
Abstract
Cardiovascular tissue engineering and regeneration strive to provide long-term, effective solutions for a growing group of patients in need of myocardial repair, vascular (access) grafts, heart valves, and regeneration of organ microcirculation. In the past two decades, ongoing convergence of disciplines and multidisciplinary collaborations between cardiothoracic surgeons, cardiologists, bioengineers, material scientists, and cell biologists have resulted in better understanding of the problems at hand and novel regenerative approaches. As a side effect, however, the field has become strongly organized and differentiated around topical areas at risk of reinvention of technologies and repetition of approaches across the areas. A better integration of knowledge and technologies from the individual topical areas and regenerative approaches and technologies may pave the way toward faster and more effective treatments to cure the cardiovascular system. This review summarizes the evolution of research and regenerative approaches in the areas of myocardial regeneration, heart valve and vascular tissue engineering, and regeneration of microcirculations; and discusses previous and potential future integration of these individual areas and developed technologies for improved clinical impact. Finally, it provides a perspective on the further integration of research organization, knowledge implementation, and valorization as a contributor to advancing cardiovascular tissue engineering and regenerative medicine.
Impact Statement
Despite ongoing convergence of disciplines, research in the field of cardiovascular tissue engineering and regeneration is organized and differentiated around focal areas, including myocardial regeneration, heart valve tissue engineering, vascular tissue engineering, and engineering of microcirculations. Cross-area integration of knowledge, supported by a more holistic, overarching research approach, may lead to faster and more effective treatments and prevent the reinvention of technologies across the areas. Herein, we review the evolution of research and technologies in the individual focal areas and discuss how to enhance integration of–and collaboration between–these areas for improved scientific and clinical impact.
Introduction
The human cardiovascular system is a hierarchically organized and integrated system engineered by nature to perform its complex mechanical, electrical, and biological functions. In essence, the system consists of the heart (including the myocardium, conduction system, and heart valves) and the vascular system (composed of arteries, veins, and capillary beds). At the macroscale, these elements act in perfect synchrony to serve the metabolic needs of the body. At the microscale, each element expresses a functional, often layered, morphology, wherein multiple cell types and specialized extracellular matrix (ECM) interact in space and time to continuously fine-tune local hemodynamics. Because of its crucial role in human physiology and health, diseases and failure of the cardiovascular system have high impact and often affect multiple organs.
In fact, one-third of mortality worldwide is caused by cardiovascular diseases, with an increasing trend due to an ever-aging population and the progressive aspects of the diseases.1,2 Systolic heart failure following myocardial infarction, often as a result of macrovascular disease, is particularly lethal, with a 5-year survival rate of <50%. 3 Similarly, (cardiac) microvascular disease is increasingly recognized to be a causative factor for diastolic heart failure, a major contributor of mortality, morbidity, and hospitalization costs. 4
In the context of regeneration—and contrary to cardiovascular pathophysiology—the cardiovascular system is very rarely considered in toto. Rather, clinicians and basic scientists investigate, replace, and regenerate the separate parts in isolation and often within their own disciplines. As outlined by Zilla et al., 5 the field of cardiovascular tissue engineering and regeneration was pioneered in the late 1970s by cardiothoracic surgeons who strived to improve the interaction between nonliving implants and blood via implant endothelialization, followed by the in vitro engineering of living, autologous heart valves and large vessels under their guidance. Later, at the turn of the millennium, cardiologists instigated myocardial regeneration in their search of much needed clinical solutions for cardiac failure.
Over the decades, the mere complexity of the cardiovascular system as well as the knowledge required to progress cardiovascular regeneration has led to a vast growth of multidisciplinary research consortia, convening expertise from bioengineering, stem cell biology, materials science, immunology, and clinical translation in an integrated approach. Thus, cell biologists learned from bioengineers to culture cells in three-dimensional (3D) microenvironments and under hemodynamic loading instead of two-dimensional static conditions 6 ; material scientists, together with biologists and clinicians, designed bioactive materials that not only facilitate endothelialization but also immunomodulation and antimicrobial activity upon implantation 7 ; and basic tissue engineers realized that clinical translatability is the most relevant aspect of their outcomes and should be incorporated in the very first steps of their designs. 8
Yet, with silos of multidisciplinary researchers still concentrating on isolated, focal topics, like myocardial regeneration, heart valve tissue engineering, and vascular tissue engineering, integration of knowledge is far from what is needed for improved cardiovascular health in patients. What is the value of a perfectly engineered aortic heart valve if it cannot be integrated within the left ventricular outflow tract? How should we judge a 3D printed microcirculation if it has not been integrated in a beating myocardium; let alone an ischemic myocardium? As experts with an accumulated 80+ years of experience in the field, we are concerned that this topical differentiation of the field—although relevant for gaining the required in-depth knowledge to progress the individual areas—is becoming exemplary of the focused, one-sided knowledge development of monodisciplines.
An additional aspect that comes with differentiation is the reinvention of technologies across the areas. As examples, one could refer to the design of layered scaffolds for vessels that were reinvented for heart valves,9,10 or the design of strut-based, biofunctionalization stents, reinvented for vascular scaffolds to accelerate, for example, in vivo endothelialization.11,12 Acknowledged reinvention is ideal if the application is successful, but disastrous if failures in one area are ignorantly copied to another.
Tissue engineering and regenerative medicine are interdisciplinary fields par excellence and integration of knowledge and methods from different fields is at the heart of any successful translational achievement. But what is the best way to add an extra layer of integration and move to a more holistic, overarching research approach that benefits from knowledge exchange between the individual areas in the field of cardiovascular tissue engineering and regeneration? Should this be driven bottom-up by mutual and more generic research questions? Or should we organize this top-down in large consortia? And who will initiate and lead such consortia? Is the researcher the linking pin? The clinician? Or even the patient, supported by patient organizations?
In this article, we review some of the essential developments and key challenges within the field of cardiovascular regeneration, focusing on the myocardium, heart valves, arteries, and the microcirculation. We will highlight how interdisciplinary collaborations as well as integration of methods and approaches have evolved the different areas and explore how exchange of knowledge across the areas might progress the field. Finally, we will discuss how to organize and potentially improve further integration of knowledge and interdisciplinary collaboration, based on our experience in large cardiovascular research consortia in the Netherlands.
Myocardial Regeneration
Structure-function properties and their regeneration
The myocardium is primarily composed of cardiac muscle fibers and is responsible for pumping blood through to other organs. Coordinated contraction of the atrial and ventricular myocardium is initiated by electrical activation, originating from specialized pacemaker cardiomyocytes (CMs) in the sinoatrial node, located in the right atrium. Electrical impulses travel through the atrial myocardium, causing atrial contraction, followed by rapid conduction via the cardiac conduction system to the ventricular myocardium. Subsequent propagation of electrical signals occurs from the apex of the ventricular myocardium to its base, ensuring efficient synchronized contraction and causing the ejection of blood.
It is evident that any disturbance in these highly orchestrated events may have adverse functional consequences for the heart, leading to life-threatening conditions. Since the adult human heart lacks regenerative capacity, as opposed to certain fish and amphibian hearts,13,14 or even fetal or neonatal mammalian hearts, 15 loss of viable CMs after myocardial infarction (e.g., when blood and oxygen supply via the coronary arteries to the myocardium is blocked), is one of the main causes for morbidity and mortality. 16 Consequently, this has inspired scientists in the past decades to bring forward various strategies to rebuild or regenerate the heart and restore heart function.
