
Abstract
The temporomandibular joint (TMJ) disc is a fibrocartilaginous tissue located between the condyle of the mandible and glenoid fossa and articular eminence of the temporal bone. Damage or derangement of the TMJ disc can require surgical removal (discectomy) to restore function. Removal of the TMJ disc, however, leaves the joint space vulnerable to condylar remodeling and degradation, potentially leading to long-term complications. No consistently effective clinical option exists for repair or replacement of the disc following discectomy. This study investigates the use of an acellular scaffold composed of extracellular matrix (ECM) derived from small intestinal submucosa (SIS) as a regenerative template for the TMJ disc in a porcine model. Acellular SIS ECM scaffolds were implanted following discectomy and allowed to remodel for 2, 4, 12, and 24 weeks postimplantation. Remodeling of the implanted device was assessed by longitudinal magnetic resonance imaging (MRI) over the course of 6 months, as well as gross morphologic, histologic, biochemical, and biomechanical analysis (tension and compression) of explanted tissues (disc and condyle) at the time of sacrifice. When the scaffold remained in the joint space, longitudinal MRI demonstrated that the scaffolds promoted new tissue formation within the joint space throughout the study period. The scaffolds were rapidly populated with host-derived cells and remodeled with formation of new, dense, aligned fibrocartilage resembling native tissue as early as 1 month postimplantation. De-novo formation of peripheral muscular and tendinous attachments resembling those in native tissue was also observed. The remodeled scaffolds approached native disc biochemical composition and compressive modulus, and possessed 50% of the tensile modulus within 3 months postimplantation. No degradation of the condylar surface was observed. These results suggest that this acellular bioscaffold fills a medical need for which there is currently no effective treatment and may represent a clinically relevant “off-the-shelf” implant for reconstruction of the TMJ disc.
Impact statement
Extracellular matrix (ECM) scaffolds remodeled into temporomandibular joint (TMJ) disc-like tissue as early as 3 months postimplantation in a porcine model after disc removal. The properties of the new tissue remained stable up to 6 months postimplantation. These results show the efficacy of ECM scaffolds to replace the TMJ disc.
Introduction
Epidemiological surveys report 20–25% of the population have symptoms of temporomandibular joint (TMJ) disorder (TMD), 1 including painful clicking and locking, which dramatically affect quality of life and interfere with normal activities. These symptoms are managed noninvasively when possible. However, internal derangement and other disc pathologies do present in patients with more severe TMD and removal of the disc may be indicated. For example, TMJ disc dislocation without reduction has an incidence estimated at 2% to 8%2,3 of TMD patients.
When disc dislocation presents with chronic (>4 weeks) locked jaw or closed lock and the patient does not improve maximal mouth opening following conservative treatment, 4 an optional approach is removal of the disc (discectomy). 5 Discectomy is generally effective at restoring TMJ function (range of motion), but leaves the joint space vulnerable to condylar remodeling and degradation. This degeneration often leads to further pathology and the potential need for additional surgery.
Tissue engineering has emerged as a potential regenerative medicine technique to replace the TMJ disc to offset the negative outcomes of discectomy. 6 Recent efforts have focused on both cell-based and scaffold-based solutions; however, only a small number of these approaches have been translated into animal studies to date.7–11 Acellular extracellular matrix (ECM)-based scaffold materials have shown promise in canine studies, remodeling into a site-appropriate tissue that resembles the native TMJ disc within 6 months of implantation.12,13
This study investigates the use of small intestinal submucosa (SIS)-ECM as a graft replacement for the TMJ disc in a porcine model, considered the “gold-standard” animal model for TMJ function and mechanical properties. 14 The results of the study clearly demonstrate that ECM-based scaffold materials can act as inductive templates for in situ constructive remodeling of the TMJ disc and have potential as clinically relevant grafts for TMJ reconstruction.
Materials and Methods
Scaffold production
As the majority of Food and Drug Administration (FDA)-approved ECM grafts used in humans are isolated from xenogeneic sources (e.g., porcine and bovine), small intestines were harvested for the preparation of ECM scaffolds in this study, obtained from adult dogs and prepared as previously described for implantation in the porcine model. 15 The intestine was rinsed with water and split longitudinally. The resulting intestinal sheet was then placed with the luminal side up, and the luminal layers of the mucosa were mechanically removed with an acrylic scraper. The intestine was then flipped and the abluminal side was scraped to remove external muscle layers. The resulting tissue consisting of the tunica submucosa and basilar layers of the tunica mucosa was rinsed and cut into ∼12 inches in length.
The tissue was decellularized and disinfected as previously described. 12 Briefly, the tissue was treated in a 0.1% peracetic acid/4% ethanol solution on a shaker at >300 rpm for 2 h. The tissue was then washed in phosphate-buffered saline (PBS) and water repeatedly to remove cellular remnants and traces of the peracetic acid and ethanol solution. This rinsing also adjusted the pH of the tissue to 7.4.
The decellularized tissues were then used to formulate the TMJ grafts as previously described.12,13 In brief, the (acellular) ECM was frozen and lyophilized, cut into 1–3 mm pieces, and powdered using a Wiley mill with a No. 60 mesh screen. A hard plastic mold was used to create an oval depression with the approximate size of the porcine TMJ disc (10 × 14-mm oval and 2-mm depth). The mold contained a flat surface surrounding this depression to allow the formation of a pillow-like core. Two hydrated sheets of ECM were then cut and pressed into the shape of the depression.
Two to three hundred milligrams of the particulate ECM created by the mill was used to fill the depression, and two more hydrated sheets were placed on the surface to create a pillow-shaped device with a peripheral rim of flattened multilayer ECM (Fig. 1). The scaffolds were then placed in a vacuum press to dry and seal the scaffold. Once dry, the scaffolds were sterilized with ethylene oxide.
