered intraorgan, were based on injection of cell suspension (36%), use of a membrane/scaffold (16%), and use of a gel (<1%) (Supplementary Table S5).
Therapies for cardiovascular, musculoskeletal/rheumatological, and miscellaneous indications used all four modes of delivery, whereas those for neurological, gastrointestinal, and hematology/oncology indications administered cells either by i.v./i.a. or in suspension intraorgan (Fig. 4). Interestingly, in the last 4 years, the intraorgan injection of cell suspensions has become the dominant means of cell delivery for the miscellaneous indications. When comparing with the previous years, indications for musculoskeletal/rheumatological, neurological, and hematology/oncology have maintained similar percentages of the different modalities of cell delivery. In contrast, cardiovascular indications have been treated with cells delivered in variable ways and—since 2016/2017 for the first time—also in combination with a gel (Fig. 4).

Comparative analysis of indications for cell and tissue-engineered therapies in Europe for the combined years of 2016 and 2017, sorted by delivery mode. Data used for this chart were derived from this study, and five previous reports (1–5). i.v. or i.a., intravenous or intra-arterial.
Clinical procedure
As cellular and tissue-engineered therapies advance, they may move from single case studies and clinical trials to routine therapies. For the surveys of 2016 and 2017, a query to the practitioners was included about the context in which the therapies were offered to the patients. In 2016/2017, cellular and tissue-engineered therapies for cardiovascular, neurological, and gastrointestinal indications were predominantly proposed as clinical trials and case studies. Nonetheless, few procedures for cardiovascular (peripheral artery disease) and neurological (multiple sclerosis and stiff person syndrome) indications were reported as routine therapies.
Surprisingly, the majority of musculoskeletal/rheumatological (orthopedic cartilage repair, arthritis, intervertebral disc degeneration, tendon/ligament, bone repair, scleroderma, periodontal tissue repair, pump syndrome, and femoroacetabular impingement, fibromyalgia, as well as reconstructive surgery/tissue enhancement), hematology/oncology (GvHD and HSC graft enhancement), and miscellaneous (adrenoleukodystrophy, autoimmune disease, bone marrow aplasia, Epstein–Barr virus, Histiocytosis X, infection, necrobiotic xanthogranuloma, primary immune deficiency, relapsing cytomegalovirus reactivation, sickle cell disease, vasculitis, and skin—aging, facial deformities, and vitiligo) indications were reported as routine therapy offers (Fig. 5 and Supplementary Table S6).
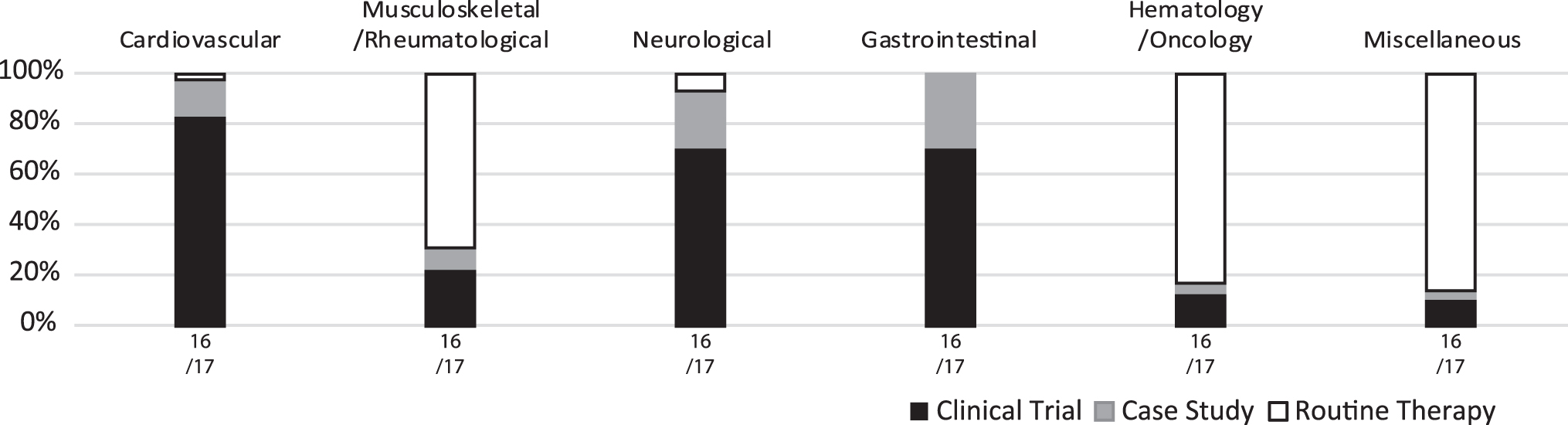
Comparative analysis of indications for cell and tissue-engineered therapies in Europe for the combined years of 2016 and 2017, sorted by clinical procedure.
