
Abstract
Extensively researched tissue engineering strategies involve incorporating cells into suitable biomaterials, offering promising alternatives to boost tissue repair. In this study, a hybrid scaffold, Gel-DCM, which integrates a photoreactive gelatin–hyaluronic acid hydrogel (Gel) with an oriented porous decellularized cartilage matrix (DCM), was designed to facilitate chondrogenic differentiation and cartilage repair. The Gel-DCM exhibited excellent biocompatibility in vitro, promoting favorable survival and growth of human adipose-derived stem cells (hADSCs) and articular chondrocytes (hACs). Gene expression analysis indicated that the hACs expanded within the Gel-DCM exhibited enhanced chondrogenic phenotype. In addition, Gel-DCM promoted chondrogenesis of hADSCs without the supplementation of exogenous growth factors. Following this, in vivo experiments were conducted where empty Gel-DCM or Gel-DCM loaded with hACs/hADSCs were used and implanted to repair osteochondral defects in a rat model. In the control group, no implants were delivered to the injury site. Interestingly, macroscopic, histological, and microcomputed tomography scanning results revealed superior cartilage restoration and subchondral bone reconstruction in the empty Gel-DCM group compared with the control group. Moreover, both hACs-loaded and hADSCs-loaded Gel-DCM implants exhibited superior repair of hyaline cartilage and successful reconstruction of subchondral bone, whereas defects in the control groups were predominantly filled with fibrous tissue. These observations suggest that the Gel-DCM can provide an appropriate three-dimensional chondrogenic microenvironment, and its combination with reparative cell sources, ACs or ADSCs, holds great potential for facilitating cartilage regeneration.
Impact statement
In this study, we developed a hybrid Gel-DCM scaffold and demonstrated its efficacy in promoting chondrogenic differentiation and facilitating cartilage regeneration. Our findings underscore the potential of this scaffold, especially when combined with adipose-derived stem cells and articular chondrocytes, to enhance the process of cartilage repair. By providing a conducive three-dimensional chondrogenic microenvironment, the Gel-DCM scaffold offers promising prospects for clinical translation in cartilage regeneration therapies. This research lays a solid foundation for further exploration and development of advanced tissue engineering strategies aimed at addressing cartilage defects and improving patient outcomes.
Introduction
Cartilage injury is a common disease in sports medicine. Owing to its inferior self-healing capacity, articular cartilage can hardly regenerate after injury. If not treated properly, this condition often leads to tissue degeneration and, eventually, severe osteoarthritis of the entire joint. 1 Tissue engineering treatment, which integrates specific cells and diverse scaffolds to develop reparative constructs for tissue repair, is a constantly promising and evolving strategy for cartilage repair and regeneration.2,3 In tissue engineering, scaffolds play a crucial role and garner considerable attention because of their significance in providing mechanical and biological conditions essential for modulating cell development, thereby enhancing integrity and compatibility. 4 The ideal scaffold should possess appropriate physicochemical properties, desirable biocompatibility, and mechanical properties that provide a molecular and structural foundation conducive to residing cells’ attachment, growth, migration, and differentiation. 5 Moreover, the original scaffold should undergo effective degradation and replacement following the formation of regenerative tissues. 6
From a developmental perspective, the extracellular matrix (ECM) stands out as the most appropriate natural material, which not only provides a delicate environment but also allows cells to leverage their characteristics and engage in molecular interactions within this intricate network. Along with the development of tissue, ECM can also undergo self-renewal and biodegradation. 7 During the cartilage matrix decellularization process, cells and other immunogenic components are nearly eliminated, whereas crucial structural proteins are mostly preserved. 8 Decellularized ECM-based tissue engineering techniques have made significant strides in promoting chondrogenesis and cartilage injury repair.9–11 Various forms of biofabrication, such as ECM hydrogel, electrospinning, and three-dimensional (3D) printing with bioink, have been widely used in this endeavor. Numerous studies have demonstrated the ability of ECM and its derivatives to promote chondrogenesis to varying extents.7,11,12 However, it is important to note that in certain situations, ECM derivatives may not achieve the anticipated effects.13,14 One hypothesis posits that this discrepancy may be linked to the loss of bioactive components in ECM during the dissolution procedure crucial for the biofabrication of ECM derivatives. 15 Regarding scaffold functionality, both composition and pore size play critical roles. Typically, decellularized ECM is fabricated into porous scaffolds with pore sizes at the millimeter level. Research indicates that the biological functions of the scaffold can be influenced by variations in pore size.16,17 Although the consensus suggests that the pore size of a hard scaffold should exceed that of the cells, allowing for cell distribution and migration, it is essential to recognize that excessively large pores may lead to uneven cell distribution, thereby affecting cell adhesion, growth, differentiation, and ECM deposition.18,19 Conversely, research indicates that within a suitable and relatively smaller range, scaffold pore size can create a specialized microenvironment conducive to 3D cell aggregation, leading to a notable increase in the cell-specific synthesis of cartilaginous matrix proteins.16,20,21
Hydrogels are 3D polymer networks that are highly hydrous and porous, permitting the diffusion of diverse micromolecules, nutrients, and the ingrowth, proliferation, and differentiation of cells. 22 Owing to its capability of generating unique 3D microenvironments and ultrastructures similar to the ECM on a microscale, hydrogel has been applied as a promising alternative scaffold for repairing various types of tissue. 23 Gelatin–methacrylate (GelMA), a photoreactive hydrogel, has been thoroughly examined for its physical and biochemical attributes across diverse applications. 24 GelMA has become a favored option in tissue engineering owing to its adjustable properties like composition, crosslinking, density, degradation rate, and mechanical strength. This versatility makes GelMA promising for tissue repair, allowing manipulation during synthesis and processing. 25 In our study, we used a composite photoreactive hydrogel comprising GelMA and hyaluronic acid, in combination with lithium phenyl-2,4,6-trimethylbenzoylphosphinate, which is a photoinitiator to initiate photoreactive cross-linking. The hydrogel has a pore size of around 50 μm and a water content exceeding 90%. 26
For reparative cells source, autologous articular chondrocytes (ACs) are typically used in articular cartilage repair and have achieved satisfactory clinical outcomes. 27 As multipotent stem cells, adipose-derived stem cells (ADSCs) are frequently used in tissue engineering owing to their wide distribution, easy accessibility, and potential for multidirectional differentiation. Under efficient induction, ADSCs can differentiate into various cell types, including chondrocytes. Research works have shown the significant potential of ADSCs in promoting cartilage regeneration in animal experiments. 28
Based on the aforementioned information, we developed a hybrid scaffold, Gel-DCM, by harnessing the advantages of ECM materials and optimizing scaffold pore size. Through integrating a photoreactive hydrogel composed of gelatin and hyaluronic acid into an oriented porous decellularized cartilage matrix (DCM) scaffold, our goal was to achieve dual optimization of structure and composition. This innovative approach was designed to overcome the limitations of conventional scaffold designs and create a platform that closely mimics the native cartilage environment. By incorporating ECM for biomimetic composition and using the hydrogel to facilitate 3D cultivation, the Gel-DCM scaffold was engineered to create an optimal microenvironment conducive to the proliferation and chondrogenic differentiation of both human articular chondrocytes (hACs) and human adipose-derived stem cells (hADSCs). In addition, the effectiveness of the Gel-DCM scaffold in combination with hACs and hADSCs was evaluated for enhancing in vivo cartilage repair in a rat model. The study’s overall design is depicted in Figure 1.
