
Abstract
Fractures occur commonly with multiple injuries, and their incidence has increased in recent years. Trace amounts of cobalt are necessary for many living organisms as it stimulates hematopoiesis and improves bone health. However, cobalt is also toxic, as it might cause allergic reactions and tissue destruction. These factors limit the application of cobalt in some medical fields. We studied the tea polysaccode-cobalt complex (TPS-Co) prepared from Qingzhuan Dark Tea polysaccharides. We used 6-week-old Sprague-Dawley rats to establish a femoral fracture model and evaluated the effects of CoCl2 and TPS-Co on the healing of femoral fractures. In this study, treatment with TPS-Co for the same content of cobalt intake decreased the side effects associated with CoCl2 treatment and accelerated the healing of femoral fractures in rats. This treatment method promoted angiogenesis by upregulating the expression of vascular endothelial growth factor and hypoxia-inducible factor. Bone formation was promoted via the upregulation of the expression of bone morphogenetic protein 2 and serum bone alkaline phosphatase. TPS-Co was found to actively regulate bone and vascular systems, resulting in significant bone regeneration effects. Therefore, the Qingzhuan Dark Tea polysaccharide cobalt complex might be used as an additive or drug to promote fracture healing, and thus, it might have a huge market value.
Impact statement
At present, the application of cobalt in the medical field is limited because it causes a series of adverse reactions in the human body. To find a way to retain the excellent active function of cobalt while mitigating its adverse reactions, we prepared the Qingzhuan dark tea polysaccode-cobalt complex (TPS-Co). The effects of cobalt compounds and organocobalt complexes on femoral fractures in rats were also evaluated. Our results showed that TPS-Co positively regulated the vascular and skeletal system and had a significant promoting effect on bone regeneration. These results may have positive implications for future cobalt applications.
Introduction
Fractures occur commonly with multiple injuries, and their incidence has increased in recent years.1,2 Although fractures usually heal spontaneously, about 2–20% of patients develop serious complications for various reasons, such as delayed union or even nonunion of the fracture.3,4 Thus, it is an urgent public health concern, and new treatment strategies and drugs need to be developed to address this problem.
Cobalt is an essential trace element for humans and animals, and it plays several important physiological and metabolic roles in the body. 5 Cobalt ions are involved in the synthesis of vitamin B12, which is essential for humans. 6 Cobalt also promotes hematopoiesis and bone health.7,8 However, it is toxic and might cause allergic reactions and tissue destruction.9–11 Excessive intake of cobalt can harm the body; for example, it can aggravate heart diseases and damage the nervous system. 12 Thus, cobalt has limited applications in some medical fields.
The formation of a vascularization network strongly promotes bone repair as blood vessels provide necessary nutrients, oxygen, and growth factors to bones.13,14 Vascularization can also stimulate cells in bone tissue to release growth factors, such as bone morphogenetic protein (BMP) and osteoblast growth factor, which can promote the proliferation and differentiation of osteoblasts, thus promoting the formation of new bone tissue.15–18 Cobalt ions can promote angiogenesis and induce hypoxia-inducible factors (HIFs), which can facilitate the coupling between osteogenesis and angiogenesis. This process can activate several proangiogenic factors, including vascular endothelial growth factor (VEGF).19,20 Cobalt plays a favorable role in angiogenesis and bone regeneration and might be a promising tool for bone regeneration.
Several studies have determined the role of cobalt in bone regeneration.21,22 However, most studies investigated and tested the application of cobalt-based materials in orthopedics; studies on the oral administration of cobalt for treatment are limited. Therefore, minimizing the harmful effects of cobalt while fully utilizing its excellent properties is challenging. Metal ions form metal complexes with ligand molecules, which might be a way to reduce metal toxicity. Cobalt ions are suitable metal ions for the synthesis of a new class of drugs. 23 Complexes of Co (II) and the quinolone antimicrobial enrofloxacin were found to be effective antibacterial agents and inhibitors of DNA replication. 24 Some cobalt complexes show cytotoxic and anticancer effects against various cancer cell lines and cause lower systemic toxicity than other agents.25,26
In a study, several Co (III) Schiff base complexes with broad-spectrum antifungal activity were administered at doses of up to 266 mg/kg, and they were tolerated without side effects. 27 The preparation of cobalt complexes is an effective method to reduce their toxicity.
In this study, we used the prepared cobalt complexes of Qingzhuan dark tea polysaccharides. A femoral fracture model was established in 6-week-old Sprague-Dawley rats. The rats were treated with CoCl2 and tea polysaccode-cobalt complex (TPS-Co) for 2, 4, and 6 weeks, respectively, and the effects of cobalt compounds and organic cobalt complexes on femoral fractures in rats were evaluated at different periods.
