
Abstract
Researchers have been exploring alternative methods for bone tissue engineering, as current management of critical bone defects may be a significant challenge for both patient and surgeon with conventional surgical treatments associated with several potential complications and drawbacks. Recent studies have shown mesenchymal stem cell sheets may enhance bone regeneration in different animal models. We investigated the efficacy of implanted scaffold-free bone marrow-derived mesenchymal stem cell (BMSC) sheets on bone regeneration of a critical bone defect in a weight-bearing rat model. BMSCs were isolated from the femora of male Sprague–Dawley rats 5–6 weeks of age and cell sheets were produced on temperature-responsive culture dishes. Nine male Sprague–Dawley rats 6–8 weeks of age were utilized. A bilateral femoral critical bone defect was created with a bridge plate serving as internal fixation. One side was randomly selected and BMSC sheets were implanted into the bone defect (BMSC group), with the contralateral side receiving no treatment (control). Rats were anesthetized and radiographs were performed at 2-week intervals. At the 8-week time point, rats were euthanized, femurs harvested, and microcomputed tomography and histological analysis was performed. We found a statistically significant increase in new bone formation and bone volume fraction compared with the control. Histomorphometry analysis revealed a larger percent of newly formed bone and a higher total histological score. Our results suggest that scaffold-free BMSC sheets may be used in the management of large weight-bearing bone defects to complement a different surgical technique or as a standalone approach followed by internal fixation. However, further research is still needed.
Impact statement
We investigated the biological enhancement of bone healing with bone marrow-derived mesenchymal stem cell (BMSC) sheet treatment compared with no-cell base treatment in a critical-sized femoral bone defect. The treatment group had enhanced bone regeneration after 8 weeks. Our study's contribution is the demonstration of BMSC sheet's bone healing enhancement in a critical bone defect model of a weight-bearing bone. This suggests BMSC sheets may be a potential treatment for patients with large bone defects in load-bearing regions, as an augment to other therapies or as a standalone approach.
Introduction
Critical-sized bone defects resulting from musculoskeletal tumors, infections, trauma, and developmental deformities represent a tissue deficit that is larger than the spontaneous healing ability of osteoblasts and are not expected to heal without surgical intervention. 1 Regeneration and repair of large bone defects occur through secondary bone healing, a process that hinges on osteogenesis, osteoinduction, and osteoconduction.1–3 Specifically, mesenchymal stem cells (MSCs) located within the bone marrow, periosteum, and surrounding soft tissues create the osteoprogenitor cells that differentiate into osteoblasts and osteoclasts. The recruitment and differentiation of MSCs are mediated by osteoinductive factors such as proinflammatory cytokines, growth factors (e.g., bone morphogenic protein), and angiogenic factors (e.g., vascular endothelial growth factor [VEGF]). Finally, an osteoconductive scaffold, which permits bone growth onto its surface (e.g., hematoma or cartilage callus) is important for bone healing.3–5
The management of these large defects can be a serious orthopedic challenge for both surgeon and patient with a significant clinical and economic impact. Conventional treatment options consist of bone transfer through distraction osteogenesis, induced membrane technique, and bone grafting, each associated with its own potential complications and drawbacks.3,5,6 An alternative and promising approach that has been gaining focus in the past years is bone tissue engineering by stem cell therapy.7,8 Traditionally, this would involve injecting stem cells into the defect or transplanting a scaffold embedded with them. These methods utilize trypsin to harvest cells, which can degrade cell membrane proteins and impede cell–cell and cell–extracellular matrix (ECM) interactions, thereby adding to impaired adhesion and proliferative activity.9,10 Moreover, any mismatch between the rate of scaffold degradation and cell activity may hinder rates of remodeling and bone tissue formation, which might explain the high rates of cell death with cell-seeded scaffolds. 11
Okano et al. described a technique called “cell sheet tissue engineering.” Using changes in temperatures during preparation, the group was able to harvest cell sheets without the use of proteolytic enzymes, thus preserving cell–cell-binding proteins, membrane-adhesive molecules, and ECM, and thus obviating the need for a scaffold.9,12,13 Various therapeutic uses for different type cell sheets have been reported for the regeneration of different tissues, including: cornea, lungs, heart, esophagus, middle ears, periodontal tissue, blood vessels, skin, and cartilage.9,14 Several groups have studied the application of scaffold-free bone marrow mesenchymal stem cell (BMSC) sheets in bone tissue and found a positive effect on bone regeneration in fracture, nonunion and bone defect animal models.9,10,15–18
In our study, we intended to investigate the therapeutic role of scaffold-free BMSC sheets in a rat critical bone defect model of a load-bearing bone.
