
Abstract
Large skeletal muscle defects owing to trauma or following tumor extirpation can result in substantial functional impairment. Purified exosomes are now available clinically and have been used for wound healing. The objective of this study was to evaluate the regenerative capacity of commercially available exosomes on an animal model of volumetric muscle loss (VML) and its potential translation to human muscle injury. An established VML rat model was used. In the in vitro experiment, rat myoblasts were isolated and cocultured with 5% purified exosome product (PEP) to validate uptake. Myoblast proliferation and migration was evaluated with increasing concentrations of PEP (2.5%, 5%, and 10%) in comparison with control media (F10) and myoblast growth medium (MGM). In the in vivo experiment, a lateral gastrocnemius-VML defect was made in the rat hindlimb. Animals were randomized into four experimental groups; defects were treated with surgery alone, fibrin sealant, fibrin sealant and PEP, or platelet-rich plasma (PRP). The groups were further randomized into four recovery time points (14, 28, 45, or 90 days). The isometric tetanic force (ITF), which was measured as a percentage of force compared with normal limb, was used for functional evaluation. Florescence microscopy confirmed that 5% PEP demonstrated cellular uptake ∼8–12 h. Compared with the control, myoblasts showed faster proliferation with PEP irrespective of concentration. PEP concentrations of 2.5% and 5% promoted myoblast migration faster compared with the control (<0.05). At 90 days postop, both the PEP and fibrin sealant and PRP groups showed greater ITF compared with control and fibrin sealant alone (<0.05). At 45 days postop, PEP with fibrin sealant had greater cellularity compared with control (<0.05). At 90 days postop, both PEP with fibrin sealant and the PRP-treated groups had greater cellularity compared with fibrin sealant and control (<0.05). PEP promoted myoblast proliferation and migration. When delivered to a wound with a fibrin sealant, PEP allowed for muscle regeneration producing greater functional recovery and more cellularity in vivo compared with untreated animals. PEP may promote muscle regeneration in cases of VML; further research is warranted to evaluate PEP for the treatment of clinical muscle defects.
Impact statement
Regenerative properties of purified exosome product can assist in myogenesis that can be applied to volumetric muscle loss, as seen with sarcoma resection or traumatic injuries. Continued research in this regard can also shed further insight into biologics that can improve functional outcomes.
Introduction
Volumetric muscle loss (VML) is the loss of skeletal muscle, which can occur following trauma or surgery.1,2 Severe traumatic injury to the limb often requires radical debridement to remove foreign materials and necrotic tissue, exacerbating further muscle loss.1–3 Similarly, in oncological cases, adequate amount of tissue must be resected to obtain clear margins to reduce risk of recurrence. Large skeletal muscle defects can ultimately leave patients with substantial functional and psychosocial impairments. Thus, a clinical need exists for regenerative solutions to treat VML allowing for improved functional outcomes.
Skeletal muscle has some regenerative capability owing to remnant satellite stem cells. However, in the case of major muscle loss, normal regeneration is disrupted and scar tissue forms. 4 There are currently no drugs approved by the Food and Drug Administration in the treatment of VML, although several products have been explored.
Autologous muscle grafting, one treatment option, must be weighed against the risk of donor site morbidity and studies have shown limited functional recovery and even poor cosmesis following such procedures.1,5,6 Physiotherapy also plays an important role as an adjunct to muscle recovery through promotion of muscle hypertrophy, especially when combined with regenerative products; however, in order for regeneration to occur, adequate amount of native stem cells are needed within the defect. 7 The use of an extracellular matrix scaffold alone or combined with stem cells have shown promising results, 8 but functional recovery is inconsistently reported.9–12 Despite these advances, there is still a clinical need for an off-the-shelf, cell-free product to help treat VML.
Interest in exosomes, which are small (diameter = 30–100 nm) extracellular vesicles produced by almost all endogenous cells, to treat VML has grown because of their potential regenerative properties. They contain a variety of cytoplasmic products including mRNA, microRNA, proteins, and several growth factors.13–15 Exosomal research has increased, especially in applications to regenerate cardiac myocytes.16,17 However, there is currently limited studies evaluating their effects on skeletal muscle regeneration.18,19
Purified exosome product (PEP) is a lyophilized powder that is stored at room temperature, and has demonstrated regenerative properties in wound, nerve, and tendon healing.20–23 Only one study thus far has applied PEP on skeletal muscle (urethral sphincter and latissimus dorsi), which has shed light on some of its regenerative capabilities. 24 The purpose of this study was to further investigate PEP's regenerative effects on skeletal muscle and functional recovery using a rat VML model.
Materials and Methods
In vitro
PEP preparation for myoblast culture
PEP was produced at Advanced Product Incubator (API, Rochester, MN) and provided by Rion™, LLC (Rochester, MN). A vial of sealed PEP was dissolved in 1 mL Ham's F-10 Nutrient Mix (ThermoFisher Scientific, Waltham, MA), which was then defined as 100% PEP. 20 F-10 nutrient mix alone is commercially available media that is serum free. Myoblast growth medium (MGM) is an F-10–based media that can be made by supplementing it with fibroblast growth factor (Life Technologies, Carlsbad, CA) and 10% fetal bovine serum (ThermoFisher Scientific, Gibco™, Waltham, MA). MGM provides a selective advantage for myoblasts over fibroblasts. 25 The PEP solution was then filtered using a Steriflip-GP sterile 0.22-μm system (Millipore Sigma, Burlington, MA). PEP was then further diluted using Ham's (F-10) media to achieve a concentration of 2.5%, 5%, and 10% to investigate its regenerative properties at different concentrations.