Materials and Methods
Animal surgical procedure
Male Sprague-Dawley rats (6 weeks old; n = 36) were selected for the experiment. All rats were housed following a 12-h/12-h light-dark cycle and were provided free access to food and water. The temperature of the experimental environment was adjusted to 24 ± 2°C, and the relative humidity of the experimental environment was maintained at 40–65%. The animal surgical protocol was approved by the Animal Use and Management Committee of Hubei University of Science and Technology. Animal modeling was performed as described in another study. 28
The rats were anesthetized by intraperitoneal injection of 3% sodium pentobarbital (30 mg/kg) prepared in advance. A longitudinal incision was made on the right lateral thigh of the rats in the left prone position, and the scalpel sliced the skin and subcutaneous tissue in turn. The lateral femoral muscle was bluntly separated, and the femoral shaft was fully exposed. A Kirschner wire was inserted retrograde from the proximal end of the fracture and passed through the greater trochanter of the femur. After a reduction of the fracture end, the Kirschner wire was moved forward through the subchondral bone of the distal femur to ensure that the Kirschner wire was in the bone marrow of the femur. The model was evaluated by X-ray analysis. The rats with fracture were randomized for placement in the experimental groups.
The groups included the Control group (femoral fracture; intragastric administration of normal saline); (2) the CoCl2 group (femoral fracture, gavage of CoCl2·6H2O 10 mg/kg/day); and (3) the TPS-Co group (femoral fracture, intragastric administration of TPS-Co 65 mg/kg/day), which matched the daily cobalt intake of rats in the CoCl2 group. TPS-Co was prepared following the method described in our previous study. 29 The administration of group-specific treatment began on the day of modeling, and four animals in each group were euthanized after 2, 4, and 6 weeks. Fresh rat blood was rapidly collected from the abdominal aorta. The supernatant serum was collected by centrifugation and stored in the refrigerator at −20°C. After making an incision at the fractured femur, the muscle tissue attached to the femur was removed, and the recovery status of each femur was recorded.
Radiological analysis
All fractures were analyzed using an X-ray machine (Anjian Medical Device Co., Shenzhen, China). The rats were anesthetized by intraperitoneal injection of 3% sodium pentobarbital (30 mg/kg) prepared in advance. When the rats were in a coma, the right hind limb of the rats was fixed, and the fracture site of all rats was irradiated with X-ray (60 kV, 320 mA, 16 ms, and 5 mAs). Radiographs were obtained 2, 4, and 6 weeks after surgery. A radiologist who was blind to the experiment analyzed the radiological results. The X-ray images of rat fractures were scored following the method described by Wei et al. The degree of fracture healing was scored as follows: grade 1: no calcification; grade 2: patchy calcification; grade 3: calcification appears as a callus; grade 4: callus bridging across the fracture gap; grade 5: continuity of bone trabeculae; and grade 6: remodeling to normal bone. 30
Histological analysis
The femur was immediately immobilized in 4% paraformaldehyde for 24 h and then decalcified in 10% EDTA at 37°C for 21 days. Then, the femur was dehydrated, paraffin embedded, and paraffin sectioned (6 μm thick). Next, hematoxylin and eosin (H&E) staining and tartrate-resistant acid phosphatase (TRAP) staining were performed following the method described by Colucci et al. 31 The area of newly formed bone trabeculae and the number of osteoclasts were measured using Image Pro Plus (MEDIA CYBERNETICS, Maryland).
Immunohistochemical staining
Immunohistochemical (IHC) staining of the femoral tissue sections was performed as previously described. 32 The sections were incubated with primary antibodies containing rabbit anti-BMP2 (ab284387; Abcam, Cambridge, United Kingdom) and rabbit anti-CD31 (1:1000, ab182981; Abcam). The sections were incubated at 37°C with a secondary antibody conjugated to horseradish peroxidase (ab6721; Abcam). The selected areas were photographed under a light microscope (Olympus, Tokyo, Japan). The Image Pro Plus software was used for the semiquantitative analysis of BMP2-positive and CD31-positive areas after IHC staining.
Detection of bone metabolism indicators
The serum levels of bone alkaline phosphatase (BALP) and VEGF and the expression of HIF-1 in rats were determined using an enzyme-linked immunosorbent assay (ELISA) kit (Enzyme-Linked Biotechnology Co., Ltd., Shanghai, China).