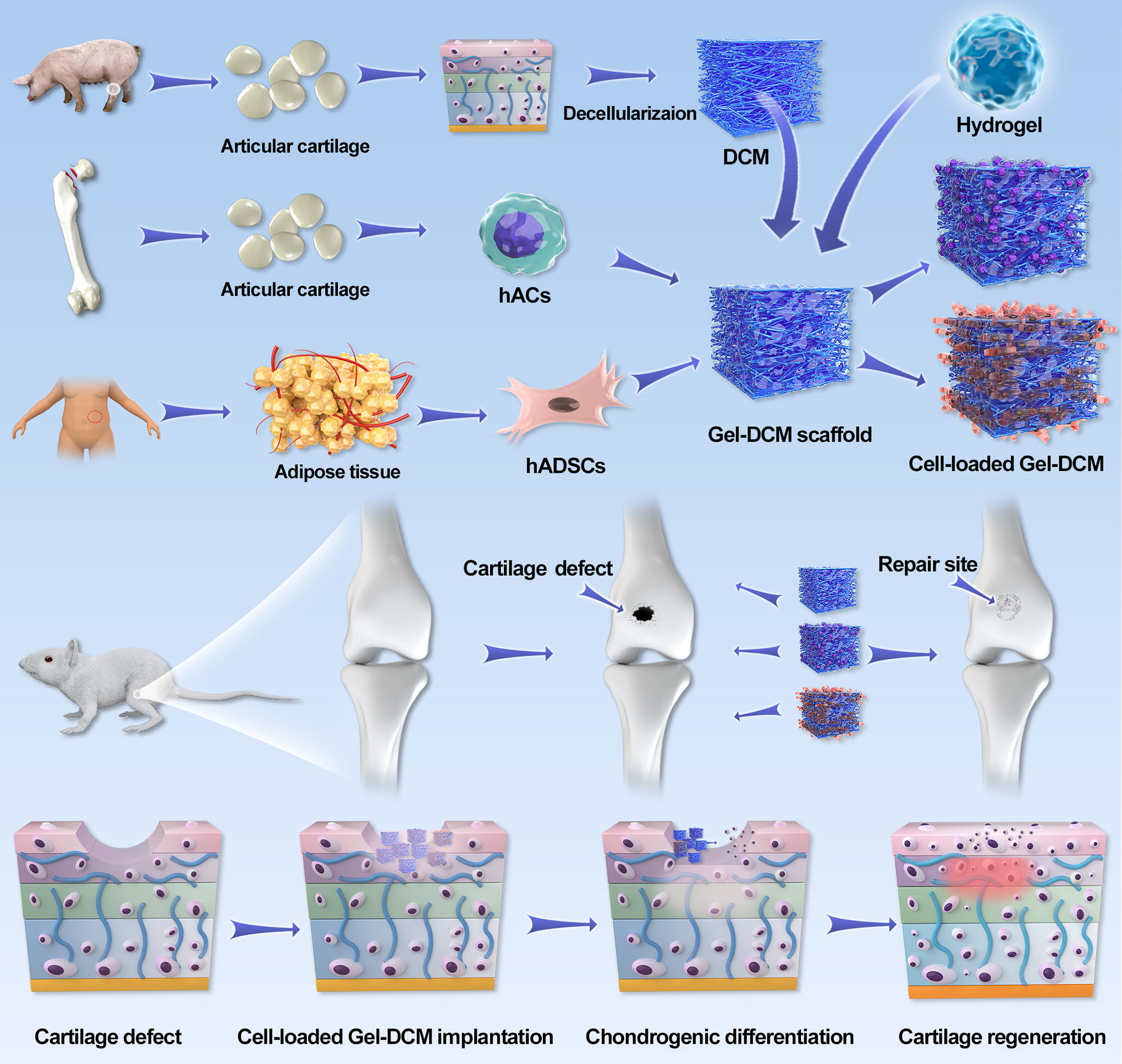
Graphical illustration of the study.
Materials and Methods
Isolation and culture of hADSCs and hACs
Human subcutaneous adipose tissue was obtained from four obese donors who underwent abdominal liposuction in the plastic surgery department. The donors’ ages ranged from 18 to 35 years, and the procedures were carried out with the approval of the Ethics Committee of Beijing Friendship Hospital, Capital Medical University. The collected adipose tissue underwent three washes with sterile phosphate-buffered saline (PBS) solution, and any connected muscle and vessels were removed. Subsequently, the tissue was placed into a 50 mL centrifuge tube and subjected to digestion with collagenase type I (0.075%) (Gibco) for 45 min on a shaker at a constant temperature of 37°C and centrifuged at a speed of 1800 rpm for 10 min. The cells sedimented were resuspended in Dulbecco’s modified Eagle’s medium (DMEM) of low glucose (1000 mg/L) (Gibco) supplemented with fetal bovine serum (10%) (FBS, ThermoFisher Scientific Life Sciences), streptomycin (0.1 mg/mL), and penicillin (100U/mL). Cells were plated onto sterile cell culture dishes at a density of 4 × 104/cm2. Passaging of cells occurred upon reaching 80–90% confluence, and passage 3 hADSCs were used for the following studies. Unless otherwise specified, all subsequent culture media for hADSCs followed the formulation described earlier.
Human articular cartilage was collected from the femoral head cartilage of four patients with femoral neck fractures within 7 days of undergoing total hip arthroplasty. The patients, aged between 55 and 65 years, underwent procedures following approved protocols by the Ethics Committee of Beijing Friendship Hospital, Capital Medical University. The cartilage slices were scraped off from the femoral head and cut into pieces (approximately 1 mm3). Subsequently, the cartilage pieces underwent three washes with sterile PBS. The tissue was placed into a 50 mL centrifuge tube and digested with 2 g/L collagenase type II (Gibco) at 37°C for 6 h on a shaker. The digestive mixture was filtered, and the solution was centrifuged for 10 min at 1200 rpm. The cells sedimented were resuspended in complete DMEM/F12 (Gibco) culture medium supplemented with FBS (10%), streptomycin (0.1 mg/mL), and penicillin (100 U/mL) and transferred to 75 cm2 culture flasks. Cells at passage 2 were used in the subsequent studies. Unless otherwise specified, all subsequent culture media for hACs followed the formulation described earlier.
Preparation and characterization of the DCM
The oriented porous DCM scaffold was prepared following the previously described method. 29 Briefly, cartilage tissue from porcine knee joints was harvested under aseptic conditions within 6 h of sacrifice from a local slaughterhouse. The harvested cartilage was segmented into pieces and subsequently rinsed twice with sterile PBS. After decellularization, the cartilage matrix was physically pulverized and made into a 3% (w/v) suspension for differential centrifugation to obtain DCM filaments. Next, the DCM filament suspensions were treated with genipin (Sigma) at a concentration of 0.2% (w/v) at 37°C for 120 min for cross-linking. Afterward, the mixtures were placed into a 5 mm cylinder mold, and the DCM scaffold was formed by freeze-drying. Finally, DCM scaffolds with a diameter of 5 mm were obtained and sterilized by 60Co γ-irradiation. Staining for 4′,6-diamidino-2-phenylindole (DAPI) was used to evaluate the result of decellularization.
Fabrication of the hybrid Gel-DCM scaffold
The hybrid Gel-DCM scaffold was fabricated by integrating a photoreactive hydrogel (Avatarget Biotechnology Co. Ltd.) into the DCM scaffold. This photoreactive hydrogel, a blend of gelatin methacryloyl and hyaluronic acid, remains in liquid form at room temperature and transforms into a gel under 405–420 nm blue light irradiation for 1 min. This gelation is facilitated by the acylation and cross-linking of lysine in gelatin and hydroxylysine amino acids. The hydrogel possesses a pore size of approximately 50 μm and a water content exceeding 90%. The DCM scaffold displays a porous architecture with microfilaments oriented in a wide direction, allowing for the incorporation of the hydrogel. The liquid hydrogel permeated the spongy DCM scaffold and evenly dispersed. Gelation is initiated by blue light irradiation for 1 min, resulting in the formation of the hybrid Gel-DCM scaffold. Scanning electron microscope (SEM) analysis was used to visualize the microstructure of the hybrid scaffold.
Cell seeding on the hybrid Gel-DCM scaffold
Human ADSCs at passage 3 and hACs at passage 2 were used in the experimental investigation. The cell suspension was prepared in serum-free medium at a density of 106 cells/mL and mixed with the liquid photoreactive hydrogel at the ratio of 2:3, resulting in a total volume of 200 μL, and thoroughly mixed. Subsequently, 20 μL cell-loaded liquid hydrogel, containing approximately 8000 cells, was added into a sterile cylindrical mold. After 1 min of irradiation under 405–420 nm blue light, a cylindrical cell-loaded gel was prepared for in vitro study. For the cell-loaded Gel-DCM composite, 20 μL cell-loaded liquid hydrogel was infused into the porous DCM with 1 mm thickness and 1.5 mm diameter. Gelation was then initiated by blue light irradiation for 1 min.
Cell viability and chondrogenic differentiation assessment
After 3 and 7 days of cultivation, live/dead staining was conducted to assess cell viability within the scaffold. The percentage of live cells, indicated by green fluorescence, and dead cells, indicated by red fluorescence, was calculated.
After 7 days of cell culture within the scaffold, RNA was extracted, and gene expression level was analyzed. The total RNA was extracted using Trizol Reagent (Invitrogen), and complementary DNA was synthesized from 2 µg total RNA per sample using a cDNA synthesis kit (Takara Bio Inc.). The expression of collagen type I (COL1A2), collagen type II (COL2A1), SOX9, aggrecan (ACAN), collagen type X (COL10A1) was determined through quantitative polymerase chain reaction (qPCR). The primers designed for qPCR are listed in Supplementary Table S1. To perform qPCR, the target gene expression was analyzed using a Power SYBR Green PCR master mix (Applied Biosystems) in a conventional culture flask under two-dimensional (2D) cultivation conditions. The expression level of each targeted gene was determined using the 2−ΔΔCt method and normalized to that of GAPDH.
