
Abstract
Fibrosis of the knee is a common disorder resulting from an aberrant wound healing response and is characterized by extracellular matrix deposition, joint contraction, and scar tissue formation. The principal regulator of the fibrotic cascade is transforming growth factor beta-1 (TGF-β1), a factor that induces rapid proliferation and differentiation of resident fibroblasts. In this study, we demonstrate successful inhibition of TGF-β1-driven myofibroblastic differentiation in human fibroblast-like synoviocytes using a small molecule TGF-β1 receptor inhibitor, SB-431542. We also demonstrate successful encapsulation of SB-431542 in poly(D,L-lactide-co-glycolide) (PLGA) as a potential prophylactic treatment for arthrofibrosis and characterize drug release and bioactivity in a three-dimensional collagen gel contraction assay. We assessed the effects of TGF-β1 and SB-431542 on cell proliferation and viability in monolayer cultures. Opposing dose-dependent trends were observed in cell proliferation, which increased in TGF-β1-treated cultures and decreased in SB-431542-treated cultures relative to control (p < 0.05). SB-431542 was not cytotoxic at the concentrations studied (0–50 μM) and inhibited TGF-β1-induced collagen gel contraction in a dose-dependent manner. Specifically, TGF-β1-treated gels contracted to 18% ± 1% of their initial surface area, while gels treated with TGF-β1 and ≥10 μM SB-431542 showed no evidence of contraction (p < 0.0001). Upon removal of the compound, all gels contracted to control levels after 44 h in culture, necessitating sustained delivery for prolonged inhibition. To this end, SB-431542 was encapsulated in PLGA microspheres (SBMS) that had an average diameter of 87.5 ± 24 μm and a loading capacity of 4.3 μg SB-431542 per milligram of SBMS. Functional assessment of SBMS revealed sustained inhibition of TGF-β1-induced gel contraction as well as hallmark features of myofibroblastic differentiation, including α-smooth muscle actin expression and connective tissue growth factor production. These results suggest that SB-431542 may be used to counter TGF-β1-driven events in the fibrotic cascade in the knee cartilage.
Impact statement
Arthrofibrosis is the most prevalent comorbidity resulting from orthopedic procedures such as total knee arthroplasty that is characterized by excess deposition and accumulation of extracellular matrix. Despite its prevalence, treatments are generally palliative, and there is no effective prophylactic therapy. We report that the small molecule transforming growth factor beta-1 (TGF-β1) receptor inhibitor, SB-431542, can inhibit the TGF-β1-driven myofibroblastic differentiation of fibroblast-like synoviocytes. To provide sustained inhibition, we explored the use of SB-laden microspheres as a prophylactic therapy in a three-dimensional contraction model of fibrosis and propose that such therapies will have the potential to improve the standard of care for arthrofibrosis.
Introduction
Arthrofibrosis is the most prevalent comorbidity resulting from routine orthopedic procedures such as total knee arthroplasty (TKA) and anterior cruciate ligament reconstruction, leading to pain, loss of mobility, and reduced quality of life.1–3 The pathology of arthrofibrosis is characterized by joint contractures, accumulation of excess extracellular matrix (ECM), and the formation of scar tissue observed as a complication of joint injury and osteoarthritis (i.e., idiopathic arthrofibrosis).4–6 Despite the prevalence of knee arthrofibrosis, its impact on postoperative patient quality of life, its economic burden, and prophylactic treatments have largely been understudied. Currently, the standard of care for arthrofibrosis includes physiotherapy, manipulation under anesthesia, and arthroscopic surgery. Treatments for arthrofibrosis are generally palliative, and do not cure or reverse the pathological changes. Furthermore, there is no prophylactic treatment currently available to affected patients.7–10 In addition, arthritis-related knee pain and inflammation are treated with limited corticosteroid injections (e.g., 3–4/year) due to rapid joint clearance rates and systemic side effects of steroids.11–14 Recent developments have focused on surgical strategies and while minimally invasive, they are still subject to increased risk of infection as well as low patient willingness to undergo surgery.15–19 To overcome the challenges of arthritis treatment, vehicles such as microspheres and drug-loaded scaffolds for prolonged low-dose drug delivery are being explored.20–24
Overexpression of the transforming growth factor beta-1 (TGF-β1) is implicated in inflammation and aberrant wound healing, which are key features of knee joint diseases and fibrosis pathology. 25 The concentration of active TGF-β1 in healthy knee joints is negligible, while in diseased conditions, TGF-β1 concentrations range from 4 ng/mL in osteoarthritis patients to 10 ng/mL in patients with rheumatoid arthritis.26,27 In addition, downstream mediators of the canonical TGF-β1 signaling pathway such as connective tissue growth factor (CTGF), as well as the families of vascular endothelial growth factor and fibroblast growth factors (FGFs) are all elevated during wound healing. 28 As such, TGF-β1 is a key regulator of the wound healing cascade. Additional studies have shown that its concentrations peak in the first 2 weeks after injury and repair in various in vivo models of knee and tendon injury.29–32
The profibrotic effects of TGF-β1 overexpression and its canonical signaling pathway via SMADs 2/3 have been studied in numerous organ systems.33–41 TGF-β1 induces myofibroblastic differentiation of resident fibroblast-like synoviocytes (FLS), characterized by upregulation of alpha-smooth muscle actin (α-SMA; Fig. 1). 42 Because myofibroblasts are responsible for the hallmark features of arthrofibrosis such as joint contractions and uncontrolled fibrotic tissue accumulation, 43 studies targeting TGF-β1 and its receptors have yielded promising preclinical results.33,37,38,40,44,45 For example, humanized antibodies against TGF-β1 for the treatment of systemic sclerosis were shown to be safe in Phase I/II clinical trials and were used for the treatment of diabetic kidney fibrosis.25,46

Application of SB-431542 to block key features of the fibrotic cascade. Arthrofibrosis is characterized by joint stiffening and contractures due to abnormal accumulation of ECM by differentiated myofibroblasts. TGF-β1 is a key regulator of fibrosis and it acts by inducing proliferation and myofibroblastic differentiation of resident FLS through the canonical SMAD signaling pathway. SB-431542, a small molecule inhibitor of TGF-β1 receptor is incorporated to abrogate key features of the fibrotic cascade in FLS isolated from human synovium. ECM, extracellular matrix; FLS, fibroblast-like synoviocytes; TGF-β1, transforming growth factor beta-1. Color images are available online.
