
Abstract
An essential aspect of cardiovascular in situ tissue engineering (TE) is to ensure balance between scaffold degradation and neo-tissue formation. We evaluated the rate of degradation and neo-tissue formation of three electrospun supramolecular bisurea-based biodegradable scaffolds that differ in their soft-block backbone compositions only. Scaffolds were implanted as interposition grafts in the abdominal aorta in rats, and evaluated at different time points (t = 1, 6, 12, 24, and 40 weeks) on function, tissue formation, strength, and scaffold degradation. The fully carbonate-based biomaterial showed minor degradation after 40 weeks in vivo, whereas the other two ester-containing biomaterials showed (near) complete degradation within 6–12 weeks. Local dilatation was only observed in these faster degrading scaffolds. All materials showed to some extent mineralization, at early as well as late time points. Histological evaluation showed equal and non-native–like neo-tissue formation after total degradation. The fully carbonate-based scaffolds lagged in neo-tissue formation, presumably as its degradation was (far from) complete at 40 weeks. A significant difference in vessel wall contrast enhancement was observed by magnetic resonance imaging between grafts with total compared with minimal-degraded scaffolds.
Impact statement
An essential aspect in successful in situ tissue engineering is to equilibrate tissue formation and scaffold degradation. Too slow as well as too fast degradation of biodegradable scaffolds can be harmful to our patients. We demonstrated the impact of electrospun vascular scaffold materials with varying ester contents on then degradation susceptibility in vivo and tissue formation. The new insights presented in this study contribute to correct the decision-making on scaffold materials for our patients.
Introduction
I
Electrospun synthetic scaffolds of supramolecular biodegradable polymers are promising candidates for in situ TE of cardiovascular constructs, because their features are highly tunable, either chemically (e.g., nature of the used material), physically (e.g., strength, elasticity), or morphologically (e.g., shape of constructs).1,2
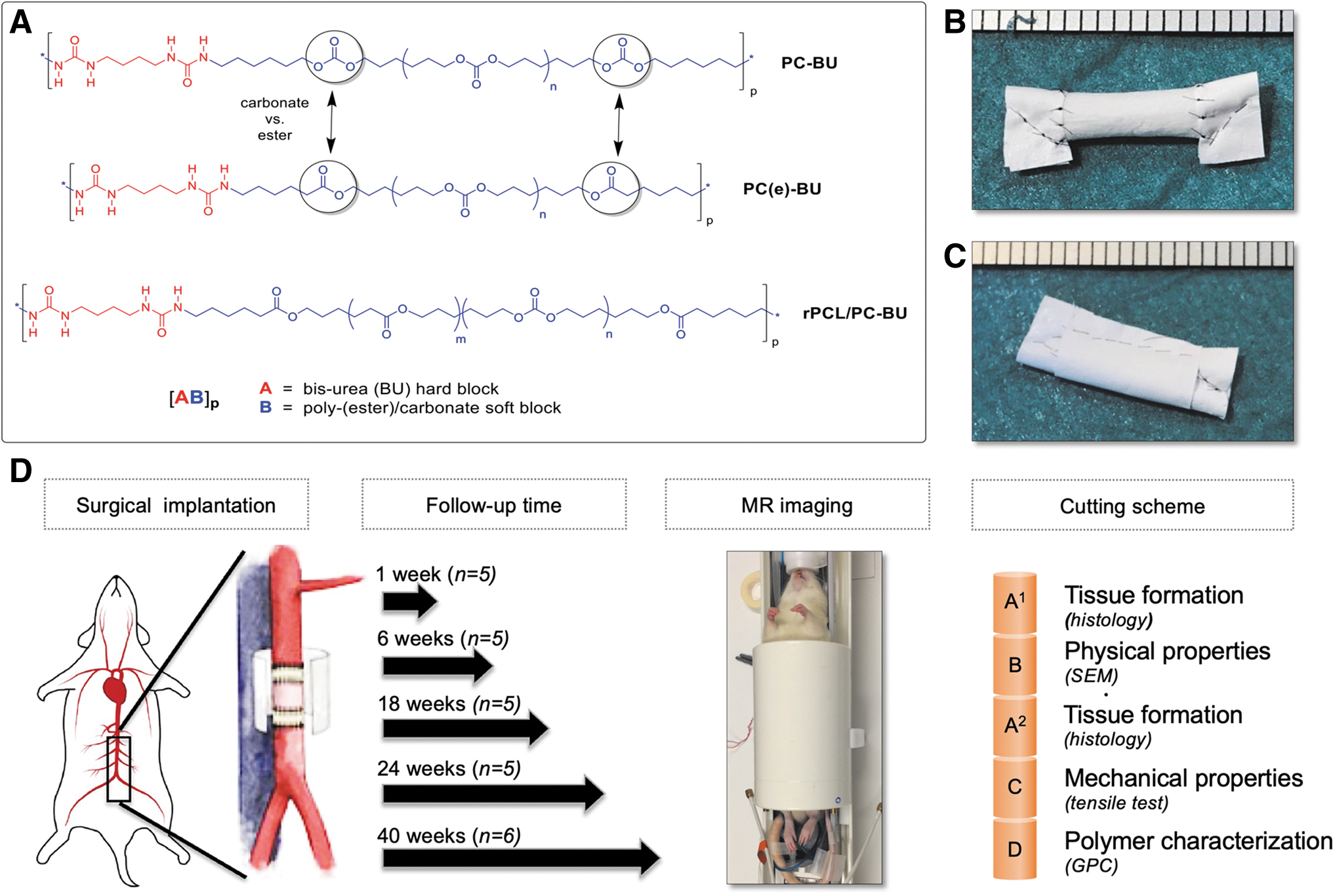
Our previous insights in pulmonary heart valves showed that polycaprolactone-bisurea (PCL-BU) scaffolds degraded too fast, whereas polyhexylcarbonate-bisurea (PC-BU) scaffolds were still present 1 year after implantation.3,4 In an attempt to balance scaffold degradation rates, we here introduce two scaffold materials with rate of degradation profiles intermediate to those of PCL-BU (100% ester groups) and PC-BU (100% carbonate groups). Polyhexylcarbonate-ester-bisurea (PC(e)-BU) and random-polycaprolactone-polyhexylcarbonate-bisurea (rPCL/PC-BU) differ from PCL-BU and PC-BU in their ester and carbonate content only. All these scaffold materials are the same with regard to their hard block bisurea (BU) moieties, but are different with respect to their soft block backbones (i.e., level of carbonate/ester content).
The developed BU-based biomaterials have a well-defined sequence-controlled molecular architecture with strictly alternating hard and soft blocks. This feature imparts a highly elastomeric nature to these polymers, suitably mimicking the elastic character of cardiovascular tissues, particularly those of heart valves or vessel walls.
Previous in vitro analyses of a series of scaffolds electrospun from PC-BU, PC(e)-BU, and PCL-BU materials showed that (small) changes in the macromolecular structure led to significant differences in observed degradation kinetics. 5 These in vitro experiments give a valuable initial comparison between biomaterials of interest, but they cannot give all-encompassing results as in vitro tested grafts do not truly become exposed to a heterogenic, dynamic, and complex in vivo environment that exists inside an organism. 6
In this study, we have implanted vascular grafts—PC-BU, PC(e)-BU, and rPCL/PC-BU—in the abdominal aorta in a rat model and evaluated graft functionality, scaffold degradation, and neo-tissue formation after 1, 6, 12, 24, and 40 weeks.
Materials and Methods
For details of the method see Electronic Supplementary Information (ESI).