In vivo cartilage repair by cell-loaded Gel-DCM composite
Healthy female Sprague–Dawley rats (32 rats, with 8 knees per group for each time point), weighing 200–250 g, were anesthetized using 3% sodium pentobarbital (40 mg/kg body weight, intraperitoneal injection). The knee joint was accessed through a medial parapatellar approach. The patella was laterally displaced and dislocated to reveal the patellofemoral groove. A sterile punch was used to generate a full-thickness cylindrical osteochondral defect, measuring 1.5 mm in diameter and 1 mm in depth, at the trochlear groove’s center. The dimensions of the Gel-DCM scaffold were tailored to match the defect size precisely. To achieve this, the DCM was trimmed to a diameter of 1.5 mm and a thickness of 1 mm. Subsequently, it was loaded with 20 µL of liquid cell-loaded hydrogel or blank hydrogel (without cells) as appropriate for the experimental condition. Following the loading process, the scaffold was cross-linked under blue light. The scaffolds were all prepared under sterile conditions and immediately transferred to fill the defect area once the defect modeling was completed. These rats were categorized into four groups: osteochondral defect without treatment (control group), defect filled with cell-free Gel-DCM scaffold, defect filled with hACs-loaded Gel-DCM, and defect filled with hADSCs-loaded Gel-DCM. After surgery, rats were placed back into cages without joint immobilization. At 6 and 12 weeks, rats were sacrificed for harvesting the knee joint. Femur end samples from each group at each time point were collected for gross observation and quantitative macroscopic scoring based on the International Cartilage Research Society (ICRS) macroscopic morphology scoring system as shown in Supplementary Table S2.
Microcomputed tomography analysis
Microcomputed tomography (micro-CT) (GE) was used to assess the subchondral bone reconstruction. Rat distal femoral condyles (n = 8) were initially fixed for 48 h in paraformaldehyde (4%), followed by micro-CT scanning. A region of interest with a diameter of 1.5 mm and a height of 1 mm was selected, which is akin to the defect scale. Bone mineral density (BMD) and the ratio of bone volume to tissue volume (BV/TV) values were calculated and analyzed by using Micro ViewTM ver.2.2.
Histological evaluation
Rat distal femoral condyles (n = 8) were fixed using 4.0% paraformaldehyde for 1 week, followed by decalcification in a 10% ethylenediaminetetraacetic acid solution over 3 weeks. Post-decalcification, the distal femoral condyles were embedded in paraffin wax and sliced along the sagittal direction of the defect, with each slice having a thickness of 5 μm. These slices underwent various staining procedures: hematoxylin and eosin (H&E) staining for morphological assessment, Safranin-O/Fast Green and toluidine blue staining to evaluate glycosaminoglycan (GAG) deposition, and immunohistochemical staining targeting COL 2A1 (rat, 1:200, ab34712) for assessing cartilage-specific matrix content. Semiquantitative analysis of Safranin-O and COL II staining of repaired tissue was conducted using ImageJ-Pro Plus v6.0 software (National Institutes of Health). A histological scoring system was used to assess cartilage repair in rat chondral defects. It contains seven aspects relating to the description of neo-formed tissue and adjacent cartilage as shown in Supplementary Table S3. The total score was obtained by adding the score values of each aspect. The scoring was conducted blindly by three independent researchers.
Statistical analysis
All data were expressed as mean ± standard deviation and analyzed by one-way analysis of variance with a post hoc test. A significance level of p < 0.05 was deemed statistically significant, with asterisks denoting significance levels (*p < 0.05, **p < 0.01, and ***p < 0.001).
Results
Characterization of the hybrid Gel-DCM scaffold
After the decellularization procedure, DAPI staining indicated the removal of most nuclear components within the cartilage lacuna (Fig. 2a). SEM results demonstrated that the DCM scaffold exhibited a multimicroporous configuration with directional microfilaments oriented in parallel within the vertical cross-section. This structure not only replicates the architecture of the natural matrix but also enables the integration of the photoreactive hydrogel. In addition, SEM examination confirmed the architecture of the hybrid Gel-DCM scaffold, illustrating the integration of the hydrogel into the pores of the DCM (Fig. 2b).

Decellularization, fabrication, and characterization of scaffolds.
Biocompatibility of the hybrid Gel-DCM scaffold
As demonstrated by live/dead staining (Fig. 3a–b), the majority of hADSCs and hACs within the pure photosensitive hydrogel, DCM, and hybrid scaffold exhibited robust viability following 3- and 7-day incubation periods, with minimal occurrence of dead cells. Across all groups, living cells consistently maintained a ratio exceeding 90%. These results demonstrate the satisfactory biocompatibility of the hybrid Gel-DCM scaffold, affirming its competence to effectively bolster cell survival and growth.
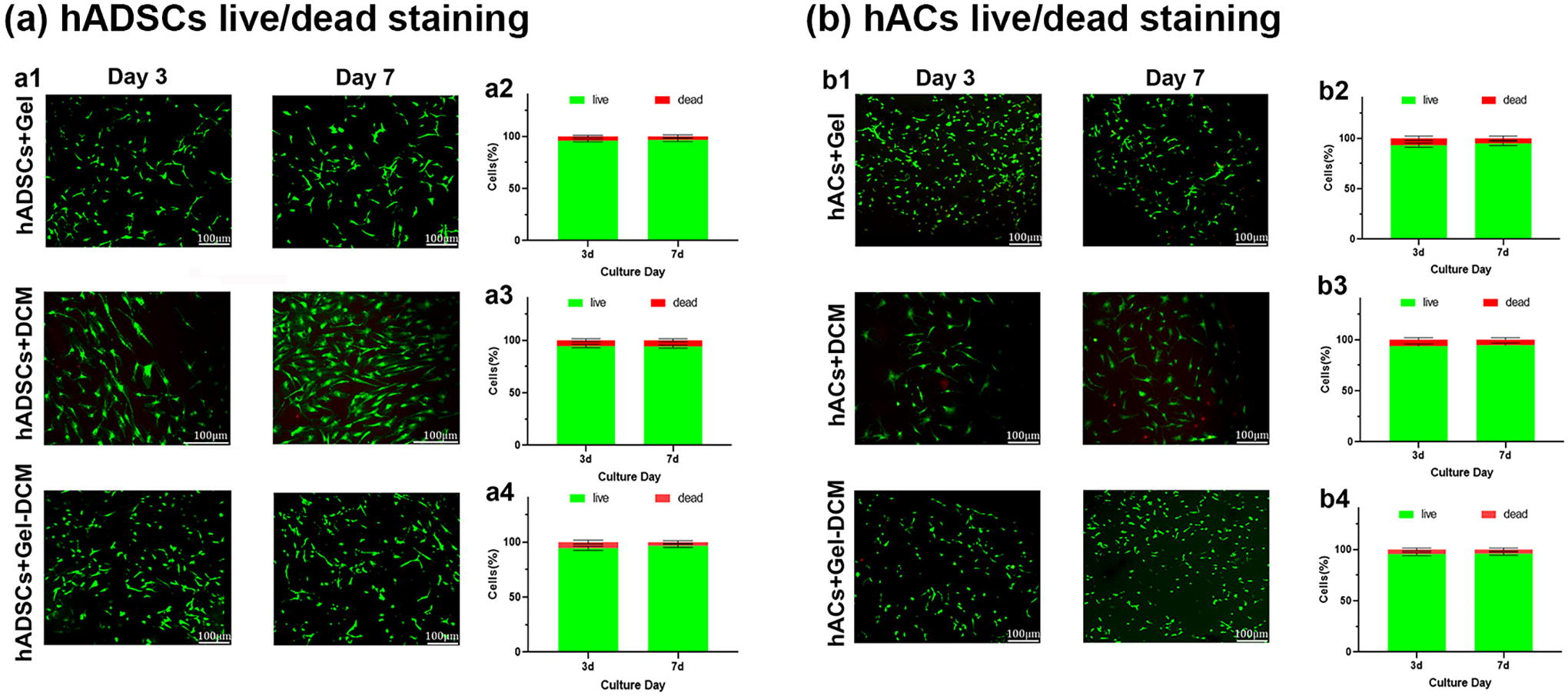
Biocompatibility evaluation of scaffolds for hADSCs and hACs.
In vitro chondrogenic differentiation
The scaffold’s role in chondrogenic differentiation was confirmed through qPCR of chondrogenesis markers (SOX9, ACAN, COL2A1), dedifferentiation marker (COL1A2), and hypertrophic marker (COL10A1). For hADSCs, in comparison with the 2D flask cultivation control group, the expression levels of SOX9, ACAN, and COL2A1 were notably increased in the Gel-DCM and Gel groups (p < 0.05). In addition, the expression levels of these three genes were significantly higher in the Gel-DCM group compared with the Gel group (p < 0.05) (Fig. 4a1–a3). Moreover, the COL1A2 expression in the Gel-DCM group was comparable with that in the control group but notably reduced compared with the Gel group (p < 0.05) (Fig. 4a4). In comparison with the control group, the relative expression of COL10A1 showed an increase in both the Gel-DCM and Gel groups, whereas the expression in the Gel-DCM group exhibited a significant decrease in contrast to the Gel group (p < 0.05) (Fig. 4a5).
