
Abstract
A few treatment options exist for patients experiencing xerostomia due to hyposalivation that occurs as a result of disease or injury to the gland. An opportunity for a permanent solution lies in the field of salivary gland replacement through tissue engineering. Recent success emboldens in the vision of producing a tissue-engineered salivary gland composed of differentiated salivary epithelial cells that are able to differentiate to form functional units that produce and deliver saliva to the oral cavity. This vision is augmented by advances in understanding cellular mechanisms that guide branching morphogenesis and salivary epithelial cell polarization in both acinar and ductal structures. Growth factors and other guidance cues introduced into engineered constructs help to develop a more complex glandular structure that seeks to mimic native salivary gland tissue. This review describes the separate epithelial phenotypes that make up the gland, and it describes their relationship with the other cell types such as nerve and vasculature that surround them. The review is organized around the links between the native components that form and contribute to various aspects of salivary gland development, structure, and function and how this information can drive the design of functional tissue-engineered constructs. In addition, we discuss the attributes of various biomaterials commonly used to drive function and form in engineered constructs. The review also contains a current description of the state-of-the-art of the field, including successes and challenges in creating materials for preclinical testing in animal models. The ability to integrate biomolecular cues in combination with a range of materials opens the door to the design of increasingly complex salivary gland structures that, once accomplished, can lead to breakthroughs in other fields of tissue engineering of epithelial-based exocrine glands or oral tissues.
Impact statement
Millions of people worldwide suffer from xerostomia/dry mouth owing to hyposalivation from disease, injury, or aging. Loss of saliva impairs eating, swallowing and leads to oral disease. Tissue engineering of salivary glands using primary adult stem/progenitor cell populations encapsulated in customized hydrogels offers a permanent solution. New materials are being developed to provide cues to encourage salivary cells to organize into functional structures that resemble acini connected to functional, branched ductal networks. Once formed, it is envisioned that these salivary neotissues can be implanted to restore salivation and improve the quality of life for xerostomic patients.
Introduction
Salivary glands and the fluid saliva they produce enable chewing, swallowing, and speaking. Salivary components also provide the first barrier to prevent oral infections. Three major gland pairs, the parotid, submandibular, and sublingual along with ∼1000 minor glands in the oral mucosa, comprise the salivary system. When salivary glands are damaged, as often occurs in individuals undergoing radiation therapy for head and neck cancers1–3 or living with autoimmune diseases such as Sjögren's Syndrome4–6 or chronic graft-versus-host disease, 7 salivary output diminishes, a condition known as hyposalivation. Lack of saliva perceived as dry mouth, or xerostomia, is also induced by medications and aging8,9 and it negatively impacts an individual's quality of life and interferes with normal daily functions. 10
Xerostomic patients experience oral pain and have difficulty talking and swallowing (dysphagia). 11 Appetite suppression can lead to weight loss, and in some patients social marginalization can accompany declining oral health associated with diminished anti-microbial and innate immune responses that increase the risk of dental caries and oral diseases. 12 Currently, limited treatments exist for xerostomia 13 and sufferers are left with a few options to treat the symptoms of hyposalivation.
Common palliative treatments include use of oral rinses, aerosols, lozenges, gels, and chewing gum. Oral sialagogues, pilocarpine, and cevimeline13–17 are routinely prescribed; however, they rely on the existence of functional secretory units in the glands. Side effects and contraindications complicate the treatment schemes for some individuals with cardiovascular or pulmonary disease. 18 Unfortunately, the xerostomia that results from atrophy of salivary secretory units renders these drugs largely ineffective.2,19 The lack of effective treatments creates a clinical need for a permanent solution that could be achieved by replacing or augmenting salivary gland functions through use of tissue engineering approaches.
Despite several decades of work, beginning with the pioneering approaches developed by Dr. Baum, 20 the long-sought goal of controlling and building a fully formed and functioning replacement salivary gland remains elusive. Recent advances have successfully isolated and expanded specific subpopulations of human stem/progenitor cells (hS/PCs) found in the resected salivary glands of nonradiated surgical patients.21–24 By exploring parallels between developmental biology and tissue regeneration, approaches have been developed to coach these hS/PCs to develop differentiated properties of saliva-producing neotissues in vitro.25–27 Researchers have systematically examined the nature of the ideal biomaterial in which to grow the three-dimensional (3D) neotissues28–30 and considered which encapsulated cell type(s), ranging from stem/progenitor to partially differentiated to fully differentiated neo-organs, would provide the optimal implant material.31–34
This review briefly describes the biology and structure of each of the major cell types in the salivary gland followed by current strategies to engineer that cell with a focus on function and form. Current approaches to develop salivary gland functional units and their ability to stimulate salivary flow on implantation in animal models are also discussed. Other potential applications of these techniques beyond regenerating the salivary gland, including the development of new ex vivo models to mimic salivary gland dysfunction and disorders, conclude this review.
Salivary Gland Structure, Development, and Function
The major salivary glands consist of a network of branching ducts that terminate into secretory acini, which can be serous, mucous, or mixed. 35 Connected to the acinar structures are hollow tubes made from ductal cells that transport and modify the saliva as it flows from the secretory acini, through the ducts and into the oral cavity. 36 Contractile myoepithelial cells surround the acinar bulbs that are connected to the ductal network and are assumed to be associated with salivary secretion. 37 Underlying epithelial cells in both acini and ducts is a basement membrane, which, in addition to providing structural support and separating epithelium from stroma, creates a contiguous capsule around the gland that extends inward to create lobules. 35 Lying juxtaposed to the basement membrane in the nearby stroma, salivary glands are supplied richly with blood vessels and are innervated by the parasympathetic and sympathetic nervous systems. 35 Together, these structures assist in the production of ∼1.5 L of saliva daily,38,39 the vast majority of which is produced during the waking hours.40,41
During development, the salivary gland begins with a single invaginated bud that undergoes repeated branching, a process called branching morphogenesis.42,43 Once formed, the invaginated bud invades the underlying collagen-rich mesenchyme tissue. 44 Next, cleft formation begins wherein fibronectin-containing indentations 45 appear and deepen to initiate branching. 42 The single bud then undergoes cycles of proliferation and outgrowth and propagates progressively to form a more complex branched structure. 45 Many of the cues involved in initiating and perpetuating the branching morphogenesis process are provided by the mesenchyme, extracellular matrix (ECM), and later cues from the nervous system.42,44,46 Removal of the parasympathetic submandibular ganglion dramatically decreases the extent of branching morphogenesis that is observed. 47
Salivary Gland Function Versus Form in Tissue Replacement
The structural complexity of salivary glands makes them more difficult to build than more homogeneous tissues such as cartilage. Major salivary glands contain sophisticated networks of ducts originating at secretory acini and ending in the oral cavity (Fig. 1A). All three major epithelial cell types, acinar, ductal, and myoepithelial, uniquely contribute to saliva production. 35 Without acinar cells, the salivary gland cannot produce salivary components or transport water. 48 Without contractile myoepithelial cells, saliva does not move effectively into the collecting ducts. 37 Without ductal cells, saliva lacks the right consistency and does not contain the appropriate osmolarity and concentration of ions: sodium, potassium, and bicarbonate. 48 The acinar cell composition in the gland determines whether the saliva is watery or mucous-like. 49 The ductal system actively changes the ion composition and volume of the saliva by electrolyte transport mechanisms. 50 The labyrinth of ducts is much more difficult to build than a straight tube such as a trachea. 51

Composite diagram of a salivary gland and two generations of patented tissue-engineered replacements.
