
Abstract
Translational research, which can be explained as the principle of combining advances in both basic research and clinical understanding in a bedside-to-bench-to-bedside approach, has become one of the central themes of present-day medical research. One orthopedic problem that has strongly benefited from such an approach is tissue-engineering-enhanced primary repair of the anterior cruciate ligament. Recent years have shown a clearer definition of the clinical problem and established an underlying mechanistic cause of the incapacity of the anterior cruciate ligament to heal—the premature loss of provisional scaffold in the wound site. These clinical findings were then translated into a research objective, namely, to replace the missing scaffold with a biomaterial with appropriate structural and bio-stimulatory characteristics. Subsequently, a tissue-engineering-based treatment using a collagen–platelet composite was developed and tested in vitro. After proofing the efficacy of this new treatment in the laboratory, it was translated into a potential clinical application, which showed highly successful results in structural integrity and biomechanical capacity in large animal testing. This approach of defining the scientific mechanism underlying a clinical observation and then using that information to design new therapies is but one example of how translational research in tissue engineering can help define and develop new treatments for challenging problems faced by patients.
Introduction

Outlined is the two-way principle of translational research, which aims at the incorporation of basic science and clinical problems into a joint approach.
Translational Research in Orthopedic Surgery
Compared to medicine and other fields of surgery, orthopedic surgery has a relatively modest research base. Further, orthopedic research has been characterized by practical empiricism, prioritizing problem solution over problem origination, for most of its history. It was predominantly during the course of the last 50 years that basic science, basic clinical science as well, was introduced into the field. 1 During this period, however, there was a breathtakingly fast development, leading to outstanding achievements in both science and patient care, but also to a situation that ails many other fields of medical research—a growing divide between orthopedic research and clinical orthopedics. Translational research aims at bridging this gap by creating stronger ties between problems from the bedside and results from the bench. The most intensively researched fields in orthopedics, such as osteoarthritis (OA), osteoporosis, and sports medicine, already exhibit a strong tendency toward translational processes. A strong role of tissue engineering in many of these fields has already demonstrated the value of integrating investigators from different fields, such as clinical physicians, engineers, and experts in life sciences.
A characteristic of surgery in general, but especially of orthopedics, is that one of the most successful strategies in dealing with disease is to replace the diseased organ, rather than addressing the underlying problem. Such an approach is justified if the underlying problem is mechanical in nature or simply wear and tear. However, as our understanding of the pathogenesis of orthopedic diseases has grown, the meaning of other risk factors, such as genetic predisposition, microtrauma, and gender, has become apparent. Yet, there is still much to learn about even the most prevalent problems in orthopedics to advance and optimize the available treatments. Thus, the first task in translational research in orthopedics can often be to translate the problem at the bedside into a research question to be answered at the bench, before aiming at translating basic research findings into potential clinical applications.
The Clinical Problem of ACL Ruptures
The ACL, which protects the knee against abnormal anterior–posterior translation and rotation, is among the most commonly torn ligaments of the knee. Current estimates of the prevalence of reported ACL tears range at 4.8% of ambulatory individuals between 50 and 90 years of age, but it is very likely that the actual number, including asymptomatic tears in patients with low demand, is even higher.2,3 The risk of ACL tears is significantly increased by participating in particular sports, especially those involving pivoting, and for women.4–8 ACL tears are serious injuries causing immediate pain and loss of mobility. They predispose patients for subsequent OA, which in turn causes further pain and immobility and reductions in quality of life and ability to work; 50–90% of untreated patients develop OA within 10–15 years after injury.3,9–11 The current gold standard of treatment is ACL reconstruction using autografts.12–14 However, despite promising short- and intermediate-term outcomes, questions have arisen concerning the long-term efficacy of current ACL treatments to prevent OA.3,7,15–28 Frequently occurring comorbidities such as meniscus tears further increase the risk of OA after ACL replacement, as do concomitant chondral and subchondral damages sustained during the initial trauma.19,21–26,28 Additionally, it has been shown that even after completed ligamentization, which describes the transformation of a graft in to an ACL-like structure after implantation, there are important differences in the ultrastructure,29–31 vascularization,32,33 and innervation34–38 between an ACL graft and a native ACL. These differences may not be critical determinants of the immediate and intermediate clinical outcome, but might contribute to degenerative processes on different levels, suggesting that a repair that retains structure, innervation, and the bone–ligament interface might be more beneficial for long-term knee health than simple replacement. Development of new techniques in ACL treatment may benefit from consideration of these differences.