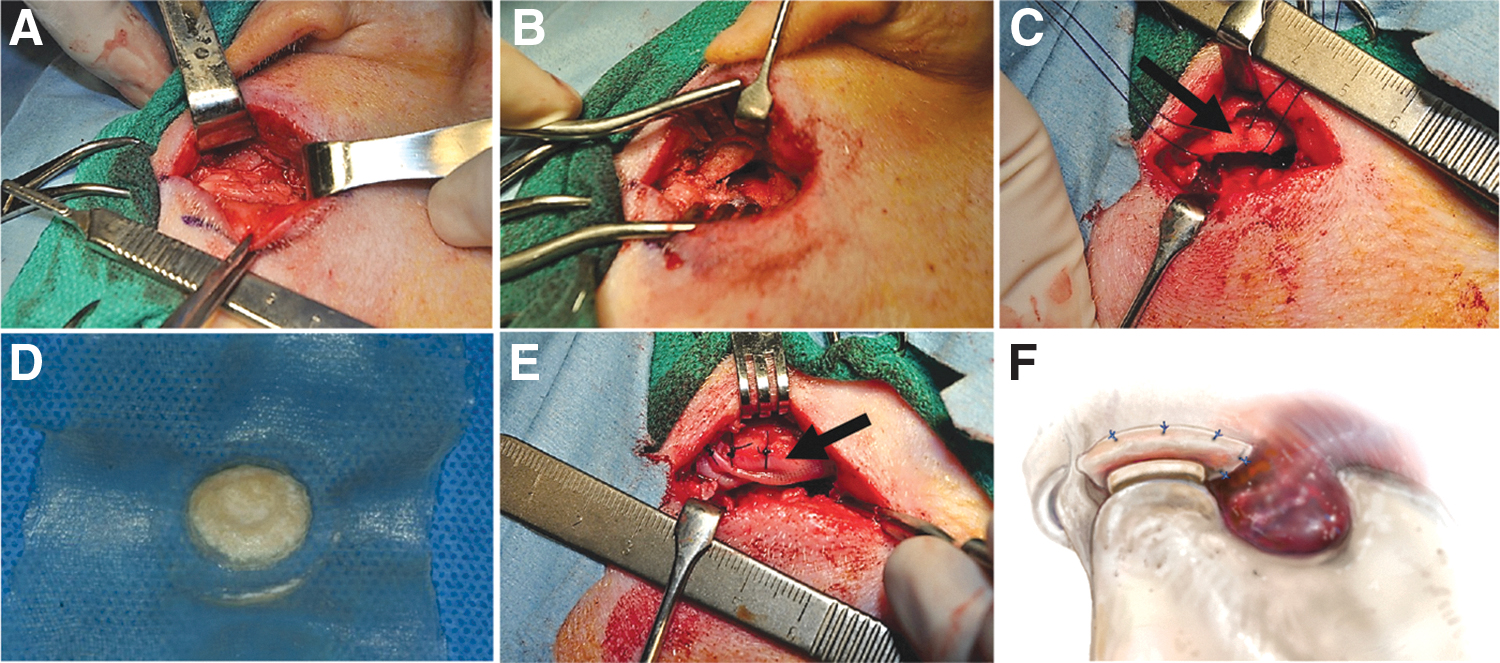
A porcine surgical model of TMJ reconstruction was developed. Briefly, (left to right) the joint space is accessed
Surgical procedure, postoperative care, and euthanasia
Although the properties of the TMJ disc derived from pigs are frequently described as the “gold-standard” target for regenerative medicine approaches to reconstruction of the TMJ disc, these assertions are largely based upon postmortem investigation of the TMJ disc in isolation. In adult farm pigs and minipigs, the zygomatic arch impedes access to the joint in skeletally mature animals, making the surgical approach and discectomy exceedingly difficult. Fracturing the arch is an alternative, but we did not want to introduce the confounding factor of bone healing. There are also modified procedures to access the disc, but these are not clinically relevant.14,16
We chose to still perform this study in the porcine model to compare the biochemical and mechanical properties of the remodeled disc to those reported in the literature, most of which is in the porcine model. For these reasons, female juvenile farm pigs at ∼3 months of age, weighing 25–30 kg, were used in the surgical model to allow for improved access and more predictable access and full removal of the TMJ disc.
Anesthesia was induced with acepromazine (0.1–0.5 mg/kg) and maintained on isoflurane (1–5%). The surgical approach involved an incision immediately anterior to the tragus, with soft tissue dissection preserving the local innervation and vasculature (especially the facial nerve) (Fig. 1A). The TMJ disc was isolated, removed in its entirety (Fig. 1B), in both joints (bilaterally). Two holes were drilled through the zygomatic arch and then sutures were passed through the hole (Fig. 1C). The disc was then replaced by the rehydrated SIS-ECM scaffold (Fig. 1D) unilaterally, with the two sutures through the zygomatic arch (Fig. 1E), leaving the other joint empty.
A schematic of the placement of the scaffold within the joint space is shown in Figure 1F. Buprenorphine (0.005–0.01 mg/kg IM or IV q12h) was administered for 5 days for pain, and then as needed. Pigs received cephalexin (35 mg/kg q12h) for 5 days as a prophylactic antibiotic. Due to the nature of the surgical procedure, all pigs were fed a soft diet for 5 days postsurgery and returned to normal dry feed diet thereafter. At the predetermined time of euthanasia, pigs were sedated with acepromazine (0.1–0.5 mg/kg BW SC). The anesthesia was induced with 5% isoflurane, and then the animals were given pentobarbital sodium IV (390 mg/4.5 kg BW). All procedures were approved by the Institutional Animal Care and Use Committee of the Cornell University College of Veterinary Medicine.
Control specimen procurement
As this was a growing animal, and no contralateral disc was present for assessment at the time of sacrifice, we utilized age-matched controls harvested from separate animals to account for potential growth and changes in the properties of the disc with age. For control groups, female pigs (n = 10 per age group) were obtained from a local abattoir at 3, 6, and 9 months of age and the TMJ discs and mandibular condyles were immediately excised. All discs and condyles were assessed morphologically to assure absence of signs of degeneration. All specimens were wrapped in gauze, soaked in 0.1 M PBS, and frozen at −20°C until used for biochemical and biomechanical testing.
Magnetic resonance imaging
Animals were anesthetized by a board-certified veterinary anesthetist and underwent magnetic resonance imaging (MRI) scanning to determine remodeling of the ECM construct after implantation. Animals were scanned in dorsal recumbency with a 1.5 Tesla magnet (Toshiba Vantage Atlas, Toshiba Medical Systems, Tustin, CA) located within Cornell University Hospital for Animals. The scanner utilized 10 integrated coil parts with a standard 16-channel array, and an actively shielded gradient coil (33mT/m, SR200).
The following MRI images were obtained with closed and open mouth positioning of each animal to best delineate the remodeling TMJ meniscus: Sagittal PD (TR 2346.5, TE 30, Matrix 336 × 408, NEX 3); Sagittal T1 (TR 540, TE 10, TA 90, Matrix 320 × 356, NEX 3); Sagittal T2 (TR 5146.5, TE 90, TA 90, Matrix 336 × 372, NEX 3); and Transverse T2.
Gross morphologic and histologic assessment
Immediately following euthanasia, the skin and connective tissues surrounding the TMJ were dissected. The joint was then removed en-bloc. Tissues were further dissected using scalpel and forceps to isolate the condyle and remodeled scaffold. Samples were photographed and placed in 10% neutral buffered formalin, processed and embedded in paraffin, and sectioned at 5 μm for staining with hematoxylin and eosin. All histologic samples were evaluated qualitatively on a Nikon e600 light microscope.
Biochemical analysis
The DNA, collagen, and glycosaminoglycan (GAG) content of the remodeled scaffolds, native discs, mandibular condyles, and preimplantation devices were measured as a percentage of dry weight (DW) of original samples as per published protocols.13,17,18 All assays were performed from the same digest.
Tensile testing
Tensile testing was performed as previously described 19 on scaffolds at 4, 12, and 24 weeks postimplantation, and on native TMJ discs from 3, 6, and 9-month-old age-matched controls. Briefly, before testing, 8 mm dermal punches were used to create anterior-posterior dogbone shapes of the intermediate zone of native discs and remodeled ECM scaffolds. These samples were 1–3 mm wide in the thinnest portion of the dogbone. Samples were fixed to a platen using freezing medium and sectioned inferiorly/superiorly to 300–400 μm using a cryotome, producing multiple sections per disc, which were all tested. Sections were collected for testing after a single complete section was shaved off the dogbone sample to ensure uniform thickness for all samples.
For testing, dogbone specimens were allowed to equilibrate at room temperature, with 0.1 M PBS, for at least 1 h before testing. Specimen width and thickness were measured using a micrometer and calipers, respectively. Samples were gripped using 440 grit sandpaper and placed in pneumatic clamps on a uniaxial mechanical testing apparatus (Instron Model 5566; Canton, MA). Testing occurred in air at room temperature, and the sample was hydrated with 0.1 M PBS using a felt tip applicator right before testing. Samples were then preloaded to 0.2 N to straighten the specimen.