Initial studies focused on different cell sources for cardiac repair to replace damaged or lost CMs after myocardial infarction. Cell-based therapies included the use of skeletal myoblasts, mesenchymal stem cells and subpopulations of bone marrow cells, cell populations that shared characteristics of host CMs, or were thought to have the ability to transdifferentiate to CMs. 17 After evaluation of numerous clinical trials, the consensus is that beneficial effects on heart regeneration and function are very modest. 18 From the various cell sources that have been used in clinical trials, mesenchymal stem cells are most promising with only a moderate improvement of cardiac function, most likely due to its immunomodulatory properties without rebuilding the myocardium. 19
With the groundbreaking discovery by Yamanaka and colleagues, mouse and human somatic cells were reprogrammed in vitro to so-called induced pluripotent stem cells (iPSCs), which have the capacity for self-renewal and the potential to differentiate to any cell-type of the body,20,21 including cardiovascular cells. 22 This incited new strategies for tissue engineering and regenerative medicine. Initial studies showed that although transplanted human PSC (hPSC)-derived CMs survived in the host myocardium, cardiac engraftment was very inefficient and proper integration of grafted cells and long-term functional improvement of the heart proved to be difficult in xenograft studies. 23
Previously, transplantation of hPSC-CMs in nonhuman primates showed remuscularization of the infarcted area, blood flow of the engrafted area by host vasculature and electromechanical coupling between the grafted cells and the host myocardium. 24 Although ventricular arrhythmias were observed, it was shown in a recent follow-up study that this was most likely caused by transplantation of a heterogenous CM population, including pacemaker cells, which hampers synchronous activation of transplanted and host CMs. 25
Although these studies show the proof of concept that rebuilding the heart is feasible, a more holistic approach is required, which will permit interaction and integration of multiple cardiac cell types in the appropriate microenvironment. Instead of single cells or small aggregates, 3D tissues, either multiple stacked layers of cardiac cells (for example, CM and endothelial cell [EC] layers cultured on temperature-sensitive polymers for generation of cardiac sheets) 26 or engineered heart tissues (EHTs) (created either by fibrinogen or collagen gels mixed with CMs and fibroblasts), were used for engraftment in various species.27,28 To increase the chance of success of functional integration of these cardiac tissues in the host myocardium, it is of utmost importance that knowledge and experience is exchanged between the different disciplines of tissue engineering, stem cell biology and cardiac pathophysiology.
In general, multicellular 3D cardiac tissues display a higher level of maturity concerning molecular, metabolic, and functional aspects when compared to single cells or CM monolayers.29,30 Nevertheless, these 3D cardiac tissues are still more comparable to fetal or neonatal cardiac cells and therefore would require further maturation in vitro or in vivo for a better integration with the host tissue. Previously, it was shown that transplantation of 3D EHTs in the infarcted region of rodents resulted in enhanced engraftment, CM maturation and long-term survival, although cardiac function was not improved. 27
More recently, large, EHT patches, sewn on the epicardium of the infarcted rabbit heart, showed vascularization from the host, CM alignment and improved function, although electrical coupling between the grafted patch and the host myocardium was not observed. 28 Although most of these experimental approaches are still far from clinical applications, a Japanese clinical study, enlisting a small group of patients (<10) suffering from severe ischemic cardiomyopathy, was conducted to examine the safety and efficacy of transplantation of iPSC-based muscle sheets.
In situ regeneration and morphogenesis
Besides efforts to repair the heart, using cells, tissues, or materials that are injected in the myocardium or sewn or glued on the heart, it is an attractive idea to attempt to regenerate the heart from within the organ itself. Current strategies include regeneration of the damaged myocardium by exploring mechanisms that are responsible for the expansion of viable CMs in situ, comparable to the zebrafish heart. Other endogenous cell sources that may contribute to repair of the heart are represented by the epicardial cells at the outer layer of the myocardium, which undergo epithelial-to-mesenchymal transition and migrate and differentiate to coronary blood vessels and fibroblasts and promote myocardial growth during development. 31
In the injured heart, the epicardium is reactivated and plays an important role in the repair of the heart, including the formation of fibrotic scar tissue.32,33 Excessive fibrosis may be converted to cardiac tissue by direct reprogramming of host fibroblasts to CMs, which can be achieved by overexpression of cardiac transcription factors GATA4, MEF2C, and TBX5 (GMT). This approach is different from the earlier described reprogramming to iPSCs since CMs are directly transdifferentiated from fibroblasts without the need to transition through a PSC state. 34 However, although additional factors for direct reprogramming have been described (epigenetic factors, microRNAs, or small molecules), this procedure is still very inefficient. 35
Lessons learned from above-mentioned strategies to activate endogenous cardiac repair and lineage-specific differentiation in combination with recent advances in generating multicellular organ-like structures (organoids), inspired researchers to study self-organizing properties of cardiac cells or their progenitors. Although key signaling pathways and transcription factors have been identified for early cardiac development and differentiation toward myocardium, endocardium, and epicardium, a clear understanding of how these cell layers organize in a functional heart chamber with a spatial and temporal resolution is lacking.
Recently, it was shown that hPSC-derived cells differentiated to the cardiac lineage have the capability of self-organization, leading to the formation of so-called organoids: 3D tissues with patterning, morphogenesis, and functional properties that are (partially) comparable to the organ in vivo.36,37 Although these heart organoids (cardioids) are still far from the organization and function of a full-fledged heart organ, these steps are crucial for understanding spatio-temporal organization of the heart and facilitate generation of advanced engineered 3D cardiac tissues in vitro that have the capacity to fully integrate into the host myocardium or even operate as an independent functional pumping organ.
Multidisciplinary perspectives and challenges
While still many hurdles need to be taken, it is encouraging that by multidisciplinary bioengineering approaches, a multitude of organ-like engineered cardiac structures, including vascularized microtissues, microfluidic heart-on-chips, and pumping heart chambers, have been developed, using either molds, recellularization of natural ECM, geometrical confinement, hydrogel matrices, or 3D bioprinting technologies. 38 It is intriguing to speculate that the combined progress in these disciplines may lead to the formation of a functional human heart organ or to the repair of patient's heart ex vivo, in situations where a temporary artificial heart has been implanted to bridge the time required for repair. In fact, temporary implantation of total artificial hearts in patients with severe end-stage heart failure,39,40 may provide the time needed to repair the heart of the patient ex vivo, which may enable regeneration of the myocardium and ultimately restored heart function.
In summary, although clinical objectives to regenerate the myocardium are still far from being achieved, it is promising to see that in the last 10–15 years, spectacular advances have been made in the fields of tissue engineering and regenerative medicine (Fig. 1). Moreover, the use of patient's derived stem cells for both cardiovascular tissue engineering and mimicking cardiovascular disease using advanced organ-like in vitro models offers exciting opportunities to move toward personalized medicine. Nevertheless, there is an increased awareness that a multidisciplinary approach is required to solve major challenges, such as realization of a perfusable vascular network, optimal survival and integration into the host myocardium (especially in an injured, hostile environment), and proper organization and maturation of cardiac tissues.