Rat myoblast purification
Primary myoblasts were isolated and prepared from one male adult Lewis rat according to Hindi et al. 25 In brief, after euthanasia, the biceps femoris and quadriceps muscles were isolated, washed, and finely minced. Muscles were digested with collagenase II solution (Collagenase, Type II; ThermoFisher Scientific, Gibco), serially filtered, and centrifuged. The remaining pellet was resuspended in MGM. The suspension was then seeded onto a 10% Matrigel Matrix (Corning®, Glendale, AZ) dish where it was incubated for 72 h at 37°C. Next, the myoblasts were purified via “pre-plating,” which is a process that involves the transfer of the supernatant onto a noncoated dish for 45 min. Fibroblasts have quicker attachment than myoblasts. 25 Thus, when the suspension was plated on a noncoated dish, the fibroblasts quickly attached, leaving myoblasts suspended in the supernatant, which were then transferred to another Matrigel-coated plate. This process was repeated four times as previously reported. 25
Myoblast proliferation assay
The proliferation assay was used to assess myoblast viability. The myoblasts were seeded at 50,000 cells/well in a 24-well plate and incubated at 37°C with 5% CO2 for 144 h (6 days). Five groups were based on myoblast cocultured with the designated study media, which were: F-10 only, MGM, and 2.5%, 5%, or 10% PEP diluted in F-10. Plates were divided into five groups of four wells each. After 72 h, all media were changed. Cell proliferation was analyzed in real-time by using IncuCyte® S3 Live Cell Analysis System (Essen BioScience, MI).
Myoblast migration assay
To assess the two-dimensional motility of the myoblasts in cell culture, the “scratch test” was used to simulate a theoretical “healing wound.” 26 In brief, myoblasts were seeded at 240,000 cells per well in the 24-well plate and incubated in MGM at 37°C with 5% CO2 for 8 h to permit adhesion of cells to the bottom. After complete cell adhesion, MGM was removed from all the 20 wells and substituted with the culture media according to our five designated study groups. Next, a linear scratch was made on the bottom of each well using a 200 μL pipette tip (Sigma-Aldrich, St. Louis, MO). The myoblasts migrating toward the “scratch” were captured in real-time using IncuCyte S3 Live Cell Analysis System (Essen Bioscience).
PEP uptake assay
The results of the proliferation and migration assay were then used to confirm intracellular PEP uptake, which revealed that 5% PEP was comparable in cellular regeneration with that of MGM. In brief, the PEP exosomes were marked with Vybrant™ CM-Dil solution per manufacturer protocol (ThermoFisher Scientific, Invitrogen™, Waltham, MA). Myoblasts were then cocultured with 5% PEP on a eight-well Nunc® Lab-Tek® II Chamber Slide™ System (ThermoFisher Scientific) for several time periods (1, 4, 8, and 12 h). After fixation with 4% paraformaldehyde solution (Santa Cruz Biotechnology, Dallas, TX), cells were blocked with 5% bovine serum albumin (Millipore Sigma). Cells were stained with F-actin Alexa Fluor™ phalloidin (No. A12379; ThermoFisher Scientific, Invitrogen) and Hoechst 33342 (ThermoFisher Scientific, Invitrogen). PEP exosome uptake was evaluated using confocal laser microscopy (LSM 780, Zeiss, Germany).
In vivo
Optimizing PEP in vivo concentration
At the start of the study, there were no preexisting studies that showed the optimal concentration of PEP on myoblasts. Qi et al. found that keratinocytes and tenocytes had higher proliferation and migration in vitro with 10% PEP, 23 rather than 5%. We then inferred that an in vivo concentration of 7–8% was likely optimal for healing. However, a higher concentration would likely be needed because of the potential for systemic absorption. In addition, a carrier solution such as a fibrin sealant like TISSEEL (Baxter, Deerfield, IL) would allow for local delivery. According to the release profile of PEP in TISSEEL (Baxter), to obtain a constant PEP concentration of 7–8% over a period of 2–3 weeks into the wound, a 20% concentration of PEP-TISSEEL (Baxter) was used.
PEP-TISSEEL preparation
Earlier studies20–22 utilized a carrier solution to promote local delivery of PEP. Similarly, we used TISSEEL (Baxter), a fibrin gel, to deliver PEP given its wide usage in wound closure, consistent formulation, and viscous properties.20–22 To reconstitute PEP in TISSEEL (Baxter), two kits of 2 mL TISSEEL (Baxter) were used. We first combined the PEP powder in the first TISSEEL (Baxter) fibrinolysis inhibitor (FI) solution to create a 100% PEP-FI solution (1 mL total volume). To obtain a 20% PEP-TISSEEL we proceeded as follows: 400 μL of PEP-FI were used to replace 400 μL of the second FI, obtaining a new concentration of 40% PEP-FI while maintaining a volume of 1 mL. After that, all preparation followed the manufacturer's instruction to prepare and load PEP-TISSEEL solution onto the double-barrel syringe. The final concentration of PEP-TISSEEL contained 20% PEP.
Rat VML model
Experimental procedures were approved and conducted in accordance with guidelines set forth by our Institutional Animal Care and Use Committee (No. A00004013-18). A total of 144 male Lewis rats (Charles River Laboratories, Boston, MA) that were 2.5 months old (weighing 250–300 g) were used. The single gender was used to minimize biological variability. Rats were randomized into four potential treatment groups: (1) surgery-only or control, (2) TISSEEL-only, (3) PEP-TISSEEL, or (4) platelet-rich plasma or PRP (Biological Specialty Corp., Colmar, PA) alone. Next, each group was randomized again into four potential recovery groups: 14, 28, 45, or 90 days. There were nine rats per group, unless indicated.
Before surgery, rats were premedicated with ibuprofen–water (15 mg/kg), which was also continued until 48 h after surgery for analgesia. Perioperatively, enrofloxacin and buprenorphine were subcutaneously administered. Rats were anesthetized with isoflurane for the duration of the procedure; they were induced with 2–3% isoflurane and maintained at 1–2%. Rats were placed in the lateral position, and the right hind limb (defined as the standardized operative limb) was shaved. Surgery was performed under aseptic techniques.
The steps of the surgery are given in Figure 1A–E. In brief, the right lateral gastrocnemius (LG) was exposed as previously described and a 3-cm incision was made over the right lateral side of the hindlimb. 27 The insertion point of the biceps femoris was incised and reflected to expose the LG muscle. Using an 8-mm punch biopsy instrument, a full-thickness defect was created on the LG muscle at the level of mid-tibia (Fig. 1A, B). The muscle was removed, which measured roughly 20–25% of the total LG muscle mass.
