
Abstract
Rotator cuff tears constitute a vast majority of shoulder-related injuries, occurring in a wide population range and increasing in incidence with age. Current treatments for full thickness tears use suture to secure the ruptured tendon back to its native attachment site and often retear due to improper enthesis regeneration. To reduce the occurrence of retear, our laboratory developed an engineered tendon graft for rotator cuff repair (ETG-RC) to serve as an underlayment to traditional suture repair. We hypothesize the ETG-RC will aid in the repair of the torn rotator cuff tendon by promoting the regeneration of a functional enthesis. This devitalized graft fabricated from ovine-derived bone marrow stromal cells was evaluated for biomechanical and histomorphology properties in an ovine infraspinatus rotator cuff repair model. Compared with a current standard practice Suture-Only model, the ETG-RC repair showed comparable high strain-to-failure forces, greater fibrocartilage deposition, regeneration of zonal gradients, and Shapey's fibers formation, indicative of enthesis regeneration. Enthesis regeneration after rotator cuff repair should repair mechanical properties and alleviate the need for subsequent surgeries required due to retear. The ETG-RC could potentially be used for repairing other tendon injuries throughout the body.
Impact statement
Rotator cuff tears constitute an orthopedic injury for which no ultimate surgical intervention has been found. Using tissue engineering, we demonstrate the ability for a tissue-engineered graft to restore the enthesis of a torn infraspinatus tendon promoting better healing and regeneration, progressing the technology used to repair rotator cuff tears.
Introduction
The rotator cuff comprises four primary tendons and muscles designed to hold the humerus to the scapula, creating the highly mobile shoulder joint. 1 Shoulders repeatedly perform high range of motion movements that wear the tendons and musculature, weakening the tendon–bone structure over time and contributing to an increasing prevalence of rotator cuff tears with age. 2 A study done by Minagawa et al. showed that ∼22% of male subjects 50–60 years old presented with full thickness rotator cuff tears, the majority of which were asymptomatic. 2
It has also been noted that 50% of the population over the age of 50 years has a rotator cuff tear to some extent.2,3 Often, surgery is required to resolve the symptoms of a rotator cuff tear and allow for the return to normal activities of daily living.
Typically, a patient will undergo general rehabilitation of the injured shoulder before surgical intervention with the hopes of regaining the ability to return to normal activities. 4 Surgical interventions are indicated when rehabilitation efforts are insufficient for restoring strength and reducing pain. 5 The three widely used surgical interventions are open rotator cuff repair, 5 miniopen repair, 5 and arthroscopic repair.6,7 These surgical techniques are often accompanied by various suture techniques to secure the ruptured tendon back to its native origin site.
However, these repair techniques have limited effectiveness and result in the prevalence of recurrent tears (retear) after surgery. 8 A study done by Galatz et al. observed a recurrent tear of arthroscopic rotator cuff repair in 89% of patients studied. Most of these patients had initial relief of pain and recovery of function, but experienced recurrent symptoms of a torn rotator cuff ∼2 years after the initial repair. 9 Extensive efforts are being put forth to reduce the occurrence of retears and much of this research focuses on proper enthesis regeneration.
The enthesis tissue provides the mechanical strength needed to secure tendon to bone. A typical native rotator cuff enthesis consists of a zonal fibrocartilaginous region that transitions from dense connective tissue in the tendon to uncalcified fibrocartilage, calcified fibrocartilage, and bone. The uncalcified and calcified fibrocartilage are demarcated by a characteristic basophilic line. These structures combine to provide the strength needed to withstand repeated use and heavy loading.10,11
Many emerging techniques for rotator cuff repair focus on reducing incidence of rotator cuff retear by more effectively regenerating the enthesis. Examples of extracellular matrices, 12 synthetic scaffolds, 13 biological augmentation, 14 and scaffoldless tissue constructs 15 broadly encompass possible avenues for novel tendon repair techniques. 16 Snyder et al. explain that augmentation of rotator cuff repair using biological scaffolds has been shown to improve enthesis regeneration, 17 however, these studies evaluated cadaveric biomechanical strength immediately after repair instead of using a living model and allowing time for the graft to integrate with the body before biomechanical testing.18,19
Similarly, a polylactic acid scaffold, evaluated in a study done by Koh et al., has been shown to increase immediate repair strength, but a longitudinal study evaluating the long-term efficacy of repair has not been performed. 20 A biphasic scaffold, comprising poly lactide-co-glycolide (PLGA) and PLGA-hydroxyapatite, has also been designed for rotator cuff repair and shows great promise, yet studies evaluating retear reduction are required. 21 Thus, numerous technologies are being developed and optimized with aims of alleviating the burden of retear.
Previous study from our laboratory has introduced scaffoldless tissue-engineered constructs that successfully repair various injury models including anterior cruciate ligament and rotator cuff injuries.15,22 Our rotator cuff repair technology, the engineered tendon graft for rotator cuff repair (ETG-RC) graft, was evaluated in this study to further characterize its effectiveness. Initial evaluation of this technology by Novakova et al. demonstrated promising enthesis regeneration seen in graft-repaired shoulders contrary to Suture-Only repair. 15
The Novakova et al. study analyzed the tangent modulus of the repair site, providing tendon tissue level biomechanics without mechanically damaging the enthesis. This type of analysis was done to preserve enthesis structure for histological evaluation. To further characterize the biomechanical properties of the ETG-RC repair, this study measures the force required for strain to failure by applying an increasing linear load directly on the repaired infraspinatus tendon until the tendon fails. Based on our previous study, 15 and other tissue engineering technologies, 22 we hypothesize that the ETG-RC repair technique would show equivalent strain-to-failure mechanical integrity and enhanced enthesis regeneration when compared with a Suture-Only technique.
Methods
Animal use
The sheep is a suitable model because the rotator cuff tendons are similar in size to that of humans. Castrated male Wethers sheep (n = 10 sheep ordered from Oswalt Farm, weight: 45–55 kg) were determined to be healthy by physical examination by a veterinarian at the University of Michigan's Unit for Laboratory Animal Medicine (ULAM). All 10 sheep were housed in groups within approved large animal facilities for the duration of the study and randomly assigned to one of two experimental groups: ETG-RC repair (n = 5) or Suture-Only repair (n = 5). The left shoulder was designated as the experimental RC tear and repair with the unoperated contralateral right shoulder serving as control for all animals in the study.
All animals were acclimated to the ULAM husbandry facilities at the University of Michigan for at least 1 week before procedure. Sheep were given access to food and water ad libitum. All animal care and animal surgeries were performed in accordance with The Guide for the Care and Use of Laboratory Animals, 23 and the experimental protocol was approved by the University Committee for the Use and Care of Animals.
