
Abstract
Lung transplantation remains the only curative treatment for end-stage pulmonary disease. Lung ischemia–reperfusion injury (IRI) is a major contributor to primary allograft dysfunction and donor organ nonutilization. The alveolar macrophage is a key inflammatory mediator in IRI. Ex vivo lung perfusion (EVLP) has been investigated to rehabilitate lungs before transplant but has failed to provide significant improvements after IRI. We hypothesized that liquid ventilation (LV) could be utilized for ex vivo lung reconditioning in a rat IRI model. We compared EVLP with LV in an isolated ex vivo rat lung with an aqueous ventilant using quantitative physiological and immunological parameters. We observed improved physiological parameters and mechanical clearance of alveolar macrophages and cytokines halting the propagation of the inflammatory response in IRI. While the wide applicability to large animal or human transplantation have yet to be explored, these findings represent a method for lung reconditioning in the setting of significant IRI that could widen the lung organ donation pool and limit morbidity and mortality associated with ischemia-induced primary graft dysfunction.
Impact statement
Lung transplantation remains the only curative treatment for end-stage pulmonary disease. Ischemia–reperfusion injury (IRI) is a major contributor to primary allograft dysfunction and donor organ nonutilization. In this study, we report a novel method for ex vivo lung reconditioning after significant ischemic injury with improved, clinically relevant physiological parameters using liquid ventilation (LV). These improvements may result from mechanical clearance of alveolar macrophages and inflammatory cytokines, which blunt the propagation of IRI in addition to minimizing mechanical stress during the early reperfusion period. LV is a potential method for lung reconditioning that could widen the lung organ donation pool and make a positive clinical impact on patient outcomes.
Introduction
Lung transplantation remains the only curative treatment for patients with end-stage pulmonary disease. 1 The shortage of donor lungs and the troublingly low rate of donor organ utilization increases wait list mortality. 1 Only 15% of donor lungs are deemed to be acceptable for transplantation after organ offer. 2
Ex vivo lung perfusion (EVLP) was developed in an effort to increase the pool of available lungs for transplantation by allowing ex vivo functional assessment.3,4 It soon became apparent that this platform could be used to precondition and improve lung function before transplantation, revitalizing an organ that would have initially been rejected into a usable allograft. 5 Increasing the donor organ pool and decreasing both wait list time and wait list mortality are achievable goals with ex vivo organ treatment. EVLP has also become an emerging tool in mechanistic studies of lung injury and recovery in an organ-specific environment.6–8
Despite efforts to minimize lung ischemia during organ procurement and transport, lung ischemia–reperfusion injury (IRI) is still a major contributor to posttransplant allograft dysfunction. 9 Mechanistic studies in this area indicate that activation of alveolar and interstitial macrophages plays an instrumental role in the initiation and progression of lung IRI. 10 During ischemia, macrophages are exposed to hypoxic and oxidative stress leading to cytokine secretion, which promotes neutrophil recruitment, endothelial activation, and mast cell degranulation.9,11 The subsequent inflammatory response results in the physiological hallmarks of IRI, such as interstitial and alveolar edema, decreased lung compliance, and increased pulmonary vascular resistance (PVR) followed by poor oxygenation and primary graft dysfunction. 12 Macrophage depletion using liposomal clodronate has been established in murine models to investigate the role of macrophages in pathological processes.13–15 In IRI, depleting macrophages could prevent the development of macrophage-propagated lung injury. 10
When considering methods for lung rehabilitation from significant IRI, we revisited the concept of total liquid ventilation (LV) but in an ex vivo setting. Total LV is a process by which the gaseous inflation of the lung is replaced with a fluid. The fluid is cyclically exchanged as air is normally during inspiration and expiration. This fluid can have a variety of compositions from an oxygen-carrying fluorocarbon to a simple crystalloid solution. The literature is sparse regarding the benefits of LV as a respiratory treatment. LV was first introduced to minimize lung injury by reducing alveolar surface tension during mechanical ventilation to prevent injury related to repeated atelectasis and barotrauma.16,17 LV has shown promise for premature lung diseases by decreasing alveolar surface tension, promoting homogeneous lung expansion, and increased gas exchange. 18 Patients with severe respiratory failure on extracorporeal life support have been treated with LV as a salvage with some improvement in gas exchange.19–22 LV has the additional benefit of mechanically removing proinflammatory mediators and debris from the respiratory system. 23
Airway lavage have been studied in posttransplant lung function after gastric aspiration injury, which reduced proinflammatory cytokines and lung inflammation. 24 Partial LV has been trialed as a lung preservation method before transplantation25–27 or to improve allograft injury after transplantation28,29 with mixed and marginal results. Presently, there are no published data on the use of ex vivo total LV to recondition marginal or extended criteria lungs for transplantation.
In this study, we describe a unique and novel method of ex vivo lung reconditioning using a rat model of total LV with a liquid ventilant for use in transplantation. We hypothesized that alveolar macrophage-mediated inflammation and IRI can be reduced. We believe LV clears harmful damage-associated molecular patterns (DAMPs), which facilitate macrophage activation, neutrophil migration into the pulmonary interstitium, and endothelial dysfunction. Additionally, the mechanical clearance of proinflammatory cytokines released into the alveolus under cellular stress in the early ischemia–reperfusion phase may allow for cellular metabolic recovery during LV. We further attempted to isolate the pathological contribution of macrophages to the inflammatory response by depleting macrophages in the organ with liposomal clodronate.
Materials and Methods
Experimental groups
Thirty single left rat lungs were sorted into five unique groups (n = 6/group). Single lung experiments were performed to facilitate homogeneous airway pressure changes during LV. Rat left lungs are a single lobe, and the lobar bronchi are relatively collapsible making the multilobed right lung suboptimal for this proof-of-concept set of experiments. It is important to note that not all experimental endpoints could be performed for each experiment due to differences in tissue handling for terminal analysis. This resulted in smaller groups for certain experimental endpoints.
The “control” lungs were procured immediately after cardiac death, flushed with preservation solution, exposed to 4 h cold preservation, then placed on EVLP for 6 h for assessment. The control group was still exposed to cold preservation to mirror current practice providing a clinical correlate. There were four “experimental groups,” in which all underwent warm ischemia followed by an intervention. The “warm ischemia” lungs were exposed to 4 h of in vivo warm ischemia (sacrifice followed by 4 h at room without thoracic cavity violation), followed by lung procurement, flush with preservation solution, 4 h of cold preservation, and 6 h of EVLP assessment.