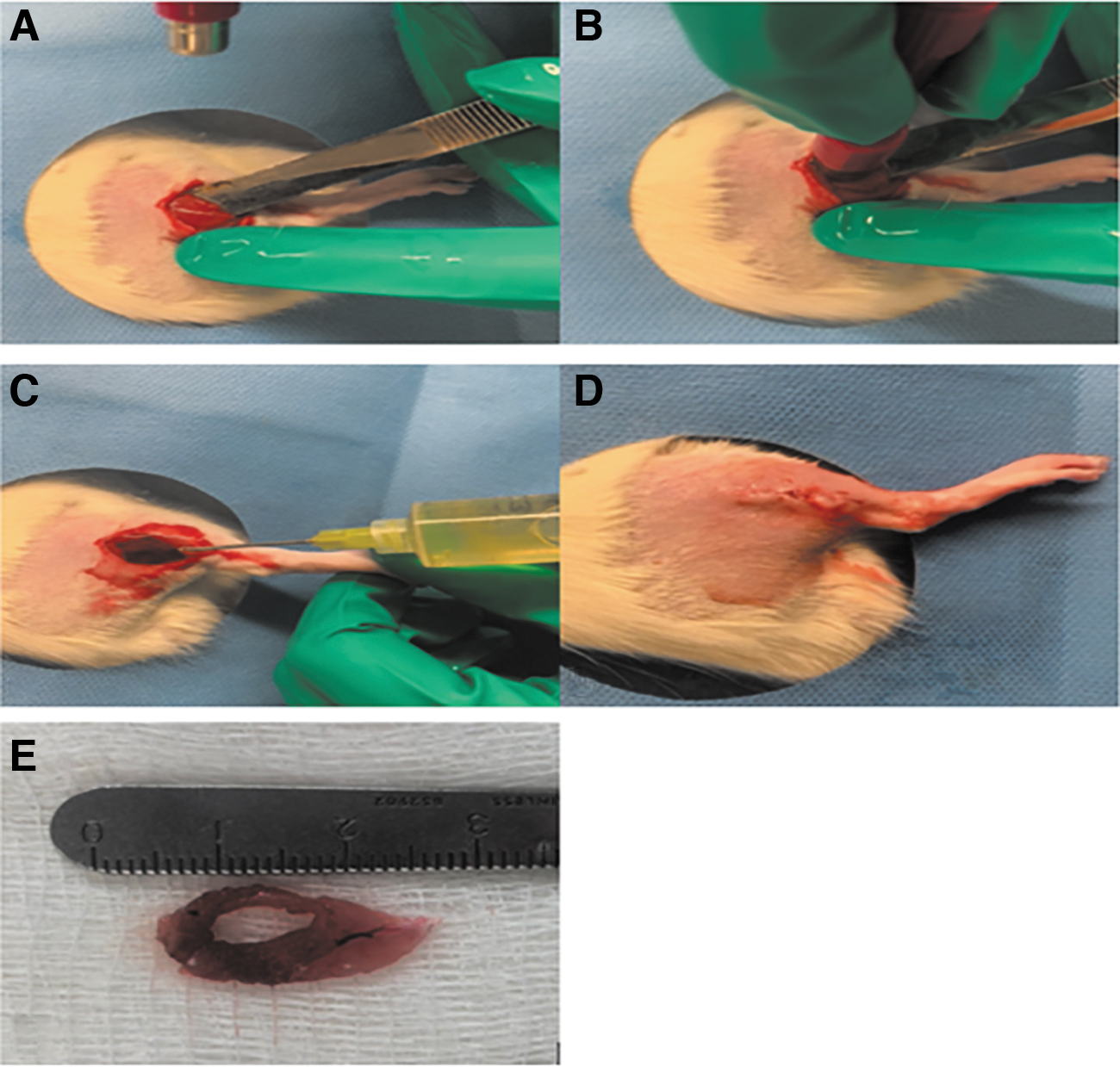
Next, the defect was treated according to the randomized group. The control (surgery-only) group did not have any material injected. In treatment groups, either 1 mL of TISSEEL alone or 1 mL of PEP-TISSEEL was injected directly onto the defect (Fig. 1C). PRP was obtained from commercially available donor human serum, centrifugated once, until a platelet concentration of >1000 × 109/L was obtained. Defects were filled with PRP and left intact. The biceps femoris was reapproximated using 5–0 Prolene sutures and the skin was closed with absorbable subcutaneous running sutures (Fig. 1D), and triple antibiotic ointment was applied. The operated limb was not immobilized after surgery. 28
Isometric tetanic force measurement and sample harvest
At each designated time point, isometric tetanic force (ITF) of the muscle was performed to demonstrate the degree of functional recovery. First, the rats were anesthetized with intraperitoneal injection of 10 parts ketamine (100 mg/mL), 2 parts xylazine, and 0.3 parts of acepromazine (10 mg/mL), at a dosage of 0.3 mL/kg bodyweight.
The experimental set-up for ITF is given in Figure 2. The posterolateral hindlimb was approached from the dorsal aspect to optimally expose the sciatic nerve and its distal bifurcation. Next, a skin incision was made and carried distally to the calcaneus, along the lateral aspect of the limb to expose the posterior muscles. The skin flap was reflected to expose the biceps femoris that was later incised and reflected to further expose the gastrocnemius. It was isolated from the skin and surrounding muscles. Once isolated, the medial and LG were separated from each other distally.