Fabrication of ETG-RC
The ETG-RC was constructed using an expanded cell source of bone marrow stromal cells harvested from the iliac crest of a single ovine donor. Cells were passaged four times and preserved in a 10% dimethyl sulfoxide cryopreservation solution in liquid nitrogen before use. To create the graft, cells were thawed and plated on 100 mm tissue culture plates fabricated with two stainless steel pins protruding from the polystyrene cell culture surface at 6 cm apart. Monolayers were fed a bone growth medium (described below) for 6 days, feeding every other day. Medium was changed to bone differentiation medium to initiate spontaneous delamination and three-dimensional (3D) formation of a singular cylindrical tendon.
Six tendon constructs were combined into a three forked configuration with the six combined constructs separating into three paired outcroppings at the midpoint of the construct (Fig. 1). Constructs were held in place using stainless steel minutien pins pierced into tissue culture plates coated in a layer of silicone elastomer—Sylgard 184 (Fisher Scientific Cat. No. 50-366-794), allowing for the constructs to be secured in the correct orientation and at a fixed length of 6 cm. Suture was also used to hold the midbelly of the construct together to ensure fusion at the construct junction.
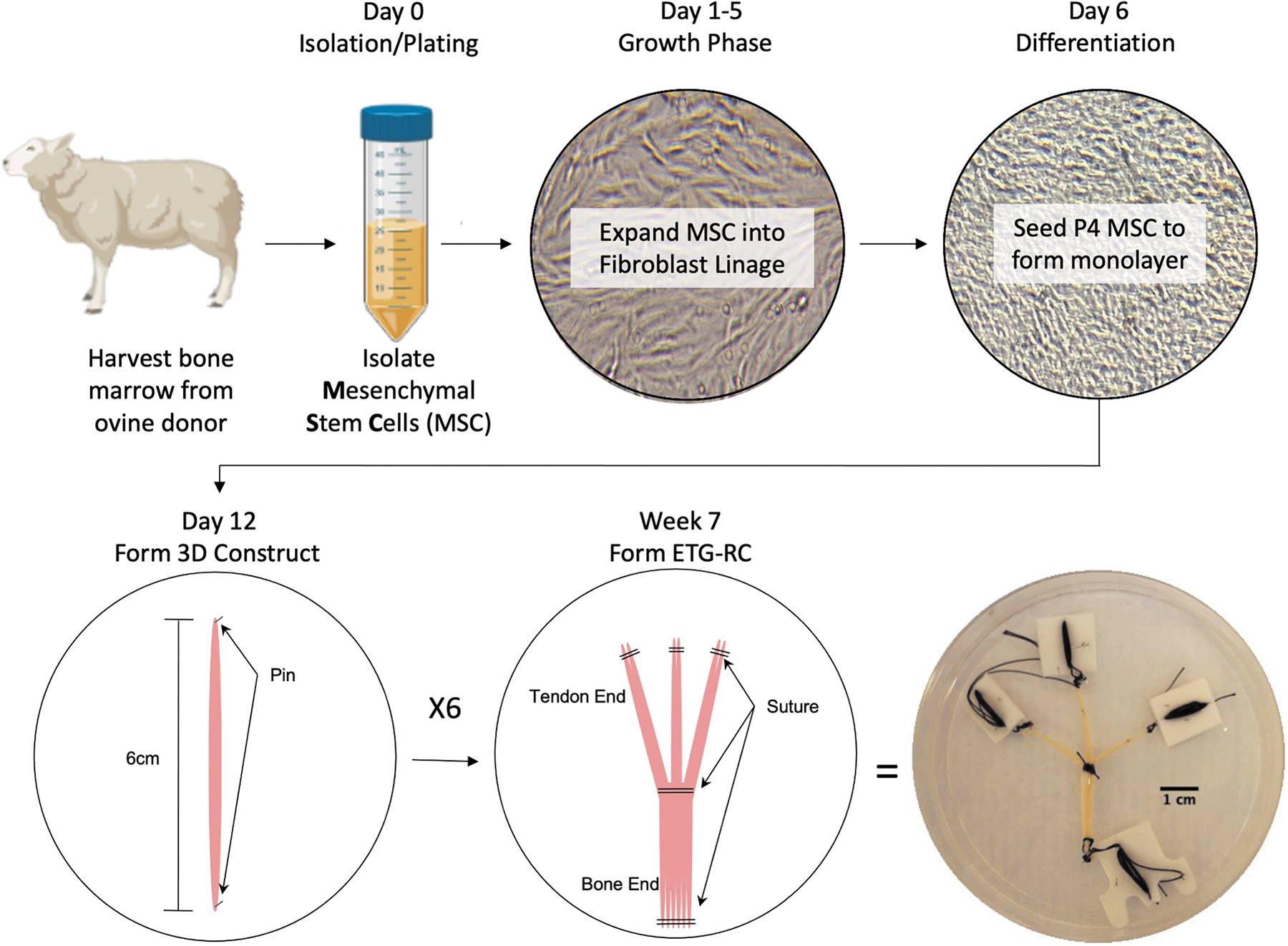
Fabrication of ETG-RC: The process of fabricating the ETG-RC involved multiple steps, starting with harvesting bone marrow from a single ovine donor and isolating MSCs from the bone marrow. The MSCs are then expanded into a fibroblast lineage and plated after four passages to create a monolayer that is differentiated down a tendon lineage. Six individual tendon grafts (6 cm in length) are made from a spontaneously delaminated monolayer. The six constructs were then combined into a conformation consisting of a thick Bone-Insertion End that is six constructs wide and three smaller prongs consisting of two constructs each (the Tendon-Insertion-Ends). The final graft is held together using suture. Constructs are ∼6 cm long and 1 mm in diameter at the prong end and 3 mm in diameter at the bone end. The bifurcation of the prongs from the Bone-Insertion End occurs at midlength or 3 cm. ETG-RC, engineered tendon graft for rotator cuff repair; MSCs, mesenchymal stem cells.
Constructs were cultured for an additional 7 weeks to fully mature. After culture, the constructs were frozen without cryopreservatives at −20°C for 48 h to devitalize the graft and stored at 4°C until implantation. Further detail regarding ETG-RC fabrication can be found in previous study. 15
Media components
Bone growth medium formulation: 78% Dulbecco's Modified Eagle Medium (DMEM) (Fisher Scientific Cat. No. 10569044), 20% fetal bovine serum (Fisher Scientific Cat. No. 10437028), 2% antibiotic–antimycotic (Fisher Scientific Cat. No. 15240062), growth factors: 10 μL/mL Fibroblast Growth Factor-b (Peprotech Cat. No. 100-18B-50UG), and 10 μL/mL dexamethasone (Millipore Sigma Cat. No. D8893-1MG). 10 μL/mL of 13 mg/mL Ascorbic acid, 5 mg/mL Proline (Millipore Sigma Cat. No. A8960-5G/81709-10G).
