
Abstract
Organoids are three-dimensional (3D) in vitro tissue models that are derived from stem cells and can closely mimic the structure and function of human organs. The ability to create organoids that recapitulate the complex cellular architecture of organs has emerged as an innovative technique in biomedical research and drug development. However, traditional methods of organoid culture are time consuming and often yield low quantities of cells, which has led to the development of 3D bioprinting of organoids from bioinks containing suspended cells and desired scaffolds. A comparison across different organoid-building techniques, focusing on 3D bioprinting and its benefits, may be helpful and was yet to be distinguished. The goal of this review is to provide an overview of the current state of 3D bioprinting of organoids and its potential applications in tissue engineering, drug screening, and regenerative medicine.
Impact statement
The potential benefits of three-dimensional (3D) bioprinted organoids are significant, and as the technology continues to evolve, we can expect to see more applications in disease modeling, drug discovery, and regenerative medicine. However, there are still several challenges that need to be addressed before 3D bioprinted organoids can be routinely used in the clinic. Nonetheless, the future of 3D bioprinting of organoids is exciting, and it has the potential to revolutionize the field of tissue engineering and regenerative medicine.
Introduction
Organoids are three-dimensional (3
Complex protocols have been advanced to successfully build organoids, with 3D bioprinting recently being explored as an easier alternative to construct organoids from scaffolds and single-cell suspension bioinks.
It is important to distinguish organoid from a spheroid, which is a different type of 3D culture. Spheroids are typically scaffold-free cell aggregates of lower complexity and random cell proliferation, whereas organoids are embedded in a matrix gel and display higher organization and polarization.
They can contain multiple cell types, being better suited for long-term cultures. In simpler terms, organoids may be originated from embedding spheroids or single-cell suspensions directly in a scaffold. Ultimately, organoids self-organize into “miniorgans” and typically retain their heterogeneity. 4 On a different note, organoids may have a spheroidal shape. Either 3D culture type may be appropriate, depending on the specific purpose of the experiment.5,6
The ability to create organoids that recapitulate the complex cellular architecture of organs has emerged as an innovative technique in biomedical research and drug development. However, traditional methods of organoid culture are time consuming and often yield low quantities of cells, which has led to the development of 3D bioprinting of organoids. This technique, which has been evolving since the early 2000s, utilizes cells, biomaterials, or active biomolecules as a bioink to print living structures. Thus, these may encompass nondegradable or active degradable biomaterials, as well as living cells that are layered to construct and mimic the environment of a specific 3D tissue.7,8
Other methods to develop organoids include electrospinning 9 ; manually assembling the biological or synthetic ECM scaffold into small droplets to culture in low attachment plates or in micropatterned surface microplates, also coated to be nonadherent 10 ; and microfluidics techniques.3,11 There are some important advantages of utilizing 3D bioprinting over other traditional methods—higher accuracy in spatial architecture design, enabling high-precision organoids; faster and more cost-effective fabrication; and enhanced translational effectiveness 12 (Table 1).
Summary: Main Advantages and Disadvantages of Different Organoid-Building Techniques
2D, two-dimensional; 3D, three-dimensional; CO2, carbon dioxide; MODS, microfluidic organoids for drug screening.
Parihar et al., for instance, describe the potential of 3D-printed human organoids in tackling the high cost and lengthy process of drug screening for personalized therapy and treatment during the COVID-19 pandemic. 13 Although every organoid-building technique presents strong advantages and disadvantages, choosing one seems to depend on the specific end goal and organoid type in study. Overall, 3D bioprinting techniques despite requiring an initial equipment investment seem to be one of the most advanced, highly accurate, and with less complex protocols, similarly to microfluidic techniques, however, with extended versatility in its use.
The goal of this review is to provide an overview of the current state of 3D bioprinting of organoids and its potential applications in tissue engineering, drug screening, and regenerative medicine.