Vascular grafts
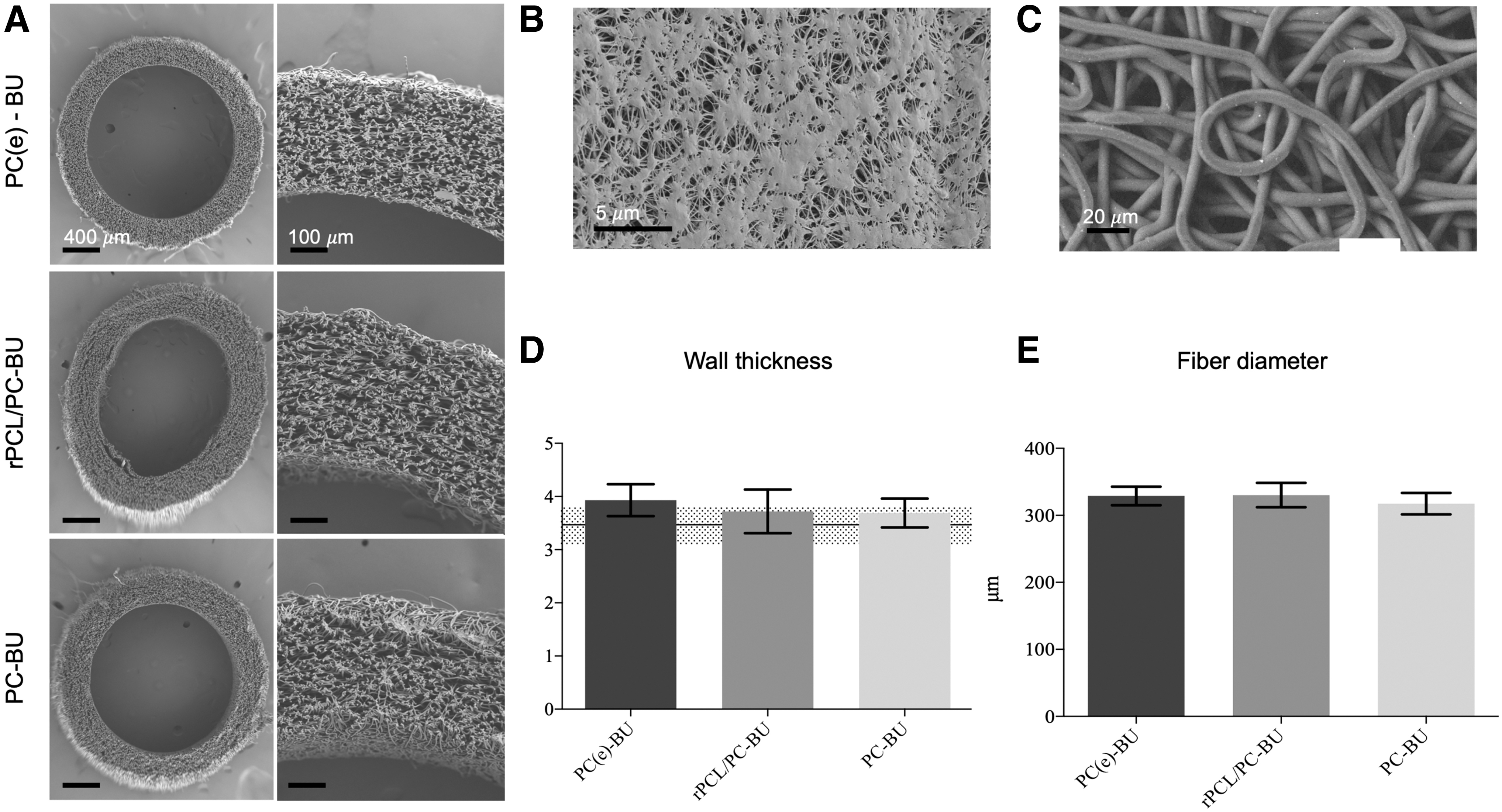
PC-BU and PC(e)-BU were synthesized as previously described,3,5,7 and rPCL/PC-BU as described in ESI. Tubular scaffolds (2 mm inner diameter, 10 mm length, wall thickness 326.1 ± 16.5 μm) grafts were fabricated using a fully climate-controlled EC-CLI electrospinning machine (IME Technologies, Waalre, Netherlands; Fig. 1). Average fiber diameters (micrometer) and pore sizes (square micrometer) were quantified on two representative electron microscopy images per specimen with at least n = 30 measurements on randomly selected fibers/areas using the ImageJ software (U.S. National Institutes of Health, Bethesda, MD). To prevent transanastomotic and transmural cell ingrowth the vascular scaffolds were shielded with low-porosity 0.1-mm-thick expanded polytetrafluoroethylene (ePTFE; Gore, PRECLUDE®; also known as Gore-Tex) before implantation 8 (see ESI Fig. SI-10).
Scaffolds before implantation.
In vivo experiments
All animal experiments were approved by the Medical Center Animal Ethics Committee (Netherlands) on April 3, 2017 (AVD118002017844) and conform to the guidelines for the use of laboratory animals, as formulated by the Dutch Law on animal experimentation and performed according to the previous study. 8 Randomization, blinding, and surgical details are presented in the ESI. All animals received pre-, peri-, and postoperative analgesics. For details see ESI.
Each experimental group comprised 26 animals, which were scheduled for a follow-up of 1 (n = 5), 6 (n = 5), 12 (n = 5), 24 (n = 5), or 40 weeks (n = 6). At the end of follow-up, the animals underwent magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) under full anesthesia. Next the grafts were explanted in toto and the Gore-Tex was removed. A distal and proximal segment of the native abdominal aorta was collected. The explanted graft was sectioned conform a standard cutting scheme to provide, resulting samples A 1 , A2, B, C, and D as schematically shown in Figure 2.
Implantation materials, procedure and experimental groups.
Experimental readouts
The scaffold fiber morphology was examined by scanning electronic microscopy (SEM). Circumferential mechanical properties of the explanted graft and of at least two nonimplanted controls were characterized using uniaxial tensile tests. “From the stress-strain curves, the tangent moduli were determined in the low-strain (5%) and high-strain (10%) regimes.” Gel permeation chromatography (GPC) was used to determine number averaged molecular weights (Mn) and weight averaged molecular weights (Mw), both relative to polyethylene glycol standards. Vessel patency was evaluated using in vivo MRI scans just before explantation on a preclinical 7.0T MRI scanner. Grafts were defined as patent in case the lumen area was at least 50% compared with their initial reference values. In addition, scaffold contrast-enhancement (sCE) values were determined by calculating the ratio between 15 min postcontrast and precontrast signal intensities within the graft.
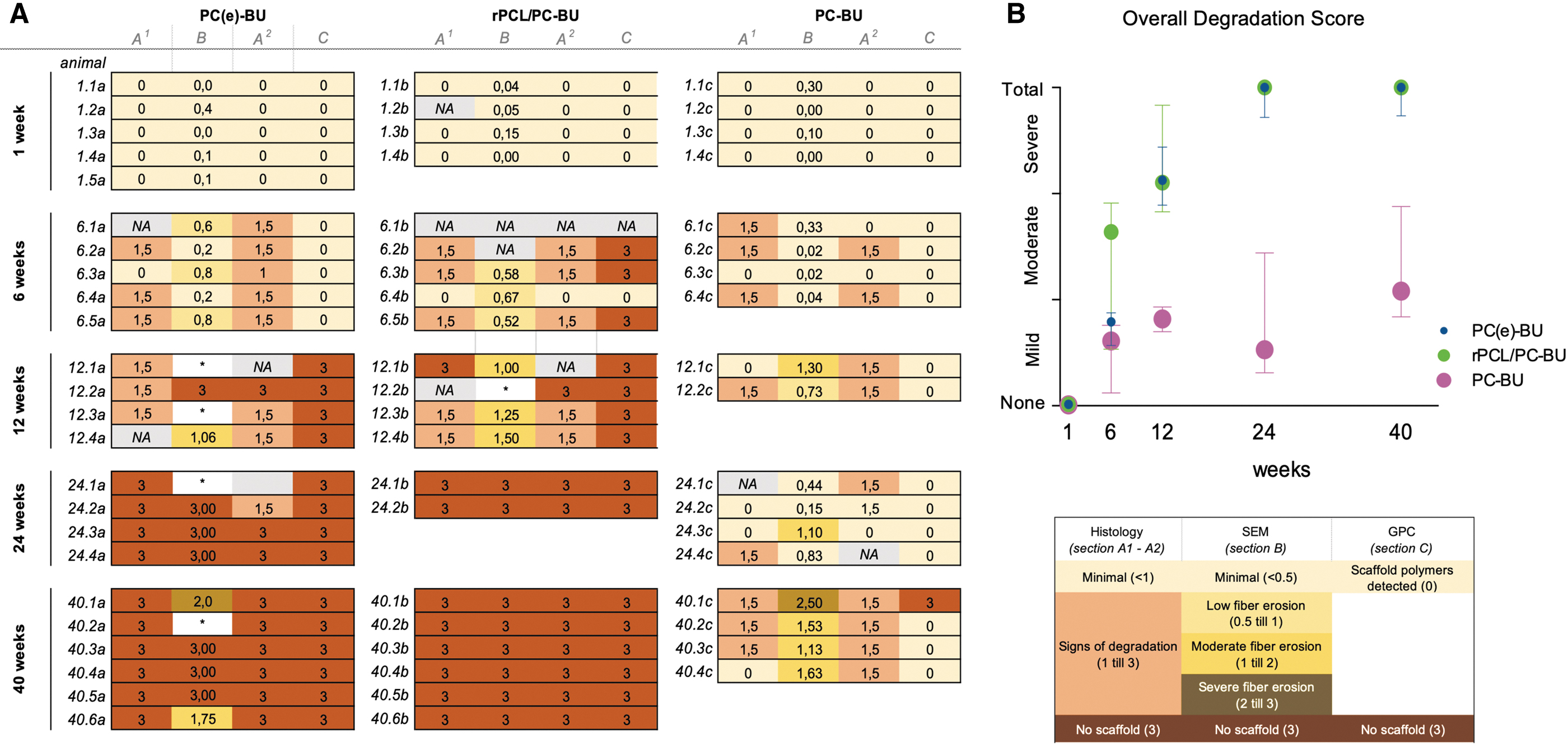
Tissue formation was evaluated with histology. Qualitative analyses were performed by two reviewers (MU and A.v.d.W.) who were blinded regarding the studied scaffold type. To gain an overall insight on the level of degradation we first calculated the degradation score (DS) of each graft by taking the mean of the scores of four graft segments (A 1 , B, A2, and D from proximal to distal, respectively). Subsequently, we calculated the overall DS (ODS) for each material [PC(e)-BU, rPCL-BU, or PC-BU] at each time point (1, 6, 12, 24, or 40 weeks). To calculate the DS, three segments of each graft were scored qualitatively by histological (A 1 and A2) and SEM (B) images and one segment was scored quantitatively by GPC (D). Because the temporal degradation of the three materials is mainly characterized by fiber morphological changes, we preferred DS scoring over, for example, temporal porosity changes of the scaffolds. The qualitative histology and SEM assessments were performed by two reviewers (both blinded for the polymer material type), by using a predefined scoring system using reference images (see ESI). The Cohan's kappa was calculated to measure the observer agreement and showed agreement >60%.