Statistical analysis
The data were statistically analyzed using the GraphPad Prism software. All continuous data are presented as the mean ± standard error (X ± S). The differences among groups were assessed by one-way and two-way analysis of variance. All differences were considered to be statistically significant at p < 0.05.
Results
TPS-Co promoted femoral fracture healing
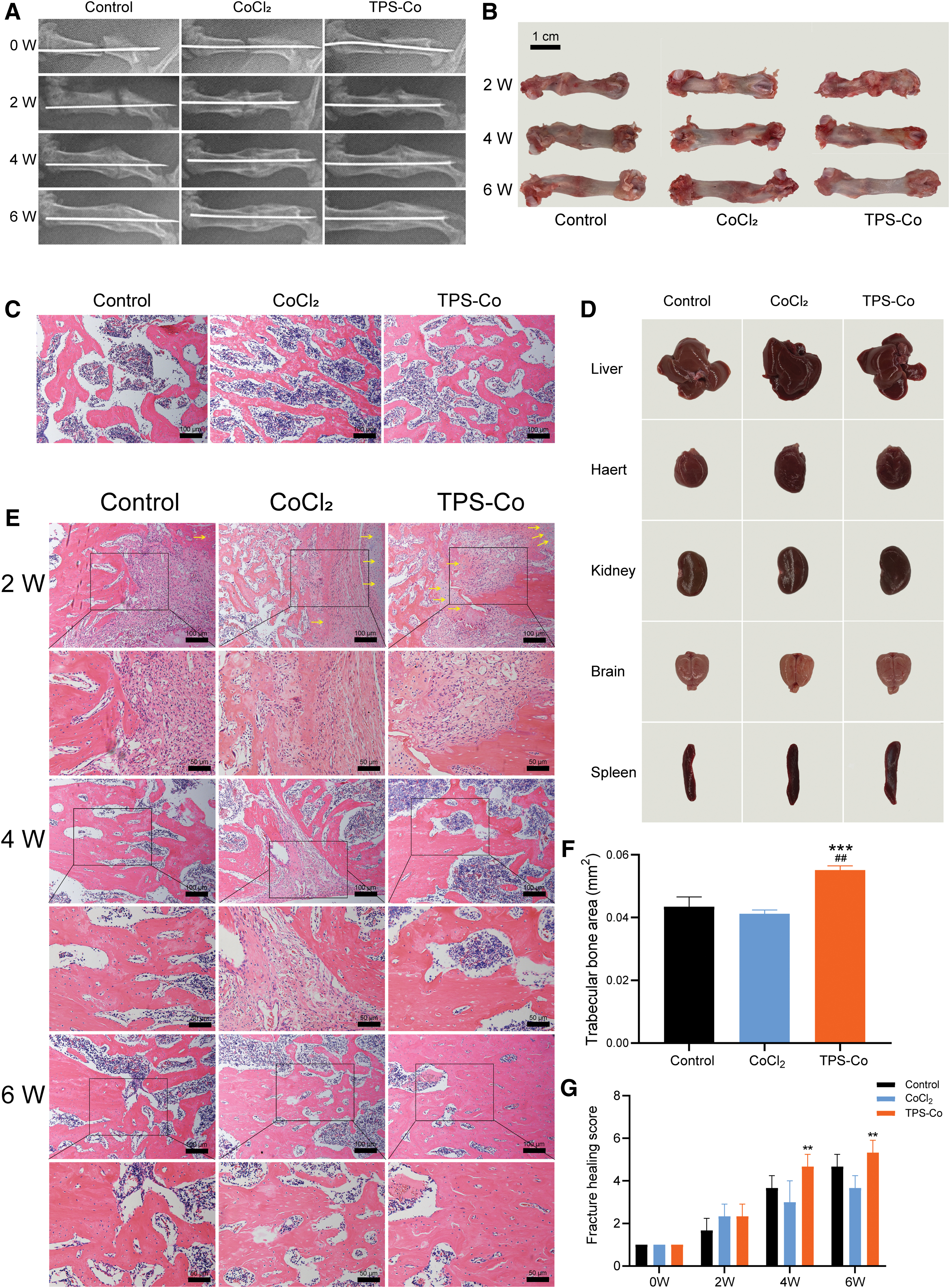
The femoral fracture model of the rats was determined by X-ray imaging after the surgery, and the continuity of the middle femoral bone in the model was interrupted by X-ray films (Fig. 1A). Two weeks after the surgery, X-ray films showed prominent enlargement of the fibrous callus in the control group, but the fracture line was clear. In the CoCl2 group and the TPS-Co group, a small amount of fibrous callus filling and bridging was observed at the fracture end, and the fracture line was slightly blurred. Four weeks after the surgery, the X-ray films showed prominent fracture lines in the control group and the CoCl2 group. The fracture bridging in the CoCl2 group was weaker, and the fracture end connection was not anastomosed compared to that in the control group. The TPS-Co could resolve this problem; the fracture line became blurred, and the fracture end bridge was complete.