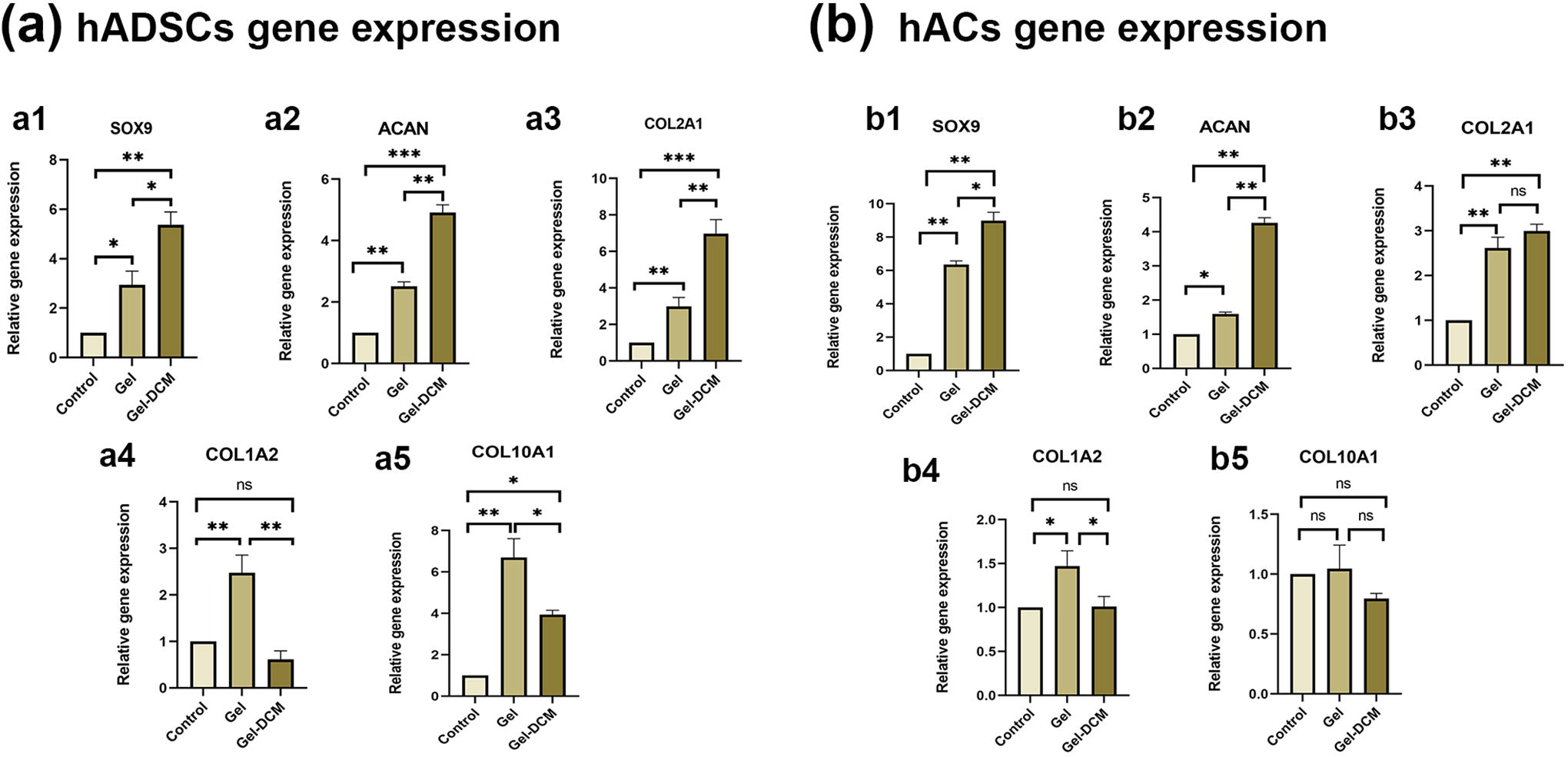
Chondrogenic differentiation of hADSCs and hACs.
For hACs, the expression levels of SOX9 and ACAN were notably elevated in both the Gel-DCM and Gel groups in contrast to the control group (p < 0.01). Furthermore, the Gel-DCM group exhibited notably higher expressions of these markers compared with the Gel group (Fig. 4b1–b2). In addition, COL2A1 expression was notably elevated in both the Gel-DCM and Gel groups (p < 0.05), with no discernible difference between them (Fig. 4b3). Conversely, the expression level of COL1A2 showed a significant increase in the Gel group in contrast to both the Gel-DCM and control groups, whereas no noticeable difference was observed between the Gel-DCM and control groups (Fig. 4b4). Notably, the expression of COL10A1 did not display statistically significant differences among all groups (Fig. 4b5).
Macroscopic assessment of the repaired tissue
At 6 weeks after the operation, macroscopic examination showed that the defect was scarcely filled in the control group, with an uneven surface and clear defect boundaries. In the Gel-DCM group, defects were filled by granulation and fibrous tissue with an obvious tissue boundary, exhibiting poor integration. In comparison, in the hACs + Gel-DCM group, it was observed that the defect was filled with tough tissue, with color and texture similar to that of the surrounding normal cartilage surface. The repaired tissue surface was relatively smooth, but the boundary between the defect and the surrounding normal cartilage could still be observed, with slight integration present. In the hADSCs + Gel-DCM group, the defect site was filled with transparent and shiny tough tissue, with color and texture similar to that of the surrounding normal cartilage surface. The surface of the repaired tissue was smooth and even, with partial fusion between the repaired tissue and the surrounding normal cartilage. The boundary at the fusion site was almost indistinguishable (Fig. 5a). At 12 weeks, the cartilage defect was mostly filled in all groups. However, the surface was still unsmooth, and the defect boundaries were still clear in the control group. Compared with 6 weeks, better tissue regeneration and integration were observed in the Gel-DCM and hACs + Gel-DCM groups. However, the tissue boundary between the regenerated tissue and the normal cartilage remained clearly visible. In the hADSCs + Gel-DCM group, the defect was completely filled with regenerated chondroid tissue whose color and texture of the regenerated tissue were nearly indistinguishable from that of the normal cartilage, indicating desirable integration (Fig. 5a).
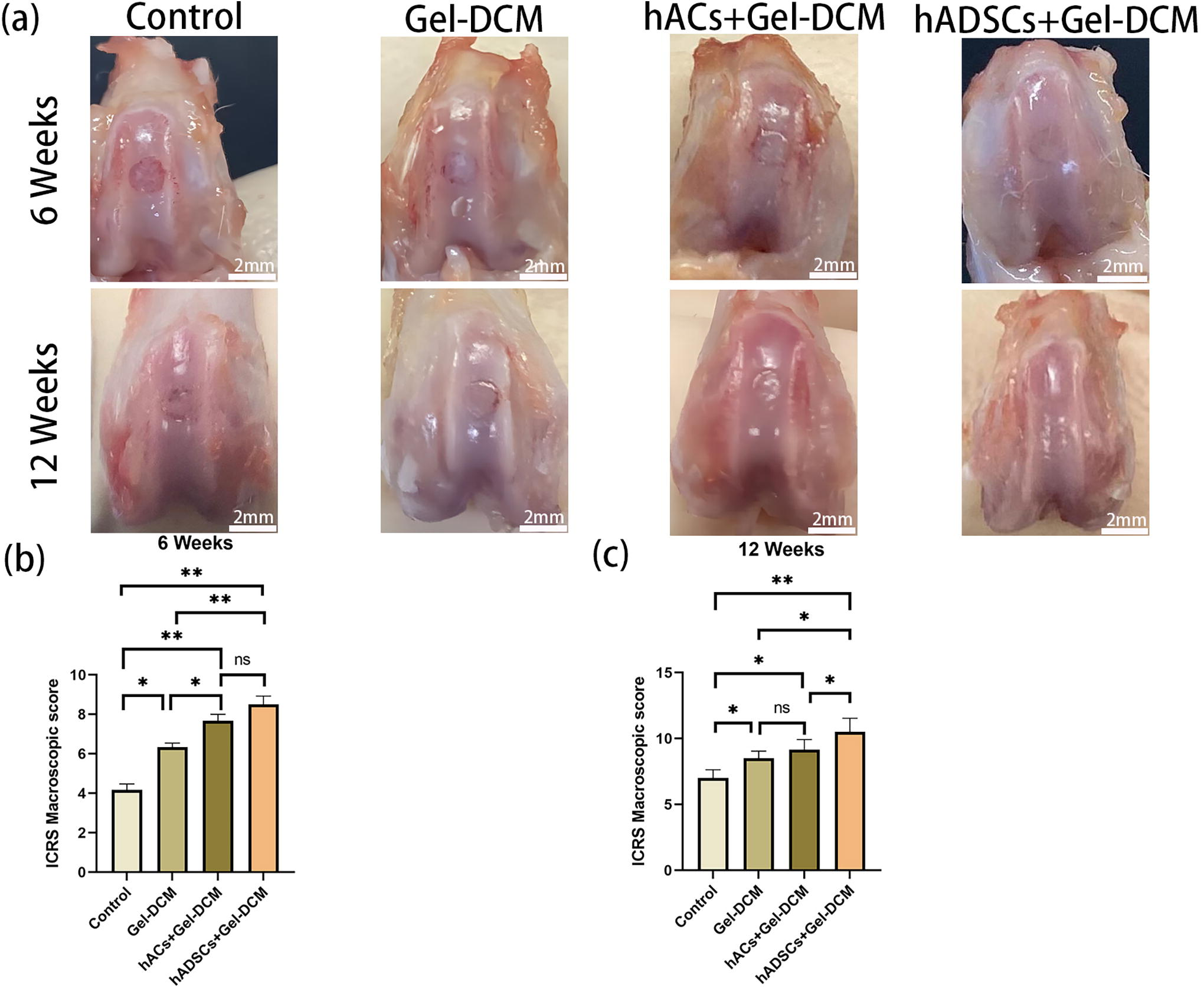
In vivo repair of cartilage defects in rat knee joints (n = 8).