This period of ischemia was selected to induce significant physiological injury to the organ, much greater than is currently clinically acceptable, to evaluate the effect of each experimental condition on organ recovery. The “liquid ventilation” lungs were treated similar to the “warm ischemia” lungs with the exception that the 4 h of cold preservation was replaced with 4 h of LV (see “Liquid ventilation protocol” section). The “EVLP-Clodronate” and “LV-Clodronate” groups were similar to the “warm ischemia” and “liquid ventilation” groups, respectively, with the exception that liposomal clodronate was added to the flush solution after lung procurement. Figure 1 provides an experimental flowchart for the treatment groups.
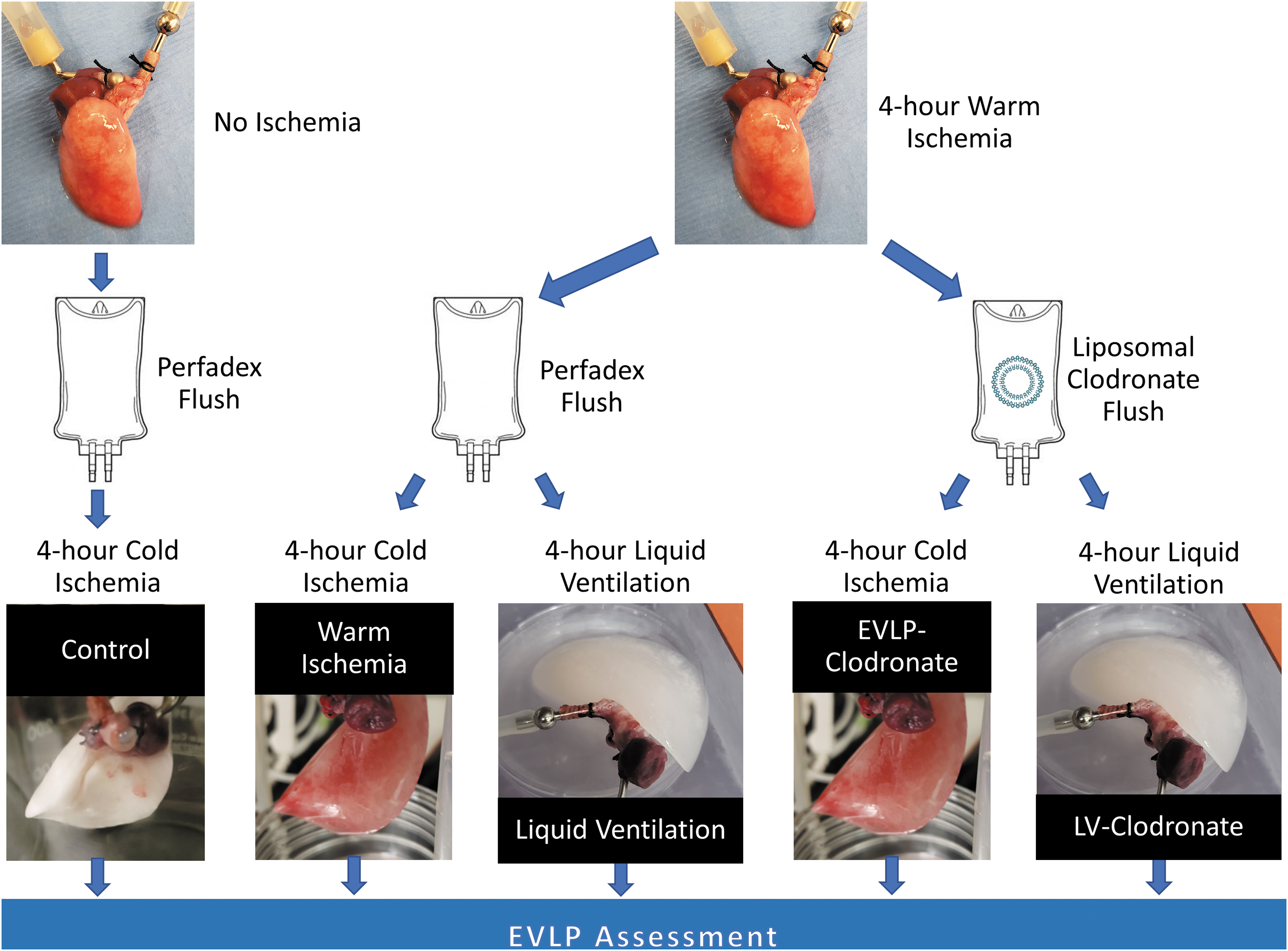
Experimental flowchart delineating the protocol for each treatment group. EVLP, ex vivo lung perfusion; LV, liquid ventilation. Color images are available online.
Lung procurement, treatment, and assessment
All animal studies were approved by the Massachusetts General Hospital Institutional Animal Care and Use Committee Protocol No. 2019N000059 and conducted in accordance with The Guide for the Care and Use of Laboratory Animals. Lungs were explanted from outbred adult male Sprague–Dawley rats (250–450 g, Charles River Laboratories, Wilmington, MA). All rats were pair housed and given unrestricted access to chow and water. Animals were anesthetized with 5% isoflurane, a laparotomy was performed, heparin was administered, and the animal was sacrificed through exsanguination.
Following sacrifice and warm ischemia time (if applicable), the heart and lungs were procured en block.30,31 The heart apex and left atrial appendage were resected to allow for pulmonary venous outflow. An arterial cannula was inserted in the pulmonary artery through the right ventricular outflow tract and secured. Similarly, a cannula was secured in the trachea. A right pneumonectomy was performed. The left lung was either recruited with ∼3.0 mL air or 3.0 mL phosphate-buffered saline (PBS; Life Technologies Corporation, Grand Island, NY) for the EVLP alone groups or LV groups, respectively. An antegrade flush was performed with 30 mL of cold low potassium dextran solution (PERFADEX, XVIVO Perfusion Inc., Gothenburg, Sweden). For clodronate groups, 5.25 mg liposomal clodronate (Liposoma BV, Amsterdam, Netherlands) was added to the flush solution. The lungs underwent either cold storage or LV for 4 h before EVLP assessment, depending on group assignment.