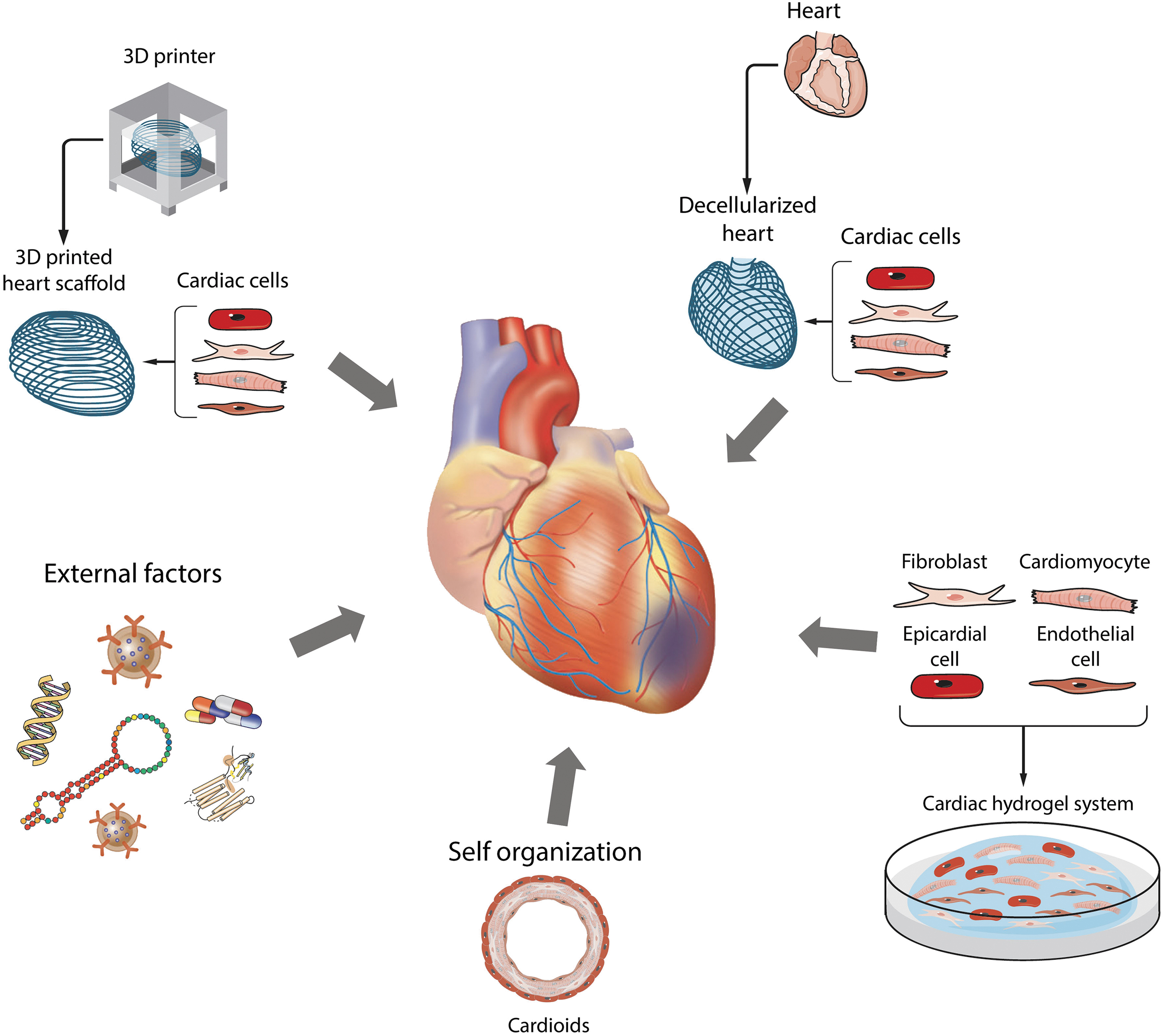
Multidisciplinary strategies to regenerate the injured heart, including the 3D printing of a scaffold for seeding of cardiac tissue or bioprinting of cardiac constructs, the use of decellularized hearts for seeding cardiac cells, generation of cardiac hydrogel tissues or patches, generation of self-organized cardiac tissues, or the use of external factors (e.g., genetic manipulation, exosomes, proteins, microRNAs, etc.). Figure adapted from Devalla and Passier, Salvatori et al.22,171 3D, three-dimensional.
Although it may be a utopia to perfectly speak each other's language in multidisciplinary consortia consisting of clinicians, engineers, biologists, material scientists, and mathematicians among others, it is crucial to fully understand each other's objectives and hurdles. Furthermore, communication and interaction with other parties, including regulatory offices, governments, industries, patient and societal organizations, and media, are of equal importance to convey the latest developments and outstanding challenges and to achieve a clear understanding of reciprocal needs, which should be incorporated in educational programs for the scientists of tomorrow.
Heart Valve Tissue Engineering
Structure-function properties and their replication
The heart is equipped with four heart valves that collectively control directed blood flow through the organ: two atrioventricular valves (mitral and tricuspid valve), controlling the blood flow from the atria into the ventricles, and two semilunar valves (pulmonary and aortic valve), controlling the blood flow from the ventricles into the large arteries. Valve opening and closing behavior is driven by mechanical forces exerted by the blood and the cyclic contraction of the heart. 41 Valvular dysfunction can result from congenital or acquired diseases and may affect the valve tissue directly or secondary to diseases of the heart. 42 Despite the availability of nonliving surgical and transcatheter heart valve prostheses, tissue-engineered heart valves remain a highly desired solution for valve dysfunction requiring valve replacement. 43
This is mainly due to their proposed self-repair, remodeling capacity, and hence longevity compared to current bioprostheses44–46 as well as their potential to prevent thromboembolic complications common to mechanical valve prostheses. 47 Because of high clinical needs of durable semilunar valve replacements worldwide,48–50 heart valve tissue engineering has been centered around the creation of the pulmonary valve and the aortic valve. Both valves consist of three pliable leaflets, attached to the arterial root in a U-shaped, or semilunar, manner at the crown-shaped annulus. Together with three sinuses in the arterial root, they form cusps that fill with blood and tightly fit together during valve closure. The leaflets are sufficiently thin (∼500 mm) to be nourished by diffusion from the blood, 51 facilitating the engineering of these structures.
In cross-section, the leaflets consist of three layers with different composition and mechanical behavior, of which the collagen-rich fibrosa on the arterial side is the main load-bearing structure. This layer comprises a typical hammock-like collagen architecture, with thick collagen bundles running in circumferential direction, and more diverging bundles in the center region. This natural fiber reinforcement is strikingly similar between pulmonary and aortic valves 52 and creates anisotropic mechanical behavior, resulting in high strength in circumferential direction during valve closure, and high flexibility in radial direction during valve opening.53,54 The cells maintaining the semilunar leaflets are the valvular interstitial cells (VICs) that mainly home in the middle layer of the leaflets and the valvular endothelial cells (VECs) that cover the leaflets.55,56
In mature valves, VICs adopt a quiescent fibroblast-like phenotype with regulated contractile function, 57 whereas in developing, adapting, or diseased valves, VICs switch to a myofibroblast phenotype with an enhanced matrix remodeling function. 58 VECs share not only the same phenotypic markers and hemostatic properties as other ECs but also possess characteristics that distinguish VEC mechanobiology on one side of the valve from the other, and from other endothelial linings in the cardiovascular system.59–62
Traditionally, heart valve tissue engineering focused on the in vitro creation of autologous valves with properties as close as possible to native valves. Strategies involved the harvest and expansion of autologous cells, cell seeding onto preshaped, fast degrading scaffolds, and prolonged tissue culture in bioreactors before implantation. As VICs cannot be harvested autologously, various fibroblast and myofibroblast sources were tested,63–70 with vascular-derived myofibroblasts resulting in the strongest, collagen-rich engineered leaflets. 71 In contrast to cardiac regeneration, particular attention was paid to obtaining a functionally organized ECM architecture.72–75 To this end, mechanical conditioning protocols in bioreactors were designed, and computational modeling was used to understand and predict matrix architecture during tissue growth and remodeling.76–81
However, despite successful and predictable in vitro outcomes, preclinical studies showed suboptimal performance due to valve leaflet retraction caused by myofibroblast activity and ongoing matrix remodeling82,83—a process that could only be counterbalanced by removing the cells and adapting the shape of the leaflets.84,85
In situ tissue engineering
Thus, cell-free approaches developed wherein engineered heart valves were grown in vivo (e.g., subcutaneously)86,87 or in situ (i.e., directly at the functional site) from various acellular starter matrices. 88 Because of its more straightforward approach, offering cost-effective and off-the-shelf availability, in situ heart valve tissue engineering is currently gaining significant clinical and industrial interest. The procedure involves the implantation of a slow-resorbable, fibrous scaffold that is gradually remodeled by the recipient body into a living autologous valvular substitute via the recruitment of endogenous cells. Hence, the outcomes are orchestrated by both the scaffold and the recipient of the scaffold.89,90 Scaffolds that have been successfully used for in situ heart valve tissue engineering include decellularized homografts, 91 decellularized in vitro engineered matrices,92–94 and bioresorbable polymers of natural, synthetic, or hybrid origin. 89
Fresh decellularized homografts have the advantage of carrying the natural ligands and binding sites for cell adhesion and matrix remodeling and have demonstrated recellularization and long-term performance up to 10 years in clinical trials. 95 Yet, this method has limited availability as it requires human donor valves and shows donor-to-donor variability. Engineered tissue matrices and polymer scaffolds offer more controlled scaffold properties and can be created with high porosities to allow for proper cell engraftment and neo-tissue production. 94 Polymer scaffolds—in particular supramolecular synthetic scaffolds—have the additional benefit that they are scalable and highly tunable with respect to their resorption rate and their mechanical, chemical, bioactive, and microstructural properties.96–98 This is relevant in view of harnessing the foreign body response to the implant.
