
Abstract
Volumetric muscle loss (VML) is the loss of skeletal muscle that exceeds the muscle's self-repair mechanism and leads to permanent functional deficits. In a previous study, we demonstrated the ability of our scaffold-free, multiphasic, tissue-engineered skeletal muscle units (SMUs) to restore muscle mass and force production. However, it was observed that the full recovery of muscle structure was inhibited due to increased fibrosis in the repair site. As such, novel biomaterials such as hydrogels (HGs) may have significant potential for decreasing the acute inflammation and subsequent fibrosis, as well as enhancing skeletal muscle regeneration following VML injury and repair. The goal of the current study was to assess the biocompatibility of commercially available poly(ethylene glycol), methacrylated gelatin, and hyaluronic acid (HA) HGs in combination with our SMUs to treat VML in a clinically relevant large animal model. An acute 30% VML injury created in the sheep peroneus tertius (PT) muscle was repaired with or without HGs and assessed for acute inflammation (incision swelling) and white blood cell counts in blood for 7 days. At the 7-day time point, HA was selected as the HG to use for the combined HG/SMU repair, as it exhibited a reduced inflammation response compared to the other HGs. Six weeks after implantation, all groups were assessed for gross and histological structural recovery. The results showed that the groups repaired with an SMU (SMU-Only and SMU+HA) restored muscle mass to greater degree than the groups with only HG and that the SMU groups had PT muscle masses that were statistically indistinguishable from its uninjured contralateral PT muscle. Furthermore, the HA HG, SMU-Only, and SMU+HA groups displayed notable efficacy in diminishing pro-inflammatory markers and showed an increased number of regenerating muscle fibers in the repair site. Taken together, the data demonstrates the efficacy of HA HG in decreasing acute inflammation and fibrotic response. The combination of HA and our SMUs also holds promise to decrease acute inflammation and fibrosis and increase muscle regeneration, advancing this combination therapy toward clinically relevant interventions for VML injuries in humans.
Impact statement
Volumetric muscle loss (VML) is a clinically relevant problem for which current treatment methods are limited and are not 100% effective. Tissue-engineered skeletal muscle and commercially available hydrogels (HGs) are promising novel therapeutic options. This study aimed to access the biocompatibility of commercially available poly(ethylene glycol), methacrylated gelatin, and hyaluronic acid HGs in combination with our tissue-engineered skeletal muscle units to treat VML in a clinically relevant large animal model (sheep) after a 6-week recovery.
Introduction
Despite the innate regenerative capacity of skeletal muscle, traumatic injuries such as volumetric muscle loss (VML) overwhelm the muscle's self-repair mechanism and result in irrecoverable loss of muscle tissue and lead to fibrotic scar tissue in the defect site.1–3 These injuries impact both civilian and military populations alike, contributing to an annual health care expenditure of $800 billion dollars in the United States. 4 Nevertheless, the military demographic experiences a disproportionate effect from VML injuries, accounting for ∼77% of battlefield injuries and resulting in health care expenses ranging between $340,000 and $440,000 per patient.4,5
Current standard of care for VML injuries involves surgical muscle transfer by translocating autogenic tissue from a donor site into the wound. 6 However, this treatment is limited by tissue availability, poor engraftment, and donor site morbidity, as well as poor vascularization and denervation, which can lead to incomplete cosmesis and functional deficits.7–9 As a result, there has been an emphasis on developing tissue engineering technologies as a promising treatment option for large-scale VML injuries as it has the ability to resolve the issues of tissue availability and morbidity associated with current therapeutic options.10,11
Specifically, our laboratory has developed scaffold-free, multiphasic, tissue-engineered skeletal muscle units (SMUs). Previous studies from our laboratory have demonstrated the success of our SMUs in restoration of muscle function following a 30% VML injury in rat and sheep.12–16 Following 3- and 6-month studies to assess the effectiveness of the SMU to repair VML in a sheep model, we demonstrated the ability of our SMUs to restore muscle mass to a degree statistically indistinguishable from the contralateral muscle. However, histological analyses of the muscles repaired with the SMU showed significant fibrosis and poor structural recovery, which have been attributed to acute inflammation and increased fibrosis in muscle tissue.17,18
Because excessive fibrotic infiltration of the repair site is one of the biggest obstacles for regeneration of healthy skeletal muscle tissue,19,20 various regenerative medicine strategies, such as hydrogels (HGs), are being developed to decrease the acute inflammation and fibrosis that occur with VML.21,22 HGs are water-swollen polymer networks that can be engineered to develop highly tunable, biocompatible, nonimmunogenic biomaterials to acutely protect the implanted tissue from acute inflammation and fibrosis. Because of their high-water content and porosities, HGs are ideal materials that embody environments for cell survival and structures that mimic native tissues and thus have promise in preventing fibrotic capsule formation.23,24 Hyaluronic acid (HA)-based HGs, for example, embody material features that play an integral role in encouraging tissue development and repair. 25 Thus, in combination with our SMU technologies, we hypothesized that the combination of HG and our SMU technology would reduce acute inflammation and fibrotic infiltration and enhance the capabilities of the SMU for VML repair.
To study the efficacy of the HG and SMU combination to repair VML in a clinically relevant large animal model, we created an acute 30% VML injury in the ovine peroneus tertius (PT) muscle and repaired the defect using SMUs large enough to fill the 30% VML site. We evaluated muscle structure after a 6-week recovery. Previous studies have demonstrated the effectiveness of our scaffold-less tissue-engineered approaches in rat VML model 12 and in sheep models of tendon, 26 ligament, 27 and muscle repair.17,18 To supplement the SMU engraftment, three prominent HGs [poly(ethylene glycol) (PEG), methacrylated gelatin (GelMA), and HA HGs] were chosen to be implanted in the VML site either alone or along with an SMU graft. These HGs were chosen for their demonstrated efficacy in reducing fibrotic response and embody features for robust muscle regeneration.25,28,29
Therefore, the goal of this study was to better understand the biocompatibility of PEG, GelMA, and HA HGs in an ovine VML model and select the HG with the least inflammation, measured as swelling of the incision site and white blood cell (WBC) counts at day 7 of recovery. The most promising HG would then be implanted in conjunction with our SMUs and evaluated for its ability to restore muscle mass following a 6-week recovery period in a clinically relevant large animal model: sheep receiving an acute 30% VML injury in the PT muscle before no treatment (VML-Only), treatment in the form of the HG only (PEG, GelMA, HA), SMU only (SMU-Only), or SMU and HA HG (SMU+HA).
Materials and Methods
Animal care
Ten-week-old castrated male Polypay breed sheep (n = 30 sheep ordered from Oswalt Farm, weight = 19–32 kg) were determined to be healthy by physical examination by a veterinarian at the University of Michigan's Unit for Laboratory Animal Medicine (ULAM). All sheep were housed in groups within American Association for Accreditation of Laboratory Animal Care accredited large animal facilities for the duration of the study and randomly assigned to one of six experimental groups: VML-Only (n = 5), PEG (n = 5), GelMA (n = 5), HA (n = 5), SMU-Only (n = 5), SMU+HA (n = 5). The left hind leg was designated as the experimental VML injury and repaired. The unoperated contralateral right hind leg served as the control for all animals in the study. All animals were acclimated to the ULAM husbandry facilities for at least one week before any procedure. Sheep were given access to food and water ad libitum. All animal care and animal surgeries were performed in accordance with The Guide for the Care and Use of Laboratory Animals, 30 and the experimental protocol was approved by the University of Michigan's Institutional Animal Care and Use Committee.
SMU fabrication
As previously described,17,18 frozen skeletal muscle cell isolates harvested from the PT of sheep muscle were thawed and provided muscle growth media (MGM) (60% F-12 Kaighn's Modification Nutrient Mixture [Gibco; cat. no. 21127-022], 24% Dulbecco's modified Eagle's medium with GlutaMAX supplement [DMEM; Gibco; cat. No. 10564-011], 15% fetal bovine serum [FBS; Gibco; cat. no. 10437-028], 2.4 ng/mL basic fibroblast growth factor [PeproTech, Rocky Hill, NJ; cat. no. 100-18B], 1% antibiotic-antimycotic [ABAM; Gibco; cat. no. 15240-096], and supplemented with an additional 10 μL/mL 1 μM dexamethasone [DEX; Sigma; cat. no. D4902]).