The clamp-to-clamp length was taken as the initial specimen length and used to calculate percent strain. Samples were preconditioned to 5.5% strain for 20 cycles at a strain rate of 10 mm/min. As determined by initial tensile testing, 5.5% strain was determined to encompass the toe region of the stress–strain curve. For preconditioning, an upper (1.1 N) and lower (0.6 N) bound for the first peak of the preconditioning cycle was established as an acceptable load for native samples. Any native sample outside the established boundary conditions for preconditioning was discarded. These bounds were not applied to remodeled scaffolds. Following preconditioning, samples were loaded to failure at a strain rate of 10 mm/min.
The samples were analyzed for the peak tensile stress (tensile stress at failure), the tensile modulus (slope of stress–strain behavior between 4% and 8% strain), and the failure strain (clamp to clamp strain at failure [SF]). Each remodeled ECM scaffold or native disc specimen yielded 3–7 tensile samples, which were averaged into one value per specimen.
Compression testing
Unconfined compression testing and analysis were performed (as described previously19,20), on remodeled scaffolds at 4, 12, and 24 weeks postimplantation and their respective mandibular condyle cartilage. Native TMJ discs and their respective mandibular condyle cartilage from 3-, 6-, and 9-month-old pigs were used as age-matched controls. A 4 mm biopsy punch was used to obtain samples from the intermediate zone of native discs, remodeled scaffolds, and mandibular condyles.
Statistical analysis
All quantitative data were represented as average ± standard deviation. Statistical comparisons were made for collagen content, GAG content, DNA content, tensile stress, tensile modulus, tensile SF, compressive stress, and compressive modulus. Specifically, a two-way analysis of variance was performed to determine main effects for treatment (native disc and remodeled scaffold, or native condyle and condyle from treated joint) and time (1, 3, and 6 months postsurgery), and their interaction with significance set at p < 0.05. Tukey's posthoc analysis was then used to examine pair-wise differences between groups. Only differences between treatments at each time point are shown. Outliers at least two standard deviations away from the means were not used in the analysis.
Overall, the number of scaffolds that remained in the joint was 29 out of 48, which is 60%. Analysis is shown for all specimens in which the remodeled scaffold was present in the joint. For example, for tensile testing analysis, 27 treated joints were planned for 1-, 3-, and 6-month time points at n = 9 per time point. However, only 11 scaffolds remained in the joint of those dedicated to tensile testing, providing enough tissue for the testing at n = 3 for 1 month, n = 4 for 3 months, and n = 4 for 6 months.
While it is difficult to predict overall in vivo performance from individual ex vivo measurements, a functionality index (FI) where ex vivo measurements are averaged has been suggested for regenerated tissues for TMJ disc replacements. 21 For this study, we define the FI, with
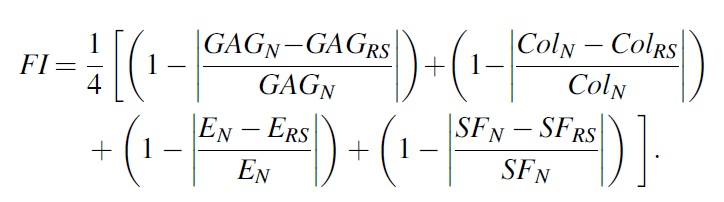
In FI, we gave equal weight to GAG content, collagen (Col) content, and the tensile moduli (E), and the tensile SF. “RS” indicates the properties of the remodeled scaffold and “N” indicates native TMJ disc properties. We chose to not include the compression properties in the index in this study because the magnitude of properties under compression is much lower than tension for the TMJ disc, and thus are not indicative of overall function. FI of each remodeled tissue sample at each time point was calculated by comparing each individual sample parameter (GAG, collagen, tensile moduli, and strain) to the average native properties at each age.
Results
Longitudinal MRI
MRI was performed longitudinally in animals to be sacrificed at the 6-month time point. Imaging studies were performed presurgically and then at times of 1, 3, and 6 months postimplantation. Imaging demonstrated a healthy, intact joint space in all animals at the presurgical time point. In control joints (no replacement), a decrease in the joint space was observed with the condyle in close approximation with the articulating fossa. Mild changes in the shape of the condyle were observed at the 6-month time point in one animal, but no significant pathology was observed in the articulating surfaces by MRI. In contrast, joint space was characterized by evidence of disc-like tissues in ECM-implanted joints throughout the 6-month study duration.
The size of the disc tissue was observed to increase with the relative size of the animal and joint space, and the distinctive “bowtie” like appearance was observed at the 6-month time point, suggesting an anterior and posterior band-like tissue structure similar to that of the native TMJ disc. Representative images of MRI outcomes can be seen in Figure 2.
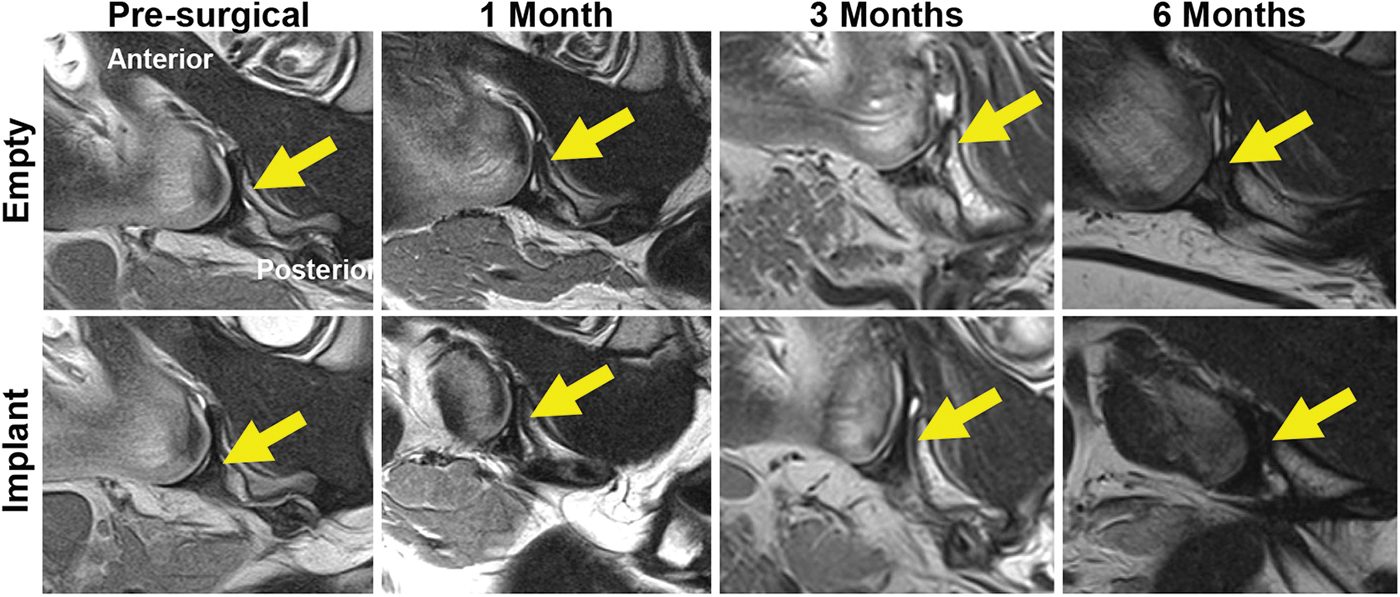
MRI was used to track device remodeling over time. T2 weighted images are shown (arrow = disc/joint space). Collapse of the joint space and no evidence of new disc formation are seen in control animals (top). Animals receiving an implant (bottom) showed maintenance of joint space and disc-like tissue formation at 6 months. MRI, magnetic resonance imaging. Color images are available online.