Translating the Clinical Problem into a Research Objective
The problem at the bedside of a patient suffering from an ACL rupture is the virtually complete incapacity of the ACL to heal. The medial collateral ligament (MCL) of the knee, which is merely inches away from the ACL and often torn in association with it, heals completely and without operative treatment within a few weeks. This observation translates into the following research objective: What is the reason behind the lack of a productive response of the ACL to injury? Initially, it was believed that the missing realignment of the proximal and distal stump, which are continuously pulled apart by mechanical forces during joint motion, would prohibit healing. Thus, early surgical treatments were primary suture repairs to approximate the stumps close enough to allow healing.39,40 However, these endeavors yielded relatively high failure rates, and were soon abandoned.41,42 Subsequently, the first systematic histological studies of the human ACL after rupture characterized four distinct phases consisting of inflammation, epiligamentous repair, regeneration, and remodeling. 43 During these phases, there is a considerable increase in fibroblast proliferation and revascularization, which can be observed to lead to healing in other connective tissues. Comparative analyses clearly showed equivalent patterns of cell proliferation, extracellular matrix production, and cell migration in the healing MCL.44–47
In this histologic study, the observation was made for the first time that for the human ACL, despite bleeding from the ligament ends at the time of injury, there was no fibrin clot spanning the defect between the two torn ligament ends, and thus no protected space for the wound where inflammatory cells could populate and start a functional healing process. One possible reason for the lacking intra-articular clot formation is increased levels of u-PA- and t-PA-activated plasminogen after trauma.48,49 The effect of the premature loss of the provisional fibrin scaffold is a complete block of the inflammatory cascade in the wound site, and loss of the potential for cell migration and subsequent tissue remodeling. The prevention of these events consequently leads to the incapacity of a torn ACL to heal (Fig. 2). The historically high failure rates of primary ACL suture repair can be explained by such a persistent gap between the sutured ends due to the lack of clot formation.39,42,50 This problem has also been shown for rotator cuff repair, which is another intra-articular collagenous structure with a clinical incapacity to heal. 51 In summary, the problem at the bedside was characterized and translated into a research question: How to bridge defects in the ACL or other tissues in the joint in lieu of a fibrin clot?

Histological sections of a central defect in the medial collateral ligament (MCL) and the anterior collateral ligament (ACL) 7 days after wounding in a canine model, stained immunohistochemically for fibroblast-growth factor. Whereas the MCL demonstrates continuous gap fill and strong FGF expression, the ACL defect is completely empty with only a small amount of FGF expression along the wound edges. Color images available online at www.liebertonline.com/ten.
A Potential In Vitro Model
With the mechanism of premature provisional scaffold failure identified, the next step one might consider would be to search for an appropriate substitute to be placed in the wound site. Among all biomaterials currently used in tissue engineering, collagen has a long-standing record as a biocompatible, biodegradable, and safe material for orthopedic applications and is the main constituent of the ACL. 52 Thus, such a biomaterial would be one candidate for a component of a viable alternative scaffold to replace a fibrin clot. Further, collagen can be applied as a hydrogel in and on the defect, thus filling the defect easily and completely. 53 Yet, it is important to note that a fibrin clot that typically serves as a provisional scaffold material is more than a mere scaffold for cellular migration. One of the most important intrinsic properties of such a clot is the release of growth factors and other cytokines that stimulate and regulate the inflammatory process that leads to tissue remodeling and finally defect healing. This fact must be considered in the design of a substitute material. Yet, the addition of the correct combination of cytokines and their orchestrated release in a controlled manner can be complicated. One potential solution to this problem is the use of a platelet-concentrate in connection with a collagen biomaterial. Platelets are activated by collagen and secrete an abundance of cytokines, most importantly growth factors such as PDGF, TGF-β, and VEGF, thus acting as a preprogrammed growth factor delivery system. 54 One study suggested that the mix of cytokines released does not only stimulate cell growth but might also suppress inflammation. 55 These stimulatory effects are also being investigated for potential uses in bone healing,56,57 cartilage, 58 and meniscus repair, 59 as well as treatment of degenerative disc disease.60,61 The orchestrated interaction of a collagen scaffold and a platelet concentrate could be used to enhance primary repair of the ACL, which, in contrast to replacement, would retain the native insertion sites and proprioceptive fibers of the ACL.