On the one hand, the foreign body response is essential for the inflammation driven formation of new tissue using the scaffold properties; on the other hand, it may cause excessive or chronic inflammatory responses, 99 necessitating more stratified or even personalized immunomodulatory approaches.90,100,101
Cell-free engineered tissue matrices and supramolecular polymer scaffolds have been extensively tested for the in situ creation of living heart valve replacements following surgical as well as transcatheter implantation in preclinical large animal models; so far, mainly for the pulmonary position.85,102–106 In general, these studies not only show good functionality and tissue outcomes but also some unpredictable intra- and intervalve variation in scaffold remodeling and degradation. 107 In addition, both scaffold types have been tested in clinical trials as vascular (access) grafts,108,109 while supramolecular scaffolds have recently entered the stage of clinical trials for pulmonary heart valves. 110
Multidisciplinary perspectives and challenges
To conclude, 25 years of heart valve tissue engineering research have resulted in a range of in vitro, in vivo, and in situ approaches, repetitious searches of the right combinations of scaffolds, cells, and mechanical conditioning, and an immense growth in multidisciplinary scientific output and topical journals. 111 Slowly, the field is entering the transition to clinical translation, specifically for off-the-shelf available in situ strategies. At the same time multidisciplinary consortia are exploring the use of living, in situ engineered valves for the repair of donor hearts or the application in total artificial hearts.112,113
Today's outstanding challenges for in situ heart valve tissue engineering include a profound understanding of scaffold-driven tissue formation in dependence of scaffold (degradation) properties and patient characteristics (e.g., sex, age), and under pathophysiological conditions. Although in situ tissue engineering starts with the proper scaffold, it is not sufficient to perform extensive laboratory research on heart valve scaffold production and design, while little to nothing is known about how the body will deal with such designs. As an illustrative example, it was observed during long-term in vivo follow-up in a sheep model that native heart valve mimicking, anisotropic leaflets, created by sophisticated electrospinning techniques, were remodeled back by the body into isotropically behaving leaflets. 114
From subsequent in vitro studies, it was concluded that aligned, anisotropic scaffold fibers are more quickly degraded by immune cells than their isotropic counterparts. 115 This example shows that basic and translational research should go hand in hand (Fig. 2). To this end, the field can learn from in situ regenerative approaches for applications in the vascular realm or the myocardium, as well as from in vivo immunoengineering strategies, 100 but should not omit the morphology and hemodynamic environment relevant for heart valve growth and remodeling. Mechanistic understanding should then be implemented in predictive models—both experimental and computational—to enable the development of safe and reliable patient-centered heart valve tissue engineering strategies that outperform inert implants in quality of life and cost-effectiveness.
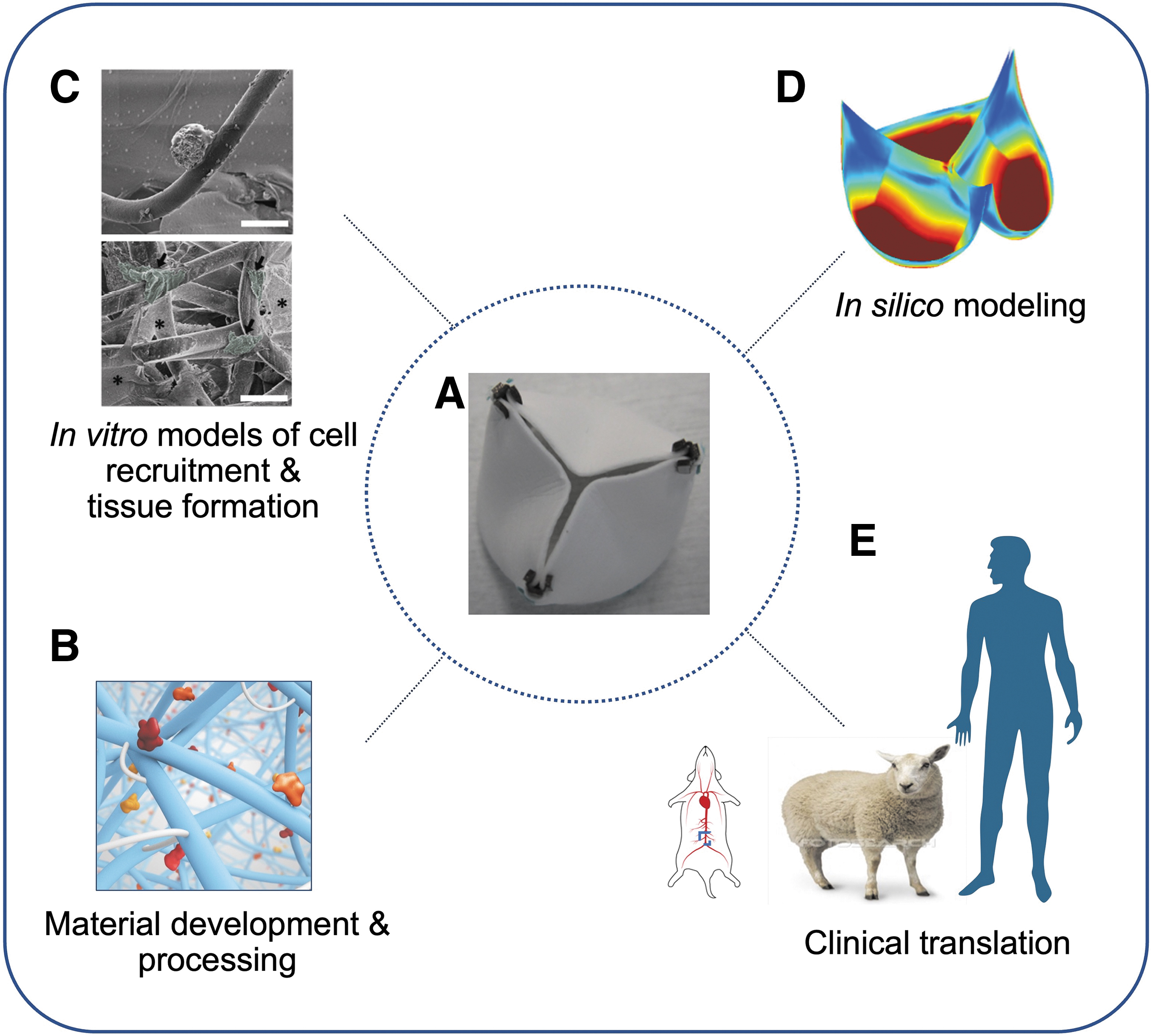
Convergence of disciplines for material-driven in situ heart valve tissue engineering.