The histological slides of one hematoxylin and eosin (HE) and one picrosirius red (PSR) staining were scored on the amount of scaffold degradation (visible as transparent or yellowish areas). For each explanted graft the HE and PSR-stained slides were analyzed using their proximal (A 1 ) and middle (A 2 ) sections. Each slide was scored using the following categories: no sign of degradation (0 points), signs of degradation (1 point), and total degradation (3 points). In case of disagreement, a third reviewer was consulted to reach a common agreement.
Fiber erosion of each graft was analyzed by SEM images (1.00 kx magnification) and was performed by two reviewers (both blinded for the material type), who used references images for rating (see ESI). For each graft three images were analyzed and scored on 4 regions of interest (ROI). Each ROI was scored as follows: minimal signs of degradation (0.5 points), signs of degradation (1 point), and total degradation (3 points). The mean (±standard deviation [SD]) score for each graft was calculated by all the ROIs of the two reviewers. In case of disagreement (mean score difference >0.5 points) a third reviewer was consulted to reach common agreement.
GPC analysis was used to identify the presence of scaffold polymers in the explanted graft (0 points) or the absence of polymers in the graft (3 points, indicates total degradation).
The DS of each graft was calculated by taking the mean of the scores of the four segments. Subsequently, the ODS for each material at 1, 6, 12, 24, or 40 weeks was calculated by the median and (25–75%) interquartile ranges (owing to non-normal distribution). For readability reasons the median scores between 0 and 1 are presented as mild, 1–2 as moderate, and 2–3 as severe signs of degradation. Statistics were performed, in case a minimum of four samples per measurements were available with GraphPad.
Results
Electrospun vascular scaffold materials with varying ester contents differ in susceptibility to in vivo degradation
Scaffold morphology and degradation in vitro
The overall Mw of PC-BU, PC(e)-BU, and rPCL/PC-BU are ∼34.5 ± 0.5, 52.3 ± 0.5, 63.6 ± 4.0 kDa, respectively (Table 1).
Properties of the Electrospun Vascular Scaffolds
Mw, weight averaged molecular weight; PDI, poly dispersity index.
Differential Scanning Calorimetry studies (ESI Table SI-1) and Dynamic Mechanical Thermal Analysis studies (ESI Figs. SI-3–5 and ESI Table SI-2) on the thermal and mechanical properties of the three biomaterials highlight that the materials are elastomeric, as they display a flat rubber plateau in the temperature region of interest, that is, well below and well above 37°C. In addition, the three materials show similar storage moduli at the rubber plateau ranging from E′ = 14 MPa to 17 MPa, indicating that the materials are relatively and comparably soft.
The in vitro degradation tests on thin film samples show that hydrolytic degradation by NaOH is more prone to occur for rPCL/PC-BU and PC(e)-BU than for PC-BU (ESI Fig. SI-6). The differences are even more clear when considering enzymatically catalyzed hydrolysis. Using this assay PC-BU is not affected, whereas rPCL/PC-BU and PC(e)-BU degrade upon the action of lipase (ESI Fig. SI-7). The oxidative degradation tests show no mass loss for any of the three materials. Subsequent analysis by GPC shows a decrease in Mn for PC(e)-BU and even more so for rPCL/PC-BU, whereas no significant change in Mn is observed for PC-BU (ESI Fig. SI-8).
Scaffolds
Before implantation the electrospun vascular scaffolds showed equal wall thicknesses, fiber diameters, and pore sizes (Table 1). The overall mean fiber thickness was 3.8 ± 0.13 μm, mean pore size was 738 ± 439 μm2, and the overall graft wall thickness was 326.1 ± 16.5 μm. The surface topology and porosity of the three scaffolds exhibited a micro-porous morphology enabling cellular infiltration. In contrast, the Gore-Tex sheet material is dense and therefore cannot be infiltrated by cells.
Scaffold morphology upon degradation in vivo
The ODS showed a clear difference between the three materials at 6 weeks, with mild degradation for PC(e)-BU (median [interquartile range (IQR) 25%–75%]: 0.79 [0.57–0.88]) and PC-BU (0.61 [0.12–0.76]) and moderate for rPCL/PC-BU (1.64 [0.53–1.9]; Fig. 3B). At 12 weeks rPCL/PC-BU and PC(e)-BU scaffolds showed extensive degradation (2.10 [1.83–2.83] and 2.13[1.98–2.43], respectively). At 24 and 40 weeks PC(e)-BU and rPCL/PC-BU were totally degraded. In contrast, PC-BU showed only mild degradation until the 24-week time point and mild–moderate degradation at 40 weeks (1.1[0.84–1.9]; Fig. 3A).
Scaffold degradation of PC(e)-BU, rPCL/PC-BU, and PC-BU.
