
Abstract
Normothermic ex vivo liver machine perfusion (NEVLP) has been developed to address the increasing organ shortage in liver transplantation, through optimal preservation, assessment, and conditioning of grafts from extended criteria donors. There remains a need to establish simple and standardized animal models that simulate clinical NEVLP to test novel therapies. Liver grafts from 36 Sprague-Dawley rats were perfused for 6 h in a dual-vessel NEVLP system with a Dulbecco's modified Eagles medium-based perfusate supplemented with rat plasma and erythrocytes. Varying doses of the clinically used vasodilator epoprostenol, Kupffer cell inhibitor glycine, and a Steen™-based perfusate were assessed. Perfusion pressures and bile production were recorded, and perfusate was analyzed for transaminase secretion. Tissue samples were evaluated histologically, and levels of cytokines and 8-Isoprostane were measured. Increasing levels of epoprostenol and the addition of glycine resulted in a stepwise decrease of transaminase secretion and improved bile production. Steen further decreased transaminase release and interleukin 1 beta levels. Liver grafts perfused with the optimized Steen-based protocol exhibited lowest levels of oxidative stress and best-preserved liver integrity. In conclusion, epoprostenol seemed to ameliorate liver function and prevent cellular damage beyond its vasodilatory effect, with glycine acting synergistically. The anti-inflammatory and antioxidative properties of Steen further improved the outcome of perfusion. Our rodent NEVLP system may be used to rapidly test new agents for the pharmacologic conditioning of livers and help translate findings from bench-to-bedside.
Impact statement
Normothermic ex vivo liver machine perfusion (NEVLP) enables objective assessment of the quality of marginal liver grafts and provides the opportunity for organ conditioning. To optimize perfusion and assess new pharmaceutical interventions, simple and standardized animal models of NEVLP remain necessary. Our NEVLP system is a scaled-down version of a clinically used setup that we believe has potential to enable rapid translation of new findings from bench to bedside.
Introduction
The prevalence of end-stage liver disease has been rising for the last decade, 1 while unfortunately, the number of transplants performed has been recently declining across Europe. 2 The increased demand for liver allografts is challenged by a limited supply, mainly due to an aging population, 2 as well as the detrimental effects of a high prevalence of fatty liver disease and fibrosis on graft quality. 3
Substantial advances have been made in the clinical use of normothermic ex vivo liver machine perfusion (NEVLP) for improved preservation and quality assessment of organs that were previously considered suboptimal or even unfit for transplantation.4–7
Using conventional static cold storage, the decision to accept or decline an organ offer depends on donor characteristics, duration of ischemia, histopathological assessment of the graft, and ultimately the transplant surgeon's subjective assessment of the graft's macroscopic appearance. NEVLP yields several objective parameters for viability assessment such as bile production, lactate clearance, and perfusate pH and glucose levels, which have proven to be relevant for post-transplantation outcome.8–10 Moreover, the prospect of increasing organ preservation time 11 and expansion of the donor pool through pharmaceutical conditioning and repair of marginal grafts 12 continues to drive scientific interest in NEVLP.
In efforts to investigate novel therapies in NEVLP, animal models are necessary to simulate clinical conditions as closely as possible and thus allow rapid translation from bench-to-bedside. In a reverse “bedside-to-bench” approach, the aim of this study was to develop a reproducible small animal NEVLP model by scaling down a clinically used NEVLP system. Perfusion of the liver through the portal vein and the hepatic artery remains the standard in clinical NEVLP. The dual-vessel setup has also been proven to be superior in a rodent model, 13 but is currently not widely used in this context.14–16
The presented setup combines a dual-vessel perfusion previously described by our group 13 with perfusate composition and vasodilators as described in the human NEVLP trial by Selzner et al. 17 using the OrganOx metra® device. Pharmacological vasodilation is necessary in dual-vessel perfusion systems because arterial spasms may be caused by intraoperative manipulation, cold storage, and upon reperfusion.18,19 Moreover, physiological flow conditions represent a major viability criterion for liver grafts. Prostacyclin analogs such as epoprostenol are recommended for the OrganOx metra by the supplier 20 and represent the most widely used vasodilators in clinical trials, 21 with the additional benefit of reducing hepatic ischemia reperfusion injury (IRI) through inhibition of inflammatory signaling. 22
While not a clinical standard, glycine is known to decrease the expression of proinflammatory cytokines through temporary inhibition of Kupffer cell activation. 23 Since the positive effect of glycine on perfusion outcome has already been proven in a single-vessel system, 14 we herein systematically evaluated the impact of glycine supplementation in our dual-vessel setup. The cell culture medium Dulbecco's modified Eagles medium (DMEM) was used as perfusate, which constitutes a standard in small-animal NEVLP systems. 24 After evaluation of the glycine effect and optimal epoprostenol doses, a final experimental group was performed with Steen™ solution. Steen solution was originally developed for ex-vivo lung perfusion, but is now used for clinical NEVLP as well.13–15,17,25
Methods
Study design
A total of 36 rat livers were explanted and perfused for 6 h in a normothermic dual-vessel ex-vivo liver perfusion system using different protocols. After randomization of animals, n = 4 livers per group were perfused using varying doses of epoprostenol (0, 250, 1000, and 2000 ng/h). In four corresponding groups, glycine was supplemented to the circuit at a concentration of 12 mM. Second, the best-performing protocol (as evidenced by assessment of liver damage parameters) was repeated with Steen solution as base perfusion medium instead of the previous combination of DMEM supplemented with rat plasma. The study design is schematically depicted in Table 1.
Study Design and Group Characteristics
All groups performed as n = 4.