Afterward, quantitative macroscopic scoring was conducted. At 6 weeks, ICRS scores were notably elevated in the Gel-DCM, hACs + Gel-DCM, and hADSCs + Gel-DCM groups compared with the control group. Moreover, both the hACs + Gel-DCM and hADSCs + Gel-DCM groups demonstrated higher score than the Gel-DCM group, whereas there was no discernible distinction between the hACs + Gel-DCM and hADSCs + Gel-DCM groups (Fig. 5b). At 12 weeks, the ICRS score for the hADSCs + Gel-DCM group was superior to that of the other three groups. The Gel-DCM and hACs + Gel-DCM groups showed no statistically significant difference, but both received higher scores than the control group (Fig. 5c).
Histological assessment of the repaired tissue
At 6 weeks after the operation, HE staining revealed that the defect areas in both the Gel-DCM and control groups were partially occupied by fibrous tissues. In addition, no deposition of GAG and COL II fibers was observed through Safranin-O and toluidine blue staining, as well as immunostaining against COL II (Fig. 6, 7). In addition, the surface of the repaired area displayed irregularities and lacked proper integration with the surrounding healthy cartilage. Conversely, defects in the hACs + Gel-DCM group were predominantly filled with repaired tissue exhibiting moderate GAG and COL II deposition (Fig. 6-7). Notably, the hADSCs + Gel-DCM group demonstrated hyaline cartilage regeneration, characterized by evident cartilaginous matrix deposition within the neo-formed tissue, showing robust GAG content and strong staining with anti-COL II antibody (Fig. 6, 7).
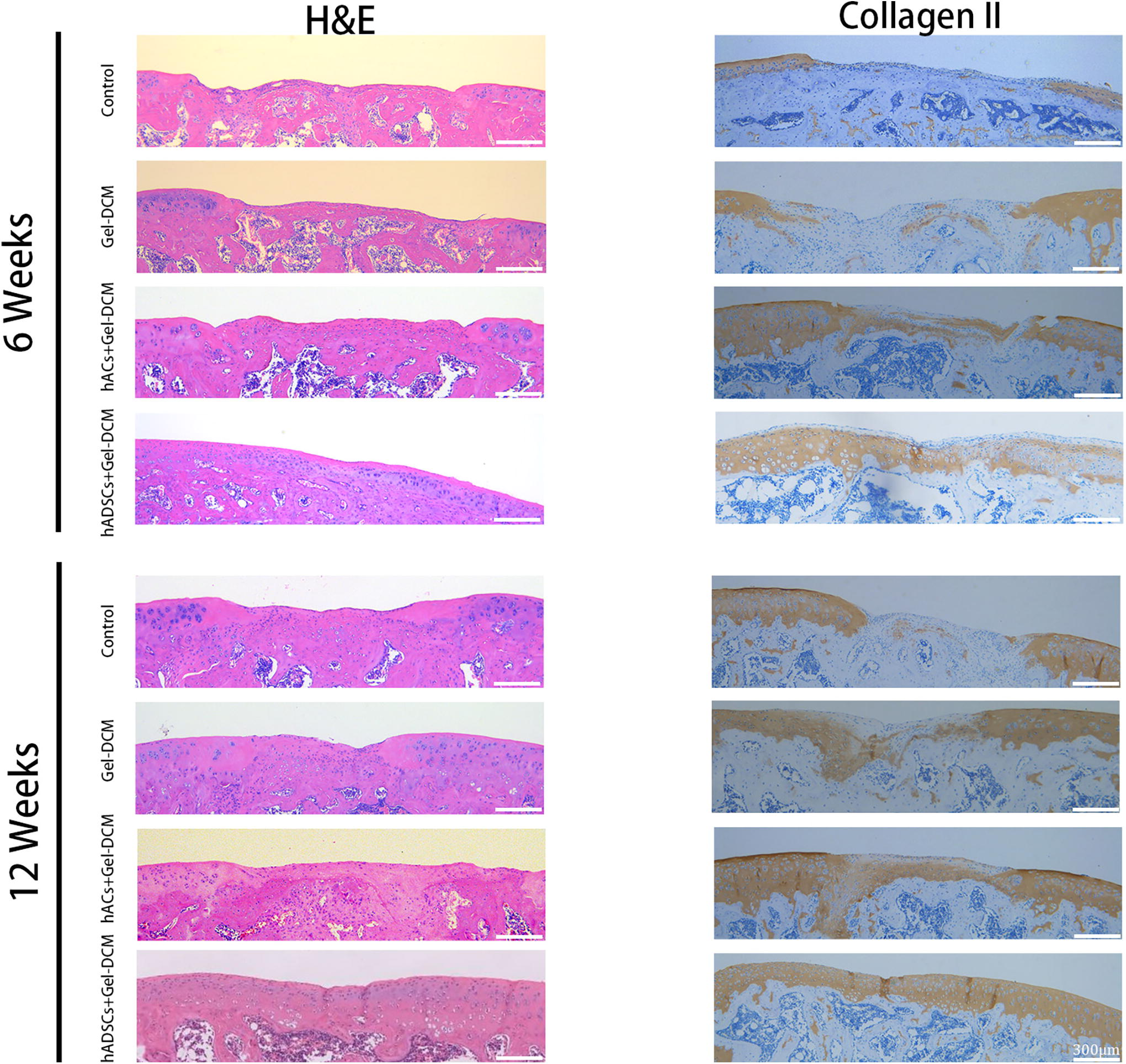
Histological evaluation of repaired tissue at 6 and 12 weeks (n = 8). Representative H&E staining and collagen type II immunostaining images of repaired rat knees at 6 weeks and 12 weeks. H&E, hematoxylin and eosin.
