
Abstract
Osteoarthritis (OA) and chronic low back pain due to degenerative (intervertebral) disc disease (DDD) are two of the major causes of disabilities worldwide, affecting hundreds of millions of people and leading to a high socioeconomic burden. Although OA occurs in synovial joints and DDD occurs in cartilaginous joints, the similarities are striking, with both joints showing commonalities in the nature of the tissues and in the degenerative processes during disease. Consequently, repair strategies for articular cartilage (AC) and nucleus pulposus (NP), the core of the intervertebral disc, in the context of OA and DDD share common aspects. One of such tissue engineering approaches is the use of injectable hydrogels for AC and NP repair. In this review, the state-of-the-art and recent developments in injectable hydrogels for repairing, restoring, and regenerating AC tissue suffering from OA and NP tissue in DDD are summarized focusing on cell-free approaches. The various biomaterial strategies exploited for repair of both tissues are compared, and the synergies that could be gained by translating experiences from one tissue to the other are identified.
Impact statement
Joints affected by osteoarthritis (OA) and degenerative (intervertebral) disc disease (DDD) share similarities in tissue composition and in the degenerative disease processes. This has led to the development of similar tissue engineering approaches to repair the articular cartilage (AC) and the nucleus pulposus (NP), in the context of OA and DDD, such as injectable hydrogels. In this review, recent developments in injectable hydrogels for repair of AC and NP tissues are summarized, biomaterial strategies are compared, and synergies are identified focusing on cell-free approaches. The summarized developments are expected to inspire more cross talk between both research fields.
Introduction
Currently, degenerative joint diseases like osteoarthritis (OA) and degenerative (intervertebral) disc disease (DDD) are two of the major causes of disabilities worldwide. On one hand, low back pain affects millions of people and leads to a high socioeconomic burden.1,2 In the Netherlands alone circa 2 million patients suffer from this disease. 3 One of the major causes for low back pain is intervertebral disc (IVD) degeneration. Due to the multifactorial etiology of the degenerative process, including biomechanical, biophysical, and cellular changes within the disc,4–7 treatment options are limited and need to satisfy a complex set of parameters.
On the other hand, OA is a progressive disease characterized by degeneration of articular cartilage (AC), the development of osteophytes, and mild to moderate inflammation, resulting in pain and loss of joint function. 8 In the Netherlands, more than 1.5 million patients suffer from this disease in one or multiple joints. 9 Currently, there are no approved therapeutics that can reverse, halt, or even just decelerate the disease progression. 10 Although OA occurs in diarthrodial or synovial joints and DDD occurs in amphiarthrodial or cartilaginous joints, the similarities are striking (Fig. 1).
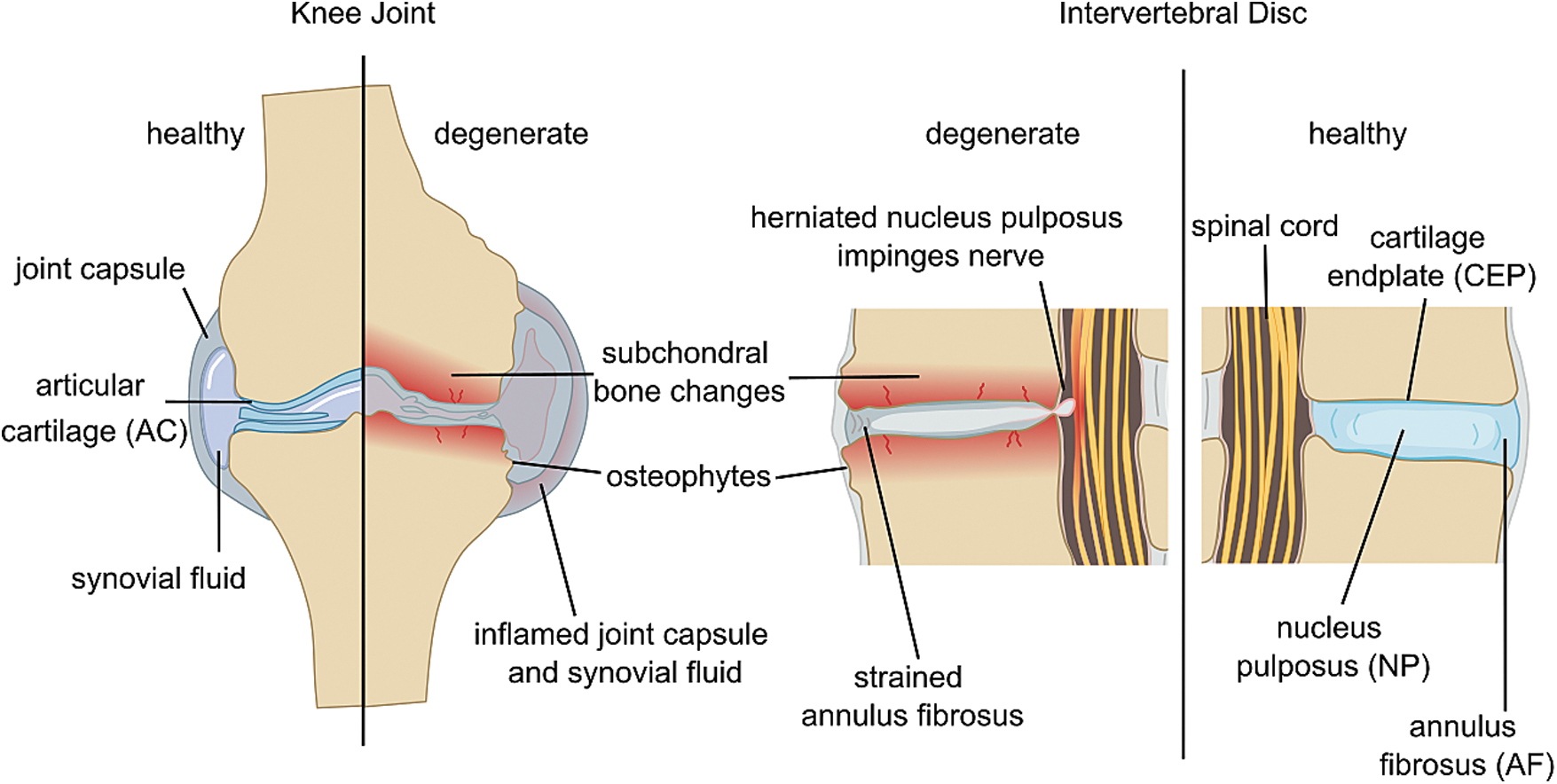
Changes in knee joint OA and DDD follow similar trends. OA, osteoarthritis; DDD, degenerative (intervertebral) disc disease.