From a functional standpoint, individual salivary units must be sealed and organized correctly to ensure that saliva flows directionally from the acinar cells into the ductal system where the saliva can be altered, and then on to bathe the oral cavity. Fluid flow must occur without tissue spillage. An unorganized, leaky structure or structures that lack functional polarity cannot provide the correct flow for saliva. Saliva that fails to reach the oral cavity could accumulate in tissue, pool, and form cysts.52,53
Any tissue engineering strategy to replace the gland must ensure that differentiated cells in neotissues work together to provide and transport saliva that can lubricate the oral cavity, solubilize and digest food, and protect the mouth from oral disease. It can be debated whether these goals can be accomplished without exact replication of the structure of the native gland, as was the case for the patented “blind end tube” model, 54 which is a much simpler model than that in our patented branched design 55 (Fig. 1B, C). We here will discuss approaches in which the engineered neotissue seeks to mimic native salivary tissue structure as much as possible, but we acknowledge that other strategies could employ designs that might differ substantially from the native gland.
ECM Instructs Salivary Gland Form and Function
The ECM plays both structural and instructive roles in salivary gland morphogenesis, differentiation, and function. 43 Key matrices include the basement membrane, filtering transport between epithelium and stroma, and the stromal matrix, where fibroblasts, nerve cells, and blood vessels provide water, nutrients, growth factors, and signaling molecules to salivary epithelial cells.43,56 The ECM components present in the salivary gland include heparan sulfate (HS) proteoglycans such as perlecan/HSPG2, 57 collagen IV, 58 and laminin 43 present in the basement membranes' underlying ducts and individual acini, and fibronectin and collagen I in the interstitial matrix. 45 Forming contiguous specialized networks containing precisely organized macromolecules, these matrix components both initiate and control the continuation of branching morphogenesis during development.43,59–61
The stromal ECM interacts directly with the basement membrane to provide organizational cues through interactions with integrins on salivary epithelial cells.62,63 We recently reported that the α1β1-integrin, in particular, establishes a human salivary gland coordinated structure and function, and that its activation in tissue-engineered systems is essential to tissue assembly. 64 In addition, for salivary gland branching morphogenesis to occur, the ECM must be extensively remodeled by matrix metalloproteinase (MMP) cleavage. 58
In tissue engineering applications, the ECM both establishes and maintains cellular phenotype and function throughout the duration of culture. 57 Therefore, during hydrogel design, it is critical that material composition reproduces native interactions between cells and ECM to specify a program that supports branching morphogenesis and achieves cellular polarity. Typically, the ECM used in tissue engineering models is the hydrogel in which the salivary structure is grown, which de facto serves as the initial connective tissue not unlike the invaginating bud seen during development.29,60,65,66
Given the importance of the ECM in initiating and perpetuating branching morphogenesis, a major research effort has focused on determining the appropriate physical and chemical cues needed to allow for branching to occur. Studies in two-dimensional (2D), 2.5D (monolayers on 3D substrates), and 3D all have sought to reorganize salivary structures with a proper orientation.21,26,29,61,67–69 Common gel compositions used as a primary matrix for salivary gland regeneration are Matrigel®, 33 hyaluronic acid (HA),64,70,71 collagen type I, 72 fibrin, 68 enzymatically degradable poly(ethylene)glycol (PEG)-based hydrogels, 28 as well as scaffolds using silk73,74 or poly(lactic-co-glycolic acid) (PLGA)75,76 (Table 1).
Matrices for Salivary Gland Tissue Engineering
2D, two-dimensional; HA, hyaluronic acid; PEG, poly(ethylene)glycol; PLGA, poly(lactic-co-glycolic acid); ECM, extracellular matrix.