Bone differentiation medium formulation: 91% DMEM (Fisher Scientific Cat. No. 10569044), 7% horse serum (Fisher Scientific Cat. No. 16050122), 2% antibiotic–antimycotic (Fisher Scientific Cat. No. 15240062), growth factors: 20 μL/mL transforming growth factor-β (Peprotech Cat. No. 100-21-10UG), 10 μL/mL ascorbic acid/Proline (Millipore Sigma Cat. No. A8960-5G/81709-10G), 10 μL/mL dexamethasone (Millipore Sigma Cat. No. D8893-1MG). Media components were stored at 4°C or −20°C according to manufacturer recommendation and warmed to 37°C before use in cell culture procedures.
Rotator cuff repair surgical procedure
Twenty-four hours before surgery, fentanyl patches (75 mcg/h) were placed on chosen animals. On the day of surgery, animals were administered IM injection of Xylazine (22 mg/kg; MWI Animal Health) 15 minutes before induction for mild sedation. Blood samples were taken from each animal before being dosed with intravenous Propofol (6 mg/kg; MWI Animal Health) for induction. After induction, an endotracheal tube and rumen tube were inserted into the trachea and esophagus, respectively. Isoflurane (MWI Animal Health) was used to keep animals in a deep plane of anesthesia during surgery.
Surgical procedure began with an incision over the left shoulder exposing the fascia that was manipulated to expose the infraspinatus muscle. The muscle was then followed to the insertion point into the humerus, locating the desired tendon. The infraspinatus was cut from the humeral head at the enthesis simulating a full thickness rotator cuff tear at the enthesis. For both the ETG-RC and the Suture-Only repair, four holes were drilled in the humeral head using a Steinmann pin to keep accurate orientation while drilling. For all drilling procedures, an orthopedic drill (Stryker, Kalamazoo, MI) was used with a #5 or #6 sized drill bit.
After the four holes were drilled, suture anchors were inserted into the holes and secured in the bone. The suture was passed through the resected tendon and tied in a crossed pattern, securing the ruptured tendon back to the enthesis surface. For the ETG-RC repair, after placement of the suture anchors, two holes were drilled perpendicular to each other on the superior and lateral aspects of humeral head such that the tunnels intersected in the interior of the humerus. The bone-end of the ETG-RC construct was introduced through the superior tunnel and into the lateral tunnel and sutured to the periosteum on the lateral aspect of the humeral head.
Three small (2 mm) slits were then made in the tendon to accommodate the three tendon-end prongs of the ETG-RC, which were passed from the inferior tendon surface and sutured to the superior surface using 4-0 PDS suture (Ethicon). The tendon was then sutured using the suture anchors as described for the Suture-Only method to provide mechanical support. The ETG-RCs were implanted as an underlay that was interposed between the infraspinatus tendon and bone in combination with the double-row suture technique.
After both repair procedures, the muscle, fascia, and skin were closed with suture. Skin was closed with staples and coated using Alushield (Producer's Pride). Cefazolin was administered as a general antibiotic (MWI Animal Health). Animals were then removed from isoflurane and administered 100% oxygen for a short period of time. Recovery was monitored by laboratory staff until animal was fully self-ambulatory. Animals were then transferred to a pen to fully recover.
Explant of rotator cuff repair site
Animals were housed for 6 months after the initial surgical procedure to allow for adequate time for healing and tissue regeneration, based on previous studies.15,24–26 After the 6-month recovery time, blood was first drawn from each animal. Animals were then euthanized according to institutional animal care and use committee protocols using sodium pentobarbital (195 mg/kg; MWI Animal Health) and a bilateral pneumothorax. Explanation began by making an incision to the ventral aspect of the shoulder joint between the thorax and humerus.
This incision was carried around the circumference of the shoulder and the skin was reflected to reveal the shoulder musculature. All muscles attached to the scapula were severed allowing the scapula to be removed from the animal. Then, all muscles except the infraspinatus were severed and removed from the humerus and scapula. The elbow joint was dislocated, and the distal portion of the arm was removed. The infraspinatus muscle was separated from the scapula and musculature was scraped off the tendon using a scalpel blade.
The humerus with infraspinatus tendon was then cleaned, wrapped in plastic, and transferred to a mechanical testing facility on ice. Testing commenced on the same day as explant procedures on all except for two samples. Two samples required freezing at −20°C to preserve the tissue; biomechanical properties of these samples were not significantly different from other tests in respective groups.
Mechanical tensile testing
Before mechanical testing, all remnants of muscle belly were scraped off the intramuscular tendon with a double-ended microspatula. Soft tissue was removed from the lateral tuberosity with a scalpel blade to increase fixture-to-bone contact. The cross-sectional area (CSA) of each specimen was assumed to be rectangular, and its average dimensions were measured with a caliper within 10 mm of the tendon midsubstance distal from the humeral attachment. The mechanical testing device consisted of two main assemblies (Fig. 2): the humerus fixture (bottom) and the tendon gripper (top). Both assemblies were mounted onto the hydraulic tensile testing machine (MTS 810, 50 kN load cell, 10 kN calibrated signal conditioner) and roughly aligned with the main loading axis before each test.
