
Abstract
Tissue engineered bone grafts have the potential to be used to treat large bone defects due to congenital abnormalities, cancer resections, or traumatic incidents. Recent studies have shown that perfusion bioreactors can be used to generate grafts of clinically relevant sizes and shapes. Despite these scientific and technological successes, there is uncertainty regarding the translational utility of bioreactor-based approaches due to the perceived high costs associated with these procedures. In fact, experiences over the past two decades have demonstrated that the widespread application of cell-based therapies is heavily dependent on the commercial viability. In this article, we directly address the question of whether bioreactors used to create bone grafts have the potential to be implemented in clinical approaches to bone repair and regeneration. We provide a brief review of tissue engineering approaches to bone repair, clinical trials that have employed cell-based methods, and advances in bioreactor technologies over the past two decades. These analyses are combined to provide a perspective on what is missing from the scientific literature that would enable an objective baseline for weighing the benefit of extended in vitro cultivation of cells into functional bone grafts against the cost of additional cultivation. In our estimation, the cost of bioreactor-based bone grafts may range from $10,000 to $15,000, placing it within the range of other widely used cell-based therapies. Therefore, in situations where a clear advantage can be established for engineered grafts comprising patient-specific, autologous cells, engineered bone grafts may be a clinically feasible option.
Introduction
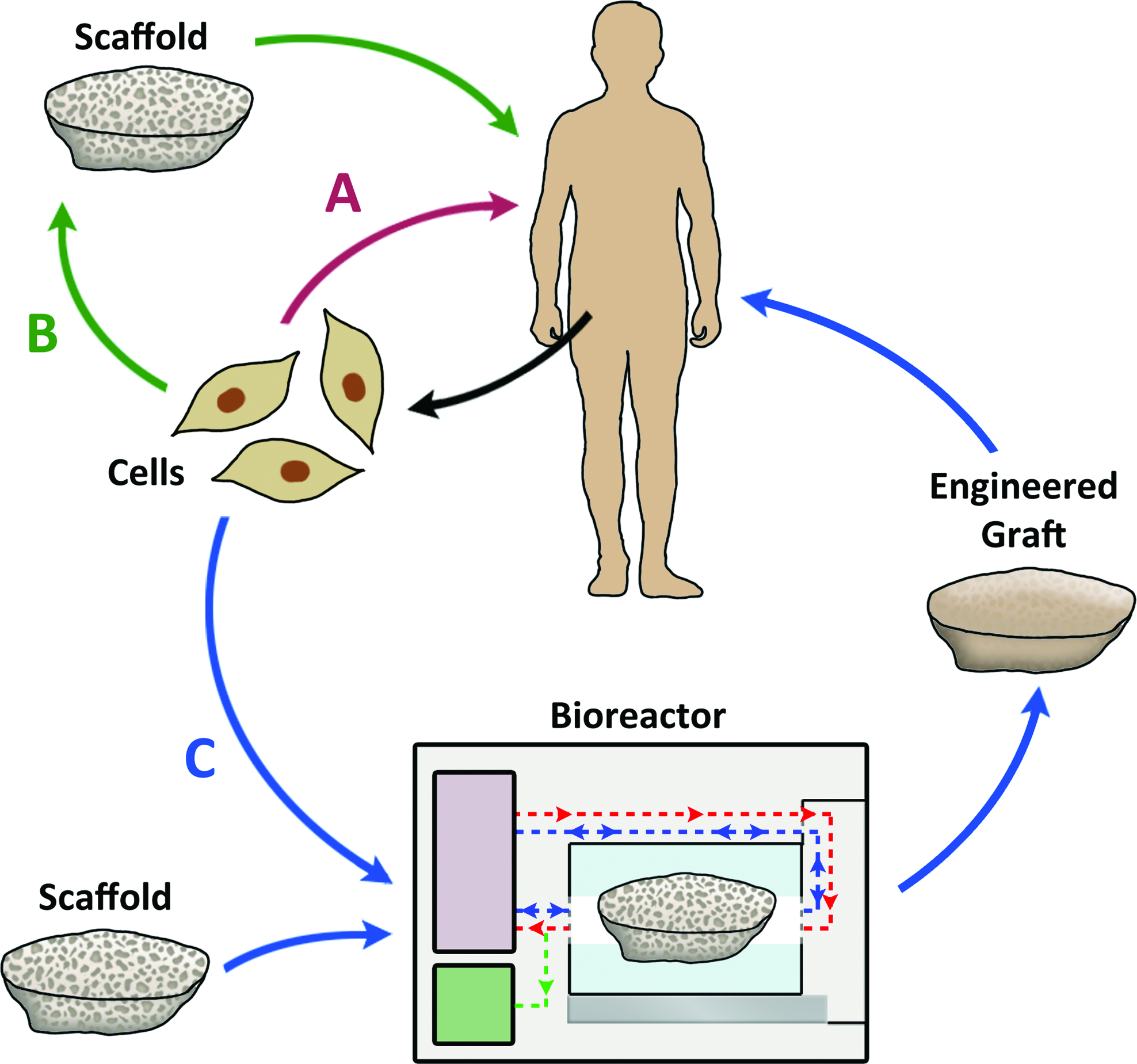
Cell-based therapy options for bone regeneration. Current technologies and small-scale clinical trials have utilized either direct injection of autologous cells
The cultivation of osteoblasts in three-dimensional scaffolds was first reported circa 1990.2–6 These early experiments were conducted in traditional culture dishes using “static” medium conditions. Static cultures are insufficient for growing cells in large constructs of clinically relevant sizes (centimeters) as the limited diffusion of oxygen and nutrients will support cell viability only through a depth of several hundred micrometers.7,8 This problem has been reconciled through the use of perfusion bioreactors, which provide convective mass transport of oxygen and metabolites to cells and facilitate the uniform development of tissue throughout the constructs.9,10 In addition to greatly enhancing mass transport, perfusion also introduces shear stress stimulation, which enhances osteogenic differentiation and calcium deposition by bone marrow-derived mesenchymal stem cells (MSCs).10,11 As a result, bioreactors have been readily adopted by the bone tissue engineering field as an enabling technology, capable of playing a crucial role in translating engineered bone grafts into clinically applicable products.