Some of these gels, including Matrigel®, collagen, and fibrin gels, are isolated from animal tissues or include bound growth factors that could be tumorigenic or immunogenic, thus preventing their use in humans.77–79 HA is a glycosaminoglycan that lacks a protein component, is highly biocompatible, and does not trigger an immune response71,80; thus, it is increasingly used as an implant material.81,82 Likewise, an increased interest in synthetic biocompatible materials is emerging. Both HA and synthetic materials offer the advantage that they are readily modifiable, allowing for the addition of instructive peptides.29,70 The ability to “mine” the ECM for motifs that can be used to modify synthetic or native scaffolds for tissue engineering purposes was reviewed. 65
Strategies to Replicate the Native Gland: Apicobasal Polarity
Acinar cells are specialized secretory subtypes that can be either serous or mucous. 35 Serous cells are more conical shaped and produce watery secretions, whereas mucous cells are rounder with a larger central lumen, producing more viscous secretions. 36 Acinar cells exhibit an apicobasal polarity with basement membrane proteins, including laminin, collagen type IV perlecan, and nidogen localized to the basal portion of the cell. 43 Tight junction proteins such as occludins and claudins are localized to the lateral sides of each cell where they seal and form a barrier to the movement of large solutes between the apical/luminal and basal/stromal sides, 83 ensuring no “back flow” of proteins secreted in saliva. Aquaporins appear on the apical side of acinar cells where they assist in water flow into saliva. Acinar cells form spheroid clusters (∼50 μm in diameter)64,80 that develop a collecting lumen directly connected to intercalated ductal cells.80,84 Unlike the hollow round lumen in the ducts, the acinar lumen is irregular in shape and resembles the shape of a “chicken foot” when collapsed. Common markers used to identify salivary acinar cells are the transcription factor MIST1/BHLHA15 and α-amylase. 70
Establishing apicobasal polarity in hydrogels
Obtaining polarized cells with proper apical-basolateral positioning is critical to engineer a gland that is able to produce saliva. Common apical markers used to identify polarized cells are transmembrane member 16a (TMEM16A/chloride transporter) and aquaporin 5 (AQP5).85,86 Basolateral markers include Na–K–Cl cotransporter protein (NKCC1) and β1 integrin. 64 Stable lateral junctions typically are identified by expression of tight junction protein 1 zona occludens-1 (ZO-1). 87 Human submandibular gland cells grown in 3D in Matrigel® expressed tight junction proteins ZO-1, claudins1–5, and occludin suggesting that the components of Matrigel® that include basement membrane proteins laminin, collagen type IV, perlecan, and nidogen are needed to establish acinar polarity. 88
Similarly, many hydrogels containing some components of the basement membrane ECM trigger expression of one or more tight junction proteins.26,89,90 Our group found that encapsulation of hS/PCs in HA-based hydrogels containing a peptide from perlecan domain IV readily reorganized, expressed ZO-1, underwent acinar differentiation, and formed lumens.26,57 These hydrogels also allowed the acinar cells to express AQP5. Another biocompatible hydrogel type being investigated is fibrin, but encapsulated cells thus far have shown limited polarity even when polymerized with growth factors. 68
Cellularized silk/chitosan scaffolds also provide conditions for improved cellular differentiation as well as mechanical properties for a cyclic loading environment.74,91 Other groups have found success in obtaining polarized cell types with synthetic hydrogels made from PEG28,92 or PLGA. 76 These hydrogels are especially successful in driving correct localization of NKCC1, ZO-1, and AQP5 when combined with MMP-cleavable sequences. 28 Enzymatically degradable sequences inserted in hydrogels allow the salivary gland cells to undergo dynamic morphogenesis as they grow, proliferate, and polarize by clearing a path in the hydrogel. 93 MMPs, specifically, are expressed by salivary glands and are important in remodeling of the mesenchyme during development.58,94
Can acinar cells form lumens in 3D?
Once acinar spheres are polarized, the next step is to induce lumen formation to allow for collection and passage of saliva. Matrigel®, containing key components of basement membranes including laminin, has provided insights into factors needed to support lumen formation.33,34 When salivary cells were encapsulated in Matrigel®, apoptosis was observed at the center of the spherical clusters, which resulted in “donut” formation indicating the beginning of a forming lumen. 33
Biocompatible fibrin hydrogels conjugated to laminin-derived L1 peptides induced actin reorganization and lumen formation seen through F-actin staining. 68 HA hydrogels containing recombinant perlecan domain IV showed similar central apoptosis, indicating the start of a lumen. 26 These lumen-containing structures, however, were not sealed. Treatment of these structures with neurotransmitters triggers “dumping” of amylase-containing vesicles; however, these vesicles surround the structure in the hydrogel rather than entering the central lumen. 23 As will be discussed further later, it now appears that although acinar spheroids in the proper hydrogel matrix will form a spheroid structure with lumens, full maturation to polarized, sealed acini able to vectorially secrete salivary components into a central collecting lumen requires neural cell input, and perhaps myoepithelial cell input.
How is acinar function measured?
Acinar cells in salivary glands have a specific function: to generate saliva. Saliva production by cultured cells in the lab is often measured by assaying release of α-amylase. Many hydrogel formulations, including Matrigel®,34,88 HA,23,70 and enzymatically degradable PEG-hydrogels, 28 can support acinar production of α-amylase. In addition, functional responses are also assessed by measuring calcium oscillations that occur on stimulation from β-adrenergic or muscarinic neurotransmitters such as carbachol or acetylcholine, respectively.95,96 Our lab has shown that acinar-like cells in HA gels produce calcium oscillations when stimulated with neurotransmitters, demonstrating the potential for activation of a fluid path. 23 In both small and large animal models, direct cannulation of salivary ducts is used to measure rates of fluid output.97,98
Integrative challenges in producing replacement saliva
One difficulty in tissue engineering is the repopulation and regeneration of salivary acinar cells. In native tissue, acinar cells are likely repopulated through self-duplication, 99 but ex vivo acinar cell proliferation and maintenance has been difficult to achieve to date.22,100 One potential solution has been to modify the substrate or hydrogels in which acinar cells are grown or encapsulated.
Once the ECM's role in maintaining acinar cell proliferation was discovered, this challenge was partially overcome.66,101 MMP-cleavable hydrogels are among the most successful in allowing acinar cells to retain their phenotype, proliferate, and acquire function. 28 However, acinar cells often lose their polarity and phenotype in long-term culture, marked by a reduction in the levels of the acinar cell marker MIST1 and the transporter AQP5. 92 Recent evidence suggests that acinar cell markers are downregulated when acinar cells undergo cellular stress or injury perhaps shedding some light on this loss phenomenon. 69
Work is ongoing to identify cues and molecular pathways that encourage acinar cells to regenerate. 102 Because acinar cells are the most sensitive of all salivary cells to delayed radiation loss, 103 it may be that common pathways account for both loss and regain of function. Replacement of secretory cells in mouse models has been reported to require SOX2. 104 Proliferation of SOX2-positive cells can be stimulated with acetylcholine, suggesting that acinar cell expression also can be controlled by the incorporation of neural signals. 102 Studies that seek to understand the mechanisms that foster branching morphogenesis have highlighted a role for the nervous system in inducing and maintaining acinar polarity.46,105 Building a detailed understanding of these interactions such that they can be duplicated for tissue engineering purposes requires the development of biomimetic model hydrogel systems in which multiple cell types, including acinar cells and nerve, can be co-cultured.