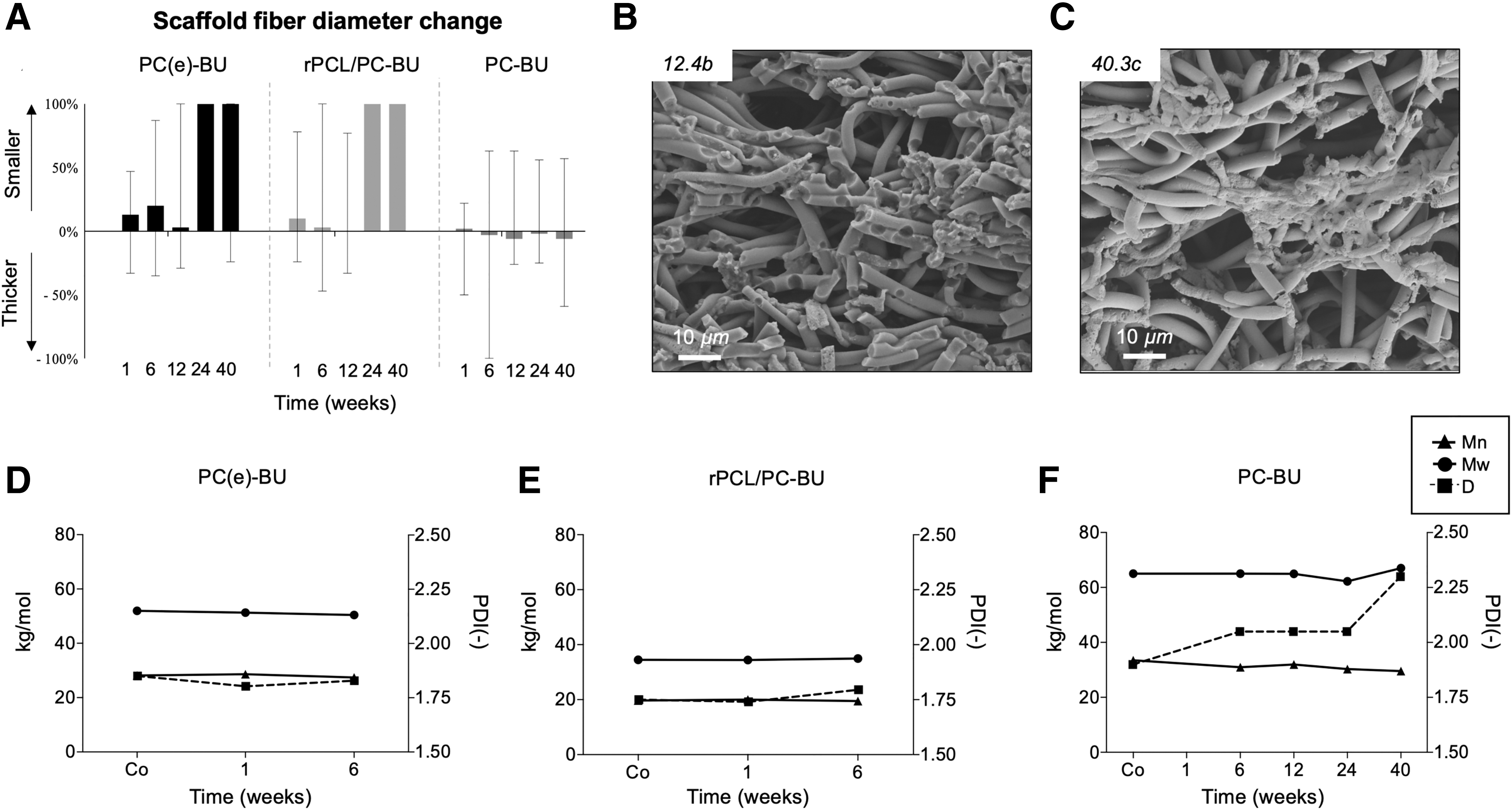
Histological evaluation of the explanted grafts mostly showed similar stages of degradation in the proximal and in the middle section. However, in six samples (n = 3 PC(e)-BU and n = 3 PC-BU) the degradation state between the sections was unequal. For example, for No. 12.1c no signs of degradation were seen proximally (score 0 on histology), whereas clear signs were seen in the middle section (score 1.5 on histology). In SEM analyses, none to minimal (mean score <0.5) superficial erosion of the fibers was seen in all materials variants at 1 week with pits and dents being visible on the fiber surface (rPCL/PC-BU: 0.10 ± 0.16; PC(e)-BU: 0.06 ± 0.06; PC-BU: 0.16 ± 0.14). At 6 weeks the rPCL/PC-BU and PC(e)-BU grafts both showed minimal to moderate surface erosion (0.51 ± 0.30 and 0.59 ± 0.07, respectively). This increased to week 12 as only one sample of rPCL/PC-BU and PC(e)-BU had remained for analysis.
In contrast, the PC-BU scaffolds showed a variation from low to moderate to severe fiber erosion at 12, 24, and 40 weeks (1.01 ± 0.40, 0.63 ± 0.49, and 1.57 ± 0.36, respectively). The average fiber diameters in PC(e)-BU and rPCL/PC-BU scaffolds gradually decreased over time, with the fibers being totally degraded at 24 weeks (Fig. 3A). In some cases, fibers were encapsulated with mineral deposits. The average PC-BU fiber diameter in vivo stayed the same, or showed minor (water) swelling, with values compared with those for nonimplant controls (1.7 ± 3.8%), diameter increase, that is, from 3.6 9 ± 0.30 μm before implantation to 3.75 ± 0.16 μm at 40 weeks. Overall, rPCL/PC-BU and PC(e)-BU scaffolds had stable molecular weights (Mw, Mn, polydispersity [PDI]) as long as the measurements were possible (up to 6 weeks), whereas the PDI of PC-BU seemed to increase slightly after 24 weeks (Fig. 4D–F). Owing to the low sample sizes, no statistics could be performed.
In vivo scaffold degradation data.
Following total degradation PC(e)-BU and rPCL/PC-BU scaffolds showed immature neo-tissue formation while PC-BU scaffolds lagged in neo-tissue formation, presumably due to incomplete degradation
Histological analyses of all scaffold material explants showed infiltration of cells (by HE). In half of the sections, we detected a homogeneous distribution of—not type specified—cells throughout the graft. In the other half of the sections, cells were unequally distributed. Specifically, local cell colonies alternated with cell-poor regions. This was seen in the proximal (38%) as well in middle (25%) sections of the grafts. Two grafts showed almost no cell infiltration at both sections [PC(e)-BU; No. 1.4a] or only at the proximal section (PC-BU; No. 1.3c). As of 6 weeks, all grafts were populated with cells. Quantitative analyses showed no statistically significant differences in cells per square millimeter count, not in time, nor in location nor per graft material (Fig. 5D).
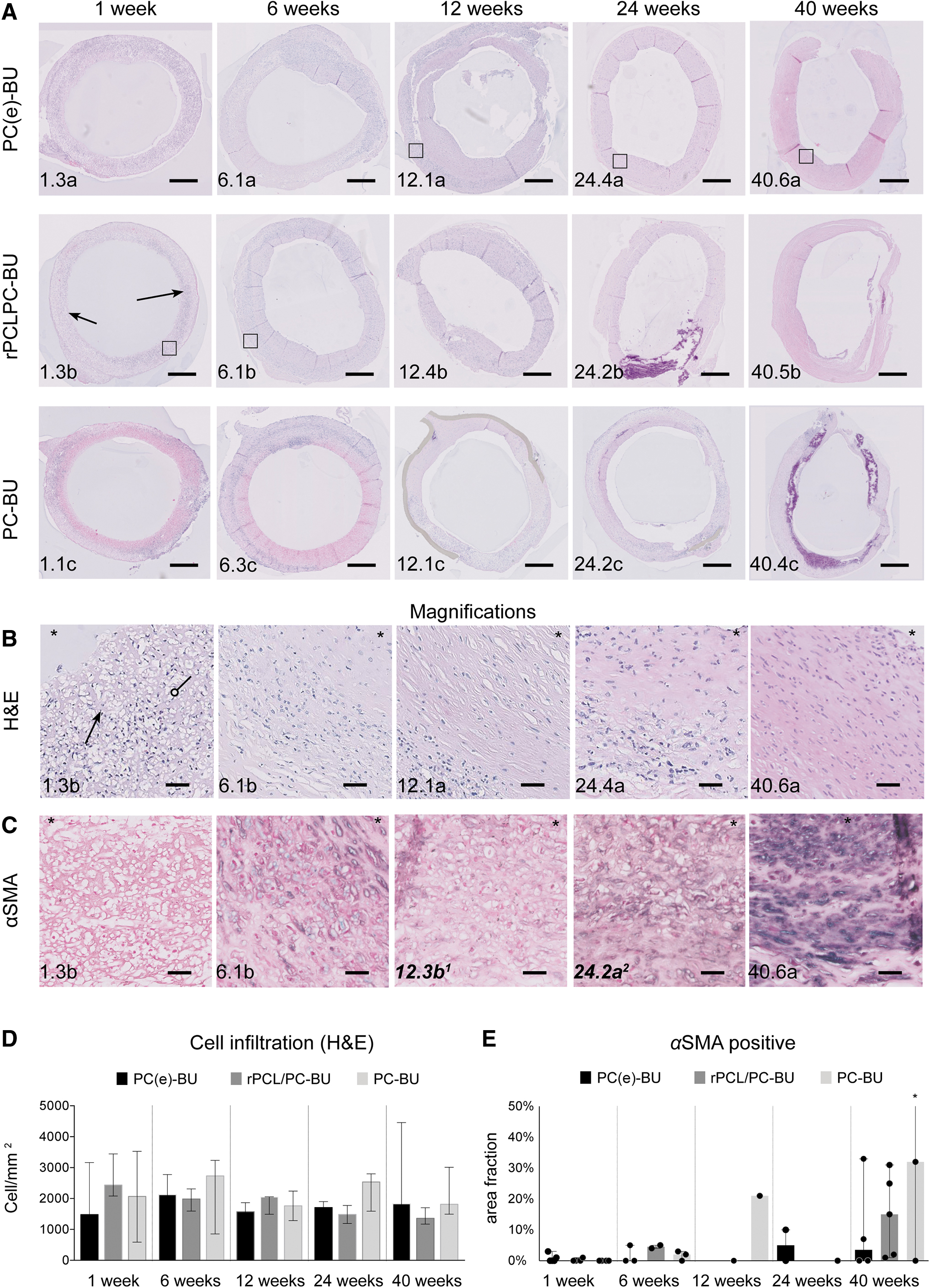
Scaffold cellularization.