Methods
Isolation and culturing of rat BMSCs
BMSCs were isolated from the femora and tibias of male Sprague–Dawley rats 5 to 6 weeks of age.19,20 Institutional guidelines for the care and use of laboratory animals were followed. Freshly euthanized rats were sterilized sequentially in 95% and 70% ethanol for 5 min before dissection. Under sterile conditions, the rat femora and tibias were isolated and transected to expose the medullary canals. The cells were flushed from the medullary canal with an 18-gauge needle using Dulbecco's modified Eagle's medium (DMEM) (Gibco, Carlsbad, CA) and passed through a 70 μm strainer, centrifuged, and resuspended in DMEM supplemented with 3.7 g/L sodium bicarbonate, 1.7 mM L-glutamine, and 10% fetal bovine serum with 1% MSC culture medium. Cells were incubated in a humidified atmosphere at 37°C and 5% CO2. The fresh medium was replaced the next day to remove the unattached cells (Passage 1).
After reaching confluence, the primary cultured cells were released from the culture substratum using trypsin-ethylenediaminetetracetic acid (Gibco, Invitrogen, Carlsbad, CA). Next, cell composition was evaluated using flow cytometry. The expression of BMSC-associated surface markers was analyzed using flow cytometry. We demonstrated positivity of CD29, CD44, and CD90 (>70%), thereby meeting minimum requirements for in vitro BMSC characterization.
Creation of the BMSC sheet
A 3 × 106 passage 3 BMSCs were seeded and cultured on specially designed 10 cm temperature-responsive culture dishes (Up-Cell®; CellSeed, Tokyo, Japan) containing prewarmed (37°C) MSC culture medium for 3 days 21 (Fig. 1). We used a prewarmed culture medium to avoid temperature drops during medium changes and subsequent undesired cell detachment. For the same reason, observation under a microscope was kept short. Before animal surgery, the temperature was lowered by placing the culture dish at room temperature (20–25°C) for 15–40 min to facilitate the detachment of a contiguous cell layer from the culture surface. Once the cell sheet was fully detached from the plate, it was implanted into the defect with the use of sterile forceps. Each femur was treated with two 25-mm diameter sheets, one on each side of the defect (total 6 × 106 cells).
BMSC sheet used in our experiment. BMSC, bone marrow-derived mesenchymal stem cell. Color images are available online.
Study design
All animal experiments were performed according to protocols approved by our Institutional Animal Care and Use Committee (Protocol number: 21561, date of approval: 02/13/2023). We treated 9 male Sprague–Dawley rats 6 to 8 weeks of age (150–250 g; Charles River Laboratories) with BMSC sheets in a femoral critical bone defect model as previously described.22,23 The surgical procedures were performed in a ventral recumbent position, under general anesthesia using inhalation of isoflurane 3% for induction and 2% for maintenance with oxygen flow of 1.0–2.0 L/min. Using an aseptic technique, a lateral incision was made on the hind limb and the vastus muscle was divided longitudinally to expose the femur. The lateral cortex was mounted with a custom-made ultrahigh-molecular-weight polyethylene jig plate (McMASTER-CARR) (Fig. 2) and fixed with six bicortical 0.3 mm smooth pins, three on each side. Using an oscillating mini saw, 2 osteotomies were made through designed slots and a 6 mm circumferential bone segment was excised from the midshaft femur creating a critical bone defect. Two 25-mm diameter BMSC sheets were implanted by wrapping the sheets around the proximal and distal edges of the osteotomized femur, one on each side. The surrounding muscle tissue was then gently sutured to prevent dislodgment of the sheets. The pins were cut flush with the plate and the wound closed in layers with 4-0 nonabsorbable sutures (Fig. 3). The procedure was then repeated for the contralateral limb without the BMSC sheet treatment (control). The left and right limbs were randomized and operated upon by the same surgeon in succession with identical technique.