Vascular Tissue Engineering
Structure-function properties and their replication
The human vascular system acts as a critical biological infrastructure that continuously ensures that blood circulation can meet the dynamic metabolic needs of the body's different organs. Although categorized into the specific segments of arteries, veins, arterioles, venules, and the capillary bed, all vessels are mainly composed of ECs and mural cells, with variations in anatomical structure to suit local function. In relation to vascular disease, large-sized arteries (>3 mm) such as the aorta, the carotids, and the coronary arteries have been thoroughly investigated as they present either the culprit sites for atherogenesis and stenosis, leading to cardiac ischemia and stroke, or detrimental remodeling, leading to aneurysms. As a result, the field of vascular tissue engineering has mainly focused on replacement strategies for large-sized arteries. 116
Nevertheless, in recent years, the focus of cardiovascular research has been shifting to smaller sized arteries, such as cardiac arterioles (100–300 μm luminal diameter), as it is recognized that myocardial ischemia also occurs in the absence of a flow-limiting stenosis in the large coronaries. This so-called INOCA (Ischemia and No Obstructive Coronary Artery Disease) is caused by structural and functional abnormalities in coronary arterioles, and is an important risk factor for adverse cardiovascular events, including heart failure, cardiac death, and stroke. 117 Representing the terminal branch of the arterial tree, arterioles are also critical for the regulation of blood flow to the microvascular bed in relationship to metabolic need. Yet, due to limitations in fabrication techniques and the loss of patency observed in vivo for small caliber (<6 mm lumen diameter) synthetic scaffolds, tissue engineering strategies for arteriole replacement remain largely unexplored.
In situ tissue engineering
Current meanstream strategies of vascular tissue engineering start from synthetic scaffolds, where electro-spinning is often used to create meshes that recapitulate the fibrous structure provided by the vascular ECM. As the technology progressed, the trajectory began to resemble that of the evolution of vascular stents, including the introduction of bioabsorbable material and the coating with biomolecules to promote cell recruitment and scaffold cellularization.11,12118 Polymer fiber thickness, alignment, and average pore size were also optimized for cell infiltration and tissue growth.119–121 More recent trends in design shifted toward bioabsorbable materials with advanced properties, such as the use of ureidopyrimidinone (UPy) polymers that allow material healing, as well as the coupling of chemical moieties that permit biofunctionalization by binding with (and slow release in situ of) organic biologically active ligands.122,123
Critical for these strategies that all largely rely on in situ tissue formation, is for locally recruited cells on the synthetic scaffolds to not only survive and proliferate, but also to acquire the desired functional phenotype. Biological concepts, such as (ligand-guided) phenotype switching of vascular cells, including from synthetic to contractile vascular smooth muscle cells (VSMCs), angiogenic to quiescent ECs, and EndMT, have been introduced to understand cell behavior during tissue formation on synthetic scaffolds.124–128 Molecular mechanisms that govern EC/VSMCs/ECM interaction such as Notch, PDGFβ, and TGFβ signaling, known to play critical roles in adverse vascular remodeling and stenosis, were further explored for scaffold-based strategies.129–132
Unlocking the key players in these mechanisms is a critical step, as this will ultimately determine function and long-term success of the vascular graft during and after polymer degradation. Moreover, as we advance our understanding of interaction between vascular and immune systems, we are beginning to use the latter in driving the in situ regeneration of the former to obtain the desired level of tissue expansion.133,134 Next generation vascular scaffold should therefore explore new strategies for material guidance of the desired vascular phenotypes through chemical modifications and biofunctionalization.
In addition, in situ generation of functional tissue with the desired phenotype is likely also determined by the response of recruited cells to hemodynamic forces.135–138 In vitro studies demonstrated that phenotype switching can be induced in VSMC by (coating) substrate stiffness 139 and by hyperphysiological levels of cyclic stretch.140,141 Similarly, EC switching from quiescent to angiogenic and EndMT is modulated by shear stress.142,143 Advanced scaffold design should therefore also include structural/chemical fiber adaptations for guiding local mechanical stimulation of recruited cells toward the desired phenotype. This is complicated by the natural local strains that govern cell behavior as it is experienced differently by ECs and VSMCs, due to differences in compositions of the ECM at their specific locations of the vessel wall.
To resolve this, the emerging concept of multilayer vascular scaffolds designs may offer a solution. Scaffold constructs composed of 2-or-more layers, each with a fiber thickness and pore size optimized for one particular vascular cell type, have already been tested and proven their feasibility.144–146 Further fine tuning of mechanical, structural, material, or biofunctionalization parameters for each dedicated layer will allow zoning according to different tissue formation strategies, such as enhanced medial infiltration and alignment for VSMCs.
Multidisciplinary perspectives and challenges
In summary, in the last decade, the field of vascular tissue engineering has greatly accelerated due to growing interaction between researchers in vascular biology and material and fabrication engineering and has boosted the development of design-guided in situ scaffold cellularization. The concepts learned from these studies highlight the key facets that future approaches need to advance to clinical translation of the technology. The near-term goal should be to introduce large artery and arteriole grafts with the inherent capacity not only to replace but also function like a native vessel, with focus on responsiveness to local metabolic requirement (vasomotion regulation via quiescent EC and contractile VSCM interaction) and if necessary, remodeling capacity for adaptation to suit the patient's physiology (Fig. 3).