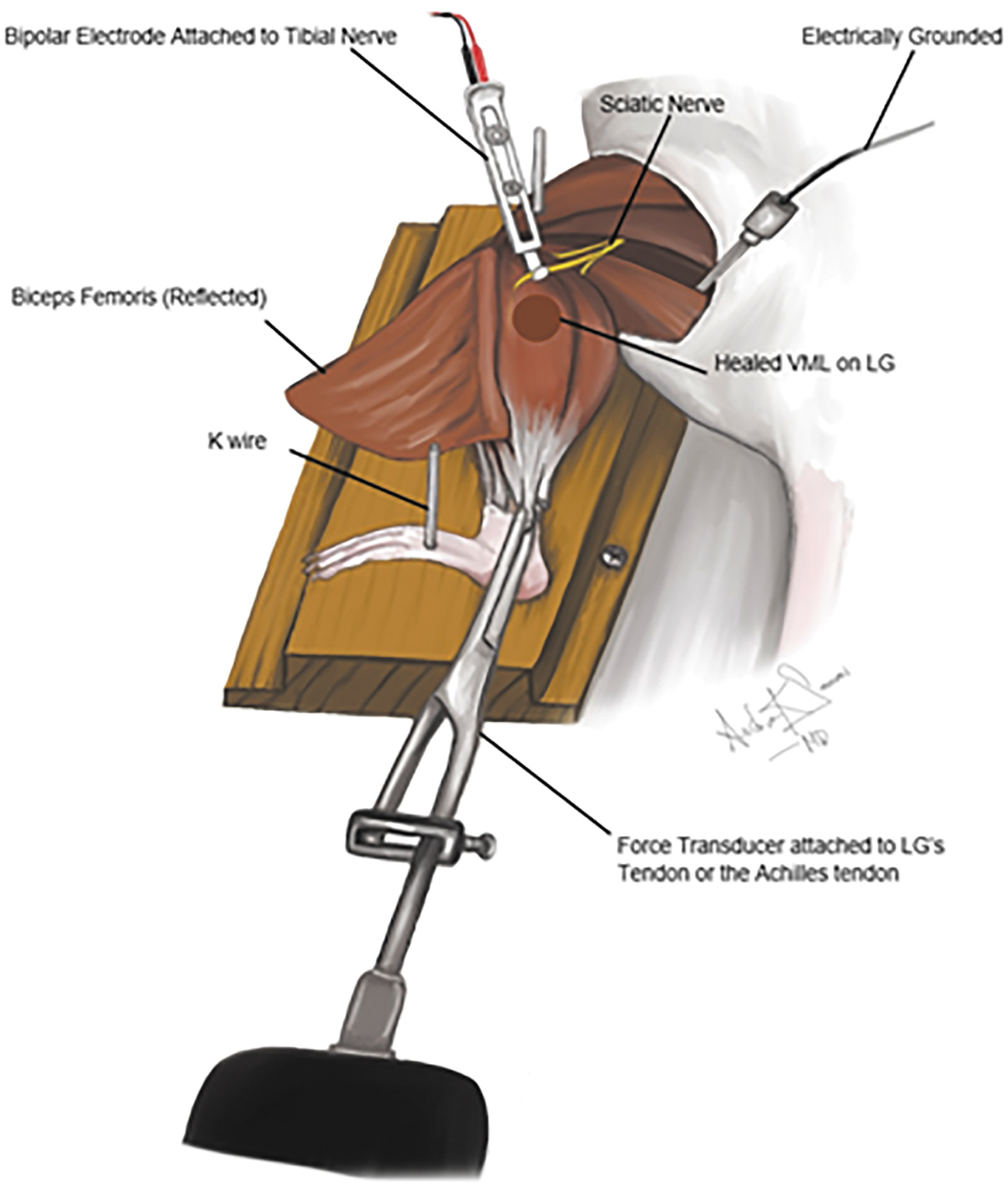
The experimental set-up of ITF at either 14, 28, 45, or 90 days post-VML creation. The limb was secured with K-wires. From the dorsal approach to the hind limb, the biceps femoris was incised and reflected, revealing the sciatic nerve with its tibial, peroneal, and sural branches. The medial and LG tendons (or Achilles tendon) were separated distally. The LG tendon was attached to a force transducer, and the bipolar electrode was attached to the tibial nerve. ITF, isometric tetanic force.
To attach the LG to the muscle lever for force measurements, the Achilles tendon was cut and tied to the transducer (MDB-2.5; Transducer Techniques, Temecula, CA). The hindlimb was secured to the testing platform with K-wires (Pfizer Howmedica, Rutherford, NJ) and the knee and hip joints were fixed in a 90° flexion position. The LG was kept moist with a saline to prevent desiccation. A bipolar stimulator (Grass SD9; Grass Instrument, Quincy, MA) was directly attached to the isolated tibial nerve (1 cm proximal to its insertion onto the LG) using a subminiature electrode (Harvard Apparatus, Holliston, MA). The nerve was kept in situ and protected throughout the procedure.
The muscle length was adjusted to the length that produced the greatest twitch force using low frequency and low voltage. Then, the maximal twitch tension was determined as previously described which states that muscle is stimulated with 150 Hz and 2–10 V for peak tetanic tension (Po). 29 Each contraction was followed by 2 min of rest. The servomotor was interfaced with the computer. The force transducer signal was processed on a computer using LabVIEW (National Instruments, Austin, TX). After the procedure, the rats were killed and both LGS (normal and operative) were harvested, and later weighed and used for histological analysis.
Histology
Muscles were fixed in 10% neutral-buffered formalin and later embedded in paraffin and sectioned. The area of the VML defect was identified and analyzed. Coronal and longitudinal sections (10-μm thick) were cut and stained with routine Masson's trichrome (MT) for cellularity/fibrosis analysis. Histology was imaged using standard microscopy as described previously.30–32 Assessors were blinded while scoring histology.
Statistical analysis
Statistical analysis was conducted using GraphPad Prism 7.0 for Mac (La Jolla, CA). Categorical variables were expressed as values and percentage, and continuous variables as means with respective ±standard errors (SEs). All statistical tests were two sided. Alpha level was set at <0.05, which denoted statistical significance. If the data were not normally distributed, then nonparametric methods were used for analysis. The myoblast proliferation assay was analyzed using the Wilcoxon signed-rank test, and the proliferation rate at different time points were compared between treatment groups. For the migration assay, the migration area (μm2) at different time points is presented with respective mean ± SE. Two-way analysis of variance (ANOVA) followed by post hoc Dunnett's test was used to statistically compare all groups. The ITF of each rat is expressed as percentage of ITF of the contralateral limb (nonoperative limb) as reference. This was carried out to control for the effect of normal animal intravariability. The results of the ITF were statistically analyzed using ANOVA with Tukey–Kramer test.
Results
In vitro experiment
PEP promotes myoblast proliferation
The results of the proliferation assay are given in Figure 3. Irrespective of the PEP concentration, the cocultured myoblasts had faster proliferation compared with F-10 alone (p < 0.05). Irrespective of concentration, PEP had comparable myoblast proliferation to standard MGM. No difference was seen in proliferation despite varying PEP concentrations.