Proof of Principle In Vitro
Murray et al. showed that cells from human torn ACL migrate into a scaffold made from bovine atelocollagen (Fig. 3) and secrete smooth muscle actin, which causes wound contraction44,45,62 (Fig. 2). ACL fibroblasts retain this ability also in the ruptured ACL, where they exhibit even higher outgrowth rates. 62 ACL fibroblasts respond to the addition of a platelet concentrate to the biomaterial by increasing proliferation and collagen production rates. 63 Further analyses have shown that this effect is clearly attributable to platelets. 64 The effects on fibroblasts of other blood cells and individual factors in the clotting cascade are still somewhat elusive.65–69
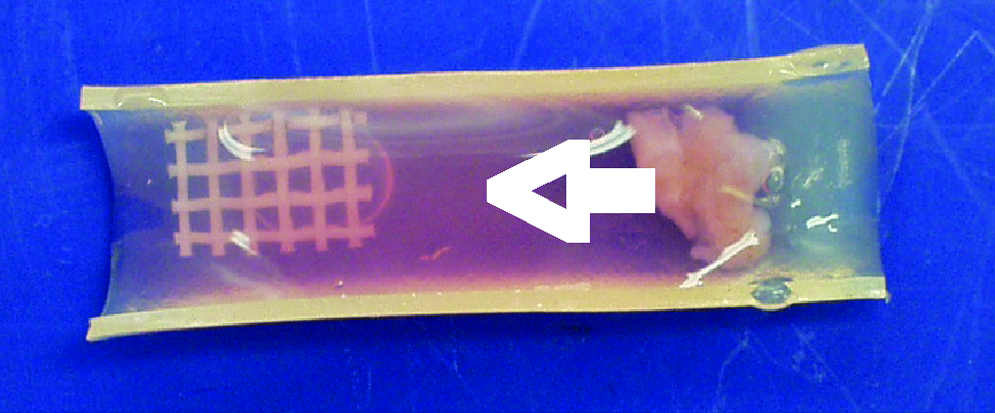
Cells migrate from embedded ACL tissue (far right) into a collagen hydrogel (white arrow). Color images available online at www.liebertonline.com/ten.
Translation into a Potential Clinical Application Tested in an Animal Model
After characterization of the behavior of ACL fibroblasts seeded in a collagen–platelet composite in vitro, an initial animal study was done to assess the behavior of the collagen–platelet composite in a canine model of a stable central ACL defect, compared to no treatment 70 (Fig. 4). This study showed good defect filling and a significant increase in the biomechanical properties of the ACL compared to the untreated group, which showed no improvement over the time course of the experiment. A later study compared treatment of a central defect in the ACL with defects in the MCL and the patellar tendon, which can be considered the natural gold standard of biological ligament and tendon healing. 47 This study confirmed the poor healing capacity of a central ACL defect, but also showed that treatment with a collagen–platelet composite can produce results that are comparable to MCL or patellar tendon healing.
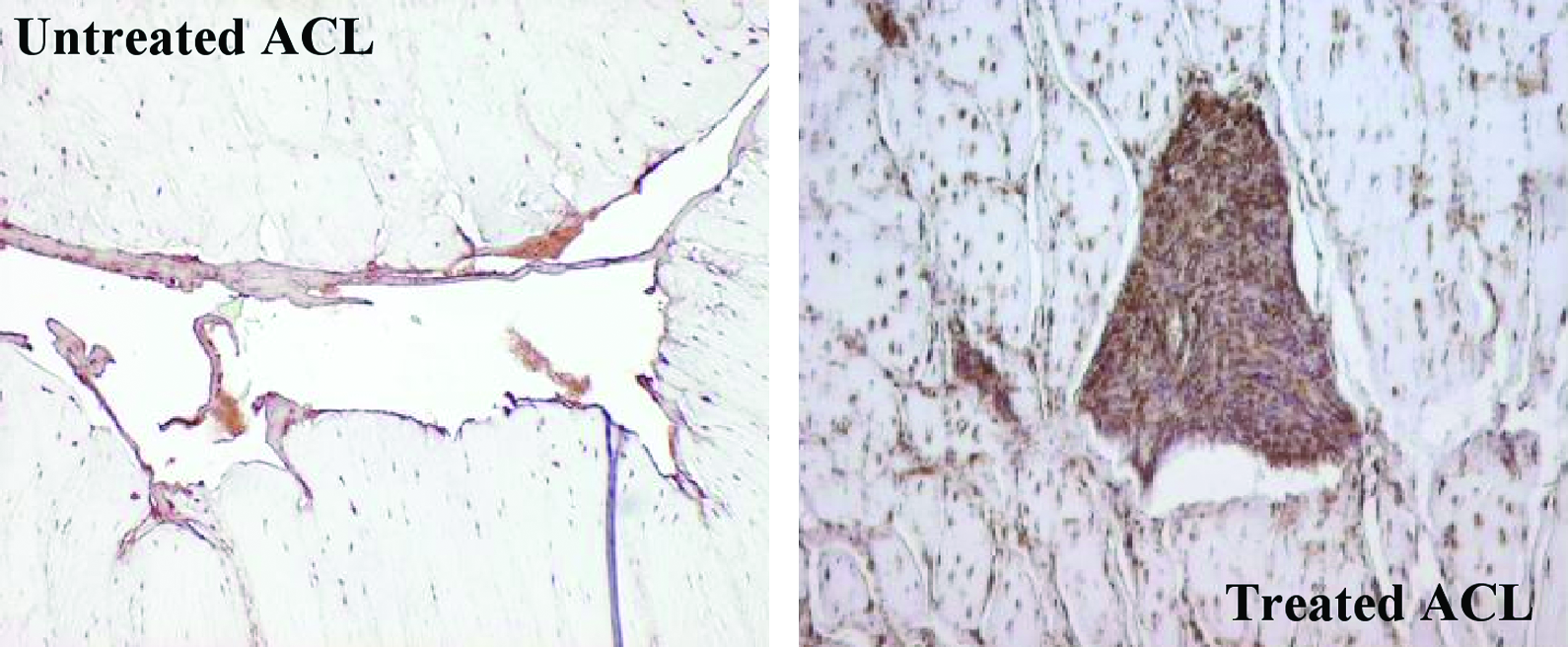
Comparison of central defects of the nonhealing ACL to a central ACL defect treated with a collagen–platelet composite. The treated defect shows complete fill and strong FGF expression. Color images available online at www.liebertonline.com/ten.
These early studies present clear evidence for the effectiveness of a collagen–platelet composite in ACL treatment in general, yet they build their results on central, partial defects while the clinical problem is a complete rupture. Thus, later studies used a complete transection model. Translation of an in vitro model into a potential clinical application requires animal testing. The choice of an appropriate model that mimics the situation in humans as intimately as possible is crucial to obtain valid results.71,72 For studies in ACL repair, a large animal should be used to recreate appropriate biomechanical stresses and to allow for suture repair. Secondly, the