Detailed analysis of treatments for musculoskeletal/rheumatological disorders
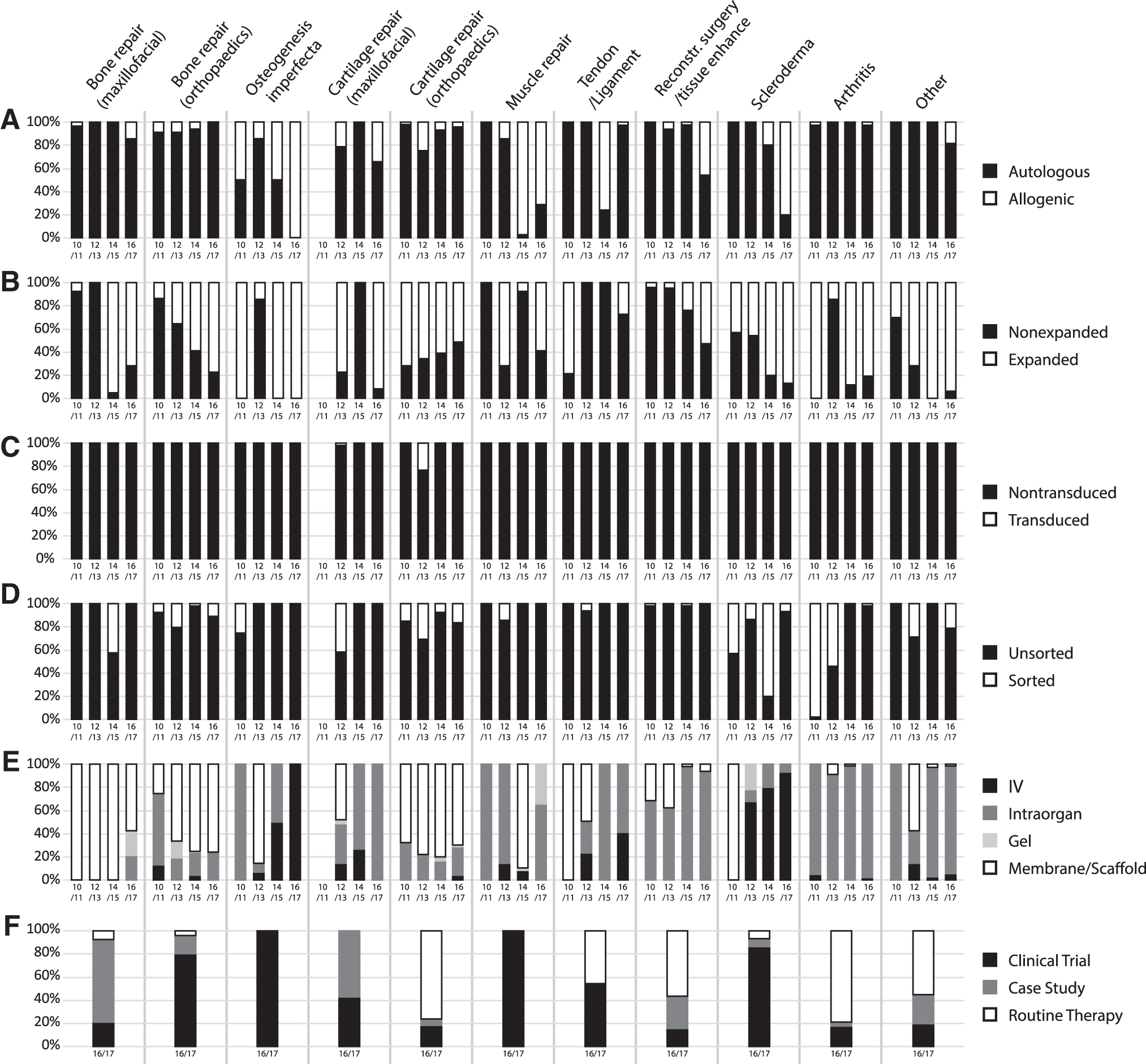
This edition of the survey reports more detailed data in the specific context of musculoskeletal/rheumatological disorders. The most commonly used cell sources for these applications were autologous cells (92%), predominantly derived from either bone marrow aspirate or fat tissue. Allogenic cells were used in >20% of the treatments for osteogenesis imperfecta, maxillofacial cartilage or muscle repair, reconstructive surgery and tissue enhancement, or scleroderma (Fig. 6A).