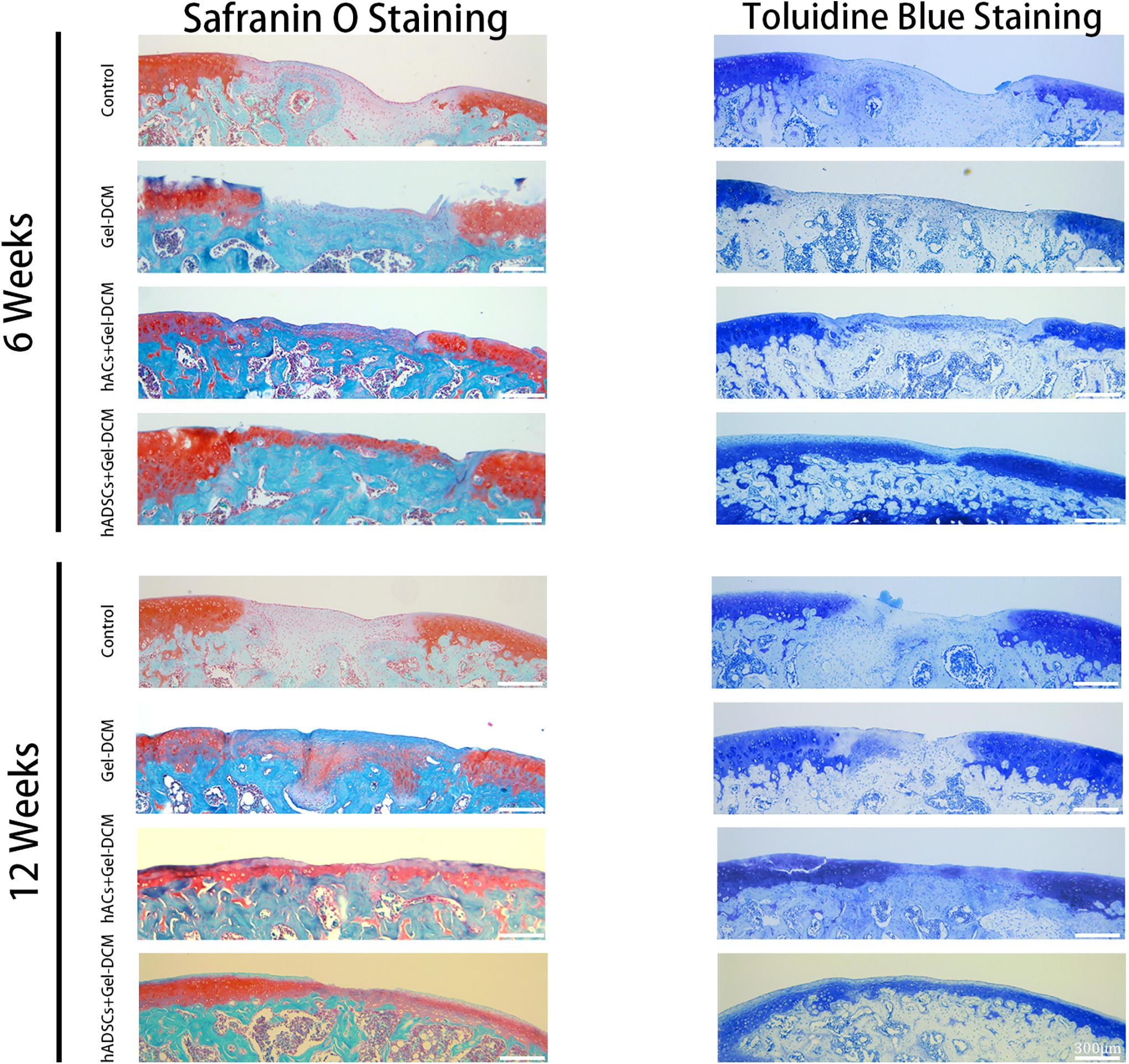
Histological evaluation of repaired tissue at 6 and 12 weeks (n = 8). Representative Safranin-O/Fast Green and toluidine blue staining images of repaired rat knees at 6 weeks and 12 weeks.
At 12 weeks, the control group continued to show repaired tissues primarily composed of fibrous tissue, with minimal GAG deposition and COL II fibers (Fig. 6, 7). In contrast, the Gel-DCM groups showed improved repair, with predominantly fibrocartilaginous tissue characterized by a flattened surface, moderate GAG deposition, and partial COL II staining compared with the 6-week time point (Fig. 6, 7). Notably, the neo-formed tissue in both the hACs + Gel-DCM and hADSCs + Gel-DCM groups displayed hyaline cartilaginous regeneration, with a layout akin to that of normal cartilage. The regenerated tissue appeared completely smooth, with significant deposition of GAGs and COL II in the matrix. Moreover, chondrocyte cellularity and distribution within the neo-formed tissue closely resembled those of the surrounding normal cartilage (Fig. 6, 7). Semiquantitative analysis revealed significantly higher Safranin-O-positive area and COL II deposition in both the hACs + Gel-DCM and hADSCs + Gel-DCM groups in contrast to the control group at both time points. Furthermore, the hADSCs + Gel-DCM group exhibited superior outcomes relative to the hACs + Gel-DCM group (Supplementary Fig. S1).
Histological scoring of the repaired tissue
Histological scoring was performed to quantitatively assess cartilage repair. At 6 weeks after the operation, the hADSCs + Gel-DCM group garnered the highest total score compared with the other three groups (p < 0.05). In addition, both the hACs + Gel-DCM and the Gel-DCM groups obtained higher total scores in contrast to the control group (p < 0.05). However, no significant distinctions were detected between the Gel-DCM and hACs + Gel-DCM groups (Fig. 8h). Scores for each aspect of the scoring system were also calculated and plotted (Fig. 8a–g). Similar findings were observed at 12 weeks, with both the hADSCs + Gel-DCM and hACs + Gel-DCM groups achieving higher total scores than the Gel-DCM and control groups (p < 0.05) (Fig. 9h). Furthermore, the total score attained in the Gel-DCM group was notably superior to that of the control group (p < 0.05) (Fig. 9a–g).
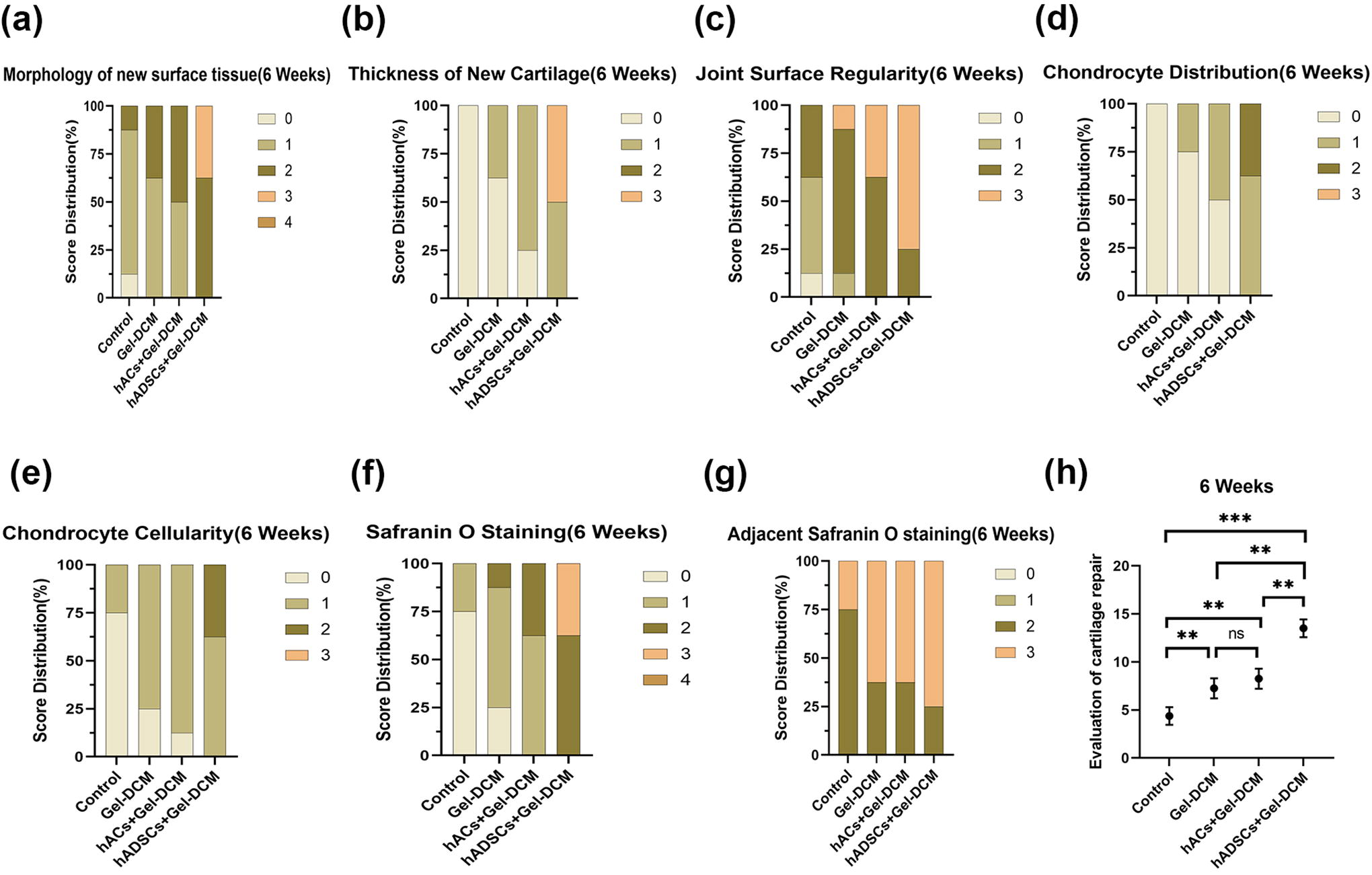
Histological evaluation of the repaired tissue at 6 weeks (n = 8).