In spite of the in vitro successes, there still remains a disconnect between the technological advances in bioreactor development and their clinical use. Why does this disconnect exist and what can we do to bridge this gap? The majority of concerns regard cost, time, and ease of application. How practical is it to apply bioreactor-grown grafts in the clinic? Current methods rely heavily on careful manual techniques, which are subject to operator-dependent variability, and make regulatory approval exceedingly difficult to obtain. The use of advanced technology would also require training of specialized technicians to monitor graft cultivation. Thus, despite its potential scientific utility, many investigators appear to be moving away from this approach to more “practical” alternatives such as growth factor or gene delivery. The future of bone tissue engineering bioreactors as more than a scientific tool has therefore been called into question. In this review, we examine the potential for translating this bioreactor-based approach to clinical scenarios and discuss key points to be addressed if we are to overcome the scientific, regulatory, and commercial barriers that have crippled previous cell-based therapeutic approaches and have so far prevented tissue-engineered bone grafts from reaching the clinic.
Bioengineering Approaches—A Case for Cell-Based Therapies
The term “bone tissue engineering” used in its most general form may involve either cell-free approaches, cell-based approaches, or combinations of both. 12 The cell-free approach consists of scaffolds or bone graft substitutes, which incorporate osteoconductive or osteoinductive attributes based on the scaffold's physical and chemical properties, added growth factors, or DNA oligomers for transfection. The cell-based approach consists of the use of either autologous or allogeneic cells capable of forming bone tissue with or without the use of scaffolds. The performance of these cells for bone regeneration may be further enhanced by genetic modifications.
Scaffolds
Advances in biomaterials and nanotechnology have revolutionized the field of tissue engineering by providing scaffolds of desired physical, chemical, mechanical, and biodegradable characteristics. Among the scaffolds made from natural polymers, collagen, hyaluronic acid, alginate, and chitosan are the most commonly used.13,14 Though natural polymers have desirable biodegradability, they lack the proper mechanical properties for bone engineering. The mechanical qualities of natural polymers can be enhanced by blending them with Food and Drug Administration (FDA)-approved synthetic polymers such as polycaprolactone (PCL), polylactic acid (PLA), polyglycolic acid (PGA), poly(lactic-co-glycolic) acid (PLGA), or ceramics such as hydroxyapatite and β- tricalcium phosphate (β-TCP).15,16 Another class of scaffolds that has been extensively studied and found to be promising for bone tissue engineering applications is synthetic bioactive glasses and demineralized bone matrix.17,18 The choices are many, each material has specific advantages and disadvantages, and the use of hybrid materials to minimize the disadvantages is an area of intensive research.
Bioactive growth factors
These enhance cell growth and differentiation, motility, and formation of new tissues. Key osteoinductive cytokines include bone morphogenic proteins (BMPs) 19 and vascular endothelial growth factor (VEGF). 20 Among the BMPs, BMP2 and BMP7 have been approved for clinical use for the treatment of nonunion fractures and spinal fusion.21,22 Certain protein mixtures derived from biological source such as blood or tissue, e.g., platelet-rich plasma (PRP), have also been found to be useful for bone tissue engineering. 23 These agents can be injected directly into bone defect regions or formulated with natural or synthetic polymers for controlled time release. Because of their short half-lives in vivo, high initial dosages are required, which in turn can lead to nonspecific effects of the growth factors outside of the target area. Moreover, the cost associated with the production of recombinant proteins is very high. Thus gene therapy has been proposed as an alternative to ensure stable and consistent production of osteoinductive proteins at the injury site. 24
Gene Therapy
Introducing osteogenic genes to cells in order to upregulate the expression of bone specific proteins can enhance cell differentiation and new bone growth. The gene delivery vector can be carried in a scaffold to induce the local host cells (in vivo gene therapy) or cells can be genetically modified in vitro and then used for transplantation (ex vivo gene therapy). 25 Nonviral gene delivery vectors are relatively safe and cost effective. However, induced gene expression is transient and transfection efficiency is low in comparison with viral gene delivery. 26 Viral delivery of genes encoding BMPs 2, 4, 6, and 7 has been evaluated for several bone defects in animal models.27–29 Though the in vivo gene delivery method appears promising, there is some associated difficulty in targeting specific cells and innate risk of inducing immune responses to the viral vector. For this reason, ex vivo gene therapy can be used as an alternative, in which the cells are isolated from the host and genetically modified under controlled in vitro cultures and then transplanted to the injury site using a cell delivery vehicle. Promising results have been observed using ex vivo gene therapy in several animal model studies.30,31 However, the effort and time involved in isolation, ex vivo culture, transfection, and then transplantation to the injury site make this therapy expensive. Currently bone regeneration using gene therapy is not in clinical use; however, active research is in progress.