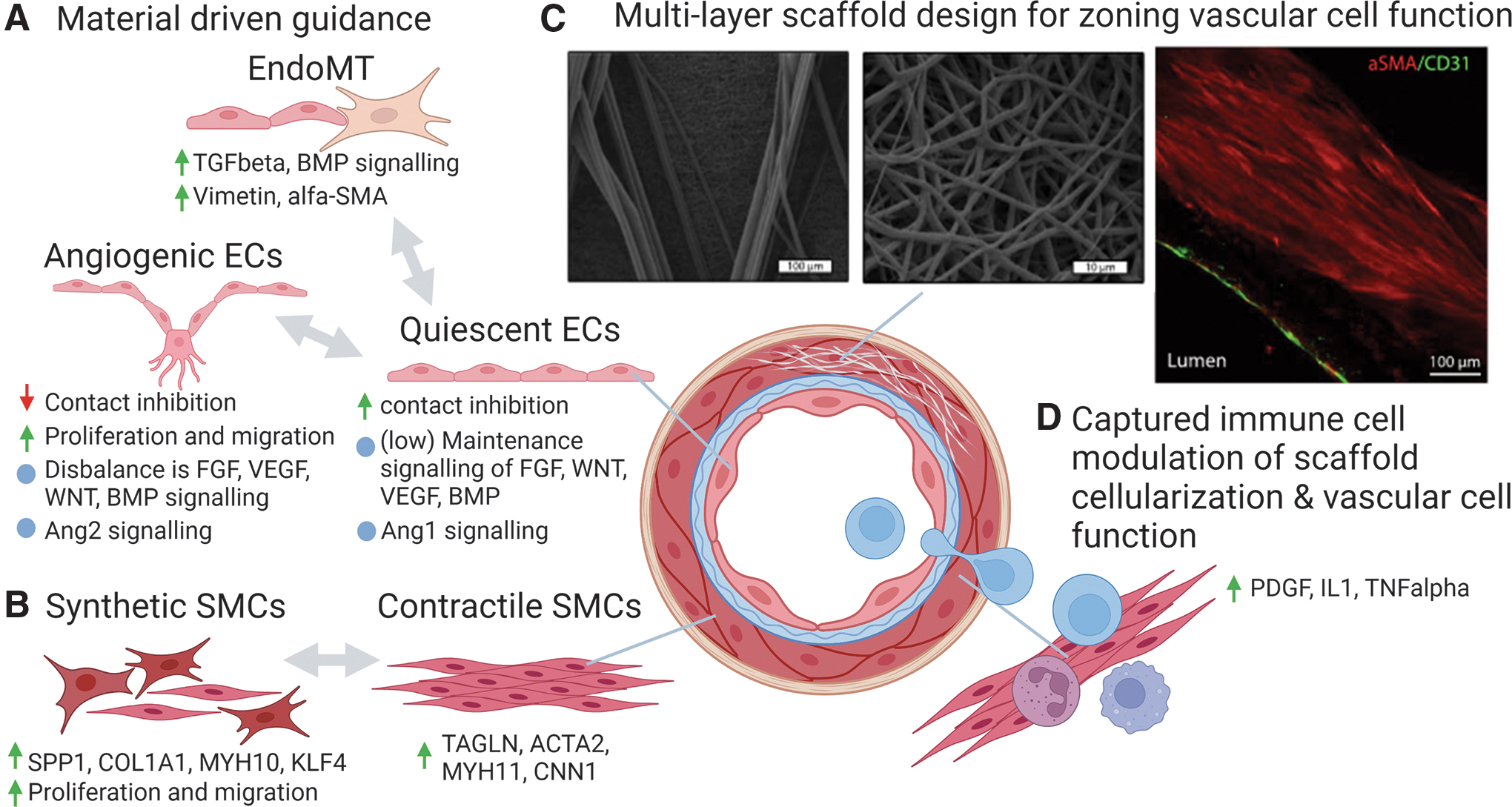
Next-generation vascular scaffolds define vascular cell function via material and design driven guidance.
If graft functionality can be achieved, the next challenge will be to connect the large artery and arteriole segments to the microvascular bed, possibly by regulating the natural branching pathways, which will then eventually open the door to pre- (or partial in situ) vascularization of complex organ grafts. Particularly for connectivity, further expansion of cross-disciplinary collaboration with researchers specialized in the biology of the target organ is crucial. Although one more or less universal vascular design might suit for the replacement of a range of large arteries and veins, a more specialized approach would be required for organ-specific vascular beds, such as for the recreation of the functional glomerular capillary clusters of the nephron unit in the kidney, or the myofibril aligned capillary structures of the heart.
Furthermore, for some patients, the origin of (cardiovascular) disease may be genetic, or the regenerative capacity of the endogenous vascular (progenitor) cells may be compromised by age. Several research groups currently are investigating the use of hypoimmunogenic iPSCs, which effectively targets adaptive as well as innate immune activation to limit allograft response.147–149 Theoretically, this makes it possible to create nonimmunogenic hiPSC lines that permit allogeneic transplantation of hiPSC-derived tissue that is immune-compatible to any patient recipient. In light of these developments, collaborations with these researchers could lead to the development protocols, in which vascular cells derived from “off-the-shelf, allogenic” hiPSC can be used for (ex vivo) cell seeding of synthetic scaffolds for treatment of these specific patient groups.
Downscaling toward the microvasculature
For midsized arterioles, the required size range (100–300 μm) test the boundaries of what can currently be achieved by the electrospinning approach. Alternatively, different strategies in biofabrication have been pursued to recreate vascular-like structures, including an array of 3D printing techniques, including droplet, light based, and extrusion bioprinting.150–154 For the fabrication of midsized arterioles, extrusion 3D bioprinting may be the most suitable. In particular, coaxial extrusion spinning, a branch of the technique that can generate layered filaments by using specific nozzles that simultaneously deposit two or more flow streams in concentric rings, has proven to be capable of producing (potentially arteriole sized) hollow tubular constructs with a bilayered wall of ECs and VSMCs encased in hydrogel.153,154
Nevertheless, the strategy requires further optimalization, as whole EC hydrogel encasement may limit EC monolayer formation. Also, current vascular biofabrication strategies are mainly focused on strategies that ensure cell survival and proliferation, but often neglect to create an environment to promote desired cell function. At the same time, follow-up studies that investigate the biological response of these biofabricated constructs to physiological levels of hemodynamic stress are often altogether lacking. Future steps should therefore focus on the optimization of the bioink environment to ensure vascular functionality and investigate the impact of hemodynamics on the biology and anatomy of these constructs. Increased collaboration between biofabrication and bioink experts with vascular biologist could accelerate this strategy.
Engineering the Microvasculature, in Connection to the Organ
Structure-function properties and their replication
Microvascular beds supply tissues and organs with blood. Due to the extent of these intricate vascular networks, most cells in the body are located within a 200 μm distance from a vessel. The branching of the microvascular network is complex but can be recapitulated by cellular self-assembly.155,156 By combining endothelial (progenitor) cells and supporting cells before implantation, functional microvasculature can be formed in small implants (e.g., in implanted cardiac patches 157 ). Such networks can connect to host vasculature and become functionally perfused with blood. For larger tissue constructs, this approach does not work. Due to their size that exceeds several millimeters in all directions, core necrosis of the tissue will be an issue within hours to days. The vascular self-organization and connection to host vasculature will take more time than the cells can survive without blood supply in tissue exceeding the millimeter scale.
To accommodate scaling up the size of engineered tissues, additional control over vascular architecture is required. When attempting to regenerate precultured larger tissues (centimeter-scale) containing vasculature and tissue cells, it is crucial to (i) sustain cell viability and functionality during culture, and (ii) connect to host vasculature upon implantation as quickly as possible to sustain cell survival.
The first point can be fulfilled, providing that the microvascular bed is sufficiently extensive to serve all cells in the engineered organ system and it has an interconnected lumen that is accessible for effective fluid or blood perfusion. If, in addition, tissue-specific cells are present that also require the supply of specific culture media, the culture system is further complicated. However, examples do exist where separate culture compartments were created to each support the ECs or the tissue-specific cells.144,158
Besides, the presence of the network, an adequate perfusion system needs to be connected to provide a laminar-like flow that is normally present in capillaries. Capillary flow stimulates vessel maturation and antithrombotic properties, although this has been rarely demonstrated for extended culture periods in vitro. Physical solid shear interactions provided by blood cells squeezing through this system are seldom considered. To test these in vitro networks, next to histological and microscopic examination of EC quality, the functional perfusion is demonstrated, typically by containment of fluorescent dyes or fluorescent microbeads in the network. 159
The second challenge requires a connection of the self-assembling microvascular network to small collecting vessels that feed into larger vascular structures of a diameter that can be sutured to host vasculature via microsurgical techniques or connected otherwise. Various approaches are under investigation, such as prevascularization of tissue (with or without an AV loop) at an ectopic location with subsequent transplantation to the defect site, including the newly formed vascular supply.160–162
But how far do we need to go in replicating the microvasculature? Is it sufficient to let cells self-organize into microvascular structures? Or do we need to use modern technologies such as 3D bioprinting to impose detailed vascular architectures?