Here, we assess the antifibrotic capability of a small molecule developed by GlaxoSmithKline, SB-431542, a specific inhibitor of the type I activin receptor-like kinase receptors, ALK-4, ALK-5, and ALK-7. 47 SB-431542 has been previously shown to have antiproliferative effects in human glioma cells and to modulate the contractile phenotype in dermal fibroblasts and renal pericytes.48–51 In addition, others have previously demonstrated the antifibrotic properties of SB-431542 in FLS treated with TGF-β1.52–55 The preclinical safety profile of SB-431542 is well-established and the compound has been shown to reduce muscle fibrosis following 6 weeks of daily intraperitoneal injections in an in vivo mouse model of rotator cuff injury.39,47 We hypothesized that SB-431542 alone will also abrogate the fibrotic processes downstream of TGF-β1 in human FLS and further propose its encapsulation in poly(D,L-lactide-co-glycolide) (PLGA) as an extended drug release delivery vehicle. PLGA is widely used in implanted medical devices (such as degradable sutures) and drug delivery devices for its biocompatibility, tunability, predictable release profiles, and approval by the Food and Drug Administration.21,56 To test our hypothesis, we investigated if SB-431542 can inhibit the fibrotic phenotype of human osteoarthritic FLS in our culture conditions with elevated TGF-β1 levels simulating a wound healing milieu. We investigated both soluble SB-431542 supplemented culture media and sustained delivery of SB-431542 from PLGA microspheres (SBMS) and also investigated the off-target effects of the drug on other resident joint cells (e.g., from cartilage and ligaments). We successfully demonstrate the in vitro antifibrotic effects of released SB-431542 within the timeframe commonly associated with postoperative arthrofibrosis through inhibition of the fibroblast-to-myofibroblast transition of osteoarthritic FLS.
Materials and Methods
Materials and reagents
Fetal bovine serum (FBS) was purchased from R&D Systems (Product no. S11150). The following were purchased from ThermoFisher Scientific: CD14 Dynabeads (Product no. 11149D), human FGF-2 (Product no. PHG0026), TGF-β1 (Product no. PHG9214), antibiotic–antimycotic (A/A; Product no. 15240062), α-minimum essential medium (αMEM; Product no. 12000022), and Dulbecco's modified Eagle medium (DMEM; Product no. 11965092). Type I collagen was purchased from Corning (Product no. 354236). Poly(
Tissue collection, cell isolation, and culture
Discarded human synovium was obtained from patients following TKA in accordance with the Institutional Review Board at Columbia University Medical Center (IRB AAAQ2703). Human cartilage samples were obtained from expired grafts provided by the Musculoskeletal Transplant Foundation. Anterior cruciate ligaments were obtained from discarded bovine calf knee joints purchased from a local abattoir (IACUC exempt). Excess adipose tissue and capsular fragments were first removed from synovium explants before digestion with collagenase type II with shaking at 37°C. Digested tissue solutions were filtered through a 70 μm nylon mesh. A population of FLS were isolated via negative selection using CD14 Dynabeads as previously described. 57 Cartilage and ligament tissues were minced and digested similarly to isolate chondrocytes and ligament cells. FLS from different donors were mixed, counted, and plated at a density of 1.76 × 103 cells/cm2. FLS were expanded in αMEM containing 10% FBS, 1% A/A, and 5 ng/mL FGF-2. Human articular chondrocytes and isolated ligament cells were cultured in DMEM supplemented with 10% FBS, 1% A/A, and 5 ng/mL FGF-2. Articular chondrocytes were also treated with 1 ng/mL TGF-β1 to maintain a chondrogenic phenotype. 57
Collagen gel contraction assay
FLS were seeded at a concentration of 8 × 106 cells/mL in a 2 mg/mL type I collagen solution based on manufacturer's instructions. Gels were cultured for 96 h in serum-free DMEM and imaged at various time points to analyze changes in surface area over the course of treatment. Image analysis and surface area calculations were conducted using ImageJ. First, the inhibitory function of SB-431542 was assessed by splitting the gels into the following experimental groups (N = 4): control, 1 ng/mL TGF-β1, and 1 ng/mL TGF-β1 + 100 μM SB-431542. Second, the dose dependency of FLS-seeded collagen gels to SB-431542 concentrations was assessed by exposing the gels to control, 1 ng/mL TGF-β1, and 1 ng/mL TGF-β1 + 0, 1, 5, 10, or 50 μM SB-431542. SB-431542 was then removed after 20 h in culture to assess whether its inhibitory effect was prolonged or dependent on the local presence of the drug.
Effects of SB-431542 and TGF-β1 on samples of native human synovium
Human synovial explants were cultured for 4 days in serum-free DMEM treated with 10 μM dimethyl sulfoxide (DMSO) as a vehicle control, or 5 ng/mL TGF-β1 with or without the addition of 10 μM SB-431542. Following the culture period, tissues were fixed and stained with hematoxylin and eosin (H&E) to identify changes in cellularity and ECM.
Effects of SB-431542 on FLS proliferation
FLS were plated and expanded as described on collagen-coated (5 μg/cm2) 96-well tissue culture plates in serum-free αMEM containing various concentrations of TGF-β1 (0, 1, 5, or 10 ng/mL) or SB-431542 (0, 1, 5, or 10 μM) for 48 h. Cell numbers after the culture period were determined with a Quant-iT™ dsDNA Assay Kit.
Cell viability
The cytotoxicity of SB-431542 was assessed in two-dimensional (2D) monolayer cultures of human articular chondrocytes and ligament cells. Cells were plated on collagen-coated 35 mm glass bottom dishes and treated with either 10 μM DMSO as a vehicle control or 50 μM SB-431542 for 48 h. Cell viability was assessed by staining live and dead cells with calcein-AM and ethidium homodimer-1, respectively. Cells were imaged on a ZEISS LSM 700 confocal microscope. FLS viability was similarly assessed at the end of the collagen gel contraction assay.