TPS-Co promoted femoral fracture healing in rats.
Six weeks after the surgery, the X-ray films showed that the fracture line had merged in the control group, but a significant gap was present at the fracture site in the CoCl2 group, which was not significantly improved compared to the situation 2 weeks ago. In the TPS-Co group, the fracture line was almost invisible, the bone marrow cavity was recanalized, and the effect of promoting fracture recovery was the most significant. By comparing the radiographic scores of X-rays in each group (Fig. 1G), we found that the scores of the TPS-Co treatment group were higher than those of the control group and the CoCl2 group 2, 4, and 6 weeks after surgery. The TPS-Co group had the highest scores at all time points, and the scores were significantly higher than those of the CoCl2 group 4 and 6 weeks after surgery (p < 0.01).
After 6 weeks, the results of gross examination of rats' organs showed that there were no obvious hyperemia, edema, atrophy, necrosis, and other organic lesions in the heart, kidney, brain, and other organs in each group, and no obvious toxic reactions were observed (Fig. 1D). However, the color of blood-rich organs such as liver and spleen changed. In the Control group, the liver color was reddish-brown, and the spleen was dark red. The color of liver and spleen in the CoCl2 group was darker and darker, which may be caused by the stimulation of free cobalt ions and the damage of liver cells and spleen cells to a certain extent. The color of liver and spleen in the TPS-Co group was similar to that in the Control group, indicating that the toxicity of TPS-Co was weaker than that of CoCl2.
The healing of the rat femur was photographed, as shown in Figure 1B. Two weeks after the surgery, the callus was completely ossified to form a completely bony callus. Expansion of the fibrous callus was observed in the control group but not in the CoCl2 group. We also detected inflammatory reactions at the fracture ends. However, TPS-Co treatment resulted in more callus growth and reduced this inflammatory response. Four weeks after the surgery, the fracture ends of the control group were firmly bridled, and a fracture line was observed at the fracture site. In the CoCl2 group, fracture bridging was incomplete, and a fracture gap was prominent at the fracture end.
The condition was better in the TPS-Co treatment group, where the callus outside the fracture site was remodeled, and no fracture line was visible. Six weeks after the surgery, the callus outside the fracture site in the control group was remodeled, and the fracture line was blurred. In the CoCl2 group, the callus outside the fracture site was slightly remodeled, and a prominent fracture line was still visible. In the TPS-Co group, the callus outside the fracture site was almost completely remodeled, and the cortical bone density was close to the level normally found in the bone.
H&E staining was performed at the femoral fracture site of the rats 2, 4, and 6 weeks after surgery (Fig. 1E). Two weeks after the surgery, a few mesenchymal cells and many fibroblasts were observed in the control group, and the fracture ends mainly consisted of loosely arranged fibrous connective tissue. In the CoCl2 and TPS-Co groups, chondrocytes, many fibroblasts, osteoblasts, osteocytes, and neovascularization started forming closely arranged fibrous connective tissue. Some osteoid appeared at the fracture ends, which enabled the bridging of the fracture ends initially. Notably, chondrocytes were observed only at this stage (indicated by the yellow arrow). Only a few chondrocytes could be observed in the control group, some chondrocytes in the CoCl2 group, and a large number of chondrocytes were observed in the TPS-Co group.
Four weeks after the surgery, a bony callus was observed in the control group and the TPS-Co treatment group, and the callus was connected by immature woven bones arranged irregularly. In the CoCl2 group, the process of conversion of fibrous callus to osseous callus was ongoing, and not many woven bones were formed. Six weeks after the surgery, all three groups were in the stage of callus remodeling, and the fracture ends were joined by many new bones. In the TPS-Co treatment group, a large area of mature plate bone was formed, while the callus remodeling in the control group was slow.
Six weeks after the surgery, H&E staining (Fig. 1C) was performed to observe the growth of femoral trabeculae in rats. The semiquantitative results of the trabecular bone area are shown in Figure 1F. The trabecular bone area in the CoCl2 group was lower, while the trabecular bone area in the TPS-Co treatment group was significantly higher compared to that in the control group (p < 0.01). The trabecular bone area was significantly higher in the TPS-Co group compared to that in the CoCl2 group (p < 0.001). Thus, TPS-Co significantly promoted the formation of the trabecular bone.