EVLP protocol
A custom EVLP system was designed to allow constant arterial flowrate with passive venous outflow. A reservoir containing albumin-based electrolyte solution (components and chemistry in Tables 1 and 2, respectively) was connected to an organ chamber through silicone tubing. Positive displacement roller pumps controlled the arterial inflow and return of venous effluent from the lung (Fig. 2A). The EVLP system was housed in a 37°C incubator for normothermic perfusion. 32
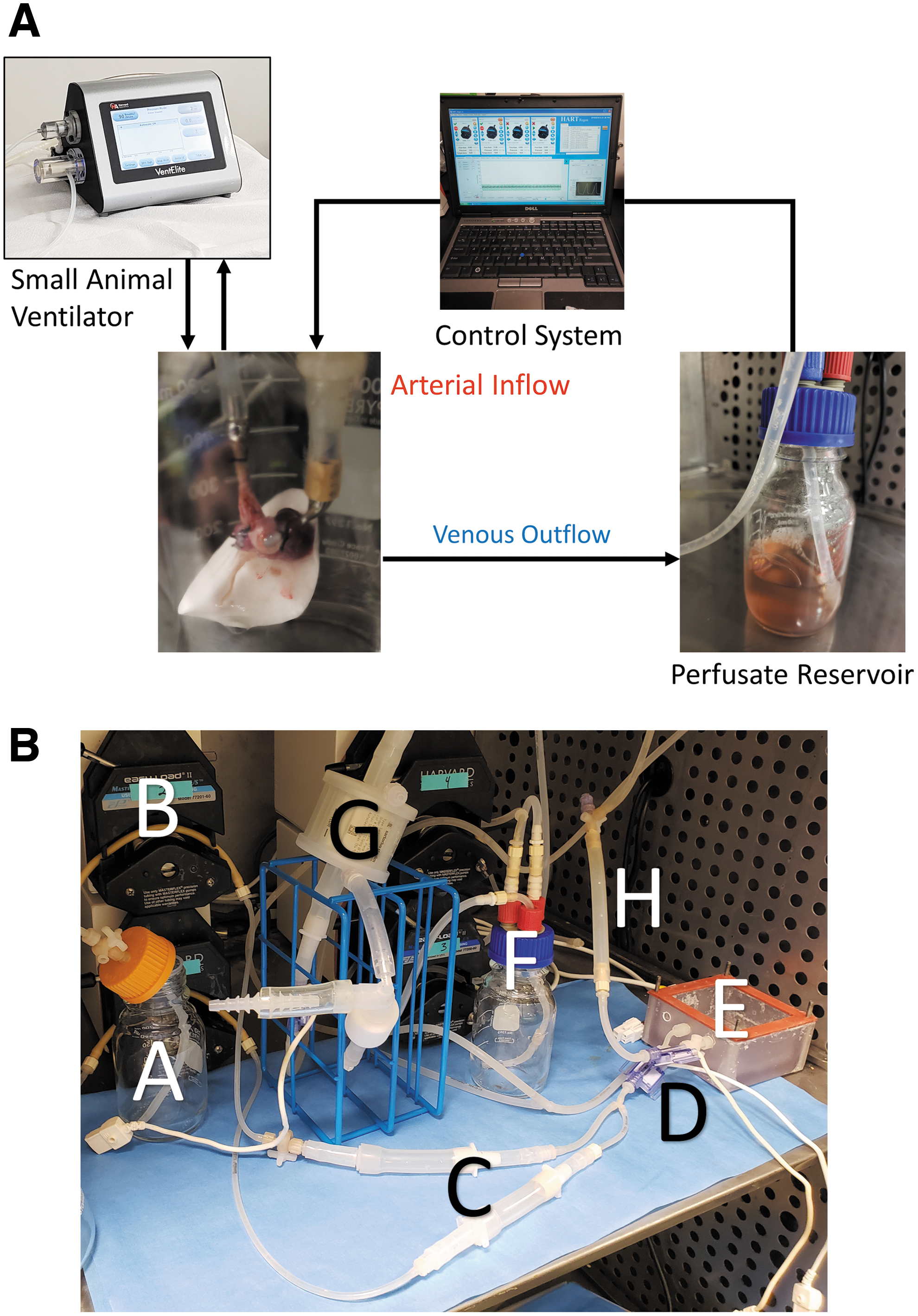
Representative system diagrams for EVLP and LV circuits.
Composition of the Albumin-Based Electrolyte Perfusion Solution Used During Ex Vivo Lung Perfusion
Chemistry Analysis of the Albumin-Based Electrolyte Perfusion Solution Used During Ex Vivo Lung Perfusion
The lung was recruited with room air at 20 mL/kg through the tracheal cannula before the initiation of perfusion. Perfusion was gradually increased over the first hour to a target flow rate of 6 mL/min/g of predicted lung weight (PLW) utilizing the formula PLW (g) = 0.0053 × body weight (g) – 0.48 adjusted for single lung ventilation. 33
Mechanical volume-controlled ventilation (VentElite, Harvard Apparatus Inc., Holliston, MA) commenced after 20 min of perfusion using a tidal volume of 6 mL/kg, a positive end expiratory pressure of 5 cm H2O, and a respiratory rate of 10 breaths per minute. Calculations were adjusted for single lung experiments. 34
Liquid ventilation protocol
A custom LV system was designed, which consisted of two separate closed circuits: one for vascular perfusion and one for LV (Fig. 2B). The vascular perfusion circuit provided a constant positive pressure arterial flowrate with passive venous outflow with the addition of a membrane oxygenator (Fig. 2B (G), Harvard Apparatus Inc.), which oxygenated the arterial inflow fluid. The LV circuit enabled a pressure-regulated mechanical LV with inspiratory and expiratory one-way valves (Fig. 2B (C)) to minimize dead space ventilation. The inspiratory flow was calibrated to a target peak positive inspiratory pressure of 6 mmHg and the expiratory flow pump was set to a target end expiratory pressure of 3 mmHg. Respirations under LV were dependent on lung compliance and size with the automated respiratory cycle gain adjusted to achieve one to two breaths per minute.
The perfusate was a Dulbecco's modified Eagle's medium (Gibco, Thermo Fisher, Waltham, MA)-based electrolyte solution, and PBS (Life Technologies Corporation) was used as the liquid ventilant. The liquid ventilant was chosen based on prior experimentation (data not shown) in an effort to minimize harm to the alveolar cells and provide an isotonic solution that would not disrupt or injure the cell wall.
The lung was connected to the organ chamber by arterial and tracheal cannulas and recruited with the liquid ventilant before perfusion (Fig. 2B). The arterial perfusion was gradually increased over the first hour to a target, weight-based flowrate. 33 LV was initiated with the described pressure control goals. LV was performed in a 37°C incubator for normothermic conditions.
After 4 h of LV, the lung passively drained the liquid ventilant by opening the tracheal cannula and placing below the level of the lung, surfactant was instilled (2.5 mg/kg body weight adjusted for single lung experiments, CUROSURF, Chiesi Pharmaceuticals, Cary, NC) to replace the native surfactant, which was diluted during the LV process, and the lung was transferred to an EVLP circuit for assessment as previously described.
Physiological assessment during EVLP
Every 2 h during the EVLP assessment period, data were collected to calculate the pulmonary dynamic compliance (Cdyn) and the PVR.
Perfusate solution lactate concentration, pH, and oxygen content were measured using an i-STAT point-of-care analyzer (Abbott, Chicago, IL) with CG4+ cartridges (Abbott). Glucose levels were analyzed with a GlucCell® monitoring system (Chemglass Life Science, Vineland, NJ). Perfusate samples were taken every 2 h during the EVLP assessment period.