Cells were plated in MGM at a density of 10,000 cells/cm2 onto 150 mm2 tissue culture plates. After seeding, the cells were left undisturbed for 4 days and subsequently fed MGM every other day. On day 8, plates were 100% confluent, and the media was replaced with muscle differentiation media (MDM) (70% M199 [Gibco; cat. no. 11150-059], 23% DMEM, 6% FBS, 1% ABAM, 10 μL/mL 1 μM DEX, 1 μL/mL insulin–transferrin–selenium-X [Sigma; cat. no. I1884], and 0.72 μL/mL 50 mM ascorbic acid 2-phosphate [Sigma; cat. no. A8960]). After 5–7 days on MDM, the monolayers were delaminated from the cell culture surface and were transferred to Sylgard-coated 150 mm2 tissue culture plates and pinned into a 3-D cylindrical construct at lengths of 10 ± 1 cm and ∼0.5 cm in diameter. SMUs were allowed to fuse down for a minimum of 3 days before surgical implantation. One SMU per VML was either surgically implanted alone or in conjunction with a HG injected to surround the SMU in the VML site.
Hydrogel fabrication and characterization
PEG is a synthetic, hydrophilic, and biocompatible polyether. PEGs are versatile and commonly used in biomedical research, such as in drug delivery and tissue engineering applications. 31 PEGs are nontoxic and approved by the FDA for use in pharmaceutical, food, and cosmetic formulations. PEG HGs can be produced by cross-linking and are commonly used as scaffolds in tissue engineering. Recently, PEG HGs have shown efficacy in wound healing applications. 31 In this study, we used the cross-linking of a two-arm thiolated PEG with silver nitrate to fabricate PEG HGs. Specifically, the PEG HGs were two-arm PEG (10 kDa; Thermo Scientific), 7 wt% and 0.05% lithium phenyl-2,4,6-trimethylbenzoylphosphinate (LAP), cross-linked using ultraviolet (UV) light (5 min, 3 mW/cm2). This HG has been shown to be easily injected or molded into the wound site and has antibacterial and angiogenic properties. 32
GelMA is a natural polymer (Allevi) based on a gelatin backbone and thus biocompatible and biodegradable using enzymatic degradation (e.g., metalloproteinase, matrix metalloproteinases). 33 GelMA HGs are prepared using UV or visible light-mediated kinetic chain polymerization, and mechanical properties can be controlled by adjusting polymer weight percentage. Specifically, FDA approved, Good Manufacturing Practice (GMP)-grade GelMA HGs were prepared by dissolving 50 mg/mL sterile GelMA in sterile phosphate buffered saline (PBS) containing 0.05 wt% LAP photoinitiator and cross-linked with UV light (5 min, 3 mW/cm2).
HA HGs are based on a HA backbone (60 kDa; Lifecore) chemically modified with 20% norbornenes (NorHA; synthesized in the Loebel lab). 34 These FDA approved, GMP-grade HGs are biocompatible and highly tunable in their degradability and mechanical properties by adjusting the type and density of di-thiolated peptide crosslinkers. HA HGs are widely used in tissue engineering applications given that HA is a major component of most extracellular matrices within the body.35,36 In addition, the low modification of the HA backbone enables cells to recognize HA through CD44 providing additional biological signals. For this study, we used nondegradable dithiol (DTT) crosslinkers (0.6 mM) to form HGs through UV-light mediated thiolene reaction.37,38 More specifically, 2 wt% NorHA was dissolved in sterile PBS containing 0.05 wt% LAP and 0.6 mM DTT and crosslinked with UV light (5 min, 3 mW/cm2).
All HGs have been characterized using rheological measurements and polymer weight percentage and crosslinker concentration adjusted to achieve elastic moduli of 3 kPa (Young's modulus). The selection of HG properties was based on previous studies that have used HGs to repair VML. 39
Surgical procedures
Twenty-four hours before surgery, all animals were fasted; a fentanyl patch (75 mcg/h) and an intravenous dose of cefazolin (20 mg/kg) were administered. The animals were weighed, sedated with intramuscular xylazine (0.2 mg/kg), and then anesthetized with intravenous propofol (8 mg/kg) and isoflurane at 2–5% to maintain a deep plane of anesthesia.
An incision was made along the midline of the lower hind leg to expose the PT muscle and peroneal nerve. Measurements of the PT were taken and 30% of muscle volume was dissected, avoiding nerve and major vasculature. The volume removed was calculated as previously described.17,18 The distal branch of the peroneal nerve with its vasculature was isolated and sutured into the VML site to aid with reinnervation and vascularization. The VML-Only animals (negative control) received the injury without any additional repair. The HG groups received the injury, the muscle fascia was sutured back over the VML site leaving a small hole for injection of the HG, and the HG was injected behind the fascia filling the VML site. The SMU-Only group received the injury and was repaired with an SMU, the approximate weight of the muscle removed. The SMU+HA group received the injury and was repaired with an SMU, and HA HG was injected behind the fascia filling the VML site. In all repairs, the fascia and skin were closed with suture and staples and sprayed with AluShield (Fig. 1A–D).
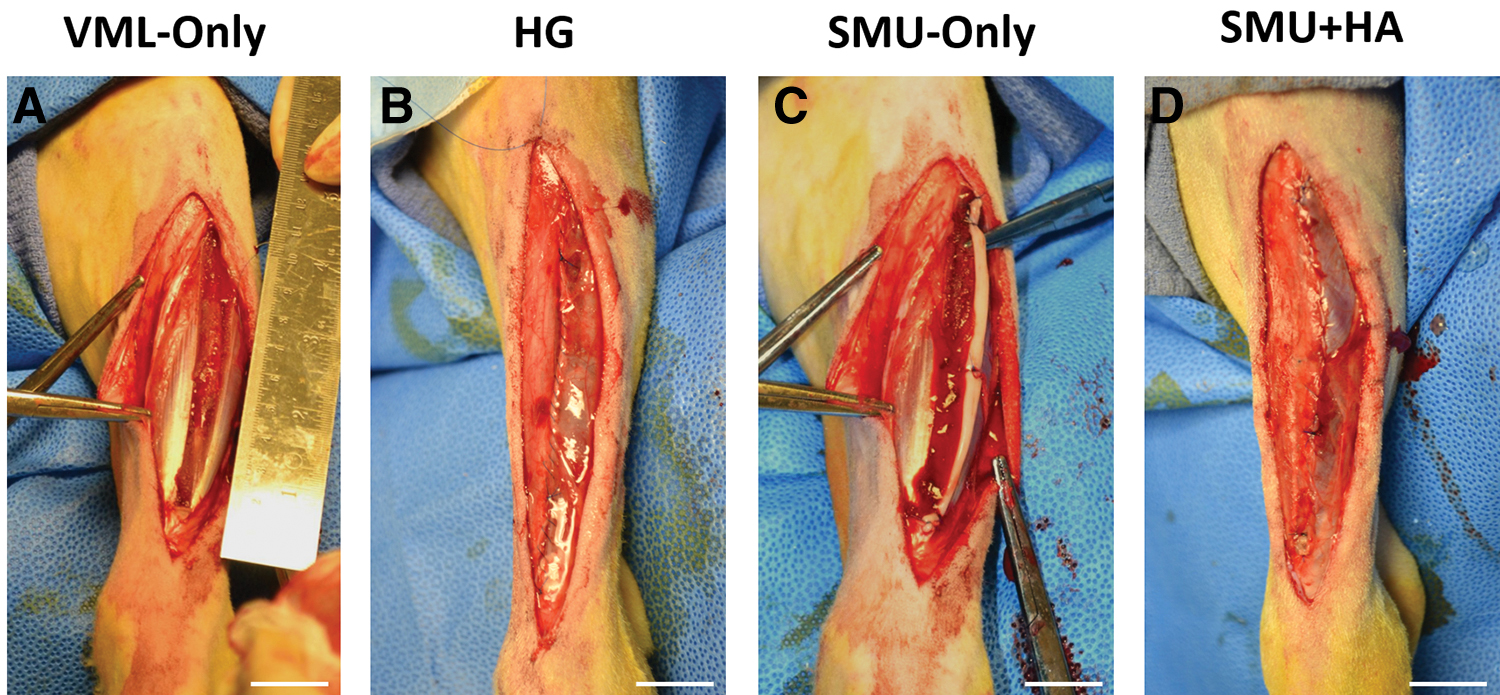
Experimental groups. In all groups, a v-cut longitudinal portion of the PT constituting 30% of the total muscle volume was dissected, avoiding nerve and major vasculature.
