
Abstract
It is currently unknown if surgeons and biomaterial scientists &or tissue engineers (BS&orTE) process and evaluate information in similar or different (un)biased ways. For the gold standard of surgery to move “from bench to bedside,” there must naturally be synergies between these key stakeholders’ perspectives. Because only a small number of biomaterials and tissue engineering innovations have been translated into the clinic today, we hypothesized that this lack of translation is rooted in the psychology of surgeons and BS&orTE. Presently, both clinicians and researchers doubt the compatibility of surgery and research in their daily routines. This has led to the use of a metaphorical expression “squaring of the circle,” which implies an unsolvable challenge. As bone tissue engineering belongs to the top five research areas in tissue engineering, we choose the field of bone defect treatment options for our bias study. Our study uses an online survey instrument for data capture such as incorporating a behavioral economics cognitive framing experiment methodology. Our study sample consisted of surgeons (n = 208) and BS&orTE (n = 59). And we used a convenience sampling method, with participants (conference attendants) being approached both in person and through email between October 22, 2022, and March 13, 2023. We find no distinct positive–negative cognitive framing differences by occupation. That is, any framing bias present in this surgical decision-making setting does not appear to differ significantly between surgeon and BS&orTE specialization. When we explored within-group differences by frames, we see statistically significant (p < 0.05) results for surgeons in the positive frame ranking autologous bone graft transplantation lower than surgeons in the negative frame. Furthermore, surgeons in the positive frame rank Ilizarov bone transport method higher than surgeons in the negative frame (p < 0.05).
Impact Statement
Our study highlights the need for interdisciplinary collaboration to exploit surgeon and biomaterial scientist &or tissue engineer synergies in the future and to achieve improvements in the treatment of patients with bone defect through purposeful development of innovative treatments with new biomaterials.
Introduction
Over the past 30 years, tissue engineering (TE) has evolved into a thriving research and commercial development field. However, applying TE strategies to routine clinical application has been challenging. To address this need, in 2008, organizers invited a small group of bioengineers, surgeons, biologists, and material scientists from academia, industry, and government to participate in a 2½-day conference to discuss threshold values of success. Surprisingly, clinical translation was not a major factor on the list. Still today, often both clinicians and researchers doubt the compatibility of surgery and research in their daily routines. This has led to the use of a metaphorical expression “squaring of the circle,” which implies an unsolvable challenge (Huber-Lang and Neugebauer, 2011). Young surgical researchers are often discouraged at an early stage because they are given the impression that the combination of surgery and research is unrealistic (Editorial Nature, 2017). As a result, they tend to concentrate mostly on their clinical performance and training. Furthermore, those interested in surgical research face a growing divide between the clinically relevant hypotheses generated from daily surgical care and the increasingly complex scientific methodology that is emerging. At times, there is even a linguistic difference between “surgery and research,” which adds to the challenge of bridging the gap between the two fields (Table 1).
Antagonisms That Arise in Everyday Work Between Surgeons and BS&orTE
Table adapted from Huber-Lang and Neugebauer (2011).
BS&orTE, biomaterial scientists &or tissue engineers.
In this study, we provide, to the best of our knowledge, the first-ever quantitative behavioral evidence comparing a large sample of surgeons (n = 208) and biomaterial scientists &or tissue engineers’ (BS&orTE; n = 59) preference for current options and future possibilities with innovative therapeutic technologies—namely, the use of biomaterial science and tissue engineering & regenerative medicine (TE&RM) in bone defect treatment and how both surgeon and scientists’ preferences may be practically impacted by cognitive (framing) bias.
Background
Bone defects after trauma, infection, or tumor resection are ongoing challenges for patients, surgeons, and BS&orTE (Laubach et al., 2023). The need for the development of innovative treatment strategies rooted in biomaterial science and TE&RM in bone defect treatment is a forward-thinking approach that is critical to effective future health care provision (Laubach et al., 2022). However, surgeons and BS&orTE are two distinctively different groups of experts. They have very different educational backgrounds, training, and fields of tertiary qualification. They have uniquely specialized day-to-day work roles, regularly interact with different types of colleagues and commercial health sector partners, and even possibly have different conceptual and scientific perspectives on current bone defect treatments and future directions (Basson, 2014). These key differences may subjectively explain why even though now in 2024 with more than 20,000 studies having been published on the topic of scaffolds and bone TE (Fig. 1), still only a handful of innovations have been translated to the point that is from “bench to bedside” (Hollister and Murphy, 2011).