These results indicated that CoCl2 inhibited femoral fracture healing in rats, and TPS-Co promoted fracture healing. In addition, fracture healing in the TPS-Co group was better than that in the control group.
Effect of TPS-Co on bone formation
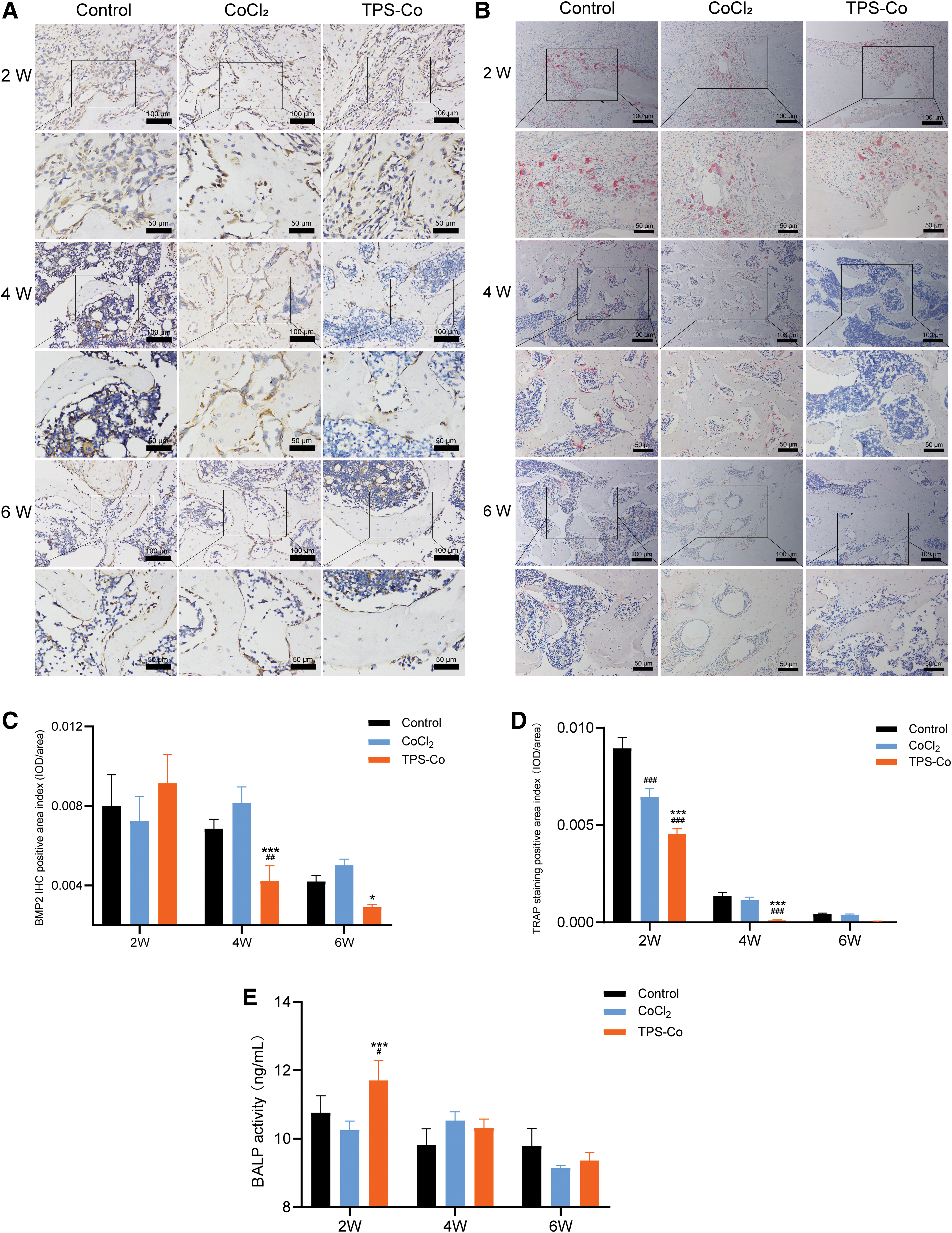
IHC staining of BMP2 (Fig. 2A) and semiquantitative analysis of the positive area in static tissue (Fig. 2C) were conducted 2, 4, and 6 weeks after surgery. The results showed that TPS-Co promoted the expression of BMP2 at the early stage of fracture repair. Two weeks after surgery, the level of BMP2 was high in all three groups. The expression of BMP2 was lower in the CoCl2 group and higher in the TPS-Co treatment group compared to that in the control group. Four weeks after surgery, BMP2 levels were higher in the CoCl2 group compared to that in the control group. TPS-Co decreased the level of BMP2 significantly (p < 0.01). The BMP2 level in the TPS-Co treatment group was significantly lower than that in the CoCl2 group (p < 0.001).