Strategies to Replicate the Native Gland: Ductal Networks
Three types of interconnected ducts exist in salivary glands. From smallest to largest, they are intercalated, granulated/striated, and excretory. 35 These three ductal types modify saliva composition as it collects and flows from the intercalated ducts, through the striated and out of the excretory duct and into the oral cavity. 106 The intercalated ducts collect saliva from the acini and consist of cuboidal epithelial cells that are involved in absorption and secretion of ions. 107 Resident stem cell populations have been mapped to the intercalated ducts to replenish acinar, myoepithelial, and ductal cells in the event of injury.108,109
The striated ducts, such as the intercalated, are involved in the secretion and absorption of ions bidirectionally between the lumen and collagen-rich stromal ECM, where the blood vessels lie, to control the composition of saliva. 106 Ductal cells are columnar in shape, allowing for formation of a lumen toward which the apical surface faces. 49 Because the exchange of ions requires significant amounts of energy, ductal cells possess numerous mitochondria. 110
The functional role, beyond saliva transport, of excretory ducts and their ability to modify saliva remains poorly understood. Because excretory ducts reside closest to the oral cavity where pathogenic agents can invade oral tissues, it is not surprising that immune cells such as macrophages and dendritic cells reside within or near to these excretory ducts where they support immune surveillance. 111 These cells also are lined on their apical surfaces by mucin-1112 that retards invasion of infectious agents into underlying tissue. 113
How is ductal structure replicated?
Most tissue engineering endeavors have focused on producing and maintaining acinar cells as they comprise the key secretory end buds that generate saliva. However, cultures of isolated salivary cells typically acquire a ductal character over time 69 and ductal cells are therefore not considered to be difficult to culture. Some groups use ductal-like cells for their tissue regeneration efforts, and, in fact, early efforts in gene therapy attempted to directly convert ductal cells into water-transporting acinar cells by transfecting them with aquaporin-1.33,88,114,115
Intercalated ducts
The cell line HSY resembles intercalated, cuboidal ductal cells and has been used to model these structures. 116 Interestingly, this cell line can express neural-like markers, suggesting that ductal cells may have originated from the neural crest. 117 HSG cells are another ductal epithelial cell line isolated from irradiated human salivary glands and have a cuboidal/conical shape. 118 When this cell line was co-cultured with the myoepithelial cell line HPA, ductal-like structures formed implying myoepithelial cells and intercalated duct cells provide cues to one another to form tubular structures. 118 HSG cells in culture on basement membrane proteins such as those found in Matrigel® have a tendency to differentiate into acinar-like cells. 89
Granulated/striated ducts
A few tissue engineering strategies have focused on culturing or maintaining this cell type. A reason for this is that granulated/striated ducts are found primarily in parotid and submandibular glands, and, depending on the source of the original cells, may not be present. 117 Further, this cell type is seen primarily in more advanced branching networks, which, thus far, have not been replicated in vitro.
Excretory ducts
Excretory ductal cell and intercalated ductal cells share many similarities, including fibroblast growth factor (FGF)-receptor2IIIb 119 and ΔN23-keratinocyte growth factor. 120 One method to isolate human submandibular gland cells resulted in an epithelial cell line with characteristics of excretory and intercalated ducts. 22 These two cell types often are not distinguished or are lumped together. A majority of early studies in tissue engineering used the HSG cell line.33,89,121–123 Initial studies using these cells grew them in monolayers, under which conditions they did not form tight junctions. 124
Controlling differentiation of ductal cells
Generally, when salivary gland tissue engineering strategies are deployed, care is made to distinguish between acinar and ductal cells and not necessarily to distinguish subtypes of ductal cells. Eventually, as lab-grown structures grow in complexity, it will be necessary to differentiate between specific ductal subtypes. As with the granulated and striated ducts, excretory ductal cell stalks are found closer to the oral cavity 107 at the end of branched lumens35,125 and thus have not been needed in the more rudimentary models that consist of acinar cells and perhaps some portion of a lumen/ductal cells.
Ductal cells are typically differentiated from salivary cells by expression of specific cytokeratins, primarily cytokeratin 19.126,127 A study utilizing PEG hydrogels found increased expression of ductal cell markers over time compared with acinar markers due to preferential ductal cell proliferation. 92 When MMP-cleavable peptides are added as cross-linkers, ductal cells remain at the outer edges of formed spheroids, indicating that PEG hydrogels with MMP-cleavable sites can support both ductal cells and acinar cells. 28 Up to now, however, a major research focus has been to culture acinar cells and monitor appearance of ductal cells, which can occur if acinar cells lose their acinar phenotype and transdifferentiate into ductal cells.
