
Abstract
Although microsuture neurorrhaphy is the accepted clinical standard treatment for severed peripheral nerves, this technique requires microsurgical proficiency and still often fails to provide adequate nerve approximation for effective regeneration. Entubulation utilizing commercially available conduits may enhance the technical quality of the nerve coaptation and potentially provide a proregenerative microenvironment, but still requires precise suture placement. We developed a sutureless nerve coaptation device, Nerve Tape®, that utilizes Nitinol microhooks embedded within a porcine small intestinal submucosa backing. These tiny microhooks engage the outer epineurium of the nerve, while the backing wraps the coaptation to provide a stable, entubulated repair. In this study, we examine the impact of Nerve Tape on nerve tissue and axonal regeneration, compared with repairs performed with commercially available conduit-assisted or microsuture-only repairs. Eighteen male New Zealand white rabbits underwent a tibial nerve transection, immediately repaired with (1) Nerve Tape, (2) conduit plus anchoring sutures, or (3) four 9-0 nylon epineurial microsutures. At 16 weeks postinjury, the nerves were re-exposed to test sensory and motor nerve conduction, measure target muscle weight and girth, and perform nerve tissue histology. Nerve conduction velocities in the Nerve Tape group were significantly better than both the microsuture and conduit groups, while nerve compound action potential amplitudes in the Nerve Tape group were significantly better than the conduit group only. Gross morphology, muscle characteristics, and axon histomorphometry were not statistically different between the three repair groups. In the rabbit tibial nerve repair model, Nerve Tape offers similar regeneration efficacy compared with conduit-assisted and microsuture-only repairs, suggesting minimal impact of microhooks on nerve tissue.
Impact statement
Peripheral nerve injuries can result in permanent motor and sensory deficits when repairs fail. Proper fascicular alignment, tension management, and nerve stump mobilization are important factors determining outcomes that current repair techniques do not fully address. In this study, we introduce Nerve Tape, a sutureless nerve coaptation device that is designed to improve peripheral nerve repairs. We tested the regeneration efficacy of the Nerve Tape and showed that it provides superior nerve conduction recovery and similar axon regeneration when compared with microsutures or conduits. This study is an important step in supporting future clinical benefit of the Nerve Tape.
Introduction
More than 2
Many prognostic factors such as degree of trauma, patient age, regeneration distance, and chronicity of injury are beyond the surgeon's control. However, technical errors of the surgical repair likely contribute to poor outcomes. While inadequate debridement and overtensioning are well-recognized surgical pitfalls, poor nerve alignment is rarely cited. Topographic alignment is obtained via visual inspection of nerve stumps and precise approximation, most commonly utilizing microsuture neurorrhaphy. Microsuture placement requires specialized training and is time-consuming. However, even when controlling for these variables, two cadaveric studies found that ∼40% of microsuture nerve coaptations suffered from unacceptable fascicular malalignment.4,5 Most of the observed failures appeared to be “overtightened,” causing the inner nerve fascicles to extrude from the coaptation site, resulting in gross overapproximation. 5
Contemporary alternatives to suture repair fail to adequately address these issues or have separate distinct shortcomings. Commercially available fibrin glues combine components of the clotting cascade to create a bloodless clot that can be applied around approximated nerve ends to form a cocoon-like adhesive cylinder. Although multiple small animal studies and one recent clinical study demonstrated improved surgical efficiency and the potential for comparable or superior recovery,6–8 fibrin glue has a low tensile strength, and catastrophic repair failure is a distinct risk.9,10 Fibrin glue may only be applicable in ideal scenarios as illustrated in one recent study. Following the sharp transection of a mouse sciatic nerve, fibrin glue repairs performed by a naive microsurgeon achieved equivalent functional recovery compared with those performed by an expert microsurgeon.
However, the insertion of an isograft, despite the lack of nerve tissue loss, implied that the results were only possible if natural tension was artificially eliminated. 11
As demonstrated in a cadaveric nerve study, the addition of an entubulating conduit to standard suture neurorrhaphy appeared to splint and direct approximating fascicles. 5 The overapproximation noted in microsuture-only repairs was much less pronounced, and the technical alignment of the nerve coaptation was clearly improved even across a spectrum of surgical skill sets. 5 Entubulation of the repair site may also create a protected microenvironment allowing for the accumulation of neurotrophic factors and prevention of axonal escape.12,13 This technique, however, still requires microsurgical skills and the incorporation of microsutures, and can be time-consuming.
Nerve Tape was developed as a novel, sutureless coaptation device incorporating opposing tissue grabbing/stabilizing Nitinol microhooks embedded in a biocompatible, decellularized porcine small intestinal submucosa (SIS) extracellular matrix backing (Fig. 1). As designed, Nerve Tape offers the theoretical advantages of entubulation while avoiding the technical challenges of microsuturing. Both the Nitinol hooks and the SIS wrapping are biocompatible; the latter currently utilized clinically in nerve wraps and conduits/connectors. With multiple attachment points, the device is designed to distribute and disperse tension away from the nerve coaptation, which has been shown in experimental models to improve axon regeneration.14,15 Recent biomechanical testing of the Nerve Tape device confirmed equivalent or superior repair strength compared with clinically relevant microsuture neurorrhaphy. 16
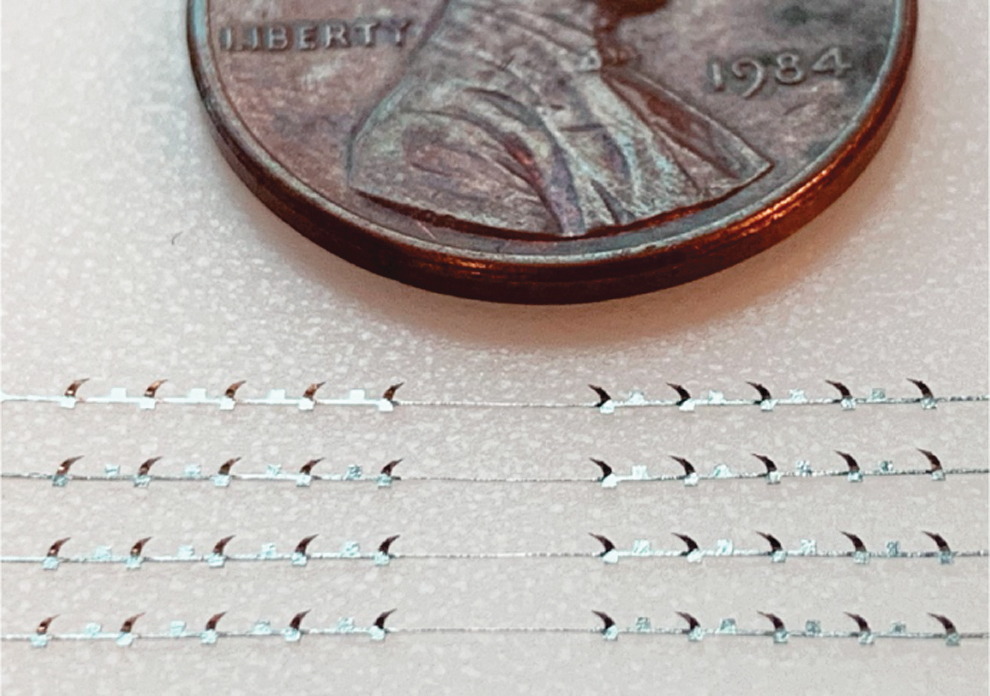
Microscale hooks are embedded within a flexible biologic backing to form Nerve Tape.