Custom-designed UHMWP jig plate.

Femoral bone defect of 6 mm fixed with a mounted plate–pin construct and BMSC sheets wrapped around each osteotomized end. The asterisk indicates the center of the bone defect. Color images are available online.
After surgery, analgesia was provided to all rats through a subcutaneous injection of Buprenorphine SR (1.0 mg/kg animal weight) and unprotected weight bearing permitted. At 2, 4, 6, and 8 weeks postoperatively rats were anesthetized and radiographs taken to qualitatively evaluate bone healing (Fig. 4). Eight weeks after surgery rats were euthanized, femurs harvested, and specimens underwent a microcomputed tomography (micro-CT) scan for a quantitative analysis. Finally, specimens were prepared, sectioned, and sent for histological analysis to evaluate the cell composition of the defect.

Representative radiograph and sagittal micro-CT reconstruction of the femoral bone defect of rats 2, 4, 6, and 8 weeks after surgery. Notice the developed callus that is visible in the BMSC group from the first X-ray taken after 2 weeks, while no callus is observed in the early X-rays of the control group. micro-CT, microcomputed tomography.
Micro-CT analysis
The harvested rat femurs were scanned using a micro-CT (SkyScan 1276 micro-CT system, Bruker, Kontich, Belgium) with 20 μm resolution at 2016 × 1344, Al 1 mm, 85 kV, 200 μA, with 2 average frames at every 0.4° angle step. Data were reconstructed using the 1.6 version of NRecon software and analyzed by GEMS MicroView software (eXplore MicroView v.2.5, Analysis Plus; GE Healthcare, Toronto, Canada). For the analysis, bone volume (BV) and bone volume fraction (BVF) of the defect area in the midshaft femur were evaluated. In short, a 4-mm diameter × 6-mm length cylindrical region of interest (ROI) was positioned to cover the original femoral defect region (Fig. 5): the total volume (TV, mm3), BV (mm3), and BVF were measured. BVF was measured as the fraction of bone volume per tissue volume (BV/TV). A threshold value of bony tissue was determined by a phantom.

Cylindrical 4 × 6 mm ROI positioned over the original femoral defect region. ROI, region of interest. Color images are available online.
Histological analysis
Six of the harvested femurs (three from each group), were fixed in 10% formalin solution, neutral buffered for 24 h, decalcified in decalcifying solution (Sigma-Aldrich, Inc.), and embedded in paraffin for subsequent histomorphometry analysis. Plates were removed and sections (5 mm thick) were taken parallel to the long axis of the femur, stained with Alcian Blue–Orange G–Hematoxylin–Eosin, and placed in xylene for mounting. The histological sections were evaluated using a quantitative histological scoring method described by Han et al. Briefly, each specimen underwent histomorphometry analysis and a score was given in each one of four categories: newly formed bone (NB), cartilage (CA), fibrous tissue (FT), and remnant defect (RD) according to the percentage of the original bone defect (OBD). Finally, scores from each parameter are added together to form a final score from 0 (no bone healing) to 40 (complete bone healing). 24 Analysis and quantitative evaluations were performed using light microscopy (KEYENCE BZ-X800; Neu-Isenburg, Germany) and image analysis software (KEYENCE ANALYZER; Neu-Isenburg).
The original osteotomy cut lines were demarcated by measuring a distance of 2.3 mm from the closest pin hole on each side (Fig. 2) and the BD area was determined by demarcating and measuring the area between the demarcated osteotomy cut lines. The area of the OBD, NB, CA, and FT were identified, marked, and measured in mm2 using the “Hybrid Cell Count” of the image analysis software (KEYENCE ANALYZER; Neu-Isenburg). The RD area was calculated by subtracting NB from OBD.