Gross morphology
The TMJ was resected en-bloc at times of 2, 4, 12, and 24 weeks postimplantation (Fig. 3). In control joints (not implanted), no formation of new disc-like tissue was observed within the joint space; however, dense connective tissues were present at the periphery of the joint at the 6-month time point. There were few, if any, signs of gross pathologic changes to the articulating surfaces of the condyles in the ECM-implanted joints. Minor areas of apparent thinning of the articulating surface were observed, but they were not considered physiologically relevant. Implanted joints were characterized by rapid and progressive remodeling of the implanted ECM material into tissue, which was similar to the native TMJ.
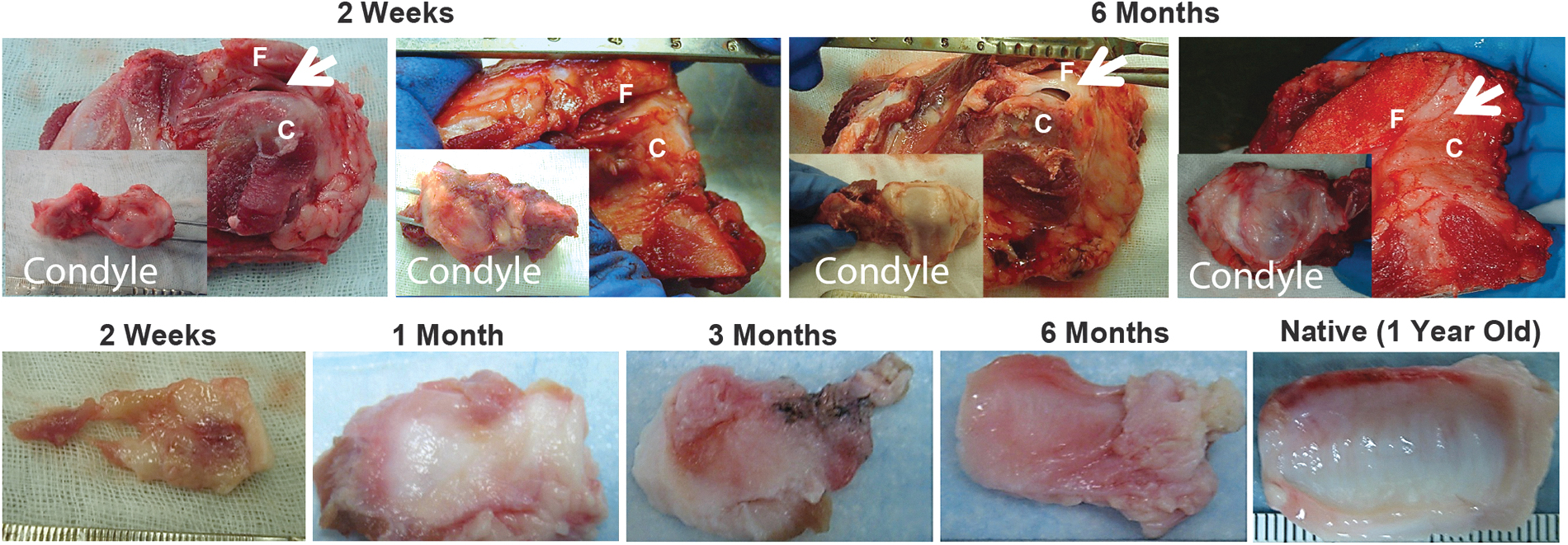
Gross morphologic results indicate rapid remodeling of the ECM device into disc-like tissue. Gross morphologic appearance of TMJ at 2 weeks and 6 months postimplantation is shown (F = fossa, C = condyle, and arrow = remodeled implant). Condylar surfaces were found to be smooth with no sign of pathology at 2 weeks and 6 months (top inserts), and device was rapidly remodeled at 2 weeks with tissue highly resembling native disc persisting at 6 months postimplantation (bottom). No new tissue formation was shown in control (unimplanted) joints. Color images are available online.
Evidence of incorporation of the rim of the scaffold material into the surrounding connective tissues and musculature was observed. No pathologic change in the articulating surface of the condyle was found. Synovial fluid was present during dissection of ECM-implanted joints, but not in empty control joints. The remodeled ECM discs increased in definition and robustness over the course of the 6-month study. By 6 months, the discs had significant definition and a concave, striated articulating surface on the condylar aspect, resembling the anterior-posterior alignment of collagen fibers in the intermediate zone of the native disc. Figure 3 shows the gross morphologic appearance at the 2-week and 6-month time points. No acute or chronic pathologic change in the condyle was observed following ECM implantation.
Histologic appearance
At 2 weeks postimplantation, the ECM bioscaffold showed a robust infiltration of host-derived mononuclear cells, with early signs of new ECM deposition throughout the remodeling scaffold material. A significant portion of the originally implanted material was recognizable within the site of implantation. By 1 month postimplantation, the mononuclear cell response was markedly decreased and a spindle-shaped cell population was present within the bulk of the scaffold material.
The remodeling implant material was observed to be slightly hypercellular at the articulating surfaces compared to native tissue, and limited vascularity was present. By 3 months, the ECM bioscaffold was characterized by a moderate spindle-shaped cell population within mostly mature collagenous tissue that showed an anterior-posterior alignment. Vasculature was decreased at the 3-month time point compared to the 1-month time point, and fewer cells were observed at the articulating surfaces of the ECM bioscaffold.
Few changes in the histologic appearance of the remodeled tissue were observed by 6 months postimplantation compared to the 3-month time point, suggesting that the majority of remodeling had occurred by 3 months postimplantation and that the newly formed tissue was maintained through the 6-month study period. By 6 months postimplantation, the neo-disc tissue was thicker than at either the 1- or 3-month time point.
Representative histologic images of the explanted disc tissues at each time point are shown in Figure 4. Additional investigation was performed at the peripheral attachments of the remodeled ECM bioscaffold to the other TMJ structures. Histologic evidence of contiguous TMJ disc-like tissue, connective tissue, and musculature was observed, suggesting that the ECM scaffold material integrated with surrounding tissues in a site-appropriate manner.