DMEM, Dulbecco's modified Eagle medium.
Surgical procedures
Male Sprague-Dawley rats (Janvier, France) were kept under species-appropriate conditions and all procedures were approved by the local animal welfare authority (LaGeSo Berlin, project numbers G0012/18 and T0301/17). Surgical procedures were performed as described by Claussen et al. 13 The animals were anesthetized, the abdominal cavity was opened, and the liver was mobilized followed by injection of 500IE heparin and finalization through blood withdrawal through the aorta. The celiac trunk was cannulated through the aortic patch after ligation of all other arterial branches, except the proper hepatic artery. Then the portal vein was cannulated, and both were flushed with 20 mL of 4°C histidine-tryptophan-ketoglutarate (HTK) solution (Dr. Franz Köhler Chemie GmbH, Germany), with or without glycine respective to the experimental groups. Bile duct and inferior vena cava were cannulated using customized tubing. The explanted liver was stored in 4°C HTK±glycine. At procurement, livers weighed between 255 and 355 g.
Perfusate composition and perfusion setup
The base perfusion medium consisted of DMEM containing 1 g/L D-glucose and pyruvate (Thermo Fischer, USA) or Steen Solution (XVIVO Perfusion, Sweden). When DMEM was employed, 35 mL was mixed with 5 mL of frozen rat plasma and 10 mL of isolated rat erythrocytes. When using Steen solution, 40 mL was mixed with 10 mL of rat erythrocytes. Hematocrit was set to 15% according to the registration study for Steen solution. 26 Further additives in both groups included 1.3 mL aminoplasmal 10% (B. Braun, Germany), 25 mg cefazoline (MIP Pharma, Germany), 12.5 mg metronidazole (B. Braun), 0.5 mmol sodium-bicarbonate (B. Braun), and 250IE heparin (Ratiopharm, Germany).
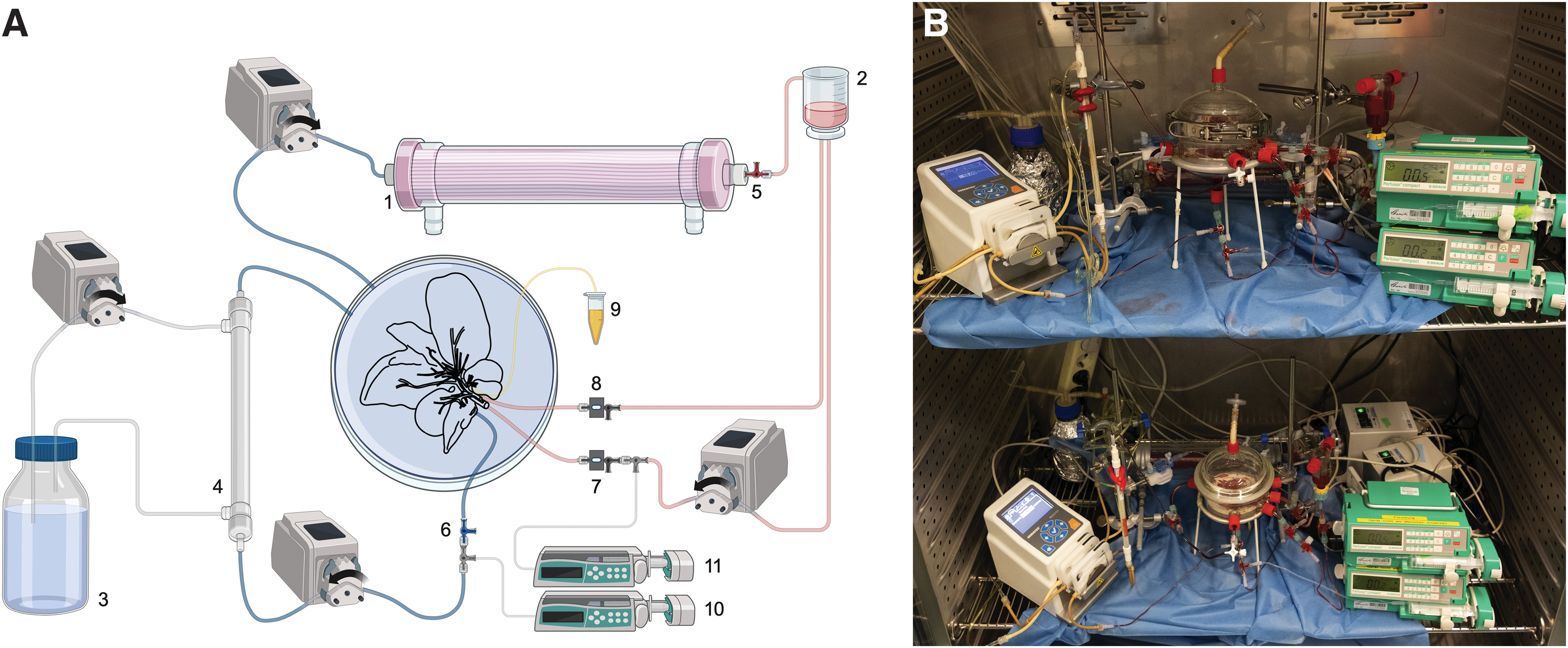
Insulin lispro (Lilly, USA) was added at 1.5IE/h and taurocholic acid (Acros Organics, USA) at 3.5 mg/h using a syringe driver. Additives are presented in Table 2. Epoprostenol (Panpharma, Germany) was injected in varying concentrations in respective groups using the hepatic artery canula. Glycine was added for priming as well as continuously in respective groups. The dual-vessel perfusion system was sustained for 6 h at 37°C by placing the perfusion circuit inside a laboratory incubator. After flushing with 20 mL of sodium chloride (NaCl) 0.9%, the organ was placed inside a custom-made bioreactor (Glas Gaßner, Germany), doubling as perfusate reservoir (Fig. 1A, B) and the cannulated vessels connected to the circuit. FiO2 was set at 90% using a silicone tubing oxygenator (Radnoti LTD, Ireland), while a bubble trap prevented air embolisms into the organ.