Annual growth of studies on scaffolds for bone tissue engineering published in PubMed between 1996 and 2022. Evaluation performed on January 8, 2023, using the RISmed package in R statistical software (version 4.0.2; R Foundation for Statistical Computing, Vienna, Austria) with the search strategy “((engineering) AND (bone)) AND (scaffold)”.
For the gold standard of surgery to move forward, there must naturally be synergies between these key stakeholders’ perspectives, where scientific curiosity meets the practical surgical application (Laubach et al., 2023). More specifically, little is known about the (a)symmetry of preferences or behavior of these pivotal groups when it comes to the positive benefits or negative drawbacks for applying biomaterial science and TE&RM to develop better clinically relevant bone defect treatments and, also, if surgeons and BS&orTE process and evaluate information in similar or different (un)biased ways.
A recent British Journal of Surgery systematic review exploring bias in surgical performance and patient outcomes (Armstrong et al., 2023) identified more than 30 different types of cognitive bias (in 39 separate peer reviewed studies). The social science discipline of behavioral economics is an innovative quantitative instrument to identify such, providing key insights into how surgical experts and patients communicate and make choices (Whyte et al., 2021), in identifying bias in surgical decision-making (Whyte et al., 2022a), for understanding how cosmetic augmentation patients evaluate risk in informed consent processes (Whyte et al., 2023), and even exploring surgeon, nurse, and patient preference for biomaterials and/or TE&RM technology alternatives in future practice (Whyte et al., 2022b).
Materials and Methods
Our study uses a behavioral economics framing experiment methodology (Whyte et al., 2022a) to explore surgeon and BS&orTE perceptions of current standards and new bone defect treatments “framed” in two different ways. The first, if treatment alternatives are framed as positives (benefits), and the second, if treatment alternatives are framed as negatives (drawbacks) (Kahneman, 2011). Theoretically and in practice, we assume that humans act in logical and rational ways, and as such, the way in which choice alternatives are framed should not explicitly impact or differentiate surgeon or BS&orTE decision-making when these frames differ. Surgeons and scientists’ preferences should logically be transitive (i.e., treatment option A > B > C > D, so A > D) irrespective of the way in which they are presented. Deviations from this principal assumption of rational transitive preference naturally create significant problems for all parties involved in health care setting decision-making. For example, in how surgeons and BS&orTE communicate, interact, and work together on new technological innovations and any eventual adoption in surgical practice for patients.
Using this behavioral economics methodology, we asked participants (surgeons and BS&orTE) to rank their preferences for four different bone treatment options, including the following: (1) an autologous bone graft transplant, (2) an Ilizarov bone transport method, (3) a vascularized free bone transfer procedure, and (4) a new method of scaffold-guided bone regeneration. Participants in our study were randomly allocated into one of the two frames, one in which all four frames were positive and one in which all four frames were negative.
Data capture
Our study collected survey data (both in person and at European surgical conferences—and ex poste via email) between the dates of October 22, 2022, and March 13, 2023. All research was conducted in accordance with the Queensland University of Technology University Human Research Ethics Clearance no. LR 2022–6352-11321. The study was also preregistered at Open Science Framework (OSF). 1
Descriptive statistics
Our study sample included n = 267 survey participants, with the composition differentiated by specialization being surgeons (n = 208; 77.9%) and BS&orTE (n = 59; 22.1%). The sample population had a highly skewed sex ratio dominated by males (n = 184 surgeons and n = 40 BS&orTE) compared with females (n = 24 surgeons and n = 16 BS&orTE), with n = 3 participants choosing not to disclose their sex. Geographically, the majority of participants were based in Germany (n = 164), along with the United States (n = 23), Netherlands (n = 12), and Australia (n = 12). Surgeons and BS&orTE both had extensive experience with bone defect treatment (15.4 years [10.6 standard deviation (SD)] and 9.9 years [8.7 SD], respectively) and with biomaterials (12.1 years [10.3 SD] and 13.4 years [10.1 SD], respectively).