The details of similarities and differences between OA and IVD degeneration have been reviewed elsewhere, 11 but in general, both joints have commonalities in their degenerative processes during disease. In both cases, multiple joint tissues fail, and the cross talk between them contributes to the vicious circle of degeneration leading eventually to disease. This cross talk among the involved tissues (e.g., between AC, subchondral bone, and the synovial membrane in diarthrodial joints) further precipitates tissue damage, degeneration, and inflammatory processes,12–14 leading to structural and biomechanical dysfunction and, ultimately, impaired patient mobility. The latter relates primarily to morbid pain, originating from the joint, with daily life activities.
Synovial joints, for example, the knee joint, have a synovial joint cavity filled with synovial fluid that separates the adjacent bones. The synovial fluid acts as a lubricant allowing for swift and frictionless movement, nourishes the AC that covers the apophyseal bony ends, and is a medium for cross talk between the joint tissues. In contrast, the IVD is a cartilaginous joint and lacks a synovial cavity with fluid, although the tissue of the IVD is rich in interstitial fluid. The adjacent vertebral bodies are directly connected by the interposed IVDs. The core of the IVD, the nucleus pulposus (NP), is a porous and viscoelastic gel contained by the fibrous annulus fibrosus (AF) and the cartilage endplates (CEPs) that interface centrally to the vertebral bodies (Fig. 1).
In the following subsections, the similarities in tissue composition in the AC and in the NP are presented, and the degenerative processes during disease are compared.
AC and NP tissue composition
AC and IVD are composed of tissues rich in extracellular matrix (ECM) with relatively low cell densities. The tissues are composed of one cell type which is specific to the particular tissue: that is, chondrocytes in AC and CEP, notochord-derived cells in NP, and tenocyte-like cells in AF. Although sparse, they are responsible for maintaining the ECM from which these tissues/organs derive their unique functional properties. In particular, the ECM of AC and NP is rich in proteoglycans entrapped within a network of collagen fibers. The main proteoglycan is aggrecan, made up of a protein core to which a multitude of negatively charged sulfated glycosaminoglycan (GAG) side chains is attached. Furthermore, because aggrecan binds to a hyaluronic acid backbone, these are entangled around, bound to, and immobilized by the collagen fiber network.
The GAG in turn bind cations and are responsible for large water uptake of AC and NP by osmosis. In both AC and IVD, this osmotic potential allows for the creation of a load bearing internal swelling pressure because the sGAG-rich ECM is restricted from swelling by the collagen fiber network. In the case of AC, these are the collagen-II fibers arranged in the Benninghoff arcades, whereas in the IVD the swelling of the NP is restricted by the collagen-II and collagen-I rich lamellae of the inner and outer AF, respectively.
Both synovial joints and the IVD are loaded during daily life activities. Some of the compositional and structural differences between AC and IVD tissues relate to differences in these loads. The healthy NP has a much higher ratio of GAG:collagen (i.e., 27:1) compared to AC (1:2.5). 15 Despite these differences, the unloaded swelling pressures and the load bearing stresses/pressures in AC and NP are comparable.16,17 The other major difference is the loading direction. In AC this is mostly unidirectional compression, while the NP is exposed to tension, compression, and shear load in 6 degrees-of-freedom. This complex loading thus requires the complex architecture of the AF in addition to the simple but mobile NP compared to the relatively uniform structure of AC.
Physiologically, there are also some similarities between AC, NP, inner AF, and CEPs. They are all aneural avascular tissues which rely for their nutrition on nutrient diffusion, with the core of the IVD being the most challenging environment from a nutritional perspective. The NP is nourished through diffusion of nutrients 18 coming in from the small capillaries superficially penetrating into the outer annulus and through the vertebral endplates. 19 This limited nutrition further contributes to an ever harsher tissue environment once degeneration sets in, where low oxygen tension and low levels of nutrients facilitate high local concentrations of lactic acid with negative effects driving further tissue catabolism. 20 Furthermore, tissue regeneration requires high metabolic activity, which is compromised by low oxygen and low nutrients. This restricted solute transport environment also applies to the avascular AC, which is nourished by diffusion through the synovial fluid and the subchondral bone.
