
Abstract
Commercially available cultured epithelial keratinocyte sheets (KSs) have played an essential role in wound healing over the past four decades. Despite the initial uptake by the dermal elements, the survival rate of KS on the dermis-like tissue generated by conventional artificial dermis (AD) is low, making this method unsuitable for standard treatments. Therefore, an innovative AD such as collagen–gelatin sponge (CGS) that maintains the release of human recombinant basic fibroblast growth factor (bFGF) may promote wound healing. In this study, we examined whether combination therapy with KSs and CGS with bFGF (bFGF-CGS) could enhance KS survival by heterologous grafting by transplantation of human-derived KSs in an athymic nude rat wound model of staged skin reconstruction. The CGSs were implanted into skin defect wounds on athymic nude rats, which were then divided into two experimental groups: the bFGF group (CGSs containing bFGF, n = 8) and the control group (CGSs with saline, n = 8). Two weeks after implantation, human epithelial cell-derived KSs were grafted onto the dermis-like tissue, followed by assessment of the survival and morphology at 1 week later using digital imaging, histology (hematoxylin and eosin and Masson's trichrome staining), immunohistology (von Willebrand factor), immunohistochemistry (cytokeratin 1-5-6, Ki-67), and immunofluorescence (collagen IV, pan-cytokeratins) analyses. The bFGF group showed a significantly higher KS survival area (86 ± 58 mm2 vs. 32 ± 22 mm2; p < 0.05) and increased epidermal thickness (158 ± 66 μm vs. 86 ± 40 μm; p < 0.05) compared with the control group, along with higher dermis-like tissue regeneration, neovascularization, epidermal maturation, and basement membrane development. These results indicate that the survival rate of KSs in the dermis-like tissue formed by bFGF-CGS was significantly increased. Therefore, combination treatment of bFGF-CGS and KSs shows potential for full-thickness skin defect reconstruction in clinical situations.
Impact statement
This study highlights how using a combination of cultures, keratinocyte sheets, and collagen–gelatin sponge containing basic fibroblast growth factors can significantly improve cell survival in athymic nude rats with staged skin reconstruction. Our study makes a significant contribution to the literature because it highlights a novel and improved strategy for treating a very common condition such as skin wounds arising from many conditions. Clinical translation of this study may be useful for treating skin wounds.
Introduction
Modern advancements in research of wound healing and bioengineering technologies have led to the development of improved therapeutic modalities. Artificial dermis (AD), which functions as a scaffold, has been established as the standard treatment for expediting the wound healing process of full-thickness skin defects.1–3 AD has been used in numerous reconstructive surgeries to treat full-thickness skin defects caused by wounds from severe burns and acute trauma.4,5 In general, two-stage surgery is required to achieve wound closure and epithelialization: first, the AD is transplanted, and then, an autologous skin graft is placed on the top of the dermis-like tissue. Between the initial and second surgery, 2–3 weeks are required before the angiogenic AD is constructed. 6 Additionally, establishment of a culture technique for human keratinocytes by Rheinwald and Green and subsequent reports of clinical application to treat burn injuries have enabled cultured epithelial keratinocyte sheets (KSs) to play an essential role in wound healing for the past four decades.7–9 An example of a currently commercially available KS system includes the public health insurance system-approved (2009) cultured epithelial autograft called JACE® (Japan Tissue Engineering Co., Ltd., Aichi, Japan) for severe burn injuries in Japan. In contrast, the role of KSs in graft loss in full-thickness skin defects without dermal structures has not been examined, although some studies have shown suboptimal outcomes when using KSs in the clinic.10–17 Although combination therapy of KSs and AD appears to be effective for full-thickness skin defects such as severe burns, the survival rate of KSs on the dermis-like tissue generated by conventional AD is low. Hence, combination therapy has not been established as a standard treatment in this field.8,18
In 2008, Morimoto and colleagues 19 developed an innovative AD consisting of a collagen–gelatin sponge (CGS) containing 10% alkali-treated gelatin having a drug delivery system for basic fibroblast growth factor (bFGF). In Japan, human recombinant bFGF (Fiblast® Spray; Kaken Pharmaceutical, Tokyo, Japan) has been commercially available since 2001 and is used as a highly effective treatment for chronic skin ulcers, skin avulsion injuries to the extremities, and second-degree burns.20,21 Furthermore, combination therapy with conventional AD and bFGF has been reported, with bFGF applied multiple times during the course of one treatment.22,23 As its half-time is very short in vivo, bFGF in its free form cannot remain bioactive over a prolonged period. 19 In contrast, CGS can sustain the release of bFGF for more than 10 days to promote angiogenesis and engraftment of the inactivated dermis much earlier than with the conventional AD. Therefore, combination therapy with CGS and bFGF (bFGF-CGS) may accelerate wound healing.24–27 We previously demonstrated favorable outcomes in promoting epithelialization following reconstructive surgery with bFGF-CGS to treat acute full-thickness skin defects, such as digital amputation, deep dermal burn, or open fracture. 28
Based on these findings, we predicted that bFGF-CGS, which can steadily deliver bFGF, would promote angiogenesis and the regeneration of dermis-like tissue, leading to an increased survival rate of KSs grafted on the AD. Therefore, in this study, we evaluated the potential of combination therapy of KSs and bFGF-CGS by heterologous grafting by transplanting human-derived KSs on bFGF-CGS in a nude rat wound model of staged skin reconstruction.