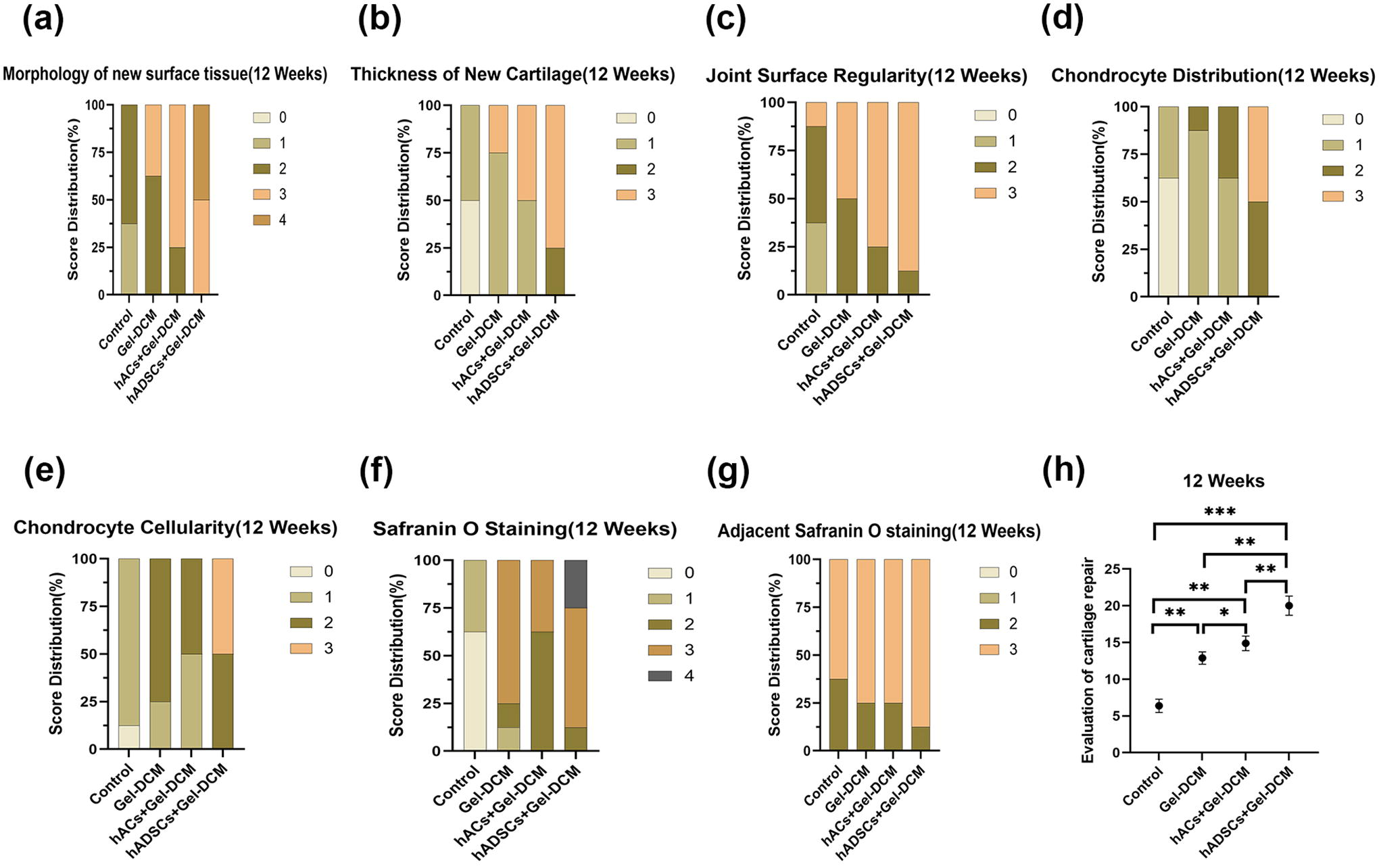
Histological evaluation of the repaired tissue at 12 weeks (n = 8).
Evaluation of subchondral bone reconstruction
Micro-CT scanning illustrated that subchondral bone trabecula reconstruction followed a pattern from the periphery to the center and from the bottom to the top in all groups (Fig. 10a, –b). At 6 weeks, the hADSCs + Gel-DCM, hACs + Gel-DCM, and Gel-DCM groups all showed increased formation of neo-formed bone trabeculae compared with the control group (Fig. 10a). Correspondingly, BMD and BV/TV values in these three treating groups exhibited a remarkable increase compared with those in the control group (p < 0.05). Moreover, the hADSCs + Gel-DCM group exhibited higher values for both BMD and BV/TV compared with the Gel-DCM group (p < 0.05) (Fig. 10c, d).
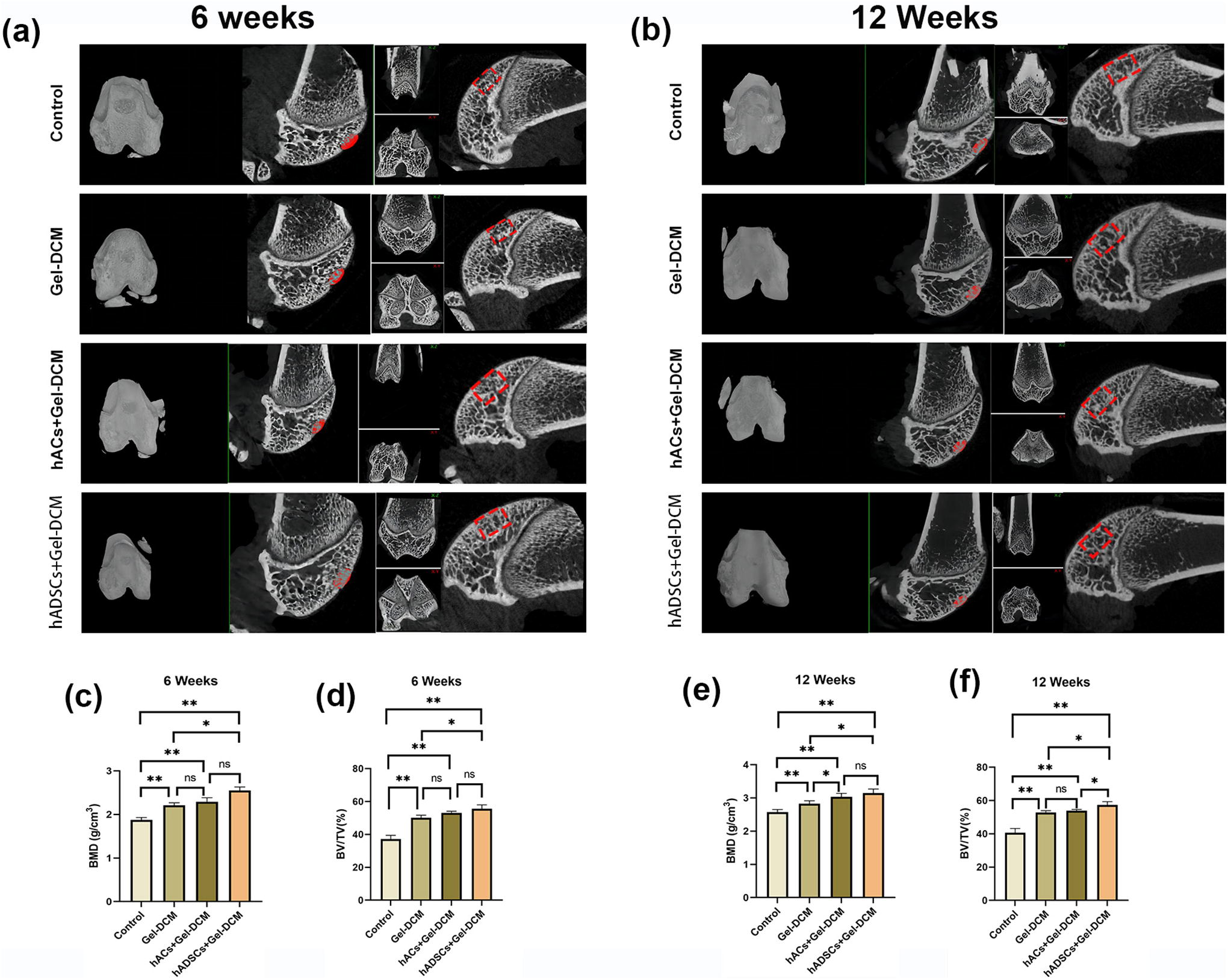
Microcomputed tomography (micro-CT) scan of repaired knees at 6 and 12 weeks (n = 8).
At 12 weeks, the BMD and BV/TV values were markedly elevated in both the hADSCs + Gel-DCM and hACs + Gel-DCM groups, as well as in the Gel-DCM group, in contrast to the control group (p < 0.05) (Fig. 10e, f). Regarding BMD, both the hACs + Gel-DCM and hADSCs + Gel-DCM groups obtained higher values than the Gel-DCM group (p < 0.05); however, there was no notable distinction between the hACs + Gel-DCM and hADSCs + Gel-DCM groups (Fig. 10e). Concerning BV/TV, the hADSCs + Gel-DCM group achieved a higher value than both the Gel-DCM and hACs + Gel-DCM groups, whereas no notable disparity was noted between the Gel-DCM and hACs + Gel-DCM groups (Fig. 10f).