After 1 week, alpha-smooth muscle actin (α-SMA) positive cells were sporadically present in low fractions (1–3%) in PC(e)-BU (2/5) and rPCL/PC-BU (1/5) grafts but were not traced in the PC-BU grafts. At later time points, inconsistencies in α-SMA–positive cell counts were seen. At each time point and in each scaffold material, some grafts were α-SMA positive, whereas others were negative. In the α-SMA–positive grafts, the fraction increased with time (Fig. 5C, E). One graft with a large thrombus showed a very high area fraction of α-SMA (No. 40.1c; mean ± SD; 76 ± 12%).
Evaluation of collagen formation revealed an increase of collagen per area in the first 3 months for all three materials (Fig. 6). Thereafter, the collagen area fraction stabilized. Owing to the small sample sizes, statistics could not be performed. However, we observed a lower area fraction of collagen in the PC-BU material at 6, 12, 24, and 40 weeks (median [IQR] 25–75% of 11.7% [8.7–19.5], 9.6% [3.0–22.3], 13.4% [2.9–19.1], 25.5% [18.9–30.7]) compared with PC(e)-BU (4.9% [1.6–17.15%], 19.5% [14.0–32.8], 31.2% [25.7–42.5], and 24.3% [21.4–35.3]) and rPCL/PC-BU (14.4% [8.0–16.0], 32.5% [16.4–42.8], 30.3% [32.2–37.7], and 29% [12.5–36.8]).
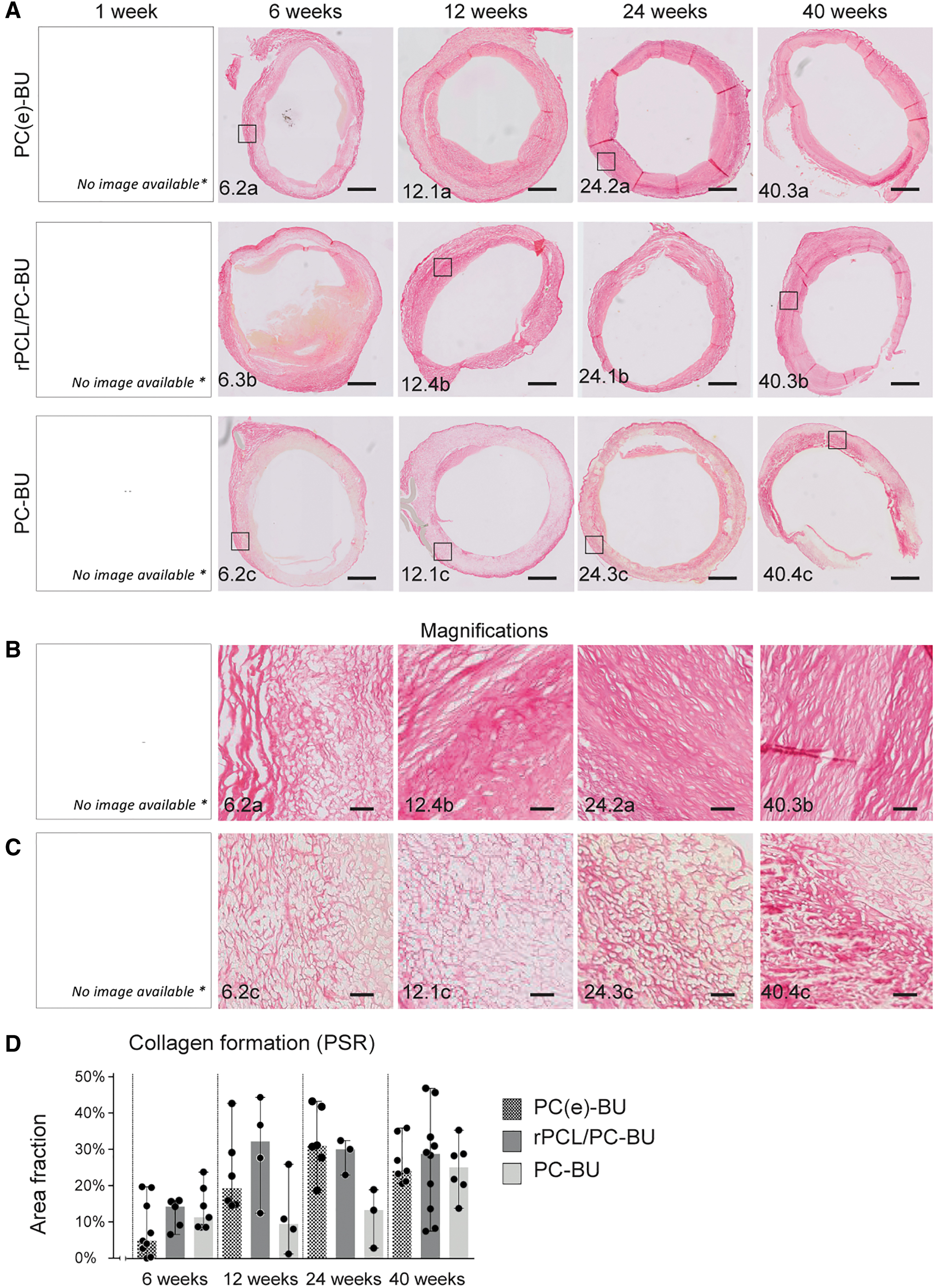
Collagen formation.
With time, the PC-BU scaffolds demonstrate an increased scaffold replacement by collagen fibers, although far from complete within the 10-month follow-up. In the samples with fully degraded scaffolds, circumferentially orientated and multilayered bundles of collagen fibers were seen. In addition, in some of these samples, loose collagen fibers with orientation toward the center of the vessel wall were observed.
At 24 weeks, fragments of elastin fibers were seen randomly distributed in the PC(e)-BU (n = 3/3), rPCL/PC-BU (n = 2/2), and PC-BU (n = 3/4) scaffolds. Similarly, immature and randomly distributed elastin fibers were present at 40 weeks in the PC(e)-BU (n = 3/6), rPCL/PC-BU (n = 1/6), and PC-BU (n = 2/4) scaffolds (Fig. 7D–F).