Microsphere formulation
SB-431542 was encapsulated in poly(
Characterization of microspheres and drug release profiles
Microspheres were imaged using a ZEISS Sigma VP scanning electron microscope to determine particle size and distribution. The loading capacity of microspheres for SB-431542 was determined by dissolving 5 mg microspheres in DCM and spectrophotometrically quantifying the absorbance at 329 nm. Absorbance readings were compared to a standard curve of known SB-431542 concentrations. Drug release from SBMS was determined by incorporating microspheres in a 2% (w/v) agarose (A4018; Sigma) gel at a concentration of 5 mg/mL in 1 mL phosphate-buffered saline (PBS) to simulate a depot of injected microspheres. At each time point, a 500 μL aliquot of the release medium was removed and replaced with fresh PBS to maintain perfect sink conditions. Release samples were frozen at −80°C until the end of the study period and assessed spectrophotometrically as described above.
Immunohistochemistry
FLS-seeded collagen gels were fixed in 4% formaldehyde for 24 h before being embedded and sectioned in paraffin wax. Histological sections were serially hydrated in ethanol and subjected to heat-mediated epitope retrieval with citrate buffer at 90°C for 30 min. Samples were permeabilized in 0.05% Tween-20 in PBS (PBS-T) and blocked with 10% goat serum in PBS-T. Primary antibodies for α-SMA (ab5694, 1:100; Abcam) and vimentin (ab137321, 1:100; Abcam) were applied at 4°C overnight. Alexa Fluor 488-conjugated secondary antibodies were applied at room temperature for 1 h (ab150077, 1:200; Abcam) and sections were mounted using ProLong™ Diamond Antifade Mountant with DAPI as a nuclear counterstain. Slides were visualized with a ZEISS LSM 700 confocal microscope.
Growth factor analysis in tissue media
The collagen gel contracture assay was repeated (N = 5) and media samples were collected for analysis of secreted CTGF. 58 A CCN2/CTGF ELISA Kit (DY9190-05; R&D Systems) was used to assess media concentrations. Control and SB-431542- treated samples did not require dilutions, while TGF-β1-treated media samples were diluted 1:5. A standard curve of known concentrations was fitted to a four-parameter logistic curve and used to extrapolate media CTGF concentrations according to manufacturer's instructions.
Statistical analysis
Data were analyzed on GraphPad Prism 8. The Shapiro–Wilk test was used to confirm normality and Bartlett's test was used to confirm homogeneity of variances. Logarithmic transformations were done to normalize cell proliferation fold change data. Two-way analysis of variance with time and treatment condition as factors was used to determine differences between groups with Tukey's post hoc test (α = 0.05). All data are presented as mean ± standard deviation.
Results
SB-431542 inhibits TGF-β1-induced hyperplasia in native human synovial explants
The effect of TGF-β1 on synovium and the ability of SB-431542 to abrogate these effects were observed for native human synovium harvested following TKA. Explant tissues treated with TGF-β1 displayed increased cellularity as well as thickening of the intimal layer compared to control (Fig. 2B, red arrows). In addition, the subintimal layer exhibited increased matrix density in the presence of TGF-β1. These structural changes were not observed in absence of TGF-β1- (Fig. 2A) and in SB-431542-treated tissues, where TGFβ-1-induced hyperplasia was successfully mitigated (Fig. 2C).

SB-431542 inhibits TGF-β1-induced hyperplasia of human synovial explants. H&E staining of native synovium treated with
SB-431542 and TGF-β1 have differential effects on FLS proliferation
The individual effects of TGF-β1 and SB-431542 on FLS were examined in 2D monolayer cultures. Dose-dependent inhibition of cell proliferation following SB-431542 treatment was observed (Fig. 3A), while the opposite trend was observed for TGF-β1-treated cells, with 10 ng/mL inducing the largest fold-change compared to control cultures (Fig. 3B).
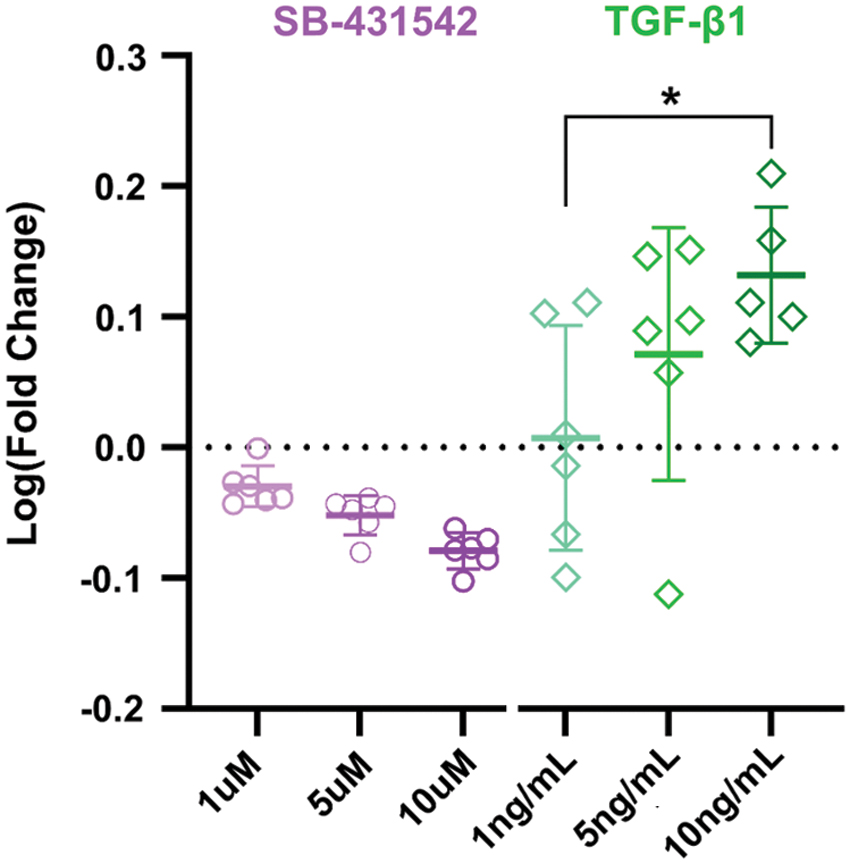
Differential effects of SB-431542 and TGF-β1 on FLS proliferation. SB-431542 (purple) and TGF-β1 (green) have differential effects on FLS proliferation in two-dimensional culture. Opposite trends in proliferation were observed in
SB-431542 inhibits TGF-β1-induced FLS contraction
The inhibitory function of SB-431542 was tested by collagen gel contraction assay in the presence and absence of TGF-β1. Treatment with TGF-β1 alone induced significant contraction of the collagen gels by day 5 of culture compared to control and SB-treated groups (p < 0.01), ultimately shrinking the samples to 8.1% ± 1.6% of their initial surface area by day 7. Control gels also exhibited a baseline contraction on day 5 and ultimately shrunk to 43.7% ± 15.5% of their initial surface area by day 7. Complete inhibition of TGF-β1-induced contraction was observed when gels were treated with 100 μM SB-431542 (Fig. 4). To further assess the potential dose dependence of FLS contraction to SB-431542 concentration, FLS-seeded collagen gels were cultured in the presence of 1 ng/mL TGF-β1 with increasing concentrations of SB-431542 and with 10 μM DMSO serving as a vehicle control.