Statistical analyses
All data are expressed as mean ± standard deviation. The Shapiro–Wilk test was used to test for normality. Parametric and nonparametric data were assessed using paired t-tests, and Mann–Whitney U testing, respectively. All statistical analyses were performed using SPSS version 26.0 (SPSS, Inc., Chicago, IL). A p < 0.05 was considered statistically significant.
Experiment
Radiographic analyses
Radiographs taken at 2 weeks after sheet transplantation showed callus formation around the defect site in seven specimens from the BMSC group and two specimens from the control group. At 4 weeks postsurgery, both groups had exhibited callus formation, however, the control group had minimal callus formation compared with the robust callus in the BMSC group. Additionally, a bridging callus of the defect was observed in two specimens from the BMSC group. At 6 weeks and 8 weeks after surgery, the BMSC group showed bridging of the defect in three and four specimens, respectively. One specimen from the control group showed bridging at 8 weeks. At 8 weeks bone edges in both groups were sclerotic implying that further healing was not expected.
Micro-CT analyses
Micro-CT analysis was employed to quantify the volume of new bone formation and BVF within the ROI in the critical femoral bone defect 8 weeks after surgery. One of the untreated specimens was severely infected and was therefore excluded from the study. The final analysis included nine specimens from the BMSC group and eight from the control group. For the BMSC group, the mean BV was 20.78 ± 12.95 mm3 and mean BV/TV was 22.8 ± 18.97. The control group showed a mean BV of 8.26 ± 3.84 mm3 and the mean BV/TV was 6.35 ± 2.82. Statistically significant differences were observed in both BV (p = 0.019) and BV/TV (p = 0.006) in favor of the BMSC group (Fig. 6).
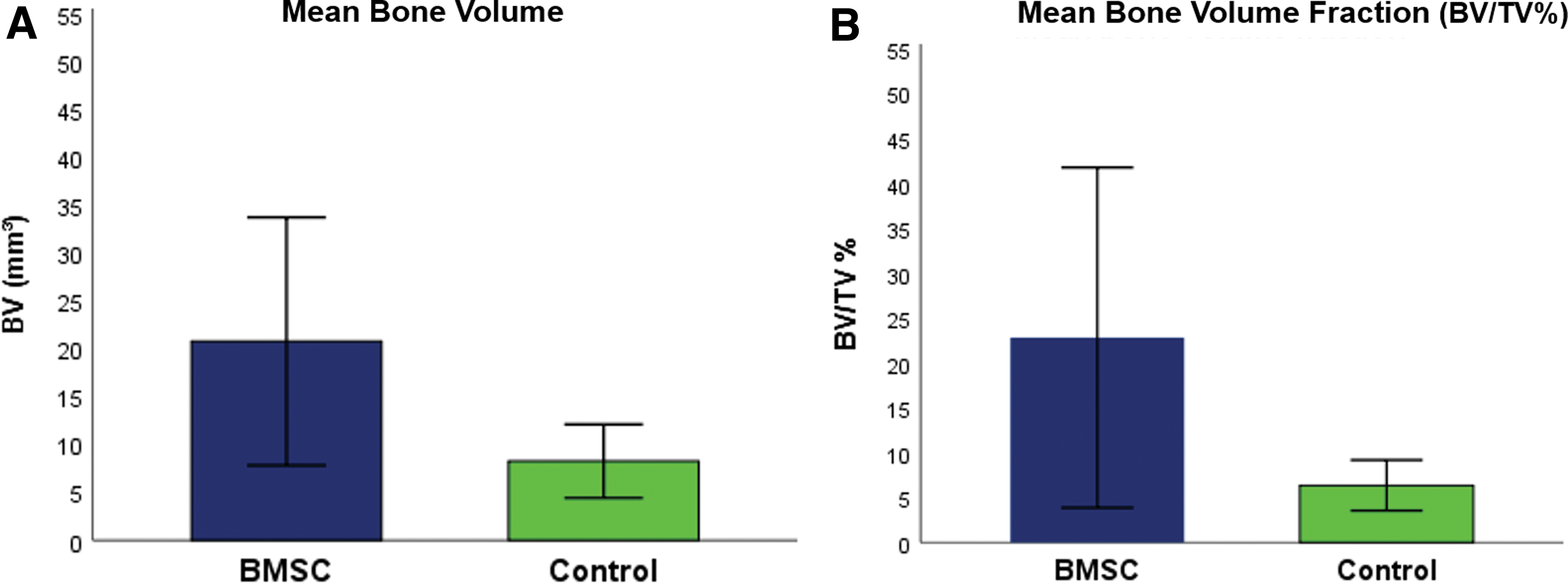
The volume of new bone formation, as determined by micro-CT data.