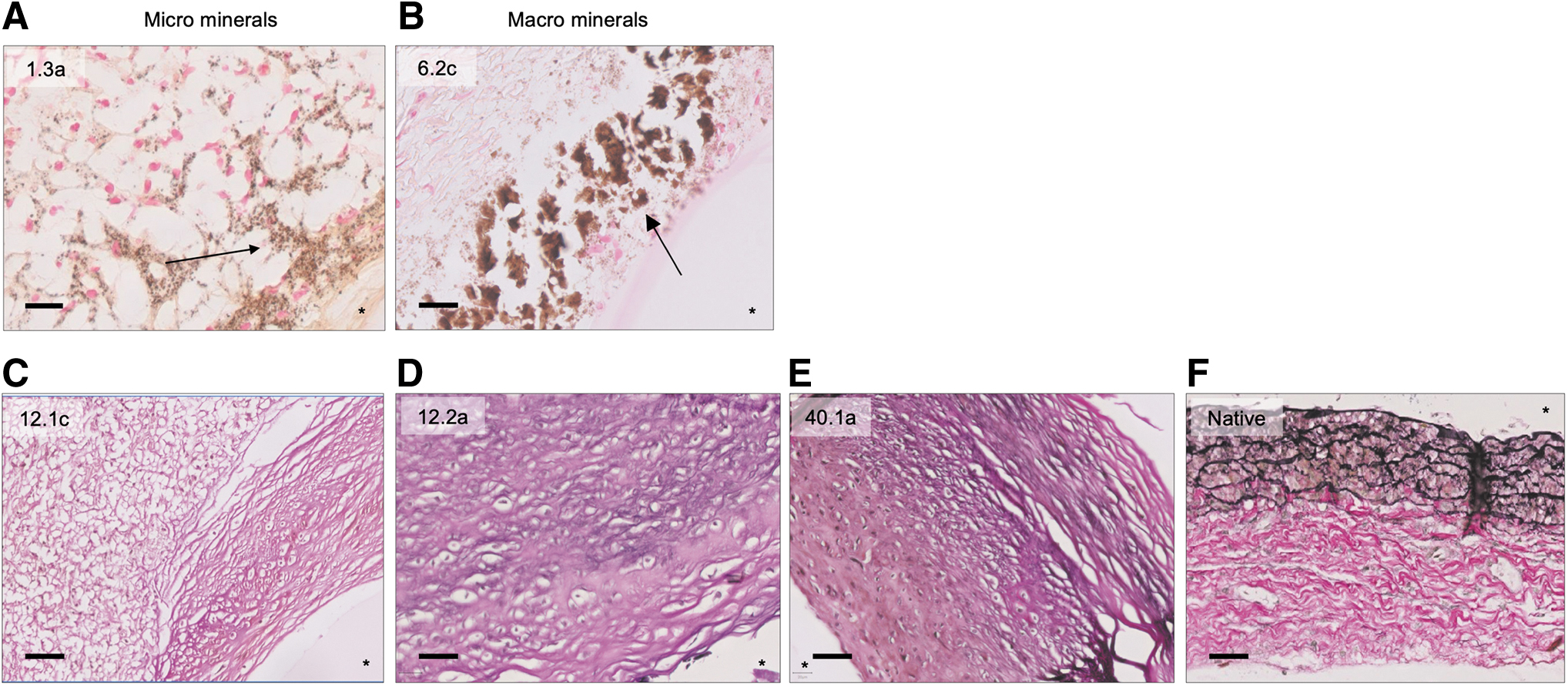
Mineralization and elastin formation. Images of minerals in the vessel wall with
CE-MRI does not correlate with scaffold DS or collagen formation
Initial simple linear regression analyses found a significant association between sCE values and ODS values (p = 0.025) and between CE and collagen area fraction (p = 0.021). However, we observed a high CE in all 1-week measurements (i.e., for all scaffolds that had not degraded and that had not displayed collagen formation), and therefore sensitivity analyses were performed to evaluate whether the found association may be owing to outcomes for this 1-week subgroup. In these analyses the ODS and the collagen area fraction were no longer found to be significantly associated with CE (Figs. 8, 9). For reference we also collected CE values for nearby native vessels (nCE) and found similar results for the sCEs and the nCEs (see ESI Figures SI-14 and 15 for details).
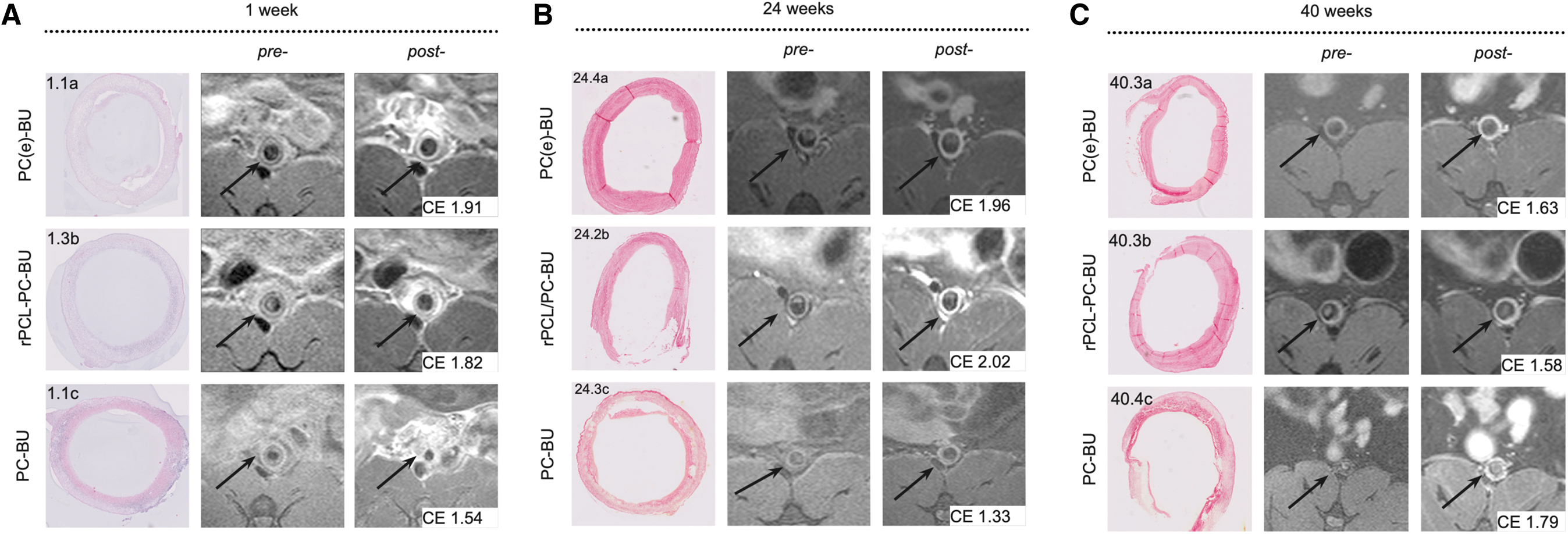
CE of implanted grafts during scaffold degradation by MRI. Representative histological images (left) at 1 week (HE), 24 and 40 weeks (both PSR; collagen staining) and the corresponding pre- and postcontrast MR images (middle and right, respectively) of the scaffold (black arrow) and the correlated CE value (bottom right corner). CE, contrast enhancement; MRI, magnetic resonance imaging; PSR, picrosirius red.

Linear regression analyses. sCE and
Adverse events occur independently of scaffold material
The overall survival of the animals was 89%, 80%, and 70% for the PC(e)-BU, rPCL/PC-BU, and PC-BU scaffolds and nonsignificantly different (ESI Fig. SI-13 and ESI Table SI-3). Necropsy of animals that died unexpectedly did not reveal any graft ruptures. Macroscopically, granulation tissue was seen on the adventitial side of the Gore-Tex sleeves.
One week after implantation, MRA evaluation demonstrated an increase of the lumen area of rPCL/PC-BU with 40% compared with nonimplanted (2 mm diameter) controls. The lumen area of PC(e)-BU and PC-BU material both increased with 17%. Because of the low sample size, significance could not be measured statistically.
MRA showed that nearly all grafts of the surviving animals were patent (not more than 50% lumen reduction) until 24 weeks. Two rPCL/PC-BU grafts (at 6 and 12 weeks) and one PC-BU graft (12 weeks) had >50% lumen reduction. One of these animals with a rPCL/PC-BU graft (No. 6.5b) showed clinical signs of graft obstruction (black tip of the tail). The MRA and termination date of this animal was brought forward to 12 days after implantation. It was found that the animal showed total occlusion of the graft and extensive collateral formation. At 40 weeks, the lumen size of three PC(e)-BU (75%), one rPCL/PC-BU (16.7%), and three PC-BU (75%) grafts were reduced by >50% in the absence of clinical signs. One PC-BU graft was totally occluded and lower limb blood supply was achieved by extensive collateral formation (Fig. 10B).
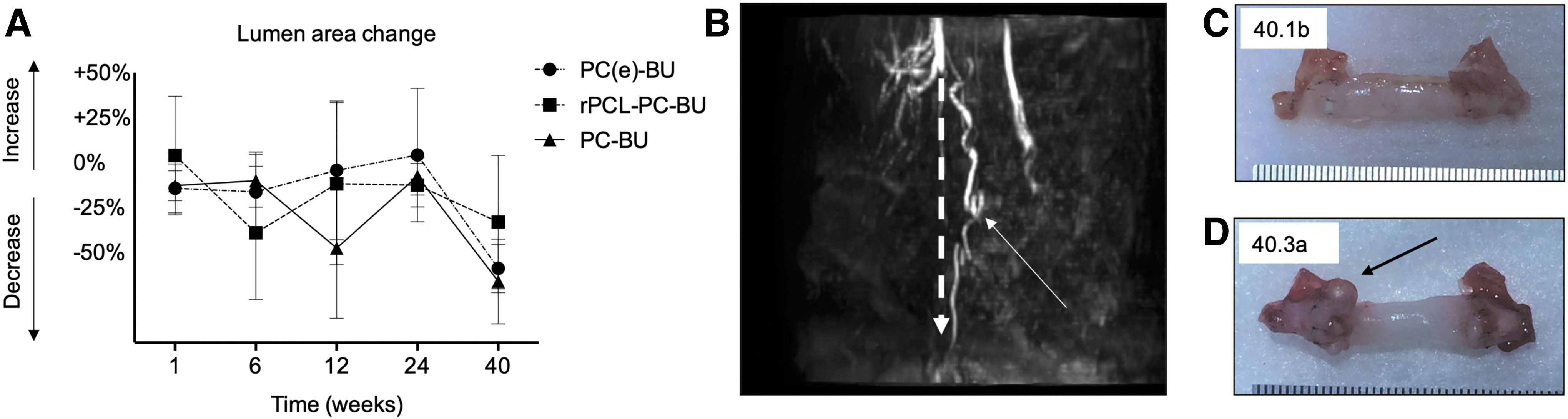
Graft patency.