Postsurgery, the animals received an intramuscular dose of flunixin (2.2 mg/kg) with subsequent doses administered 24 h postop. All animals were upright and weight bearing within 60 min. The fentanyl patch was removed 48 h after surgery. Animals were monitored daily for 14 days postsurgery by veterinary staff; staples were removed and then returned to herd housing. During daily monitoring, the animals' gait was monitored to see if the animals were exhibiting “toe-touching,” a sign of pain when load-bearing the surgical leg. Additional signs of pain such as elevated blood pressure, increasing respiratory rates, changes in eating habits, lack of herding, and lethargic behavior were assessed.
To evaluate swelling in the surgical leg, a criterion based on percentage increase above normal at 10%, 20%, and 30% was used to separate normal, moderate, and severe swelling, respectively. Blood samples collected during implantation, week-1 postsurgery, and explant (week-6) monitoring were sent to the University of Michigan ULAM In-Vivo Animal Core for laboratory testing and analysis. Blood differential test results were obtained and assessed for normal versus high determinations based on established ranges by ULAM for total basophil, lymphocyte, and WBC counts.
At 6 weeks, animals were euthanized with a lethal dose of sodium pentobarbital (195 mg/kg) and bilateral pneumothorax. Following the surgery, one animal from the HA group stopped eating. Even with daily veterinary care the animal showed continued signs of appetite and weight loss. As per veterinary recommendation, this animal was euthanized and eliminated from the study, reducing the HA group to n = 4. Following dissection, one PT muscle from the VML-Only group was 40% smaller than the average mass of the remaining VML group. This may have been attributed to severe denervation. This animal was statistically eliminated from the study, reducing the VML-Only group to n = 4. Due to the incipient nature of the repair process at the 6-week recovery period, biomechanical measures were not performed.
Histology
Following 6 weeks of recovery, all animals were euthanized and both surgical and contralateral PT muscles were dissected, weighed, and gross measurements were taken. The muscles were prepared for histology in one of three ways: the sample was either coated in Tissue Freezing Medium and frozen in dry ice-chilled isopentane or fixed in 10% formalin for 15 min and then frozen with Tissue Freezing Medium. Frozen samples were cryosectioned at 10 μm and stained with hematoxylin and eosin (H&E), Masson's trichrome, and Picrosirius Red to visualize morphology of the repair site and monitor collagen alignment and content.
The sections were then immunohistochemically stained to identify myosin heavy chain (1:200 dilution; DSHB MF-20c), laminin (1:200 dilution; Abcam; cat. no. ab7463), fast myosin isoform (1:200 dilution; Abcam; cat. no. ab91506), slow myosin isoform (1:200 dilution; Abcam; cat. no. ab11083), M1 and M2 macrophages (1:100 dilutions; Abcam; cat. no. ab125212 and ab111250), and neutrophils (1:100 dilution; Abcam; cat. no. ab62817). Longitudinal samples were sectioned at 25 μm and stained with Picrosirius Red and immunohistochemically stained for acetylcholine receptors (α-bungarotoxin, 1:2000 dilution; Life Technologies; cat. no. B1601), SV-2 (1:300 dilution; DSHB SV2c), and neurofilament (1:2000 dilution; BioLegend; cat. no. 837904) to identify the presence of neuromuscular junctions (NMJs), as well as CD31 (PECAM-1) (1:200 dilution; Abbiotec cat. no. 250590), to assess the presence of vascularization.
Cross-sectional area
To evaluate the number and cross-sectional area (CSA) of muscle fibers in the native and graft site regions, a mid-belly cross-section of each PT muscle was immunohistochemically stained for MF20 (muscle) and laminin (extracellular matrix). To determine the average CSA (μm2) and to mitigate bias of the individual measuring the fiber CSAs, the areas selected to measure fiber CSA were randomly selected by a person blinded to the sample group. The blinded assistant dropped a grid with four 0.51 mm2 square boxes on the muscle cross-section. Within each of these individual boxes, the freehand tool in ImageJ/FIJI was used to measure the CSA of 50 randomly selected muscle fibers. The average CSA of the 200 fibers was determined for each muscle cross-section. To determine the average CSA of muscle fibers in the graft site, the freehand tool was used to identify the repair site in ImageJ/FIJI. All surrounding native tissue was digitally removed from the image. An automated process was used to measure the number and CSA of regenerating fibers in the graft site.
Fiber typing
To evaluate the fiber types in the muscle, a mid-belly cross-section of each PT muscle was immunohistochemically stained for slow myosin isoform to identify type I fibers and fast myosin isoform to identify type II fibers. To determine the proportion of type I and type II fibers in relation to the total CSA of the entire muscle, the amount of area positively stained for slow myosin isoform and fast myosin isoform was measured using ImageJ/FIJI and presented as percentages of total muscle CSA.
M1/M2 macrophages and neutrophils
To evaluate the number of M1 macrophages (CD68 positive), M2 macrophages (CD163 positive), and neutrophils, cross-sections from the mid-belly of the PT muscle were immunohistochemically stained, imaged, and analyzed using ImageJ/FIJI. Specifically, grids were overlayed onto the muscle cross-section in the area of uninjured muscle and the graft site. The area of each grid was measured using ImageJ/FIJI, and the images were split into three channels, each channel representing a different cell type. Due to the large number of positive cells, an automated process was used to identify and quantify the number of M1 macrophages, and the ImageJ/FIJI counting tool was used to quantify the number of M2 macrophages and neutrophils. The data were expressed as the total number of M1 macrophages, M2 macrophages, and neutrophils per area of the grid.
Collagen alignment
As previously described, 18 to evaluate collagen organization, longitudinal sections stained with Picrosirius Red were imaged under monochromatic polarized light. The birefringence of collagen fibers was semiquantitatively analyzed, based on brightness, to determine differences in collagen deposition and maturation at the site of repair. The polarization plane was rotated until maximum brightness was obtained to account for variations in specimen orientation on the slide. Digital images were taken of each tissue section at 10 × magnification during a single imaging session under identical imaging parameters. The images were imported into ImageJ/FIJI software and underwent 8-bit digitalization. Noncollagenous material was shown as black (zero), and collagenous material was assigned a grayscale value from 1 to 255. Higher grayscale values signify more organized and mature collagen. Mean grayscale values for each image were averaged for each animal to obtain a brightness value.
Statistical analyses
Statistical analyses were performed using GraphPad Prism 10 software. Statistical differences between groups where the contralateral muscle was compared to the surgical PT were assessed with two-way analysis of variance (ANOVA) with Sidak's multiple comparisons (MC) tests. Statistical difference between groups where values were normalized to the contralateral side was assessed with one-way ANOVA with Tukey's MC. Results were significant at p < 0.05. Bars on graphs indicate mean ± standard deviation.
Results
Surgical procedures
Across all VML injury groups, the percentage of muscle mass removed was on average 30.1 ± 2.73% and the actual mass removed was on average 3.98 ± 0.54 g. There was no significant difference in the magnitude of the VML injury between groups (p = 0.2856) (Fig. 2A).