However, although the microhooks are ∼425 μm in length and designed to only penetrate the outer epineurium, the potential for iatrogenic morbidity must be considered. The present study was conducted specifically to investigate the efficacy and safety of microhooks versus microsutures when used to repair a nerve in a small-animal model. In this study, we examine the impact on nerve tissue and axonal regeneration of Nerve Tape, comparing with direct microsuture and conduit-assisted repair in a rabbit tibial nerve transection model.
Materials and Methods
A rabbit nerve transection repair study was performed to assess the impact on nerve tissue and axonal regeneration of our novel nerve repair device versus conventional repair techniques. The rabbit tibial nerve model was chosen (New Zealand white rabbits), due to rabbits' more standard neural regenerative capabilities and sensitivity to implants (vs. rats). Along with Nerve Tape and standard microsuture repair, a third treatment group utilizing a conduit-assisted repair with an SIS device was included. This group served to differentiate effects of the SIS substrate from the Nitinol microhooks. Outcome testing consisted of gross inspection (scoring of local adhesions/scarring/inflammation), reinnervated muscle morphology, immunohistochemistry, histomorphometry, and terminal electrophysiological measurements. A 16-week endpoint was chosen based on an anticipated axon regeneration rate ∼3 mm/day that would allow for up to 33 cm of regeneration. 17
Surgical procedures
Thirty male and female New Zealand white rabbits weighing between 3.2 and 4.2 kg were used for the study. Animals were anesthetized using isoflurane and endotracheal intubation for continuous delivery of isoflurane throughout the surgical procedure. The left hind limb was sterilely prepped and the sciatic nerve and branches were exposed via a muscle splitting approach. The tibial nerve was isolated and transected halfway between the spinal column and the knee and repaired with: (1) Nerve Tape (n = 10); (2) conduit (Axoguard Nerve Connector; n = 10; Axogen, Inc., Alachua, FL) plus two anchoring sutures as per the manufacturer's instructions for use; or (3) four 9-0 nylon epineurial microsutures spaced 90° apart (n = 10).
The Nerve Tape device was placed, microhook side up, on the tissue bed between transected nerve stumps. The first nerve stump was laid onto the center row of the microhook array. A slight downward pressure and backward tug was utilized to induce microhook engagement. The second stump was then placed on opposing microhooks, slightly overapproximating the first stump, and the same engagement technique was utilized. Fascicular patterns were visually matched and nerve ends were adjusted as needed to ensure proper alignment. The device was then wrapped around the opposing nerve ends to passively engage the remaining microhooks while entubulating the repair to provide precise, secure, and stable alignment (Fig. 2). The incision was then closed using 4-0 nylon sutures.
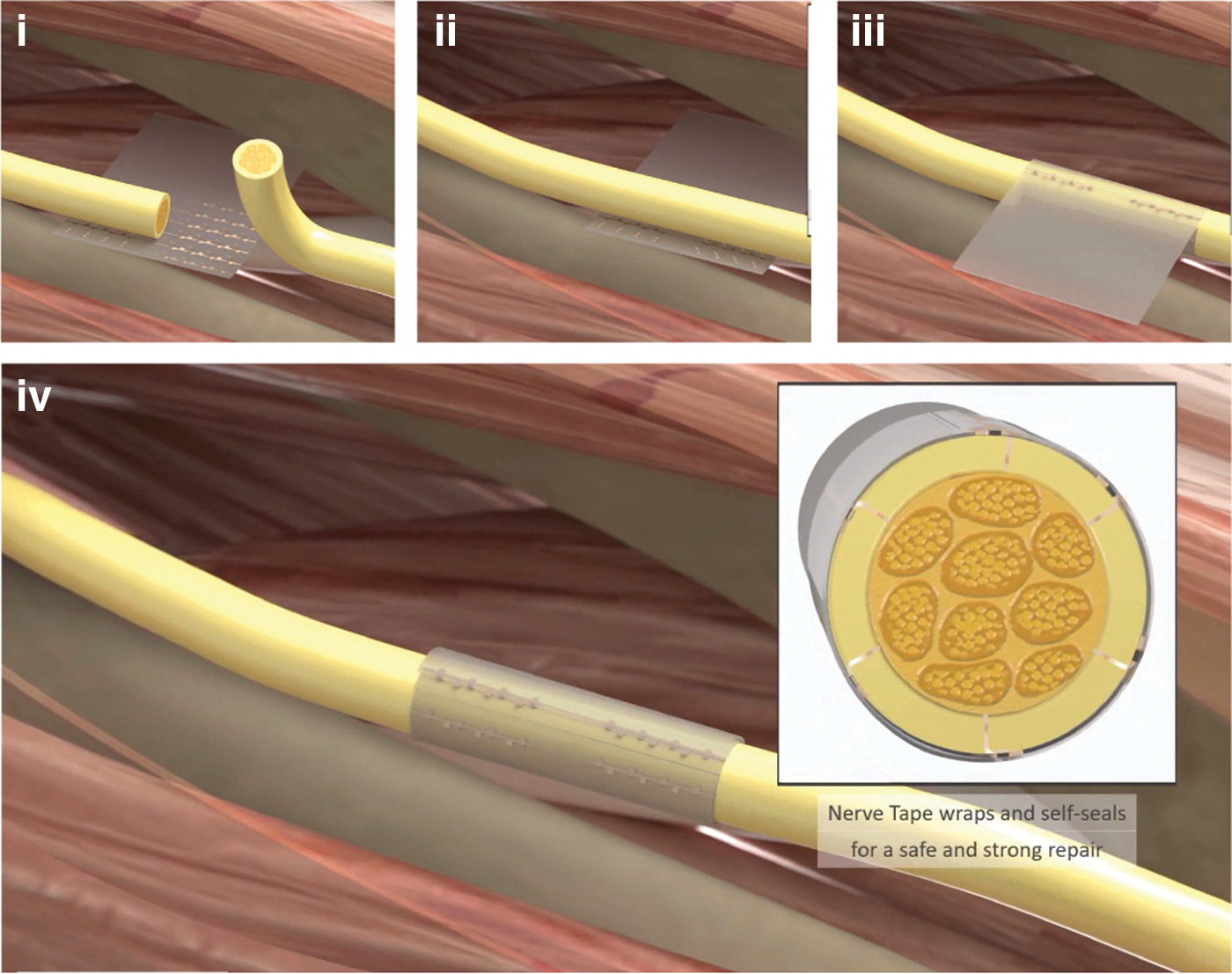
Nerve Tape enables sutureless repair of injured nerves. Nerve ends are laid onto microhooks
All animals received preoperative analgesic treatment (Buprenorphine SR LAB 0.1 mg/kg), and their operated hind limbs were wrapped in a preventive full contact pressure-relieving soft bandage to avoid the formation of pressure ulcers. Postoperative care and animal monitoring were performed for 16 weeks following surgery.
At the end of 16 weeks, animals were anesthetized and the tibial nerve of the experimental leg was exposed as described above, followed by gross assessment of the nerve and surrounding tissue, and electrophysiology (nerve conduction study) as described subsequently. After testing had been completed on the experimental limb, the contralateral control sciatic nerve was exposed and tested in the same way. After all the data were recorded, the animal was euthanized via an intravenous sodium pentobarbital injection. All animal procedures were approved by the Institutional Animal Care and Use Committee (IACUC) of the Virginia Commonwealth University in accordance with the National Institute of Health (NIH) Guide for the Care and Use of Laboratory Animals.