The wet-to-dry ratio (W/D ratio) assessed pulmonary edema and fluid clearance in three lungs per group. The parenchymal tissue of the left lung was weighed immediately after EVLP to determine the wet weight, then lyophilized and weighed to determine the dry tissue weight.
Bronchoalveolar lavage cytokine analysis
A bronchoalveolar lavage (BAL) sample was collected at the conclusion of EVLP by instilling 2.0 mL PBS through the trachea and aspirating 1.0 mL for cytokine analysis. Three lungs in each group underwent BAL sampling and cytokine analysis. Levels of IL-1a, IL-6, TNF-alpha, MCP-1, and IFN-gamma were measured using a magnetic bead-based Luminex Multiplex Cytokine Kit (Millipore, Billerica, MA) as per manufacturer's instruction. Briefly, BAL fluid was incubated overnight at 4°C with magnetic beads coated with antibodies for the above cytokines. A biotinylated detection antibody was added and incubated for 1 h at room temperature followed by Streptavidin–Phycoerythrin for 30 min. Samples were washed then analyzed using Luminex MAGPIX (Millipore) and xPONENT software (Luminex, Austin, TX).
Histology and immunohistochemistry
After the EVLP assessment period, three lungs in each group were perfusion fixed in a 4% paraformaldehyde solution for 24 h. Tissue was paraffin embedded, sectioned, and mounted on glass slides for immunofluorescent staining. Antigen retrieval was performed with a sodium citrate solution at high temperature and pressure. Sections were then blocked with 5% donkey serum (DS; Sigma, St. Louis, MO). Primary antibodies were incubated overnight at 4°C in a tris-buffered saline (TBS) with 0.5% DS solution then washed with TBS with 0.025% Triton (1:1000, F4/80, Thermo Fisher; 1:1000, vascular endothelial cadherin [VECAD], Invitrogen, Carlsbad, CA; 1:150, zonula occludens-1 [ZO-1], Invitrogen; 1:200, epithelial cadherin [ECAD], Novus Biologicals).
Secondary antibodies were incubated for 1 h at room temperature then washed with TBS (1:1000 Alexa Fluor 647, ab150064 or ab150075, Invitrogen). For staining of apoptotic cells, a TUNEL (terminal deoxynucleotidyl transferase (TdT)-mediated dUTP nick-end labeling) assay was used (Promega Corporation, Madison, WI). Slides were mounted with 4′,6-diamidino-2-phenylindole (DAPI) Fluoromount-G (Fisher Scientific, Waltham, MA). Images were captured using a Nikon Ti-PFS inverted microscope (Nikon, Tokyo, Japan).
All fluorescent images for a given protein were captured with consistent exposure time and instrument gain. Images were analyzed using ImageJ software (National Institutes of Health, Bethesda, MD). Cell counts were obtained by isolating the DAPI color channel, subtracting the background signal, converting the image to a binary image, and counting discrete nuclei. Mean fluorescence intensity was obtained by isolating the appropriate secondary antibody fluorescent channel, analyzing each image from a particular protein staining with consistent brightness and contrast, then calculating the mean fluorescence. Quantitative data were generated as a mean fluorescence per cell for each slide. Three images were analyzed for each experiment, totaling nine data points per group.
Statistical analysis
Data are presented as the mean ± standard error of the mean. Comparison of continuous variables was performed using an analysis of variance test with multiple subsequent t-tests with unequal variance when applicable. Statistical significance was defined as p < 0.05.
Results
Physiological performance during EVLP assessment
After 6 h of EVLP assessment, all ischemic lung groups had a significantly lower dynamic compliance compared with the control group (p < 0.05 for all; Fig. 3A). When comparing the experimental groups, the LV group showed a nonstatistically significant difference toward a higher dynamic compliance than the warm ischemia group (p = 0.17; Fig. 3A). Similarly, after 6 h of EVLP assessment, all experimental groups had a significantly higher PVR compared with the control group (p < 0.05 for all; Fig. 3B). When comparing the experimental groups, both the LV group and LV-Clodronate group had a trend toward lower overall PVR compared with the warm ischemia group, although this trend did not reach significance (p = 0.11 and p = 0.14, respectively; Fig. 3B).
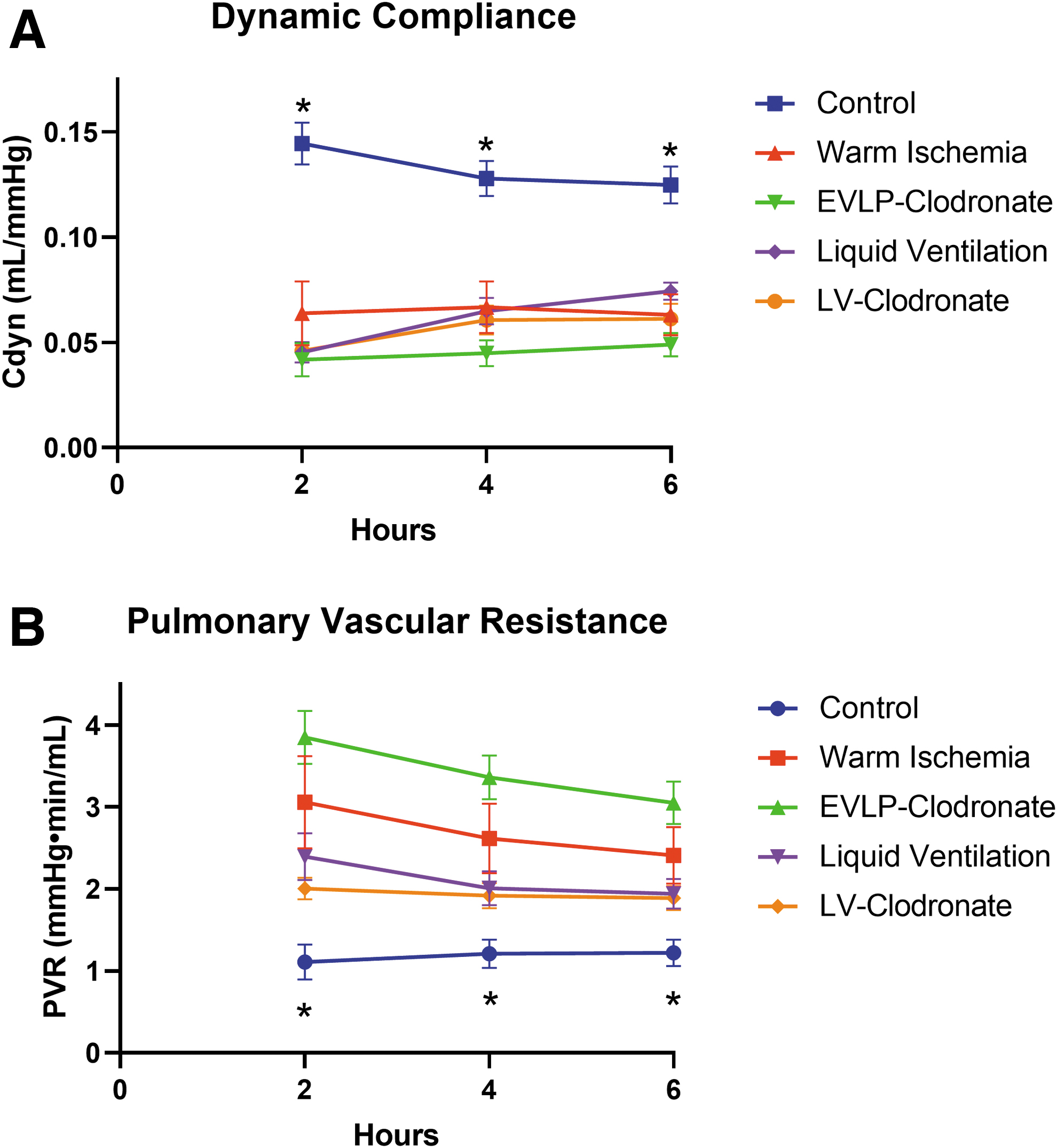
Physiological trends during EVLP assessment period (n = 6 for all time points).