Comparative analysis for cell and tissue-engineered therapies in Europe of musculoskeletal/rheumatological subindications from 2010 to 2017 for two consecutive years, sorted by mode of processing
Cells were expanded in vitro in some applications, which would likely lead to a higher proportion of progenitor cells. This report documents an extensive use (>50%) of expanded cells for the treatment of bone, cartilage or muscle repair, osteogenesis imperfecta, arthritis, reconstructive surgery and tissue enhancement, and scleroderma, as well as the other indications not explicitly listed (Fig. 6B).
Transduction of cells was only reported in rare cases for cartilage repair in the last 8 years (Fig. 6C). Sorting for a specific population was only performed in ∼10% of orthopedic bone and cartilage repair, as well as the other categories (Fig. 6D). However, even in these applications using expanded cells, cell sorting to isolate and concentrate progenitor/stem cells was rarely used.
The vast majority of cell therapy applications for orthopedic indications involved either local injection or direct cell implantation at the time of surgery, with systemic administration used uncommonly in most indications, with the exception of osteogenesis imperfecta and scleroderma (Fig. 6E). Local cell delivery was sometimes done with a “carrier vehicle,” such as a collagen membrane scaffold or injectable materials (gels), mainly used in bone repair, orthopedic cartilage repair, and muscle repair (Fig. 6E). These carrier vehicles may well affect cell behavior, so further studies are required to understand the effect of such materials on different cell types. Based on cell- and material-specific findings, the manufactured grafts could be classified from a regulatory standpoint as possible “combination products.”
Interestingly, >40% of treatments in the areas of cartilage repair, tendon/ligament, reconstructive surgery, arthritis, and other were offered as a routine therapy (Fig. 6F).
Discussion
Since 2010, the collected data have continuously increased with regard to both participating teams and patient numbers. As more clinical groups and treatments are collected, the report may provide useful data in capturing trends and innovations in the field. In this report, data of two consecutive year surveys were summed together to allow a more compact presentation, as well as to try and make trends and predictions more apparent, by reducing the impact of transient fluctuations.
Cell-based and tissue-engineered therapies for applications in the areas listed in this survey hold a great deal of promise, but these procedures are not without risk.11,12 As noted in this survey, the majority of procedures utilized autologous cells, but the use of allogeneic cells appears to be increasing in certain areas (Fig. 2B), despite the fact that they present the risk of transmission of disease from a donor to a recipient. However, this change seems to reflect the perception that use of autologous cells is often not an achievable business model in comparison with allogeneic cells, which could be “used off the shelf.”13,14
In a perfect world, it would be most expeditious to be able to isolate autologous cells from an appropriate tissue source for a specific treatment based on their cell surface phenotype or other sentinel marker of cell identity or function, and to use these cells directly without ex vivo manipulation. However, cell products for tissue regeneration other than for bone marrow transplantation generally require ex vivo expansion due to the rarity of stem/progenitor cells within a given tissue, and the need for large numbers of cells to regenerate 2D and 3D tissues.
It is well known that ex vivo manipulation can change the character of a given cell population, and maintaining their initial biological activity is imperative. Furthermore, ex vivo expansion and prolonged periods of tissue construction provide the opportunity for microbial and viral contamination of the cell product or tissue, or even unintended expansion of unwanted cell types. 12 Beyond the risks of cell processing and tissue construction, how a cell population or a reconstructed tissue is to be delivered is a major consideration, given the importance of cell and tissue interactions with a potential carrier. Furthermore, the in vivo environment, can be very hostile and may not contain the necessary nutritional and cell-signaling factors required for optimal cell differentiation and function. Biocompatibility and level of toxicity have a high impact on potential success.