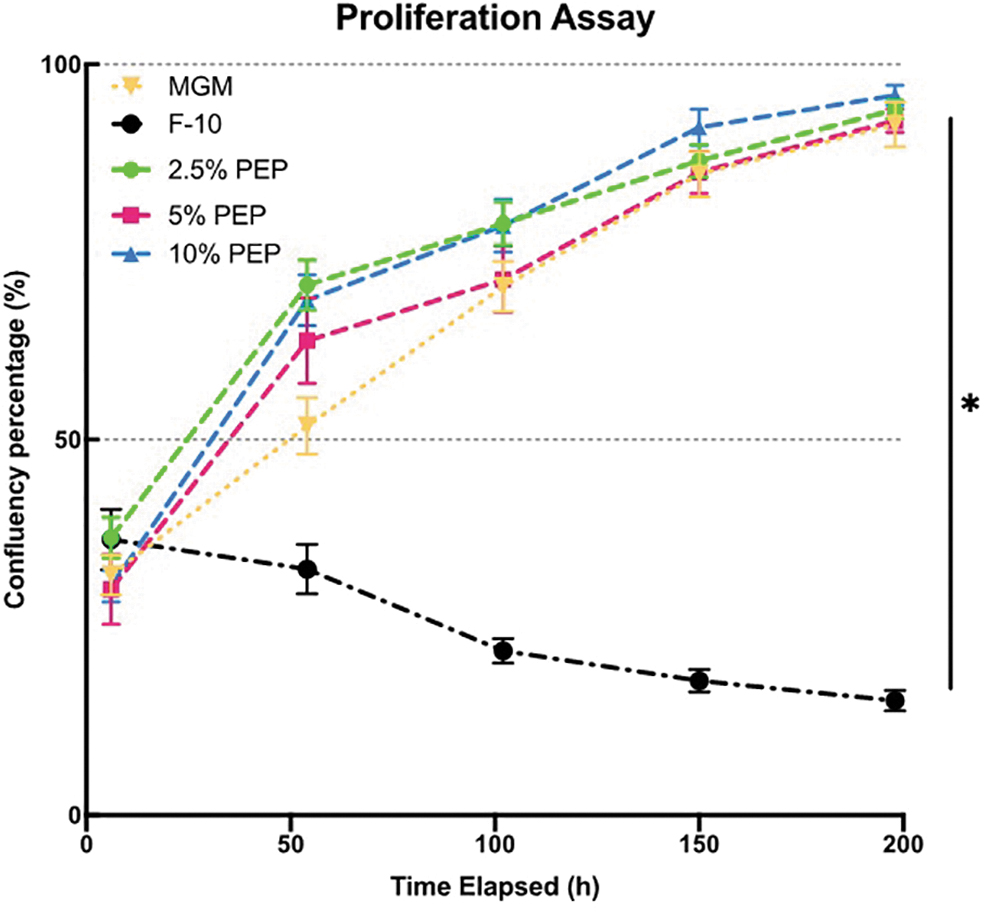
Graph of myoblast proliferation assay with different concentration of PEP (2.5%, 5%, and 10%), F-10, and MGM or growth medium. Irrespective of concentration, PEP promoted myoblast proliferation similar to standard MGM (asterisk denotes statistical significance). MGM, myoblast growth medium.
PEP promotes myoblast migration
The results of the migration assay are given in Figure 4. After nearly 30 h, myoblasts cocultured with 5% PEP had almost completely covered the linear “scratch.” The % confluence of myoblasts with MGM and 5% PEP were 97% and 91%, respectively. The 2.5% PEP group reached a final confluency rate of 82% after 30 h; however, 10% PEP was only able to reach 50% confluency. F-10 group did not show any migration. Faster migration was observed for all PEP groups and MGM cocultured myoblasts during the 8–24 h period. The cells cultured with 2.5% or 5% PEP had greater migration than 10% PEP and F-10.
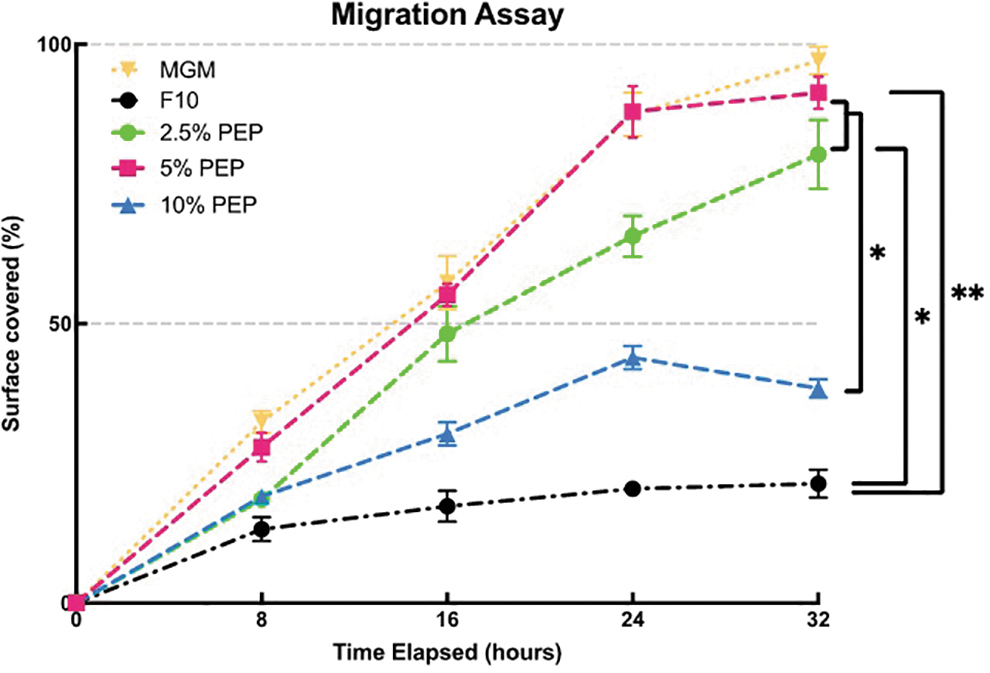
Graph of myoblast migration assay with different concentration of PEP (2.5%, 5%, and 10%), F-10 is control, MGM or standard growth medium with respect to time (hours). At 2.5% and 5% concentration of PEP, cells could migrate faster than 10% PEP and F-10 (asterisks denotes statistical significance).