Perfusate Composition
Perfusion flow was slowly increased over 10 min using flow-controlled pumps (Hugo Sachs Elektronik, Germany) until a maximum flow of 1 mL/min/g liver weight for the portal vein and 0.2 mL/min/g for the hepatic artery was reached. These values were chosen according to physiological flow measurements in vivo as well as based on our prior experience.14,27 Pressure in the hepatic artery as well as the portal vein was continuously recorded using pressure transducers (Hugo Sachs Elektronik) and BDAS 2.0 Software (Harvard Apparatus, USA). Pressure recordings were cut off at 198.2 mmHg due to technical limitations. Supraphysiological pressure was defined at above 114 mmHg for the hepatic artery and 12 mmHg for the portal vein. 28
Organ outflow through the inferior vena cava was left draining freely back into the reservoir. A multichannel pump (Ismatec, Oak Harbour, WA, USA) provided a flow of 10 mL/min into a dialysis cartridge (Spectrum Labs MidiKros 30 kDa, Gardena, USA) on the perfusate as well as the dialysate side, where 500 mL of low potassium MultiBic (MultiBic® 2 mM potassium; Fresenius, Germany) ±12 mM glycine was recirculated using the countercurrent principle. Bile was collected through the cannula in the bile duct. A complete list of materials used can be found in Supplementary Table S3.
Sample procurement
Bile was weighed and snap-frozen hourly. Perfusate samples were collected from inflow and outflow channels immediately after commencement of perfusion and at 3 and 6 h. Dialysate samples were measured after perfusion and at 6 h. Blood gas analyses were conducted with an ABL800 Flex (Radiometer GmbH, Germany). Photometric measurements of alanine transaminase (ALT), aspartate transaminase (AST), lactate dehydrogenase (LDH), urea, and total bilirubin were performed in the perfusate by a commercial laboratory (Labor Berlin–Charité Vivantes GmbH, Berlin, Germany). After perfusion, the livers were flushed with 4°C NaCl 0.9% and weighed. Tissue samples were either snap frozen or fixed in formalin. Bile ducts were dissected in the liver hilum and snap frozen. Hepatic oxygen uptake ratio (HOUR) was determined in accordance with Tolboom et al. 29
Histological analyses
Mayers' haematoxylin and eosin (HE) staining (AppliChem, Germany), TdT-mediated dUTP-biotin nick end labelling (TUNEL) staining (In situ cell death detection kit; Roche, Switzerland), and 4′,6-diamidine-2-phenylindol counter staining (Thermo Fisher) were performed on all sectioned liver lobes, as well as bile ducts according to standard protocol. Images were taken with a Zeiss Axio Observer.Z1 microscope using an AxioCam 1Cc5 for HE and AxioCam 506 mono for immunofluorescence stains and analyzed with the Zen 2.3 Pro software (Carl Zeiss AG, Germany).
Quantification of tissue edema
Tissue of E2000G+ and Steen groups was lyophilized and the tissue water content was estimated through the difference in dry to wet weight and compared to that of n = 4 nonperfused livers.
Analysis of cytokines in tissue samples
Tissue cytokine analysis was performed for interleukin 1 beta (IL-1β), IL-6 interleukin 6 (IL-6), interleukin 10 (IL-10), and tumor necrosis factor alpha (TNF-α) with a multiplex magnetic bead-based assays (Milliplex Rat Cytokine/Chemokine Magnetic Bead Panel; Merck, Deutschland) in homogenate made up of 50 mg of liver tissue, 750 μL of lysis buffer (Milliplex MAP Lysis Buffer; Merck, Germany), and 112.5 μL of protease inhibitor (complete mini protease inhibitor; Roche). After centrifugation, the assay was performed with supernatant in 1:25 dilution, the plate was read in a Luminex MagPix. Cytokine concentrations were normalized to total protein concentration, measured using a bicinchoninic acid assay (Thermo Fisher).
Analysis of 8-Isoprostane in tissue samples
8-Isoprostane (8-Iso-PGF-2α) was measured using ELISA (Cayman Chemical, USA) from liver tissue lysates made of 100 mg of tissue, 1 mL of 0.1 M phosphate buffer (pH 7.4), 1 mM ethylenediaminetetraacetic acid, and 0.005% butylated hydroxytoluene. After homogenization and centrifugation, the supernatant was frozen at −80°C. For dissolving esterified 8-isoprostane, hydrolysis was performed in potassium hydroxide following manufacturer's instructions. After purification through C-18 SPE cartridges (Cayman Chemical), 8-Isoprostane was eluted in methanol, dried under a constant stream of nitrogen, and resuspended in ELISA buffer with subsequent measurement at a 1:10 or 1:20 dilution. Normalization was again performed in relation to total protein concentration.