Cell-based therapy
Cell-based therapy depends entirely upon the activity of cells to accomplish the regenerative process. Several basic considerations have to be taken into account when selecting the cell source for bone tissue engineering. Considering the immunogenic response, an autologous cell source is preferred over an allogeneic source; several autologous cell sources have already been evaluated extensively based upon ease of availability, expansion capacity, and functional regeneration. 32 Though cell therapy based upon the injection of cell suspensions is simple to perform, there is low localization of the cells in defect regions due to the possibility of multiple homing sites in vivo. 33 A combination of encapsulating the cells in a scaffold and providing the necessary growth factors and microenvironment during ex vivo cultures is useful to fully optimize the cells' regenerative capabilities. 34
Clinical Applications of Cell-Based Approaches to Treating Bone Defects
The gold standard for autologous bone repair remains the vascularized autograft. However, in cases where this approach is not feasible, notably in patients with donor site morbidities such as infections, pain, and hematomas, allograft methods have been pursued. Fresh allografts, however, have associated risks of disease transmission, such as HIV, hepatitis B, and hepatitis C. Stem cell-based approaches, where the patient's own cells are harvested and used to enhance bone regeneration, have been seen as a viable alternative. Clinical trials have largely been divided into procedures that utilize scaffolds in addition to cells and those that are solely cell based. This division is largely dictated by the size of the bone repair that is needed. Larger defects typically require a scaffold to primarily fill the void as well as provide mechanical strength and cellular containment. Smaller defects such as nonunions are oftentimes treated with cell suspensions, as there is less of a need for a load-bearing scaffold. Several of these cases have been reported and extensively reviewed in the literature. 35 These approaches and outcomes are summarized in Table 1.
BM, bone marrow; RCT, randomized control trial; CT, computed tomography.
Although there has not been an abundance of clinical trials of cell-based treatments, there has been promising preliminary data to suggest progress in the field. For example, the applications of bone marrow (BM) cells to promote bone unionization were shown by Connolly et al. in a seminal study. 36 In this study, 20 cases of tibial nonunions were treated with BM aspirate infusion. Of these, half exhibited complete union with intramedullary nailing and 8 out of the remaining 10 demonstrated unionization with cast immobilization. 36 Subsequent BM studies optimized the conditions needed for adequate bone repair. Repeated injections of BM aspirate and increased cell concentrations were both demonstrated in separate studies to improve bone unionization.37–39 With the knowledge that more cells could result in better outcomes, subsequent studies proposed expanding the BM aspirate ex vivo and differentiating the cells in osteogenic medium before implantation. 40 This procedure of ex vivo expansion of the BM aspirate quickly became the preferred method of increasing the numbers of osteogenic cells since they are very limited in quantity in BM aspirate. The ability to osteogenically differentiate the BM cells before implantation also resulted in shorter healing time of 30.0±6.72 days/cm of defect in comparison to 51.4±26.5 days/cm in no cell therapy at all. 40
In an effort to standardize preliminary findings, there have been a few randomized, controlled trials using BM cells to improve bone defect outcomes. In 2008, Wright et al. performed a study in which they randomized patients to either BM injections or methylprednisolone therapy in the treatment of bone cysts. Although there was healing with cell therapy, it was demonstrated that the standard of care, methylprednisolone, had a greater impact on patient outcomes. 41 However, several more recent studies have contradicted these results, showing that there is tremendous significance in the details of the methods utilized for cell treatment. Increased cell number, repeat injection of BM aspirate into the site of injury, and ex vivo expansion and differentiation can all increase the capacity of bone marrow cells to repair a defect.37–40 To ensure the success of cell implantation and minimize the amount of marrow that must be taken from the patient, ex vivo expansion and differentiation should be pursued as an attractive option.
To treat larger bone defects, cells have been combined with biocompatible scaffolds to improve form and function. The scaffold provides cellular containment, enhancing delivery of cells to the affected site, and immediate mechanical stability while the BM aspirate facilitates bone healing and remodeling. One of the first studies to combine the two to treat defects in humans was in 2001 by Quarto et al., who used macroporous hydroxyapatite scaffolds seeded with ex vivo expanded BM cells. 42 Many studies, following this model in which hydroxyapatite was used as a cell scaffold, have demonstrated appropriate healing.42–44 In addition, various scaffold materials, including type I collagen and beta-tricalcium phosphate, have been used with mixed results.45–47 Unfortunately, extensive in vivo studies have not been done to directly compare effects of scaffold materials on bone healing properties. The natural progression in BM/scaffold combinations was to include a substance to maintain cells within the scaffold. This was first accomplished by Dallari et al., who performed a prospective, randomized study that incorporated platelet gel into lyophilized bone chips. The addition of cell containment by gel strongly increased the bone healing and revascularization. 45 Despite its success, gel applications have not been widely employed for cell delivery in cell/scaffold-based therapies.