Technological Advancements in Bioprinting
3D bioprinting is an emerging technology that combines 3D printing techniques with biological materials such as cells and biomaterials. This technique has enabled researchers to create complex biological structures with high precision and control. In the context of organoid bioprinting, researchers use a variety of bioprinting methods, including extrusion-based, inkjet-based, and laser-assisted bioprinting, to deposit cells and biomaterials layer by layer to create a 3D structure that mimics the architecture and function of an organoid (Fig. 1).
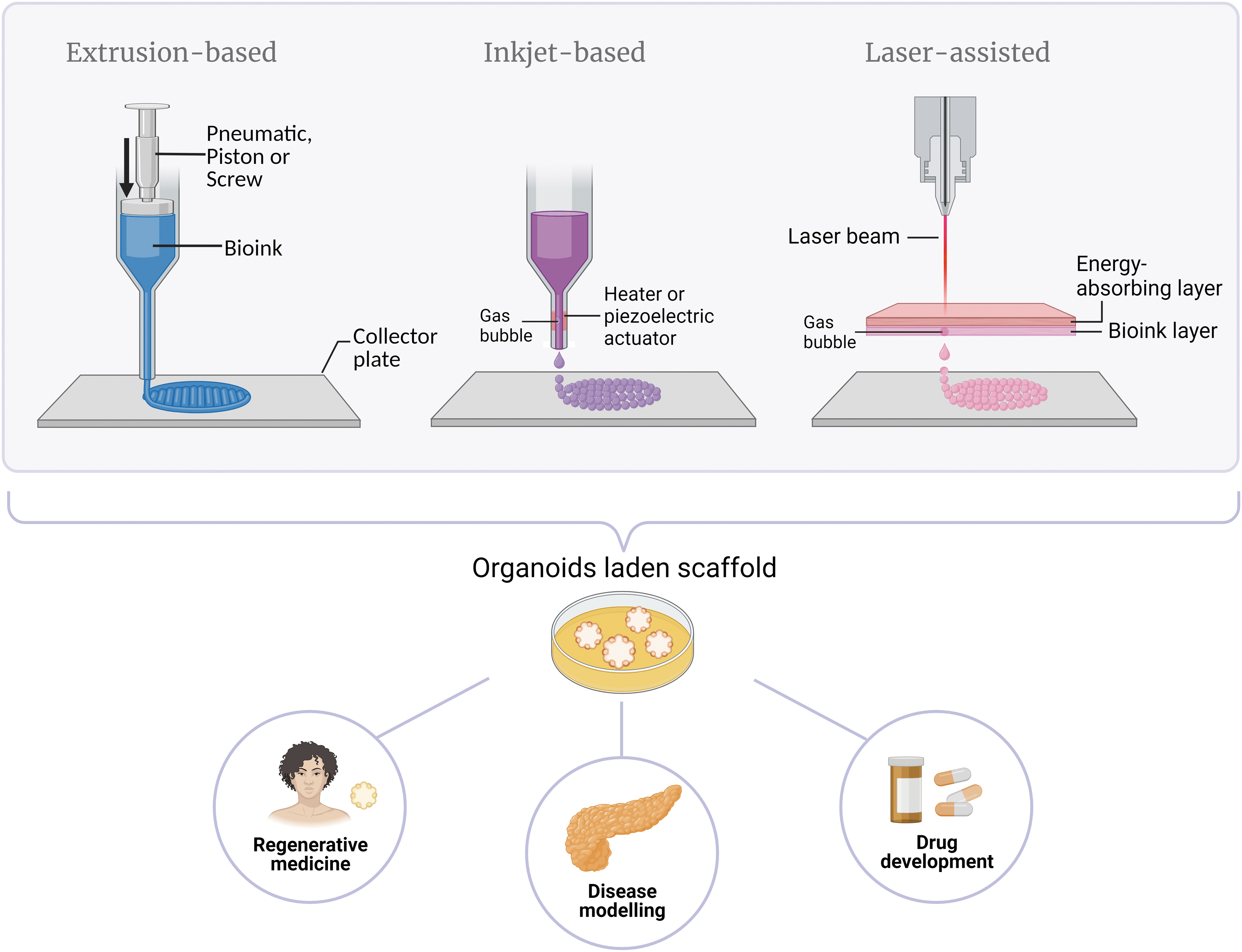
Main 3D bioprinting techniques and the prospects for 3D bioprinting of organoids. 3D, three-dimensional.