Materials and Methods
This study was approved by our Institutional Animal and Ethics (human tissue procurement) Committees and performed in accordance with the Declaration of Helsinki (June 1964) and subsequent amendments.
Impregnation of bFGF-CGS
We used a CGS (Pelnac Gplus®, Gunze, Kyoto, Japan), a commercially available AD in Japan. This AD is a modified version of the conventional bilayered AD and consists of an upper silicone sheet with a thickness of 0.12 mm and lower collagen sponge with alkali-treated gelatin with a thickness of 3 mm (Fig. 1). We prepared the bFGF-CGS by applying a solution of human recombinant bFGF (Fiblast Spray; Kaken Pharmaceutical) impregnated at a concentration of 7–14 μg/cm2 ∼10 min before application (Fig. 2A, B). We used a confirmed safe and effective dose of bFGF, which was the same as that used with CGS for acute and chronic wound healing as demonstrated in clinical studies.24,28

bFGF-impregnated CGS (bFGF-CGS).

Schematic overview of experimental procedures and intraoperative findings.
Preparation of human KSs
Cultured epithelial KSs derived from human epithelial cells (JACE, Japan Tissue Engineering Co., Ltd.) were prepared using the Rheinwald–Green method with human epithelial cells, followed by infection screening. First, human keratinocytes were subcultured once or twice and cryopreserved at −150°C until transplantation. The keratinocytes were thawed and cultured on a feeder layer until confluent, followed by detachment of the cell sheets from the flasks with dispase to prepare the grafts.
Surgical procedure and experimental design
All animal care and handling procedures were performed in accordance with the principles of laboratory animal care of the Animal Experimentation Committee of Tokyo Women's Medical University. F344/NJcl-rnu/rnu athymic nude male rats (n = 16, 8 weeks old, ∼200–250 g), obtained from CLEA, Inc., (Tokyo, Japan), were used in this study. In rats anesthetized with 2% isoflurane via a nasal mask attached to a Univentor 400 Anesthesia Unit (Narcobit-E; Natsume Seisakusho, Tokyo, Japan), the back skin was excised while keeping the dartos fascia intact, and a 40-mm-long, 30-mm-wide full-thickness skin rectangle defect was made using surgical scissors. The rats were divided into two experimental groups: (1) bFGF group treated with CGSs impregnated with bFGF (n = 8) and (2) control group treated with CGSs prepared with saline and no bFGF (n = 8). The CGSs in each group were cut to 40 mm long, 30 mm wide, sutured using 5–0 nylon, and fixed using the tie-over dressing method onto the skin defect wound (Fig. 2B). Two weeks after implantation, formation of dermis-like tissue within the grafted CGS was visually confirmed by removing the silicone sheet by placing the rats under inhalational anesthesia (Fig. 2C). The KSs were cut into a square 20 mm long on each side and grafted onto the central portion of the dermis-like tissue (Fig. 2D), after which the wound was covered with ointment-containing gauze cut to a 35-mm diameter circle and a 35-mm petri dish (BD Falcon). As described previously, KSs, which were one size smaller, were transplanted onto the AD to accurately measure the engraftment area by demarcating the transplanted and nontransplanted areas.29,30 The top and side walls of the dish were drilled with holes and stitched in an eight-way pattern around the skin.