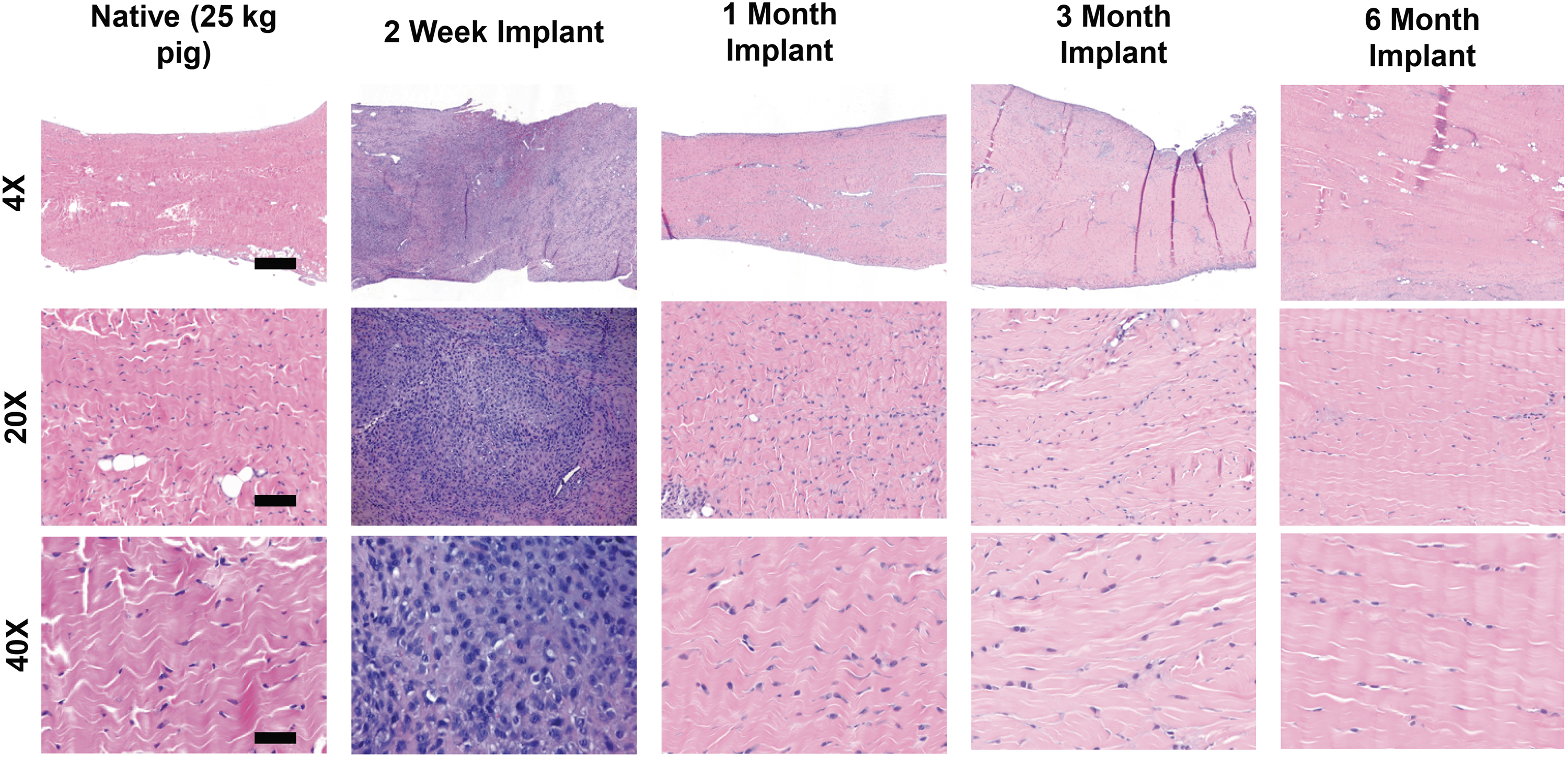
Histologic evaluation showed that the newly formed tissue highly resembles native disc tissue. Histologic appearance of native tissue at time of removal (T0), and the remodeled implant at 2 weeks, 1 month, and 6 months. The initially acellular device was rapidly infiltrated with cells by 2 weeks, and tissue resembling the native meniscus was formed by 1 month and persisted to 6 months postimplantation. Scale bars are 4 × = 500 μm, 20 × = 100 μm, 40 × = 50 μm. Color images are available online.
Biochemistry
The collagen content of native discs, remodeled ECM scaffolds, and preimplantation devices is shown in Figure 5. Approximated collagen content (% hydroxyproline/DW) was lower (p < 0.05) for the remodeled scaffolds at 1 month postsurgery when compared to all other groups. There were no significant differences in collagen content (%/DW) between TMJ discs at 3 and 6 months postsurgery and their age-matched controls. The preimplantation devices were only statistically different (p < 0.05) from the 1-month remodeled devices.
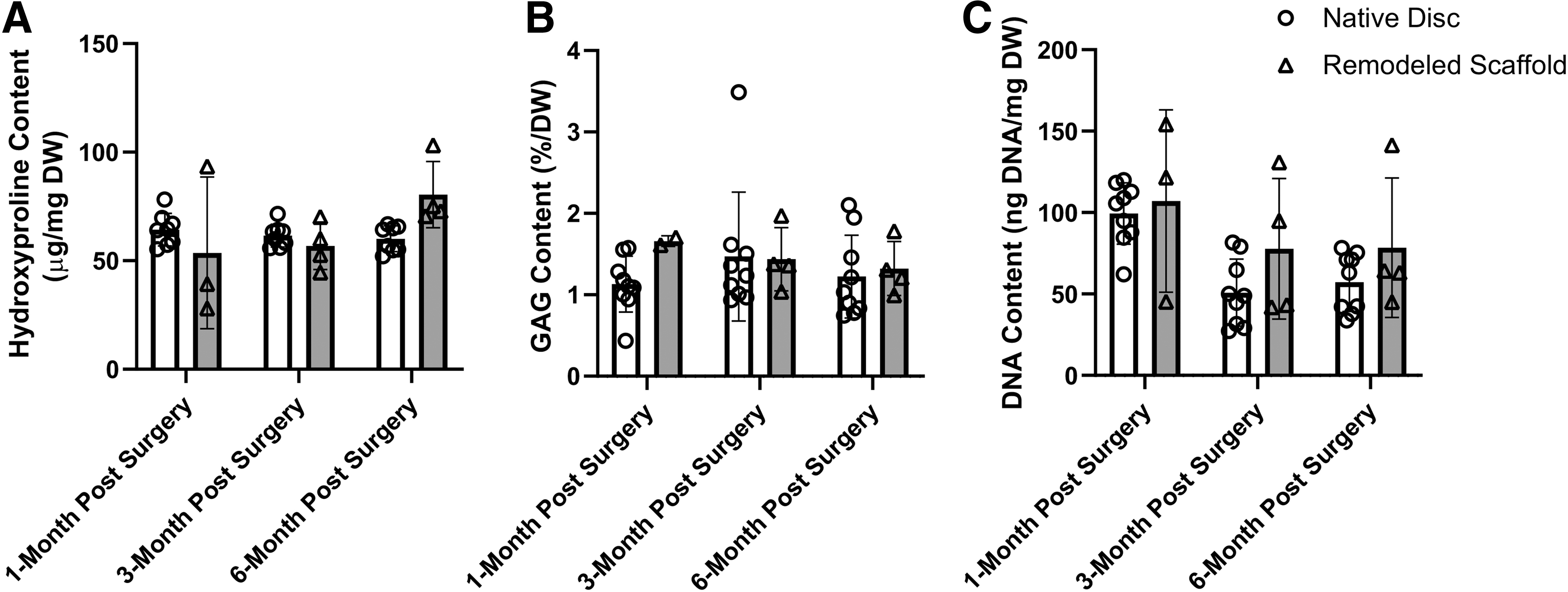
Biochemical content of age-matched control native discs and remodeled scaffolds at 1, 3, and 6 months postsurgery. All error bars represent standard deviation. Biochemical properties of
The collagen content of the condyles of the remodeled ECM side and contralateral native condyles is shown in Figure 6. There were no significant differences (p < 0.05) in approximated collagen content (%HYP/DW) between mandibular condyles at 1, 3, and 6 months postsurgery and their age-matched controls at 3, 6, and 9 months.