The effect of TPS-Co on bone formation in rats.
Six weeks after the surgery, the expression of BMP2 was low in all three groups. The expression of BMP2 was higher in the CoCl2 group than that in the control group. The expression of BMP2 in the TPS-Co group was significantly lower than that in the CoCl2 group (p < 0.05).
We performed TRAP staining (Fig. 2B) and semiquantitative analysis of the positive area of static tissue (Fig. 2D) in the fracture callus of rats 2, 4, and 6 weeks after the surgery. Our results indicated that cobalt had a stronger inhibitory effect on osteoclast formation, and TPS-Co had a stronger inhibitory effect on osteoclast formation than CoCl2. Two weeks after the surgery, the osteoclast function of the three groups was high. The number of osteoclasts in the CoCl2 group was significantly lower than that in the control group (p < 0.001). The number of osteoclasts in the TPS-Co treatment group was significantly lower than that in the CoCl2 group (p < 0.001). Four weeks after surgery, the number of osteoclasts in the CoCl2 group and the control group was similar. The TPS-Co treatment group had a significantly lower level of osteoclasts than the control and CoCl2 groups (p < 0.001).
We performed a BALP analysis 2, 4, and 6 weeks after the surgery (Fig. 2E). TPS-Co increased serum BALP in rats at the early stage of fracture repair. Two weeks after surgery, the BALP level in the CoCl2 group was lower, while it was significantly higher in the TPS-Co treatment group compared to that in the control group (p < 0.05). Four weeks after surgery, the BALP levels increased in the CoCl2- and TPS-Co-treated groups compared to that in the control group, but the difference was not significant. Six weeks after surgery, BALP levels decreased in the CoCl2 and TPS-Co treatment groups compared to that in the control group, but the difference was not significant.
Effect of TPS-Co on angiogenesis
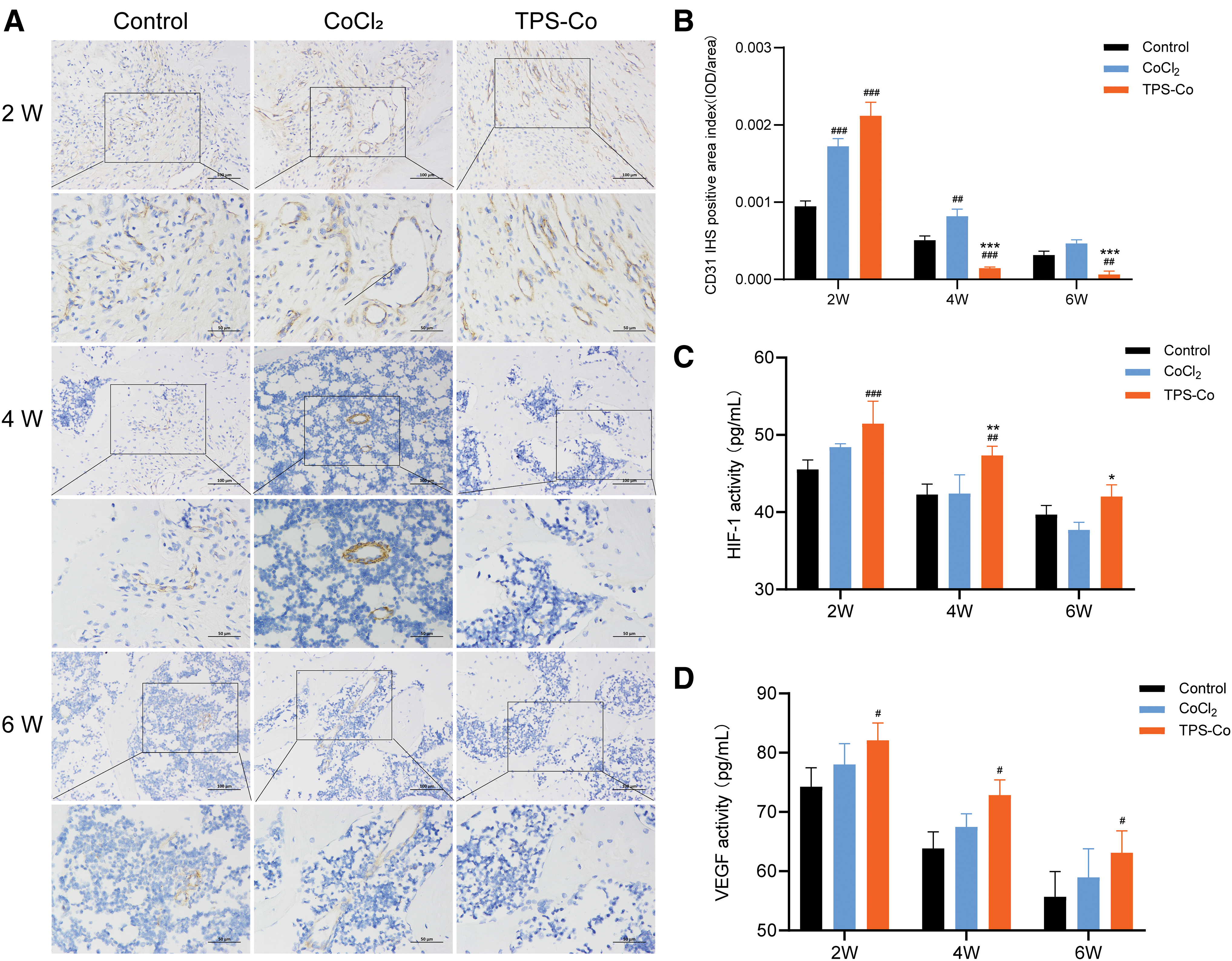
Angiogenesis greatly facilitates bone defect repair. CD31 IHC staining of the rat fracture callus was performed 2, 4, and 6 weeks after surgery to identify specific markers of vascular endothelial cells (Fig. 3A). Semiquantitative immunohistochemistry analysis can reflect the degree of neovascularization in callus tissue during fracture healing (Fig. 3B). The results showed that TPS-Co strongly promoted angiogenesis in the callus at the early stage of fracture repair in rats. Two weeks after surgery, more neovascularization was observed in the CoCl2 and TPS-Co treatment groups than in the control group, and CD31-positive area was more than two times higher in the CoCl2 and TPS-Co treatment groups than in the control group (p < 0.001).
The effect of TPS-Co on angiogenesis in rats.