Graft survival area and epidermal thickness analysis
One week after KS transplantation, the rats were anesthetized and the dressings were removed. The wounds were photographed with a standard digital camera, and the graft survival (“take”) area in each group was calculated using the ImageJ Software version 1.80 (National Institutes of Health, Bethesda, MD). The graft survival area in each group was measured by three independent double-blinded observers experienced in skin surgery. Skin specimens, including the implanted CGS and KSs, were harvested using scalpels and scissors and then sectioned. The cut sections, each ∼5 μm thick and obtained from the wound center, were stained with hematoxylin and eosin (HE) according to standard protocols and examined under a light microscope. Four 200 × magnification images of grafted KSs were vertically divided into three equal segments, and the epidermal thickness at the center of each segment was calculated using the ImageJ Software to obtain the mean of the three measurements.
Evaluation of thickness of dermis-like tissue
The 5-μm-thick sections obtained from the wound center were stained with Masson's trichrome according to standard protocols and examined by light microscopy. Two 50 × magnification images of grafted CGS over the entire wound area were vertically divided into five equal segments, and the thickness of the newly formed dermis-like tissue was calculated using the ImageJ Software. The mean of 10 measurements was calculated.
Evaluation of newly formed capillaries in dermis-like tissue
Immunohistological staining with anti-von Willebrand factor antibody was performed to detect newly formed capillaries in the dermis-like tissue. After deparaffinization and rehydration, the sections were incubated in phosphate-buffered saline (Life Technologies, Carlsbad, CA) with 0.1% trypsin (Vector Laboratories, Burlingame, GA) for 15 min at 37°C for antigen retrieval. An anti-von Willebrand factor rabbit polyclonal antibody (1:500; ab6994; Abcam, Cambridge, United Kingdom) and anti-rabbit IgG goat polyclonal antibody (No. 424144; Nichirei Biosciences, Inc., Tokyo, Japan) were used as secondary antibodies for 30 min. This incubation step was followed by color detection using 3,3-diaminobenzidine tetrahydrochloride for 5 min at room temperature. Finally, counterstaining was performed with hematoxylin. An area 500 × 500 μm in size in each image was fixed, the number of newly formed capillaries was counted, and the area of newly formed capillaries was measured manually using the ImageJ software. Three measurements per slide at different fields over the entire wound area were acquired for quantification, and the results are expressed as the average value.
Immunofluorescence staining of CGSs of KS grafts
Double immunofluorescence staining for collagen IV and pan-cytokeratin was performed to investigate the extent of protein expression in the basement membrane of the grafted KSs. Transverse sections (4-μm-thick) prepared with a sliding microtome were positioned on glass slides. The sections were then incubated with blocking solution (Blocking One; Nacalai Tesque, Kyoto, Japan) for 10 min. For immunohistochemistry, anti-human-multi-cytokeratin monoclonal antibody (No. NCL-L-AE1/AE3–601; Leica, Wetzlar, Germany) and anti-human collagen type IV polyclonal antibody (No. ab6586, Abcam) were used as primary antibodies (1/500 dilution). In addition, fluorescently labeled secondary antibodies (cocktail of Alexa488- and 594-conjugated species-specific secondary antibodies; Life Technologies) were used (1/500 dilution). The stained sections were mounted with undiluted ProLong® Gold Antifade reagent containing 4′,6-diamidino-2-phenylinode (P36935; Molecular Probes, Eugene, OR). The slides were observed under a confocal laser scanning microscope (LSM710; Carl Zeiss, Oberkochen, Germany).
Immunohistochemistry of keratinocytes of KS grafts
Immunohistochemistry was performed to analyze epidermal maturation and to detect proliferating cells on the grafted KSs in each group. Transverse sections (4-μm-thick) prepared with a sliding microtome were mounted on silane-coated glass slides. The sections were successively incubated with blocking solution (Blocking One; Nacalai Tesque) for 10 min, anti-human cytokeratin 1 monoclonal antibody (No. NCL-CK1; Leica), anti-human cytokeratin 5 monoclonal antibody (No. NCL-CK5; Leica), anti-human cytokeratin 6 monoclonal antibody (No. NBP2–34232; Novusbio, Littleton, CO), or anti-human Ki-67 antibody (No. M7240; DAKO, Glostrup, Denmark) overnight at 4°C, and secondary antibodies (No. 414191; Nichirei Biosciences, Inc.) for 30 min. Chemiluminescent reactions were performed using 3,3-diaminobenzidine tetrahydrochloride for 5 min at room temperature followed by brown color detection.
Statistical analysis
The results are expressed as the mean ± standard deviation, and p values of <0.05 were considered to indicate statistical significance. In addition, the thickness and survival areas of KSs, thickness of the newly formed dermis-like tissue, and number and area of the newly formed capillaries in both groups were analyzed using unpaired Student's t-test in GraphPad Prism version 6.00 Software for Windows (GraphPad, Inc., La Jolla, CA).