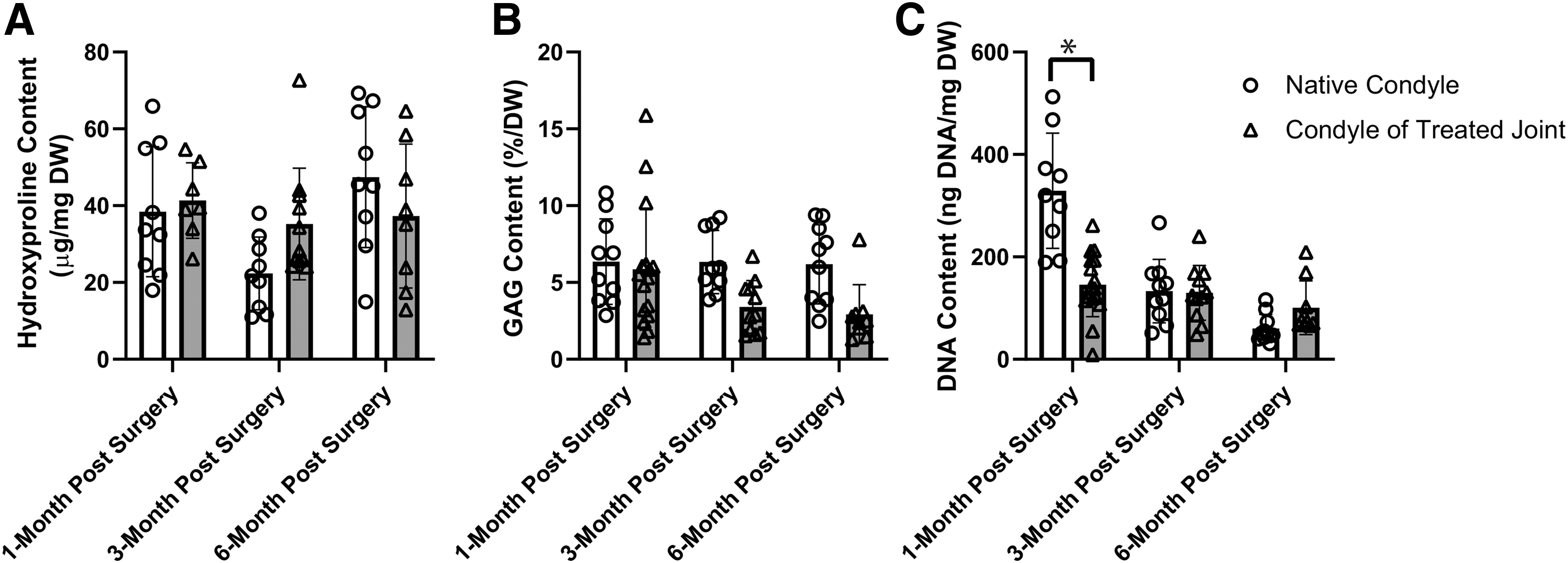
Biochemical content of age-matched control native mandibular condyle cartilage and the mandibular condyle cartilage treated with the ECM scaffold at 1, 3, and 6 months postsurgery. All error bars represent standard deviation. Significance of p < 0.05 between native mandibular condyle cartilage and the mandibular condyle cartilage treated with the ECM scaffold within each time point is denoted by *. Biochemical properties of
The GAG content of native discs, remodeled ECM scaffolds, and preimplantation devices is shown in Figure 5 There were no significant differences (p < 0.05) in GAG content (%/DW) between TMJ discs at 1, 3, and 6 months postsurgery and their age-matched controls at 3, 6, and 9 months. The preimplantation devices were not statistically different from any remodeled scaffold group. The GAG content of the remodeled ECM condyles and native condyles is shown in Figure 6. There were no significant differences (p < 0.05) in collagen content (%/DW) between mandibular condyles at 1, 3, and 6 months postsurgery and their age-matched controls at 3, 6, and 9 months.
The DNA content of native discs, remodeled ECM scaffolds, and preimplantation devices is shown in Figure 5. There were no significant differences (p < 0.05) in DNA content (ng/mg) between TMJ discs at 1, 3, and 6 months postsurgery and their age-matched controls at 3, 6, and 9 months. The preimplantation devices were not statistically different from any remodeled scaffold group. The DNA content of the remodeled ECM condyles and native condyles is shown in Figure 6. Mandibular condyles at 1 month postsurgery had less DNA (p < 0.05) than their age-matched controls at 3 months. There were no significant differences (p < 0.05) in DNA content (ng/mg) found between mandibular condyles at 3 and 6 months postsurgery and their age-matched controls at 6 and 9 months.
Tensile testing
Comparisons of the tensile peak stress (Fig. 7A), tensile modulus (Fig. 7B), and tensile strain (Fig. 7C) between remodeled scaffolds and native discs at each time point were determined. Ages in this figure are referred to as the age of the pig when euthanized. At 1 month postsurgery (4 months of age), the tensile modulus of native discs (n = 10) was higher than remodeled scaffolds (n = 3) (p < 0.05). At 3 months postsurgery (6 months of age), the tensile modulus of native discs (n = 9) was higher than remodeled scaffolds (n = 4) (p < 0.05). At 6 months postsurgery (9 months of age), there were no significant differences found between remodeled scaffolds (n = 4) and native discs (n = 9) in peak stress, modulus, or strain.
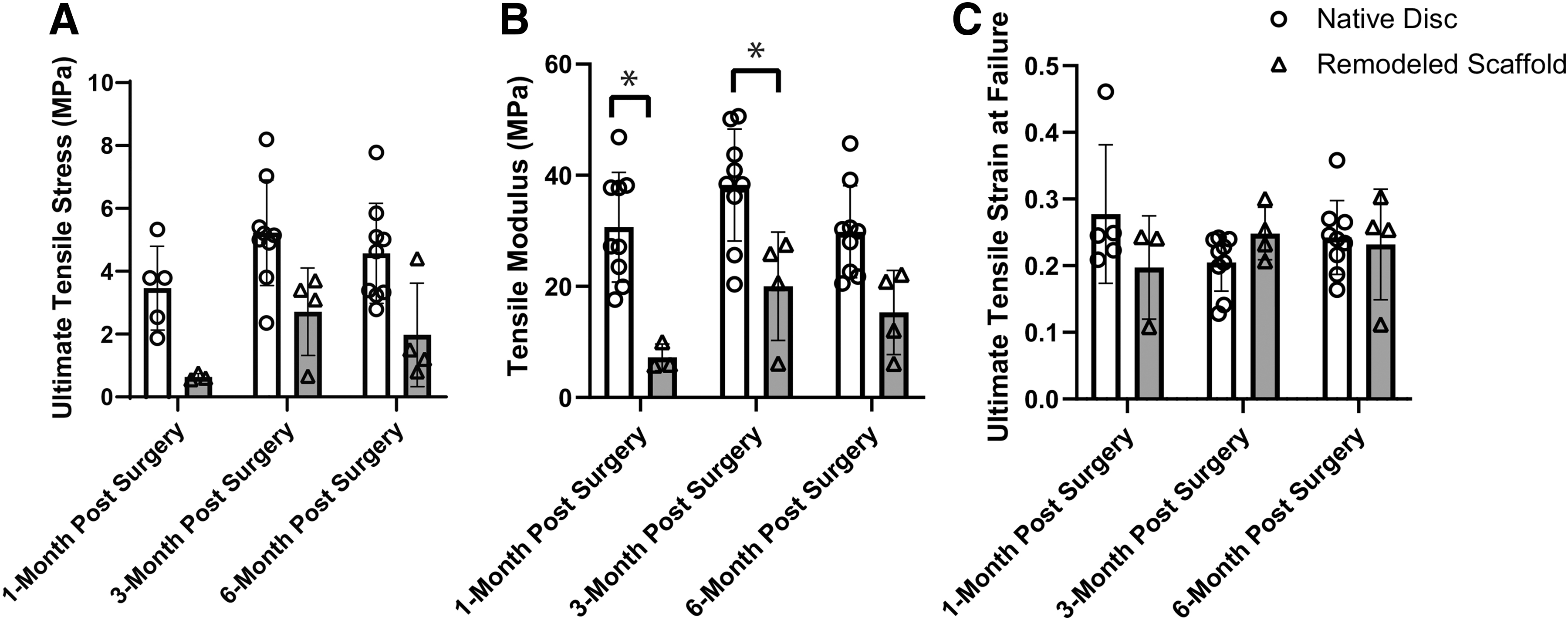
Tensile properties of age-matched control native discs and remodeled scaffolds at 1, 3, and 6 months postsurgery. All error bars represent standard deviation. Significance of p < 0.05 between native disc and remodeled scaffold within each time point is denoted by *. Tensile properties of
Compression testing
For the disc, the compressive peak stress at 30% strain step (Fig. 8A) of 9-month-old native discs was higher than 3-month-old native discs (p < 0.05). No statistical difference was found for peak stress between native discs and remodeled scaffolds at any time point. The compressive modulus at the 30% strain step (Fig. 8B) of 9- and 6-month-old native discs was higher than 3-month-old native discs (p < 0.05). No statistical differences were found for modulus between native discs and remodeled scaffolds at any time point.