Extrusion-based 3D bioprinters, introduced by Landers et al. in 2002, are widely used due to their convenience and versatility.21,22 They utilize pneumatic pressure or mechanical mechanisms, employing a piston or screws to extrude bioink continuously through a nozzle in a three-axis system. For pneumatic pressure, a pump is used to create air pressure. The piston exerts a vertical mechanical force into the surface of the bioink, whereas screws apply rotational forces. This approach allows for the use of a diverse range of cell-dense and high-viscosity bioinks. However, the high mechanical pressure and shear stress generated during extrusion may lead to reduced cell survival rates.12,23
Now it is commercialized by companies such as EnvisionTEC as the “3D-Bioplotter,” and is able to print not only in vitro, but also in situ tissue constructs. 7 Many of these printers have several printing heads to extrude different material components into a single construct. Advances keep being made to suit the specifications of the bioink, such as the incorporation of heating or cooling sleeves surrounding the syringe and hot/cold printing collector plates for physical crosslinking, as well as applying ultraviolet (UV) light for photocrosslinking between each layer or after printing.24,25
Inkjet-based methods were first reported in 1988, although the first inkjet bioprinter was developed by Wilson and Bolan from Clemson University in 2003. 26 These bioprinters operate on a droplet unit building block system, functioning at the picoliter scale, and are controlled using surface tension at the nozzle of the syringe, employing both thermal and piezoelectric principles. Thermal inkjet bioprinters have a thermal actuator that applies burst of energies at very high temperatures (∼200–300°C) in microseconds, generating small bubbles that push the bioink down drop wise.
In contrast, piezoelectric models use a piezoelectric crystal that is charged and contracts, causing vibration plates to pressure and expel the droplets. Some piezoelectric printers also work with acoustic waves. These inkjet bioprinters offer faster printing speeds and lower costs than extrusion-based methods. However, they face limitations in using bioinks with high cell density or viscosity and are known to cause high shear stress, which can damage cells. 27
To address this issue, Takagi et al. introduced a new technology in 2019, altering the architecture of the inkjet bioprinter's printing head to specifically eject live cells and successfully construct Mille-Feuille-like 3D structures containing NIH/3T3 mouse fibroblast and normal human dermal fibroblast cells. The redesigned printing head featured a disk membrane beneath the chamber that holds the cell suspension, along with an annular piezoelectric actuator fixed outside and below that membrane. This arrangement allows the actuator to vibrate with mixing movements, preventing cell clogging at the nozzle aperture. 28
Finally, laser-assisted bioprinting has a higher cost, intermediate speed, but better resolution and cell viability than inkjet printers, since there is no clogging or mechanical damage involved. 12 This technique, based on the laser-induced forward transfer effect, comprises a high-powered laser; a ribbon that includes an energy-absorbing layer usually made of gold or titanium and a bioink layer; and a receiving substrate, where the printed material is collected. The laser beam targets the energy-absorbing layer, heating it up, causing air bubbles to form on its inner side.
An increased pressure will lead bubbles to push and transfer down the bioink to the support plate in a drop-wise manner. The precision is in the micrometer scale, and it allows the usage of a wide range of biomaterials with different viscosities—both in solid and liquid phases—since there is no nozzle or mechanical contact with the bioink. These features provide a higher cell survival rate; however, the energy of the laser may still cause some cell damage. An increase in viscosity and bioink layer thickness is shown to prevent cell death.23,29
One pressing concern across all bioprinting methods, particularly in the biofabrication of organoids, is the challenge of batch-to-batch variability, which significantly impacts accurate quantitative measures, such as those used in drug screening and other applications. To address this issue and promote standardization in organoid bioprinting, cutting-edge technologies are leveraging the power of artificial intelligence (AI).