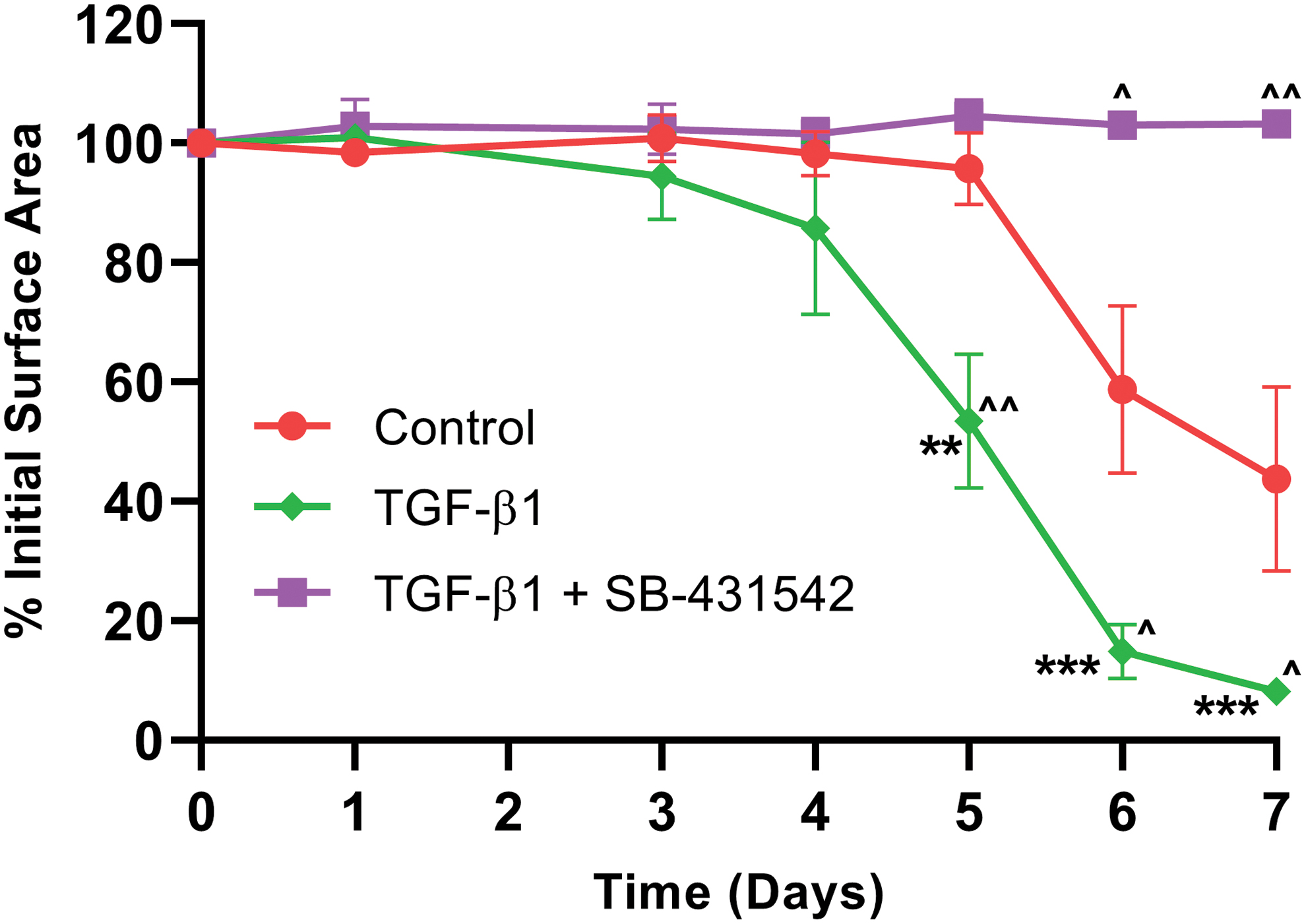
SB-431542 inhibits TGF-β1-induced FLS contraction. SB-431542 inhibits the contractile response of FLS. Collagen gels (N = 4) seeded with FLS were cultured in DMEM supplemented with or without 100 μM SB-431542 and 1 ng/mL TGF-β1. FLS exhibit a baseline contractile response that is exacerbated by treatment with TGF-β1 and inhibited by SB-431542. ***p < 0.0001; **p < 0.01 between TGF-β1-treated groups; ^^p < 0.01, ^p < 0.05 compared to control. DMEM, Dulbecco's modified Eagle medium. Color images are available online.
The dose-dependent responses of FLS to SB-431542 were evident starting at 15 h of culture. Control gels contracted to 18% ± 1% of their initial surface area, while gels treated with 1 μM SB-431542 contracted to 73.6% ± 25.6% of their initial surface area (p = 0.0562 compared to control). Gels treated with ≥5 μM SB-431542 maintained their initial surface area (p < 0.0001 compared to control). Through 20 h, gels treated with ≥10 μM SB-431542 showed no signs of contraction and as such, 10 μM SB-431542 was determined to be the minimal therapeutic concentration for further studies.
At the same timepoint, gels treated with 5 μM SB-431542 contracted only slightly to 88.7% ± 7.2% of their initial surface area (p < 0.001 compared to control) and similar trends were observed in gels treated with 1 μM SB-431542, which contracted to 50.2% ± 27.1% of initial surface area (Fig. 5A). After 20 h, SB-containing culture media were removed and all gels were subsequently cultured in control media containing TGF-β1 alone to identify any long-term effect of SB-431542 on FLS contractile function (Fig. 5, dashed line). While gel contraction rates were lower in gels treated with SB-431542 at increasing concentrations, all gels contracted in similar manner by 64 h, contracting to 11.2% ± 5.7% of their initial surface areas. Viability of SB-431542-treated collagen gels was confirmed at the end of the culture period (Fig. 5B). The safety of SB-431542 was further confirmed for chondrocytes and isolated ligament cells (Fig. 6). The observed dose-dependent decrease in cell proliferation was in agreement with the effects on FLS (Fig. 3).