Statistical analysis
All variables were checked for normal distribution using the Shapiro-Wilk test. If normal distribution was assumed, ANOVA with Tukey's post-hoc test was used for multiple comparisons. Kruskal-Wallis test was used when no normal distribution could be assumed. Statistically significant results were highlighted in the figures when comparisons between individual groups were assessed. In the comparison of basic media (DMEM vs. Steen), t-tests with Holm-Šídák were used when normal distribution was given, and Mann-Whitney U test otherwise. Unless stated, data were presented as mean ± standard error of mean and a p-value ≤0.05 was considered significant. Statistical calculations were performed with SPSS 28.0. (IBM, USA) and graphs were generated using GraphPad Prism Version 8.3.1 (GraphPad Software, USA).
Experiment
Intergroup variance
There was no significant variance between groups concerning animal weight (302.8 ± 4.7 g), liver weight (12.9 ± 0.2 g), or cold ischemia time (70.5 ± 1.3 min). Electrolytes were kept in near-physiological range for all experiments over the course of perfusion (Supplementary Table S1).
Epoprostenol, glycine, and Steen improved organ quality
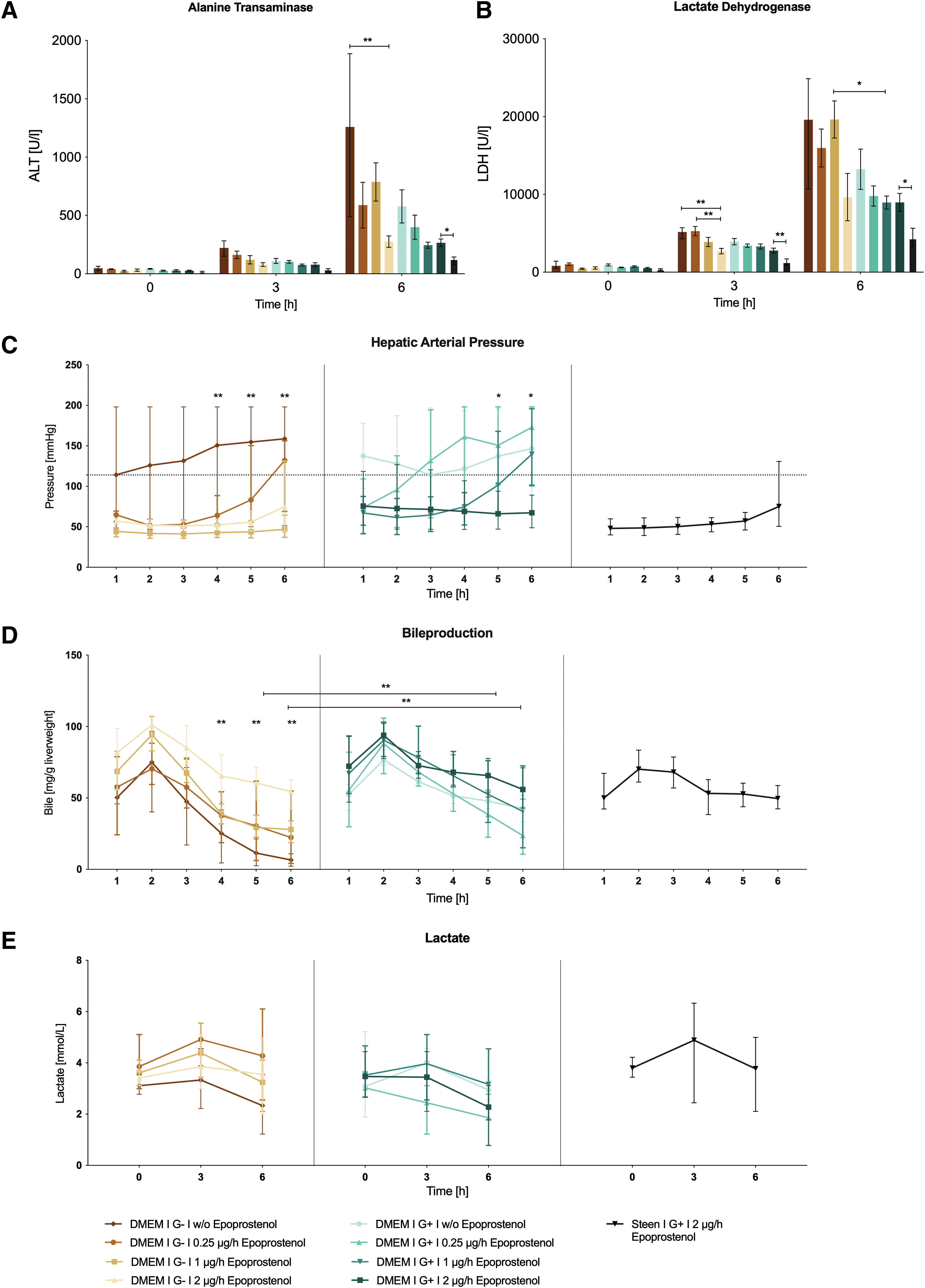
The release of transaminases and LDH was considerably less pronounced in groups where glycine was added to the perfusate, with significant differences between the E1000|G− versus E1000|G+ group (Fig. 2A, B; Supplementary Fig. S1A). Interestingly, at the highest dose of epoprostenol, no additional effect of glycine was seen. Epoprostenol showed a seemingly dose-dependent effect in the groups without glycine, with significant differences for AST and ALT between E0|G− and E2000|G− groups after 6 h. Steen solution led to a significant further decrease in all markers of cellular damage when compared to its DMEM counterpart (E2000|G+; AST: p = 0.016; ALT: p = 0.029; LDH: p = 0.011; Supplementary Table S2).
Characterization of liver grafts during 6 h of NEVLP.