A notable finding in the temporal trends of our physiological parameters was the ability of both LV groups to significantly increase the dynamic compliance over the course of the EVLP assessment period (p < 0.05 for both; Fig. 3A). This demonstrated continued physiological improvement over the 6-h EVLP assessment period not observed in the other experimental groups or the control lungs. An additional trend of decreasing PVR during EVLP was observed in the LV group, although this did not reach significance.
When the W/D ratio was calculated as a measure of pulmonary edema and barrier function, a trend toward a lower W/D ratio was observed in both LV groups compared with the other experimental groups, although this did not reach significance (p = 0.16 and p = 0.33, respectively; Fig. 4A). The control lungs had the least observed pulmonary edema with the lowest W/D ratio.
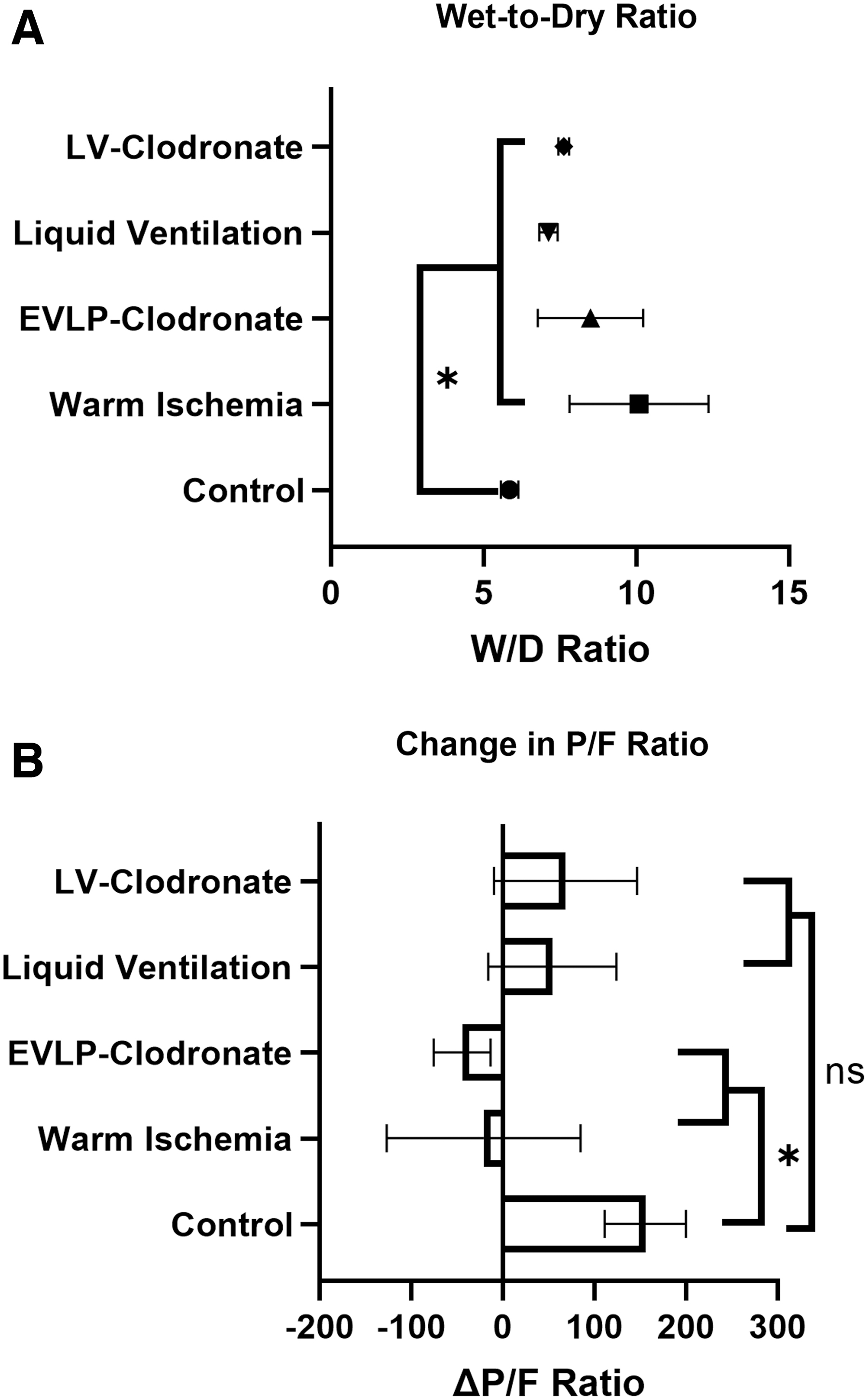
Assessment of pulmonary edema through wet-to-dry (W/D) ratio and oxygenation through ratio of partial pressure of oxygen in perfusate to fraction of inspired oxygen (P/F ratio) after the EVLP assessment period (n = 3 for all groups).
The change in the ratio of the partial pressure of oxygen in the perfusate to the fraction of inspired oxygen (P/F ratio) was calculated over the course of the 6-h EVLP assessment period. There was a significant improvement in the P/F ratio for the control group and the LV groups, while a decrease in the P/F ratio was seen in the ischemic EVLP groups. The change in the P/F ratio for the control group was significantly higher than the ischemic EVLP groups (p < 0.05), but was notably not significantly different than the LV groups demonstrating improved oxygenation in the LV groups (Fig. 4B).