Dose-dependent sustained effects of SB on FLS contraction.
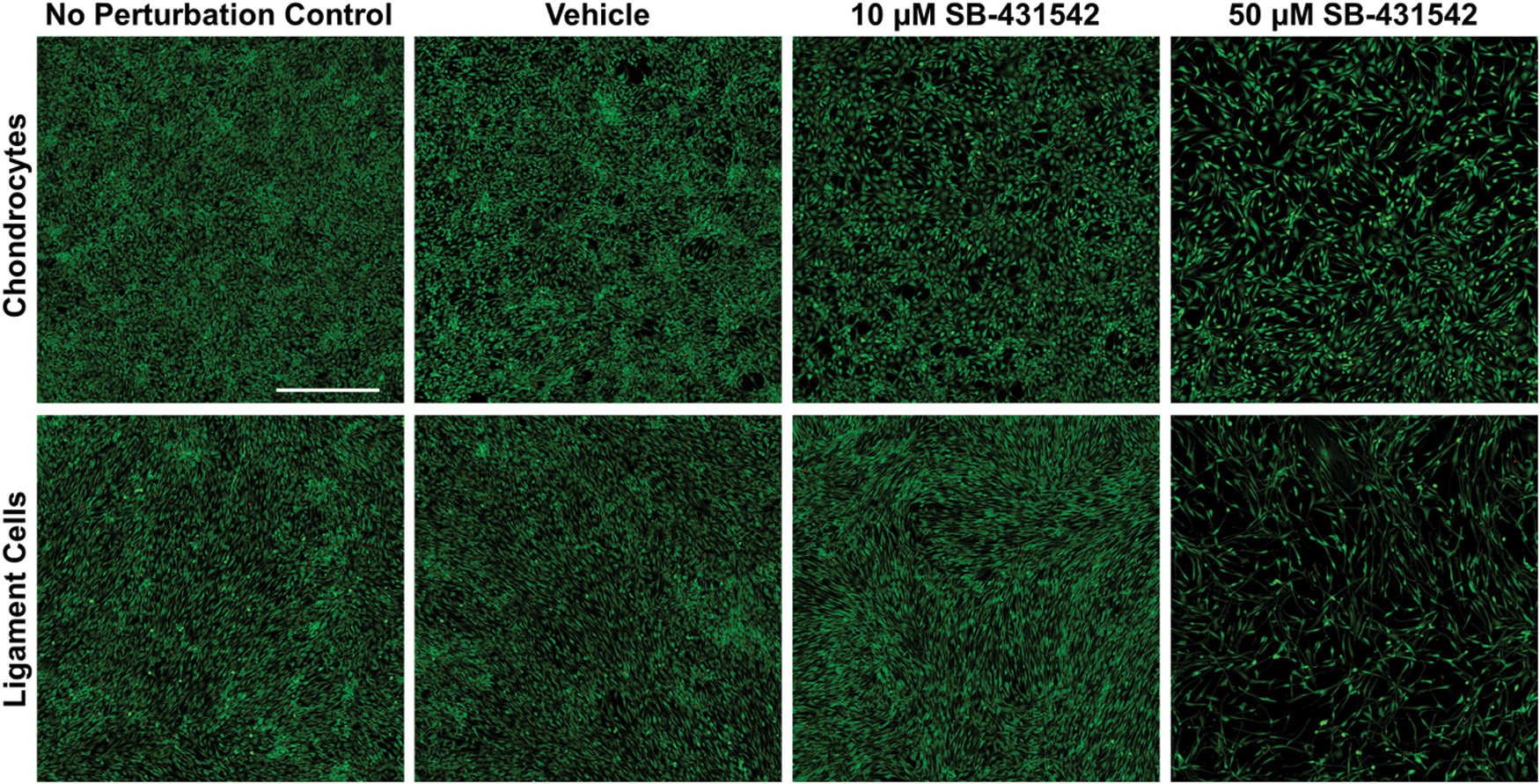
Viability of human articular chondrocytes and ligament cells after treatment with a vehicle control (DMSO) and SB-431542 for 48 h. A no perturbation control was included for baseline cell viability and proliferation. Live cells were stained with calcein-AM (green), and dead cells were stained with ethidium homodimer-1 (red). Scale Bar: 500 μm. Color images are available online.
SB-431542 encapsulated microsphere characterization
Microspheres had an average diameter of 87.4 ± 24 μm (N = 107), as assessed by electron microscopy (Fig. 7A, B). The loading capacity of SB-431542 in the microspheres was 4.3 μg SB-431542 per milligram of microspheres. Drug release from SBMS was determined by incorporating microspheres in a 2% (w/v) agarose gel at a concentration of 5 mg/mL in 1 mL PBS to simulate a depot of injected microspheres. A burst release of 6.2 ± 0.4 μg SB-431542 was observed from the gel in the first 24 h, accounting for 28.9% ± 1.7% of the total drug load. By day 11, 16.1 ± 1.2 μg SB-431542, or 75% ± 5.5% of total drug were released into the release medium (Fig. 7C).