Vascular resistance was decreased through epoprostenol, but increased with infusion of glycine
Livers perfused with or without 250 ng/h of epoprostenol frequently surpassed the upper limits of physiological hepatic arterial pressure (Fig. 2C). Epoprostenol of 1000 ng/h achieved physiological arterial pressure over the whole 6-h perfusion period without glycine, but pressures escalated at the end of perfusion with glycine (E1000|G− group 139.8 ± 20.1 mmHg versus E1000|G+ group 46.8 ± 6.3 mmHg, p = 0.119). Epoprostenol of 2000 ng/h allowed sufficient pressure control, independent of glycine. The basic medium used for perfusion had no significant effect on the hepatic arterial pressure. Portal venous pressure remained below 12 mmHg in all but one experiment (E2000|G+), where it continuously plateaued at around 15 mmHg (Supplementary Fig. S2A).
Livers remained metabolically active and maintained physiological homeostasis
The perfusate pH was at near-physiological range (7.2–7.3) throughout the time points. Baseline pH surpassed the physiological limit of 7.45 in some cases and trended downward after 3 h with a subsequent rise again toward the end of the perfusion period (Supplementary Fig. S2B). HOUR was highest at the start of perfusion in most cases and significantly declined over the course of perfusion. Initial oxygen uptake, as well as oxygen uptake after 6 h tended to be higher in groups with glycine and with higher doses of epoprostenol (Supplementary Table S1).
Bile production peaked in the second hour of perfusion in all experiments (Fig. 2D). Bile production increased in groups without glycine with rising epoprostenol concentrations. This effect was most pronounced in the second half of perfusion, with a significant difference between E2000|G− and E0|G− groups (4 h: p = 0.009; 5 h: p = 0.004; 6 h: p = 0.003). Livers perfused with glycine tended to keep producing more bile than their counterparts in the latter half of the perfusion, with a significant difference between E0|G− and E0|G+ groups after 5 h (p = 0.01) and 6 h (p = 0.007).
Glucose levels exceeded physiological limits at the beginning of perfusion in almost all experiments and consistently declined throughout the perfusion period, reaching the physiological range in most cases (Supplementary Fig. S2C). Lactate clearance was inconsistent throughout groups, with no clear correlation to a specific treatment. Individual livers in all groups showed clearance below the threshold of 2.5 mM (based on Mergental et al. 4 ) over the course of perfusion. However, a significant variance was seen between subjects within groups. In most cases, lactate concentration increased from 0 to 3 h postreperfusion and declined toward the end of perfusion (Fig. 2E). Interestingly, when accounting for plasma expansion through the dialysis circuit by calculation of absolute values of lactate produced, lowest values were seen in the E1000|G+ and E2000|G+ groups (Supplementary Fig. S2D).