Experiments
KSs grafted on bFGF-CGS show higher survival and thickness
At 7 days after transplantation, the surface of the KSs in the bFGF group appeared as horny. In contrast, the control group had a sparse and indistinct horny surface in the middle of the transplanted area (Fig. 3A, B). At low magnification (50 × ), HE staining of the sections from the bFGF group showed a thick and uniform epithelial structure, whereas that from the control group had a nonuniform epithelial structure with liquefaction degeneration (Fig. 3C, D). At high magnification (200 × ), HE staining revealed the presence of stratified squamous epithelium and homogeneous keratinized layers in the bFGF group, in contrast to the unclear epithelial structures and parakeratosis in the control group (Fig. 3E, F). At 1 week after grafting onto the CGS, the survival area of keratinocytes in the grafted area was twofold higher in the bFGF group than in the control group (86 ± 58 mm2 vs. 32 ± 22 mm2; p < 0.05) (Fig. 3G). Additionally, the epidermal thickness observed by HE staining was significantly greater in the bFGF group than in the control group (158 ± 66 μm vs. 86 ± 40 μm; p < 0.05) (Fig. 3H).

Macroscopic view, pathological features, graft survival area, and epidermal thickness of KSs of transplantation area 7 days after transplantation.
Evaluation of newly formed dermis-like tissue and capillaries
Masson's trichrome staining revealed that the thickness of the regenerated area of the dermis-like tissue in the bFGF group was greater than that in the control group (675 ± 235 μm vs. 446 ± 217 μm), although the difference was not significant (Fig. 4A, B). von Willebrand factor staining revealed that the number of newly formed capillaries in the bFGF group (11.1 ± 1.5) was significantly higher than that in the control group (9.8 ± 0.9; p < 0.05). Furthermore, the gross area of the capillaries in the bFGF group was significantly larger than that in the control group (7039 ± 1594 μm2 vs. 4404 ± 1514 μm2; p < 0.01) (Fig. 4A, B).

Newly formed dermis-like tissue and capillaries.
KSs on bFGF-CGS show higher epidermal maturation and basement membrane development
Cytokeratin 1, which marks the epithelial cell layer above the stratum spinosum, showed lower and scattered expression in the control group than in the bFGF group.
Positive staining for cytokeratin 5 (pan-epidermal cell marker) and cytokeratin 6 (a marker of migrating epithelial cells) was observed in both groups. However, the bFGF group showed a thicker and more diffused positive layer of epithelial cells than the control group. Moreover, Ki-67, which reacts with basal cells and proliferating cells, was sparsely positive on the basement of the control group, whereas it showed dense positive staining in the bFGF group (Fig. 5).

Immunohistochemistry of keratinocytes. Cytokeratin 1 (a marker of the epithelial cell layer above the stratum spinosum) expression was less scattered in the control group than in the bFGF group. Cytokeratin 5 (pan-epidermal cell marker) and cytokeratin 6 (a marker of migrating epithelial cells) expression was thicker and more diffused in the epithelial cell layer in the bFGF group than in the control group. Ki-67 (a marker of basal cells) was sparsely positive on the basement of the control group. In contrast, it was uniformly and densely positive in the bFGF group. The scale bars represent 500 μm. Color images are available online.
Double immunofluorescence staining to detect the green fluorescence signal revealed that collagen IV was widely expressed on the basal side, whereas red fluorescent pan-cytokeratin staining was stronger and more homogeneous in the bFGF group. In contrast, there was slight expression of collagen IV and a lack of uniformity in pan-cytokeratin staining in the control group (Fig. 6).
