
Abstract
Octacalcium phosphate and collagen composite (OCPcol) promotes osteogenic differentiation and angiogenesis, thereby enhancing bone regeneration. Although a newly developed freeze-dried composite of OCPcol and teriparatide (OCPcolTPTD) reinforced bone regeneration more than OCPcol, the mechanism of bone regeneration remains unresolved. In this study, disks containing OCPcolTPTD, OCPcol, or β-tricalcium phosphate (β-TCP) col were inserted into rodents with calvarial bone defects, before euthanasia 4 weeks later. Immunohistochemical and histochemical analyses were performed on bone samples to evaluate bone matrix development, angiogenesis, and osteoclast and osteoblast localization. In the OCPcolTPTD and OCPcol groups, bone regeneration was observed at the surface of calvarial dura mater and around acidophilic granular cells with abundant collagenous fiber-containing cells. Furthermore, the newly formed bone in the OCPcolTPTD group showed a larger total area and individual separated area than the other groups. Various osteogenic proteins were detected in the regenerated bone and peri-bone tissues by histochemistry and immunohistochemistry. Although the expression of several osteogenic biomarkers in the OCPcolTPTD group after 4 weeks of implantation was significantly lower than that in the OCPcol group, new bone formation by OCPcolTPTD in the center of the defect, where bone regeneration is difficult, tended to be superior to that by OCPcol. These results suggest that OCPcolTPTD enhanced bone regeneration more evenly and homogenously than OCPcol.
Impact statement
Our study suggests that octacalcium phosphate and collagen (OCPcol) together with a TPTD enhances bone regeneration in rodents with calvarial bone defects. Furthermore, we believe that composite of OCPcol and teriparatide (OCPcolTPTD) could be developed into novel clinical technique for the regeneration or repair of bone.
Introduction
Following successful oral surgeries such as tooth extraction and cystectomy, the bone volume of residual alveolar ridges generally shrinks because of bone resorption. 1 In addition, the atrophic alveolar bones might limit the functional placement of dental implants. 2 Hence, bone grafts are generally utilized for bone defects. However, issues associated with autologous bone graft application, similar to the dysfunction of donor organs, limited adaptation, and the prospect of additional surgery, 3 have led to the search for alternative clinical methods. So far, hydroxyapatite (HA) and beta-tricalcium phosphate (β-TCP) are two of the most common and widely used artificial materials for bone regeneration surgery.4,5
OCP is a precursor of biological apatite in teeth and bones in vivo. 6 OCP has bone-regenerative properties, 7 and it can be phagocytosed in vivo by multinucleated giant cells and osteoclasts. 8 An easy-to-handle composite consisting of OCP and collagen (OCPcol) that overcomes molding associated with original OCP has been developed. 9 Compared with a composite consisting of HA and collagen or β-TCP and collagen composite (β-TCPcol), 10 OCPcol demonstrates excellent bone regeneration and promotes bone maturation and vasculogenesis. 11 Following clinical studies on OCPcol for mandible or maxilla defects,12–15 clinical trials on OCPcol have started.16–19 Recently, OCPcol was approved and commercialized in Japan for use in the field of oral surgery.20,21
The parathyroid hormone (PTH) regulates the metabolism and functions of calcium and phosphate, 22 and teriparatide (TPTD) is a PTH consisting of the first 34 amino acids at the N-terminus.23,24 Recently, it was reported that a collagen sponge soaked in 20 μg of PTH TPTD was useful for bone defect. 25 Kajii et al. 26 reported that a single local dose of 1 or 0.1 μg of TPTD absorbed in the collagen sponge—a dosage similar to that used to treat osteoporosis—enhanced the recovery of a critical-sized bone defect. Besides, Iwai et al. 27 produced a freeze-dried composite of OCPcol and TPTD (OCPcolTPTD)—the OCPcol disk impregnated by TPTD solution (1.0 μg) was lyophilized—and investigated its bone regenerative properties. It was confirmed that OCPcolTPTD could induce bone regeneration as efficiently as a single local dose of TPTD absorbed in the collagen sponge.
In this study, we aimed to investigate whether OCPcolTPTD exerts positive effects on bone formation to evaluate and detect the existence and activity of cells or molecules related for bone regeneration during the early phase of healing using a rodent critical-sized bone defect model with an immunohistological approach. The differences in bone regeneration were investigated upon the transplantation of freeze-dried OCPcolTPTD, OCPcol, and β-TCPcol (control) into rat calvaria with critical-sized bone defects.