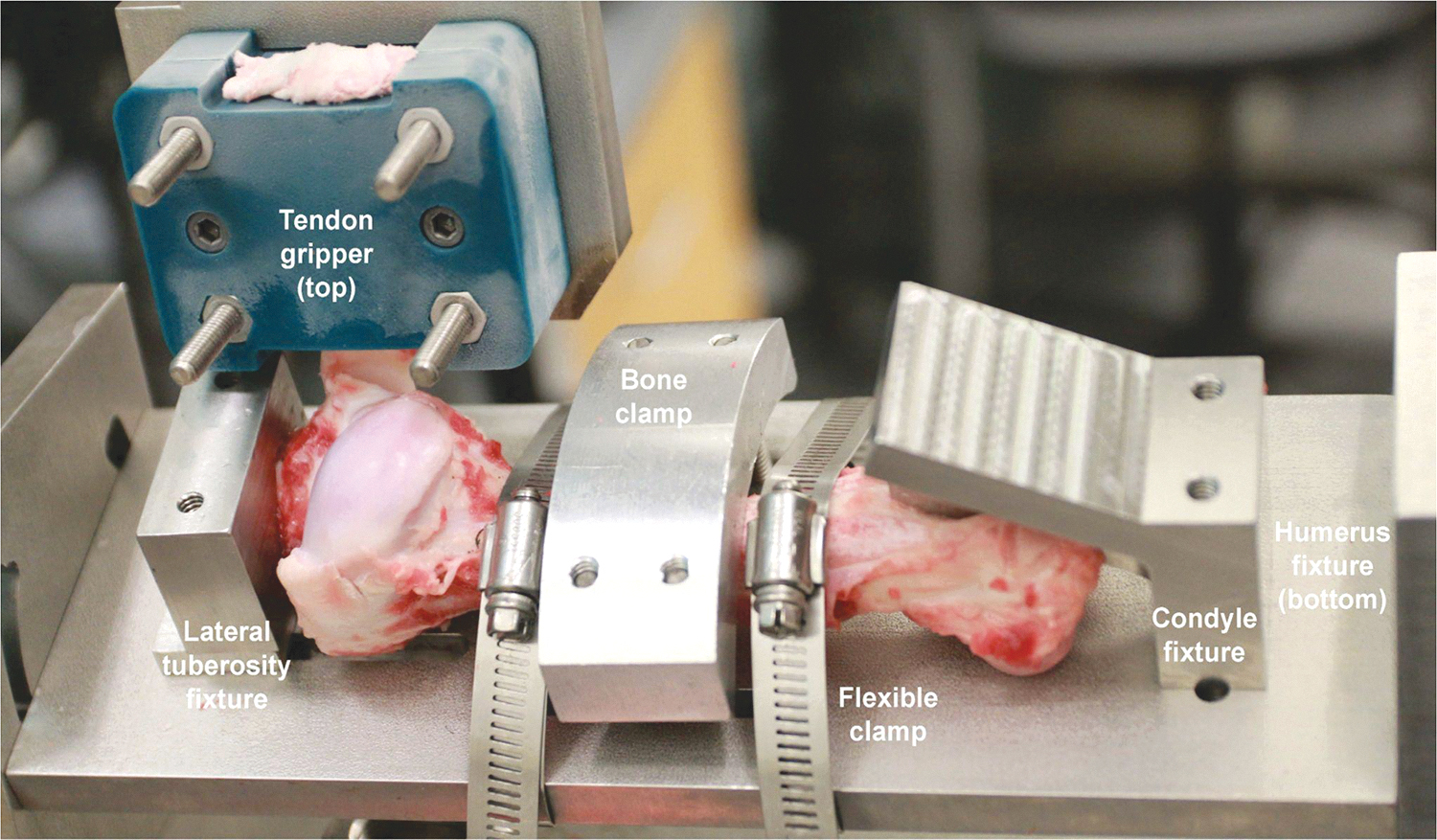
Biomechanical testing apparatus: Fixtures and clamps used in the mounting system for testing the maximum breaking load of the infraspinatus tendon. When the test is performed, the tendon gripper will move vertically away from the plate to which the humerus is clamped. The tendon gripper is connected to a load transducer (MTS 810) that relays data to a computer for recording load and displacement (LabView [2009, National Instruments]).
Each humerus was secured to the bottom assembly by the condyles and lateral tuberosity. The midshaft of the humerus was fixed with two flexible clamps. Once the humerus was in place, the bottom assembly was rotated and translated to align the long axis of the tendon with the main axis of the hydraulic machine. Then, the intramuscular tendon was tightly clamped between two 3D printed pyramidal teeth grippers and secured to the top assembly, leaving a preset grip-to-grip distance of 58 mm. To avoid tendon slippage from the gripper, the 3D printed clamp–tendon assembly was submerged into liquid nitrogen for 40 s before securely clamping the tendon tissue.
A strain to failure test was performed at a speed of 10 mm/s, which had been shown to produce rupture at the enthesis from preliminary testing. Mechanical testing parameters were controlled through a custom developed LabView (2009, National Instruments) interface. Time, load, and displacement for the entire test were automatically recorded with this program. Since our primary goal was to evaluate failure loads, there was not a strong motivation for preconditioning, which typically reduces scatter between stress–strain curves. Cryogenic gripping was used, and preconditioning time presented a risk to the efficacy of this transitory gripping mechanism.
We possess no evidence that the extra risk involved with preconditioning would have improved the results and instead may have increased the chances of obtaining inaccurate data due to tendon slippage within the grips. Samples were unmounted after the test and pictures were taken to document the failure location. Stress–strain curves were generated from load–displacement data, the average CSA, and the grip-to-grip length.
Histological and gross anatomical analyses
During the explantation of each shoulder, images were taken of the control and repair shoulders to compare anatomical characteristics such as scar tissue formation, adipose tissue deposition, and any abnormalities noted. Further images were taken before and after biomechanical testing to evaluate the nature of failure during the strain-to-failure test (to determine whether the tissue failed at the enthesis or broke the humerus bone). After testing, the diaphysis of the humerus was cut from the humeral head using a diamond band saw.