Results
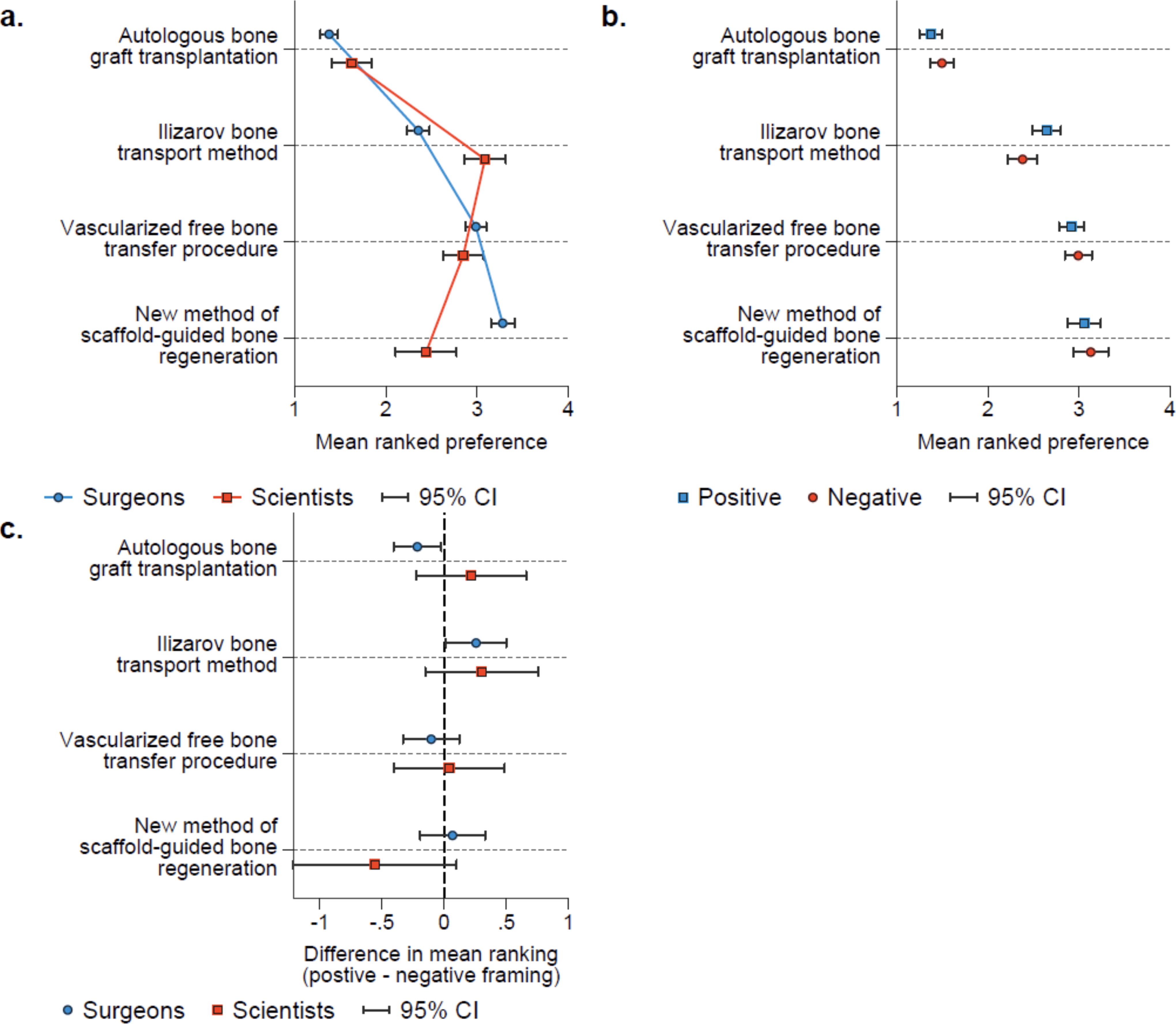
Our analysis further showed that on average, surgeons ranked the Ilizarov bone transport method lower than BS&orTE (Fig. 2a). But in contrast, surgeons ranked a new treatment concept rooted in scaffold-guided bone regeneration higher than BS&orTE. Most interestingly, for our study, we do not find any distinct positive–negative framing differences by occupation (Fig. 2b). That is, any framing bias present in this surgical decision-making setting does not appear to differ significantly between surgeon and BS&orTE specialization. In Figure 2b and Figure 2c, we explored within-group differences based on differences in frames. In this study, we see statistically significant (p < 0.05) results for surgeons in the positive frame ranking autologous bone graft transplantation lower than surgeons in the negative frame. Furthermore, surgeons in the positive frame rank Ilizarov bone transport method higher than surgeons in the negative frame (p < 0.05) (Fig. 2b). Finally, BS&orTE in the positive frame rank the new method of scaffold-guided bone regeneration lower than other BS&orTE in the negative frame (p < 0.10) (Fig. 2c).