Metabolic parameters during EVLP assessment
The pH of the perfusion solution decreased over the EVLP period in each study group. There was no significant difference in the magnitude of pH decrease over the EVLP period between any group. It is notable that both LV groups had a significantly higher pH in the perfusate than the other groups at multiple time points (p < 0.05; Fig. 5A). This is likely due to the use of a buffered solution as the liquid ventilant in these groups.
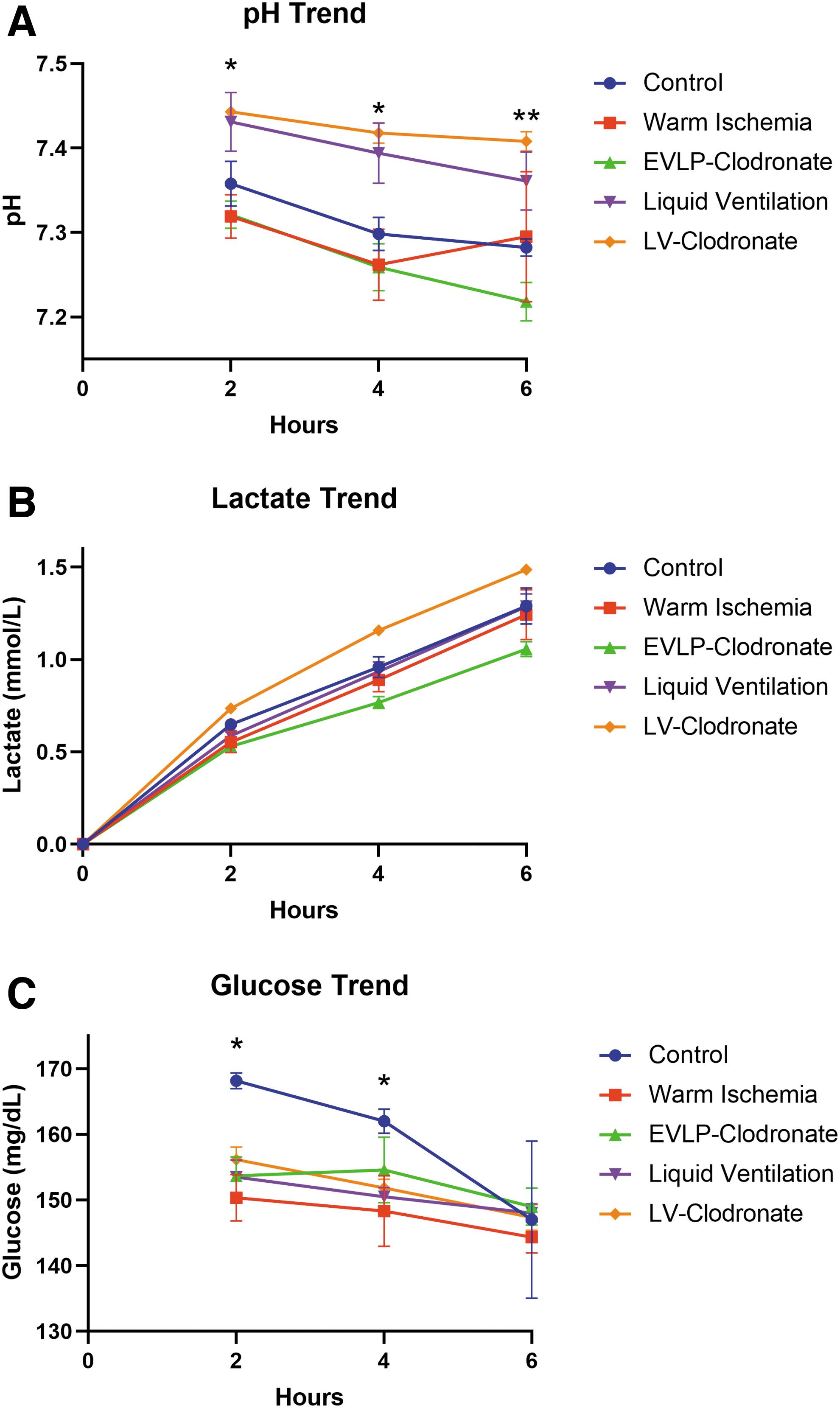
Pulmonary metabolic trends through perfusate assessment (n = 6 for all time points).
Lactate concentration in the perfusate increased significantly during EVLP in all groups (p < 0.05 for all; Fig. 5B). There was no observed correlation between the perfusate lactate concentration at the end of the EVLP assessment period and the physiological performance of the lung.
Total glucose consumption over the EVLP assessment period was similar between all groups (Fig. 5C). The only notable trend was that the control group consumed less glucose than the other groups at the 2- and 4-h time points (p < 0.05; Fig. 5C).
Cytokine markers of ischemia-mediated inflammation
IL-6, INF-γ, TNF-α, IL-1a, and MCP-1 were all quantitatively analyzed from BAL samples between groups as markers of ischemia reperfusion-mediated inflammation. All experimental groups had a significantly higher concentration of both IL-6 and TNF-α in their BAL samples compared with the control (p < 0.05; Fig. 6A, B). A trend toward lower concentrations of TNF-α was noted in the LV group compared with the other experimental groups, although this did not reach significance (Fig. 6B).