Histological analysis
Samples from the BMSC group had a mean of 27.9% ± 28.35% of the OBD filled with NB and a mean total score of 15 ± 5.29 ranging from 11 to 21, while the control group had a mean of 4.28% ± 4.18% of the OBD filled with NB and a mean total score of 7 ± 1 ranging from 6 to 8 (Fig. 7). However, differences in NB and total score were not statistically significant (p = 0.1 and p = 0.2, respectively). All samples had CA at around 1% of the defect suggesting that there would be no more bone regeneration. We also noticed muscle tissue to be present in around 30% of the OBD in all samples, which may have been impeding the process of bone regeneration. We observed bridging of the defect with woven bone in 1 out of 3 BMSC specimens compared with no bridging in the control group. None of the specimens exhibited medullary canal reconstitution or lamellar bone formation.

Representative histological slides stained with AB&OG.
Discussion
Bone grafting is a widely accepted method used in surgical treatment of various bony defects. Autologous grafts contain osteoinductive, osteoconductive, and osteogenic properties, all prerequisites for bone regeneration. However, these grafts are rarely utilized for large defects due to donor site morbidity and its unavailability in large quantities. Allograft is more readily available, but has limited osteoinductive efficacy due to storage and sterilization techniques, and there remains the possible risk of disease transmission, immunogenicity issues, failure to integrate in the host tissue.14,25 These limitations have led to the advancement of novel approaches to create tissue-engineered bone substitutes for managing patients with bone defects. A promising method developed in recent years that may potentially achieve this objective is cell sheet engineering using pluripotent stem cells.
Several preclinical studies have described the bone repair capacity of scaffold-free BMSC sheets. Nakamuro et al. reported BMSC sheets to enhance bone formation in a rodent nonunion femoral model. 16 They have also demonstrated the cells to not only survive around the fracture site after 8 weeks, but also contribute to bone formation by differentiating into osteogenic cells. Furthermore, they have shown BMSC sheets to express RNA for an angiogenic factor, VEGF-A that can possibly induce revascularization. 16 Another study by Shimizu et al. used a femoral fracture model in rats to show that percutaneous injection of intact BMSC sheets into the fracture site can enhance bone regeneration and lead to bony union. 17 In an animal study by Ueyama et al. BMSC sheets were implanted in a 2 mm mandibular bone defect, demonstrating bone continuation after 8 weeks. 15 Xu et al. demonstrated an osteogenic and endothelial sheet construct derived in vitro from BMSC to enhance new bone formation and promote rapid and functional vascularization in a rat calvarial critical bone defect. 18
The optimal tissue-engineered graft for a critical bone defect is one that would promote osteogenesis and angiogenesis while providing adequate mechanical stability. 3 Many studies have demonstrated BMSC sheets to boost bone regeneration and possibly induce angiogenesis.10,15–17 However, the major shortcoming of this technology is the lack of durable mechanical properties, which are necessary when dealing with large bone defects in weight-bearing regions. 9 As a result, numerous studies have examined the efficacy of integrating cell sheets and scaffolds in critical bone defect models to offer adequate mechanical support. Ueha et al. demonstrated in a rat model that BMSC sheets wrapped around scaffold cylinders of beta tricalcium phosphate (TCP) and implanted into femur critical bone defects had superior osteogenic and biomechanical properties compared with a construct composed of TCP and conventional BMSC. 26 Shang et al. reported bone allograft wrapped in MSC sheets to generate enhanced callus formation and possess superior biomechanical strength compared with allograft alone in a critical defect model of rodent femurs. 27
The concept of treating a critical-sized bone defect of a weight-bearing bone with cells in the absence of an artificial scaffold has been previously explored. Limori et al. have shown that cartilage generated in vitro from chondrogenically differentiated human pluripotent cells can create new bone in critical defects of rodent femurs without the use of a scaffold. 28 In our study, we sought to evaluate the effect of scaffold-free BMSC cell sheets on a critical defect of a load-bearing bone, using an internal fixation device to compensate for inherent mechanical deficiencies.