Four weeks after surgery, the positive area index of CD31 immunohistochemistry in the CoCl2 group was significantly higher than that in the control group (p < 0.01), But the index was significantly lower in the TPS-Co group (p < 0.001). The TPS-Co treatment group had a significantly lower IHC-positive area index than the CoCl2 group (p < 0.001). Six weeks after the surgery, the positive area index of CD31 immunohistochemistry in the CoCl2 group was significantly higher than that in the control group (p < 0.05), but the index in the TPS-Co group was significantly lower (p < 0.01). The TPS-Co treatment group had a significantly lower IHC-positive area index than the CoCl2 group (p < 0.001).
Hypoxia promotes HIF-1 expression, thus regulating cellular oxygen homeostasis. The analysis of serum HIF-1 was performed 2, 4, and 6 weeks after the operation (Fig. 3C), and TPS-Co treatment was found to increase the serum HIF-1 in rats. Two weeks after the operation, the level of HIF-1 in the CoCl2 group was higher than that in the control group. The level of HIF-1 was significantly higher in the TPS-Co treatment group than in the control group (p < 0.001). The level of HIF-1 was higher in the TPS-Co treatment group than in the CoCl2 group.
The levels of HIF-1 in the CoCl2 group and the control group were comparable 4 weeks after the operation. The TPS-Co treatment group had significantly higher HIF-1 levels than the control and CoCl2 groups (p < 0.01). Six weeks after surgery, HIF-1 levels were lower in the CoCl2 group and higher in the TPS-Co treatment group compared to that in the control group. The level of HIF-1 was significantly higher in the TPS-Co treatment group than that in the CoCl2 group (p < 0.05).
VEGF is a provascular endothelial cell growth factor that promotes angiogenesis. Serum VEGF analysis was performed 2, 4, and 6 weeks after surgery (Fig. 3D). The results at each time point showed that the VEGF levels increased in the CoCl2 group and significantly increased in the TPS-Co treatment group compared to that in the control group (p < 0.05). Thus, TPS-Co treatment significantly increased serum VEGF levels in rats.
Discussion
In our study, we evaluated the effects of cobalt compounds and organocobalt complexes on fracture healing in rats using a rat femoral fracture model. We found that the rate of fracture healing of rats treated with CoCl2 decreased, while the rate of fracture healing of rats treated with TPS-Co increased significantly. Liu et al. 33 showed that 1 ppm of cobalt in cobalt-containing solid materials significantly promoted bone regeneration in rats, while 5 ppm of cobalt hindered the bone healing process. The toxicity of cobalt can be decreased, while its excellent biological effect can be preserved by adjusting the dose of cobalt. The preparation of cobalt as a complex might be a more effective strategy.