Discussion
Since what is often termed a landmark workshop in 1987 (in Washington, DC), sponsored by the National Science Foundation, for the TE&RM community in which, for the first time, the term tissue engineering was officially coined, more than 50,000 studies have been published on the topic of scaffolds with more than 40% related to bone TE (Hutmacher et al., 2023). Henceforth, one might conclude that TE&RM has matured from a scientism point of view over the last four decades. And yet even now in 2024, only a small number of innovations have been translated into routine clinical application (Laubach et al., 2023). Therefore, we hypothesized that the lack of what is termed “from bench to bedside” is rooted in the psychology of surgeons and BS&orTE having very different preferences and perspectives on the state of the art and potential for innovation. In our study, we focused on bone defect treatment options, as the bone is the second most transplanted tissue.
Our study, which to the best of our knowledge used the largest sample to date of surgeons and BS&orTE (who were both very experienced in the treatment of bone defects and biomaterials), showed that there were no radically different perspectives, but, based on nuanced evaluation of the results, valuable conclusions for future research efforts should be noted. For example, the Ilizarov bone transport method, which is known and often perceived by experienced clinicians with significant patient morbidity and complications (Zhou et al., 2021), was judged to be a lesser option by surgeons, showing that, on the one hand, surgeons seek innovations such as the new method of scaffold-guided bone regeneration (Fig. 2a). On the other hand, it is an interesting finding that surgeons were influenced by a positive–negative framing of this powerful as well as highly skill-dependent and controversially discussed technique of Ilizarov bone transport method (Loker et al., 2021). This suggests that more attention should be drawn to potential bias in the training of surgeons to ensure evidence-based decision-making at all times. The observed impact of negative framing in the use of autologous bone graft, which is the current gold standard for the treatment