Gross tissue assessment
Immediately after nerve exposure during the endpoint surgery, the repair site was identified and assessed for gross morphological changes (i.e., maintenance of coaptation, evidence of inflammation or constriction, and quality of adhesions). A ruler was used to measure the width of the adherent tissue surrounding the repair site and scored based on a semiquantitative scale described in Supplementary Table S1.
Electrophysiology
The nerve was cleared of surrounding tissue to be prepped for electrophysiological recordings. The tibial nerve was isolated proximal to the coaptation (or at a similar level on the control limb) and distally near the ankle. A recording cuff electrode (Microprobes for Life Science, Gaithersburg, MD) and a stimulating bipolar electrode (Natus Medical, Inc., Middleton, WI) were placed proximal and distal to the level of the coaptation site. The active ground electrode was placed in a nonactive muscle tissue between the stimulating and recording electrodes. A headstage (A-M Systems, Sequim, WA) was utilized to manage stimulation signals, and an in-line amplifier (Model 1800; A-M Systems) used to smooth output signals for recording. The amplifier included high-pass and low-pass filters to pass signals between 1 Hz and 5 kHz and an initial × 10 k gain setting to optimize signal strength and signal-to-noise ratio.
Single square pulses of 0.2 ms duration were applied at different intensities, and the resulting waveforms were recorded at a sampling rate of 40 k/s. The recording program (LabChart Pro 24/T; ADInstruments, Sydney, Australia) also allowed the application of a mains filter to reduce noise. The stimulus strength (up to 2 V) was increased until a maximum amplitude nerve action potential waveform was recorded. Each stimulus intensity was repeated at least 30 times at 1 Hz to obtain an average response. The distance between recording and stimulating electrodes was measured with a ruler, recorded, and maintained throughout the course of the experiment to accurately calculate conduction velocities. This distance was between 15 and 17 cm for most testing sessions.
Muscle morphology, histology, and axon morphometry
Immediately after euthanasia, both hind limb tibial nerves and gastrocnemius muscles were extracted. The muscle weights were obtained, and muscle girth was measured using digital calipers (Mitutoyo America Corp., Aurora, IL). About 7 mm of the nerve tissue around the coaptation site was separately postfixed in formaldehyde, dehydrated, and embedded in paraffin (Histocore Pearl; Leica Biosystems, Germany). For Nerve Tape specimens, the outer layer of SIS material and the Nitinol hooks were peeled away to allow tissue and slide preparation.
For the first six animals in each group, immunohistology and Masson's trichrome staining were performed. Using a microtome, 12 μm transverse sections were obtained and mounted on charged slides. Unstained specimens were serially inspected under light microscopy (4 × optical magnification) to identify microhook penetration points and microsuture penetration points. Residual microhook defects and nylon suture material within the tissue were identified and followed in series until the deepest penetration point was identified. These sections were preferentially stained using the Leica “Gomori's Trichrome Special Stain Kit (Blue Collagen),” which involved a sequential fixation and staining process in 100% Bouin's solution, working Weigert's hematoxylin, and Gomori's trichrome. Brightfield images at 4 × magnification were obtained (Nikon Eclipse E 600; Nikon, Tokyo, Japan) and analyzed for microhook and microsuture proximity to inner fascicles, scar response, and overall collagen quality as described in a semiquantitative scale presented in Supplementary Table S2. Immediately neighboring sections were labeled for NF-200 (1:200, N5389; Sigma-Aldrich, St. Louis, MO) to visualize axons, P0 (1:200, ab3937; Abcam plc, Cambridge, United Kingdom) for myelin, 4′,6-diamidino-2-phenylindole (DAPI) for cell nuclei, and MAC387 for macrophages. Slides were deparaffinized, heated for antigen retrieval, permeabilized, and incubated in primary antibodies overnight followed by secondary antibodies.