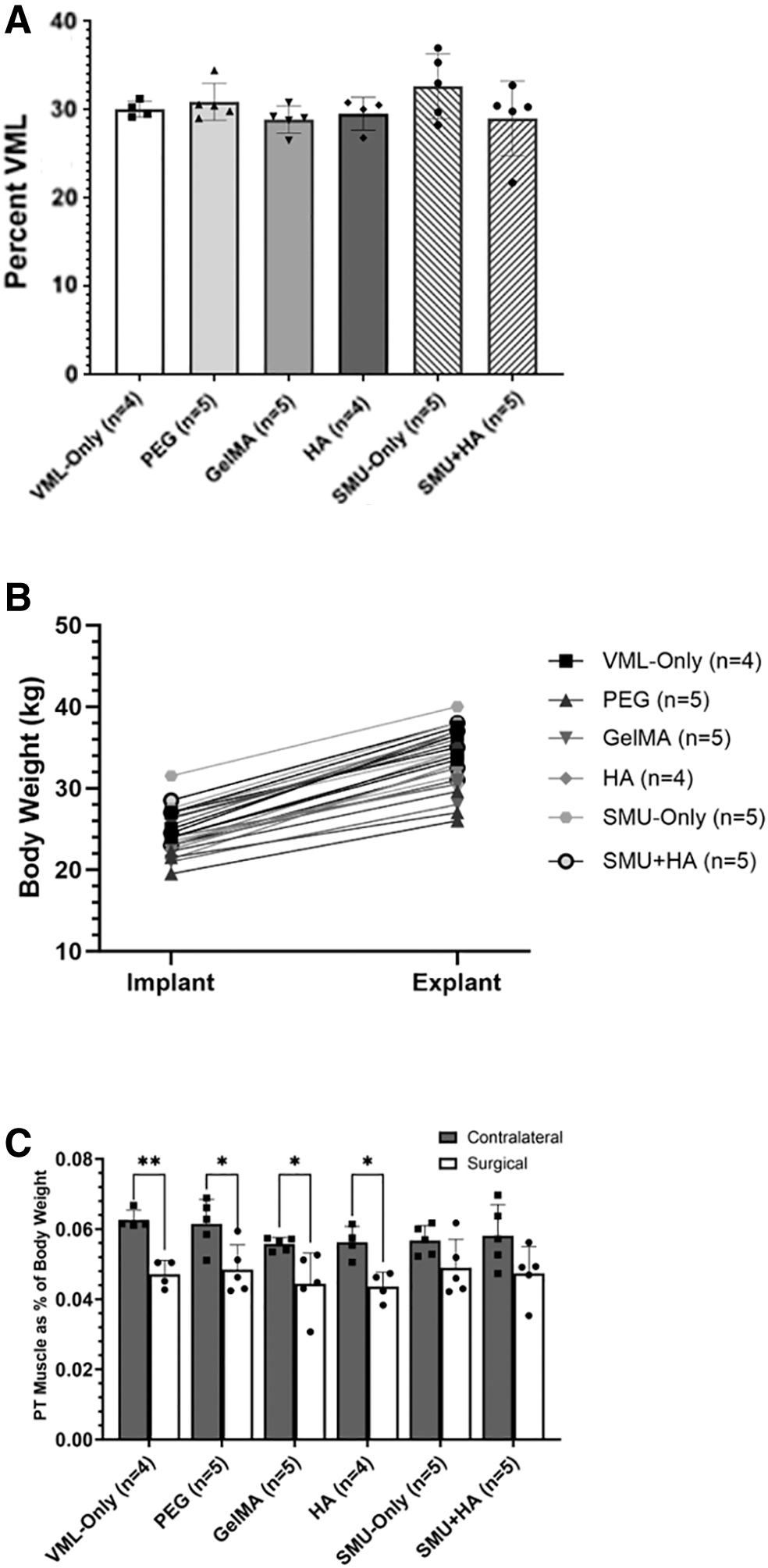
VML injury and mass recovery.
Gross morphology
Gross observations at the time of explant revealed greater amounts of connective tissue surrounding the injured PT muscle compared to the uninjured contralateral muscle. Furthermore, during the muscle dissection, it was observed that pockets of fluid were surrounding the graft site in every PEG repaired VML injury. Figure 3 is a representation in one of the dissections of a PEG repaired VML site (Fig. 3A, first incision for dissection; Fig. 3B, removal of the fluid filled sac; Fig. 3C, PT muscle completely dissected). These observations suggest incomplete integration of the PEG HG with the PT muscle.
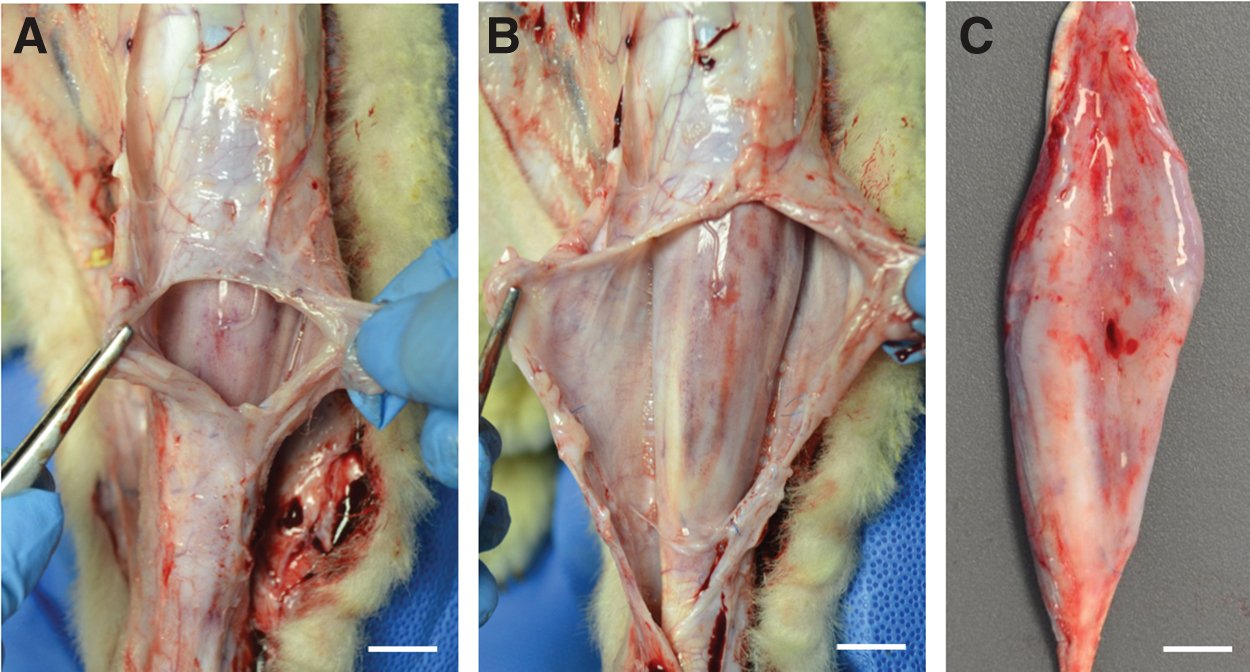
Pockets of fluid observed in PEG explants. During the dissection of muscle, we noted the presence of fluid-filled pockets with the PEG explants.
Wound site and gait analysis
Animals were awake, alert, and weight bearing within 2 h of completing surgery. Data from this study indicated that at 1-week post VML repair, gait was normal in the GelMA, HA, and SMU+HA HG animals, with n = 1 animals exhibiting “toe-touching,” a sign of pain, across VML-Only, PEG, and SMU-Only groups. Swelling at the incision site was most notable in the VML-Only group (Table 1). By 2-weeks postoperation, all animals were walking normally, and incisions were intact. However, several animals in each of the groups still exhibited mild to moderate swelling at the incision site.
One Week and Two Week Wound Site and Gait Analysis
GelMA, methacrylated gelatin; HA, hyaluronic acid; PEG, poly(ethylene glycol); SMU, skeletal muscle unit; VML, volumetric muscle loss.
Bloodwork analysis
At one week, bloodwork indicated that basophil counts (an indicator of inflammation) were significantly higher in several animals in every group. Notably, all animals in the SMU-Only and SMU+HA groups exhibited normal basophil counts, indicating the absence of inflammation in animals post SMU implant. However, only one animal per group had higher than normal lymphocyte counts (another marker of inflammation), and WBC counts did not exceed normal limits all but one of the animals 1-week post-op. In the HA group, the same animal presented both high basophil and lymphocyte counts and swelling, indicating that three of four sheep were not affected by HA in the repair site. At 6-weeks, basophil counts were normal in all animals; however, the lymphocyte counts of several animals in every group were insignificantly higher than normal lymphocyte counts, indicative of persistent inflammation in animals at 6-week postrepair. Total WBC counts for all animals were normal after 6 weeks (Table 2).
One Week and Six Week Bloodwork Analysis
Body mass and muscle mass recovery
All animals gained weight normally during the 6-week recovery period, with no significant difference in body weight between experimental groups at the time of explant (p = 0.0802, n = 28) (Fig. 2B). This indicates that the VML injury did not significantly impact the health of the animals during this 6-week recovery period. In addition, no signs of graft rejection were observed in the sheep.