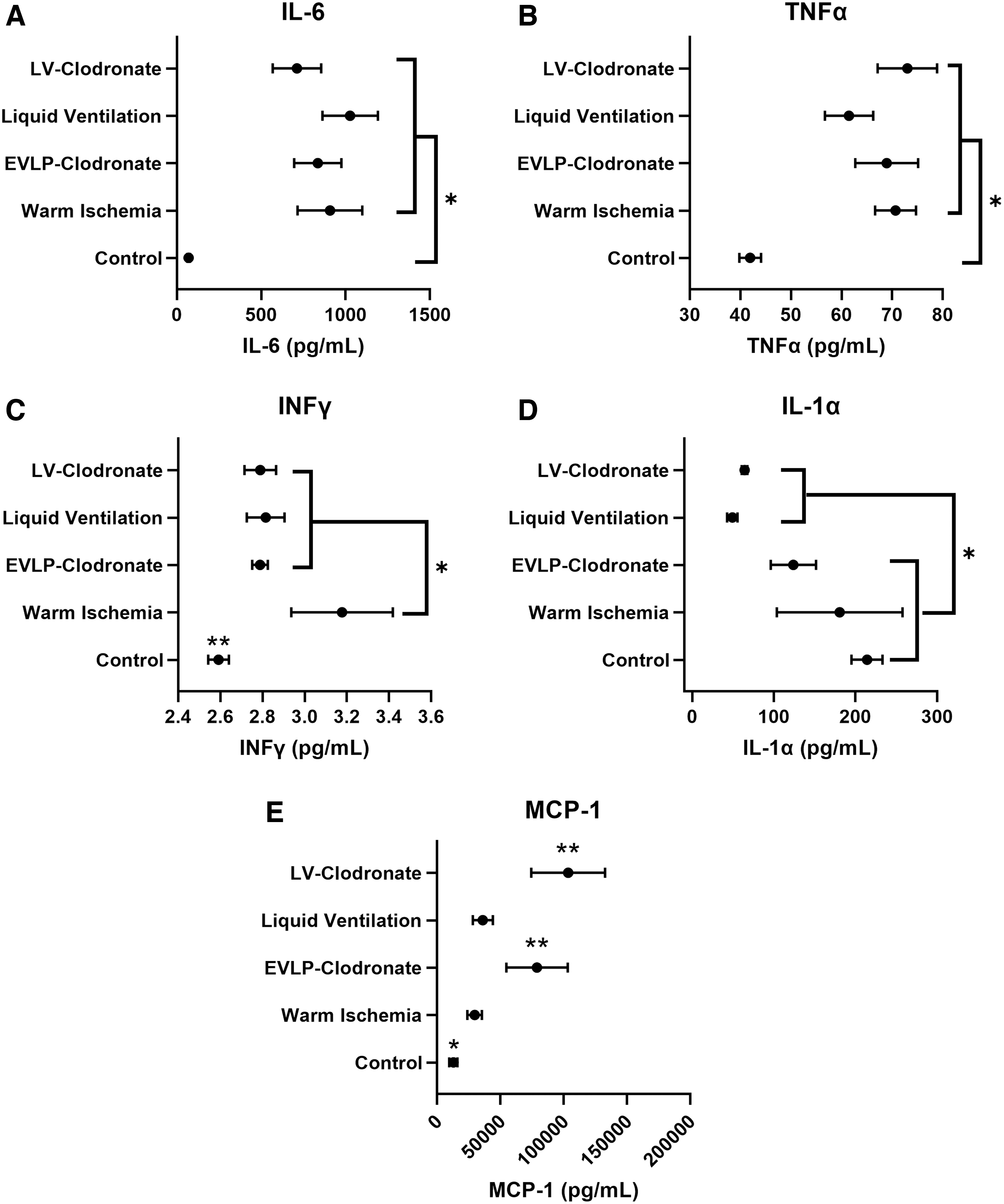
BAL fluid cytokine concentrations (presented data generated from triplicate samples from three independent experiments).
When analyzing INF-γ concentrations in BAL samples, both LV groups and the EVLP-Clodronate group had a significantly lower INF-γ concentration than the warm ischemia group (p < 0.05; Fig. 6C). As expected, the control group had a significantly lower INF-γ concentration compared with the experimental groups (p < 0.05, Fig. 6C). We also observed a significant reduction in IL-1a concentration in BAL fluid from lungs that underwent LV compared with all other groups (p < 0.05; Fig. 6D).
Lungs treated with clodronate for macrophage depletion had a significantly higher concentration of MCP-1 in BAL samples compared with the other groups. We hypothesize this is due to DAMP signaling from the injured and dying macrophages in these groups (p < 0.05; Fig. 6E). As expected, the control group had a significantly lower BAL MCP-1 concentration than the experimental groups (Fig. 6E).
Immunohistochemistry and TUNEL apoptosis assay
Semiquantitative analysis using immunohistochemistry was performed to compare relative expression of the cell junction proteins ECAD, VECAD, and ZO-1 and the activated tissue macrophage marker F4/80. The measured the mean fluorescence intensity (MFI) of ECAD, VECAD, and ZO-1 was not significantly different between all groups (Fig. 7A–C).
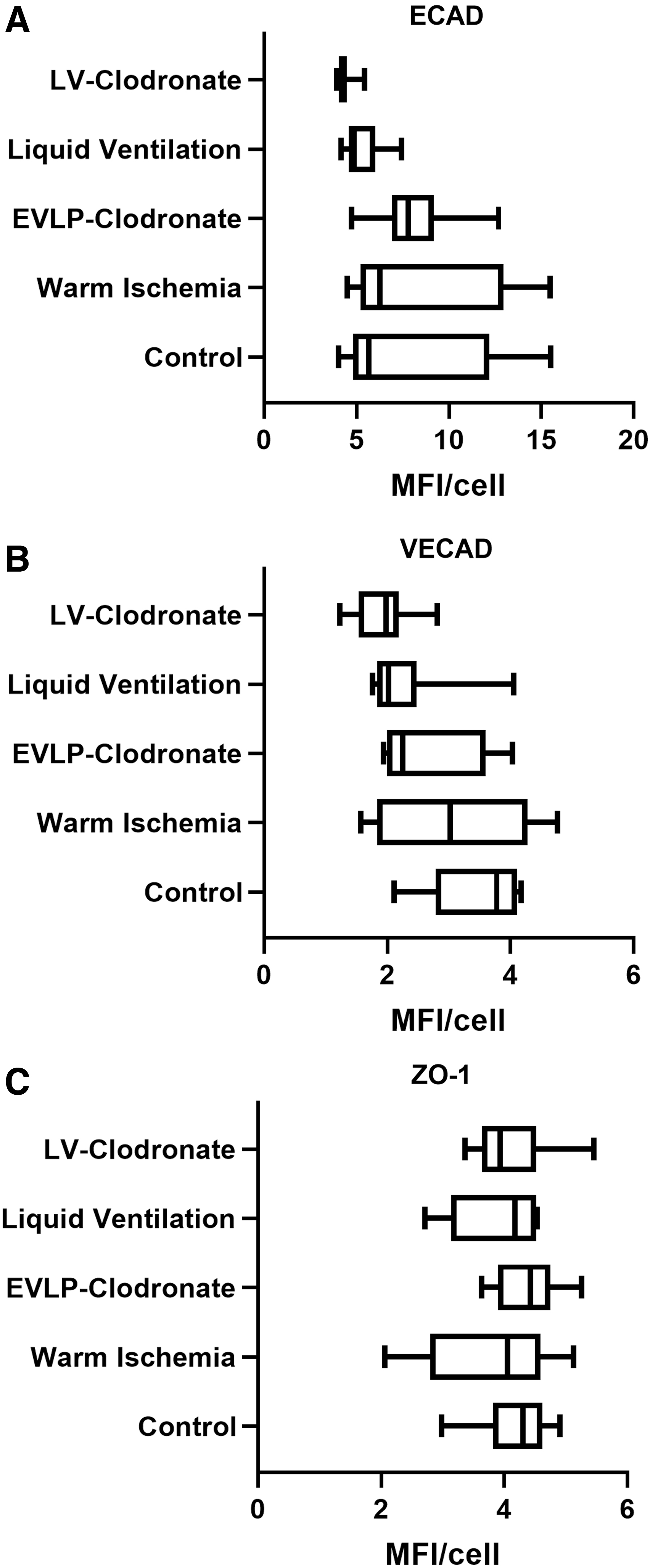
Semiquantitative assessment of cell–cell junction proteins after the EVLP assessment period (presented data generated from three images taken from each of three independent experiments).