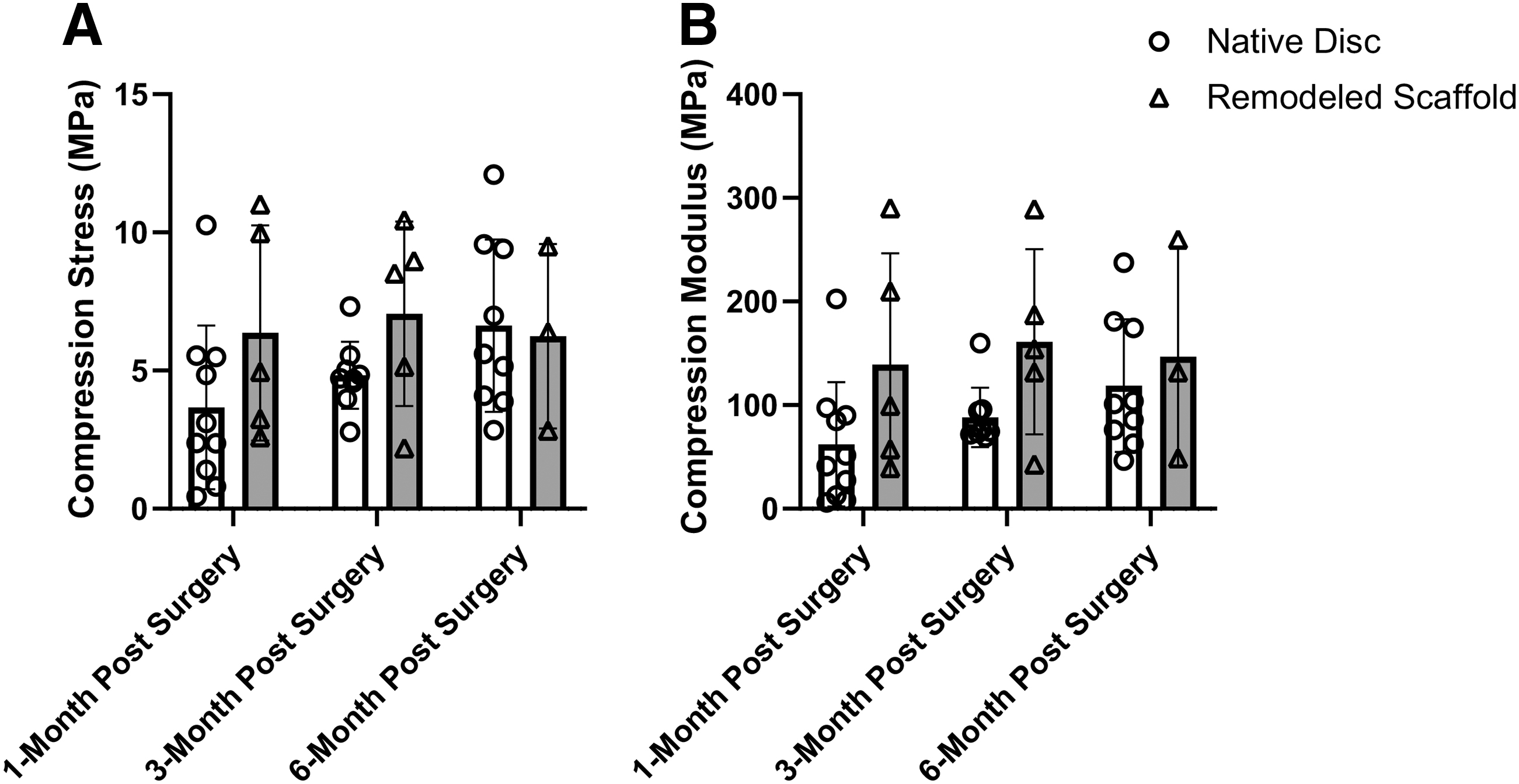
Compression properties of age-matched control native discs and remodeled scaffolds at 1, 3, and 6 months postsurgery at 10% strain step in unconfined stress-relaxation. All error bars represent standard deviation. Compression properties of
For the condyles, the compressive properties were determined for both treated condyles, defined as the condyles associated with the joint implanted with an ECM scaffold immediately following discectomy, and contralateral condyles, defined as the condyles on the contralateral side of the head, where no ECM scaffold was implanted following discectomy. The compressive peak stress at the 30% strain step (Fig. 9) of the contralateral condylar cartilage at 1 month was lower (p < 0.05) than its age-matched 3-month-old control condyle. No statistical differences were observed for the peak stresses of the 3- and 6-month treated and contralateral condylar cartilage and their age-matched controls at 6 and 9 months.

Compression properties of age-matched native mandibular condyle cartilage and the mandibular condyle cartilage treated with the ECM scaffold at 1, 3, and 6 months postsurgery, at 10% strain step in unconfined stress-relaxation. All error bars represent standard deviation. Significance of p < 0.05 between native mandibular condyle cartilage and the mandibular condyle cartilage treated with the ECM scaffold within each time point is denoted by *. Compression properties of
The compressive modulus at the 30% strain step (Fig. 9) of the contralateral condylar cartilage at 1 month was lower (p < 0.05) than its age-matched 3-month-old control condyle. No statistical differences were observed for the modulus of the 3- and 6-month treated and contralateral condylar cartilage and their age-matched controls at 6 and 9 months.
Discussion
The results of this study suggest that the ECM bioscaffold remodels in situ to form a site-appropriate replacement for the TMJ disc as soon as 3 months following implantation in a porcine model. The composition of the remodeled ECM bioscaffolds did not differ from native discs with respect to major constituents, including collagen, GAGs, and DNA content, by 3 months postimplantation. Anatomically relevant biomechanical properties of the remodeled ECM bioscaffolds also showed similarity to those of the native disc by 3 months.