At the time of explant, the weights of the VML injured PTs were compared to the contralateral sides. There was a significant muscle mass deficit between the contralateral and VML repaired PTs in the VML-Only, PEG, GelMA, and HA groups (p = 0.0074, p = 0.0135, p = 0.0433, p = 0.0421, respectively), indicating that at 6 weeks, the graft side had not regenerated. In contrast, the SMU-Only and SMU+HA groups were not significantly different from the contralateral (p = 0.3021, p = 0.0603), indicating enhanced regeneration in these groups (Fig. 2C). The 25% mass deficit experienced by the VML-Only group was expected, as the defect in the VML-Only group was not repaired with a construct or HG to facilitate the healing process in the injury site.
Histological analysis of muscles
Morphology of explanted muscle
We performed qualitative and quantitative histological analyses of mid-belly cross-section of the PT muscle in both contralateral and injured PT muscles. H&E staining in the repair site revealed disorganized tissue, as well as the recovery of vasculature and innervation in all experimental groups (Fig. 4A–G). It was observed that the wound site had been sealed off from surrounding native tissue in samples from the PEG group. Masson's trichrome staining of the injury sites indicates fibrotic regions evidenced by the presence of collagen deposition in the repair site, characterized by blue regions in the Masson's trichrome-stained sections, surrounded by native skeletal muscle (Fig. 4H–N). Revascularization was monitored using CD31 (PECAM-1) on longitudinal portions of the PT muscle that qualitatively showed extensive vascularization in the repair site in all surgical groups, suggesting angiogenesis and tissue regeneration in the repair site (Fig. 5A–G).
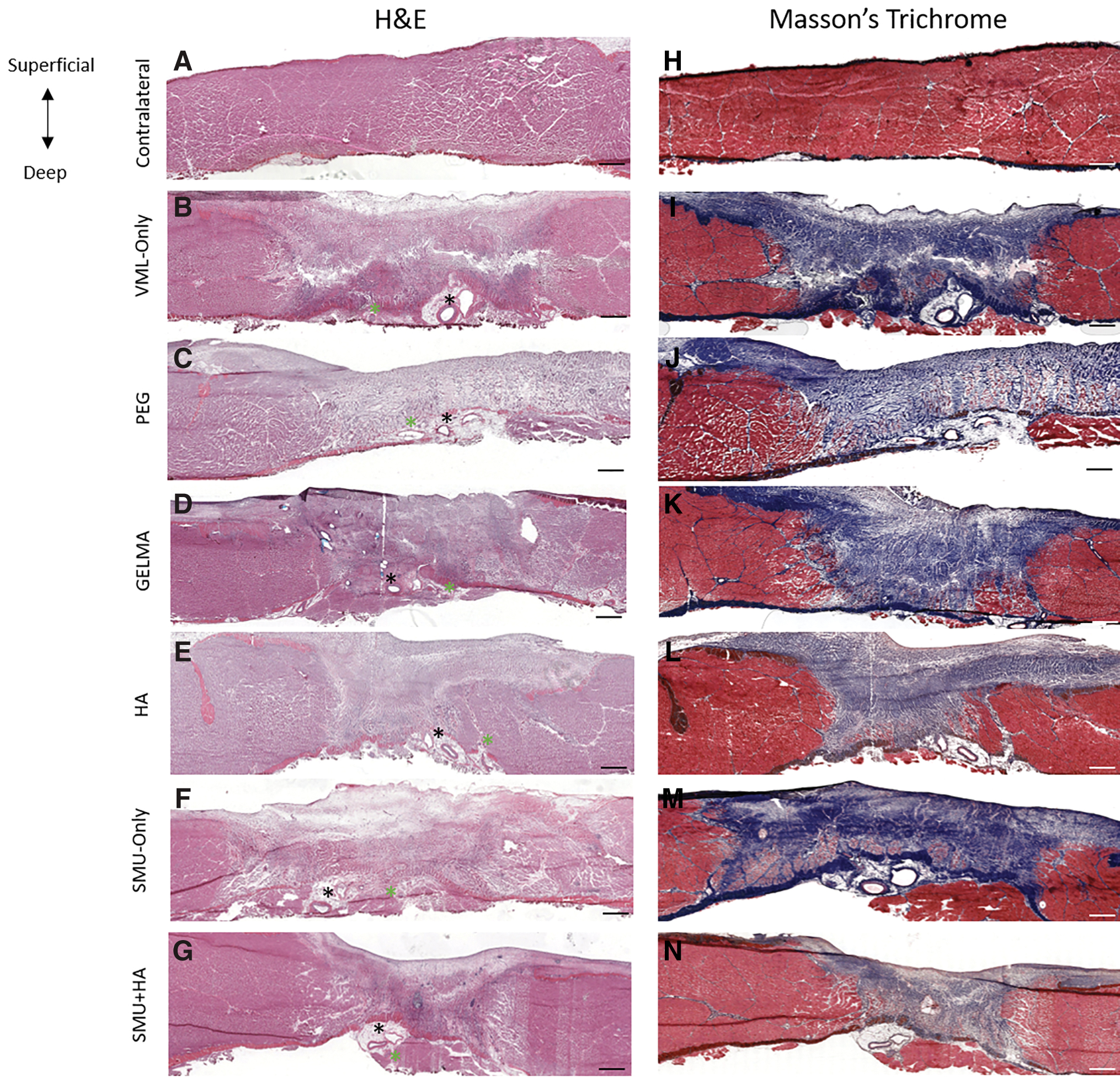
Morphology of explanted muscle. Mid-belly cross-sections of explanted PT muscle from the contralateral, VML-Only, PEG, GelMA, HA, SMU-Only, SMU+HA. Gross observations of H&E
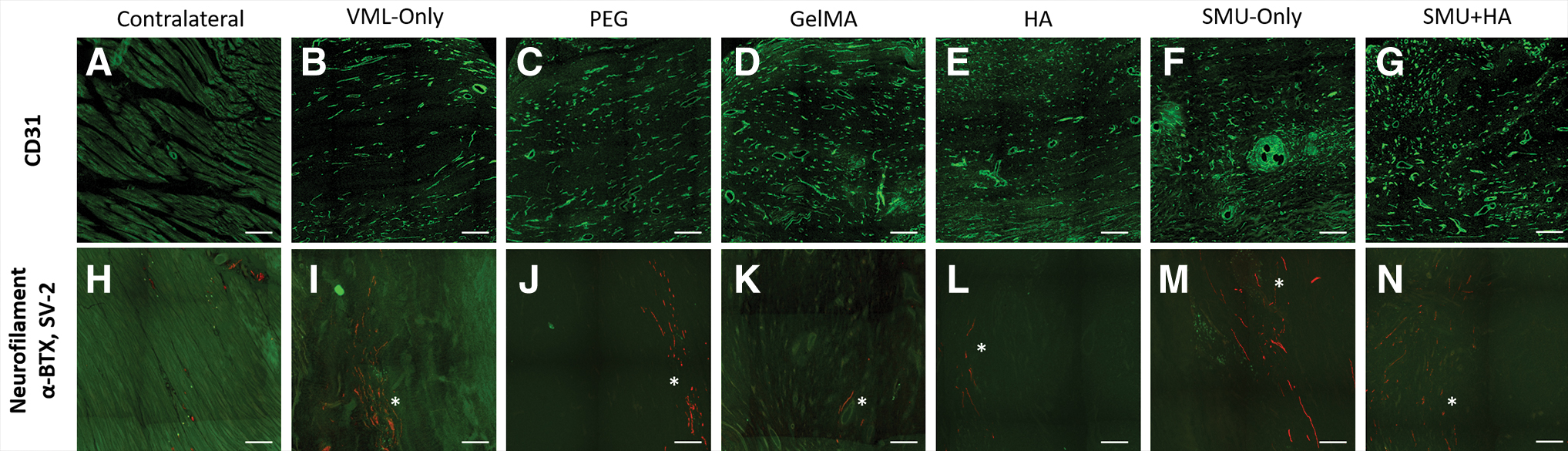
Vascularization and innervation of explanted muscle. Immunostaining for vascularization through CD31 indicates the presence of a well-developed vasculature network in the VML site following VML injury in all groups
Innervation
To detect the presence of reinnervation and NMJs in the VML injury site, longitudinal sections of the PT in the area where the peroneal nerve had been rerouted were stained with neurofilament, SV-2, and alpha-bungarotoxin (Fig. 5H–N). The identification of a functional NMJ was confirmed when presynaptic and postsynaptic structures overlapped, resulting in a yellow region due to the combination of red (neurofilament and SV-2) and green (alpha-bungarotoxin) fluorophores. 15 The presence of NMJs observed in abundance in the contralateral PT, however, was largely absent in all of the surgical groups. Neurofilament and acetylcholine receptors were observed in the VML injury site in all surgical groups but did not exhibit any overlapping structures that would suggest functional NMJs in the repair site. The observation of neurofilaments suggests new nerve growth in the injury site at the 6-week recovery time point. However, it may require more time for complete nerve regeneration and the reestablishment of functional NMJs.