Microhook and microsuture penetration points identified using the brightfield images were located on the immunohistochemistry (IHC) labeled slides, and high-magnification 20 × images were obtained using a confocal microscope (FV1000; Olympus Corporation, Tokyo, Japan) to grade the axon density and cellular density and quantify the number of local macrophages as described in Supplementary Tables S3 and S4.
Five (5) millimeters of nerve tissue (from all animals) proximal and distal to the coaptation site was excised and postfixed in Karnovsky's solution (Electron Microscopy Sciences, Hatfield, PA), dehydrated in alcohol, and embedded in resin. Thin, 1 μm transverse sections were obtained, mounted on charged slides, and stained with toluidine blue for axon morphometry analysis. High-magnification (40 × ) brightfield images were sampled throughout the nerve section to obtain six to eight images per sample (Nikon Eclipse E 600, Elements BR Image Acquisition; Nikon) and quantified using a semiautomated image analysis software (Image-Pro Analyzer; MediaCybernetics, Bethesda, MD). Axon counts and g-ratios from the images were averaged and compared between the groups.
Statistical analysis
Mean gastrocnemius muscle weights and girths, nerve conduction velocities, signal amplitudes, adhesion scores, axon counts, and g-ratios were compared between the three groups. The statistical methods selected were multiple Kruskal–Wallis w-tests and pairwise comparisons using the Bonferroni procedure at the 95% confidence level, and each run was analyzed individually without assuming a consistent standard deviation. For data where normality was confirmed using Shapiro–Wilk test (null hypothesis is that data are normally distributed; hypothesis rejected if p < 0.05) and homogeneity of variance was also confirmed using Bartlett test, ANOVA with post hoc pairwise comparison t-tests was performed with Bonferroni correction. From the data sets mentioned above, only nerve conduction velocity, muscle weight, and muscle girth met those criteria, so ANOVA was only performed on those data. Probability (p) values of <0.05 were reported as significant.
Results
Gross nerve tissue assessment
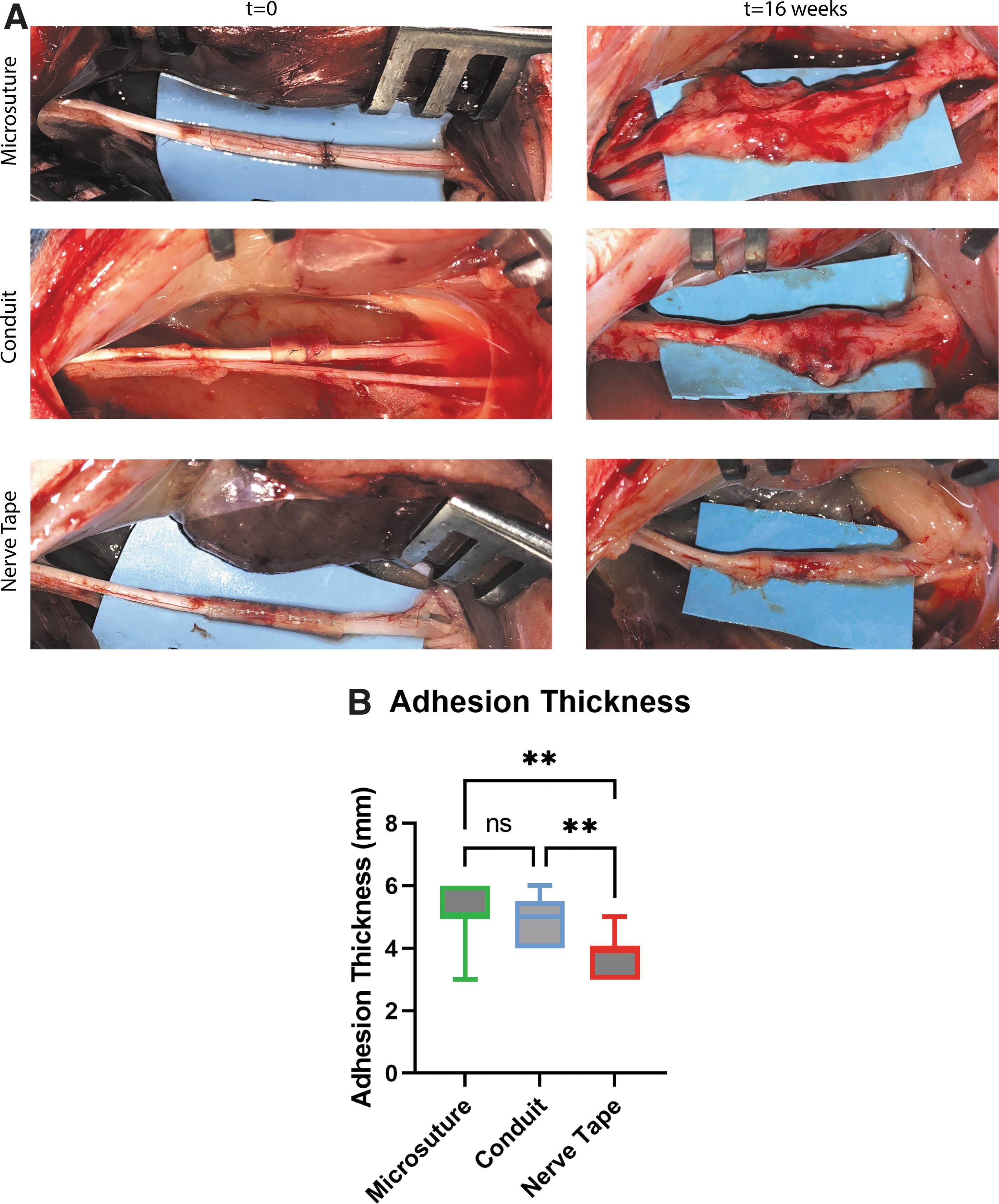
For all Nerve Tape repairs, the device remained fully wrapped at 16 weeks without any evidence of nerve constriction or inflammation (Fig. 3). One nerve repair in the conduit group suffered catastrophic failure (i.e., nerve stumps separated completely), while all other coaptations were in continuity. This animal was excluded from further analysis. Adhesion thicknesses measured at the repair site (5.1 ± 0.8 mm for microsutures and 4.8 ± 0.7 mm for conduit repairs) were significantly higher than the Nerve Tape group (3.7 ± 0.6 mm) (Fig. 3). Some perineural adhesions were graded “severe” in the microsuture and conduit repairs, but not in the Nerve Tape group.