Owing to the Gore-Tex shielding we could not systematically evaluate the risk of aneurysm formation. However, in some cases dilatation of the vessel occurred (Fig. 10C): at 6 weeks in one PC(e)-BU graft (25%) and three rPCL/PC-BU grafts (60%); at 12 weeks in one PC(e)-BU graft (25%); at 24 weeks in one rPCL/PC-BU graft (50%); and at 40 weeks in one PC(e)-BU graft (16.7%) and two rPCL/PC-BU grafts (33%). None of the PC-BU grafts showed dilatation at any timepoint.
The results of the elastic moduli are presented in the ESI (ESI Fig. SI–S16).
Histological evaluation showed mineralization deposits of different sizes for all three materials. At 7 days, one PC(e)-BU and one PC-BU graft showed microsized deposits, which were located as a single or as multiple clusters in the vessel wall (Fig. 7A). At later timepoints, the deposit sizes increased and/or the deposits merged into larger areas (0.5–1.0 mm2; Fig. 7B). After 6 months, all three materials showed some samples with mineral deposits in different sizes (Fig. 11). Remarkably, for the rPCL/PC-BU scaffolds, mineral deposits was only observed as of 24 weeks, so well after this material had fully degraded.
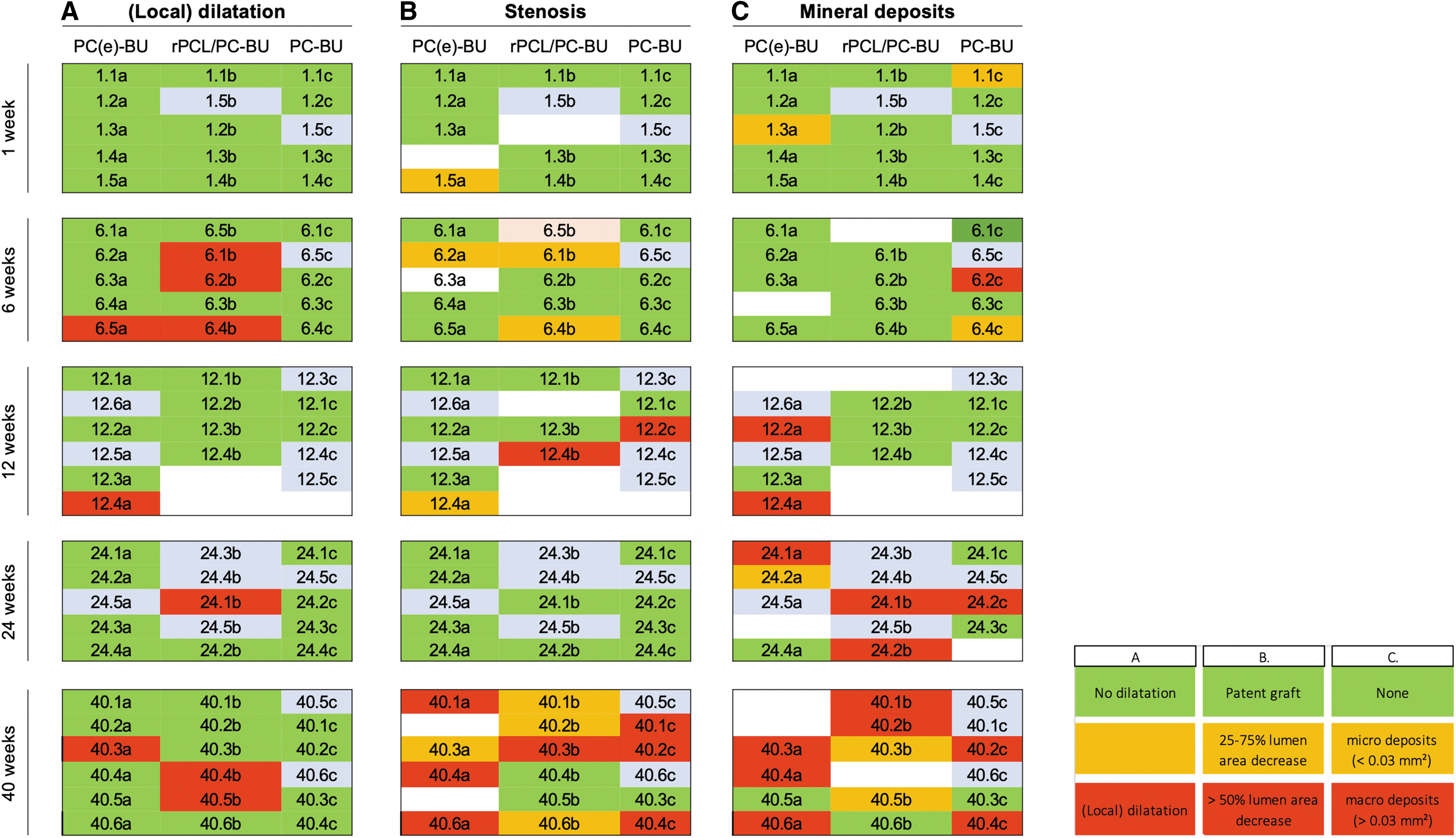
Functional outcome for all individual grafts.
Discussion
We evaluated the balance between the rate of degradation and neo-tissue formation of three biodegradable vascular scaffolds in the complex in vivo environment (rat model) over a period of 40 weeks. Two vascular graft materials with varying levels of ester-bonds in their soft-block backbones [PC(e)-BU and rPCL/PC-BU] were compared with the 100% carbonate-based PC-BU material that has shown slow degrading properties when used as pulmonary heart-valve implant in sheep.
We demonstrated extensive degradation of rPCL/PC-BU scaffolds at 6 weeks followed by the PC(e)-BU scaffolds at 12 weeks. The PC-BU implants only showed minimal-to-moderate degradation during the 40-week follow-up. Remarkably, the in vivo rate of degradation of rPCL/PC-BU (30% ester bonds) and even PC(e)-BU (12% esters only) was not that much different from that observed for PCL-BU (100% esters).9,10 Apparently, even when the ester-bonds are positioned next to the crystallized BU hard blocks—as they are in the PC(e)-BU scaffolds—they remain quite susceptible to hydrolysis, presumably enzymatic hydrolysis. This can only be assessed and validated using solid in vivo data. We observed a variation in degradation velocities within the groups.
This variation is not uncommon in (in situ) tissue engineering as TE is a multidynamic process.11–13 The extent of macrophage-driven degradation depends on the prevailing mechanical conditions (e.g., shear stress, cyclic strains). In vitro it has been shown that conditions of moderate cyclic stretch have an inhibitory effect on the macrophages secretory profile in PCL-BU scaffolds and that static conditions increase the degradation rate. In this study, our scaffolds were surrounded by Gore-Tex that has an elastic modulus about 34 MPa 14 and that thus is substantially stiffer than the bare biomaterial scaffolds (range 0.3–0.7 MPa; ESI Fig. SI-16). The Gore-Tex sheets were (loosely) layered around the vascular scaffolds with the intention to avoid mechanical support of the vascular scaffolds. However, the sheets may to some extent have restricted the distensibility of the graft to varying degrees, leading to (local) variations in degradation.
The variation in results can also be the consequence of the noncontrollable differences between individual animals. The effect on regeneration processes owing to such differences have hardly been investigated but are highly relevant for the future clinical scenarios in which patients may vary to a great extent owing to, for example, comorbidities.