Materials and Methods
Preparation of OCPcol and β-TCPcol
OCPcol was prepared as reported previously9,11 by direct precipitation. 28 We also prepared sieved granules of sintered β-TCP (OSferion; Olympus, Tokyo, Japan). 10 Collagen was prepared from lyophilized atelocollagen (NMP collagen PS; Nippon Meat Packers, Tsukuba, Ibaraki, Japan). OCP and β-TCP were mixed with the collagen (concentration: 3%, pH: 7.4). After lyophilization, the OCPcol or β-TCPcol was molded into disk shape (diameter: 9 mm and thickness: 1.5 mm). These disks were prepared by dehydrothermal treatment using a vacuum drying oven (150°C, 24 h).
Preparation of the OCPcolTPTD composite
First, the TPTD solution was prepared using chemically synthesized lyophilized teriparatide acetate (TERIBONE™ Inj. 56.5 μg; Asahi Kasei Pharma Corp., Tokyo, Japan), and it was reconstituted into a 56.5 μg/mL solution. The OCPcol disks combined with 1.0 μg of TPTD (OCPcolTPTD) were prepared as follows: OCPcol disks were placed individually in a 48-well plate and 17.7 μL of TPTD (56.5 μg/mL) was permeated into each OCPcol disk. 27 The OCPcolTPTD disks were then lyophilized, followed by sterilization with electron beam irradiation.
Implantation procedure
Twelve-week-old male Wistar rats (SLC Corp., Hamamatsu, Japan) were used. The study protocol was reviewed and approved by the Animal Research Committee of Tohoku University (2018BeA-001). The principles of laboratory animal care, as well as national laws, were followed. The Institutional Animal Care and Use Committee of the Tohoku University Environmental and Safety Committee approved all procedures in this study, under approvals. Anesthesia with a cocktail of butorphanol tartrate (2.5 mg/kg), midazolam (2 mg/kg), and dexmedetomidine hydrochloride (0.15 mg/kg) was used for experimental rats. Following an incision on the parietal skin and an ablation of the periosteum of the calvarium, a trephine defect of full thickness with a diameter of 9 mm was fabricated in the rat calvarium, while avoiding damage to the dura. An OCPcolTPTD, OCPcol, or β-TCPcol disk was then centrally implanted into the defect (n = 5 per group). Finally, the incised periosteum and skin were sutured (Fig. 1A–C). For consistency, implants of the same volume were used for all animals. To prevent wound infection, following implantation, the rats were injected subcutaneously with cephalexin (15 mg/kg). The experimental rats were euthanized with an overdose of sodium pentobarbital at 4 weeks after implantation.
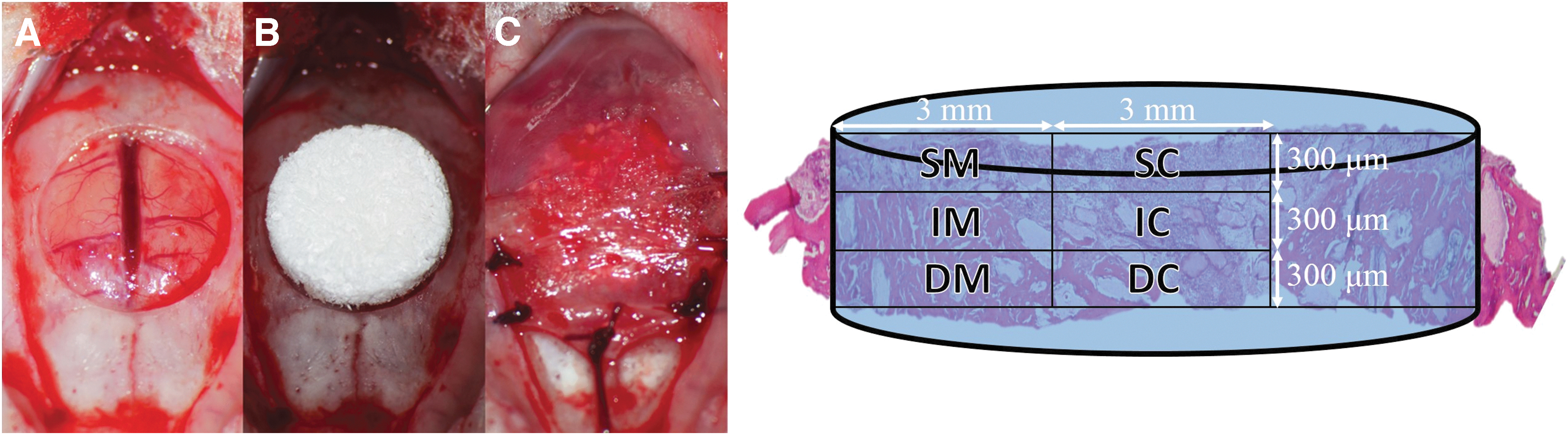
Left: Implantation procedure.