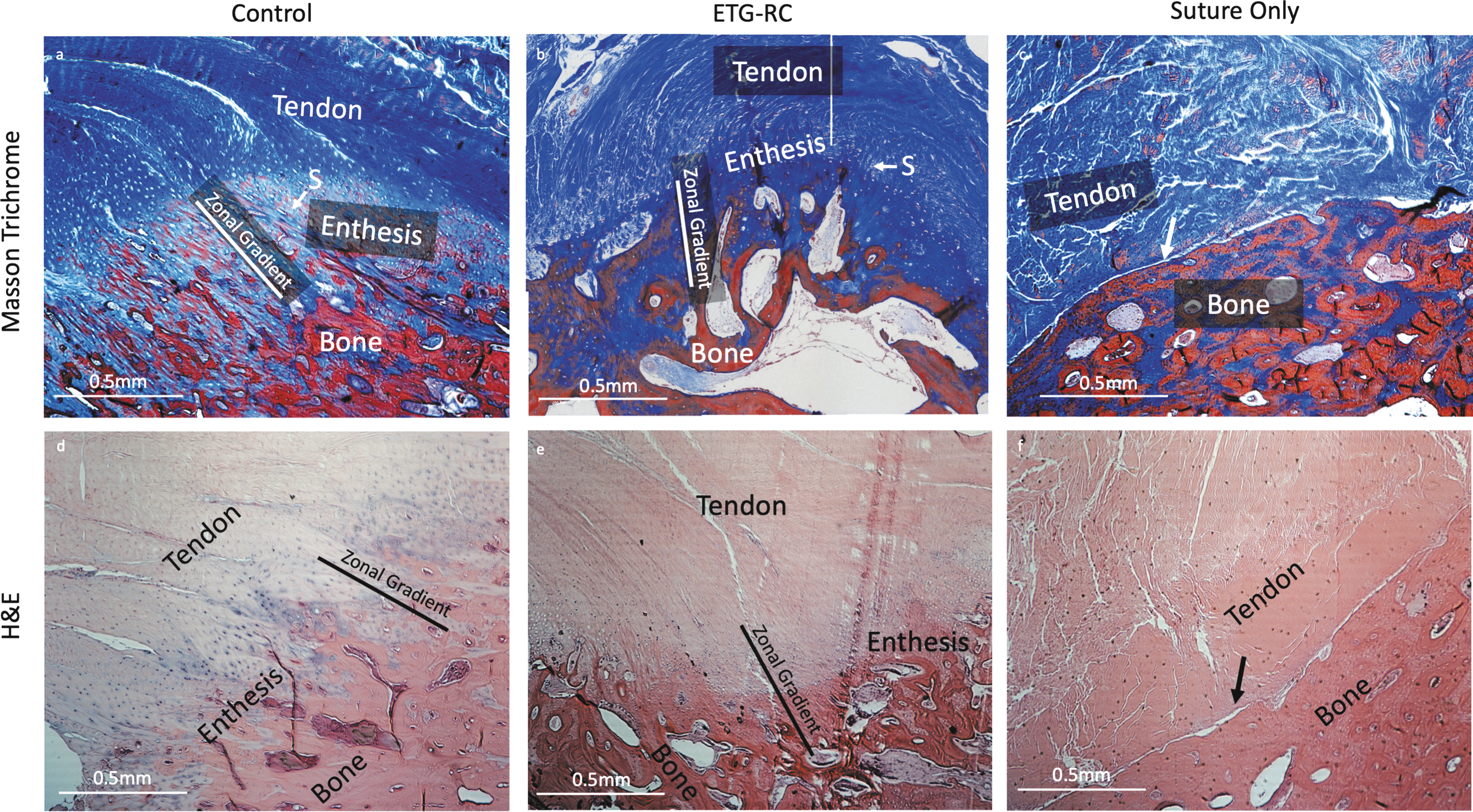
Using a manual fine-toothed hand saw, the humeral head was further dissected into multiple sections along the axis of humeral long bone extension, exposing cross sections of the enthesis. The segmented bone was then placed in 10% buffered formalin for 48 h for fixation. Samples were washed and placed in a formic acid/sodium citrate decalcification solution. After decalcification, the samples were embedded in paraffin, sectioned, and stained with hematoxylin and eosin (H&E), Safranin-O, Picrosirus Red, and Masson Trichrome.
All sectioning and staining protocols were performed by professional histologists at the University of Michigan Orthopedic Research Laboratories Histology Core, blind to the experimental groups. The H&E and Masson Trichrome stains were used to visualize general enthesis morphology and collagen and bone deposition, respectively. Safranin-O staining was used to visualize and quantify fibrocartilage formation through analyzing the percentage of positively stained area (percent red) compared with total enthesis area.
In addition, Picrosirus Red stain was used to quantify collagen alignment at the enthesis through polarized light imaging and analysis of mean gray-scale brightness value, indicating increased collagen alignment with higher gray-scale values (GSVs).
Statistical analysis
All statistical analyses were done using an ordinary one-way analysis of variance with Tukey's multiple comparisons test unless otherwise noted. Data collection and analysis were performed using Graphpad Prism 9 software. Results were significant if p < 0.05. Bars on graphs are mean ± standard deviation unless otherwise noted.
Experiment
Gross morphology