Collagen
Picrosirius Red staining was used to characterize collagen content and alignment of collagen in longitudinal sections from the PT muscle in both contralateral and VML-injured muscles through monochromatic polarized light analysis. In all surgical groups, the mean grayscale values indicated that the contralateral muscle was characterized by significantly less collagen. In contrast, the graft site was filled predominantly with collagen and indicates the presence of highly aligned collagen in all experimental groups compared to the contralateral muscle (p < 0.0001 for all groups) (Fig. 6A–G), with average grayscale values at 14.93 ± 1.87, 86.35 ± 11.71, 65.74 ± 7.16, 71.56 ± 21.50, 83.04 ± 11.28, 69.47 ± 16.64, and 80.13 ± 6.14 for contralateral, VML-Only, PEG, GelMA, HA, SMU-Only, and SMU+HA groups, respectively (Fig. 6H).
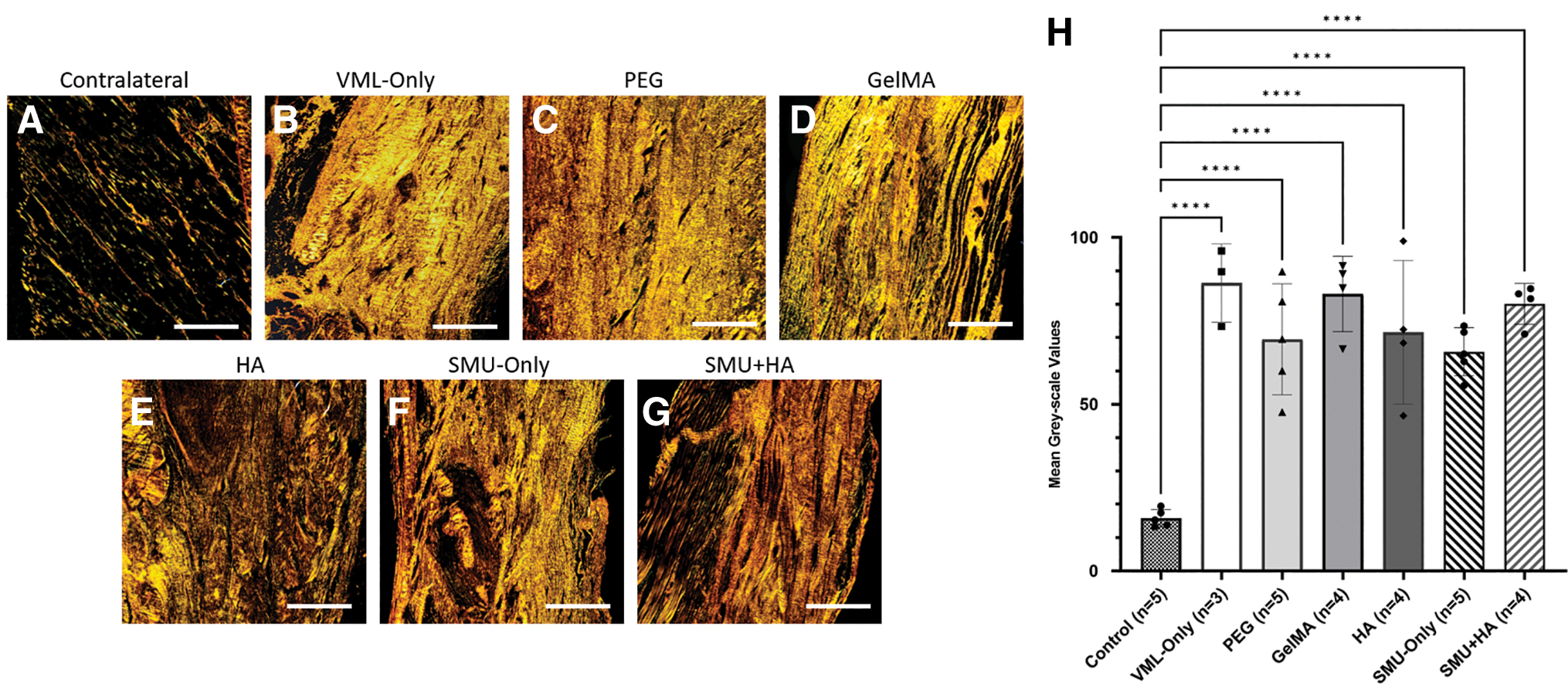
Analysis of collagen alignment and content of explanted muscle. Longitudinal PT sections were stained with Picrosirius Red and imaged in polarized light microscopy to evaluate collagen content and alignment in the VML injury site relative to the contralateral muscle
Macrophages and neutrophils
The density of M1 macrophages, M2 macrophages, and neutrophils in the native muscle surrounding the injury site was evaluated to be not significantly different from the density of M1 macrophages, M2 macrophages, and neutrophils in the contralateral (control) muscle (p = 0.1161, p = 0.0918, and p = 0.0787, respectively). A one-way ANOVA indicated that there was no significant difference in the density of M1 macrophages in the repair site between any of the surgical groups and control (p = 0.1520). In contrast, analysis revealed that the density of M2 macrophages in the repair site of the SMU-Only and SMU+HA group was significantly higher than the control (p = 0.004 and p < 0.0001). The analysis revealed that the neutrophil density was significantly greater in the VML-Only group compared to control (p = 0.0279), and the SMU+HA group had significantly greater neutrophil density compared to both the control and PEG groups, p < 0.0001 and p = 0.0107 (Fig. 7H–J).