Radiography and microcomputed tomography examination
At 4 weeks after surgery, the calvariae of live rats were examined using an in vivo microcomputed tomography (μ-CT) system (Latheta LCT-200; Hitachi Aloca Medical, Tokyo, Japan). Scanning was performed after intraperitoneally injecting the rats with sodium pentobarbital (50 mg/kg) to prevent excessive movement. CT images of 120-μm-thick slices were acquired.
Tissue samples were harvested together with the surrounding bone, following euthanasia. They were then fixed with 4% paraformaldehyde that was prepared in 0.1 M phosphate-buffered saline of pH 7.4. Radiographs of the skull were then obtained using a microradiography unit (Softex M-60; Softex Co., Ltd., Ebina, Kanagawa, Japan) at 45 kV and 1.5 mA for 2 min.
Sample preparation and histological analysis
Next, decalcification of calvarium bone specimens was performed with 10% ethylenediaminetetraacetic acid prepared with 0.01 M phosphate buffer of pH 7.4, at 4°C for 2–4 weeks. The bone samples were then excised, embedded in paraffin, and sliced to 3-μm-thick sections for histological analysis (hematoxylin and eosin [HE]; Elastica-Masson [EM]), enzyme histochemistry, and immunohistochemical staining. “n-Bone areas” of the newly formed bone in the bone defect area were measured (Adobe Photoshop; Adobe Systems Incorporated, San Jose, CA) by HE imaging. As reported previously,26,27 the n-Bone area (%) was calculated using the following formula: [area of newly formed bone (identified by the histological sections]/[whole area of the implant (9 mm width × 1 mm height)] × 100. For a detailed histological observation, the whole area of the implanted OCPcol was divided into six areas, namely, subcutaneous (upper) margin (SM), intermediate (middle) margin (IM), dural (lower) margin (DM), subcutaneous (upper) center (SC), intermediate (middle) center (IC), and dural (lower) center (DC) (Fig. 1).
Immunohistochemistry and enzyme histochemistry
Six observation areas—laterally divided into small sections—were used to evaluate bone regeneration, perform immunohistochemical analysis, and stain alkaline phosphatase and tartrate-resistant acid phosphatase (ALP/TRAP) (Fig. 1). Each section was obtained at 0–0.3, 0.3–0.6, and 0.6–0.9 mm between the dura mater and the calvaria surface. The three layers were then divided into six sections, with the outermost left portion of 0–3.0 mm and central portion of 3.0–6.0 mm from the margin of the calvarial bone defect. To evaluate appropriate bone regeneration, antibodies against osteopontin (OPN), osteocalcin (OCN), Runt-related transcription factor 2 (RUNX2), collagen I, and vascular endothelial growth factor (VEGF) (Table 1) were used. Enzyme histochemistry analysis for ALP/TRAP activity to evaluate bone maturity was performed using a staining kit (Fujifilm Wako Pure Chemical Industries, Osaka, Japan). For immunohistochemical staining, Tris and EDTA of pH 8.4 were used for antigen retrieval, and the samples were incubated with each primary antibody mentioned above for 12 h at 4°C along with 3% hydrogen peroxide to immunohistochemically block endogenous peroxidase activity. Next, samples were incubated with peroxidase-conjugated secondary antibody for 1 h at 25°C (Table 1). The expression of proteins was detected using 3,3′-diaminobenzidine (Nichirei Biosciences), and samples were stained with hematoxylin as the nuclear counterstain.
List of Primary and Secondary Antibodies
To detect mature bone matrix, vasculogenesis, and osteoclast and osteoblast distribution in the regenerated bone tissue, cell-specific biomarkers were analyzed. For the expression of OPN, OCN, RUNX2, and TRAP, immunohistochemical reactivities were evaluated based on the number of cells showing strong immunostaining of the membrane and/or cytoplasm with reference to previous research.11,29–35 According to previous studies, immunohistochemical reactivity for VEGF was assessed using the number of cells adjacent to blood vessels in the new bone.11,36 Immunohistochemical reactivity of collagen I and expression of ALP were evaluated and classified into three groups: (−) negative, (+) weekly to moderately positive, and (++) strongly positive. Immunohistochemical examination was performed by pathologists; they counted positive cells in a microscopic image magnified 200 times. The average counts were obtained for each of the three areas of each sample preparation. For comparison, the immunohistochemical patterns of each antibody in the normal calvarium bone of rats that were not subjected to surgery were assessed. All pathologists were blinded to the experimental results and treatment details.
Statistical analysis
All statistical analyses were performed using JMP Pro software (version 12.0; SAS Institute, Inc., Cary, NC). The one-way analysis of variance (ANOVA) was used to compare the differences between the groups. Nonparametric tests (Kruskal–Wallis and Mann–Whitney U-tests) were used to compare the differences between the groups. If the results of the ANOVA were significant, data were analyzed using Tukey–Kramer test as the multiple comparison test. Values are reported as mean ± standard error. Results with p < 0.05, p < 0.01, or p < 0.001 were considered significant.