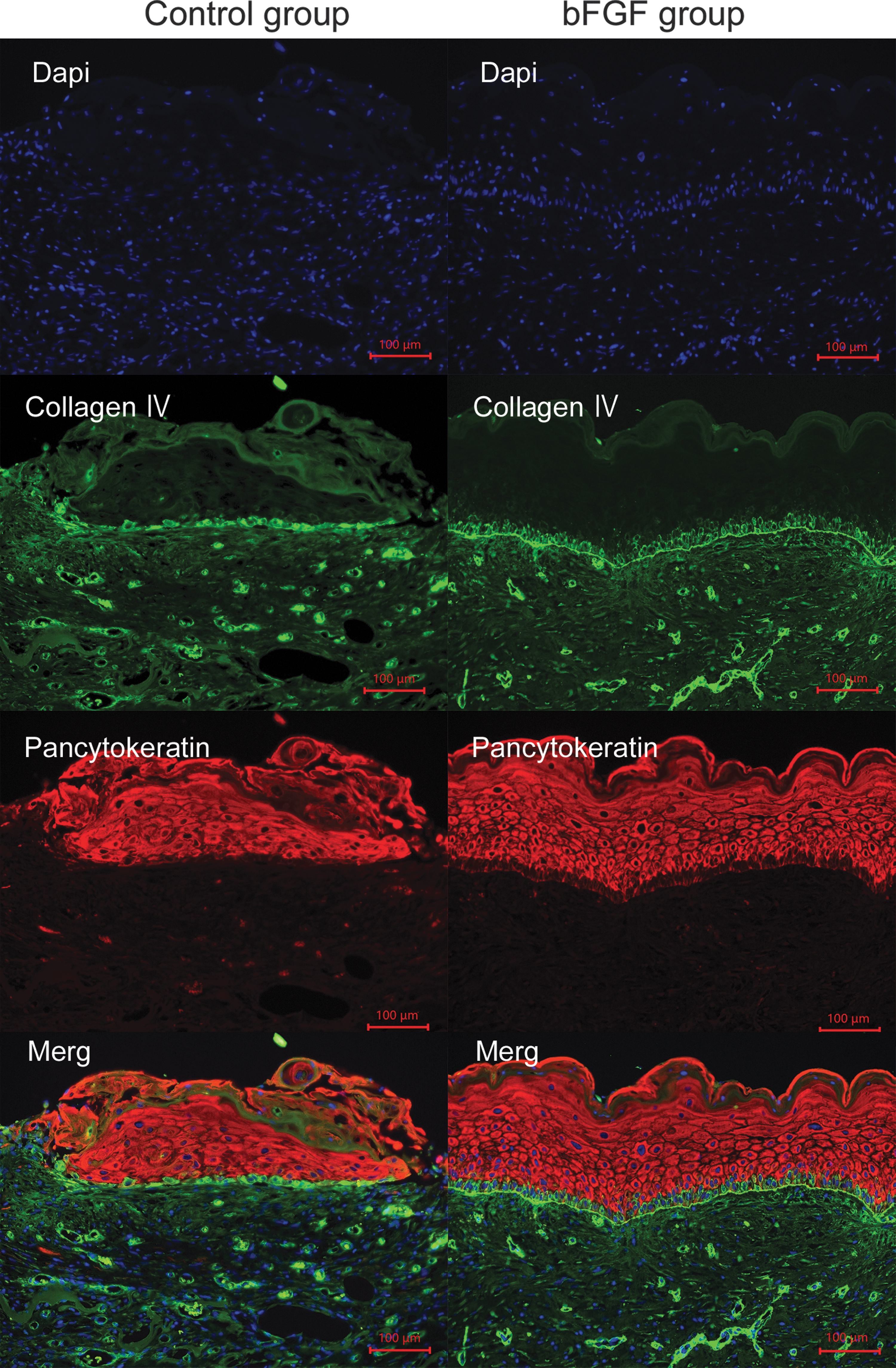
Immunofluorescence staining of the KSs grafted on the dermis-like tissue. Double immunostaining with anti-pan-cytokeratin (red) and anti-collagen IV (green) antibodies. The scale bars represent 100 μm. Color images are available online.
Discussion
Our results indicate that combination therapy with KSs and bFGF-CGS provides superior and more favorable outcomes in two-stage wound repair and skin reconstruction than conventional AD. The key findings of this study can be summarized as follows: (1) our rat model showed that the survival area (“take”) of KS grafts on the dermis-like tissue generated by bFGF-CGS was twofold larger than that generated by conventional AD; (2) bFGF-CGS induced the regenerated area of the dermis-like tissue to be thicker and increased the number of capillaries compared with the effects of saline treatment; and (3) bFGF-CGS showed higher epidermal maturation, with the basement membrane resembling the normal skin architecture compared with the control group.
According to a recent systematic review, the take rate associated with using cultured epithelial autografts in patients with burn injuries varies from 0% to 100% and that these autografts are unstable. In contrast, using the standard therapy of co-application of KSs with autologous skin grafts achieves consistent take rates of 73–96%. 31 Furthermore, early excision and allograft temporization before KS grafting are thought to minimize the risk of infections and improve KS survival in patients with burns. As described by Cuono et al., cadaver allografts have been adopted in more than two-thirds of studies.31,32 However, the limitations of allograft supplements have led to the application of AD with KS for wound bed preparation in one-third of patients suffering from burns in Japan. The KS take rate on the AD has a mean value of 43% without an autograft and 74% with an autograft. 33 Additionally, the lack of dermal elements, such as basal lamina and anchoring fibrin, causes long-term fragility of the grafted KSs on AD. Therefore, new AD grafting methods are required to improve the KS take rate.