response to injury in the model ACL should be equivalent to the human ACL.71,72 Finally, the studied animal should exhibit similar growth rates and skeletal maturation to allow for testing of the effects of age. A porcine model satisfies these criteria. A direct comparison of primary suture repair with and without a collagen–platelet composite to treat complete ACL transections in a porcine model revealed significant increases in stiffness, load at yield, and maximal tensile loads at 4 weeks after the procedure. 73 Additional ongoing work has demonstrated the persistence of improved biomechanical outcomes after 14 weeks of healing as well using the collagen–platelet composite or CPC 74 (Fig. 5), where the use of collagen 75 or platelet-rich plasma 76 alone has shown no significant improvement. Thus, the identification of the missing provisional scaffold was a key observation for this problem of intra-articular healing, and the understanding of the mechanism behind this loss (premature dissolution of fibrin by synovial enzymes) allowed for a more guided design of an appropriate scaffold substitute that preserves the biologic stimulatory function of the fibrin-platelet clot by stabilizing it for intra-articular use by collagen.

Representative histological sections of transected ACL treated with collagen-platelet composite–enhanced primary repair (
Conclusion
A translational research approach helped to identify one potential reason why the torn ACL does not heal: the lack of a fibrin clot that stabilizes the defect and serves as a scaffold for cell migration and a source for stimulating factors. Consequently, the research objective was defined as substituting this clot in its function as both a substrate for cells and a stimulator of healing. A collagen–platelet composite was developed and its effects on ACL fibroblasts were determined and modulated in vitro. The capacity of such a collagen–platelet composite to stimulate healing was tested in a central ACL defect model in canines, compared to untreated defects and defects in the MCL, which can be considered a gold standard in intrinsic ligament healing. These analyses revealed strong evidence for the effectiveness of such a treatment. Subsequently, a pig model of a complete ACL tear was developed to test the ability of the collagen–platelet composite to enhance primary suture repair. This model showed that addition of the composite, but not of its individual constituents, results in significant improvements in functional outcome of the healing ACL.
Footnotes
Disclosure Statement
Martha M. Murray is a founder and stockholder in Connective Orthopaedics. Patrick Vavken is a consultant for Connective Orthopaedics. Both authors certify that they have no other commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with this article.