Electrophysiology
Nerve conduction in the Nerve Tape group was significantly improved compared with the microsuture repair and conduit repair groups. Average conduction velocity and peak-to-peak amplitude for the Nerve Tape group (50.94 ± 7.71 m/s and 5.04 ± 2.88 mV) were significantly higher than the conduit group (34.5 ± 9.09 m/s and 2.49 ± 1.35 mV) (Conduction velocity: p < 0.05, pairwise t-test with Bonferroni correction; ANOVA: F = 6.401, p = 0.0062, degrees of freedom [Df] = 23, Critical F-value = 3.422. Amplitude: p < 0.05, pairwise Wilcox test with Bonferroni correction; Kruskal–Wallis, p = 0.0155) (Fig. 4).
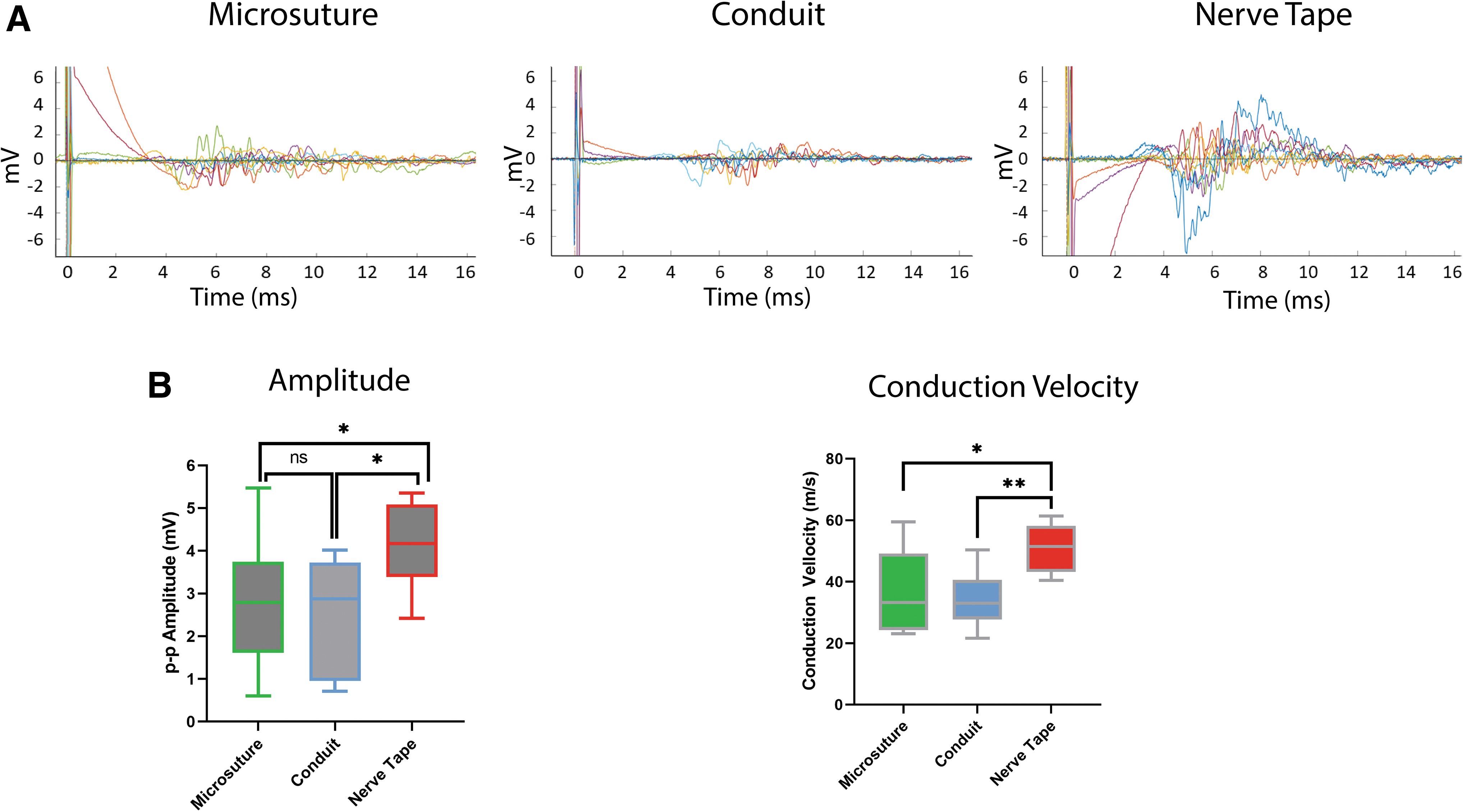
Average conduction velocity but not amplitude in the Nerve Tape group was significantly higher than the microsuture group (36.79 ± 13.41 m/s and 2.74 ± 1.51 mV) (Conduction velocity: p < 0.05, pairwise t-test with Bonferroni correction. Amplitude: p = 0.052, pairwise Wilcox test with Bonferroni correction; analysis of variance (ANOVA) and Kruskal–Wallis test details previously provided) (Fig. 4).