A notable example is the work of Ipsita Banerjee at the University of Pittsburgh Swanson School of Engineering, who recently received a substantial grant of $500,000 from the National Science Foundation. The primary focus of this research is to explore how AI can play a pivotal role in monitoring and controlling organoid biofabrication processes. By integrating AI algorithms, the aim is to achieve greater homogenization with high resolution, precise size, and optimal functionalization of the organoids, while also enabling the prediction of results. 30
In specific, machine learning algorithms are able to analyze data, then optimize and create what is the most efficient method to create an organoid in a way that variability is reduced (with higher efficiency in synthesis of scaffold, better culture conditions, and external stimuli, among others). Combined with 3D bioprinting, the ability to monitor culturing conditions enables a better assessment of how to maintain specific organoid sizes, as well as make a preclinical evaluation and possible application of these AI-enabled organoids. An example would be observing the processes of organoid development and growth and translating this to the human development of a specific disease. 31
Organoid Bioprinting
Organoid bioprinting has several advantages over traditional methods of organoid culture. Bioprinted organoids can be produced in larger quantities, making them more suitable for high-throughput screening. This is a major advantage, especially compared with manually embedding live cells or embryoid bodies into a scaffold by creating small droplets. Pipetting these individually in temperature-sensitive biomaterials, such as Matrigel, for instance, is extremely laborious. When using Matrigel, the embedding process has to be performed very quickly and on ice before incubation at 37°C to solidify the droplets. It is a procedure quite prone to human error or mishandling, not to mention that droplet sizes or shapes may not be completely homogeneous (Fig. 2).
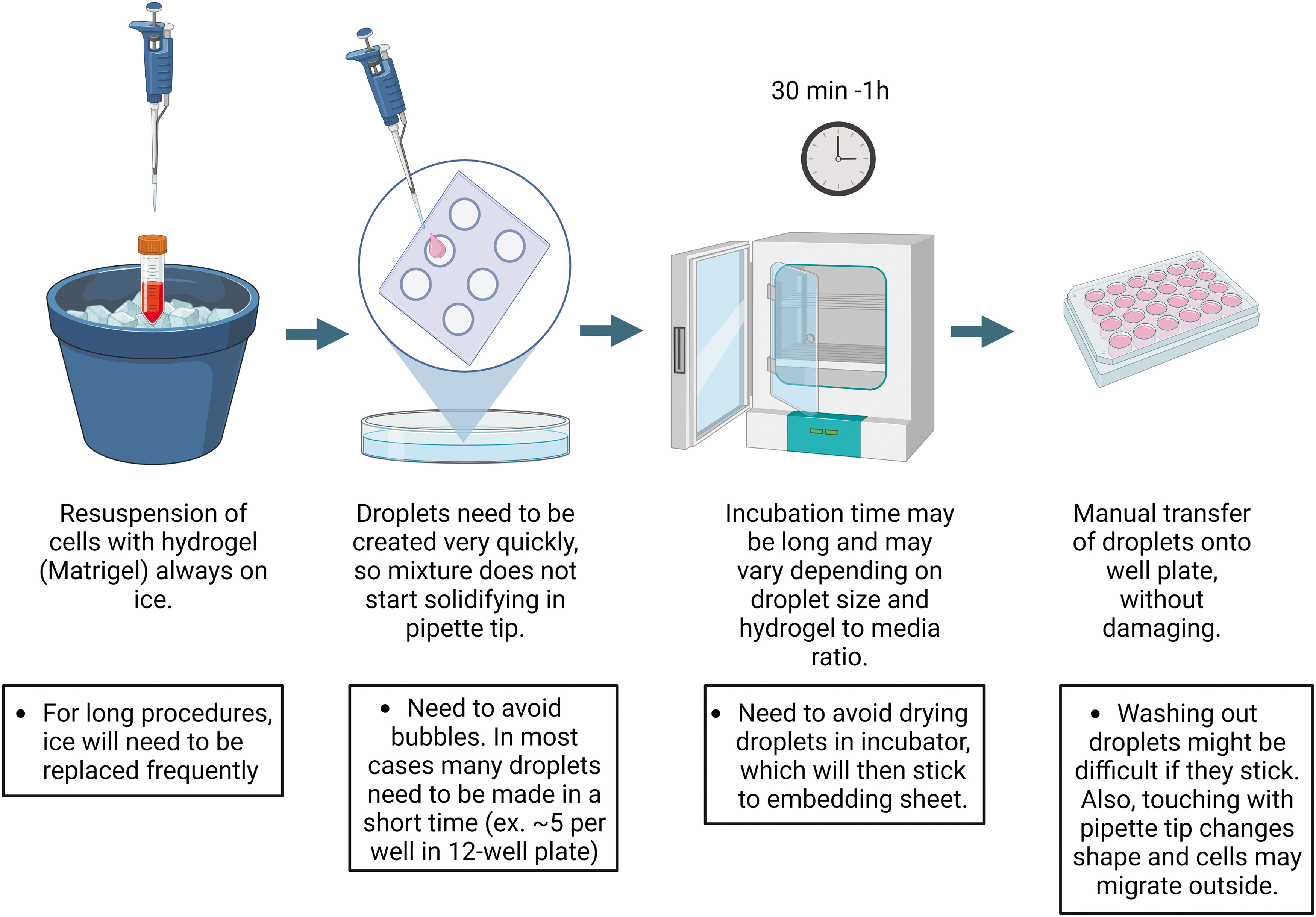
Steps for manual assembly organoid-building technique and some challenges associated.
3D bioprinting is able to standardize organoids in a more controlled and faster environment. Although an initial investment may have to be made, to acquire a bioprinter that accommodates thermosensitive biomaterials, there is most likely less waste in resources and, in consequence, less extended duration of an experiment due to mishandling of these. In addition, the ability to print different cell types in a specific spatial arrangement can better replicate the complex interactions that occur in the body.