of bone defects (Schmidt, 2021), for surgeons is likely related to the known risks of the harvest procedure and is therefore exacerbated by negative framing. Interestingly, however, this negative frame is less pronounced in the new method of scaffold-guided bone regeneration (Fig. 2b), further underscoring the need for alternative treatments despite the potential challenges associated with them.
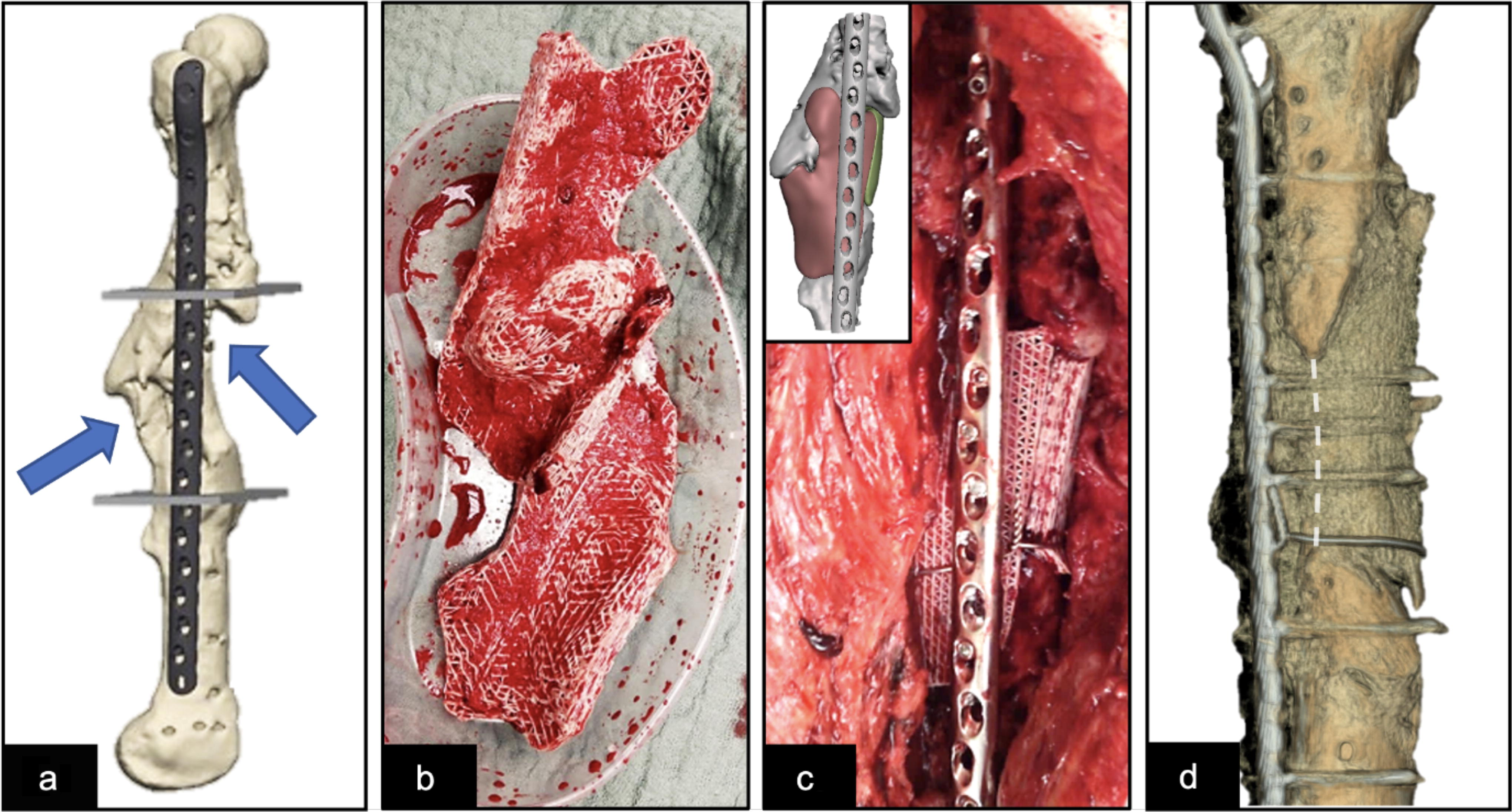
Particularly, with the advent of innovative solutions such as 3D-printed scaffolds for bone defect regeneration (Fig. 3), achieving a unified stance among key stakeholders in this domain is crucial for generating high-quality outcomes that can inform universally applicable guidelines for treatment centers globally. This is especially true for translation and implementation of innovations in bone TE as significant challenges are currently emerging in this field, including the need for guidelines tailored to specific surgical applications, developing designs for multicenter international preclinical and clinical studies that are clinically feasible, understanding the current medicolegal implications, and navigating through reimbursement processes (Ergina et al., 2009). Thus, these complexities highlight the urgent need for intensive dialog among key leaders in the field and close collaboration with industry. A dedicated stakeholder workshop focusing on the innovation of 3D-printed implants for the regeneration of long bone defects may serve as a central platform for this discussion (Laubach et al., 2023).
Noteworthy, a call for a global consensus on surgical practices is not a recent phenomenon. Over a decade ago, Atul Gawande highlighted the pressing issues in surgical care, including significant instances of fatal errors, stark variations in patient outcomes across different institutions, and unequal access to health care within the United States and internationally, with these observations dating back to the 1970s (Gawande, 2012). The quest to address bone defects, regarded as one of the most intricate and demanding challenges in orthopedics, mirrors the concerns raised by Gawande in his publication in the New England Journal of Medicine (Gawande, 2012).