Muscle morphology
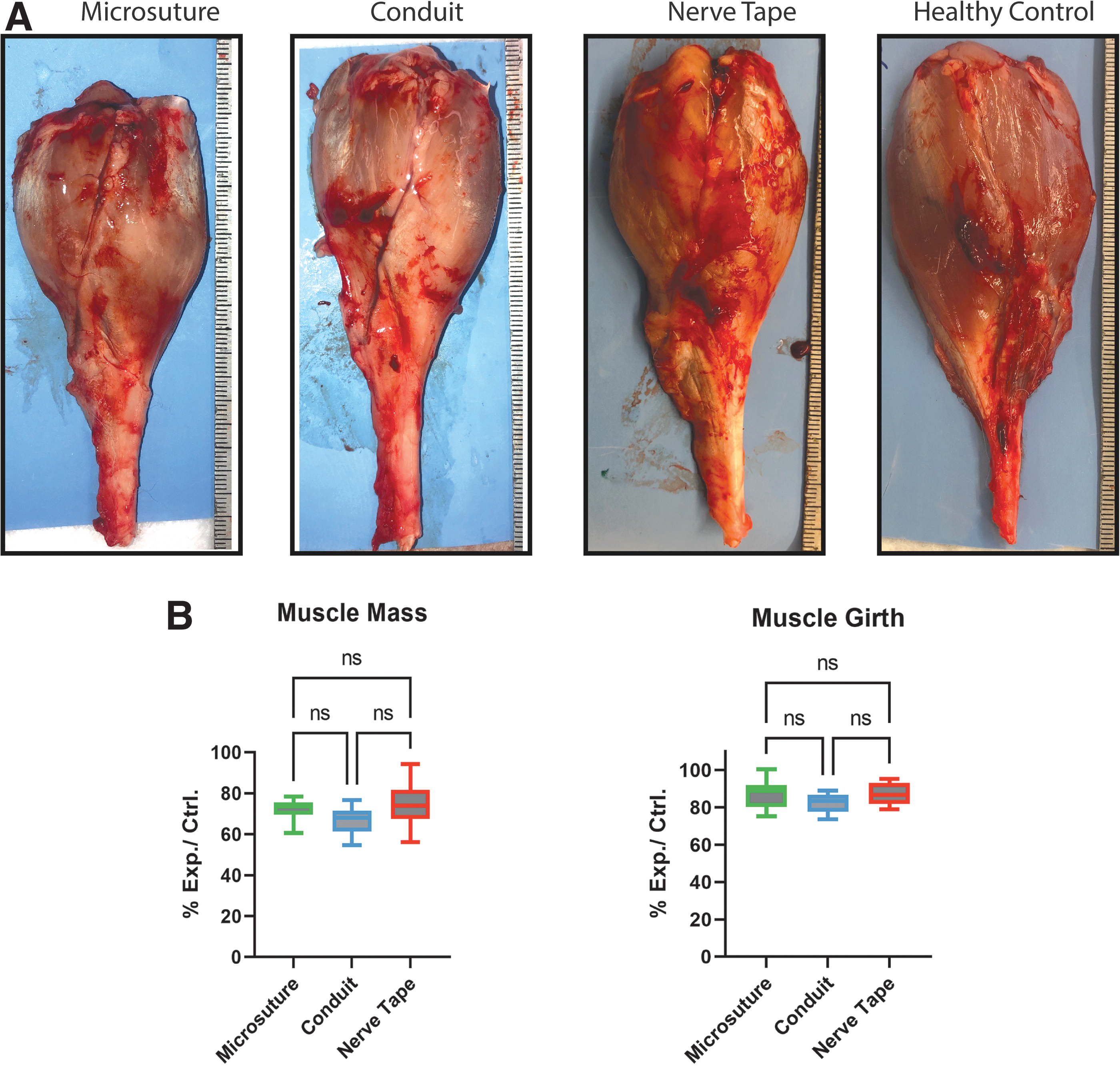
There were no statistically significant differences between groups in terms of average gross muscle mass (ANOVA: F = 2.322, p = 0.117, Df = 27, Critical-F = 3.354) or muscle girth (ANOVA: F = 1.912, p = 0.167, Df = 27, Critical-F = 3.354) (Fig. 5). Effect on muscle mass was expressed as a ratio percentage of experimental to control, with the average being 74% ± 10% for Nerve Tape group, 72.1% ± 5% for microsuture group, and 67% ± 7% for the nerve conduit group (Fig. 5).
Histology
Collagen deposition and quality scores based on Masson's trichrome staining were similar across all the three repair groups (Fig. 6). Scar tissue scores around the penetrating microhook/suture were also similar for all groups and ranged between mild and severe (Supplementary Tables S5 and S6).

Proximal and distal nerve sections for
Trichrome-stained images were used to determine whether microhooks or sutures penetrated fascicles. In no case was a microhook track found inside a fascicle. Conversely, suture material was identified within the nerve fascicles from both the conduit and microsuture groups in several specimens.
DAPI-positive cell density identified on immunohistochemistry analysis showed that cellularity around microhooks and sutures ranged between low to excessive without significant differences (Fig. 6). The density of local neurofilament and P0 labeled axons was also similar across the three groups. Very few macrophages were identified immediately around microhooks or sutures, with no differences between groups (Supplementary Tables S5, S6, and Fig. 6).