Urea concentration consistently increased over the course of perfusion (Supplementary Fig. S2E). Livers perfused with glycine showed significantly increased urea production compared to their counterparts without glycine at most epoprostenol dosages (0 ng/h: p = 0.029; 250 ng/h: p = 0.021; 2000 ng/h: p = 0.001). Plasma bilirubin levels remained below the threshold for measurement in almost all livers, with no significant difference between groups.
Optimized perfusion conditions preserve the liver architecture
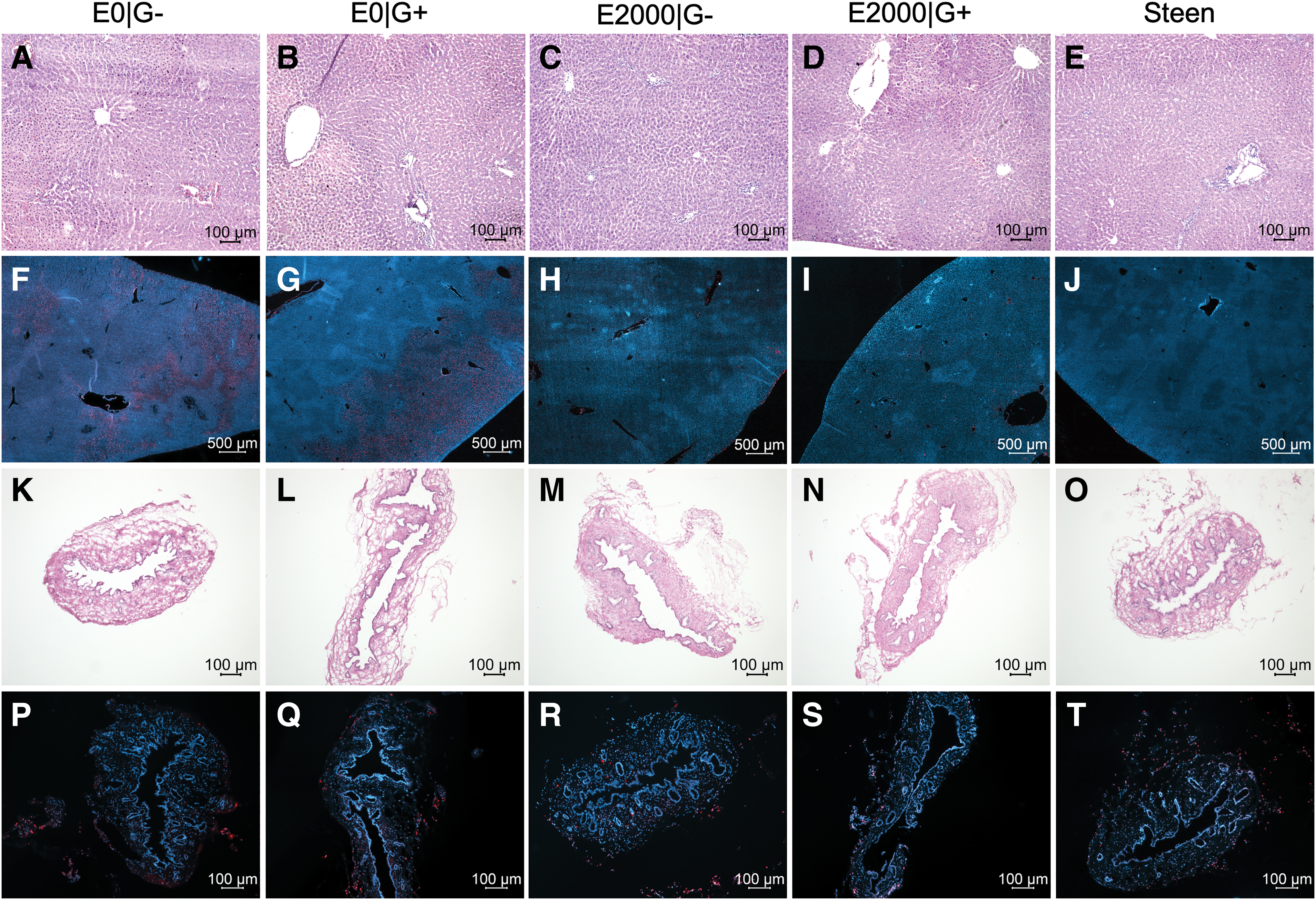
Sinusoidal congestion and large areas of necrosis were seen in groups without sufficient arterial pressure control. In contrast, livers perfused with the highest epoprostenol concentrations and Steen showed only small areas of pressure necrosis in areas the graft rested on the silicone mesh (Fig. 3A–E). Only few TUNEL-positive cells located near the liver capsule and vascular lining were seen in all groups using the highest epoprostenol concentrations (Fig. 3F–J), while larger areas of TUNEL-positive cells were found in the liver parenchyma, as well as endothelial cells in groups with lower epoprostenol concentrations. The bile duct epithelium was well preserved with little to no apoptotic cells, while the submucosa and muscularis layers exhibited varying amounts of apoptotic cells and some structural defects (Fig. 3K–T).
Histopathologic analyses of liver tissue at the end of perfusion:
Epoprostenol and Steen influence the cytokine profile
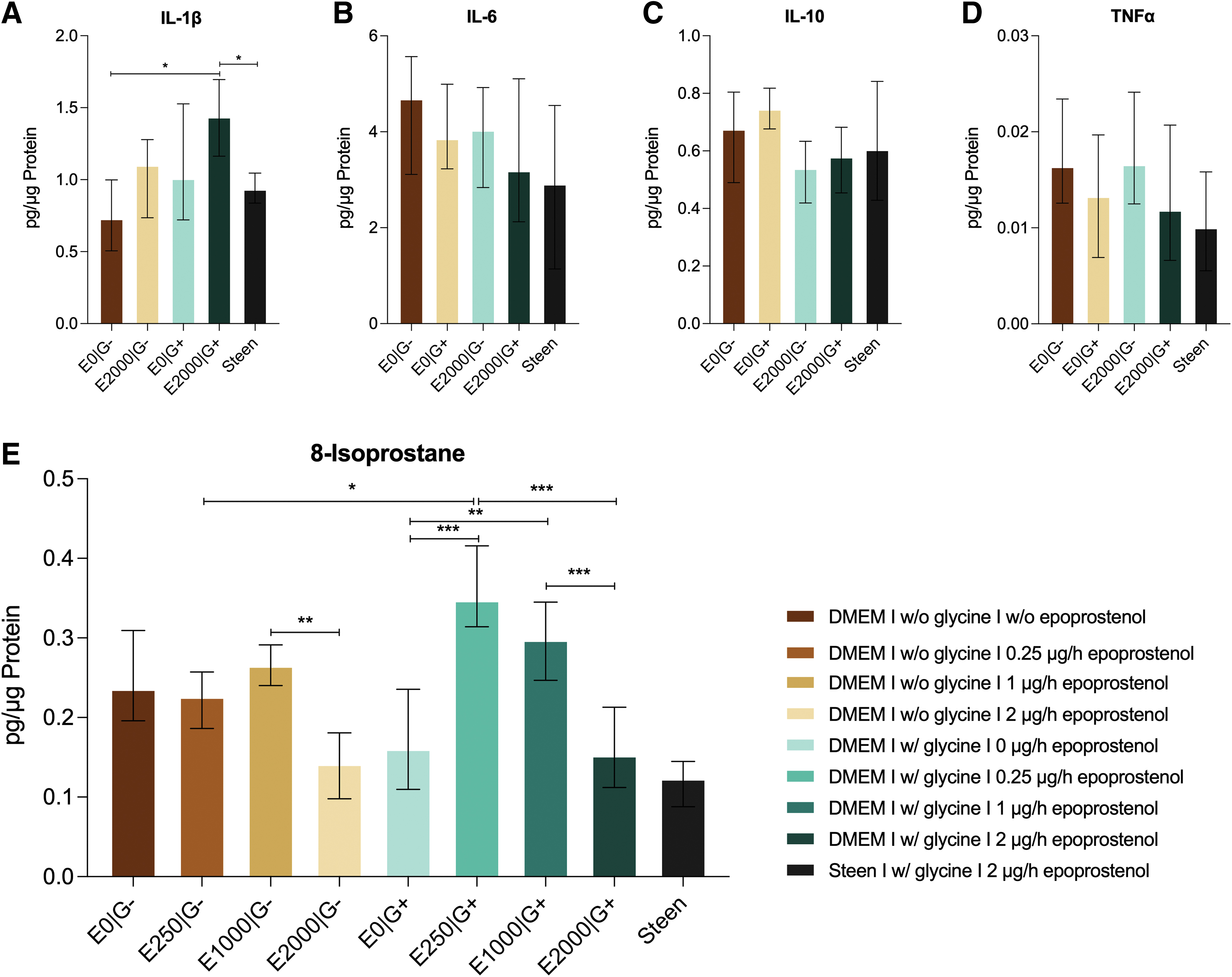
No clear correlation was seen with the addition of glycine or higher doses of epoprostenol alone and levels of either proinflammatory or anti-inflammatory cytokines in the liver grafts (Fig. 4A–D). However, the combination of high doses of epoprostenol and glycine (E2000|G+) led to higher levels of IL-1β in liver tissue compared to the E0|G− group (p = 0.019), while the other proinflammatory cytokines IL-6 and TNF-α trended lower. Using Steen solution significantly reduced IL-1β levels compared to DMEM (0.933 ± 0.044 pg/μg protein vs. 1.435 ± 0.142 pg/μg protein; p = 0.015). IL-6 and TNF-α trended lower as well, while IL-10 was higher, but differences did not reach statistical significance.