Following are some remarks related to specific findings in the area of musculoskeletal and rheumatological treatments, as a starting point for more general observations. Most musculoskeletal tissues, including cartilage, ligament, tendon, meniscus, muscle, and even bone, in case of certain critical conditions, have limited healing potential. Cell therapy and tissue engineering approaches, therefore, hold great promise for the treatment of various musculoskeletal tissues, as evidenced by the finding that 29% of the indications in this survey were for musculoskeletal/rheumatological disorders.
The most commonly used cell sources for these applications were of autologous origin, delivered without being transduced or sorted, and thus bypassing several regulatory challenges associated with extensive manipulation. Interestingly, for bone repair, there was a clear trend over time toward using expanded cells (Fig. 6B), possibly due to the recognition that the amount of tissue-resident cells available intraoperatively (e.g., within bone marrow or fat tissue) may not be sufficient to enhance processes of compromised bone regeneration. Conversely, the use of nonexpanded cells has gained popularity for cartilage repair, likely associated with the trend of combining intraoperatively available chondrocytes with an accessory fraction of stromal cells. 15
The combination of the perceived safety of autologous cells, the inherently poor healing capacity of various musculoskeletal tissues, and the current lack of effective therapies for treatment of difficult clinical problems such as osteoarthritis, chronic tendinopathy, and meniscus injury has provided the “perfect storm” leading to the often indiscriminate use of unproven cellular therapies.
It is notable that the majority of treatments (69%) reported for musculoskeletal/rheumatological disorders and diseases were offered outside the context of a clinical study and considered to constitute of “routine” clinical care. This was particularly dominant in cartilage repair, reconstructive surgery and tissue enhancement, arthritis, and the other group (Fig. 6F). While these treatments were performed within the context of legitimate treatment centers, it has to be highlighted that in none of these areas, we can find scientific evidences of verified clinical effectiveness, which would justify their broad adoption outside the framework of clinical study cohorts.
More generally, the use of cell therapies without proper scientific rationale, reasonable preclinical data, and approval by appropriate regulatory bodies has contributed to the explosion of unauthorized clinics around the world, including in Europe. It is now recognized by many that such clinics are not providing treatments approved by regulatory bodies and present real risks to unsuspecting patients who pay considerable sums of money for such unauthorized treatments.
There are several examples in the United States, where patients were treated directly with poorly characterized fat aspirates and developed blindness. 16 In another report, at least a dozen patients received contaminated umbilical cord “stem cells” for treatment of a variety of diseases and disorders, leading to their hospitalization, some for extended periods of time, 17 and it is very likely that such adverse effects have occurred worldwide.
In conclusion, it is clear that cell therapy holds tremendous potential for healing and regeneration, but realizing this potential will require carefully planned clinical trials. Progress in this field will only be achieved by the initiation of multicenter studies, possibly employing clinical registries and biospecimen repositories, which would allow the ability to correlate the composition and biologic activity of the cell formulation with the clinical effectiveness. Rigorous basic and preclinical studies, along with well-controlled and well-designed clinical trials that measure appropriate outcomes, will pave the way to making cell-based therapy and tissue engineering an effective clinical reality. In this perspective, the here described survey represents a relevant instrument to gain transparency and capture trends in a variety of diverse clinical areas.
Footnotes
Acknowledgments
We would like to acknowledge contribution by all teams participating in the survey, and their staff (listed in the Appendix A1). We are grateful to the Orthoregeneration Network (ON) for offering visibility to the program through their website (![]() ). We thank Silvia Lopa for her assistance in the head hunting of treating groups.
). We thank Silvia Lopa for her assistance in the head hunting of treating groups.
Disclosure Statement
No competing financial interests exist.
Funding Information
Supported by the different international societies and their highly committed representatives, namely ISCT-Europe (Meagan Pasternak), TERMIS-EU (Sarah Wilburn), ICRS (Stephan Seiler), IFATS (Catherine B. Foss), and EBMT (Helen Baldomero).
Appendix A1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.