Axon morphometry
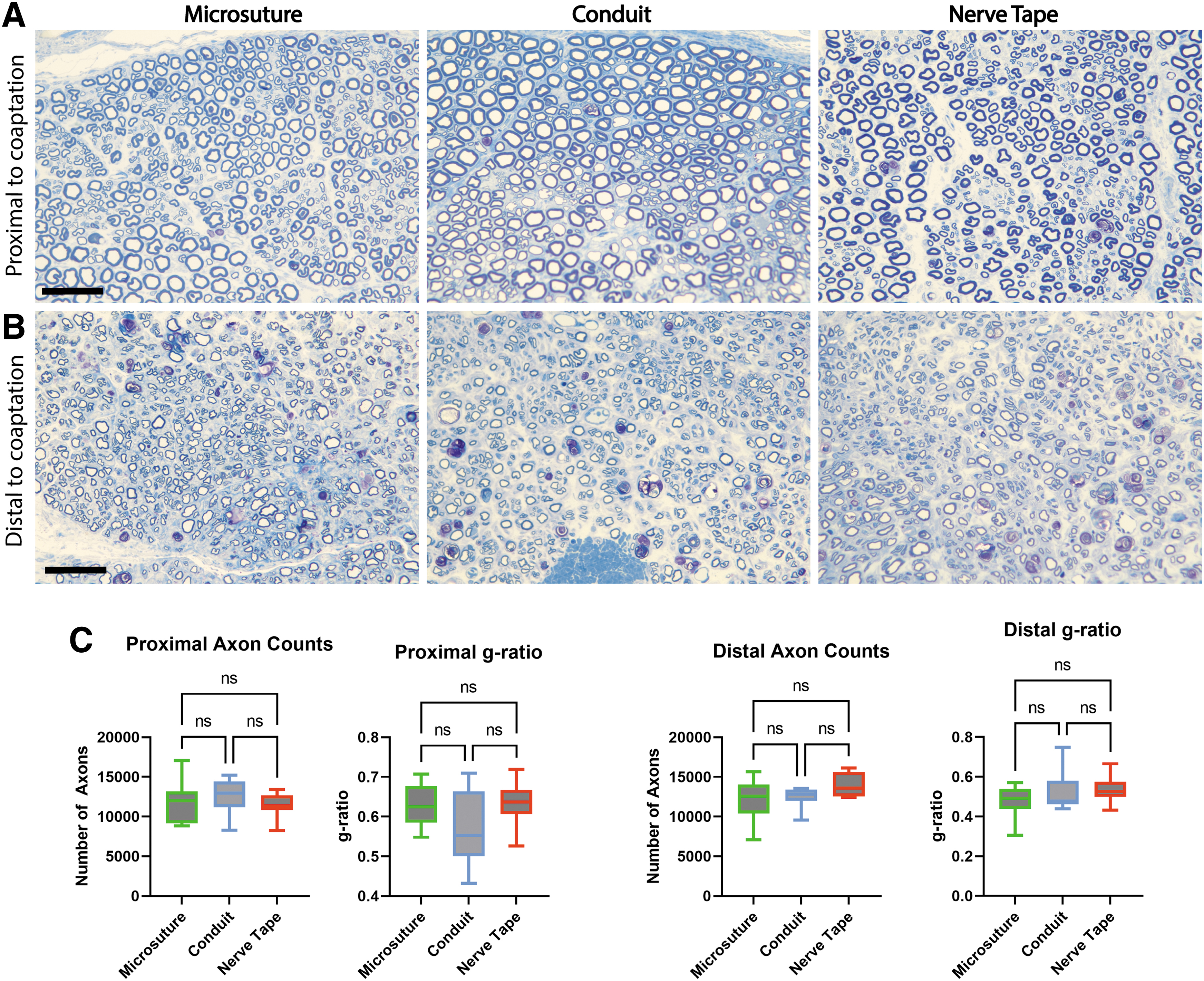
Average total distal axon counts based on toluidine blue staining were 13,859 ± 1454 for Nerve Tape, 12,466 ± 1265 for conduit, and 12,139 ± 2442 for microsuture groups (Fig. 7C). Average g-ratios for Nerve Tape, conduit, and microsuture groups were 0.54, 0.52, and 0.48, respectively. Axon counts proximal to the repair were 11,468 ± 1512 for Nerve Tape, 12,539 ± 2334 for conduit, and 11,971 ± 2523 for microsutures, with average g-ratios of 0.64, 0.57, and 0.63, respectively (Fig. 7). There were no statistically significant differences between the groups.
Toluidine blue-stained 40 × images for nerve sections
Discussion
This preclinical study was performed to assess the impact on nerve tissue and axonal regeneration of our novel nerve repair device versus conventional repair techniques. An in vivo rabbit tibial nerve model was chosen (New Zealand white rabbits), due to rabbits' more standard neural regenerative capabilities and sensitivity to implants (vs. rats). Along with Nerve Tape and standard microsuture repair, a third treatment group utilizing a conduit-assisted repair with an SIS device was included. This group served to differentiate the effects of the SIS substrate from the Nitinol microhooks. Outcome testing consisted of gross inspection (scoring of local adhesions/scarring/inflammation), reinnervated muscle morphology, immunohistochemistry, histomorphometry, and terminal electrophysiological measurements.
At 16 weeks postrepair, histomorphometry demonstrated negligible impact of the microhooks, and these data combined with our secondary outcome measures showed that Nerve Tape supported robust axon regeneration. After 16 weeks, average total axon counts and g-ratios distal to the repair were not statistically different between groups, at the observed site (1 cm distal to the repair.) Although average total axon counts distal to the repair were higher than the 8000 to 11,000 myelinated axons in intact rabbit tibial nerves,18,19 higher axon counts both proximal and distal to the repair are typical following nerve repair and attributed to antegrade and retrograde axonal sprouting. 20 The g-ratio is considered an indirect measurement of axon maturity and is influenced by both the size of the regenerating axon and the amount of myelin that has formed. Normal g-ratios, between 0.6 and 0.7, 21 are not expected postinjury. 22
Electrophysiology tests demonstrated superior regeneration in the Nerve Tape repairs compared with both conduit and microsuture repairs. The average nerve conduction velocities recorded in the control limbs, 101.7, 104.4, and 108.2 m/s for the microsuture, conduit, and Nerve Tape groups (respectively), were similar to the previously reported values ranging from 68.2 to 100 m/s. 19 The slightly lower conduction velocities in the repair groups, 36.79, 34.5, and 50.94 m/s (microsuture, conduit, and Nerve Tape), compared with the published value of 59.9 m/s following primary rabbit tibial nerve repair, 19 may be explained by our more distal recording site, which was ∼17.5 cm from the repair site and may have limited the number of functional axons and the detectable signal at that level. Regardless, the data suggest that more axons from the Nerve Tape group regenerated to that distance, compared with the conduit and microsuture group.