As previously explored with traditional techniques, bioprinted organoids can also be personalized by using a patient's own cells to create organoids that mimic the patient's disease and test various treatments in a controlled environment. There are already studies utilizing patient-derived cells to bioprint cancer models that biologically represent the individual patient's tumor. In 2022, Chen et al. report to have acoustically bioprinted patient-derived microtissues that model cancer invasiveness and predict treatment response. 32
Organoid bioprinting can be achieved through various bioprinting methods, with extrusion-based and laser-assisted bioprinting being the most commonly used techniques. In contrast, inkjet printers may not be ideal for this application due to their limitations in handling low-viscosity bioinks and lower cell densities, making the construction of complex organoid structures challenging. 12 To achieve better outcomes, different laboratories have adapted and customized extrusion bioprinters to suit their specific needs.
For instance, Bertassoni's group modified a NovoGen MMX Bioprinter™ (Organovo) originally equipped with two nozzles, one for aspirating and dispensing cells and the other for handling hydrogels separately. In their modified setup, they successfully bioprinted hepatocyte and fibroblast cells encapsulated in a GelMA hydrogel in a single step. The use of a metallic piston surrounded by a glass capillary enabled the aspiration and photopolymerization of the cells suspended in GelMA with an incorporated UV light, whereas coordinated motion of the X–Z robot and motorized stage facilitated the bioprinting process of cell-laden GelMA hydrogel fibers. 33
Tomaskovic-Crook et al. took an alternative approach to print human cerebral organoids in a GelMA scaffold, using a 3D Bioplotter. In their method, the cells and hydrogel were not mixed together. A prepolymerized solution of GelMA was loaded into the syringe barrel of the printer and then extruded onto a multiwell array using a piston. Subsequently, the GelMA scaffold was photo-crosslinked with UV light, and iPSCs were seeded on top of the GelMA layers to initiate organoid formation. 20
A third study introduced an intriguing extrusion-based printing method known as bioprinting-assisted tissue emergence. This innovative technique, when combined with a microscope system, allows for the bioprinting of organoids and their reorganization into specific shapes, serving as building blocks for large-scale tissues instead of random shapes. The microscope component provides live images, enabling spatial and temporal control over tissue development during the bioprinting process. 34
These diverse approaches showcase the versatility and potential of organoid bioprinting, as researchers continually explore and refine techniques to construct highly intricate and functional organoid structures.