Cytokine and 8-Isoprostane content in liver tissue lysate postperfusion, normalized to total protein content:
The optimized protocol led to lowest amounts of oxidative stress
8-Isoprostane as a marker for reactive oxygen species (ROS) production did not show a clear correlation with one specific treatment. However, all groups with the maximum dosage of epoprostenol consistently displayed low values (Fig. 4E). The tissue content of 8-Isoprostane varied significantly between groups, with the highest values in the E250|G+ group (0.3472 ± 0.0235 pg/μg protein), while the lowest values were seen in the Steen group (0.123 ± 0.013 pg/μg protein). While not statistically significant, the Steen group also trended lower than its DMEM counterpart (0.152 ± 0.022 pg/μg protein).
No relevant edema formation was seen with either protocol
On average, livers perfused with DMEM or Steen gained weight after 6 h of perfusion, but no difference could be seen between the two (Supplementary Fig. S1B). Upon comparison of dry-to-wet weight ratios of both perfused groups to a set of native rat livers, no statistically significant difference was observed (Supplementary Fig. S1C).
Discussion
NEVLP has quickly evolved from being an emerging technology to becoming established in clinical practice. Due to ethical and logistical challenges in conducting basic research with human organs, the development of an animal model that most accurately recapitulates the clinical environment remains imperative. Currently available small animal models lack standardization, often requiring protocols that differ heavily from clinical conditions and almost exclusively perfuse livers solely through the portal vein.14–16,24,30–32 Our goal was to create an easily translatable, yet simple, rat NEVLP model that closely resembles currently used clinical NEVLP systems and would permit high-throughput testing of different interventions.
We chose a dual-vessel system, as our previous work showed it to be superior compared to single-vessel perfusion, 13 and given that this is done clinically. We systematically investigated the dose–response relationship of epoprostenol and identified the ideal concentration of this clinically used vasodilator in our rat model that most consistently kept hepatic arterial pressures in physiological range. This dose represents a multiple of the one commonly used in human NEVLP. 21 High perfusion pressures were associated with increased levels of transaminase secretion in the perfusate and compromised histological integrity of the liver. This could likely be explained by endothelial cell damage, indicated by TUNEL staining, as well as through macroscopically visible intraparenchymal bleeding in groups without sufficient pressure control. Optimizing vasodilation is therefore an essential part of adequate perfusion.
Furthermore, higher doses of epoprostenol reduced markers of hepatocellular damage, independent of the vasodilatory effect. Although this cytoprotective effect is known, 33 a dose-dependency in a liver perfusion setup has not been shown before. No adverse effect was observed with higher doses of epoprostenol. Other vasodilators with similar anti-inflammatory effects could have potential advantages over epoprostenol, 19 but have yet to be established in clinical use. While not a clinical standard, glycine has been proven to ameliorate organ perfusion conditions in a previous single-vessel perfusion setup. 14
In this dual-vessel perfusion study, glycine also decreased markers of cellular damage, but adversely affected hepatic arterial pressure and thus increased the need for vasodilation. This effect has not been described yet and may be traced back to NMDA-co-agonism of glycine on smooth cells of the arterial wall, which triggers arterial spams. 34 Due to its overall beneficial effects, however, glycine could be incorporated as a standard additive in liver perfusion, although its potential increase of arterial pressure must be considered. As interactions like these may also occur with drug combinations, this serves as another reason to establish clinically relevant dual-vessel models for further pharmacological research during NEVLP.
Steen solution improved transaminase secretion compared to DMEM, possibly through reduction of inflammatory signaling and ROS production. As the exact composition of Steen solution is not communicated, the underlying mechanism remains speculatory. Steen consists of 70 g/L human serum albumin (HSA) and an unknown concentration of dextrane-40 at physiological salt concentrations. 26
In a study by Pagano et al., simply substituting HSA to phosphate-buffered saline did not achieve the same reduction of proinflammatory cytokines or ROS markers in cultured endothelial cells as using Steen. They postulated that the underlying mechanism is a reduction of NADPH oxidase activity, especially subtype NOX2, 35 which is expressed by Kupffer cells and hepatocytes. 36 This explanation seems consistent with our finding of minimal ROS production in the optimized Steen-based protocol. Another group recently examined different perfusion media in a porcine NEVLP model, where Steen solution achieved best results in protecting endothelial cells. This effect, possibly attributable to the dextrane content of Steen, 37 was correlated with lower levels of necrosis, lower levels of post-transplant lactate, and increased overall survival. 38
Common rat models of NEVLP use plasma as a colloid expander,13–15,25 and in a recent clinical trial, Liu et al. reported generally favorable outcomes using plasma as an additive. 39 In our study, the combination of DMEM and plasma performed worse than Steen solution alone. This may be caused, in part, by constituents of humoral immunity in plasma that aggravate inflammatory processes. The supposed primary benefit of Steen—protection against edema formation—does not seem to be a factor in the small animal model, as no relevant edema formation was seen with either base perfusion solution.