In this study, we chose a critical bone defect model to evaluate the biological enhancement of healing with BMSC sheet treatment compared with no cell base treatment without the natural healing process interfering. 29 Furthermore, we have chosen to focus on a weight-bearing long bone to examine BMSC sheet bone regeneration capabilities under load-related stresses.
In this study, we reported contiguous BMSCs without a scaffold to have a statistically significant positive effect on bone formation when implanted on the fixated bone edges of a large bone defect in a weight-bearing area. Our findings are supported by micro-CT analysis and histological staining. Micro-CT has shown a 2.5-fold increase in new bone formation in the BMSC group compared with the control (20.78 ± 12.95 mm3 and 6.35 ± 2.82, respectively, p = 0.019), with a mean of 23% of the defect being filled compared with 6% in the control group at 8 weeks (p = 0.006). Due to the large bone defect and the method of transplantation in which we wrapped the sheets around the bone edges without filling the gap we did not expect to bridge the entire gap and achieve union. Furthermore, histomorphometry analysis has revealed muscle tissue to be present in around 30% of the OBD in more than 80% of the specimens. The muscle tissue found in the defect can inhibit osteogenesis, and may be the reason we did not see bone bridging in more samples. An interesting study for the future may be to investigate the use of several larger BMSC sheets interposed between the bone edges, thereby preventing soft tissue invasion into the defect.
An in vitro study preformed on canine MSCs demonstrated that primary osteoblasts and MSCs actively make close cell–cell contact, which promotes proliferation of MSCs and osteogenic differentiation. 30 In contrary to conventional stem cell therapy techniques, BMSC sheets are harvested without damaging cell–cell junctions and other key membrane proteins, which may theoretically enable the implanted cells to bind to osteoblasts in the fracture site and induce proliferation, osteogenic differentiation, and bone formation.
There are some limitations in this study. First, CT scanning and histological evaluation were only performed once after 8 weeks from surgery, and so we do not have a timed series of quantitative evaluation of the healing process. We did, however, perform consecutive X-rays every 2 weeks for qualitative evaluation (Fig. 4). When examining the early X-rays 2 and 4 weeks after surgery, we observed more visible and developed callus in the BMSC-treated group compared with the control group. This observation may suggest BMSC sheets to not only enhance but also hasten bone healing. Second, we used rat BMSC, which cannot fully represent the effect on bone healing that human BMSC may possess. Finally, our study focused on radiographic and microscopic assessment and did not include biological investigation. We intend to rectify this in future studies that will attempt to shed light on the timing and mechanism in which BMSC sheets enhance bone formation in large bone defects.
In conclusion, we have demonstrated that despite possessing weak mechanical properties, scaffold-free BMSC sheets may significantly contribute to bone regeneration in a weight-bearing critical bone defect. These findings are generally consistent with the concept that BMSC sheets contribute to osteogenesis.9,10,14–16 However, our study's contribution is in the demonstration of this concept in a critical-sized weight-bearing bone defect. Possible future clinical implications in bone defect management could be the use of BMSC harvested from a patient's blood and implanted in the form of sheets to compliment a different surgical technique or as a standalone approach followed by internal fixation. However, further research is still needed.
Footnotes
Authors' Contributions
K.M.: Investigation (lead); Methodology (lead); Formal analysis (equal); and Conceptualization (supporting). J.L.: Writing—original draft and editing (lead); Formal analysis (equal); Investigation (supporting); and Software (supporting). W.L.: Project administration (lead); Resources (lead); Methodology (supporting); Investigation (supporting); Supervision (supporting); Writing—review and editing (supporting); and Conceptualization (supporting). C.C.: Software (lead) and Methodology (supporting). Y-.L.C.: Methodology (supporting). J.Y.: Conceptualization (lead); Supervision (lead); and Writing—review and editing (lead).
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.