Rapid remodeling and maturation of the ECM scaffold were shown in the juvenile farm pig model, an FI of 0.55 ± 0.08 for the remodeled ECM scaffold as early as 1 month postsurgery (Supplementary Fig. S1). By 3 months postsurgery, the FI reaches 0.74 ± 0.09, a value that is equivalent with near-native tissue function. This FI remained stable throughout the remodeling period until the 6-month postsurgical time point, with an FI of 0.69 ± 0.12.
No statistically significant changes were detected between these time points. It is important to note that the lack of changes in biochemical content over time when compared to changes in gross morphology, histologic appearance, and tensile properties seems to suggest that the bulk of the new tissue was deposited by 1 month postimplantation, after which the tissue started to mature, a phenomenon not detectable by biochemical assay. Future studies will observe collagen fiber alignment and amount of crosslinking of the collagen.
The high incidence (19 out of 48 scaffolds implanted) of implanted device displacement in treated joints is attributed to securing the ECM scaffolds to the zygomatic arch of a juvenile pig. It was observed that the suture attachment points of the ECM scaffold on the fossa migrate dramatically from 3 to 6 months of age. This lateral migration of the fossa likely dislocated the ECM scaffold from the joint space in many of the treated joints. Results of this study suggest that alternative fixation techniques must be employed in future studies using the juvenile pig model, such as attachment to the condyle.
The minipig is another possible choice for a porcine model, but the zygomatic arch also impedes surgical access to the disc in this species. It is recommended that an adult large animal model be considered, which does not have a skeletal obstruction to surgical access to the TMJ disc for tissue regeneration therapies, like the dog, sheep, or goat. 14 Whichever animal model is chosen, robust fixation approaches need to be developed and validated to ensure success of this therapy.
Protection of the mandibular condyle cartilage is a primary metric when evaluating the efficacy of a TMJ disc repair/replacement. The results of previous canine studies12,13 showed that implantation of an ECM bioscaffold effectively protects the mandibular condyle cartilage from degenerative changes postimplantation. No degenerative change was observed for either control, unimplanted, or bioscaffold-implanted groups in this study from a gross or biomechanical perspective. These findings suggest that the growing farm pig model may not be as sensitive to degenerative changes in the condylar surface postdiscectomy compared to skeletally mature canine model,12,13 in which significant degenerative changes were observed. For these reasons, in-depth histologic examination of the condylar surfaces was not performed; however, future studies could incorporate such testing to determine degenerative changes that may not be observable on gross examination.
While the mechanisms that lead to constructive remodeling of ECM bioscaffolds have not been fully elucidated, they are known to include rapid bioscaffold degradation with the release of bioactive degradation products and recently described matrix-bound vesicles.22,23 These degradation products have been shown to alter the phenotype of macrophages participating in the host remodeling response toward an alternatively activated, anti-inflammatory phenotype,24–29 which has been shown to be essential for constructive remodeling of ECM bioscaffolds.30–33 As previous studies with C14 radiolabeling have shown that the majority of the material degrades within the first month postimplantation,34–36 the hypothesized mechanism is that the degradation of the scaffold induced cell infiltration and changed the phenotype of macrophages, and new matrix was deposited, which then remodeled into a disc-like tissue.
The original tensile properties of SIS at the time of implantation were ∼50 MPa of ultimate tensile stress, 1400 MPa of tensile modulus, and 5% of ultimate tensile strain. These findings are in direct contrast to those observed for the remodeled tissue with about 0.6 MPa ultimate tensile stress, 7 MPa of tensile modulus, and 20% of ultimate tensile strain, at 1 month postimplantation. These results suggest, along with previous literature,34–36 that rapid degradation and remodeling of the initially stiff, acellular (Supplementary Fig. S2) SIS scaffold toward a TMJ disc-like tissue occur in this juvenile animal model.
A small number of in vivo studies have been performed to assess TMJ tissue engineering technologies.9,21,37 The smallest animal model in which a TMJ tissue-engineered therapy can be validated is the rabbit,9,37 and investigators have implanted 3D printed PCL-PLGA microsphere scaffolds seeded with allogeneic, synovium-derived MSCs. 9 While these studies showed feasibility by histological assessment, mechanical testing and articular surface protection will be required for clinical translation. Larger models, like the minipig or dog, allow for mechanical testing. One such study was recently performed in minipigs, where allogeneic costal chondrocytes were used as self-assembled, transplantable, cell-based, scaffold-free TMJ implants. 21 These implants were implanted into a partial thickness focal defect of the TMJ disc for up to 8 weeks.
The implants were found to be well integrated and the mechanical strength of the defects was more robust in the implant disc than in untreated defects. These findings provided proof-of-concept of a cell-based tissue-engineered disc replacement in an animal model; however, the requirement for autograft harvest coupled with long in vitro culture times represents significant challenges to clinical translation. The results presented in this study provide evidence for the efficacy of an off-the-shelf product to regenerate the entire TMJ disc in a large animal model.
There are several limitations to the interpretations of these findings. First, discectomy in the porcine model requires the use of juvenile animals. It is unclear what impact the use of a rapidly growing juvenile animal has upon the healing response and final quality of the remodeled tissue. Nevertheless, in all the joints that did not have a scaffold, no new tissue formation was observed, which suggests that the young animals still do not have the innate capacity to regrow the disc. When comparing the regeneration in the young pigs to our studies in skeletally mature canine models, the bulk of the regeneration seems to be more rapid, occurring by 3 months in the pig compared to 6 months in the canine, but with similar end results in properties. Second, in this study, it was not possible to investigate the function of the TMJ tissues under motion such as during mastication.
While the results demonstrate a remodeled tissue with native disc-like properties and correct anatomical position, future studies of joint kinematics during the course of remodeling could be performed to assess additional aspects of in vivo function. Finally, all ECM bioscaffolds were implanted into healthy joints immediately following discectomy, which is not representative of the clinical scenario of tissue dysfunction, inflammation, and degeneration. Thus, future work should study the remodeling of ECM bioscaffolds in an animal model of joint degeneration.
Conclusion
The results from this study suggest that an acellular ECM-based bioscaffold approach is a viable option for a long-term tissue-engineered graft replacement for the TMJ disc replacement following discectomy.
Authors' Contributions
B.N.B.: conceptualization, methodology, investigation, and writing—original draft. W.L.C.: conceptualization, methodology, investigation, and writing—review and editing. J.L.: investigation, formal analysis, and writing—original draft. S.T.L.: investigation, formal analysis, and writing—original draft. J.C.: methodology and investigation. A.J.A.: conceptualization, methodology, investigation, formal analysis, writing—original draft, and funding acquisition. S.F.B.: conceptualization, methodology, examination and interpretation of histology sections, writing—review and editing, project administration, and funding acquisition.
Footnotes
Acknowledgments
Portions of this work have been published previously in the PhD thesis of J.L.
Disclosure Statement
S.F.B. is an inventor on Patents for TMJ disc replacement, the rights for which have been licensed to ECM-Therapeutics, a company for which S.F.B. is the Chief Scientific Officer and an equity holder. B.N.B. and W.L.C. are inventors on Patents for TMJ disc replacement, the rights for which have been licensed to ECM-Therapeutics. J.L., S.T.L., J.C., and A.J.A. have no competing interests.
Funding Information
We gratefully acknowledge support from the National Institute of Health with grants RO1 DE022055 and 1F31 DE025810, and the National Institute of Biomedical Imaging and Bioengineering's Biomechanics in Regenerative Medicine T32 training grant, T32 EB003392.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.