To date, cell-seeded scaffolds have been used in clinical treatments without any precultivation to stimulate the organization of cells into immature tissues. It remains largely unknown whether in vitro cultivation—used to convert cell-seeded constructs into engineered bone grafts—would provide enhanced outcomes. Prior results from small animal studies suggest that cultured bone grafts lead to improved healing of critical sized segmental defects. Meinel et al. demonstrated that BM cell seeded silk scaffolds that were grown in a bioreactor for 5 weeks before implantation exhibited more bone formation as seen by histology and radiology than cells alone or scaffolds that were seeded just prior to implantation. 48 These results imply that engineered bone grafts may be particularly suitable for treating critical size defects. This is especially relevant in cases where a static structural support is insufficient such as congenital defects where the graft needs to grow in tandem with a developing child. To determine whether the additional benefit of growing bone constructs outweighs the costs, head-to-head comparisons where the long-term outcomes are assessed are needed in large animal models. These evaluations are missing from the clinical literature. Postoperative radiological studies are not necessarily indicative of functionality. Other factors such as fracture reoccurrence and better measures of clinical utility need to be considered to ensure functional, regenerative success. Also, a better understanding of the role that implanted cells play in the healing process is necessary to confirm that the cell-mediated therapy benefits are in fact due to the cellular component on the implant.
Additionally, as with all clinical approaches to tissue engineering, it is of the utmost importance to consider the stem cell source as well as possible donor site morbidity. Ideally, the cell source would have the characteristics of easy accessibility, ability to harvest large cell numbers, and an osteogenic differentiation potential. While BM cells have been the choice source because of their osteogenic capacity, there are still complications in their available access and ability to yield high cell counts. Other adult stem cell sources, such as adipose-derived adult stem cells (ASC), have been suggested as potential primary cell types. ASCs have the advantage of being easily accessible to a large quantity of cells while still maintaining osteogenic potential. 49 Simple subcutaneous liposuction can yield approximately 375,000 cells/mL of lipoaspirate after only 4 days of culture. 43 Other possible BM stem cell harvesting techniques, such as the reamer-irrigator-aspirator (RIA), have been proposed as prospective methods to harvest large number of BM stem cells with the added benefit of never having to leave the OR. 50 RIA also provides a method of obtaining BM stem cells in a putty-like form, which can then be molded to fit the bone defect. These differing cell sources and techniques of harvest are necessary to consider when approaching clinical applications in tissue engineering as each method has its own benefits and complications.
Apart from considerations of cell source and harvesting methods, it is also important to evaluate the physiological state of the site of implantation as the development and integration of an engineered bone graft postimplantation rely on key osteoconductive conditions. The objective of regenerative medicine is to not only replace bone deficits but also have the graft completely integrate into the recipient patient. To this end, fostering an osteoinductive environment both locally and systemically is crucial. For instance, Zhang et al. have explored manipulating bone endocrinology to facilitate regeneration through the application of parathyroid hormone in addition to calcium and vitamin D.51,52 These osteogenic factors ensure that there is ample active calcium for bone repair and integration. Other groups have utilized compounds such as bisphosphonates to inhibit osteoclast activity and prevent bone resorption, shifting the balance to positive bone formation.53,54 Based on this concept of creating the ideal environment to facilitate the integration of implanted bone constructs, other groups have pioneered the endogenous tissue engineering approach. Enabled by the idea that the body is the most capable and efficient tissue engineer, it is logical to attempt to harness the body's innate capacity for repair. This approach utilizes osteoinductive proteins or biological agents to stimulate bone repair. The emergence of BMP supplementation to bone grafts is an apt example of employing osteogenic agents to manipulate the body's own regenerative processes. 55 Additionally, others have experimented with modulating genetic components, such as Lrp5, to regulate bone mass, to achieve better bone repair. 56 However, regardless of the cell origin or harvesting techniques used, it is this optimization of systemic osteoconductive conditions that will ultimately determine the regenerative success of engineered bone grafts.