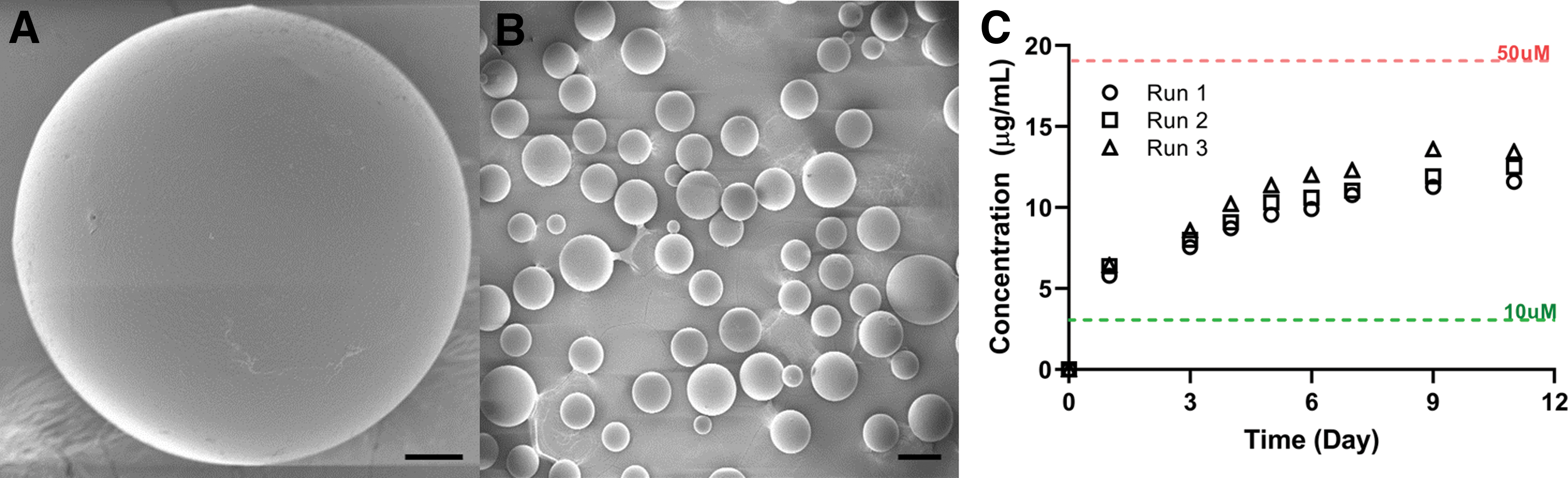
SB-431542-encapsulated microspheres.
The bioactivity of encapsulated SB-431542 was determined by an in vitro assay simulating a depot of injected microspheres adjacent to the target tissue. SB-encapsulated microspheres were mixed in a 2% agarose gel at a density of 5 mg/mL and casted in 24-well plates. Collagen gels seeded with FLS were cast on top of the agarose and treated initially with 1 ng/mL TGF-β1. Released SB-431542 from microspheres successfully inhibited TGF-β1-induced contraction, with significant differences first observed at 17 h (p < 0.01; Fig. 8). Because further culture with 1 ng/mL TGF-β1 revealed no differences compared to control through 45 h, the concentration in TGF-β1-treated groups was increased to 10 ng/mL to induce a larger effect (Fig. 8, gray line). As a result, TGF-β1-treated gels contracted significantly more by 66 h in culture (p < 0.05 compared to control and SB-431542 treated groups) and this trend was observed until the end of the culture period. SB-431542 was shown to slow the TGF-β1-induced contractile response of FLS for the duration of the study (p < 0.01 at 96 h), but not significantly compared to control (p = 0.059). Unloaded microspheres did not induce any differences in the contractile response of collagen gels.

Surface areas of FLS-seeded collagen gels placed above an agarose gel with or without SB-431542-encapsulated microspheres. FLS-seeded collagen gels were initially treated with 1 ng/mL TGF-β1, but the concentration was increased to 10 ng/mL to induce a larger effect (gray line). Released SB-431542 from PLGA microspheres remains active and inhibits the contractile response induced by TGF-β1. Representative images of collagen gels are shown (right). *Between TGF-β1 treated groups; ^Compared to control (culture media only in the absence of TGF-β1). ****p < 0.0001, ***p < 0.001, **p < 0.01, *p < 0.05, ^^p < 0.01, ^p < 0.05. PLGA, poly(D,L-lactide-co-glycolide). Color images are available online.