Applications of Bioprinted Organoids
The applications of bioprinted organoids are vast and include disease modeling, drug discovery, and regenerative medicine. In disease modeling, bioprinted organoids can be used to study diseases such as cancer, Alzheimer's disease, and cystic fibrosis. These are important preclinical studies and possible alternatives to animal models that might not recapitulate as accurately the clinical features of the disease/disorder manifested in the human environment. Bioprinted disease models may be based on human cells and be patient derived, providing a more accurate simulation of the 3D in vivo microenvironment and facilitating a comprehensive study of the interactions between pathological and healthy cells.26,35
As one of the leading causes of death worldwide, cancer is an extensively studied disease, although very challenging due to its complexity. Despite its difficulty, researchers attempt modeling in vitro tumors to study their occurrence and invasiveness. Shuangshuang Mao's group used patient-derived primary tumor cells to 3D bioprint intrahepatic cholangiocarcinoma tumor models, using a composite hydrogel system of gelatin–alginate–Matrigel.
Here they were able to confirm the invasive and metastatic phenotype of these tumor organoids, by measuring the expression levels of specific markers, matrix metalloproteinases (MMPs), the index of tumor fibrosis and liver function, among others. 36 Alzheimer's disease, a complex neurodegenerative disorder that remains elusive to scientists due to the limited accessibility of human brain tissue, necessitates alternative and advanced model systems.
In this context, 3D cerebral organoids derived from human pluripotent stem cells emerge as a good alternative to recapitulate the human Alzheimer's disease (AD) pathophysiology. 37 Zhang et al. reported the use of human neural progenitor stem cells to bioprint AD organoids with 2% Matrigel and 2% alginate as bioinks. They were able to mimic the tissue microenvironment and demonstrate an increase in Aβ proteins, as well as in gene expression of Aβ and tau, which are often associated with the progression of Alzheimer's disease. 38
Bioprinted organoids can also be used to test the safety and efficacy of drugs in a more human-like environment. One of the main advantages is the high reproducibility and predictive value for the clinical outcome. 3 In the toxicology field, organoids bioprinted from immortalized lung cells have been developed to test the toxicity of silver nanoparticles that are absorbed through contact or inhalation and were compared with 2D model counterparts. Results showed that cells were more viable in the 3D environment than in the 2D model and were able to be sustained for longer cultures, showing a reduction in oxidative stress over time.
With such dissimilarity of data between 2D and 3D models, Gerbolés et al. stress the importance of considering 3D protocols that better mimic the human in vivo environment, while supporting the replacement, reduction, and refinement (3Rs). 39 In cancer biology, there is also an urgent need for treatment with effective and patient-personalized drugs.