When assessing for relative tissue quantity of the macrophage marker F4/80, the LV-alone group surprisingly had the lowest measured MFI (p < 0.05; Fig. 8A). It is important to note that the clodronate groups did not differ significantly from controls with respect to F4/80 expression.

Semiquantitative assessment of the macrophage cell surface protein F4/80 and assessment of the level of apoptosis in the lung samples after the EVLP assessment period (presented data generated from triplicate samples from three independent experiments).
A TUNEL assay was performed on tissue sections from each group, which demonstrated a significantly lower cellular apoptotic rate for the control group compared with the experimental groups (p < 0.05; Fig. 8B). There was a trend toward higher cellular apoptosis in the clodronate group, which did not reach significance.
Discussion
LV has long been a fringe concept and treatment modality in both the medical and scientific community. With the advent of ex vivo perfusion strategies for lung preservation and recovery, new and innovative approaches to treating lungs that would otherwise be discarded are needed. We describe a proof-of-concept experiment demonstrating the potential to treat lungs that have experienced extreme (4-h warm ischemia) injury with LV. Our data did not demonstrate complete recovery of significantly injured lungs to baseline function, but we did demonstrate improved pulmonary performance over a comparable lung treated with EVLP alone, which is the current standard approach for clinical lung assessment and recovery before transplantation.
The physiological improvement of the LV groups during the EVLP assessment period lend additional credence to the idea that these lungs are being rehabilitated throughout the experiment. In clinical lung transplantation, a decreased dynamic compliance in a lung allograft can lead to failure to wean from mechanical ventilation and elevated PVR can lead to right heart strain and failure in at-risk patient populations, underscoring the importance of the improvements in these parameters experimentally. Additionally, the P/F ratio has been a longstanding evaluation tool for clinical lung transplantation. Our experimental results showed that lungs rehabilitated with LV had similar P/F ratios to healthy, control lungs. Those treated with only EVLP had significantly lower P/F ratios compared with healthy lungs, further highlighting the importance of our physiological findings in the LV groups.
More notable than the physiological improvements in lung function were the mechanistic insights gained from our cytokine analysis. IL-1 is an inflammatory cytokine that is released by endothelial cells, macrophages, and lymphocytes in times of oxidative or metabolic stress, which initiates and propagates inflammatory responses. 35 This cytokine has been identified as an important mediator of pulmonary IRI. 36 INF-γ is another prominent cytokine, which is both produced by macrophages and acts as a primer of alveolar macrophages during inflammatory states. 37 Our observed decrease in INF-γ in the LV groups compared with the warm ischemia group further contributes to the decreased inflammatory response seen in these groups. The significant decrease in both IL-1a and INF-γ concentrations in the LV lungs allows us to postulate that the LV process may clear harmful cytokines from the alveolus, which may halt the propagation of the inflammatory cascade. This anti-inflammatory property of the LV process makes it a unique treatment possibility for ex vivo lung rehabilitation.
We further attempted to explore whether macrophage activation was responsible for the physiological and inflammatory changes observed in the lungs. As stated previously, the clodronate groups were intended to deplete macrophages after lung procurement to mitigate the inflammatory process during EVLP assessment. It should be noted that the clodronate groups did not show a decrease in F4/80 signal, implying that macrophages in these groups were not adequately depleted. We think the poor efficacy issue was timing. In most studies, clodronate was administered to an organism at least 24 h before experimental protocols. We do not think enough time was given for the macrophages to ingest the clodronate, undergo lysosomal processing, and subsequent apoptosis. These groups had increased concentrations of MCP-1, an inflammatory cytokine associated with antigen-presenting cell recruitment, 38 in the BAL samples. We hypothesize this finding is related to macrophages undergoing cell injury leading to DAMPs and inflammatory cytokine release.
A key mechanistic finding, which further supports the physiological improvements in the LV group, is that this group significantly had the lowest detection of the macrophage marker F4/80. A possible explanation for this is that LV may mechanically clear alveolar macrophages thus decreasing the cell type most responsible for propagating IRI in the lung. 39 This may further explain the decrease in IL-1a, a potent inflammatory mediator released by macrophages, which propagates IRI, through mechanical depletion of alveolar macrophages. This macrophage depletion and cytokine decrease was not observed in the clodronate groups, likely due to inadequate time for macrophage apoptosis after clodronate administration.
There are several limitations to our conclusions that deserve mention. The most important is whether the physical and immunological principles reported in this study will translate to large animal or human scale models. The mechanical LV process will certainly present different challenges when scaling to a large animal model with respect to increased raw material requirements, redesign of LV hardware systems, pressure gradients across multiple lobes given differential intrinsic airway resistances between lobes, and dead-space ventilation changes. There are also many noted differences between the innate immune system of a rat and a human, which have potential to alter the magnitude of our anti-inflammatory findings associated with LV. It also should be noted that the only group to receive supplemental surfactant was the LV, which could be a confounding variable regarding the etiology of the observed improvements in this experimental group.
Additionally, logistical concerns will arise if this technology were to be applied in the clinical realm, specifically defining which lungs should be trialed on LV rather than traditional EVLP. The duration of LV is another parameter that will need to be tested and optimized when translating to a large animal model is pursued. While the translation of these data to the clinical realm will certainly require significant additional research and development, the limitations of this study should not undermine the potential conceptual advances to the field of lung transplantation.
Conclusions
In this study, we report a novel method for ex vivo lung reconditioning after significant IRI with improved, clinically relevant physiological parameters using LV. These physiological improvements are the result of the mechanical clearance of alveolar macrophages and inflammatory cytokines, which blunt the release of additional inflammatory cytokines halting the propagation of IRI. While the wide applicability of these findings to large animal or human transplantation are yet to be explored, these findings represent a method for lung reconditioning from significant ischemic injury that could widen the lung organ donation pool and make a positive clinical impact on patient outcomes.
Footnotes
Acknowledgment
The authors specially thank the MGH Center for Skeletal Research Core (NIH P30 AR075042) for paraffin processing and embedding of their tissue sections.
Authors' Contributions
D.B.: Conceptualization, Methodology, Software, Formal Analysis, Investigation, Writing Original Draft, Writing Review and Editing, Visualization, and Project Administration. H.L.: Methodology, Investigation, Writing Review and Editing, Visualization, and Project Administration. S.J.: Methodology, Software, Investigation, Writing Review and Editing, and Visualization. S.R.: Software, Investigation. J.O.: Software, Resources, and Investigation. H.C.O.: Conceptualization, Methodology, Resources, Writing Review and Editing, Visualization, Supervision, and Funding Acquisition.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by research grants from the United Therapeutics Corporation.