Intracellular PEP uptake
The migration assay showed that 5% PEP was the most optimal concentration comparable with MGM. Thus, 5% PEP was chosen as the desired concentration for the uptake study. The results of immunofluorescence of PEP uptake into myoblasts are given in Figure 5. The fluorescent staining demonstrates appropriately stained blue nuclei, green stain to the cytoplasm, and intracellular uptake of Dil (red)-labeled PEP particles (Fig. 5A). Within 1 h, cytoplasmic PEP was seen (Fig. 5A). PEP florescence (a surrogate for uptake) increased overtime with higher amounts occurring from 8 to 12 h, and the highest occurring at 12 h (Fig. 5B).

In vivo experiment
PEP promotes functional recovery
The results of ITF are given in Figure 6. Irrespective of the group, there were no differences in ITF at 14, 28, or 45 days postop. At 90 days postoperatively, there were statistically higher percent ITF in the PEP-TISSEEL and PRP groups compared with TISSEEL-only and surgery alone (p < 0.01). There was no difference in muscle mass overtime, irrespective of the study groups (Fig. 7).
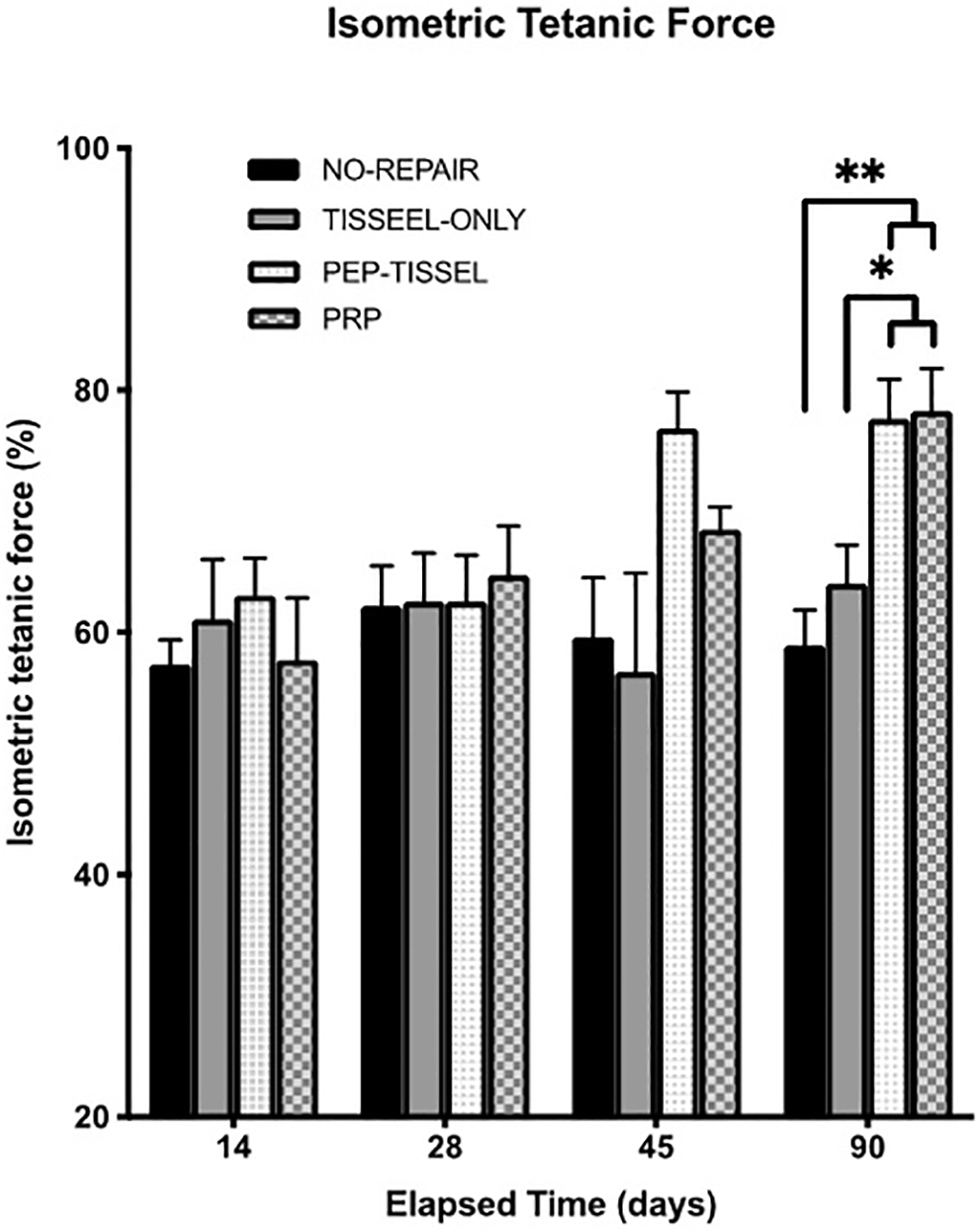
Bar graph of the ITF with respect to study periods and experimental groups. ITF was measured as percentage of force compared with the normal limb. PEP-TISSEEL and PRP groups had significantly higher ITF compared with TISSEEL and no repair at 90 days postoperatively (asterisks denotes statistical significance). PRP, platelet-rich plasma.