Xie et al. aim to address effective treatments for hepatocellular carcinoma (HCC) (liver cancer), by 3D bioprinting hepatorganoids with primary HCC cells isolated from patients. These are mixed with gelatin and sodium alginate to form the bioink. They declare to have developed a faithful model that retained parental features of HCCs, while capable of providing intuitive and quantitative drug screening results. 40
In regenerative medicine, bioprinted organoids can be used to create replacement organs, which would reduce the reliance on organ donation. Although printing large-scale functional tissues or complete organs remains a formidable challenge, significant progress has been made in constructing simple 3D-printed living tissues and organoids that hold promising applications in the treatment of in vivo tissues. 26
A notable example of such progress is the study of Kang et al., who developed the integrated tissue–organ printer, a 3D bioprinting system capable of producing human-scale tissue constructs with structural integrity. Leveraging computer modeling, this innovative system enables precise control of the motion of the printing nozzles, and the incorporation of microchannels facilitates essential nutrient diffusion to support cell viability. Presently, they have successfully fabricated tissues such as mandible and calvarial bone, cartilage, and skeletal muscle. 41
In another study, Bernal's group performed volumetric bioprinting of liver organoids using gelatin hydrogels, guided by an optical tomography system. Bioprinted organoids attained complex structures in the centimeter scale within a matter of seconds. These organoids faithfully recapitulated key features of the human liver, showcasing hepatocytic differentiation, liver-specific enzymatic activity, among others. Such findings hold tremendous promise and present astonishing possibilities for advancements in the field of regenerative medicine. 42
Challenges in Bioprinted Organoids
Despite the promise of 3D bioprinted organoids, there are still several challenges that need to be addressed. One of the main challenges is ensuring the cells and biomaterials are compatible with the bioprinting process and that the resulting structure is stable and functional. This is particularly challenging for inkjet-based printers, which have low drive pressure and are not well suited for high-viscosity biomaterials typically required for organoid fabrication, leading to printing head clogging issues. Laser-assisted printing offers advantages in this regard but may introduce side effects on the cells due to laser irradiation.
Researchers are also exploring different types of biomaterials that can mimic the ECM and provide a suitable environment for cell growth and differentiation. Bioinks need to exhibit good printability while also influencing cell behavior positively. Some popular bioinks include agarose, alginate, collagen, hyaluronic acid-based materials, among others.12 In addition, more advanced bioprinters are needed that can deposit multiple cell types and biomaterials simultaneously. A few extrusion-based printers have shown promise in this regard. Expanding these capabilities to laser-assisted printers could further enhance the benefits of this printer modality.
The fact that the acquisition of 3D bioprinting equipment may be an expensive initial investment is a challenge, especially if specific features, such as accommodation for thermosensitive biomaterials with a control system, are needed. Laboratories would need to consider this initial cost beneficial for the long-term cost-effectiveness of organoid building with higher accuracy and speed. One significant limitation of current organoids is the lack of a complete vasculature system, hindering efficient nutrient delivery and diffusion throughout the structure.
Efforts are underway to introduce a functional vascular network into organoid models, but this remains an ongoing challenge for researchers. Furthermore, ethical and regulatory considerations must be taken into account, such as the use of stem cells and the potential for unintended consequences.
Conclusion
The potential benefits of 3D bioprinted organoids are significant, and as the technology continues to evolve, we can expect to see more applications in disease modeling, drug discovery, and regenerative medicine. Although extrusion-based and laser-assisted bioprinters are currently the favored choices for organoid fabrication, other methods such as inkjet and photocuring bioprinters are also being explored. There are still several challenges that need to be addressed before 3D bioprinted organoids can be routinely used in the clinic. However, ongoing efforts to improve resolution and complexity by modifying bioprinters, integrating computer models, microscopes, and AI technologies are promising steps toward mimicking the human body more accurately.
By guiding the precise location of each cell type within the organoid's architecture, these advances bring us closer to creating specific organoid shapes and functionalities. The development of 3D bioprinted organoids marks a crucial advancement, bridging the gap between 2D model studies and animal models, with the potential to eventually replace the latter. Emphasizing the support for the 3Rs principle, it is essential to explore every avenue that aligns with ethical considerations and advances in technology. Excitingly, the future of 3D bioprinting of organoids holds the potential to revolutionize tissue engineering and regenerative medicine.
Footnotes
Acknowledgment
The authors thank Stony Brook University for supporting this study.
Authors' Contributions
M.C., K.C., and D.Z. contributed to conceptualization and project administration; M.C. was involved in writing—original draft, investigation, methodology, data curation, formal analysis, and resources; D.Z. carried out supervision and funding acquisition; and K.C. and D.Z. took charge of writing—review and editing, validation, and visualization.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.