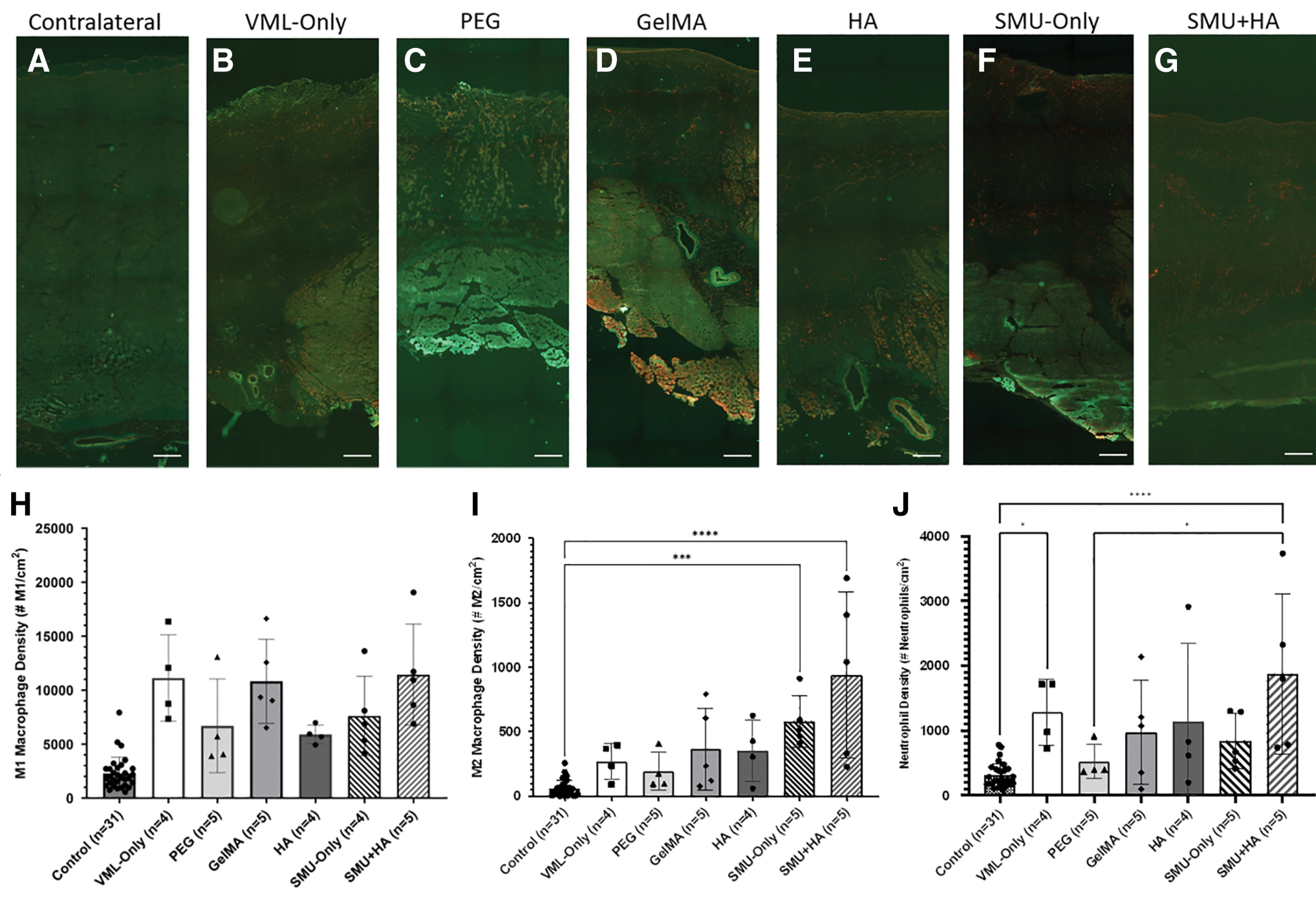
Analysis of M1 macrophages, M2 macrophages, and neutrophils of explanted muscle. Mid-belly cross-sections of PT muscle stained with CD68, CD163, and antineutrophil markers to enumerate the density of M1 macrophages, M2 macrophages, and neutrophils in tissue sections
CSA and muscle regeneration
Myosin heavy chain (MF20) and laminin staining were used to measure the CSA of individual fibers in the contralateral and surgical muscles (Fig. 8A–G). The average CSA of fibers in the native muscle surrounding the repair site (1444.9 ± 466.6 μm2, n = 23) was surgical groups and was not significantly different compared to fibers in the contralateral muscle (control) (p = 0.6398). In all surgical groups, there was a significant decrease in the CSA of individual muscle fibers found in the repair site compared to the surrounding native muscle fibers (p < 0.0001). There was no significant difference in CSA of muscle fibers between any of the surgical groups (p = 0.6398) (Fig. 8H).
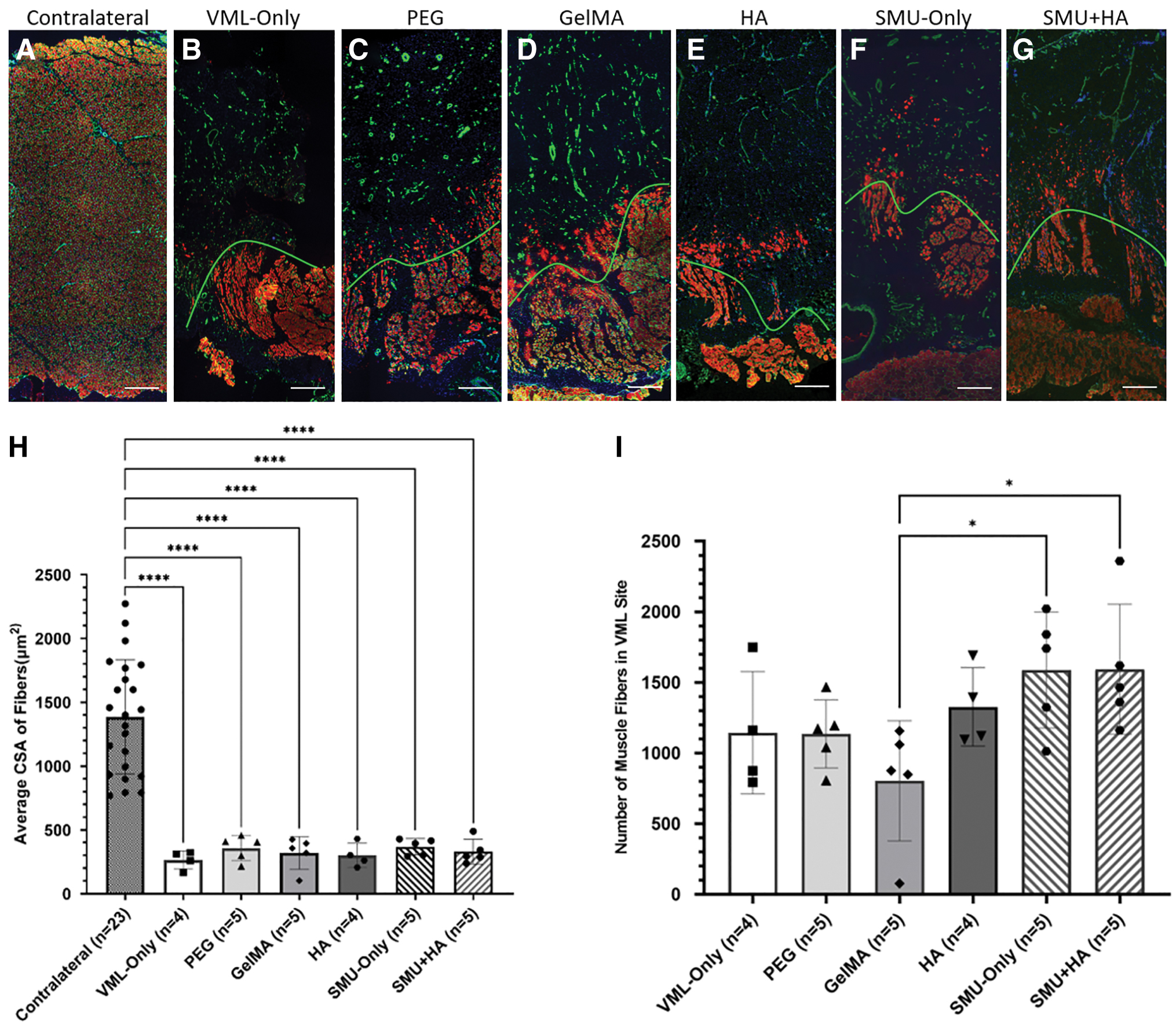
MF20 and laminin analysis in mid-belly cross-sections of PT muscle. Immunohistochemical staining for myosin heavy chain (MF20) and laminin shows that muscle is absent in a significant portion of the VML injury site
The number of skeletal muscle fibers in the repair site was assessed to determine the regenerative potential of the different HGs, SMU-Only, and SMU+HA combination. The average number of muscle fibers was as follows: for VML-Only (1144 ± 433), PEG (1135 ± 241), GelMA (803 ± 425), HA (1326 ± 278), SMU-Only (1587 ± 410), and SMU+HA (1593 ± 459). A one-way ANOVA revealed a significantly greater number of fibers in the repair site of the SMU-Only and SMU+HA (p = 0.0404, p = 0.0385, respectively) compared to the GelMA group (Fig. 8I).
Fiber type
To evaluate the percentage of type-I and type-II fibers in the PT muscle, mid-belly cross-sections of each group were immunohistochemically stained for slow myosin isoform (Type-I fibers) and fast myosin isoform (Type-II fibers). No significant differences were observed between any of the surgical groups for both slow fibers (p = 0.9891) and fast fibers (p = 0.8554). At the 6-week recovery time point, fiber type grouping was not observed in the native muscle tissue surrounding the repair site. Thus, data are presented for the PT muscle in general, indicating that the average area of slow fibers as a percentage of the total CSA was 31.33 ± 5.07% and the average area of fast fibers as a percentage of the total CSA was 68.14 ± 5.09% (n = 32).