As described by the Editorial Nature (2017), in the year 2000, a survey was conducted among academic surgeons to assess their belief in the value of basic scientific research (Editorial Nature, 2017). The majority of the respondents expressed their faith in the significance of research despite the increasing clinical and administrative duties affecting their productivity. The authors of the report conducted a survey among 1000 academic surgeons, and the results revealed that more than half of the participants considered basic research to be a priority in their departments. However, only one-third of them believed that surgeons could realistically succeed in basic research. Therefore, efforts to bridge the divide between scientific discovery and its practical health care applications necessitate a multidisciplinary approach, such as the organization of stakeholder workshops because these gatherings are pivotal in fostering a collaborative environment that aims to integrate research innovations seamlessly into clinical practice, thereby catalyzing the adoption of technical advancements and the foundation of new therapy concepts (Kaul and Ventikos, 2014). A suggested stakeholder workshop would assemble a diverse group of professionals, including surgeons, biomaterial scientists, biomedical engineers, legal and regulatory experts, patient and stakeholder engagement specialists, patient advisory board members, health economists, meta-researchers focusing on the science of conducting research, artificial intelligence specialists, and industry representatives from the biomaterial sector (Zeiter et al., 2020). Through collective intelligence, this assembly of experts would engage in a consensus-driven dialog to tackle the translational hurdles impeding translation and implementation of bone TE innovation (Functional Tissue Engineering Conference Group, 2008). Importantly, they might share insights and propose solutions from their varied vantage points, setting aside any institutional biases or agendas, in a concerted effort to advance the field. Participants may aim to reach agreement on crucial aspects that demand immediate attention, including planning and execution of (pre)clinical trials and the exploration and in-depth comprehension of the regulatory and reimbursement landscape (e.g., see project “Consensus Meeting on 3D-printed patient-specific Bone Implants,” CoMBI; https://osf.io/7jk2c/). Moreover, these challenges are described in detail elsewhere (Laubach et al., 2023) and illustrate the strategic path to be embarked upon to optimize the synergy between different facets of bone TE to overcome existing barriers and enable significant advances in the field of scaffold-guided bone regeneration for the treatment of long bone defects.
The comparison carried out between surgeons and BS&orTE has revealed a significant similarity in the cognitive bias, framing, on the topic of current state of the art and future perspectives of bone defect treatments. However, nuanced differences were also found between the two groups with regard to their preferences for the use of different treatment approaches. This highlights the need for interdisciplinary collaboration to exploit synergies in the future and to achieve improvements in the treatment of patients with bone defect through purposeful development of innovative treatments with new biomaterials (Soares et al., 2023). Overall, the study suggests that surgeons and BS&orTE share a similar cognitive bias, framing, when it comes to the topic of bone defect treatments. Despite this similarity, there are still nuanced differences between the two groups with regard to their preferences for different treatment approaches. From a more general perspective, the concept of “surgery and research” has emerged as a central tenet of modern surgical practice, reflecting the recognition that the pursuit of knowledge is an essential component of the ongoing professional development of both scientists and surgeons (Mahid et al., 2008). This emphasis on lifelong learning and the integration of research into clinical practice is seen as being in far excess of the specialist training period, highlighting the critical role that ongoing learning and research play in ensuring the highest standards of translational TE research.
Footnotes
Acknowledgments
The authors gratefully acknowledge the support of the Alexander von Humboldt Foundation and Queensland University of Technology, jointly funding a Feodor Lynen Research Fellowship of the Alexander von Humboldt Foundation awarded to M.L. The authors thank the various surgical (here in particular the German Society for Orthopaedics and Trauma Surgery, DGOU) and biomaterials and TE societies for their active support in providing their members the opportunity to participate in this survey study.
Authors’ Contributions
M.L., S.W., H.F.C., U.D., and D.W.H. designed the study. S.W.: programmed the survey software. M.L. and D.W.H. promoted the study to the participants. H.F.C. analysed the data. M.L., S.W., H.F.C., and D.W.H. wrote the draft, and all authors reviewed the article.
Data Sharing Statement
Data and code are available from the corresponding author upon request.
Author Disclosure Statement
D.W.H. is a cofounder of BellaSeno GmbH, an ISO 13485-certified medical technology company and a cofounder and shareholder of Osteopore International. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Funding Information
The Australian Research Council provided financial support for this project through the ARC Training Center for Multiscale 3D Imaging, Modeling, and Manufacturing (M3D Innovation, project IC 180100008).