Cartilage degeneration: AC versus NP
In both AC and NP, degeneration follows a similar process; GAGs are lost from the tissue altering the ratio of GAG:collagen. In the NP, a marked reduction of GAG:collagen ratio is observed for the degenerate tissue compared to the healthy NP (5:1 vs. 27:1, respectively). 15 In the AC case, the loss of GAGs precedes the loss of collagens and is much less pronounced than in the NP and primarily represented by qualitative changes. 21 Nonetheless, in end-stage OA disease, both GAG and collagen are reduced and experience higher turnover rates 22 resulting in bone-to-bone contacts without a cartilage intermediate.
The loss of GAGs results in a loss of swelling pressure and more compressive straining of the collagen fibers and their eventual damage, causing even further loss of GAGs. In addition, there is very limited collagen turnover with an estimated half-life of collagen type II in AC of 80 years23,24 contributing to the limited repair capacity of cartilaginous tissues. Increased collagen turnover in OA comes at the cost of increased collagen denaturation, that is, no functional tissue is obtained. 22
Mechanical, inflammatory, and metabolic factors drive further tissue degeneration resulting in a switch of the balance toward catabolic processes that ultimately result into structural failure of the joint and/or the IVD and the inability to meet the biomechanical demands, a circle that is maintained by the ongoing low-grade inflammation13,25 and by-products produced by matrix breakdown. 26
Because of the similar nature of the tissues and their disease, similar tissue engineering treatment approaches have been developed and both fields could learn from each other. One commonality is the use of injectable hydrogels for AC and NP repair, which is the topic of this review. In this study, we summarize the recent literature (2015–2021) with respect to injectable hydrogels developed for repairing, restoring, and regenerating AC tissue suffering from damage and/or OA and NP tissue in DDD. We compare the biomaterial approaches exploited for regeneration of both tissues and identify the synergies that could be gained by translating experiences from one tissue to the other.
Search Criteria
Articles included in this review were selected according to the following premises: We focused on reports published in English language within 2015–2021 to provide an overview of the most recent developments on injectable hydrogel biomaterials for AC and NP repair. We concentrated on acellular approaches but included cell-delivery studies whenever they featured an acellular control. Reports based on injectable formulations for drug delivery were intentionally excluded because these formulations were not intended for tissue engineering and immediate restoration of the tissue biomechanics; these formulations at best have disease modifying properties in the long term and have been reviewed elsewhere. 27 As with cells, suitable biomaterials may easily be combined with drugs for a synergistic approach to tissue regeneration.
Search criteria included injectable hydrogels tested in large animal preclinical studies (including goat, dog, pig, sheep, cow, monkey, and horse models), clinical studies, and commercially available materials. Large animal models in preclinical development are considered within the AC and IVD field as the ultimate translational step to demonstrate the proof of concept. Large animal models are preferred in IVD regenerative strategies because they provide for a comparative IVD geometry, 28 biomechanical behavior,29,30 and similar pathology, as reviewed elsewhere. 31 Furthermore, large animal models allow for complementary outcomes at the macroscopic, microscopic, and clinical level from each treated joint. 32
Similarly, large animal models have gained considerable interest in the AC field particularly since frequently used small animal models, such as mouse, rat, and rabbit, have much higher endogenous repair capacity than human and thus have poor translational power.33,34 For NP repair and due to the scarcity of in vivo preclinical reports, we additionally included reports on large animal ex vivo studies. To the best of our knowledge, no materials for NP repair have made it to the commercial stage. In contrast to this, commercialized biomaterials for AC repair were found, already highlighting the different stages of development in tissue repair of the two research fields.
Injectable Hydrogels Used for AC Repair
Biomaterials tested in large animal models (in vivo)
In this section, we particularly refer to hydrogels used for the treatment of focal cartilage defects, although the engineering of the subchondral bone has also received attention in some approaches. Injectable hydrogels have been successfully demonstrated to promote AC repair in large animal models such as dogs, minipigs, horses, and monkeys, with preclinical studies spanning from 1 month up to 1 year (Table 1).
Recent Examples of Injectable Hydrogels for Articular Cartilage Repair Tested in Large Animal Models
ASC, autologous adipose stromal cells; Sox9, sex-determining region Y-type high-mobility group box 9 transcription factor; lacZ, lactose operon gene encoding beta-galactosidase, which degrades lactose; micro-CT, micro-computed tomography; IGF-I, insulin-like growth factor I; MSC, mesenchymal stromal cell; MRI, magnetic resonance imaging. Note: Cell-free biomaterial-based approaches are included here; studies using cell-based approaches are only referred to when there is an acellular biomaterial control.
Regarding biomaterial composition, the following features can be noted. The use of polymers of natural origin (e.g., fibrin, collagen I, alginate, chitosan, and cellulose) has prevailed over synthetic ones (e.g., poloxamer). Note that bio-based precursors typically require prior chemical modification to introduce specific reactive groups for in situ gelation. Regarding crosslinking strategies, physical, enzymatic, and other covalent chemical crosslinking strategies have been applied. In addition, these injectable hydrogels often contained encapsulated cells or were complemented with biologics (e.g., platelet-rich plasma, gene carriers, or growth factors) to enhance the therapeutic response.
Critical-size (osteo)chondral defects created in stifle joints (sometimes in combination with microfracture procedure35,36) are filled with the injectable gel before closing the wound. At a given time point postimplantation, the healing of the tissue is evaluated through macroscopic observation, histological, and immunohistochemical analyses. The hydrogel-filled defect is compared to the empty control defect and/or to the defect filled with the control gel (e.g., lacking the added cells or biologics), and the success in promoting cartilage repair is scored using scoring systems developed specifically for in vivo studies (e.g., the modified O'Driscoll repair scoring or more recently the ICRS2 scoring system 37 ), considering among others the amount and quality of newly deposited tissue, as well as its integration with surrounding cartilage.