At the end of the experiment, gels were fixed and assessed for markers of fibrosis and the myofibroblastic phenotype, such as α-SMA and vimentin. TGF-β1 treatment increased expression of these markers compared to control and this effect was mitigated by treatment with SB-431542 (Fig. 9). Control gels also expressed basal levels of α-SMA and vimentin higher than that of SB-431542-treated gels, corresponding to their observed inherent contractile response. H&E staining of gels further revealed increased matrix density and cellularity with TGF-β1 treatment that was abrogated by released SB-431542. In an experimental repeat, culture media was assessed for CTGF, a downstream marker of fibrosis upregulated by TGF-β1. Media CTGF concentrations were significantly upregulated by TGF-β1 (4060 ± 1728 pg/mL) compared to control (517.5 ± 112.6 pg/mL) and microsphere-treated groups (379.4 ± 119.6 pg/mL, p < 0.0001; Fig. 10).
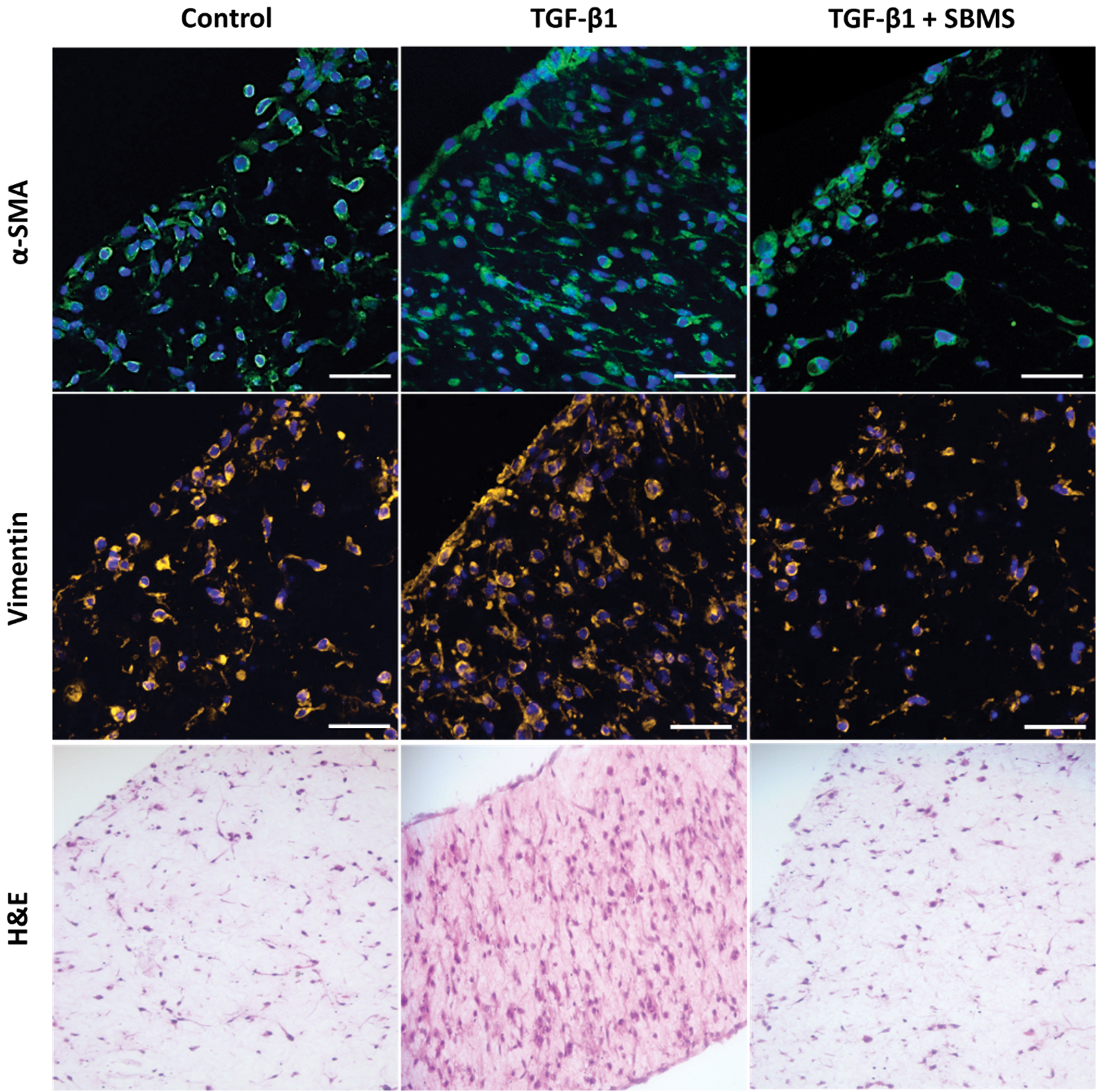
Upregulation of α-SMA and vimentin expression with TGF-β1 treatment is abrogated by SB-431542 released from microspheres. FLS-seeded collagen gels were fixed and stained for α-SMA (green), vimentin (orange), and nuclei (blue). Scale bar: 50 μm. H&E demonstrates increased density and cellularity of gels treated with TGF-β1 only (20 × magnification). α-SMA, alpha-smooth muscle actin. Color images are available online.
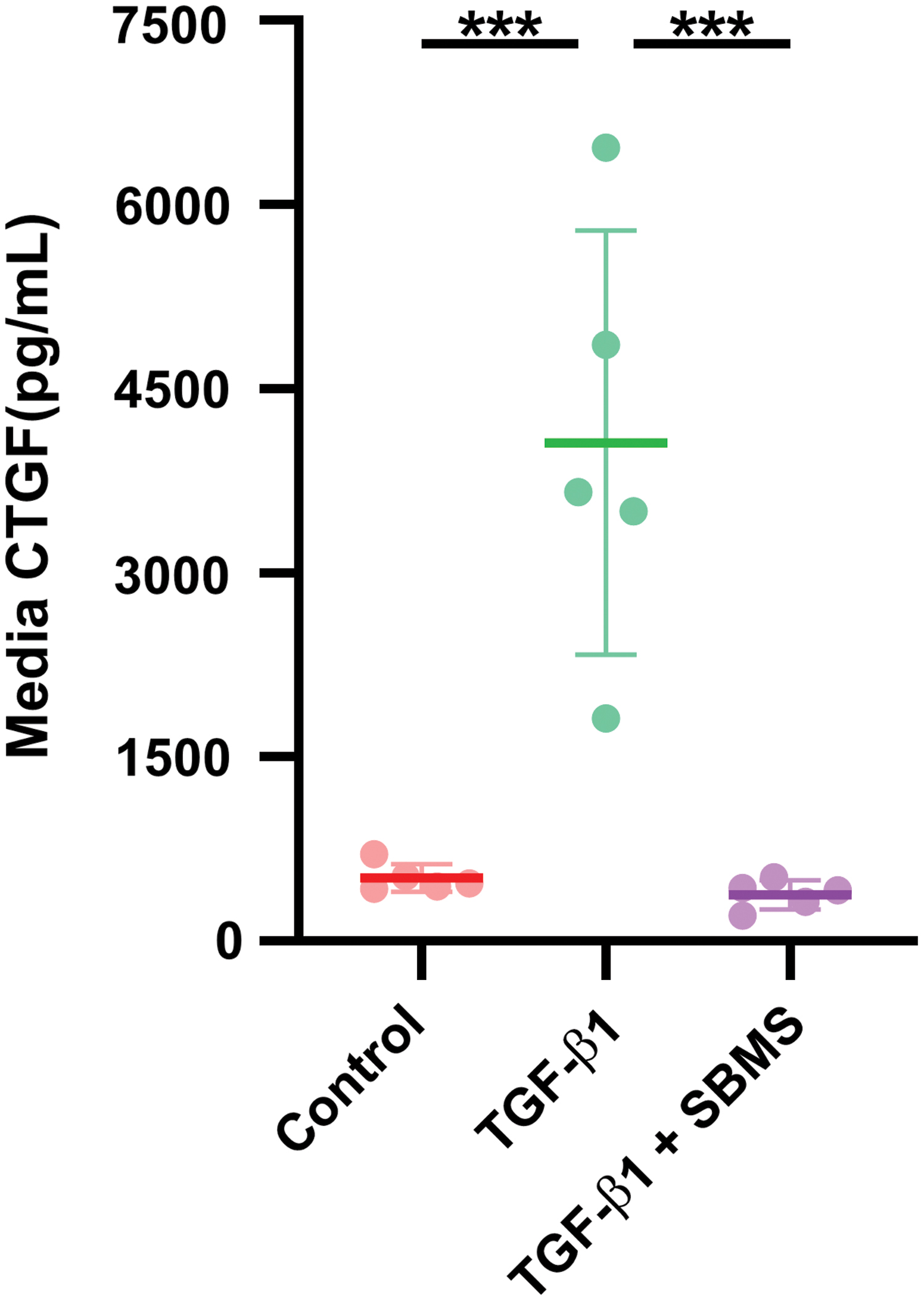
Secreted CTGF by FLS-seeded collagen gels. TGF-β1 (green) upregulated FLS-seeded collagen gel secretion of CTGF as measured by an ELISA, which was absent in control (red) and TGF-β1 + SB-431542-treated (purple) gels (N = 5). ***p < 0.0001. CTGF, connective tissue growth factor; ELISA, enzyme-linked immunosorbent assay. Color images are available online.