All animals were housed in appropriate conditions and monitored by veterinary staff for ∼6 months. During this time, one animal died due to Clostridium perfringens type D. Tissues from this animal were harvested at time of death, 5 months postsurgery. Veterinarian records indicated uneventful recovery after surgery with no previously noted clinical signs before death. For all other animals, endpoint blood samples were analyzed for complete blood count and general chemistries. All animals showed abnormally high creatine phosphokinase levels, otherwise no additional abnormalities were noted.
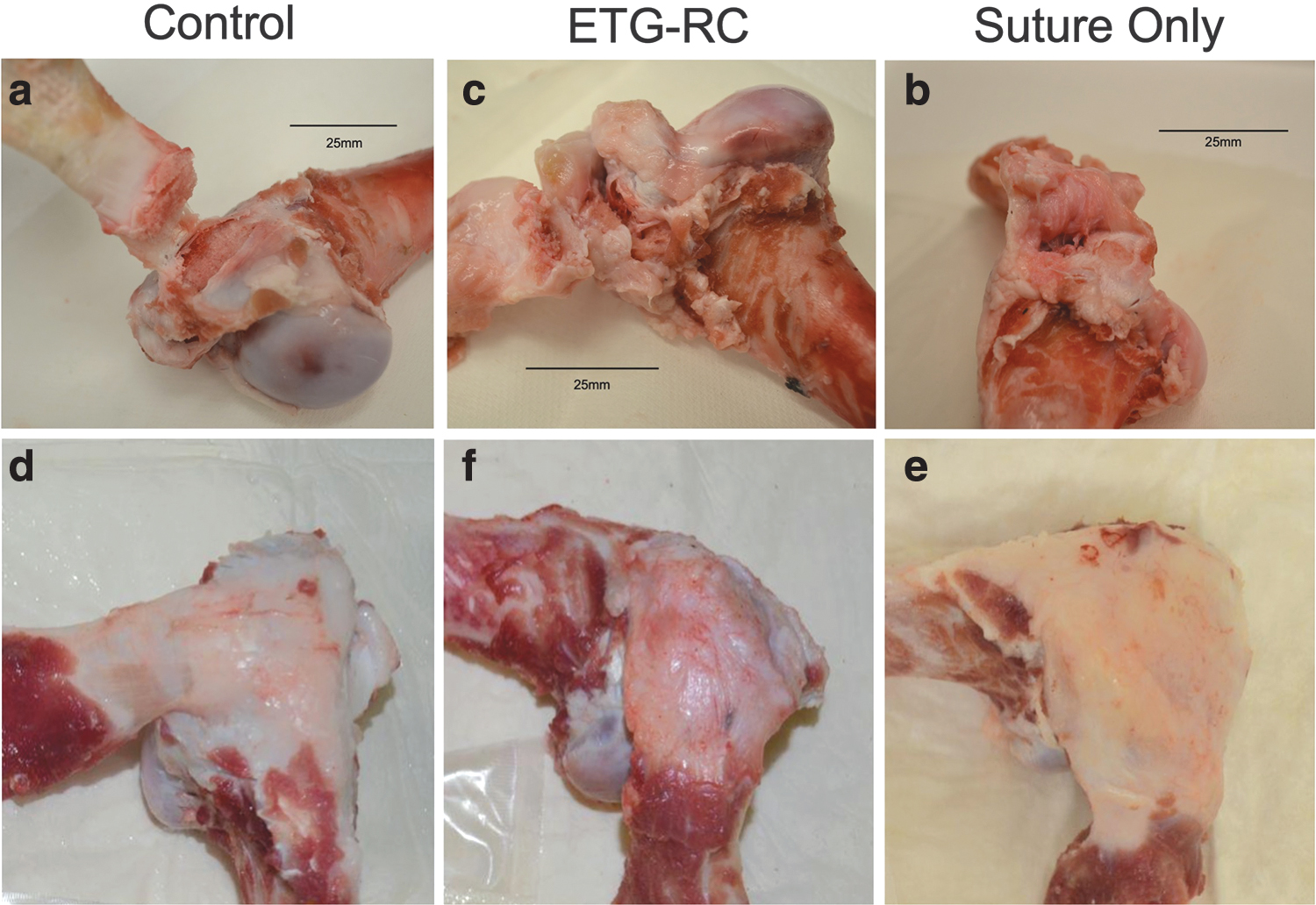
After blood draws, animals were sacrificed, and gross observation of the surgical site was conducted before explant of the limb. Two animals in the ETG-RC group presented with large bulges of connective tissue beneath the skin at the operation site and showed abnormal morphology upon inspection of the repaired tendon with large accumulations of adipose and connective tissue. All other animals presented with minimal swelling. After dissecting to expose the infraspinatus tendon, both surgical shoulders appeared to have substantially increased scar tissue accumulation compared with the control shoulders.
The ETG-RC repaired tendons appeared to have similar levels of connective tissue deposition in the repaired area when compared with the Suture-Only repair (Fig. 3d–f). Measurements of CSA were used to quantify connective tissue deposition.
Digital images of dissected tendons: Digital images were taken of the inferior
Tendon CSA
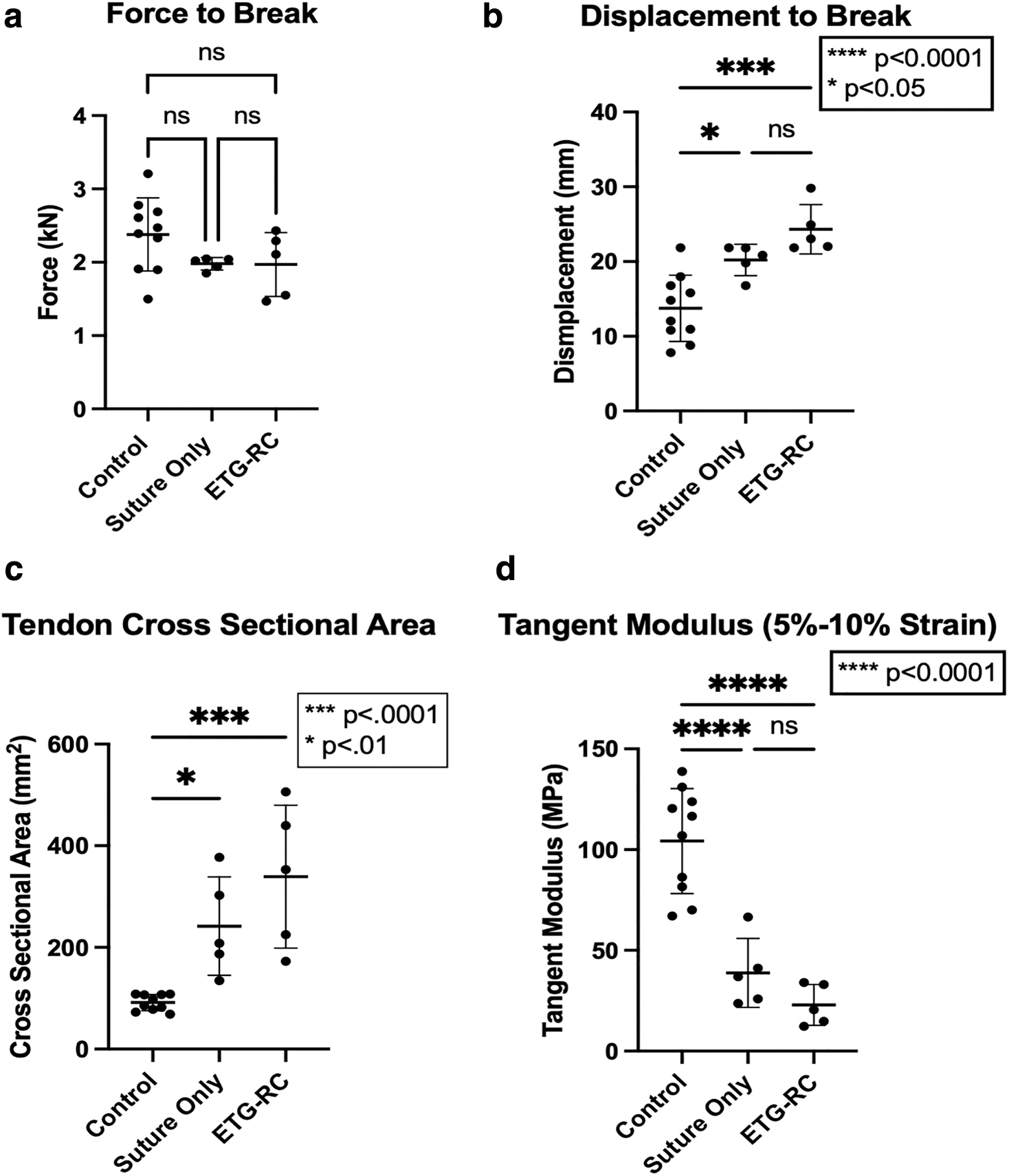
CSA of each tendon was measured after mechanical testing. control tendons showed an average CSA of 91.58 ± 15.73 mm2. The average CSA for Suture-Only tendons was 242.0 ± 96.83 mm2, and the average CSA for ETG-RC repair tendons was 339.4 ± 140.4 mm2 (Fig. 4c). Suture-Only and ETG-RC tendon CSAs were significantly different from those of control tendons (p-values: 0.0115 and 0.0001, respectively), but not significantly different from each other.