Results
Radiography and μ-CT imaging analysis
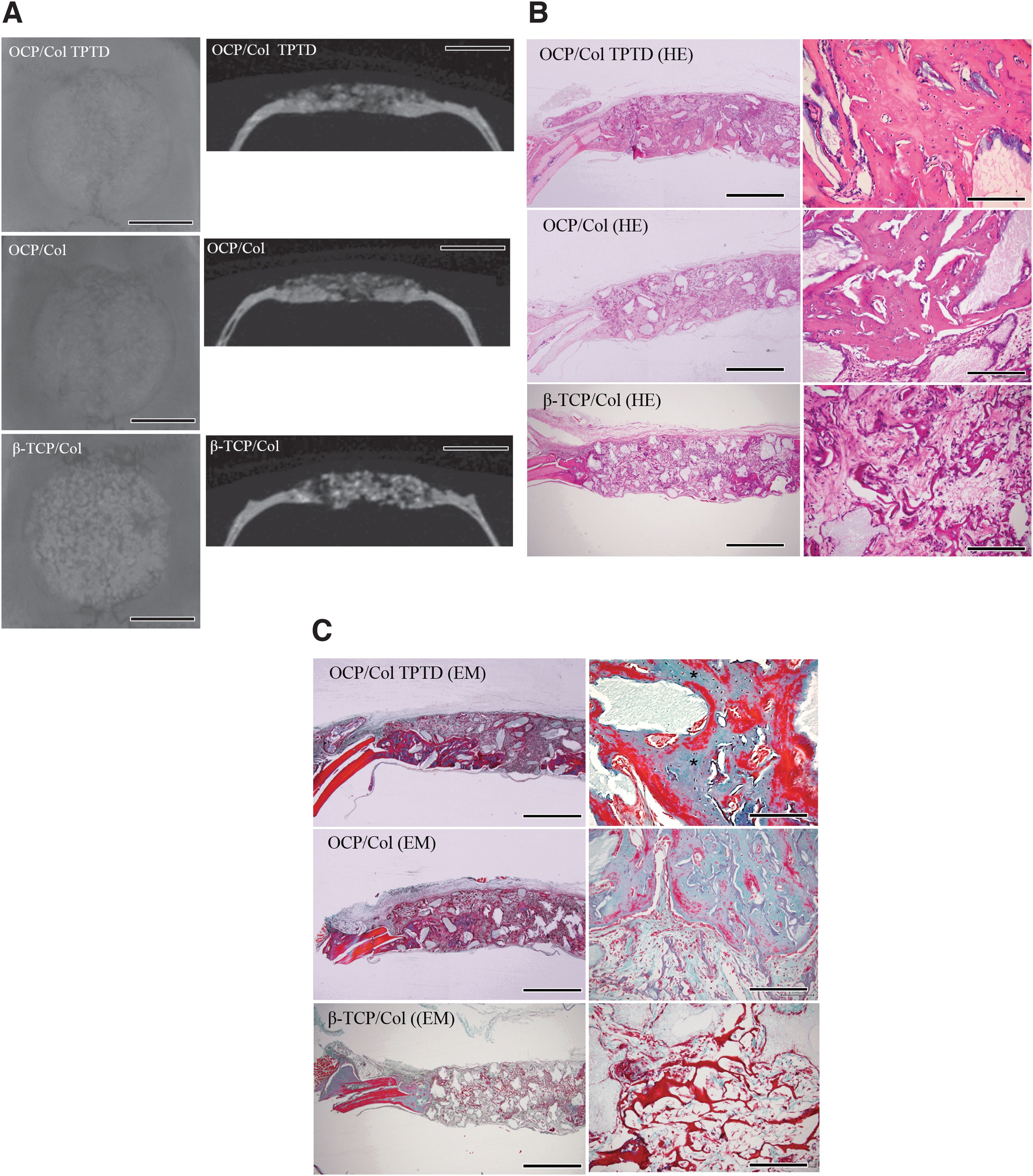
In the OCPcolTPTD group, most of the defects were covered by radiopaque lesions, which were dense and granulose, and they had a relatively uniform radiopacity close to that of the original bone (Fig. 2A). A new bone was detected in the μ-CT scan, and a radiopaque area of density similar to that of the original bone was found, extending from the defect margin toward the center of the calvarium bone defect. Radiography revealed a slightly higher number of residual granules in the OCPcol group than in the OCPcolTPTD group. However, a thin axis of the impermeable region of the OCPcolTPTD group was observed inside and at the edge of the bone defect. Although the OCPcol group presented similar μ-CT findings, it showed slightly more residual granules than the OCPcolTPTD group, and a new bone was observed to be growing mainly at the edge of the bone defect. In the β-TCPcol sample group, isolated granulose radiopacity was predominantly detected.