On the one hand, the field is leaning toward a combination of both; where the smallest structures are self-organizing and the collecting microvessel-architecture is imposed by 3D bioprinting technologies (Fig. 4A, B 163 ). On the other hand, imposed organization of self-organization could also be useful in specific cases, such as illustrated by improved liver tissue functionality following guided endothelial self-assembly in dictated patterns within a tri-culture system (hepatocytes, ECs, fibroblasts). 164 With the ever-increasing progress on the engineering side, including higher resolutions and more accommodating bioink printing properties, current bioinks represent a compromise of bioprintability and biocompatibility, this prescribed self-assembly of microvasculature may represent a novel microvessel-patterning strategy in the field.
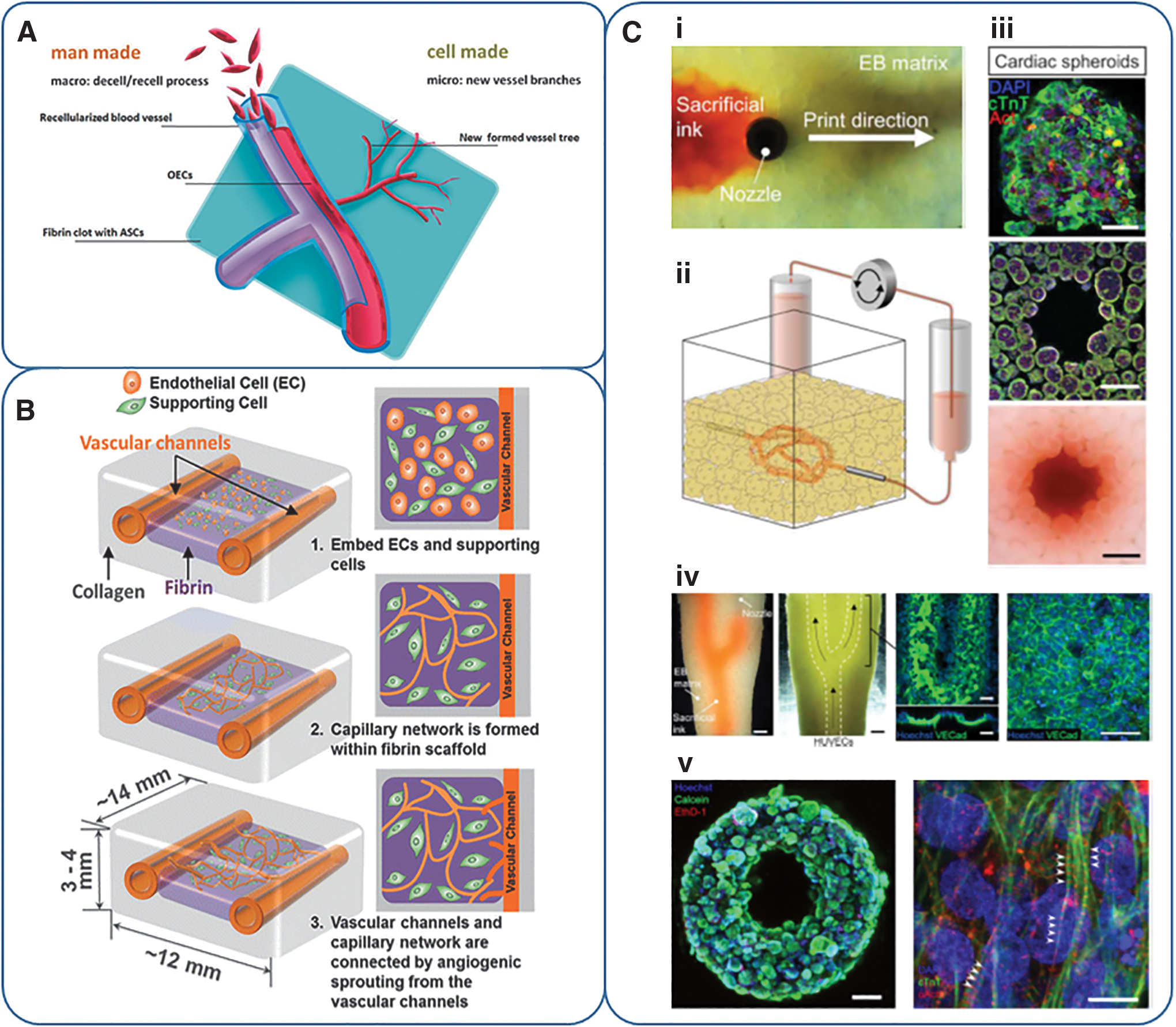
The challenge of balancing the combination of man-made vessels and self-assembled microvasculature.
Nevertheless, despite the sheer endless technological possibilities, it is crucial to not only focus on what is technically possible, but to also realize what is needed in terms of tissue biology, functionality, and integration (of microvasculature within the target tissue, and by anastomosing to vessels of the adjacent scale and to the host vasculature). In current engineering approaches, the collecting vessels are mostly channels that are at times seeded with an endothelium, without taking a layered structure of the vascular structures into account. Characterization of the endothelium and creating a supporting layer of mural cells is often overlooked, while integrity and confluence of the endothelium and cellular interconnection (e.g., connexin 43, VE-cadherin), as well as formation of a shared basal membrane (e.g., collagen type IV) also deserves attention.
Interesting new biofabrication techniques such as SWIFT (Sacrificial Writing Into Functional Tissue) have been developed that can generate hollow channel structures directly in a dense tissue bulk, yet still at rather low resolution. 165 This technology was applied to generate channeled cardiac tissues with improved functionality upon perfusion, although without the simultaneous presence of a functional endothelium (Fig. 4C). To advance this approach, scale-up, resolution, combinatory culture of endothelial, vascular, and tissue cells, and survival of such tissues remain challenges to be tackled.
Reports on interconnection of a self-assembled capillary bed and collecting channels are still relatively rare and progress is in its infancy.166,167 For example, Lee et al. 166 showed interconnection of the endothelium inside collecting channels with capillary-like structures in a bulk hydrogel. However, upon perfusion of the vascular channels, sprouting and interconnection were halted, rather than stimulated. The field's understanding of the hemodynamic demands for the development of these delicate interconnections is limited, and studies involving perfusion of multiscale vasculature inside a target tissue are scarce, especially for culture periods exceeding 24–48 h.
The creation of the microvascular bed in general has been studied extensively, but the simultaneous generation, survival, and maturation of a target tissue, in which it is embedded, are often lacking. In addition, perfusion of channeled target tissues is often reported, but rarely while an endothelium is present inside the channels; or if present, it is not characterized under such circumstances. Further progress in this area will require tissue-specific approaches by combining vascular and tissue-specific cells, matrices, culture supplements, fabrication techniques, and culture periods.
Multidisciplinary perspectives and challenges
Concluding, biologists, tissue engineers, material scientists, and biomedical engineers have tackled several challenges of microvasculature reconstruction and/or guided self-organization. Expertise is becoming more and more combined, resulting in advanced prevascularized culture systems, but clinical application of these approaches is not within sight. The field now demands a fresh perspective to keep moving forward. Existing consortia should intensify their collaboration and consider the involvement of developmental biologists studying the vascular tree or microvascular surgeons to realize development of multiscale vascular systems and their potential to be anastomosed to one another or the host circulation. In addition, involvement of target tissue experts and bioreactor engineers can extend the generation of vascular systems inside a living target tissue that can be maintained until anastomosis.