BMP2 is a major factor inducing bone and cartilage formation in vivo, and its expression increases during the early stage of fracture repair.34,35 The activity of BALP is often increased during bone formation and development.36,37 The results of our experiments showed that BMP2 and serum BALP levels increased after 2 weeks of TPS-Co treatment. This suggested that the osteogenic environment in the TPS-Co-treated group was beneficial. After 4 and 6 weeks of treatment, BMP2 and BALP levels decreased in the TPS-Co treatment group relative to that in the Control and CoCl2 groups (Fig. 2). This indicated that the rats in this group had a shorter fracture repair process and entered the late stage of fracture repair prematurely, which caused BMP2 and BALP to gradually return to normal levels.
The osteoclastogenesis system strongly influences bone formation and function; bone formation requires a balance between osteogenesis and osteoclast production. Osteoclasts are important for bone maturation and function. However, the overactivation of osteoclast generation might affect bone regeneration negatively. 38 TRAP staining showed that Co can inhibit the formation of osteoclasts, and TPS-Co had a stronger effect than CoCl2 (Fig. 2). Also, CoCl2 (10 mg/kg) negatively affected the expression of BMP2 and BALP at the early stage of fracture repair, while TPS-Co accelerated the process of bone regeneration by upregulating the expression of BMP2 and BALP and inhibiting osteoclasts at the early stage of fracture repair.
Regarding angiogenesis and regeneration, Co ions can induce hypoxia-like responses and significantly enhance the formation of new blood vessels and new bone tissue in vivo. After 2 weeks of TPS-Co treatment, the results of the CD31 IHC analysis showed increased angiogenesis. The expression of HIF-1 and VEGF was upregulated, indicating active vascularization in the early stage (Fig. 3). HIF-1 can regulate the expression of a variety of growth genes, thereby affecting the growth and development of cartilage. This was also verified by the histological results. As bone formation progresses, newly formed bone tissue gradually develops into mature plate bone. 39 The newly formed blood vessels then continue growing and developing to accommodate the deposition of new bone material. Therefore, in the later stages of fracture repair, the original fresh granulation tissue gradually degenerates, leading to a decrease in the number of blood vessels.40,41
Although the rate of angiogenesis decreased in the TPS-Co-treated group after 4 and 6 weeks of treatment, this does not imply that the TPS-Co treatment negatively affected angiogenesis. Instead, it indicates that fractures in the TPS-Co-treated group were at a late stage of repair, whereas fractures in the control and CoCl2 groups were repaired at an earlier stage. In conclusion, we found that the probone regeneration effect of TPS-Co results from dual regulation of the bone and the vascular system.
These results indicated that fracture repair was accelerated in rats treated with TPS-Co, while CoCl2 negatively affected fracture repair in rats with the same daily intake of cobalt. Some of the adverse effects of inorganic cobalt can be reduced by preparing cobalt as a polysaccharide complex. This strategy can positively regulate the osteoimmune environment, angiogenesis, and bone formation. Our findings were similar to those of another study. 27 Thus, the preparation of cobalt as complexes can effectively reduce the toxicity of cobalt while maintaining its excellent biological activity.
Conclusions
For the same amount of cobalt administered, TPS-Co treatment reduced adverse reactions and accelerated femoral fracture healing compared to CoCl2 treatment in rats. It promoted angiogenesis by upregulating the expression of VEGF and HIF-1. Bone formation was promoted by the upregulation of the expression of BMP2 and serum BALP. TPS-Co positively regulated the skeletal and vascular systems and significantly enhanced bone regeneration outcomes. Therefore, the dark tea polysaccharide cobalt complex can be used as an additive or drug to promote fracture healing, and thus, it has a huge potential market value.
Footnotes
Authors' Contributions
M.Z.: Supervision and Conceptualization; Y.C.: Writing—Original Draft and Investigation; Z.W.: Formal analysis; C.X.: Methodology; Chi Zhou: Data Curation; L. W.: Data Curation; F.X.: Data Curation; L.L.: Visualization; J.X.: Supervision; C.W.: Investigation; H.Z.: Conceptualization and Writing—Review and Editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Key Scientific Instrument Special Project of China's National Natural Science Foundation (Project No. 81727805), Xianning key special project for scientific and technological research and development (2021SFYF003). Hubei University of Science and Technology Research innovation team project (2023T10), Hubei Provincial Department of Education scientific Research Programme (B2019159), Doctor start fund project (BK201803), and Hundred schools and hundred counties project (BXLBX0794, BXLBX0795).