Histopathological analysis
Bone regeneration around acidophilic granules, along with excessive collagen fibers, was observed in the OCPcolTPTD and OCPcol groups 4 weeks postimplantation through HE and EM analyses (Fig. 2B, C). In the β-TCPcol group, bone regeneration was also observed to a less extent. In addition, bone matrix and collagen fibers were detected at levels lower than those in the other groups. With respect to the n-Bone area, the OCPcolTPTD group (45.92% ± 14.60%) showed significantly higher bone formation in total defect and in each area than the OCPcol (34.95% ± 14.65%) and β-TCPcol (7.02% ± 8.84%) groups. In particular, the extent of bone formation in the OCPcolTPTD group was exceptional in terms of overall bone growth, including bone growth in the SC, IC, and DC areas, which were the central parts of the bone, as well as in the SM and SC areas, which were the superior parts of the bone (Fig. 3).

Histomorphometric examination of n-Bone areas in the three groups based on area. The percentage of n-Bone areas was higher in the OCPcolTPTD group than that in the other two groups in all areas. *p < 0.05, **p < 0.01. NS, not significant. Color images are available online.
Immunohistochemical and enzyme histochemistry analyses
Typical staining results detected in the newly formed calvarial bone of the OCPcolTPTD samples are shown in Figure 4. OPN is a major noncollagenous protein promoting osteoclastogenesis and osteoclast activity; OPN-positive cells were present in the osteoblasts and around the trabecular bone and connective tissues surrounding the new bone. OCN, a biomarker for bone formation secreted by osteoblasts, was detected in tissues, extracellular matrix, and cells around the regenerated bone. RUNX2 is a key transcription factor associated with osteoblast differentiation and collagen I production in the bone.
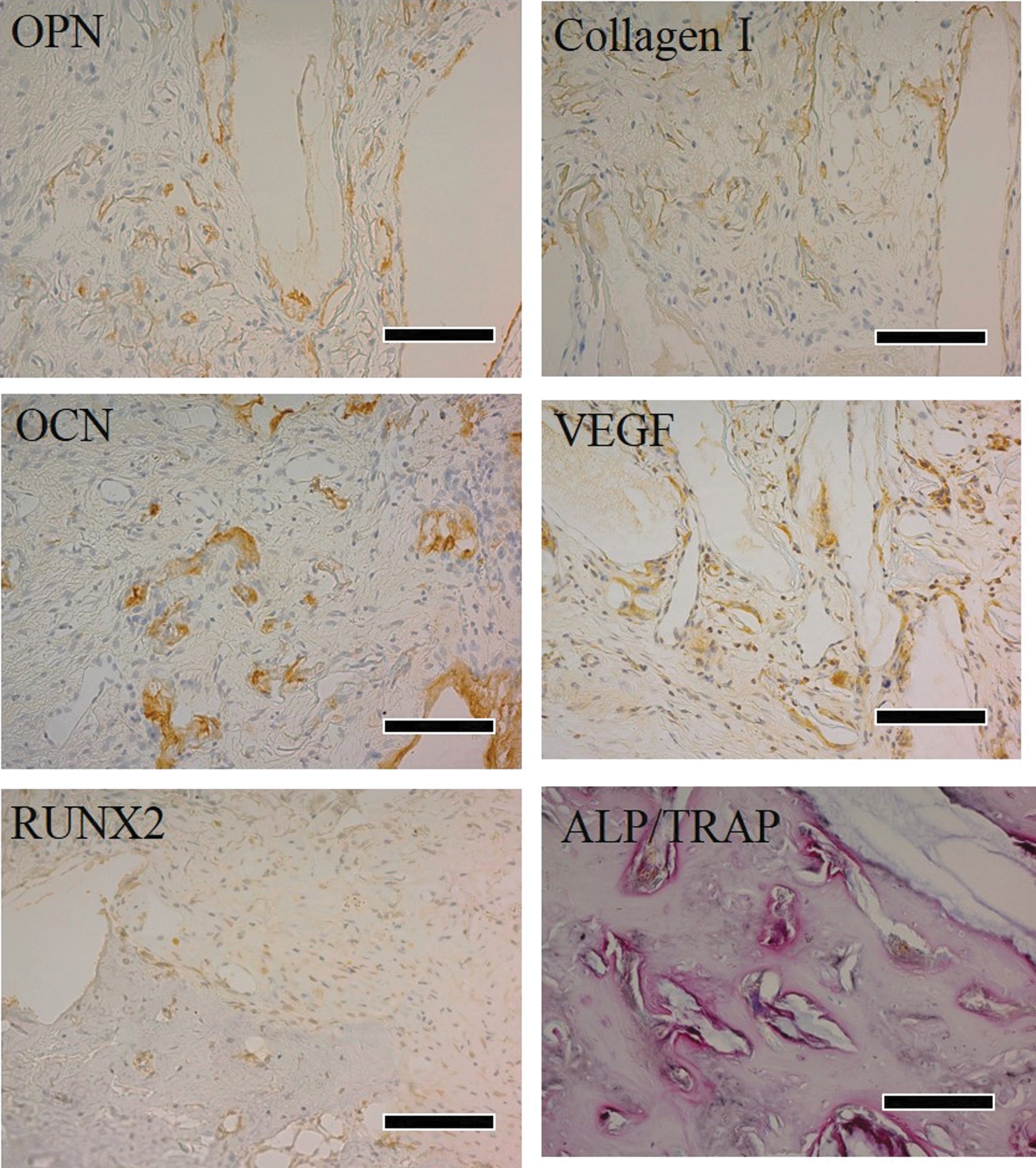
Immunohistochemistry to check for OPN, OCN, RUNX2, VEGF, and collagen I expression, as well as ALP/TRAP 4 weeks after implanting the OCPcolTPTD disk. Expression of OPN, an osteoblast and osteoclast marker, was observed on the dura surface and connective tissues. Immunohistochemical expression of OCN, the specific marker for osteoblasts, was expressed in the regenerated bone and extracellular matrix of connective tissues. The expression of RUNX2, a transcription factor essential for