The choice of animal model is considered critical in which regulatory bodies prefer extended testing in large animal models such as dog, minipig, and horse over rabbit models. As shown in Table 1, recent reports demonstrate promising results in biomaterial-guided regeneration of AC across different large animal models. At present there is no consensus in the field about which of the large animal models has the best translational power, with each model having its own pros and cons.
When comparing the diverse reported approaches, some points can be highlighted. First, the biomaterial design is straightforward (typically involving 2–3 components at most), which seems advantageous for upscaling and future clinical application. Second, acellular gel strategies seem to predominate since cellular hydrogels have not necessarily demonstrated better performance than acellular ones, at least in some of the case studies.38,39 In fact, these findings add to the ongoing debate in the literature on whether inclusion of cells in a biomaterial positively impacts on cartilage repair outcome in the long term.39,40 Cell-free hydrogels are populated by migrating endogenous cells that subsequently deposit the repair tissue. 41
A third remark relates, surprisingly, to the seldom evaluation of mechanical properties of these biomaterials (e.g., stiffness, tribological properties; in vitro or in vivo), with few reports including mechanical characterization of the hydrogels and of the repair tissue.38,39 Consequently, the effect of hydrogel mechanics on AC repair often cannot be extracted from these data. Note that some of the natural polymer-based hydrogels used here, such as collagen type I and fibrin, are known for their poor mechanical properties.
Biomechanical testing has been rarely performed in animal studies. 39 One outstanding example in which biomechanical testing has been performed reports on the use of a platelet-rich fibrin hydrogel either or not laden with mesenchymal stromal cells (MSCs) in a horse chondral defect model. Cartilage load-bearing function was evaluated by indentation testing in different regions (in and around the repair tissue), and structural stiffness was calculated. These studies were complemented with micro-CT-based analysis of material stiffness and histological analysis for GAG deposition. Neither material nor structural stiffnesses were positively affected by the inclusion of cells in the hydrogel. Interestingly, Hexabrix-enhanced micro-computed tomography (micro-CT) findings were correlated with the histological results based on Safranin-O staining of GAG. High Hexabrix concentrations in the defects of both treatment groups indicated a GAG content lower compared with normal AC, in agreement with the histochemical findings and the decreased structural and material stiffnesses within the lesion in comparison with the control AC. 39
Another important aspect to mention is the tissue adhesion properties of the reported injectable hydrogels and their possible benefit for the fixation of the biomaterial in the chondral defect. The tissue adhesion property of these biomaterials has been highlighted in two reports.38,39 Moreover, it should be noted that only a few studies assessed integration of the repair tissue in native cartilage as an important outcome parameter.35,39,40 For example, a study involving an MSC-laden collagen gel on a monkey model analyzed the cartilage integration and tissue response, where the repair tissue was evaluated regarding surface regularity and surface of graft edge, among other aspects. 40 In this example, MSC-containing hydrogels showed better quality cartilage with regular surface and seamless integration with neighboring native cartilage in comparison to cell-free gels.
Another aspect involves the duration of these in vivo studies lasting for 1 year maximum. One can question whether this time frame is long enough, particularly since the repair AC is expected to last for at least 10–15 years in postponing joint replacement surgery. Clinical studies have shown that microfracture is as effective as cell therapy in the first years after the procedure, but that after 3 years cell therapy shows persistent beneficial effects that are attributed to the generation of better-quality cartilage with improved biomechanical properties compared to microfracture. 42 A biomaterial approach should thus result in repair tissue with biomechanical properties that outperform the microfracture procedure both in terms of quality and persistence. Longer lasting studies in a large animal model might provide a deeper understanding of the durability of the repair tissue and its resistance to mechanical loading.
Altogether, the highlighted examples show that injectable hydrogels for AC repair have achieved significant progress in this field. It is expected that future developments will include other less frequently investigated, but just as important, biomaterial properties, such as mechanical strength, tribology, or tissue adhesive properties, as well as perform biomechanical testing and biomaterial/tissue integration evaluations.
Biomaterials undergoing clinical studies and commercialization
In line with injectable hydrogels used in preclinical studies, the injectable hydrogels available on the market are composed of 1–3 components. Considering the cell-free in situ gelatin injectable hydrogels (Table 2), no biologics are added to these biomaterials. However, when using BST CarGel, the solution is premixed with the patient's whole blood.43,44 Most systems rely on their ability to enhance the outcome of microfracturing, often referred to as Autologous Matrix-Induced Chondrogenesis, rather than replacing the method. Exceptions are JointRep (in case of smaller defects) and ChondroFiller. The former is using a polyglucosamine/glucosamine carbonate (PG/GC) based thermogelling injectable system.45,46 The latter fills the cartilage defect with a collagen I (murine) matrix,47–49 providing a scaffold for migratory chondrocytes to attach and proliferate, resulting in ECM production and the repair of the defect with collagen type II-rich cartilage. 50
Clinically Tested Commercially Available Injectable Hydrogels for Articular Cartilage Repair
Cell-free biomaterial-based approaches are here included.
PEG, polyethylene glycol; HA, hyaluronic acid; HMW, high molecular weight; RCT, randomized controlled trial; MRI, magnetic resonance imaging; MOCART, magnetic resonance observation of cartilage repair tissue; IKDC, international knee documentation committee; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
Next to serving as a scaffold for cell attachment and ECM production, all products claim a good fixation to the cartilage defect. However, only ChonDux uses a primer: a multifunctional adhesive chondroitin sulfate (CS) base is used before the application of the PEG hydrogel, ensuring the immobilization of the CS to the defect surface while crosslinking to the PEG hydrogel during photopolymerization. 51 For BST CarGel and JointRep, the cationic nature of the chitosan increases the adhesion of the biomaterial to the cartilage lesions.52,53 CartiFill is fixed by fibrin glue54,55 while GelrinC and ChondroFiller form three dimensionally stable implants mechanically interlocking with the surrounding tissue.