Efforts to grow neoglands from primary hS/PCs or their mouse equivalents have borrowed lessons from development to induce salivary spheroids or “salispheres” to branch.128–130 For instance, FGF10 seems to be necessary to promote ductal elongation. 131 As seen in Figure 2, both FGF7 and FGF10 are needed for branching morphogenesis in explants (Fig. 2A), whereas FGF10 in the presence of exogenesis HS/heparin (Hp) was more useful in engineered constructs with hS/PCs (Fig. 2B). Cell-seeded hydrogels with gradients of Hp-binding growth factors designed to drive cell differentiation and morphogenesis are now feasible. 61
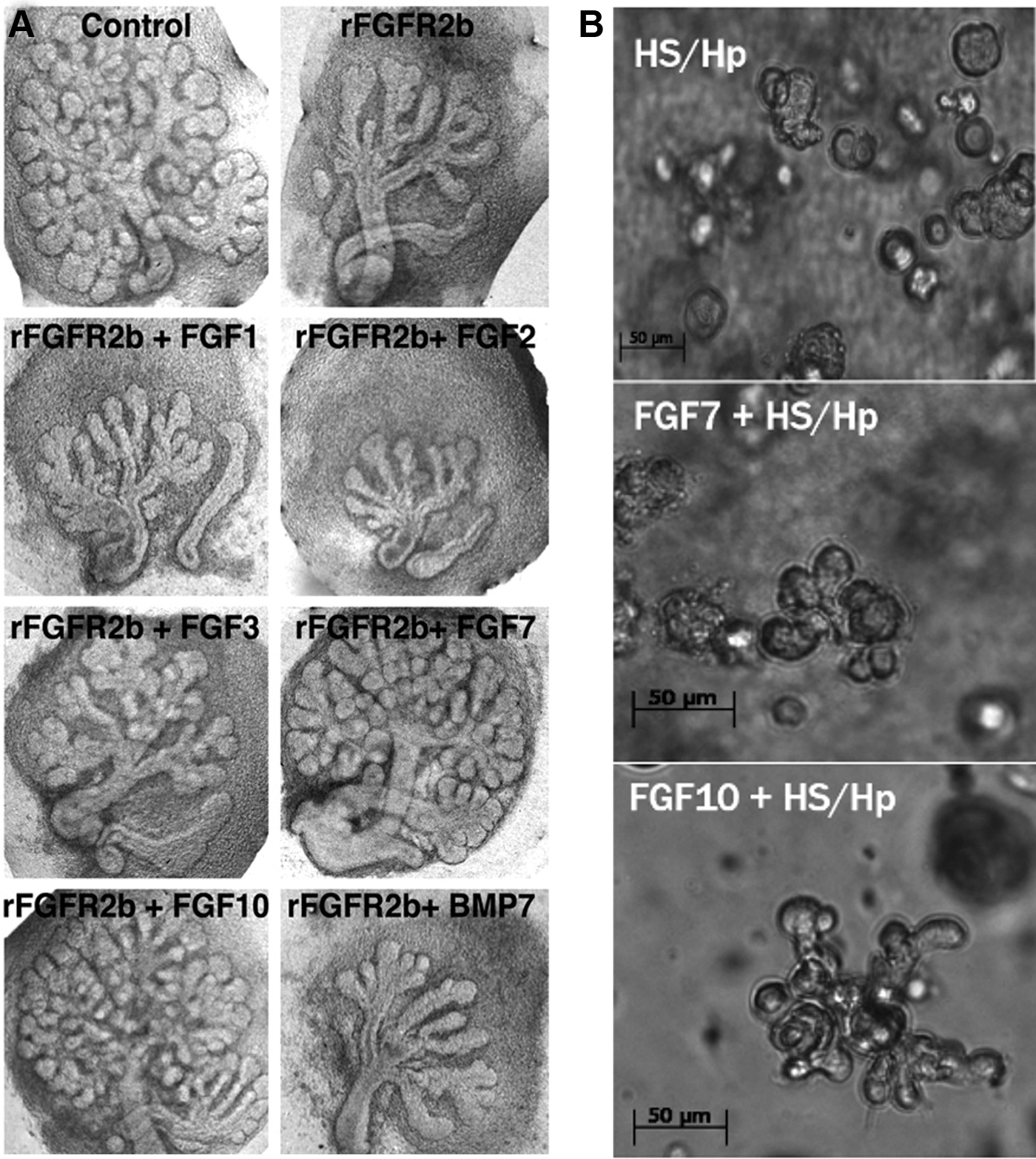
FGFs support branching morphogenesis in tissue explants and in 3D hydrogels.
How is function replicated?
Most of the studies examining functions of ductal cells have been performed in monolayers. HSY cells mimicking intercalated duct cells can secrete α-amylase. 116 The HSG cell line demonstrated the ability to assume an acinar-like phenotype and secrete α-amylase, 89 especially in the presence of ECM proteins. 123 These cells also can respond to neurotransmitters and produce calcium oscillations when grown in monolayers.121,122 Limited data exist on the ability of ductal cells to function in vitro and even less work has used 3D culture systems. Key areas for future work should consider two key aspects of ductal cell function: (1) basal and stimulated transport of water and salivary components directionally through an open lumen; and (2) modification of saliva composition to a minimally functional form that could lubricate the oral cavity and begin the digestion of food needed to restore taste and assist swallowing.
Integrative challenges in transporting replacement saliva
Achieving elongated and highly branched networks of ductal cells from hS/PCs is not yet possible. Adding additional cues from the ECM, other cell types or specific molecular signals such as myoepithelial cells, neural signals, or growth factors could assist in developing more highly branched ductal networks.42,43,128,132
Once formed, it is not clear how the ductal networks will be connected to the saliva-producing acinar cells to ensure unidirectional flow into the oral cavity. Direct ligation of a salivary bioengineered organ germ has been reported in mice, 133 but it is not clear how this will be achieved in humans. The buffering and functional capabilities of ductal cells acting on saliva can be assessed by directly studying its composition.134,135 To produce the minimally useful saliva formulation produced by an engineered gland, it may be necessary to focus on creating the ductal cell subtypes that are necessary to change the salivary composition. Saliva requires a specific viscosity, composition of small ions such as sodium, as well as the enzymes needed to break down food. 136 All these functions are a result of the three ductal subtypes as saliva moves from the acini and into the oral cavity. Producing highly branched, sealed, functional ductal networks remains a frontier in tissue engineering.
Strategies to Replicate the Native Gland: Myoepithelial Cells
Myoepithelial cells are star-shaped contractile cells that wrap around acinar cells and intercalated ducts to promote the movement of saliva out of the cells and into the ductal network. Myoepithelial cells are attached to the acinar and ductal cells by desmosomes and are surrounded by basement membrane. 137 Despite being associated with both acinar and ductal cells, myoepithelial cells are slightly different in shape depending on their location. On intercalated ducts, myoepithelial cells are smaller and more spindly, whereas on acinar cells they appear larger with thicker extensions. 138
Contraction of myoepithelial cells occurs from the nerves that innervate the gland. 139 Originally deriving from the epithelium, these cells help maintain acinar cell polarity and structure. 35 During development, myoepithelial cells secrete a majority of basement membrane proteins, helping to promote branching morphogenesis. 140 Although the primary role of myoepithelial cells is the expulsion of saliva from acinar cells and through the ductal network, recently they have been found to have additional functions, including, perhaps, polarization of acini. 37 In mammary tissue, myoepithelial cells appear to have a tumor-suppressive role. 141
How is myoepithelial structure replicated?