Steen solution should be considered a standard for optimal organ perfusion in rat NEVLP, although DMEM and plasma may be considered a more cost-effective alternative for basic research. The high bicarbonate content of MultiBic provided excellent buffer capacity, maintaining perfusate pH closer to physiological range than dialysates previously used by our group.13,14 Across all groups, TNF-α levels in liver tissue were halved compared to previously published data from a single-vessel protocol. 14 Cytokine kinetics are a complex process and dependant on multiple factors, as the half-life times of these molecules are extremely short. Ischemia and reperfusion elicit an inflammatory effect, that is on the one hand associated with cellular damage to organs, but on the other a necessary stimulus for regenerative processes.
Of the cytokines measured in this study, the fastest kinetics are considered to be IL-1β and TNF-α, while IL-6 and IL-10 react slower and stay elevated for longer. 40 Since cytokines were only measured from tissue after 6 h of perfusion, no argument in terms of kinetic profiles can be made. Possibly, the significantly higher levels of IL-1β in the E2000|G+ group compared to the E0|G− group may be due to an earlier increase in IL-1β and a subsequent earlier drop at the time of measurement. In the E2000|G+ group, due to less cellular damage, the immune response may be delayed so that the peak falls into the measurement window. This hypothesis would be consistent with the findings of Baier et al., who found IL-1β levels in rat liver tissue after IRI to decline at 6 h after an initial peak. 41
Using Steen instead of DMEM seems to have the tendency to decrease proinflammatory cytokine release overall, so the significantly lower levels of IL-1β might be considered a marker of overall lower inflammation. To further investigate this hypothesis, regular measurements of relevant cytokines in the perfusate should be considered in follow-up studies. Lactate clearance, considered one of the most relevant parameters for assessment of liver graft quality clinically, was not consistently seen. However, this phenomenon is common in small animal models.16,42–44 The greater perfusate-volume to liver weight ratio compared to human or porcine liver perfusion may be a contributing factor, as erythrocytes are a large source of lactate production. The clinical threshold, usually considered to be around 1.7–2.5 mM after 2–4 h of perfusion, 45 is therefore not necessarily relevant for our model.
In considering the goal of simulating clinical NEVLP devices and conditions, our study has several considerations that warrant mention. The most notable limitation is the absence of a group that uses the optimal vasodilatory dosage (2000 ng/h epoprostenol) and Steen without glycine as we only investigated the optimal composition of additives and vasodilation with Steen instead of repeating all experiments. This decision was made due to cost, and to adhere to the 3R principles. Furthermore, even though longer perfusion periods have been described in human trials, we perfused rat livers for only 6 h, which seems to be the viability limit for subsequent transplantation in rat NEVLP models.15,32,46
We also opted to use a dialysis membrane, which is currently not performed in human or porcine NEVLP. Once more, this was most likely necessary because of a greater ratio of perfusate volume to liver weight in this model, which leads to significant accumulation of potassium and urea over the course of perfusion if dialysis is not utilized.14,15 The use of a dialysis membrane might influence the predictive value of lactate and glucose, as well as the pH in our system. However, the effect of a dialysis membrane on the interpretation of lactate clearance seemed to be negligible, since lactic acid only passes the dialysis membrane slowly. 47 Despite these limitations, besides the applicability of our rodent NEVLP perfusion system for transplantation research, it may also be used as a whole-organ perfusion model for pharmacological research with the premise of reducing animal harm in accordance with the 3R principles.
We herein report a meaningful and reproducible rodent NEVLP system, which has been designed as a platform to promote basic research. The optimized perfusion protocol closely mimics clinical NEVLP protocols and demonstrates the least amount of hepatocellular damage, oxidative stress, and cytokine surge. Importantly, application of this protocol will potentially enable rapid testing of novel therapeutics for the reconditioning of marginal liver grafts.
Footnotes
Acknowledgments
The authors would like to thank Dr. rer. med. Anja Reutzel-Selke and Dr. rer. nat. Jörg Mengwasser for their methodological and general scientific support.
Authors' Contributions
Writing of the original article was done by F.S. Conceptualization was performed by J.M.G.V.G., M.S.P., N.R., and F.S. Methodology and supervision were provided by J.M.G.V.G. and N.R. F.S., J.M., J.M.G.V.G., V.M., K.K., and M.Z. were involved in conducting the investigations (operations, experiments, and laboratory analyses). Formal analyses and visualization were performed by F.S. and S.M. Resources and funding were provided by N.R., I.M.S., and J.P. M.S.P. provided proofreading during the revision process as requested. All authors were involved in reviewing and editing of the article.
Disclosure Statement
All authors have read the journal's authorship agreement and policy on potential conflicts of interest and concluded that there were no relevant conflicts of interest to declare.
Funding Information
This work was funded by institutional financial support of the Charité–Universitätsmedizin Berlin and by the German Research Foundation (grant number: RA 3044/3-1). S.M., N.R., and J.M.G.V.G. are participants of the BIH Charité Clinician Scientist Program funded by the Charité–Universitätsmedizin Berlin and the Berlin Institute of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.