Although all products are injectable hydrogels, GelrinC and ChonDux require UV light for crosslinking.56,57 Therefore, clinical studies have so far been performed mostly through mini-arthrotomy, giving these products a major disadvantage due to increased patient morbidity. To reduce this burden, strategies are under development for the arthroscopic application of these materials. The other hydrogels form in situ based on the physical interactions or enzymatic-based chemical reactions. Given the initial fluidity of the injectable hydrogels, most of them are applied in a semi dry environment, either by draining synovial fluid from the defect or by inflating the joint with CO2 to better retain the hydrogels in the defect, before crosslinking, and to improve fixation in the defect.58–60
Injectable Hydrogels for Intrinsic NP Regeneration and Mechanical Restoration
Biomaterials tested on large animal models (ex vivo and in vivo)
There are two major approaches to reestablish joint biomechanics by treating the NP in IVD degeneration: (1) directly, by biomaterial application, or (2) indirectly, by regenerating the NP tissue through administration of small molecules, growth factors, and/or (progenitor) cells. Hydrogels are used in both approaches due to their injectability, soft mechanical properties, and water swelling capacity similar to NP tissue or as a carrier/release system for regenerative agents. Treatment efficacy is judged functionally on restoration of disc height or spinal motion segment biomechanical characteristics, for example, range of motion (ROM), neutral zone (NZ), etc. ex vivo, as well as IVD tissue health using magnetic resonance imaging (MRI, Pfirrmann grade), 61 pathomorphologically (Thompson grade) 62 or histological characteristics (Boos score) in vivo.62,63 For in vivo studies, degeneration of the IVD can be induced in various ways, including complete or partial removal of the NP (nucleotomy), NP tissue disturbance, or injection of enzymes (reviewed in Refs.32,64). Key to successful NP augmentation or regeneration over time is keeping the biomaterial within the NP. This requires an intact AF with minimal damage sustained from injecting the biomaterial.
Hydrogels for NP regeneration have been made from natural (e.g., collagen, decellularized tissues) or synthetic (e.g., polyurethane) sources. Although many biomaterials have been investigated, few of them have been validated in preclinical ex vivo or in vivo models so far, and meaningful comparisons between biomaterials are hindered due to nonstandardized biomaterial characterization approaches in the field. 65 Harmonization efforts are actively being pursued, and consensus methods are increasingly established.32,65–67
Most ex vivo-testing approaches in recent years have utilized naturally occurring polysaccharide- or protein-based precursors for hydrogel formation, to confer the water uptake capacity of the NP (Table 3). Additional components such as marine collagen/gelatin have provided cell adhesion sites.68–70 Crosslinking strategies mainly focused on covalent crosslinking of chemically modified polysaccharides, enzyme-based fibrinogen-thrombin crosslinking, 71 dynamic crosslinking, 72 or physical crosslinking.72,73
Hydrogels Used for Nucleus Pulposus Augmentation and Regeneration: Properties and Preclinical Evaluation
Cell-free biomaterial-based approaches are included here, studies using cell-based approaches are only referred to when there is an acellular biomaterial control.
CMC, carboxymethylcellulose; HA, hyaluronic acid; BMP, bone morphogenetic protein; PU, polyurethane; MC, methylcellulose; ROM, range of motion; NZ, neutral zone; NIPAM, N-Isopropylacrylamide; DMAc, dimethylacrylamide; MRI, magnetic resonance imaging; NPC, nucleus pulposus cell.
Stability of newly formed crosslinks and crosslinking density have immediate effect on mechanical properties of hydrogels and thereby on cell response.74–76 Enzymatically degradable or dynamically crosslinked hydrogels improve cell infiltration77–79 and ECM deposition by cells.80,81 To the best of our knowledge, there are to date no biomaterial-driven strategies reporting specifically on the NP, neither in vitro nor in vivo aiming at intrinsic repair of earlier stages in IVD degeneration.
There is a paucity in studies on cell-free approaches for IVD regeneration to the degree we had to include cell-based approaches featuring a cell-free control in our search criteria for this review (see Search Criteria section). Cell-based regeneration approaches have substantially increased in number over the last 2 decades, 82 although treatment efficacy is not always enhanced.68,73,83 This may stem from the hypoxic and nutrient-poor environment found within the IVD rendering cell survival difficult. 84 Critical discussions as to which cells are most suited for the purpose of cell therapy 82 and further translational problems remain, as it has been reviewed by Sakai and Anderson 85 and by Binch et al. 86
Administering growth factors for intrinsic NP regeneration may provide an alternative treatment route and have produced varying results so far (BMP-2/7 vs. notochordal cell-derived factors),71,73,87 highlighting the importance of growth factor choice in therapeutic approaches. Small molecule delivery alongside biomaterials into the NP has been explored, although few studies have been conducted ex vivo or in vivo. 88 Local controlled delivery of celecoxib (a nonsteroidal anti-inflammatory drug) from a PCLA-PEG-PCLA hydrogel, and later from polyester amide microspheres, in dog patients resulted in less pain interference in their daily life activity, but the therapy failed to show regenerative effects at the tissue level at three months follow-up on quantitative MRI.89,90 Gefitinib for inhibiting aberrant epidermal growth factor receptor activity in DDD showed maintained or improved Pfirrmann grades in a case study. Its inclusion in hydrogels led to increased collagen II production by encapsulated NP cells (NPCs), as well as improved disc height 12 weeks postinjection in rats, 91 and may prove promising for future large animal studies. The outlook is similar for approaches including Link-N peptide or the growth factor GDF-5.92–94 Interesting is also the use of hydrogel scavenging reactive oxygen species95–97 to deplete excessive levels found in the degenerated IVD,98,99 but their effect on NPCs and translation to large animal models are yet to be demonstrated.