Human salivary myoepithelial cells (hSMECs) can be isolated from primary tissues and cultured in vitro. 142 Human salivary tissue must first be minced and incubated with collagenase I for 20 min before size exclusion centrifugation by using a cell strainer and hSMECs require different media components than hS/PCs acinar and ductal cells. 142 Isolated hSMECs can then be cocultured with hS/PCs to wrap around hS/PC clusters mimicking native tissue. Because of their similarity to smooth muscle tissue, myoepithelial cells can be identified by their expression of α-smooth muscle actin, smooth muscle myosin heavy chain, and cytokeratin 14 (K14). 37 hSMECS maintained these phenotypic markers when cultured in HA-based hydrogels and express β2-adrenergic and muscarinic receptors in 2D and 3D culture. 142 hSMECs also can be cultured with hS/PC spheroids in microwells where they wrap around and envelop the spheroids to replicate the native structures. 142 When encapsulated in HA hydrogels, such structures maintained their phenotype without stimulation of neurotransmitters for up to 48 h.
How is function replicated?
The function of myoepithelial cells is to respond to neurotransmitters and apply contractile forces to acinar and ductal cells during fluid flow. 37 Given the ability of myoepithelial cells to express neurotransmitter receptors when cultured in 2D, experiments were performed to determine whether these cells could be stimulated by neurotransmitter agonists. 142 On stimulation with carbachol, myoepithelial cells exhibited calcium spikes and oscillations, indicating a functional capacity to respond to neuronal signals. 142 When plated in collagen hydrogels, myoepithelial cells viewed by fluorescent imaging demonstrated the ability to spread throughout the gel, and to contract the surrounding hydrogel. Further, when myoepithelial cells were co-cultured with hS/PC spheroids produced in microwells and encapsulated in HA hydrogels, the myoepithelial cells “wrapped” the spheroids and retained the ability to respond to neuronal signals. 142
Integrative challenges using myoepithelial cells
To date, a few studies have utilized myoepithelial cells cultured in vitro. One reason for this is that typical yield from tissue is low, and our experience is that expansion of this cell population without dedifferentiation is difficult. 142 Initially, these cells were difficult to identify and previous markers such as S-100 were found not to be specific for myoepithelial cells. 118 Studies seeking to understand the molecular cues that give rise to branching morphogenesis recently have begun to examine the role of myoepithelial cells in branching.143–145 With this new understanding, the role of these highly specialized cells in promoting polarity, lumen formation, basement membrane formation, and acinar sealing against fluid backflow requires further exploration. This work would benefit from learning the biochemical cues needed to differentiate expanded populations of hS/PCs into premyoepithelial cells.
Sourcing and Engineering Whole Major and Minor Glands
Anatomically, salivary glands in the maxillofacial complex are found bilaterally as the three major glands (parotid, submandibular, and sublingual) as well as ∼800–1000 minor glands spread throughout the oral cavity. 35 Each of the four gland types has a unique structure and specialized function. The parotid gland is the largest of the major glands and is located toward the back of the jaw and in front of the ears in humans. 35 The parotid consists almost exclusively of serous acini and produces 50% of all saliva. 146 The submandibular gland is located under the mandible and contains both mucous and serous acini, and the sublingual gland is located below the tongue and in front of the submandibular gland and is the smallest of the major glands, consisting primarily of mucous-producing cells. 36 Together, the three major glands produce 90% of all saliva made, whereas the minor glands produce the remaining 10%. 146 The submandibular gland is involved primarily in basal salivary secretions, whereas the parotid is the predominant contributor to stimulated salivary secretions. The sublingual gland contributes to both basal and stimulated rates, whereas the minor glands serve primarily to lubricate the oral cavity. 147
Salivary gland functions
Given that the parotid gland contains serous cells and produces half of the saliva produced in a day, it is functionally one of the most important glands. Serous cells produce α-amylase that breaks up starches and begins digestion. 146 Because of the importance of the parotid gland, the focus of tissue engineering techniques has been to primarily create serous-producing salivary functional units. To date, primary salivary cells for tissue engineering purposes have been obtained mostly from unaffected regions of cancer patients undergoing surgical resection before radiation therapy or from those undergoing routine salivary gland surgery for benign conditions.24,80 However, in considering autograft tissue sources of cells for noncancer patients such as those with Sjögren's Syndrome, the depth and location of the parotid, including its intimate association with the facial nerve, must be considered a hurdle to obtaining tissue from which to isolate hS/PCs for tissue engineering.
The submandibular gland contains a mixture of serous-producing and mucous-producing cells. 35 Serous cells are important in aiding digestion and breaking up food, whereas mucous is important for lubricating the mouth and esophagus. 49 The submandibular gland also plays a role in altering the viscosity of the mucus, allowing more or less flow. 35 The sublingual gland also has a mixture of serous- and mucous-producing cells, but it contains mostly mucous-producing cells. 49 The submandibular gland and sublingual glands, such as the parotid, are difficult to access and obtain tissue from for cell isolation.