Bone Bioreactors—Growing Functional Bone Grafts in Vitro
Various types of convection-based bioreactors have been developed to aid in the cultivation of large, three-dimensional grafts. Goldstein et al. 57 compared three such systems: the spinner flask, 58 the rotating wall vessel, 59 and the perfusion bioreactor, 60 to determine the relative effectiveness of each. PLGA foam scaffolds were seeded with rat marrow cells and cultured in the three systems for up to 2 weeks. Scaffolds cultured under traditional static conditions were used as controls. At 7 days, the perfusion system yielded the most uniform cell density throughout the construct, whereas the other systems showed preferential cell density at the construct boundaries as would be expected for systems in which mass transport into the construct center was insufficient for cell viability. By 14 days, only the perfusion system had statistically significant levels of alkaline phosphatase (ALP) expression. Together, these results demonstrated that only the perfusion system could adequately support uniform bone differentiation throughout the construct. 57
Medium perfusion also imparts shear-stress to the cells. Biophysical forces, such as shear, have been strongly implicated in regulating osteocyte function in vivo, and perfusion bioreactors provide a means for mimicking physiological loads to 3D cultures of osteogenic cells. 61 In 2002, Bancroft et al. seeded rat marrow cells throughout a titanium mesh scaffold and showed that matrix and mineral deposition increased throughout the scaffold as a function of medium perfusion rate. 61 It was unclear, however, whether this improvement resulted from enhanced nutrient transport or the increased biophysical stimulation of cells. The same group was able to use their perfusion system and decouple the effects of shear from that of mass transport by increasing medium viscosity while maintaining the same flow rate, demonstrating that the shear applied to cells was a major factor contributing to de novo bone growth. 62 Further studies have investigated specific parameters of the flow through tissue engineering constructs to achieve optimal bone formation, such as the effect of oscillatory flow or of flow velocity.10,63 These studies established the ability of the perfusion bioreactor to accommodate tissue engineering constructs of clinically relevant sizes. Our group utilized this approach while also incorporating grafts with anatomically shaped geometry. 64 Using a computed tomography (CT) image and computer software to extract the 3D anatomical shape of the temporomandibular joint condyle, it was possible to generate trabecular bone scaffolds in the exact geometry of the condyle. The scaffold, now clinically relevant in both size and shape, was seeded with bone marrow-derived mesenchymal stem cells and cultured in perfusion bioreactors for up to 5 weeks. Again, perfused constructs exhibited significantly enhanced matrix formation and mineral deposition relative to constructs grown in static conditions. 64 Fluid flow through these constructs was modeled and correlated with patterns of tissue growth and matrix deposition. 64 This represents a critical proof-of-concept that the perfusion bioreactor technology can indeed engineer clinically relevant tissues. While a detailed review on the effects of shear stress and bioreactor culture on cell growth in tissue engineered bone grafts is not the focus of this review, two recent reviews cover these topics in depth.65,66
Despite such advances, the perfusion bioreactor has not been employed for clinical use. Several reviews of the challenges facing this technology and preventing its widespread use have been published.67–69
A critical requirement of a translational bioreactor is the minimization of operator dependency, since this may result in inconsistency and a lack of quality control between grafts. To facilitate bioreactor use in clinical settings, the user interface must be restricted to nontechnical considerations (e.g., cell injection, medium changes, and sampling), as these would enable traditional hospital staff to operate the system effectively (Fig. 2). It is clear that any such system would need to be equipped with the following basic features:
1. Automation. Unlike other engineering disciplines in which physical and chemical interactions may be accurately predicted, accounting for biological complexity and donor-to-donor variations in cellular responses introduce challenges for engineering grafts with precise, reproducible qualities. This problem is exacerbated when the quality of the product is heavily dependent on the individual skill and technique of the operator. Automation of cultivation procedures such as cell seeding reduces variability between manual operators, allows for processes to be scaled up to reduce cost, and can limit the potential for contamination of cultures through repeated manual operations. In particular, the ability to grow grafts in duplicate or triplicate for a single application, and a means to select the “best” graft, may increase the chances for successful clinical outcomes. This approach is practical however, only in automated procedures enabling process scale-up and the simultaneous cultivation of multiple grafts. Furthermore, enhanced quality control is an essential prerequisite for regulatory approval. Advanced technology has already facilitated automation of a number of clinical processes, for instance, algorithms for precise, image-guided needle placement by surgical robots (termed visual serving) allow for reproducibility in minimally invasive surgeries.
70
Such technology automates the traditional manual alignment process surgeons would otherwise undertake prior to needle insertion. Given our current capabilities to model the effects of perfusion rate and medium flow patterns on tissue development,
64
feedback control might be used to modulate inlet and outlet flows in perfusion systems. Likewise, the same principles of automating processes via user-programmed spatial and temporal parameters can also be applied to various aspects of bioreactor culture, allowing for minimization of operator-dependent effects on the final graft. To achieve this, however, further studies are needed in the development of relevant quantitative biomarkers. 2. Uniform cell seeding. The creation of any large graft requires uniform cell seeding that results in homogeneously distributed and viable cells. Bioreactors have long been employed to this end. In one of the earliest studies employing spinner flask bioreactors for cell seeding, Vunjak-Novakovic et al. demonstrated uniform cell seeding of poly[glycolic acid] scaffolds up to 10 mm in diameter and 5 mm in height.
58
Since then, various bioreactor designs have been developed to seed scaffolds. Griffon et al. conducted a study comparing four different types of bioreactors—the spinner flask, the perfusion system with a vacuum chamber, an orbital shaker with a vacuum chamber, and an orbital chamber alone.
71
This study revealed that seeding with a perfusion/vacuum system resulted in ∼95% cell attachment within the first 2 h and constant cell retention up to 48 h later. In another study, the tissue culture under perfusion (T-CUP) system was developed to simplify the complicated set-up required for most perfusion bioreactors.