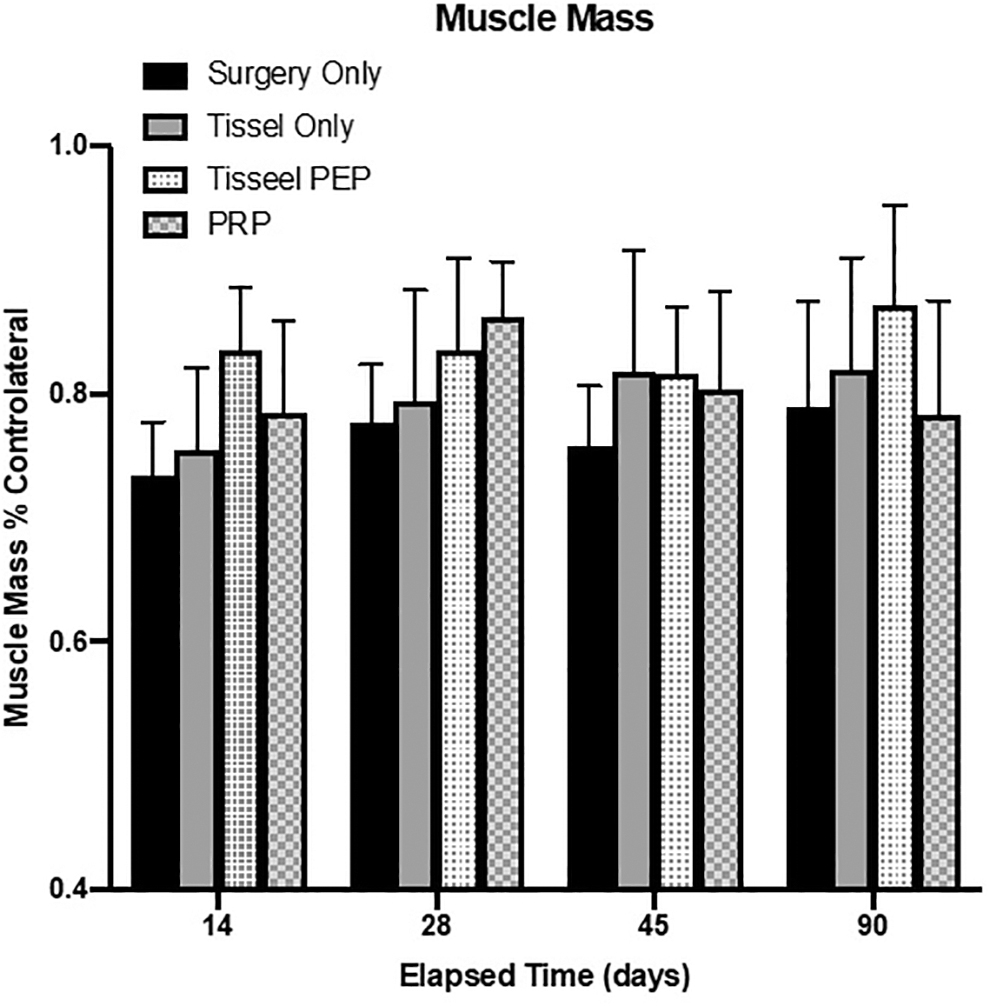
Muscle mass graphic representation for each study group at different time points. Surgery-only study group muscle mass remains low and does not seem to increase throughout the entire recovery time. Statistical significance among the other group was not observed.
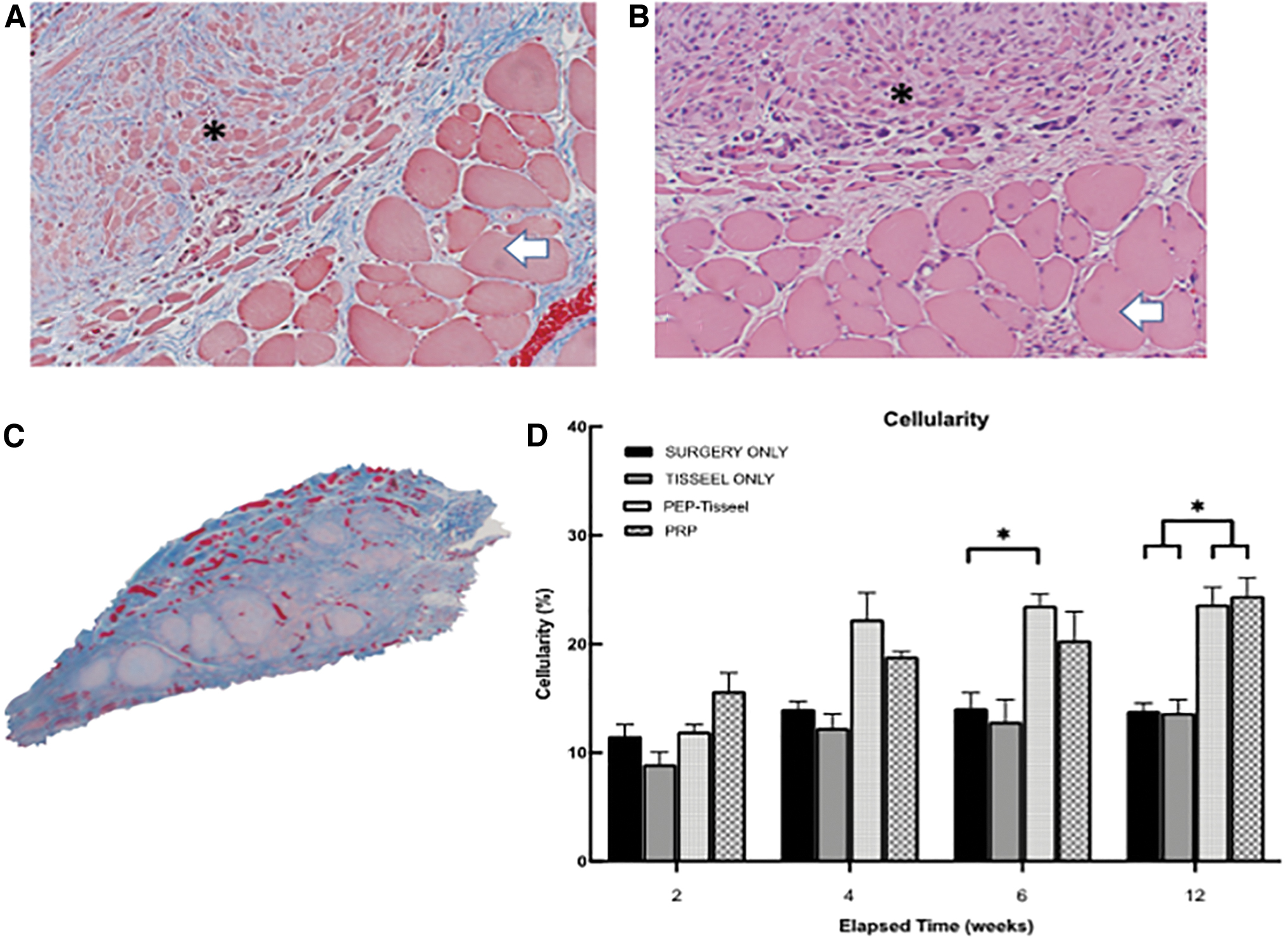
PEP promotes muscle cellularity
Histology was assessed of all harvested samples at the respective study time intervals (14, 28, 45, and 90 days postoperatively) for fibrosis and cellularity with MT stain (Fig. 8A–D). The results showed increased cellularity in the PEP-TISSEEL and PRP group at specific time points (Fig. 8D). Quantitative assessment of the percent surface area of cells (red) relative to collagen (blue) also confirmed the MT staining as there was increased overtime in the PEP-TISSEEL group (Fig. 8C). Irrespective of time, there were no changes in percent cellularity in either surgery-alone or TISSEEL-only group.