The minor glands are numerous, easily accessible, and less complex and they consist of serous and mucous cell types. 148 Although they only produce 10% of all saliva, minor glands are easily obtained through a minimally invasive minor lip biopsy procedure. 149 These numerous and easily accessible glands make them an ideal cellular source for tissue regeneration for noncancer patients with hyposalivation disorders. 148
Regenerating an entire salivary gland
To date, there has not been a fully reconstructed major gland made by using tissue engineering techniques. At present, organized structures containing the three primary cell types, acinar, myoepithelial, and ductal, have not been accomplished in 3D hydrogels. Obtaining 3D branched structures in vitro beginning with stem/progenitor populations has seen limited success, but the role of the ECM and the other cues needed to maintain each of these cell's phenotypes has brought this objective closer.26,43,65 Currently, the engineered replacement consists of a hydrogel packed with primary partially differentiated acinar cells and likely a few ductal cells or myoepithelial cell progenitors.22,150
One consideration has been whether the implantation of these functional units may be sufficient to restore function once implanted in one of the major glands. Alternatively, it should be possible to make less complex, but more numerous, structures similar to native minor glands and implant those in the oral mucosa. In addition, many regeneration techniques have focused on keeping assemblies of fully differentiated cell types propagating in vitro with the idea of implanting a functional lab-produced neogland. Given the ongoing identification of unique stem cell populations in the salivary glands, a new source of material may be available for propagation and differentiation into mature cell types in situ after implantation.148,151
Stem Cells and PCs
The unique ability of a stem/PC to self-replicate and become a differentiated mature cell type has given rise to the accepted concept of using these cell populations for tissue engineering salivary secretory units to restore function.24,25,27,70,104,129,142,148,152,153 Initial work in murine models demonstrated the presence of cells bearing stem cell markers in the salivary gland.129,154 In murine models, the primary markers for ductal PCs are KIT and KRT14. 109 KRT14+ cells in the murine submandibular gland give rise to granulated ductal cells, whereas KIT+ cells in the sublingual gland give rise to intercalated ductal cells. 109
Since then, many markers have been used to identify stem and PCs in humans. Although some debate exists as to the exact location and cellular markers of true stem cell populations, markers for stem or PCs identified in parotid and submandibular glands include CD34, CD29, CD49f, CD44, CD54, CD73, CD90, and CD105. 152 cKit 24 and CD2425 also have been used as potential markers. Expression of CD49f is often used as a stem cell marker in salivary glands,27,155–157 but some have found these cells to be CD49f negative in minor glands. 151 Stem cells isolated from minor salivary glands are negative for c-KIT, but they are positive for markers CD90 and CD105.148,151 We demonstrated that hS/PCs positive for K5, K14, KIT, and MYC could be isolated, passaged, and grown in 3D hydrogels while maintaining these PC markers. 70 Such hS/PCs exhibited “stemness” demonstrated by the sphere assay where primary spheroids developed in 7 days and secondary spheroids could be seen at day 3. 70
Differentiation strategies
Since stem and PC populations were identified, researchers have begun to identify the necessary reagents and culture conditions needed to expand and differentiate these cells in vitro. In collagen I and Matrigel®-based hydrogels, CD24hi/CD29hi cells formed ductal-like structures indicating differentiation whereas CD24lo/CD29hi and CD24hi/CD29lo showed more lobular-like structures, indicative of cell populations with higher degrees of stemness versus cell populations with a more committed lineage. 25 In humans, c-KIT-positive cells can be isolated from excretory ducts and expanded in vitro in growth factor reduced Matrigel®. 24
Our lab identified hS/PCs and successfully expanded these cells in HA-based hydrogels.64,70 In our hands, these hS/PCs expressed K5, K14, MYC, ETV4, and ETV5 PC markers. 70 In addition, these cells maintained these progenitor markers for at least 15 passages in HA-based hydrogels. Finally, hS/PCs could be differentiated into acinar-like cells; however, complete acinar-like architecture may require additional polarization signals from myoepithelial cells 70 or nerve. 102 More work is required to understand all the cues required to assemble ductal, acinar, and myoepithelial cell phenotypes to form a fully functional gland. Another challenge is how to maintain stem cell populations in neoglands such that they retain the capacity for self-renewal that will ensure long-term gland survival after implantation.
Implantation of stem cells and secretory units to restore function
Although the complete development of a full gland replacement may still be several years away, the discovery of resident stem cell populations may produce a new therapeutic option. Insights on mechanisms that maintain the stem-cell like state or lead to differentiation into mature salivary cell types have led to transplanting these cells into irradiated salivary glands to restore function.24,129,133,156 During head and neck cancer treatments, the radiation field damages the salivary organ as well as the surrounding nerves and blood vessels.56,158 Although these effects are not seen immediately, after a few weeks to several months postradiation treatment, acinar cell atrophy is evident.159–161
To identify the therapeutic potential of stem cells, these cells were transplanted either in their stem cell state or after being predifferentiated. Transplanted cKIT+ stem cells isolated from mouse salivary glands and enriched by fluorescence-activated cell sorting sorting restored function in irradiated glands and acquired an acinar phenotype as demonstrated by α-amylase expression. 129 cKIT+ cells removed before radiation and cultured ex vivo were reintroduced after radiation treatment where they evaded acinar atrophy to partially return salivary function to the gland. 156 The stem cell function of cKIT+ cells, however, remains controversial and is not yet accepted. 162
A three-fourth parotid resection model was developed in our labs where we showed long-term viability of implanted hS/PCs in HA hydrogels with retention of acinar phenotype. 80 Although these, and other, proof-of-concept cell therapies have yet to move into clinical use, these preclinical experiments demonstrate the therapeutic potential of reintroducing stem cells into the irradiated salivary gland to restore function. The insights from these studies are paving the way to large animal studies ongoing in several laboratories, with the minipig becoming a well-accepted preclinical model.97,163
Where Biology Meets Engineering: Integration with Host Tissues After Implantation
To develop a fully functional salivary gland replacement, the integrated functions that other cells in the environment play must be considered. The nervous, vascular, and immune systems all impact outcomes from any transplant approach to salivary gland reconstruction.133,156,164
Nervous system
Biology
The sympathetic and parasympathetic branches of the nervous system innervate the salivary glands.35,105 In humans, the sympathetic nervous system innervates all salivary glands through the superior cervical ganglion that also innervates the blood supply. 96 The sympathetic nervous system primarily acts on salivary glands through norepinephrine that acts on alpha and beta adrenergic receptors on acinar cells and some ductal cells. 165 The parasympathetic nervous system innervates the salivary glands through various cranial nerves and primarily releases acetylcholine and vasointestinal polypeptide. 96
The human parotid is innervated primarily from the glossopharyngeal nerve (cranial nerve IX) and facial nerve (VII).35,56 The submandibular gland and sublingual gland are primarily innervated from the facial nerve (cranial nerve VII). The sublingual and minor glands have sparse direct sympathetic innervation and instead have more sympathetic innervation of their respective blood vessels. 96
The nervous system aids branching morphogenesis. 166 Ex vivo studies blocking nerve development during early embryonic stages or complete removal of the nerve demonstrated inhibited branching morphogenesis. 46 Further studies demonstrated an important role of the nervous system in maintaining salivary stem PCs. 166 In addition, removal of the neural ganglion from ex vivo salivary gland rudiments significantly stunted branching morphogenesis, suggesting a neural role in branching, polarization, and differentiation. 166
Tissue engineering
Despite the role that the nervous system plays in the development of the salivary gland and the maintenance of unique stem/progenitor populations, only recently have studies begun integrating nerves with salivary cells.
167
One group recently used magnetic 3D printing to generate salivary organoids by using neural-crest derived mesenchymal stem cells and dental pulp stem cells in a gold and iron-oxide nanoparticle solution that was crosslinked with poly-
Some tissue-engineered salivary gland microstructures can be stimulated by β-adrenergic and muscarinic agonists such as norepinephrine and acetylcholine, respectively. 23 This suggests that the epithelial structures are functional and able to be modulated by the nervous system. Ongoing work in our and other labs seeks to demonstrate integration of tissue-engineered implants with the host nervous system present in the salivary glands.164,168 Neural integration remains a difficult challenge for the field, especially in patients who have previously suffered organ and nerve damage due to surgery or prior radiation.