Translation from the laboratory to the clinic
There is an ongoing debate about the translational validity of current outcome measures, since biomechanical restoration does not necessarily result in pain relief. Few published in vivo studies include pain relief as an outcome, and typically the animal model of choice is still a rodent100,101 while scarcely clinically relevant large animal models have been reported.32,89 As such, meaningful pain relief will often first be addressed in human subjects. Current clinical trials concentrate efforts on restoration of disc height through swelling or filler materials (Table 4). The investigated materials are relatively simple in composition, using ≤3 components; these are either noncrosslinked, crosslinked covalently, or crosslinked enzymatically (through fibrin-thrombin polymerization).
Previous and Current Clinical Trials (Listed on clinicaltrials.gov) Investigating Biomaterials for Nucleus Pulposus Regeneration/Augmentation
Cell-free biomaterial-based approaches are here included; studies using cell-based approaches are only referred to when there is an acellular biomaterial control.
Notably, these materials do not necessarily approach the mechanical properties of the IVD102,103 in terms of stiffness and swelling. These parameters are usually linked (swollen gels have a lower Young's modulus than in their nonswollen state),104,105 and the cyclic loading within the NP and resulting stiffness changes contribute to NPC proliferation106–109 and IVD homeostasis by encouraging nutrient transport through loading-induced convection. 110 Hydrogels mimicking this cyclic loading behavior may therefore benefit biological regeneration of the IVD for long-term strategies compared to filler materials.
Compared to AC regeneration approaches, and despite the progress achieved in the NP field,111–125 there are currently no injectable NP augmentation products commercially available to our knowledge. Adapting treatment strategies used in AC research to foster strategies for intrinsic NP repair may aid the development of such materials in the foreseeable future.
Comparison of Biomaterials Used for NP & AC Repair
Demand for material properties varies between NP & AC
Conceptualization of biomaterials for AC or NP repair differs somewhat since they need to fulfill different requirements based on the anatomy of the target tissue. While AC biomaterials are only laterally confined within the AC defect, NP biomaterials need to be administered into the space enclosed by the AF and CEPs in all directions. The different levels of confinement dictate levels of nutrient diffusion, therapeutic dose, and thereby recovery and degradation time frames; the latter are generally thought to be longer in the NP than in AC, resulting in longer biomaterial retention time in the NP. Consequently, material selection may differ between approaches to regenerate these two tissues.
An important difference is related to the hydrogel's mechanical strength. Materials for AC regeneration are generally stiffer than biomaterials for use in the NP. While matching in situ tissue stiffness is advisable for purely augmentative/restorative approaches, softer materials typically allow for easier cell infiltration and these materials better match the mechanical properties of the pericellular matrix whose stiffnesses are sensed by the embedded cells: AC pericellular matrix is characterized by presence of collagen VI and several proteoglycans and has a stiffness between 15 and 25 kPa, while the stiffness of the interstitial cartilage matrix can approach 1000 kPa. 126 Mimicking the stiffness and composition of the pericellular matrix has shown favorable results for material-induced intrinsic regeneration increasing cell viability, proliferation, and matrix production. 38
In contrast, the NP pericellular matrix stiffness has to date not been determined, to our knowledge. Studies so far indicate a composition similar to the AC pericellular matrix with notable presence of collagen VI, syndecan, and laminins.127–129 Studies on relating composition to material properties and biological effect onto NPCs are warranted for further progression in NP biomaterial development.
Encapsulation of cells in a microgel mimicking the pericellular matrix before injection in the defect could be a viable strategy to match, on the one hand, the cell's demand for a matched stiffness of the surrounding ECM optimally supporting tissue formation, while another hydrogel could provide a much more resilient extraterritorial matrix that can withstand biomechanical loading. 130
A major difference is the swelling of biomaterials, which is avoided for AC to prevent overfilling of the defect, while it is advised for NP augmentation. The swelling degree of a biomaterial also informs about its therapeutic volume, as overpressurization of the neighboring tissues must be avoided to prevent tissue trauma, inherent pain, and/or herniation of the injected biomaterial that may cause neurologic deficiencies, specifically in the NP application. Injectable volumes for the NP depend on the disc's degenerative state (with more severe degenerate IVDs allowing for higher volumes of biomaterials to be injected without significantly increasing the intradiscal pressure). Volumes may reach up to 2 mL intradiscally in human patients, 131 whereas a range of 30–500 μL (depending on the IVD size of the animal model used) has been reported in the preclinical animal studies mentioned above.83,90,116
In comparison, therapeutic volume for AC repair depends on the size of the defect fill. For example, commercial products for AC repair (Table 2) need to fill an average defect size of 3 cm2, which assuming an AC thickness of 2 mm gives a volume of ca. 600 μL. Thus, a range of 60–1600 μL injection volume can be assumed based on commercial products and 2-mm AC thickness. Therefore, comparable injectable volumes (∼1–2 mL) for both AC and NP repair are required.