72
In this design, the scaffolds were moved up and down through a “stationary” cell suspension. Using this approach, they were successfully able to seed various cell types at high efficiency (>75%) and viability (>95%) in a variety of scaffolds. These studies further demonstrated the feasibility of utilizing perfusion bioreactor system not only in providing mass transport and mechanical stimuli, but also in effecting homogeneous cell seeding. This is an essential component of a translatable bioreactor system. 3. Checkpoint markers and feedback control. Relevant biomarkers are needed to serve as checkpoints throughout tissue development, allowing engineers to track the developmental progress of each graft. Yet, to date, no rigorous correlations have been established between specific biomolecules and particular stages of bone development or construct mineralization. Investigation into bone cytokines has pointed to interleukin (IL)-11 as a possible candidate biomarker. IL-11 is secreted by developing osteoblasts and is crucial for bone remodeling, meaning it would be present throughout a developing bone graft.
73
Since IL-11 is a soluble factor, it can be detected noninvasively with a tagged antibody in the media, or by incorporating available quantification technologies (such as ELISA). However, further developmental biology-based research is needed to identify other tissue-specific biomarkers as well as “normal” expression levels and kinetic changes of these soluble markers associated with adequate new bone formation and mineralization. The acquisition of these types of data would enable the application of automated feedback control loops into the bioreactor design as variations from normal expression levels may indicate the need for changes in frequency of medium changes, perfusion rates, or other cultivation parameters. Soluble molecules are not the only potential biomarkers. With further research, it may be possible to use imaging modalities to provide relevant biomarkers of tissue development. 4. Imaging compatibility. Noninvasive imaging can provide useful information for correlating with biochemical markers. It is therefore crucial that the bioreactor design be compatible with specific imaging modalities so that the graft could be monitored during development. An imaging-compatible bioreactor would enable longitudinal evaluation of tissue growth without compromising graft sterility. Imaging compatible bioreactors have been designed by a number of groups to accommodate a variety of imaging modalities, including micro-CT,74,75 confocal microscopy,
76
magnetic resonance imaging (MRI),
77
nuclear magnetic resonance (NMR),
78
optical coherence tomography,79,80 and Doppler optical coherence tomography.81,82 In the case of bone grafts three imaging modalities may prove most beneficial: micro-computed tomography (micro-CT), cone-beam CT (CBCT), and optical coherence tomography (OCT). There are relative advantages and disadvantages of each technique as well as potential limitations to its use in a clinically relevant bioreactor. a. Micro-CT is a relatively cheap and high-resolution imaging modality that has been used effectively to examine small animals and bony scaffolds on a scale of 1–50 μm.83–87
The duration of a micro-CT scan varies according to resolution, but can be as little as 30 min.
83
Micro-CT compatible bioreactors have already been developed by several groups.74,75 Hagenmüller et al. designed a micro-CT-compatible bioreactor for the purpose of monitoring the osteogenic progress of cells in scaffold culture.
75
In this system, scaffolds can be housed in bioreactor cartridges made of polysulfone, a material with low radio opacity, which allowed the scaffolds to be scanned via micro-CT without removal from the sterile cartridge housing. The cartridges could also be placed into a mechanical stimulation unit (MSU) to provide loading stimulation. Hagenmüller et al. found that this system allowed for the acquisition of high-quality CT images of a bone biopsy sample placed in the cartridge that were comparable to images obtained when the sample was housed in a scanning vial. There is no currently published data on the use of this system to monitor mineral deposition over time; however, the cartridge approach and the ability to add a mechanical stimulation component make this a potentially valuable system for the growth and monitoring of bone scaffolds. Another group was able to examine the amount and rate of mineralization of bone constructs cultured under perfusion by modifying the construct chamber geometry to accommodate a standard micro-CT scanner.
76
The reactor was sized such that it would fit into the scanner and the wall thickness was reduced to match standard micro-CT chambers, demonstrating again that designing an imaging-compatible bioreactor is technically feasible. Such baseline studies may establish “normal” parameters, such as mineralization rate, that a graft should meet throughout culture. The study also validated the efficacy of the approach by scanning twice versus once within a 5-week period and evaluating cell viability and mineral deposition. They demonstrated that scanning multiple times did not negatively affect the graft in the short term. However, given that the main concern with micro-CT is the high radiation dose, it may be necessary to establish the long-term effects of micro-CT scanning on cultured constructs. b. An alternative is cone-beam CT (CBCT), which allows for image acquisition using a single rotation, resulting in lower radiation (0.1–1 cGy vs. 10–100 cGy for micro-CT)88–91
and faster scan times (on the order of 1–3 minutes).92–94
This makes CBCT a potentially superior choice to micro-CT for scaffold imaging as it is more amenable to multiple, longitudinal scans to provide insight into tissue development. The resolution of cone-beam CT, however, is considerably lower than that of micro-CT, making it significantly less quantitative.