Overall histological evaluation of the grafts showed equal collagen formation for the two ester containing biomaterial scaffolds at week 24, whereas PC-BU lagged in collagen formation. Independent of the materials degradation rate or stage, we detected immature and randomly distributed fragments of elastin fibers in some explants. Elastin formation is still an unmet challenge but a fundamental factor in in situ vascular TE, as it plays both a mechanical and cell-signaling role in blood vessels. 15 It provides elasticity and resilience; it prevents adhesion of platelets and leukocytes and inhibits smooth muscle cell proliferation.16,17 Although elastin fibers are reported in multiple studies on in situ TE, the newly synthesized elastin fibers are noncontinuous and loose fibers rather than lamellar structures.8,15,18
The used Gore-Tex model is not designed to systematically evaluate dilatation or aneurysm formation. Nonetheless, we observed six explants of the fast-degrading rPCL/PC-BU and three of the PC(e)-BU scaffolds with (local) dilation, for both materials already within 6 weeks of implantation. In contrast, the PC-BU scaffolds did not show dilatation. However, the PC-BU scaffolds were not totally degraded within the study period. Consequently, we cannot rule out dilation after total degradation of the PC-BU scaffolds. Even longer follow-up periods are needed to evaluate if formed neo-tissue in the PC-BU grafts will be strong enough to allow systematic circulation after full PC-BU degradation.
Multiple studies have reported on the benefits of fast degrading scaffolds in view of avoiding (risks of) calcification.19–21 It is suggested that adverse events are related to the prolonged foreign immune reaction to remaining scaffold fibers or to mismatches between dimensions of implants and native vessels (i.e., compliance mismatches). Although studies showed a reasonable and well-substantiated relationship between degradation rate and calcification, these studies often involved shorter follow-up periods and/or scaffolds that were not totally degraded.21,22 For example, Mugnai et al. studied biodegradable PCL scaffolds and (nondegradable) ePTFE vascular grafts for 18 months. 23 No aneurysmal dilatations were found in either group. Of importance, the PCL scaffolds were not fully degraded and showed calcification, although to a lesser extent than observed for the ePTFE grafts. Similar results were seen in the study of Zhao et al. They examined the performance of PCL/fibrin versus PCL grafts in vivo using nanofiber structures. 20
The PCL/fibrin grafts had a faster rate of degradation than the PCL grafts, but were nevertheless not fully degraded (35 ± 3.5% remaining material after 9 months). The PCL/fibrin grafts showed no dilatation and less calcification than the PCL grafts. On the contrary, Duijvelshoff et al. found total scaffold degradation, aneurysm formation, and calcification to appear together. 12 These results are generally more in line with findings in this study. Duijvelshoff evaluated PC(e)-BU in electrospun bilayered scaffolds—containing a porous inner layer to allow for cellular infiltration and a dense outer layer to provide strength—as small vascular grafts in a nonshielded abdominal aorta rat model with a follow-up of at maximum 5 months. Most explants exhibited aneurysmal changes with a large interindividual variation in overall appearance.
After 3 months, the scaffolds were totally degraded (note: this seems to be faster than observed for the Gore-Tex shielded single-layered PC(e)-BU grafts studied in this work), but explants nevertheless showed calcific deposits randomly in time and location. We observed mineral deposits independently of the material variation. As vonKossa staining cannot distinguish between phosphate and calcium deposits, further research needs to be carried out to distinguish between these two. The first (micro)deposit was already seen at 6 weeks in slow (PC-BU) as well as in faster (PC(e)-BU) degrading scaffolds. At the latest two time points, all three BU-based materials showed noduli to some extent. Of interest, for rPCL/PC-BU we only found mineral deposits in explants in which the material had fully degraded already, that is, minerals seemed to occur or onset without synthetic material present.
These results indicate that a prolonged foreign immune response owing to scaffold remnants is not the only mechanism that contributes to calcification. Several other factors are mentioned to be related to calcification, such as specific scaffold characteristics (e.g., pore sizes), the anatomical location of the implant, vessel compliance mismatches, and related flow/shear stress conditions. In the study of Sologashvili et al., a difference in calcification rate between high- and low-compliant grafts was observed. 24 Their carotid explants were well endothelialized with early cellular infiltration, showed less intima hyperplasia, and less calcification compared with the grafts implanted in the aortic position. However, the latter showed a lower occlusion rate. The underlying mechanism of calcification in in situ TE is most probably a highly multifactorial and complex process.
In our small animal model, CE-MRI lacked specificity to accurately follow the process of graft degradation and neo-tissue formation. Of interest, grafts with an ODS of 0 (mainly from the earliest 1-week timepoint) showed increased and highly variable CE values. This indicates that the porous grafts allow entrapment of contrast agent material. Increased contrast enhancement compared with later time points (and higher ODS scores) could also be owing to an initial inflammatory response and formation of a fibrous tissue layer, which is known to exhibit strong contrast enhancement patterns.25,26 This explanation is supported by a similar pattern in CE values in the corresponding control native vessels (ESI Fig SI-15): the native vessels showed an increased CE at the 1-week time point and significant decrease over time. The assessed native vessels were relatively close to the graft implantation site and may also have been affected by a certain degree of inflammation.
In the initial stage after graft insertion, possible postsurgical inflammation processes, such as edema and immune cell attraction, may also be associated with an increase in extracellular space, leading to a higher degree of contrast enhancement. It would have been interesting to have quantitative data on the degree of porosity or permeability of the graft, which in theory is possible with dynamic contrast-enhanced MRI at very high temporal resolution. Unfortunately, such techniques are currently incompatible with the additional requirements for blood flow suppressed and high spatial resolution imaging. In literature it is speculated that MRI methods using targeted (e.g., collagen-specific) contrast agents, may allow for more direct assessment of neo-tissue formation. 27 However, the limited availability of such probes as well as other factors (e.g., lower signal intensities because of lowered sensitivities, concern for Gd-probe toxicities) may complicate clinical translation of such methods.
In conclusion, the ester containing materials rPCL/PC-BU and PC(e)-BU are presumably unsuitable for clinical application in the high-pressure vascular environment because of their relatively fast degradation. Clinically unfavorable results such as local dilatation were seen for scaffolds produced from these biomaterials. This does not mean that for locations that need other scaffold characteristics, these biomaterials might be clinically useful. From the studied materials, PC-BU, in the current small-animal model, is most promising as it balances the degradation best with neo-tissue formation. Polymer combinations of, for example, PC-BU and PC(e)-BU may be interesting options for further study, where PC-BU provides mechanical stability over a longer period of time precluding dilation phenomena, and PC(e)-BU degrades faster thus initiating quicker neo-tissue formation. The class of BU-based biomaterials has the beneficial option of supramolecularly incorporating BU-based (bio)actives. 28
In an alternative approach, slower-degrading materials—possibly even slower than PC-BU—may be better choices for in situ TE, despite the obvious drawback that implanted biomaterials then remain in the body for extended periods of time.
Footnotes
Authors' Contributions
M.U.: conceptualization; data curation; formal analysis; funding acquisition; investigation; methodology; project administration; resources; software; supervision; validation; visualization; writing—original draft; writing—review and editing. B.F.C.: data curation; formal analysis; investigation; methodology; resources; software; supervision; validation; writing—review and editing. J.-W.v.R.: investigation; methodology. S.H.M.S.: data curation; funding acquisition; investigation; resources; writing—review and editing. M.H.C.J.v.H.: investigation; resources. W.S.: methodology; project administration; resources. L.R.: investigation; resources. H.M.J.: conceptualization, data curation; funding acquisition; investigation; resources; writing—review and editing.
A.v.d.W.: supervision; writing—review and editing. B.A.J.M.d.M.: resources; supervision; writing—review and editing. C.V.C.B.: conceptualization; funding acquisition; resources; software; supervision; writing—review and editing. G.J.S.: conceptualization; funding acquisition; resources; software; supervision; visualization; writing—review and editing. P.Y.W.D.: conceptualization; funding acquisition, methodology; resources; writing—review and editing. J.K.: conceptualization; funding acquisition; investigation; resources; supervision; validation; visualization; writing—original draft; writing—review and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research forms part of the One Valve project, powered by the Netherlands Cardiovascular Research Initiative (Grant No. CVON 2012–01): The Dutch Heart Foundation, Dutch Federation of University Medical Centers, the Netherlands Organization for Health Research and Development and the Royal Netherlands Academy of Sciences.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.