Future approaches to biomaterial development for AC and NP repair may include supramolecular gelation mechanisms, which allow for easier cell infiltration and self-healing properties.132,133 Furthermore, incorporation of pericellular matrix-derived ligands into AC and NP biomaterials would allow harnessing of natural cell–matrix interactions to promote cell phenotypic maintenance. An ideal biomaterial would of course be a close mimic of the healthy tissue to be regenerated. The increasing research in both AC and NP fields into decellularized ECM speaks to the efforts in developing these materials, although hurdles regarding clinical translation remain. 134
One challenge in AC and NP material development is the balancing of local tissue regeneration and postoperative conditions for the patient during recovery. As noted above, NP regeneration after treatment is currently thought to lag AC regeneration, which already can take 6–9 months, including ≥4 weeks of joint unloading followed by a prolonged period of reduced loading. 135 In contrast to AC recuperation, unloading of the IVD by distraction is invasive. 136 Temporary distraction has been shown to facilitate IVD regeneration in small animal models 137 and thus far its feasibility has only been described in a dog patient for treatment of IVD degeneration. 138
Long-term spinal unloading has also been correlated with downstream spinal instability. 139 This necessitates two major approaches for NP augmentation: mildly degenerated NPs in young patients benefit from a regenerative approach (potentially including cell injections) over several years, and patients with severely degenerated NPs see a prioritization of IVD biomechanics restoration. An immediate restoration of swelling pressure and thereby load distribution across the AF and NP is advised in any case to prevent further pathological load bearing by the AF, leading to later degeneration. 140
Thinking in the long term, the injected materials need to be integrated into their surrounding tissues. For AC this requires a material that allows both tissue adhesion and cell infiltration, as well as new matrix deposition and collagen fiber alignment, within the implant and across the interface with adjacent cartilage. For the NP, tissue adhesion is an optional point due to its omnidirectional confinement by AF and CEP. On the flip side, NP materials need to be injectable through small needle gauges so that puncture through the AF does not cause further IVD degeneration. 141 Note that for highly degenerated AF, collagen fiber alignment strategies developed for AC may be relevant 35 ; however, these approaches are beyond the scope of this review.
Strategies to evaluate material-mediated tissue regeneration
Pain outcome parameters are lacking in the design of the latest in vivo studies particularly in IVD. 32 Perhaps because disability, in addition to pain, motivates patients to seek care in treatment for lower back pain. 142 In addition, there are no established large animal models for spinal pain evaluation. 32 In contrast, pain is the number one reason for OA patients to seek medical attention. Indeed, in many animal experiments, objective gait analysis, including force plate measurements, and/or kinematics are included as surrogate markers for joint pain. These outcomes are, in the case of preclinical studies involving companion animals enrolled in veterinary trials to demonstrate proof of concept of AC or NP repair, complemented with owner reported outcomes using validated questionnaires (e.g., the Canine Brief Pain Inventory (CBPI) and Liverpool Osteoarthritis for Dogs (LOAD)). Such functional readouts may consequently take priority over pain assessment until pain experimental models have been validated for large animal models.
Additional functional pain outcomes can be grouped into invasive and noninvasive procedures: especially for AC regeneration, (2nd or 3rd look) arthroscopies and, potentially, biopsies are available to monitor tissue regeneration. Novel techniques such as infrared spectroscopy or mass spectrometry can give further information about the regenerative state of the tissue,143–145 but are yet to be adapted in the clinic. However, given the inaccessibility of the IVD for invasive methods, these methods are not viable options to evaluate NP regeneration.
Noninvasive procedures relying on quantitative MRI are preferred for monitoring NP regeneration as they circumvent repeated injury to the AF for biopsies and have been shown to quantitatively and qualitatively assess the NP tissue composition in large animal models. 146 In the patient population younger than 50 years of age, MRI pathological findings significantly associate with lower back pain. 147 Furthermore, quantitative MRI has been shown to discern more accurately early IVD degeneration compared to the classical Pfirrmann grading system 61 and as such will be more valuable in the longitudinal follow-up of NP regeneration.
Especially MRI-based monitoring has been adopted within the OA field for treatment follow-ups within the last years with several scoring systems available using automated segmentation methods. 148 Depending on the parameters evaluated, recorded relaxation times provide information about the tissue contents and degenerative state.149,150
Similar to the NP-specific Pfirrmann score, OA MRI scoring may need an update, as it was developed for images acquired on a 1 Tesla MR scanner, 151 but more powerful setups are available nowadays. From a comparative perspective, artificial intelligence and deep machine learning are finding their way in both the AC and NP fields for automated and objective qualitative assessment of the regenerated/engineered tissue quality.152,153
Nonetheless, it remains to be determined how MRI modalities are influenced by the specific biomaterials used and their behavior over time. No AC or NP specific algorithms have been approved by the FDA to our knowledge, 154 but may be adapted from already approved algorithms for other tissues and indications. As such, MRI scoring systems are still under development for regular clinical use and complemented by further outcome measures.
In addition to objectively measurable outcomes, self-reporting by patients using validated Patient Reported Outcome Measures (PROMS) is still the gold standard to assess clinical treatment success. Several questionnaires have been developed across the NP and AC fields, often combining assessments for pain perception, joint mobility, and physical limitations in everyday life.155–157 These PROMS include, for example, the WOMAC pain score and the KOOS for knee OA and the Oswestry Disability Index for the IVD.