Biomechanical measurements:
Biomechanical analysis
All tendon–bone assemblies failed by tendon avulsion (enthesis detachment) or humerus fracture, without showing visible damage in the tendon grip-to-grip length. The average load to failure for the control, Suture-Only, and ETG-RC groups was 2.38 ± 0.50 kN, 1.99 ± 0.09 kN, and 1.97 ± 0.44 kN, respectively (Fig. 4a). These results were not significantly different. Displacement to failure was greater in the ETG-RC group, with an average of 24.33 ± 3.30 mm, whereas the Suture-Only group displayed an average displacement of 19.82 ± 2.10 mm. The ETG-RC and Suture-Only groups showed significantly greater displacements to failure than the control group (13.76 ± 4.43 mm, p < 0.0001); however, the two repair groups were not significantly different from each other (Fig. 4b).
The tangent modulus was calculated for each specimen from its stress–strain curve (data not shown), using data in the 5% to 10% strain range. The ETG-RC graft had the lowest tangent modulus among the three groups, with an average of 22.94 ± 10.15 MPa, being significantly lower/more compliant than the control group, with an average of 104.26 ± 26.02 MPa (Fig. 4d). Similarly, the Suture-Only group had a significantly smaller average tangent modulus of 38.86 ± 17.13 MPa as compared with the control group (Fig. 4d).
Enthesis regeneration
After biomechanical testing, samples were processed for histological analysis. Before decalcification, digital images were taken of each enthesis to compare the nature of the failure caused by biomechanical testing (Fig. 3). Control shoulders primarily failed within the matrix of the bone, separating the tubercle from the remainder of the humerus (Fig. 3a), typically rendering the samples with an intact or slightly torn entheses. This differed from Suture-Only and ETG-RC repaired shoulders where both groups of repaired tendons primarily retore at the enthesis leaving the bone mostly intact (Fig. 3b, c). Histological data may be confounded due to mechanical disruption of the enthesis during biomechanical testing, however, analysis of histology shows similarity to our previous study wherein the enthesis was not mechanically torn during the biomechanical testing. 15
Paraffin-embedded samples were sectioned and stained with H&E, Masson's Trichrome, Pircosirus Red, and Safranin-O (Figs. 5 and 6). All stains except for the Picrosirus Red were imaged with light microscopy, the Picrosirus Red stain was imaged with polarized light microscopy. Enthesis histology of control samples showed integration of tendon into bone identified by zonal gradients of tendon, fibrocartilage, and bone regions, as well as Sharpey's fibers and the increased presence of nuclei at the enthesis region identified utilizing the stains mentioned above (Figs. 5a, d, and 6f).
Histological analysis:
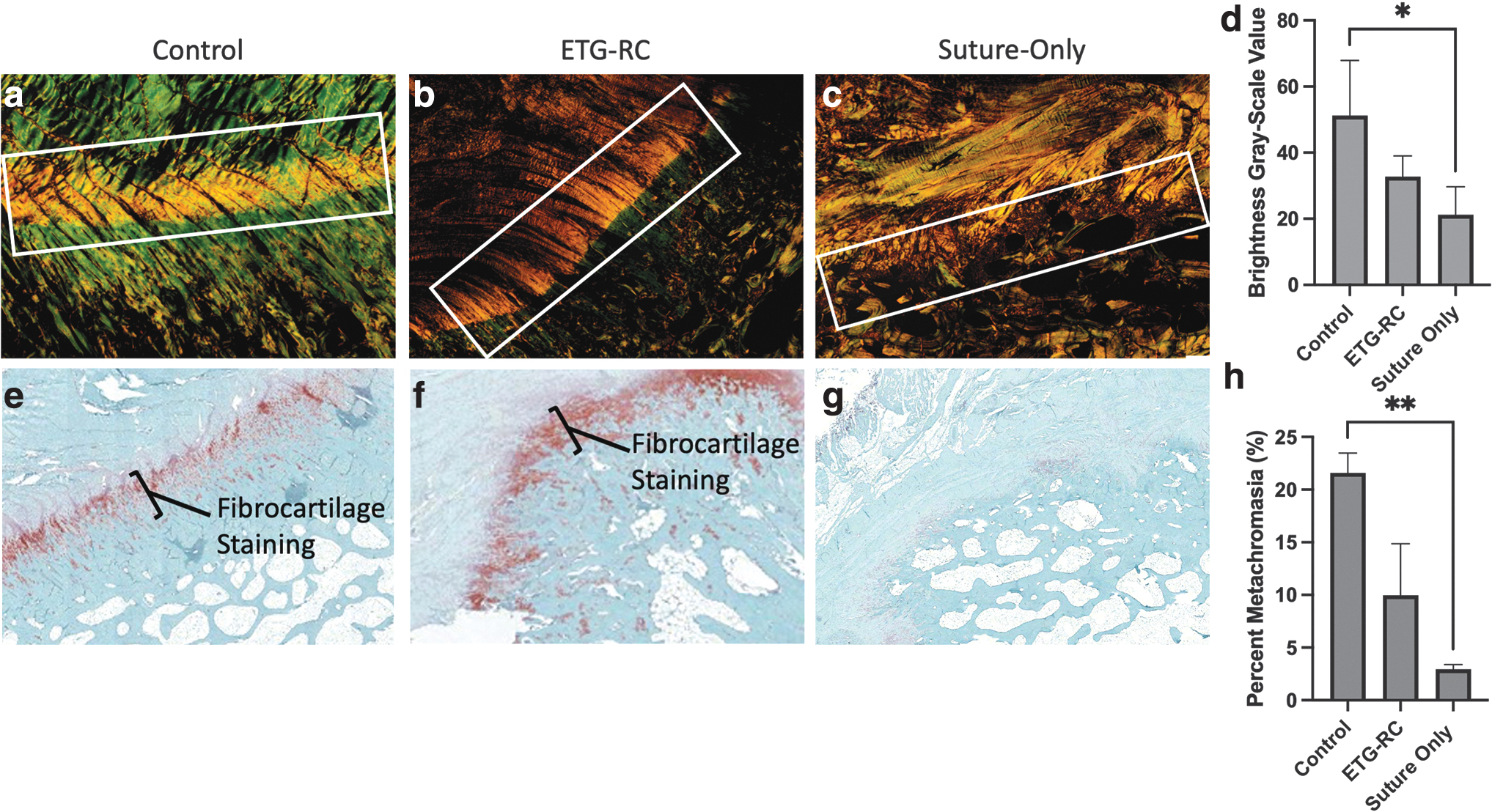
Picrosirus Red and Safranin-O analyses: Sections from ETG-RC, Suture-Only, and control groups were stained with Picrosirus Red and imaged with polarized light microscopy at 2.5 × magnification
Quantification of percent of positively stained fibrocartilage area at the enthesis, using the Safranin-O staining, indicated the highest fibrocartilage formation in control samples (21.59% ± 3.74%), followed by intermediate levels in ETG-RC (9.97% ± 9.78%) and lowest levels in Suture-Only (2.95% ± 0.87%) samples. Control samples had significantly higher percentages than Suture-Only samples (p = 0.0063) (Fig. 6h). Control entheses also showed increased collagen alignment in the enthesis demonstrated by the presence of aligned green fibers seen in Picrosirus Red-stained sections imaged using polarized light (Fig. 6a).