osteoblast differentiation, was detected in new bone cells and extracellular matrix. Type I collagen, a major protein bone matrix, was observed throughout the newly formed calvarial bone matrix. VEGF expressions were detected in connective tissues around the new bone matrix, confirming the abundance of angiogenesis. Magnification: 200 × , bars: 200 μm. ALP/TRAP, alkaline phosphatase and tartrate-resistant acid phosphatase; OCN, osteocalcin; OPN, osteopontin; RUNX2, Runt-related transcription factor 2; VEGF, vascular endothelial growth factor. Color images are available online.
In this study, RUNX2 was expressed in the cell membrane of regenerated calvarial bone cells and in the extracellular matrix around the newly formed bone. The endothelial cell marker VEGF is an essential signaling protein involved in both vasculogenesis and angiogenesis. In this study, many VEGF-positive cells were diffusely detected mainly in the soft tissue adjacent to the bone matrix, suggesting blood vessel neogenesis. Collagen I, the main and vital bone matrix protein for the process of new bone maturation, was ubiquitously expressed throughout the extracellular matrix. ALP was detected on the cell membranes of the newly formed bone, suggesting an increase in osteoblasts. In the OCPcolTPTD and OCPcol groups, the presence of many TRAP-positive cells resulted in a high activity of osteoclasts in the regenerated calvarial bone.
There was no significant difference in the expression of collagen I and ALP in the OCPcolTPTD and OCPcol groups, although the expression of OPN, OCN, RUNX2, VEGF, and TRAP in the OCPcolTPTD group was significantly lower (p < 0.01) than that in the OCPcol group (Fig. 5). In addition, the expression of most of the antibodies in the β-TCPcol group was significantly lower than that in the two groups (p < 0.01 or p < 0.05).
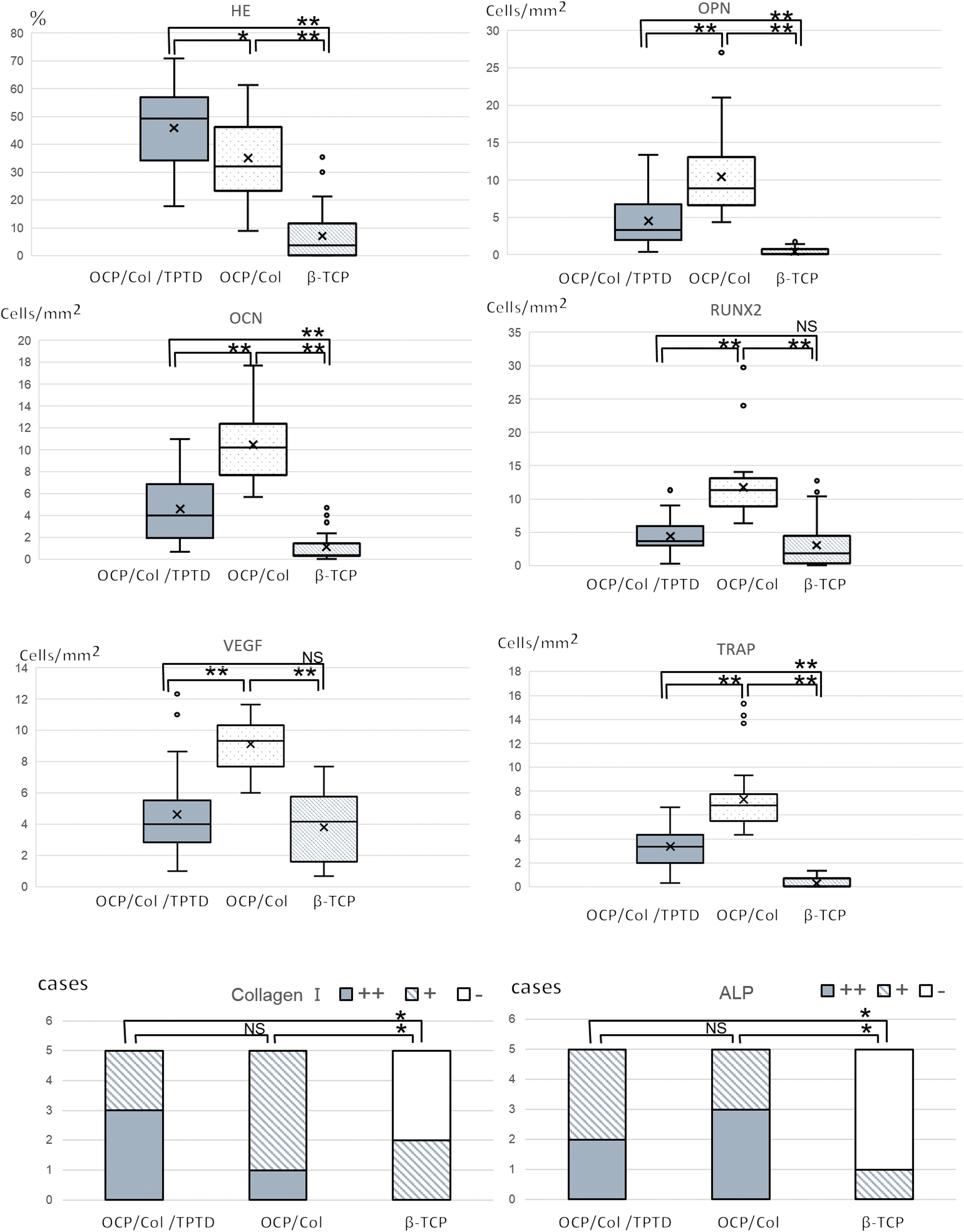
Immunohistochemical and ALP/TRAP staining in OCPcolTPTD, OCPcol, and β-TCPcol groups. No significant difference was found between the OCPcolTPTD and OCPcol groups for collagen I and ALP expression. Expression of OPN, OCN, RUNX2, VEGF, and TRAP in the OCPcolTPTD group was significantly lower (p < 0.05) than in the OCPcol group. OCN, RUNX2, ALP, and TRAP tended to be upregulated area SM or IC. Expression of Collagen I and ALP: −, negative; +, weakly to moderately positive; ++, strongly positive; *p < 0.05, **p < 0.01. NS, not significant. Color images are available online.