Several studies have revealed that bFGF promotes reepithelization in the wound healing process by stimulating keratinocyte proliferation.34–36 However, the precise mechanism of bFGF in the epidermis and its interaction with other growth factors in promoting keratinocyte growth remain unclear. Koike et al. 37 demonstrated that treating wounds with FGF2 promoted keratinocyte epithelial–mesenchymal transition, accelerating wound closure. In this process, keratinocytes shift from a polarized cuboidal morphology to a more spindle morphology with an extended cytoplasm to rapidly migrate and close wounds. Therefore, wound edge keratinocytes form thickened and multilayered epithelia and migrate individually toward the wound center.
We hypothesized that engrafted KS further proliferated via this mechanism and that epithelialization was expanded, resulting in a significant difference from the control group. The ability of fibroblasts to synthesize the basement membrane is well known. 38 Fibroblasts stimulate the expression of basement membrane components, leading to the formation of a basement membrane zone, suggesting that fibroblasts produce laminin and type IV and VII collagens or influence the effects of keratinocytes on basement membrane formation through a keratinocyte–fibroblast interaction. 38 Yamabe et al. 39 reported that bFGF stimulates type IV collagen production in cultured human fetal mesangial cells in dose- and time-dependent manners via a transforming growth factor-β-dependent mechanism. Collagen IV and laminin are important factors affecting the shape of basal cells. Collagen IV and laminin 5 are necessary to adhere to epithelial keratinocytes and dermal matrix in reconstructing the human oral mucosa. 40 Matsumine et al. 30 demonstrated that KSs prepared with temperature-responsive culture dishes have significantly enhanced survival because the basement membrane and intercellular adhesion proteins are preserved. In addition, Soejima et al. 41 attempted to promote basement membrane protein production at the recipient site by treating AD with mesenchymal stem cells to promote post-cultured epithelial autograft production and the deposition of basement membrane proteins, including collagen IV, laminin-5, and anchoring fibrils, at the dermal–epidermal junction. We predicted that bFGF could also promote the synthesis of basement membrane proteins during the generation of dermis-like tissue after AD grafting.
The lack of a vascular plexus leads to slower vascularization of KSs because of neovascularization compared with vascularization of the split-thickness skin autograft by inosculation. 41 Hence, topical nutrition is essential during neovascularization, which may directly promote keratinocyte survival and viability by providing nutritional support and indirectly releasing angiogenic compounds by viable keratinocytes. 42 Supp and Boyce 43 reported that overexpression of vascular endothelial growth factor in genetically modified cultured skin substitutes enhances early vascularization, contributing to greater graft stability and improved engraftment of cultured skin. Furthermore, FGFs potentially induce angiogenesis via their powerful proliferative effects on endothelial cells and fibroblasts and facilitate endothelial cell migration by regulating proteolysis and adhesion molecules. 44 bFGF was reported to similarly promote angiogenesis in CGS applications, particularly with a peak at the optimal concentration of 7 μg/cm2. 25 In our study, the number of newly formed capillaries and their gross area in the bFGF group were significantly higher than those in the control group. This result suggests that bFGF-CGS accelerates angiogenesis and dermis-like tissue formation, leading to improved KS neovascularization and a higher take rate.
The main limitation of this study is that we used only an immune-deficient rodent model, xenologous cell grafts, and surgical skin to support our method. Therefore, further clinical trials of patients and pathological conditions are required to validate our method.
In conclusion, we confirmed that the survival rate of KSs was significantly improved in the dermis-like tissue formed by bFGF-CGS. Our results suggest that combination treatment with bFGF-CGS and KSs can be used for full-thickness skin defect reconstruction in clinical situations. In this study, we analyzed the promoting effects of KS engraftment in a xenograft model in which human KSs were transplanted to rats. Additional studies are needed to evaluate the wound healing effect of KSs on bFGF-CGS with a rat “allograft” model.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the GUNZE Foundation, Japan, Japan Tissue Engineering Co., Ltd. (J-TEC), Japan, and Institute of Laboratory Animals (ILA), Tokyo Women's Medical University.