92
In their study comparing CBCT to micro-CT, Loubele et al. reported micro-CT delivers, on average, a 20 times more effective radiation dose than does CBCT,
92
and has the advantage of achieving much higher resolution (as low as 1 μm as opposed to 100–500 μm for CBCT).92–94
A CBCT-compatible bioreactor has requirements and considerations similar to the one used for micro-CT
76
: modified chamber dimensions to allow for imaging without removing the scaffold and housing material that would not interfere with scans. c. Another possibility for imaging is optical coherence tomography (OCT), which is a light-based technique and therefore delivers no radiation. It can achieve 1-μm resolution imaging up to a depth of around 2 mm.
95
OCT or Doppler OCT has already been utilized in several perfusion bioreactor setups to monitor tissue growth or flow.80–82
For example, Bagnaninchi et al. used an OCT-compatible perfusion bioreactor to assess cell seeding/growth and ECM deposition in microchannels of a porous chitosan scaffold seeded with porcine tenocytes.
80
In this case, the scaffold had a small enough diameter to allow OCT imaging through the clear sample chamber. Beyond the 2-mm penetration limit, as would be the case with larger grafts, OCT imaging may utilize a needle in order to provide increased penetration.
96
OCT scanning using needles could quite conceivably be interfaced using these perfusion needles without much need for altered bioreactor design. However, as is the case with soluble biomarkers, considerable research is required in order to correlate data derived from this modality with quantitative measures of bone growth and tissue maturity. 5. Ease of use. Much like MRI scanners and other high-tech clinical tools, it is essential to design a bioreactor that provides sophisticated technology, while remaining intuitive and simple to operate. Operators in the clinic, such as nurses or technicians, would need minimal training to use the bioreactor. An easy-to-use device also reduces operator dependency, as no specialized skill is required for operation.

Clinical bioreactor for bone tissue engineering. The principal underlying consideration is that the system should have a simple user-interface. The automated bioreactor will have three user inputs. A porous, prefabricated scaffold is encased within a sterile disposable cartridge. The cartridge is internally molded to anchor the custom-shaped scaffold and guide perfusion flow evenly through the scaffold. Once placed within the bioreactor, input and output perfusion ports will pierce the sides of the cartridge. Cells isolated from the patient are injected directly into a chamber of the bioreactor pump. The cells are seeded in the scaffold via oscillatory, bidirectional perfusion (blue line), followed by a short period of static culture to allow cell attachment. A culture medium cartridge is connected to the perfusion pump, which circulates medium through the scaffold cartridge (red line). An automated sampler (green) will periodically take samples of the culture medium to assess sterility, pH, oxygen tension, etc. This information will be processed by an external feedback controller that can adjust the cultivation parameters as necessary and send alerts to the operator via a graphic user interface. Once the predetermined cultivation period is complete, the engineered graft can be transported in its original cartridge to the operating room. Color images available online at www.liebertonline.com/teb
Estimated Cost of Bone Grafts
Even accounting for these scientific and practical considerations, the biggest challenge in translating bioreactor-based approaches to the clinical applications arises from financial considerations. The feasibility of bioreactor technology for medical use depends greatly on whether the cost of implementing such technology would outweigh the benefits. The prospective cost should also be compared to the costs of currently available or developing cellular/scaffold technologies. In addition, for bioreactors to become a useful clinical technology we must identify and address the economic bottlenecks in bioreactor design and use. We have compared the major cost factors, scale-up considerations, and potential economic bottlenecks of TE-based technologies for orthopedic applications (Table 2). We also compare, when available, the cost of commercial products in these categories. In the case of cell treatments, the table is also broken down according to how the cells are prepared for the procedure, i.e., traditional flask culture, bioreactor culture, or no in vitro cultivation. Each of these options has their own economic considerations that will cause differences in costs.
BMP-2, bone morphogenetic protein; PLGA, poly(lactic-co-glycolic) acid; MSCs, mesenchymal stem cells; BR, bioreactors; MTF, Musculoskeletal Transplant Foundation.