Discussion
TGF-β1, its receptors, and downstream mediators of the wound healing cascade are common biological targets for the treatment of fibrosis in various organ systems. 59 We explored SB-431542 as a candidate therapeutic for inhibiting the contractile response of differentiated myofibroblasts, using a collagen gel contraction assay. Quantitative data support our hypothesis that SB-431542 can abrogate the downstream fibrotic response to TGF-β1 in human FLS. Specifically, TGF-β1 (1 ng/mL) induced contraction of FLS-seeded collagen gels, which was inhibited by SB-431542 in a dose-dependent manner with no apparent cytotoxic effects up to 50 μM (Fig. 5). We determined that a therapeutic concentration of 10 μM SB-431542 was necessary for complete inhibition of contractile function, and that the maintenance of local concentrations of SB-431542 was needed for prolonged inhibitory function. We also confirmed that the loss of contractile function was not due to cell death (Fig. 5B), but rather to the inhibition of the fibroblast-to-myofibroblast differentiation as evidenced by decreased expression of the hallmark marker, α-SMA (Fig. 9). These results are in agreement with previous reports on the toxicity profile of SB-431542 and its use to inhibit tumor metastasis in human cancer cell lines.47,48
Because of its ability to specifically inhibit the canonical TGF-β1 signaling pathway, SB-431542 has also been explored as an antifibrotic agent. Studies have shown inhibition of ocular scar formation following filtration surgery by preventing the myofibroblastic transdifferentiation of human Tenon's capsule fibroblasts. 60 SB-431542 has also been shown to inhibit the myofibroblastic differentiation of dermal fibroblasts as well as to downregulate downstream mediators of this signaling pathway such as plasminogen activator inhibitor-1 and CTGF.39,49 While the safety of SB-431542 has been confirmed over the course of 6 weeks in an in vivo rodent model of rotator cuff fibrosis, the compound was intraperitoneally injected daily, which may pose a barrier to clinical translation due to lower patient compliance for repeated injections and increased risk of infection. 39 As a potential solution, recent findings have suggested an implantable method of long-term drug delivery for arthrofibrosis treatment in an in vivo rabbit contracture model of fibrosis.24,61,62 Previous studies of gene expression of profibrotic factors involved in the wound healing cascade suggest spikes in TGF-β1, plasminogen activator inhibitor-1, and CTGF immediately postinjury and prolonged elevation over the course of 2 weeks.29–31,63 Here, we expand these initial findings and establish the therapeutic feasibility of SB-431542 encapsulated microspheres as a local prolonged delivery system by leveraging the biocompatibility of PLGA and the antifibrotic properties of SB-431542.
The release profile of the SBMS was consistent with the timeline of elevated growth factors observed in in vivo models of fibrosis, with ∼75% of encapsulated SB-431542 being released by 11 days, and a burst release of ∼30% in the first 24 h (6.2 ± 0.4 μg; Fig. 7). The bioactivity of SB-431542 following encapsulation was confirmed using the collagen gel contraction assay (Fig. 8). Released SB-431542 was most successful in inhibiting contraction in the first 24 h, and was able to suppress gel contraction over the course of 96 h compared to controls and TGF-β1-treated gels. At the end of the study, gels were stained for the myofibroblastic markers α-SMA and vimentin to elucidate the cellular mechanisms driving TGF-β1-induced contraction in osteoarthritic FLS.42,43,64 Gels treated with TGF-β1 alone exhibited increased α-SMA and vimentin expression, along with more dense H&E staining, which was mitigated with SBMS treatment to levels of control gels (Fig. 9). In addition, media CTGF was significantly elevated in TGF-β1-treated gels in the absence of SB-431542 (4060 ± 1730 pg/mL vs. 379 ± 120 pg/mL).
However, given that TGF-β1 is necessary for a proper wound healing response, it may be undesirable to completely desensitize FLS to the beneficial effects of TGF-β1 and its downstream mediators. 25 The ability of the collagen gels to still contract at slower rates may be indicative of more subtle and controlled activation of the fibroblast-to-myofibroblast differentiation mechanism required for proper wound healing or the ability of FLS to maintain their intrinsic contractile behavior in the presence of modest concentrations of SB-431542.
While the results of the current study suggest the therapeutic potential of SB-431542 and the use of SBMS as a mode of extended drug delivery, the in vitro contraction model system using FLS-seeded collagen gels has its limitations as it is not completely representative of native synovium in both tissue structure and overarching mechanisms. For example, contraction physiologically only represents one specific stage of wound healing that otherwise includes processes such as angiogenesis and inflammatory cell recruitment. 65 Tissue-engineered platforms could circumvent the limitations in donor tissue availability. Our laboratory has recently described a functional in vitro tissue-engineered model of the synovium that captures such changes in the context of inflammatory cytokines and steroid treatments involved in osteoarthritis. 66 Future studies could leverage this model to incorporate other relevant tissue types in fibrosis and wound healing (e.g., adipose-derived mesenchymal stem cells from the infrapatellar fat pad, synovium-, and blood-derived macrophages). It is anticipated that a more biomimetic, high-throughput in vitro system incorporating engineered tissues of consistent sizes will allow future screening for various therapeutics as well as additional downstream targets involved in the fibrotic cascade.
In summary, we demonstrate the therapeutic capacity of SB-431542 in inhibiting the TGF-β1-driven phenotypic changes in FLS. We also present a potential novel prophylactic treatment of arthrofibrosis via local delivery of SBMS that was successful in inhibiting the myofibroblastic phenotype of FLS while maintaining cell viability. Future in vivo studies will incorporate recently developed contracture models of arthrofibrosis to further test the therapeutic capacity of SBMS under physiologic conditions.24,62,67,68 While translation to the clinic for human applications will require studies in both small and large animal models, the demonstrated safety profile of SB-431542 on human tissue-derived cells makes this compound a promising candidate as a prophylactic therapeutic for arthrofibrosis. We further speculate that local, prolonged, and low-dose microsphere delivery of SB-431542 will overcome the challenges associated with rapid clearance rates in the joint and the ease of applying SBMS during common orthopedic procedures such as TKA will offer a novel treatment for knee arthrofibrosis.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by funding from NIH (Grant Nos.: R01AR068133, P41 EB027062, and F31AR078004) and the Orthopedic Scientific Research Foundation.