Discussion
Given the constrained regenerative capacity of cartilage injuries, achieving functional hyaline cartilage regeneration remains challenging. Typically, the outcome is fibrocartilaginous repair lacking elasticity and strength, or damage spreading to adjacent structures, possibly leading to severe osteoarthritis. Current strategies include microfracture, osteochondral transplantation, autologous chondrocyte transplantation, and tissue engineering techniques. 30 These aim to achieve cartilaginous repair by introducing reparative components or inducing cellular repair in situ. Tissue engineering has revolutionized regeneration concepts, offering diversified and personalized reparative units through the integration of bioactive molecules, seeded cells, and functional scaffolds, adaptable to various tissue injuries. 31 Effective biofunctional scaffolding systems are essential for promoting cellular normal physiological development at the injury site to facilitate tissue regeneration. 32
The ECM is the external microenvironment secreted by cells during their growth and development, comprising fibrous structural proteins, proteoglycans, GAGs, and various cell growth factors and enzymes. It serves to provide support, facilitate communication between cells and molecules, and regulate cell differentiation and physiological activities. 33 Research has shown that coculture chondrocytes with decellularized cartilage sheets could enhance the chondrogenic effect, and no additional growth factors were required, as the required growth factors including transforming growth factor Beta (TGF-β) and bone morphogenetic protein (BMP) were preserved in the DCM. 34 In order to mimic the natural ECM from both structural and compositional perspectives, after the removal of immunogenic substances, the ECM components left are ideal biological scaffolds to mimic the natural microenvironment. Native cartilage ECM-derived bioscaffolds have been extensively used in cartilage regenerative treatment and have shown a conducive effect for enhancing cartilage repair.11,12
Based on our findings regarding the ultrastructure of DCM and current research works on the pore size of DCM, nondissolving DCM has internal pore sizes much larger than the size of cells, which cannot support the spreading and aggregation of cells in a conducive 3D microenvironment.16,20,35 GelMA hydrogel is favorable for the 3D aggregation of cells in terms of pore size and structure. However, owing to limitations in its composition, its functionality in chondrogenesis is not particularly prominent when used alone. 14 So, in such a scenario, we contemplated combining the compositional advantages of DCM with the structural benefits of GelMA to construct a composite scaffold, aiming to achieve dual optimization of composition and structure.
In our work, we developed a novel hybrid scaffold consisting of a 3D hydrogel that is synthesized based on a natural ECM component, hyaluronic acid, and DCM. As mentioned earlier, the DCM contained natural components of cartilage ECM, and the photoreactive hydrogel displayed suitable porous networks similar to natural ECM architecture. The combination of hydrogel and DCM not only mimics the composition of native cartilage but also truly realizes the 3D culture for cells at the gel status. Taking into account the aforementioned points, it can be concluded that the Gel-DCM scaffold creates a biofunctional environment supportive of both cell growth and chondrogenic differentiation. Masaeli et al. discovered that hACs and hADSCs seeded on decellularized ECM-refined scaffolds exhibited higher levels of chondrogenic gene expression in comparison with cells seeded onto scaffolds without ECM modification. This suggests that the inclusion of decellularized ECM components may direct the chondrogenic differentiation of ADSCs. 36 Our in vitro results similarly concluded that the hybrid scaffold exhibited superior chondrogenic induction. Interestingly, we observed upregulation of chondrogenic genes in hADSCs cultured in the hydrogel. The inclusion of hyaluronic acid in the photosensitive hydrogel might explain this phenomenon, given its role as a crucial component of the cartilage matrix. Previous research has demonstrated that bioscaffolds derived from hyaluronic acid can stimulate the chondrogenic differentiation of stem cells and facilitate cartilage regeneration. 37 In terms of COL 10 expression, indicative of chondrocyte hypertrophy and ossification, the Gel group exhibited higher levels in contrast to the Gel-DCM group. This suggests that the hybrid Gel-DCM scaffold possesses greater potential to induce hADSCs toward a chondrogenic lineage. In addition, during hACs cultivation, dedifferentiation inevitably occurs as chondrocytes undergo monolayer expansion in 2D mediums, resulting in inferior cartilaginous matrix deposition. 38 In our study, compared with the control group, both the Gel and the Gel-DCM groups showed significant upregulation in the expression levels of chondrogenic genes SOX9, ACAN, and COL2A1. Moreover, these genes showed higher expression in the Gel-DCM group than in the Gel group, particularly for SOX9 and ACAN. Notably, the Gel group exhibited higher expression levels of COL1A2 compared with both the Gel-DCM and control groups. These findings suggest that 3D scaffold cultivation helps maintain chondrocytes in a chondrogenic phenotype in vitro, with this effect being more pronounced when using the hybrid scaffold. Overall, Gel-DCM provides a suitable microenvironment for cell chondrogenic differentiation.
By introducing exogenous cells or recruiting endogenous reparative cells, a biological scaffold is able to fulfill its function for enhancing tissue repair. It is certified that implanting cells onto a scaffold before transplantation could potentially enhance the functionality and effectiveness of tissue repair. 39 ADSCs are a preferred choice in tissue engineering because of their easy availability and multidirectional differentiation potential. 40 Next, we evaluated the functionality of cartilage injury repair of the hybrid scaffold loaded with hADSCs and hACs in a rat cartilage defect experimental model. Histomorphometry and radiographic analysis revealed that at both 6 and 12 weeks after the surgery, the hADSCs + Gel-DCM group presented excellent regeneration resembling hyaline cartilage, along with effective subchondral bone reconstruction. Although not as effective as the hADSCs + Gel-DCM group, the hACs + Gel-DCM group also showed some degree of hyaline-like cartilage repair at both time points. In contrast, the primary results in the control groups were mainly fibrous tissue repair at both time points. These findings underscored the beneficial role of the Gel-DCM scaffold and highlighted the exceptional potential of hADSCs as a reparative cell preference for cartilage regeneration. There is existing literature suggesting that chondrocytes and stem cells exhibit similar outcomes in articular cartilage repair. 41 However, in our study, hACs demonstrated inferior cartilage repair outcomes compared with hADSCs. We speculate that this variance could potentially be ascribed to the cellular origin used in the investigation. hADSCs were obtained from young donors, whereas hACs were isolated from elderly patients. In comparison with our previous study, 29 where we found the limited efficiency of DCM alone for cartilage repair, our present research is centered on enhancing the performance of the DCM scaffold. By incorporating the photoreactive hydrogel component, our results confirm that the composite materials can provide an appropriate 3D chondrogenic microenvironment and hold great potential for facilitating cartilage regeneration. Upon careful analysis, we did not observe significant animal-to-animal variability in the quality of repair within each experimental group. In addition, we have included histological data from another animal in Supplementary Figure S2 and Supplementary Figure S3.
At present, many porcine organs and tissues have become an important source of xenotransplantation or biomaterials for basic researches and clinical treatments.42,43 ADSCs have been considered as an accessible choice for current stem cell therapy because of their wide distribution, convenient isolation, and strong chondrogenic differentiation potential. 28 Considering materials’ accessibility and practical value, it would be more convenient to establish cell-loaded bioscaffold in clinical applications. Our study may provide feasibility to fulfill the procedure. In clinical practice, hADSCs can be first harvested from patients through abdominal liposuction surgery. Then, hADSCs-loaded hydrogel can be incorporated into the porous DCM to prepare a reparative cartilage construct. The scale of the construct can be tailored by customizing the size and shape of DCM to suit the characteristics of the lesion. In addition, the cell-loaded hybrid scaffold could be conveyed into the cartilage defect areas through arthroscopic surgery with minimal invasion. Despite offering valuable insights, this study must recognize its constraints. One such shortcoming is that the hyaline cartilage of rats is considerably thinner than that of humans, potentially impacting the translatability of the findings to human applications. To address this gap and enhance the clinical relevance of our research, future studies will include in vivo investigations in larger animal models that more closely resemble the anatomical and physiological characteristics of human joints.
Conclusion
In our study, a hybrid scaffold comprising a photoreactive hydrogel and DCM was developed to facilitate chondrogenic differentiation and cartilage regeneration. In vitro experiments demonstrated that the hybrid Gel-DCM scaffold provided a suitable microenvironment for promoting chondrogenesis of hADSCs and maintaining the chondrogenic phenotype of hACs during cultivation. In vivo experiments further revealed that Gel-DCM loaded with hACs or hADSCs effectively promoted advanced cartilage regeneration and effective subchondral bone reconstruction in a rat osteochondral lesion model. Overall, our study indicated that in combination with ACs or ADSCs, the hybrid Gel-DCM scaffold holds great potential for enhancing cartilage regeneration and have strong clinical translation prospects.
Footnotes
Authors’ Contributions
N.D., A.G., and H.Y. conceived and designed the study. J.Z., Z.Y., Y.D., Y.D., and Z.F. performed the experiments and wrote the article. Z.Y.L. and L.F.M. analyzed the experimental data. All coauthors have read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from the Beijing Natural Science Foundation (L234073, J230007), the National Natural Science Foundation of China (NSFC No. 82301751), the Beijing Hospitals Authority Youth Program (code: QML20230119), and the Beijing Tongzhou Health Development Special Project (No. KJ2023CX008).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.