Although we did not specifically assess the axon regeneration speed, we observed equivalent axon numbers 1 cm from the repair site, and faster regeneration and maturation would account for more axons and superior amplitude distally. Possibly the multiple microhook engagement points in the Nerve Tape dispersed tension to positively influence regeneration. Kechele et al. and Schmidhammer et al. have both demonstrated faster recovery with analogous tension distribution strategies.15,23 The statistically inferior conduction parameters found in the conduit repaired tibial nerves may reflect a slight detrimental constricting effect of the conduit construct versus the more expandable Nerve Tape construct 24 —although gross inspection was not indicative of constriction in any of the groups. Reinnervated muscle to contralateral control muscle weight and girth ratios (recognized surrogates for reinnervation) 25 were not significantly different between the three repair groups.
The experimental limbs were immobilized for much of the recovery period as a necessary step to prevent heal ulceration and autophagia. This immobilization might have limited the expected reversal of muscle atrophy following reinnervation. Muscle force testing was not possible due to known anesthesia-related muscle flaccidity issues well documented with this experimental model. 26 Other functional outcome measures in rabbits have not been developed.
Both Nerve Tape and the conduit are manufactured utilizing a decellularized porcine small intestine submucosal extracellular matrix that incorporates within the mesoneurium. 27 The addition of this material to the coaptation site would be expected to increase the thickness of the nerve, making retrospective determination of the actual microhook/suture penetration depth inconclusive. Therefore, microhook/suture penetration depths and the overall nerve cross-sectional data were not included. The observation of increased adhesion thickness in the microsuture repair group was inclusive of the additional tissue scaffold in the other two groups (i.e., the SIS materials had not been removed before measuring).
Whether utilizing microsutures or microhooks, some penetration into the nerve is necessary to maintain nerve end coaptation, without which axonal regeneration and functional recovery would not be possible. The relative benefit of one technique versus another must be weighed against relative risk. While some microhooks appeared in direct contact and even indenting fascicles, none of these microhooks violated the perineurial layer or otherwise appeared to harm the neural fibers within. Some contact with fascicles was not surprising based on the ∼2 mm diameter of the rabbit tibial nerves.
We theorized that independent gliding of the fascicles within the inner-epineurial connective tissue envelope allowed them to slide away from the microhooks. By contrast, despite efforts to place sutures as superficially as possible, nylon was identified within fascicles of subjects in both the conduit and microsuture repair groups. From a long-term safety standpoint, the penetration of the perineurium and violation into the fascicle are the critical issues. The perineurial layer is an extension of the blood–brain barrier from the central nervous system, and the intrafascicular environment is normally protected and isolated. Contact with fascicles is likely not detrimental, as long as the perineurial layer is not disrupted. This question has been extensively explored in the implantable neural electrode literature. Intrafascicular electrode placement (analogous to microhook or suture penetration inside the fascicle) results in fibrosis and neural damage (including demyelination, decreased axon size, and degeneration of distal fibers).28,29 Interfascicular electrodes on the contrary are not associated with any of this morbidity. 28
Additional evidence of the importance of the perineurial layer in comparison with the epineurial layer is highlighted by the clinically accepted practice of internal neurolysis, in which the entire epineurium layer can be removed without affecting nerve function. 30 In other words, interfascicular microhook placement should be safe and should not affect long-term nerve function, while intrafascicular placement would damage the nerve and could (at least theoretically) compromise end results. Regardless, whether within the intrafascicular or inner epineurial spaces, neurofilament-labeled axons were demonstrated around comparable microhooks and microsutures in similar densities. Although a nonspecific tissue reaction measurement, cellular densities (per DAPI labeling) immediately around microhooks and microsutures were also similar.
Histology also indicated a similar inflammatory response in the three repair groups. Macrophages, a strong cellular marker of foreign body-induced inflammatory response, were labeled, but only a few identified immediately adjacent to the microhook, and none along suture paths. A more expansive quantification of labeled macrophages across the entire nerve cross section may have produced higher numbers due to nerve wrap material-induced inflammation. 31 However, these data would not have been specific to the microhook versus microsuture localized foreign body response and were therefore not assessed. Neutrophils are also a strong inflammatory marker but typically peak shortly after implantation (so less meaningful at 4 months),32,33 and identification of these cells was not attempted. Immunolabeling for neutrophils is not available for the rabbit animal model.
Intraneural fibrosis around microhooks and sutures, as a marker of chronic-phase foreign body reaction, 34 was similar across groups and generally classified as mild to moderate. No other microhook-related complications were observed in any of our animals.
Conclusion
These results demonstrate that Nerve Tape provides a consistent means of sutureless nerve repair, does not cause disproportionate intraneural damage, and supports nerve regeneration equivalent to, if not slightly better than, conduit or microsuture for primary nerve repair.
Footnotes
Authors' Contributions
G.B., R.C., M.S., I.C., and J.I. designed the experiments. G.B., L.D., M.S., I.B., M.F.G., R.C., J.M., F.G., and M.S. performed the experiments and collected the data. G.B., R.C., J.M., J.G., I.C., and J.I. analyzed the data. G.B. wrote the original draft, J.I. led the review and editing, and all the authors provided feedback on the final article. I.C. and J.I. wrote the grant that supported this work.
Data Availability
Data included in this article can be shared upon request.
Disclosure Statement
R.C., J.M., F.G., M.S., J.G., and I.C. are employees of BioCircuit Technologies. J.I. and I.C. have patent “Devices and methods for repairing damage to a tissue” jointly awarded to the Virginia Commonwealth University and BioCircuit Technologies, Inc., J.I. receives license-related income from BioCircuit Technologies, which has licensed the Nerve Tape device. J.I. and G.B.'s institution receives license-related income for licensing the Nerve Tape device. The other authors have no conflict of interest.
Funding Information
This work was supported by NIH NINDS grant R44NS097113.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.