Conclusions and Outlook
In the following, a list of highlights identified in this review from the comparison of biomaterial development for the AC and NP fields is presented:
The AC field is considerably more advanced than the NP field with respect to completion of clinical trials and commercialization. AC commercial products contain max. three components and are mostly acellular, which most probably accelerated the development of these products. While these products have CE mark, they have not been FDA approved yet. In comparison, products for NP repair have not reached commercialization so far, but do share similar advantages in terms of simplicity of composition, which is expected to benefit the progress of the NP field. Injectable hydrogels that mimic AC pericellular matrix in terms of stiffness and/or ligand composition have been reported as beneficial for AC repair. The same strategy could be a promising avenue for developing novel hydrogels for NP repair, for example, using decellularized ECM matrices. However, note that to date the stiffness of NP pericellular matrix remains to be characterized. Biomaterial swelling capacity is ideally higher for NP than for AC, allowing for increasing IVD height and restoring biomechanical joint function due to the swollen materials' confinement by the AF and cartilaginous endplates. In contrast, AC biomaterial scientists tend to avoid swelling materials considering the unconfined application site. Additionally, AC biomaterials need to withstand wear and facilitate lubrication—factors not present in the IVD. Efforts to standardize characterization of biomaterials used for NP and AC repair would facilitate comparison of performance. In the NP field, harmonization efforts have led to consensus guidelines for standardized biomaterial testing of the biomechanical properties at the in vitro, ex vivo, and in vivo levels.32,65 In contrast, this is not yet reported for AC biomaterials. Biomaterial characterization approaches may be transferred and adapted from NP to AC purposes with adjusted acceptable ranges/endpoints, etc.
In the past years, considerable progress has been made in the development of injectable hydrogels for cell-free AC and NP repair. However, certain aspects of biomaterial development for both fields need more attention.
One of such aspects, particularly in the AC field, is related to the biomechanical properties of the relatively weak hydrogels and the newly formed repair tissue that must achieve durable repair. This would deserve a more systematic approach and standardized methods, preferably noninvasive or minimally invasive, to assess the biomechanical quality of the repaired tissue. This feature is now, in part, addressed by performing preclinical tests in biomechanically more challenging large animal models, with joint loading comparable to that in humans.
Another aspect that is raising increasing interest is related to the investigation of the immune response of an injected biomaterial. Such response will depend on the degenerative stage and on the vascularization of the tissue. The importance of the host's immune response to biomaterials for AC repair has recently started to be investigated. 158 It is hypothesized that immune response for tissue repair is more pronounced for AC than for NP due to the avascular nature of the IVD. Nevertheless, immune modulation/response elicited by injected biomaterials deserves attention in both fields for meaningful clinical translation.
Moreover, clinical translation in both fields would benefit from the development of more representative animal models and imaging analysis techniques. Animal models for pain evaluation within the context of OA or DDD have been developed to a different extent. Considerable work has been done for OA small animals (e.g., mostly rodents), whereas models of companion animal that suffer from naturally occurring OA, such as dogs, have also been established. 159 For larger animals (e.g., horses) assessment of pain will be mostly based on gait analysis, kinematics, and lameness evaluation. 160 Further development of objective evaluation methods will benefit both research fields. In contrast, large animal models of low back pain are scarcely studied in NP.
In addition, progress in the AC and the NP fields would clearly benefit from established and validated noninvasive imaging tools in combination with better image analysis that could provide information on the quality of the repair tissue, that is, GAG and collagen content and organization, soon after treatment, which would be predictive for long-term clinical outcome. For new product introduction in the market, this would be invaluable for these slow healing and remodeling tissues to avoid very costly clinical studies with long-term follow-up of 3 or more years at least. MRI scoring systems deserve further studies on their use in biomaterial augmented joints and could become very powerful when combined with machine learning tools for objective assessment.
In conclusion, similar approaches are being developed for AC and NP repair and much can be learned from one another to accelerate the introduction of dearly needed solutions for patients suffering from AC defects and DDD.
Footnotes
Disclosure Statement
T.C.S., B.Z., M.A.T., J.I.P.: Conflicts of interest: none.
K.I. reports a relationship with NC Biomatrix that includes contract work and silent shares through a licensing agreement for a pending patent.
M.K. reports a relationship with Hy2Care and Orthros Medical that includes a shareholder position through licensing of various patents on injectable hydrogels for cartilage repair.
Funding Information
K.I., M.A.T., T.C.S. report financial support provided by the European Union's Horizon 2020 research and innovation program iPSpine under the grant agreement #825925 (![]() ); K.I. reports financial support by Regenerative Medicine Crossing Borders (RegMed XB), a public-private partnership financed by the Dutch Ministry of Economic Affairs by means of the PPP Allowance made available by the Top Sector Life Sciences & Health to stimulate public-private partnerships. M.A.T. reports financial support from the Dutch Arthritis Society (#LLP22). M.K. reports financial support from the Dutch Arthritis Society (#LLP25). B.Z. and M.K. gratefully acknowledge the financial support of the Netherlands Organisation for Scientific Research (NWO) P15–23 (Project 1) “Activating resident stem cells” and EFRO OP-Oost 00867 Orthros TR.
); K.I. reports financial support by Regenerative Medicine Crossing Borders (RegMed XB), a public-private partnership financed by the Dutch Ministry of Economic Affairs by means of the PPP Allowance made available by the Top Sector Life Sciences & Health to stimulate public-private partnerships. M.A.T. reports financial support from the Dutch Arthritis Society (#LLP22). M.K. reports financial support from the Dutch Arthritis Society (#LLP25). B.Z. and M.K. gratefully acknowledge the financial support of the Netherlands Organisation for Scientific Research (NWO) P15–23 (Project 1) “Activating resident stem cells” and EFRO OP-Oost 00867 Orthros TR.