The rapid pace of developments of novel printing techniques, increasing printing resolution, and the emergence of more biologically compatible bioinks also warrants the inclusion of the biofabrication specialist in each team, to not miss out on any opportunity in this dynamic area. Further, consultation of clinicians as well as patients should be included to address and maximize adoption and acceptance of envisioned strategies by these end-users.
Discussion
The evolution of research in the four areas reviewed here—shows different starting points and a different integration of disciplines. Myocardial regeneration has traditionally centered around the search to replace cardiac contractile cells and can build on long-standing experience with in situ delivery of regenerative cells, drugs, materials, or other compounds, typically performed by consortia consisting of cell biologists and clinicians. With ongoing preclinical studies, many failures, and very slow progress, the field has recognized the importance of the cardiac host environment and has turned to in vitro tissue engineering and organoid technology to investigate the impact of the cellular environment on therapy outcomes and to solve other major challenges, such as the realization of a perfusable vascular network and organization and maturation of cardiac tissue.
In contrast, the areas of heart valve and vessel tissue engineering have started from in vitro tissue engineering and are only recently turning to in situ regeneration. Because of this evolution, the area has extensive know-how on how to regenerate structure-function properties, including ECM organization and layered tissue formation. Consortia working in this area originally consisted of cardiac and vascular surgeons as well as tissue engineers with expertise on scaffold fabrication, bioreactors, and structural and mechanical tissue characterization. With the shift toward resorbable scaffold-based in situ regeneration, research consortia more and more require the expertise from material scientists, immunologists, and cell biologists.
Despite an incomplete understanding of neo-valve and vessel formation in situ, particularly under complex hemodynamic loading and with patient comorbidities, the approach is currently tested in clinical trials. 43 Because in situ valve and vessel regeneration starts from cell-free off-the-shelf available implantable scaffolds, the approach is scalable, has low regulatory complexity, and is attractive for industry—and thus is expected to have clinical impact within the foreseeable future.
Finally, in the area of microvasculature regeneration, approaches where engineers precisely fabricate vascular networks or cell biologist take control of self-assembly and network formation come together. This area tackles one of the major challenges of tissue engineering: the vascularization with a complex vascular tree of engineered tissues and organs for perfusion. The involved researchers are well informed about complex tissue fabrication and the integration of tissue and vascular engineering, but the required integration of these disciplines to synergistically accelerate the field is still in its infancy.
This area might profit most from convergence of knowledge across the separate areas of cardiovascular regeneration. For instance, by building on established knowledge derived from microfluidic organ-on-chip systems on the interaction between fabricated microstructures of vascular cells and engineered cardiac tissue, or benefitting from the experience with stimulating natural anastomoses for material guided connectivity between large and microvascular structures in the area of in situ tissue engineering.
Further progress in this and the other areas can be achieved by enhanced convergence of knowledge on generic research questions, for example, related to the dependence of (vascularized) neo-tissue formation on scaffold properties, patient characteristics or pathophysiological conditions. In addition, convergence of experience in the context of regulatory requirements, clinical translation, and market introduction will enable faster and more effective strategies to cure the cardiovascular system and even fertilize other fields of regenerative medicine.
While this viewpoint and its relevance is echoed by many in the field of cardiovascular tissue engineering and regeneration, successful and effective knowledge integration across the separate cardiovascular research areas is far from common. The question is as follows: how to improve that?
Despite the challenges to manage and carry out multidisciplinary research, the field of tissue engineering has proven excellently how integrated methodologies and combined insights can tackle complex problems and extend the possibilities of discovery. 168 Multidisciplinary collaborations have resulted in new research approaches, new research groups, and even new research institutes; and hence have impacted the field as a whole. Still, cross-discipline, cross-area fertilization, and knowledge sharing are cumbersome as they may not directly benefit the individual researcher (e.g., in terms of recognition) or research area.
It may require different incentives and a different—perhaps top down—research organization, in which other parties collaborate next to scientists, clinicians, and industrial partners. In this context, we would like to illustrate the current research organization in the Netherlands. We do not argue that it is ideal and should replace other systems, but rather acknowledge its benefits and drawbacks.
The Netherlands, with its high density of researchers, universities, and university hospitals, has a strong tradition in multidisciplinary collaboration and building national research consortia. Because of the small size of the country, it is easy to tackle one of the key challenges of successful collaboration: spatial distance. 168 Starting from the early 2000's, a series of public private partnerships (PPP) was installed by national leaders in the field, and financially supported by the Dutch government. This commenced with the Dutch Program for Tissue Engineering (DPTE), followed by the Tissue Engineering and Regenerative Medicine (TERM) consortium, the BioMedical Materials (BMM) institute, and the Netherlands Institute for Regenerative Medicine (NIRM). Key to these PPPs was a strong convergence of disciplines, which still exists today.
Research programs mainly covered the cardiovascular area and musculoskeletal area, later extended with organ regeneration (e.g., kidney, islets of Langerhans), and researchers met regularly in small and larger teams. The research consortia were extended with partners from industry and patient organizations to slowly build an ecosystem for valorization and clinical implementation. The latter turned out to be more complex than anticipated and required more time. Only recently, this aspect was resuscitated under the auspices of the Regenerative Medicine Crossing Borders (RegMed XB) consortium. 169 All consortia team up with patient organizations, such as the Dutch Heart Foundation, which act as matchmakers and promotors of patient-centered, impact-oriented research.
With time, it became clear that placing the patient center stage is a strong driver for collaboration and commitment of all partners and today the role of patient organizations is quite prominent in accelerating science and achieving clinical impact. Importantly, in the so-called Cardiac Moonshot of RegMed XB, cross-area collaboration and integration is installed top-down, as partners investigating cardiac muscle regeneration, heart valve tissue engineering, cardiac neo-vascularization, and organ transplantation are closely working together to regenerate the heart in toto.
In parallel, and at the initiative of the Dutch Heart Foundation, the Netherlands CardioVascular Research Initiative (CVON) was started. This initiative centered around focal research areas driven by leading research teams. Here, multidisciplinary research collaboration between basic and translational researchers was installed top down. Recently, the research centered CVON program was extended with all leading partners in the cardiovascular community, including industrial partners, organizations for health care professionals, and organizations of academia. Together, they form The Dutch Cardiovascular Alliance (DCVA) 170 that builds on existing assets to improve the innovation infrastructure, including science, valorization and implementation, talent development and exchange of researchers between communities, and community building.
DCVA and RegMed-XB team up to leverage the field of cardiovascular regeneration and bring solutions to the patient. While only the future will learn if and how this leads to enhanced clinical and socioeconomic impact in the cardiovascular area, it has for sure resulted in a large network for exchange and sharing of knowledge, data, and infrastructure, with short lines between researchers, industry, and policy makers.
Footnotes
Authors' Contributions
All authors contributed to this review and approved the submitted version. C.V.C.B. compiled the article and oversaw its creation. R.P. wrote the section on myocardial regeneration. C.V.C.B. wrote the heart valve tissue engineering section. C.C. and I.J.V. wrote the ![]() section, while D.G. wrote the section on regenerating the microcirculation.
section, while D.G. wrote the section on regenerating the microcirculation.
Disclosure Statement
The authors declare no competing interests that may inappropriately influence or affect the integrity of the contents of the article. C.V.C.B. is nonvoting share holder of Xeltis BV. R.P. is a cofounder of Pluriomics (NCardia) and River BioMedics.
Funding Information
C.V.C.B., C.C., I.J.V., and D.G. gratefully acknowledge support by the Gravitation Program “Materials Driven Regeneration,” funded by the Netherlands Organization for Scientific Research (024.003.013).