Picrosirus Red collagen alignment quantification, based on mean GSV brightness where greater brightness correlates with greater alignment of tissue, indicated a significantly higher brightness value in control samples (51.23 ± 16.69 GSV) than in Suture-Only samples (21.24 ± 8.46 GSV) (p = 0.014). ETG-RC (32.74 ± 6.32 GSV) samples had intermediate brightness compared with control and Suture-Only groups and were not significantly different from either (Fig. 6d). The ETG-RC group showed similar morphology to control groups in Masson's Trichrome and H&E images with some evidence of Sharpey's fibers forming, presence of zonal gradients, and a slight increase in nuclei at the enthesis (Fig. 5a–e).
As previously shown, the Suture-Only group showed a sharp demarcation separating tendon and bone tissue. 11 There was little indication of a positive enthesis generation, showing morphology dissimilar to that of control samples.
Discussion
This study evaluates the use of the ETG-RC technology designed by our laboratory for reducing the occurrence of rotator cuff retears after surgical repair. We characterized the efficacy of this tissue-engineered graft by analyzing strain-to-failure biomechanical measurements and enthesis histomorphology. The ETG-RC repair procedure was compared with a double-suture technique commonly used in rotator cuff repair cases; uninjured contralateral shoulders serve as controls. Based on published data, 15 we hypothesized that the ETG-RC technique used as an underlayment to repair rotator cuff tears would elicit similar strain-to-failure characteristics as the traditional Suture-Only technique but show superior enthesis regeneration in histomorphology analysis.
Results of this study indicate that ETG-RC repaired rotator cuffs show similar biomechanical properties and enhanced enthesis regeneration characteristics, when compared with a Suture-Only repair technique. Measuring the load required for failure allowed for the comparison of the maximum mechanical strength achievable by each tendon. Each group withstood loads over 2 kN before rupture and was not significantly different from one another. This is a nonphysiological load applied directly to a tendon–bone junction used to provide a basis of comparing mechanical properties rather than mimic native mechanics.
We did not see discernable differences in the maximum load to failure between the groups, since a regenerated enthesis would only provide a marginal increase in overall strength at such high loads. However, a regenerated enthesis would provide greater resilience to a repaired rotator cuff after repeated loading over the course of years after a repair. Interestingly, given the same load, the displacement to failure data shows that the Suture-Only repair broke sooner than the ETG-RC repair, which was able to withstand maximum loads over a 16% greater distance.
Analysis of the tangent modulus at a 5–10% stretch allowed for the evaluation of mechanical properties at loads that more closely emulated what an enthesis would typically experience in the body. The tangent modulus data and displacement to failure data showed an increase in elasticity of the ETG-RC repair compared with the Suture-Only repair. This increase in elasticity of the ETG-RC repair would be advantageous in preventing retear and assist the tendon in withstanding repeated loads over time.
We have confirmed the presence of a regenerated enthesis through histomorphology. Concurring with previous data, 15 we see evidence of native entheses regeneration characteristics in the ETG-RC group marked by zonal gradients and Sharpey's fibers, which were also seen in the previous study when histology was performed on samples that were not mechanically separated during biomechanical testing. These characteristics of enthesis regeneration were not observed in the Suture-Only group.
Our devitalized ETG-RC underlayment uniquely inserts into the native bone marrow when introduced through the bone tunnel created during surgery. Other tissue-engineering techniques are sutured to the periosteum and tendon only, providing mechanical support but not effectively integrating host cells from the bone marrow into the injury site.27–29 We have shown in previous studies that the ETG-RC grafts integrate host cells into the graft tissue when implanted within a bone tunnel. 26
The enthesis regeneration seen in the ETG-RC group in this study may be attributed to the acellularized graft promoting the migration of cells necessary for regeneration into the injury site, stimulating growth of tendonous tissue into the bone to reform the enthesis. Since most rotator cuff retears are due to degenerative processes accelerated by moderate trauma, a regenerated intact enthesis promotes superior healing capable of withstanding repeated loading and may reduce the incidence of rotator cuff retear after surgery.
In conclusion, our ETG-RC tissue-engineered graft shows evidence for the regeneration of enthesis tissue that may ultimately reduce the occurrence of recurrent rotator cuff tears. A limitation to this study is the absence of a chronic repair model, the immediate repair of the ruptured tendon is unlikely to occur clinically, and torn rotator cuffs often progressively worsen over a significant length of time before surgical intervention. Chronic repair models and in-human trials will substantially add to the growing research supporting the ETG-RC graft and other tissue-engineering approaches for rotator cuff repair.
Footnotes
Acknowledgments
The authors thank Michigan Integrative Musculoskeletal Health Center: Orthopedic Research Laboratories for assistance with histology, and University of Michigan Undergraduate Research Opportunity Program (UROP) Students: Ryan Ettner, Makayla Kelley, and Luisa Nierhoff for assistance with imaging.
Authors' Contributions
C.S.K. contributed to project administration (equal), data curation (equal), formal analysis (lead), and writing—original draft (lead). C.N.V.N. was involved in methodology (equal), data curation (equal), and writing—review and editing (equal). A.P. carried out methodology (equal), data curation (equal), and writing—review and editing (equal). E.V-.S. was in charge of methodology (equal), supervision (lead), and project administration (equal). E.M.A. took charge of conceptualization (equal) and writing—review and editing (equal). L.M.L. took charge of conceptualization (equal) and writing—review and editing (equal).
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure Statement
C.S.K., Dr. L.M.L., and Dr. E.M.A. are affiliated with Skeletal Tissue Engineering Laboratory Technologies. C.N.V.N., A.P., and E.V-.S. have no disclosures.
Funding Information
Research reported in this publication was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the Institutes of Health under Award Number P30 AR069620 and University of Michigan internal funding.