Blood supply
Biology
Branches of the external carotid artery supply the parotid salivary gland. 35 The submandibular gland is supplied by the facial and lingual arteries, whereas the sublingual gland is supplied by the sublingual and submental arteries. 35 It remains unknown whether the development of blood vessels plays a role in salivary gland morphogenesis, but it is clear that they influence salivary gland patterning. 169 The endothelial niche from which blood vessels arise plays a key role in other organs that undergo branching morphogenesis such as the breast or pancreas.170,171 Given the similarities in these processes, it is likely that the endothelial cells that give rise to the vasculature of the salivary gland are involved in the induction and patterning of the gland as well as altering saliva production by vasoconstriction or vasodilation. 96
Tissue engineering
Efforts to vascularize salivary glands have been limited; however, there has been some work performed in labs that model the oral mucosa. Recently a layer-by-layer (LbL) cell coating approach was used to create in vitro oral mucosa models in which the blood vessels were made from human umbilical vein endothelial cells. 172 These LbL approaches to construct large networks of vasculature 173 may hold the key to developing a more complex salivary gland.
Interestingly, these vasculature networks require similar ECM proteins as does the salivary gland, suggesting that the incorporation of these networks into existing or peptide-modified hydrogels optimized for salivary gland tissue engineering may be supported. 173 Similar approaches could be used to develop more complex models of salivary glands and to better understand the relationship between blood vessels and salivary gland development. Likewise, the plethora of emergent 3D methods for 3D printing of vasculature can be integrated into salivary tissue replacement strategies for clinical practice. 174
Immune cells
Biology
Salivary glands contain dendritic cells, 111 plasma cells, 35 T cells, 175 and macrophages.176,177 Most of these immune cells are found in the connective tissue; unless actively repairing or fighting an infection, lymphocytes are limited. 35 Most of our understanding of the function of immune cells with respect to the salivary glands comes from salivary gland tumor biology and research on Sjögren's Syndrome.4,5,140,178
The involvement of the immune system in salivary gland regeneration or development remains largely unknown. Recently, however, macrophage involvement was shown during branching morphogenesis in submandibular tissue through the release of macrophage-colony stimulating factor. 132 In other organs such as the mammary gland, macrophages are involved in the development and organization of end bud structures. 179 Cytokines they produce also may play key roles in the stimulation of production of enzymes that are needed to remodel the tissue microenvironment that occurs during salivary gland morphogenesis. 180
Tissue engineering
A few studies to date have incorporated immune cells and salivary gland cells, especially in 3D culture systems. Typically when immune cells are cultured with salivary cells, it aims at understanding how the immune cell modulates salivary cells in cancer and Sjögren's Syndrome models and these cells are often co-cultured in 2D.181,182 One difficulty in studying the immune system's role in any aspect of biology in vitro is the difficulty in maintaining some immune cell types. 183 B and T cells can be expanded in vitro and then cultured with other cell types or with tumor organoids. 184 New technologies to overcome these limitations and model all immune cells in the native environment are being developed.
The air–liquid interface culture systems can maintain the native immune cell microenvironment for up to 2 weeks in most human tumor biopsy types. 183 More work is needed to understand the role that immune cells play in salivary gland development. In addition, understanding how the immune cells react to tissue-engineered salivary glands could provide insight into how patients' own immune systems would react to the introduction of stem/PCs delivered as autografts or allografts. Some recent studies in advanced Lupus patients receiving stem cell therapies under compassionate use approval have suggested that stem cells from nonself donors are well tolerated. 185 This offers hope that 1 day donor cells might be used for salivary gland tissue engineering for patients with long-term hyposalivation disorders for whom autografting is not an option.
Implantation Considerations for the Future
We do not know how far along tissues need to be differentiated in the lab to restore function in vivo. Stem cells can survive and differentiate once injected, but long-term survival has not yet been demonstrated. Additional considerations need to be made if full lumens, ducts, or glands are generated. How would these be surgically reconnected to existing salivary gland architecture? If not reconnected, there is the potential for these constructs to not bring saliva to the oral cavity and instead form cysts. 52 Could we rely on the native tissue remodeling to incorporate these additions? It is unclear currently how long it takes for some of these hydrogel constructs to degrade and how stiff they need to be to remain intact long enough to support gland regeneration.
Further, irradiated and atrophied glands from Sjögren's are often dry and lack many of the key factors that are required to accept and integrate these constructs.4,186 Are exogenous growth factors required to finish integrating these models? A large subset of patients that would require a salivary gland transplant are those with Sjögren's Syndrome. However, questions remain as to how chronic autoimmune disease would impact the hydrogels and whether these new glands would become immediately infiltrated with immune cells that would destroy the implant. Perhaps customized hydrogels could be modified to reduce immune cell infiltration or the cells could be modified to remove self-antigens? There is no doubt that establishing a fully functional, integrated salivary implant to correct hyposalivation disorders represents a significant challenge that will require a combination of stem cell biology, regenerative medicine, and tissue engineering approaches.
We believe that continued advances in tissue engineering will allow for better models of salivary gland diseases. Many of these salivary gland diseases impact more than just the three primary cellular components of the salivary gland. Tissue destruction impacts the surrounding neural tissue, blood vessels and often results in large expansion of immune cell populations.4,5 The addition of additional components to develop a salivary gland will likely not only provide the key molecular cues required to recreate native salivary glands but also generate new models to study salivary gland disease and disorders. Finally, many other exocrine glands such as the pancreas and mammary glands form through similar branching morphogenesis processes.45,187 Understanding the cues that lead to salivary gland development offers the opportunity to 1 day engineer a full menu of tissue-engineered exocrine glands.
Footnotes
Acknowledgments
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by National Institute of Health - National Institute of Dental and Craniofacial Research: R01DE022969 (to M.C.F.C), F32DE024697 (to D.W), U24DE0226914 (to M.C.F.C), University of Texas Health Science Center - Houston, Center for Clinical and Translational Sciences (TL1TR003169), Oral and Maxillofacial Surgery Foundation.