Immunohistochemical staining and enzyme histochemical staining were performed for all observational areas in the OCPcolTPTD group (divided into six parts from the original bone margin or the calvarial dura mater surface; Fig. 6). OCN, RUNX2, ALP, and TRAP expression tended to be upregulated in the SM and IC areas (p < 0.001 or p < 0.01 or p < 0.05).

Immunohistochemical and ALP/TRAP staining analysis of the implant area (divided into six compartments) in OCPcolTPTD group. The implant area was divided into six compartments: SM, IM, DM, SC, IC, and DC. In the OCPcolTPTD group, OCN, RUNX2, ALP, and TRAP were upregulated in the SM and IC areas. Reactivity for Collagen I and ALP: −, negative; +, weakly to moderately positive; ++, strongly positive; **p < 0.05, **p < 0.01, ***p < 0.001. Color images are available online.
Discussion
Previously, we demonstrated the detection of multiple markers—through immunohistochemical and enzyme histochemical analyses—for evaluating the formation in new bones induced by OCPcol. 11 In this study, we histologically and immunohistologically examined whether the addition of TPTD had a similar effect on the osteogenic potential of OCPcol. Some previous studies have attempted to repair experimental bone defects by leveraging the anabolic effect of TPTD through intermittent subcutaneous administration37–41 of materials such as absorbable collagen sponge, 40 demineralized bone matrix,38,40 β-tricalcium phosphate 41 , and poly-lactic acid. 37 Previous studies have indicated that the local administration of a single dose of TPTD along with OCPcol might enhance bone regeneration, and they are readily applicable in the clinical environment without any technical difficulty compared with the subcutaneous administration of TPTD.37,40–42 We previously showed that the efficacy of OCPcol to induce bone regeneration is significantly superior to that of granules or collagen sponge containing β-TCP.7,15 The application of TPTD on OCPcol may enhance the bone-promoting ability of PTH and achieve excellent bone regeneration compared with OCPcol. In addition, OCPcolTPTD has good storage stability and high versatility. 27 Most importantly, the local administration of a single dose of TPTD—similar to that used in this study—was safe and reduced pain in the treated patients.