Discussion
Muscle defects following trauma and oncologic resection remain challenging reconstructive problems. Regenerative means of restoring muscle function is needed clinically. The promotion of myocyte regeneration is attractive for VML injury as it may allow muscle to heal with minimal scaring and improved function. 19 Studies have now demonstrated that exosomes have additional functions including the promotion of cellular regeneration.16,17,20–24,33–35 The application of exosomes to skeletal tissue system is currently limited.19,24,35,36 We assessed PEP in skeletal muscle regeneration using an iatrogenic VML rodent model and found that PEP promoted myoblast proliferation and migration like standard MGM. In addition, we found greater ITF and lower fibrosis following PEP treatment.
Exosomes have shown promise in maintaining cellular viability. Qi et al. found a dose-dependent response of proliferation after coculturing tenocytes with PEP. 23 In addition, Rolland et al. found a dose-dependent growth of skeletal muscles following PEP application. 24 They found that human skeletal myoblasts cocultured with PEP were capable of faster proliferation and migration in a dose-dependent manner. 24 In our study, we found similar proliferation rates irrespective of dose. In addition, we found that myoblasts cocultured with either 2.5% or 5% PEP had faster migration than 10% PEP. In this regard, a dose-dependent response was not seen as the lower concentrations outperformed 10% PEP. Thus, it remains unclear if there is a dose-mediated regenerative response to PEP owing to discrepancy in results. This may be species or cell line–specific finding; however, further investigation is warranted.
Exosomes have the potential for improving functional recovery. Similar to our study, Rolland et al. created a 8 mm VML on a rat latissimus dorsi muscle. 24 After 8 weeks, the authors found that control animals had persistent fatty defects, whereas those treated with PEP-TISSEEL or TISSEEL had healed defects. 24 This was evaluated further on immunohistochemistry, which showed presence of desmin-positive cells in both the PEP-TISSEEL and TISSEEL-only groups, although no statistical difference was found. In contrast, we found significant differences between muscle cellularity in the injured tissue. Compared with TISSEEL-only and control, PEP-TISSEEL had greater cellularity at 6 and 12 weeks postoperatively. One potential reason for lack of statistical significance could be attributed to the shorter follow-up in the above studies' duration.
Rolland et al. did not perform functional evaluation of the latissimus dorsi; thus, its specific functional recovery remains uncertain. In our study, PEP led to greater muscle ITF compared to control particularly at longer follow-up periods (i.e., 45 and 90 days postop).
PRP is often used in clinical practice because of its proposed benefits of promoting myogenesis, neovascularization, and reducing scar tissue.37–39 We found no difference in functional outcome irrespective of PEP-TISSEEL versus PRP, which suggests that the two treatment strategies may be comparable. Clinically there are several reasons why PEP may be advantageous over PRP. PEP is stored at room temperature, and it is ready for use. It also does not require a blood draw as required with PRP. PRP also has a shorter active lifespan, and it must be stored at −80°C or in liquid nitrogen for adequate preservation.
There are several strengths to our study. We performed several in vitro and in vivo investigations simultaneously, which is rather limited in VML studies. 40 We also fostered uniformity with other PEP studies by extrapolating similar methodologies. With the intention of investigational reproduction and validation, we utilized TISSEEL as a vehicle at similar reported concentration to reproduce and further validate its role as a carrier with PEP delivery. We were able to corroborate our in vitro proliferation and migration assay with our vivo results as made evident by significant differences in cellularity and ITF.
Although our study further establishes the potential usefulness as PEP in muscle regeneration, opportunities for future investigations will involve assessment for gene expression to provide further insight on transcription and translation of markers that may have been affected by PEP. This study's histological analysis was limited to MT staining, which given the importance of collagen assessment in fibrosis and its relevance to VML was felt to be adequate and within the scope of the study. Additional histological analysis with an appropriate antibody to further evaluate in vivo markers of myogenesis would be useful for future investigations. The assessment of dynamic functional recovery (i.e., gait analysis) will be added to future studies. Although small animal studies provide useful initial insights, a larger VML model would be helpful in translating PEP's effects on a larger scale and help recreate a similar defect to clinical scenarios. Despite these limitations, this study provides both in vitro and in vivo assessment of the use of exosomes on muscle regeneration.
Conclusion
PEP can produce myocyte regeneration in a rat VML model. PEP-TISSEEL–treated defects had greater functional recovery and more cellularity in vivo compared with the control. This study is clinically relevant as we have demonstrated the regenerative properties of PEP on muscle defects. This suggests that PEP may be able to assist in functional restoration of muscle defects in humans. Further study is warranted.
Footnotes
Acknowledgment
The contents of this article were presented at the ORS Annual Presentation on February 11, 2023.
Authors' Contributions
Conceptualization: S.L.M., C.Z., A.B., L.M. Methodology: S.L.M., C.Z., A.B., L.M. Software: L.M. Validation: L.M. Formal analysis: L.M. Investigation: L.M., A.K.S., T.C.T.H., C.E.B., J.L. Resources: S.L.M., C.Z., A.B. Data curation: L.M. and A.K.S. Writing—original draft: L.M., A.K.S., T.C.T.H., C.E.B., J.L., M.T.H., C.Z., A.B., S.L.M. Writing—review and editing: L.M., A.K.S., T.C.T.H., C.E.B., J.L., M.T.H., C.Z., A.B., S.L.M. Visualization: L.M. and A.K.S. Supervision: S.L.M., C.Z., A.B. Project administration: S.L.M. Funding acquisition: S.L.M.
Disclosure Statement
A.B. has ownership rights to Rion LLC; all others have none to report.
Funding Information
The authors thank Regenerative Medicine Minnesota for funding of this study (Regenerative Medicine Minnesota Translation Award [RMM 092319 TR 013]).