Currently, the cost of using a tissue engineering (TE) scaffold can only be roughly estimated due to the progressive nature of large graft bioreactor technology. However, through careful evaluation of costs associated with bioreactor systems, cell supply, and current technologies (see Table 2), we project a cost estimate for bioreactor-grown bone grafts. The one-time cost for designing and building a bioreactor system that meets GMP standards and incorporates both biomarker monitoring and cell culture can be estimated to be between $25,000 and 35,000.97–102 The eventual cost of a graft, however, takes into account the fact that a bioreactor will be used multiple times and, as such, bioreactor costs are amortized over many grafts. For this analysis we have split the cost of the bioreactor over 10 grafts as a conservative estimate, giving a base cost of $2500–3500 per bioreactor use. Cell costs range from $500 to 1500 depending on the number of cells needed and the source (allogeneic or autologous). In our analysis, we have set the cost for cells and media per graft at $2000. Labor costs for a clinic-based system could be drastically reduced by having an on-site bioreactor with a simple user-interface that can be run by hospital nurses or technicians and by automating much of the procedure. For example, media changes, biomarker sampling/testing, and media condition monitoring (pH, O2/CO2 content) can all be automated. The cost of biomarker testing can be estimated by looking at the current market costs of biomarker ELISA kits. If we look at the cost of testing for a bone formation biomarker such as IL-11, a 96-well plate ELISA generally costs $400–500103–105 for biochemical analysis. Another cost factor that can be included is the price of imaging the construct. One proposed imaging method is CBCT, which costs an average of $200–600 per scan,106,107 while the machine itself plus installation and personnel training costs about $150,000. 108 Because CBCT can be used for many other purposes involving craniofacial diagnostics or surgery planning, 109 and does not need to be a bioreactor-specific purchase, we have only included the cost of individual scans (averaged at $400) in the bioreactor cost estimate. Assuming the graft can be imaged and assayed for biochemical markers at weekly intervals, we can incorporate these factors by multiplying the cost per assessment by weeks cultured (in this analysis we assume a highly conservative estimate of 4–8 weeks of culture). If we take into account the per-graft costs (assays, imaging, cells, and media), we come to an estimate of about $4000–$6000. The rest of the graft cost will come from the bioreactor and labor. An additional $5000 is included to cover labor costs and other factors that have not explicitly been included in the estimate, such as the cost of occasional graft failure to grow or contamination. Taking all of this into account, we project that the most conservative estimate for a bioengineered graft would likely fall into the range of $10,000–15,000. We can compare this range against current technologies to see if it is an appropriate estimate. With many of the other factors being the same, we reason that the estimated cost of the engineered bone graft should fall below that of similar cell-based procedures that utilize centralized, off-site facilities. However, a bioengineered graft would be more expensive than simply using a donor bone graft or a suspension of bone marrow/mesenchymal stem cells (without culture). Using current technology prices as lower and upper bounds for a reasonable range (Table 2),110–123 it appears that we have arrived at a reasonable ballpark range for the estimated cost of a bioreactor grown bone graft.
Although the projected cost of a tissue engineered graft aligns well with that of other cell-based approaches, it is significantly more expensive than a standard bone graft. Hence, it is important to consider under what conditions a patient would consider the increased cost justifiable. This is known as the headroom analysis and is another crucial component of feasibility assessment. 124 Tissue-engineered bone grafts may be reasonably considered when donor site morbidity associated with harvesting an autograft is a significant concern and allograft resorption and low integration typically present a problem. One such example of a niche market is spinal fusion surgeries, especially in the lumbar region. In these cases iliac crest harvesting for autografts often leads to long-lasting pain in a significant number of patients undergoing this surgery.125,126 A recent study found that a group of patients who underwent posterior lumbar spinal fusion using an iliac crest autograft as a bone graft source experienced a significant amount of pain and functional limitation even at 12 months after the surgery. 120 In addition, allografts are disadvantageous in the case of posterior lumbar fusions and often lead to incomplete integration with host bone and resorption.126–129 Tissue engineered grafts could also be useful in cases of large defects when there is not enough autogenic material to fill the defect and allograft material has shown previous problems of resorption due to limited vascular infiltration. While surgical vascularization of larger grafts is helpful in this regard, it is also a technically demanding, expensive procedure that could be avoided by using prevascularized tissue engineered grafts.130,131 Tissue engineered bone grafts may be particularly relevant in craniofacial applications where the gross geometry is crucial to function and the current best option requires calvarial bone harvesting. 132 Bone grafts could be engineered in the precise size and shape needed for cranioplasty, thus eliminating the need for bone harvest and eliminating aesthetic concerns. Thus, although the market for bone engineered grafts will be smaller due to their high cost in comparison to normal allo/autografts, it is our assessment that such a technology could prosper in cases in which normal grafts are unsuitable or have a high chance of failure.
Summary: The Application of Tissue-Engineered Bone Grafts
Currently, several multidisciplinary efforts are being made to improve the size and quality of the bone grafts that can be grown in vitro. These efforts focus largely on aspects of cell type, scaffold structure and composition, or cultivation parameters in various bioreactor systems. However, unless there is holistic consideration for how these engineered products can be employed in clinical settings, these studies run the risk of being practically and commercially nonviable from the onset. The past two decades have provided a wealth of lessons regarding the eventual feasibility of cell-based therapies. Chief among these lessons has been that commercial viability can trump science in determining whether an approach will become widely applicable. 133 Consequently, in determining whether bone bioreactors will facilitate the clinical application of engineered bone grafts, we must consider clinical scenarios in which engineered grafts would be desirable, the scientific feasibility of using engineered grafts relative to cell-seeded scaffolds, and economic aspects. The clinical need for engineered grafts, particularly in cases in which autografts are unavailable, has been firmly established and our analysis indicates that the cost of this approach lies within the range of other cell-based therapies. Therefore, many more in vivo experiments in small and large animal models need to be performed to robustly establish and quantify the benefits of using engineered grafts relative to other approaches so that these can be weighed against the costs of additional bioreactor cultivation.
Footnotes
Acknowledgments
This work is supported by a grant from the Department of Defense (DM090323). The authors would also like to acknowledge Dr. Lynne Jones for her help in cost research and insight into current use of bone grafts technologies in orthopedic medicine.
Disclosure Statement
No competing financial interests exist.