In this study, the extent of bone formation in the OCPcolTPTD group was remarkable with respect to the overall bone growth, including the central and superior parts of the bone, which are areas where bone formation and maturation are difficult to achieve. Although bone tends to develop early at the margins and the inferior areas adjacent to the residual tissue, we observed a steady progress in the other areas. It was confirmed that OCPcolTPTD induced bone formation evenly and homogenously throughout the defect.
In the OCPcolTPTD group, OPN, OCN, RUNX2, VEGF, and collagen I expression, as well as ALP/TRAP staining, could be confirmed in each observational area that was divided into six parts; OCN, RUNX2, ALP, and TRAP were significantly upregulated (p < 0.05 or p < 0.001) in the SM or IC areas, which were located in the superior and central parts of the bone defect. These findings suggest that the margins and the calvarial dura mater surfaces exhibit a high response by expressing bone formation markers, as they are areas where bone can easily form and grow.
An interesting finding in this immunohistochemical experiment was that the expression of bone formation markers was lower in the OCPcolTPTD group than in the OCPcol group. This indicated that processes involved in bone formation and remodeling, that is, angiogenesis and differentiation of osteoclasts and osteoblasts, were more active in the OCPcol group at 4 weeks postsurgery. In this study, there was no significant difference in collagen I and ALP expression between the OCPcolTPTD and OCPcol groups, although OPN, OCN, RUNX2, VEGF, and TRAP expression were significantly lower in the OCPcolTPTD group than in the OCPcol group (p < 0.01). These results indicate that the expression of osteoclast and osteoblast markers (OPN, OCN, RUNX2, VEGF, and TRAP), which are known to be involved in bone formation, had already peaked 4 weeks after transplantation of the OCPcolTPTD implant, and the expression of mature bone markers (collagen I and ALP) was dominant at that time.
Our previous study on OCPcol, radiography, and μ-CT imaging showed that new bone is generated throughout the defect of the original calvarium bone upon OCPcol disc implantation. 11 In this study, radiography, μ-CT scanning, and histopathological analyses revealed that the OCPcolTPTD-induced new bone was not restricted to regions where bone formation is likely to occur, such as the defect margin; instead, it occurred almost uniformly throughout the calvarial defect. Furthermore, the application of TPTD to OCPcol might accelerate bone formation and maturation.
Our previous immunohistochemical and enzyme histochemical findings revealed that OCPcol-induced bone regeneration—including angiogenesis and proliferation, differentiation and activation of osteoclasts and osteoblasts, as well as bone matrix formation and maturation—proceeds to cover the whole bone defect that matures irrespective of the proximity to dura surface and margin of healthy original bone. These results suggests that the regeneration and induction of bone by OCPcol are not dependent on residual healthy tissue, including original bone and the surrounding tissue, that is, OCPcol has osteoinductive and osteoconductive functions. TPTD added to OCPcol was expected to accelerate newly generated bone remodeling as it increases the number of osteoclasts and promotes osteoclast activity for osteogenesis. 24 In addition, bone formation and its maturation were confirmed to be substantially accelerated throughout the bone defect site, and this is of great advantage in clinical applications. As OCPcol is already approved for use in Japan for treating bone defects such as sinus floor elevation and alveolar clefts in oral and maxillofacial surgeries, this newly developed OCPcolTPTD, exhibiting bone regenerative properties superior to those of OCPcol, has the potential for application in more defective reconstructive surgeries.
Conclusions
In conclusion, we demonstrated that OCPcolTPTD implantation in rats with calvarial bone defect stimulated new bone formation similar to that observed upon transplantation with OCPcol. Furthermore, the combination of OCPcol with TPTD enhanced homogenous bone regeneration to a greater extent. This novel OCPcolTPTD could be a therapeutic alternative for serious bone defects, for which treatment is difficult to achieve.
Footnotes
Authors' Contributions
A.K. and S.K. conceived and designed the study, as well as performed the experiments. A.K., K.M., T.K., Y.E., and S.K. analyzed the data and interpreted the results of experiments. A.K., T.T., and S.K. prepared and edited the article. All authors read and approved the final article.
Disclosure Statement
S.K. obtained two patents in Japan ([Hard tissue replacement materials to promote bone regeneration; No. 5046511] licensed to TOYOBO Co., Ltd. and [Combination of calcium phosphate-containing porous composites and parathyroid hormone; No. 6094716]). The other authors have no conflict of interests to declare in relation to this study.
Funding Information
This study was partially supported by Grants-in-aid (Nos. 16H03159, 16K11741, and 18K19891) from the Ministry of Education, Science, Sports and Culture of Japan.