Discussion
VML injuries are a significant burden on both military personnel and civilians, resulting in minimal muscle regeneration, substantial fibrosis, and functional limitations. VML injuries often lead to chronic and debilitating conditions.2,8 The current gold standard of care for VML injuries are autologous muscle transfers, which suffer from many shortcomings such as significant donor-site morbidity and incomplete functional recovery. 3 Following an injury, skeletal muscle typically undergoes a regenerative process where following acute inflammation, satellite cells migrate into the injury site and if they survive the inflammatory environment, muscle regeneration begins. If successful, this sequence leads to the restoration of both muscle structure and function. However, in the instances of severe muscle trauma that result in VML, acute and chronic inflammation, as well as fibrotic infiltration and scar formation, impedes muscle regeneration and causes scarring of the affected muscle.40–43
Emerging regenerative medicine therapeutics target the limitations of current treatment options and include the implementation of biological scaffolds and myogenic cell replacement therapy, which are promising solutions to restore muscle function, but still face challenges with the regeneration of healthy nerve-muscle connections, as well as robust vascularization.44,45
In previous studies, our laboratory was able to scale-up and fabricate scaffold-less tissue-engineered SMU constructs and engineered neural conduits (ENCs) to evaluate the SMUs and ENCs in vitro to test the efficacy of these constructs in restoring muscle function in a clinically relevant large animal model in 3 and 6 months. While our SMUs were able to fully restore a VML injury at 3 months and partially repair a VML injury at 6 months, significant fibrosis may have played a role in decreasing the efficacy of the SMUs for muscle regeneration.17,18
Thus, we hypothesized that the use of protective HGs in combination with our SMU technologies would acutely protect the implanted tissue from fibrosis. Thus, the purpose of this study was to evaluate the efficacy of commercially available and FDA approved HGs for their capacity to reduce acute inflammation and mitigate fibrotic responses, while assessing their potential in enhancing muscle cell migration and regeneration. In addition, we combined the most promising HG with our scaffold-less tissue-engineered SMU constructs to treat a 30% VML injury in an ovine model. Specifically, PEG, GelMA, and HA HGs were fabricated and injected into the VML site alone, and the HA was additionally combined with an SMU. These novel interventions were compared to our negative (VML-Only) and positive (SMU-Only) groups.
Concurring with the previous 3- and 6-month studies, in this study we did not detect immune rejection in any of the animals receiving engineered SMUs. Furthermore, in just 6 weeks, the SMU-Only group recovered ∼15% of the VML injury, reaching a muscle mass of 85% in comparison to its contralateral muscle. In accordance with these observations, the MF20 and laminin analysis revealed an increase in the number of regenerating muscle fibers in the repair site of the SMU-Only and SMU+HA groups compared to all of the HG groups. Thus, in the groups that had the SMU implantation, we observed an increase in muscle mass recovery, suggesting that the increase in mass cannot solely be attributed to connective tissue deposition and that the contribution of the SMU led to a more effective muscle regeneration compared to the HGs alone. We also observed that the PEG and HA HGs exhibited enhanced migration of muscle cells into and more regenerated muscle fibers in the VML-injury site compared to the GelMA HG, indicating that PEG and HA may be more efficacious in providing an environment within the repair site that is more favorable to muscle regeneration compared to the GelMA HG. However, in the injury sites repaired with PEG we observed that the site was sealed off by fluid filled sacs and a decreased number of regenerated fibers compared to the HA repaired groups.
We also found that all surgical groups exhibited extensive fibrosis in the repair site of all VML injured muscles, evidenced by significant collagen deposition. We quantitatively observed the recovery of extensive vasculature and developing innervation in the repair site of all experimental groups, suggesting the establishment of an environment conducive of healing, consistent with the absence of necrosis and presence of tissue regeneration in the repair site. In addition, an analysis of the density of NMJs in the repair site revealed the presence of neurofilaments and acetylcholine receptors in the repair site; however, they were not co-stained, suggesting the embryonic nature of NMJs in the repair site. This suggests that more time is needed for the maturation of nerve growth and NMJs.
The analysis of macrophages and neutrophils showed a smaller number of M1 macrophages, pro-inflammatory markers, in the PEG and HA HG groups, which suggests that the PEG and HA HGs may have protected the PT muscle from acute inflammation more effectively than the GelMA HG. Similarly, in the M2 macrophage analysis, the data revealed a higher increase in anti-inflammatory markers in the HA group. These results are supported by the analysis of bloodwork, where the HA group presented low basophil and lymphocyte counts and no swelling, indicating that the VML site was not affected by HA. In addition to the HA group, the SMU-Only and SMU+HA groups exhibited lower lymphocyte counts, an indication of decreased inflammation, than all other repair groups at 6 weeks, further suggesting that our SMU grafts possess properties that can potentially contribute to the reduction in acute inflammation. Moreover, in the SMU+HA group, the combination therapy of the HA HG with our SMUs did not have an additive effect in the reduction of lymphocyte counts. These findings collectively underscore the promising role of our SMU constructs in mitigating inflammatory responses following VML injury and repair.
The fiber type analysis did not reveal a significant change in the percentage of fast fiber types and slow fiber types in any groups. As a shift from fast to slow fiber types is indicative of denervation and reinnervation of muscle fibers following nerve injury, the observations at the 6-week recovery period suggest that either the remaining native muscle tissue did not undergo substantial denervation during the VML injury or that at the 6-week time point, substantial reinnervation has not yet occurred. In addition, at 6 weeks, there was evidence of early neural regeneration with neurofilaments and grouped acetylcholine receptors observed in the graft area, but not fully formed NMJs. These results imply that the muscle tissue's reinnervation remained incomplete, suggesting that more time is needed for the muscle to regain complete reinnervation, full strength, and functionality.
In conclusion, these results demonstrate the efficacy of HA HG in controlling acute inflammation and fibrotic response in the repair site during muscle regeneration following a 30% VML injury and a 6-week recovery. Moreover, the synergistic potential of our SMUs in conjunction with HA HG holds promise in increasing muscle regeneration in the repair site following VML injury. However, a more comprehensive understanding of the implications and mechanisms underlying VML repair with HA HGs require longer duration studies. Our laboratory's future studies will extend the recovery period to 6 months, an interval that has proven effective in evaluating functional recovery in sheep models.
In future experiments, we would like to investigate the addition of antifibrotic growth factors in HG to further decrease fibrosis and create an environment conducive to successful engraftment and regeneration of muscle tissue following implantation while mitigating increased fibrosis in the repair site. Furthermore, previous studies conducted by our laboratory demonstrated the survival of the SMU and the contribution of satellite cells from the SMU into the repair site in a rat VML model. 12 While we were unable to monitor the implanted SMUs during this study, in future studies, we would like to explore cell or DNA tracking methodologies to assess the survival of the SMU in vivo and evaluate the contribution of satellite cell donation from the implanted SMUs in the repair of VML in a clinically relevant large animal model.
Footnotes
Acknowledgments
The authors acknowledge the University of Michigan for its internal funding, as well as Ryan Ettner, Makayla Kelley, Alexandra Kennedy, Luisa Nierhoff, Grace Yao, and Amber Yu for their technical assistance. Furthermore, the authors acknowledge the Michigan Medicine Department of Pathology for their assistance in processing our histology samples.
Authors' Contributions
E.Y.S: Data curation (equal); investigation (equal); project administration (equal); supervision (equal); formal analysis (lead); and writing—original draft (lead). C.S.K: Conceptualization (equal); data curation (equal); investigation (equal); project administration (equal); supervision (equal); writing—review and editing (supporting). E.E.V-.S: Data curation (equal); investigation (supporting); supervision (equal). B.D.P: Investigation (supporting); project administration (supporting); writing—review and editing (supporting). S.N.L: Methodology (equal). D.H.H: Formal analysis (supporting); investigation (supporting); writing—original draft (supporting). D.W.B: Formal analysis (supporting); investigation (supporting); writing—original draft (supporting). C.E.F: Investigation (supporting). C.L: Resources (lead); supervision (supporting); methodology (equal); writing—review and editing (supporting). L.M.L: Conceptualization (lead); funding acquisition (lead); methodology (lead); writing—review and editing (equal).
Disclosure Statement
The authors have nothing to disclose.
Funding Information
This project was funded by internal resources from the University of Michigan.