
Abstract
Nerve guides are increasingly being used surgically to repair acute peripheral nerve injuries. This is not only due to an increase in the number of commercially available devices, but also clinical acceptance. However, regeneration distance is typically limited to 20–25 mm, in part due to the basic tubular design. A number of experimental studies have shown improvements in nerve regeneration distance when conduits incorporate coatings, internal scaffolds, topographical cues, or the delivery of support cells. Current studies on designing nerve guides for maximizing nerve regeneration focus both on cell-containing and cell-free devices, the latter being clinically attractive as “off the shelf” products. Arguably better results are obtained when conduits are used in conjunction with support cells (e.g., Schwann cells or stem cells) that can improve regeneration distance and speed of repair, and provide informative experimental data on how Schwann and neuronal cells respond in regenerating injured nerves. In this review we discuss the range of current nerve guides commercially available and appraise experimental studies in the context of the future design of nerve guides for clinical use.
Introduction
Peripheral Nerve Injury, Clinical Treatment and Commercially Available Nerve Guides
Peripheral nerve injuries commonly result from acute trauma (e.g., road traffic or industrial accidents).1,2 For gap injuries greater than 5–10 mm autologous nerve grafts are usually considered as the “gold standard.” While relatively successful, major disadvantages include two surgical sites and donor site morbidity. 3 Nerve transfer is another surgical option where high level proximal defects are swapped with distal nerves for conversion to a lower level, but this still results in the loss of donor nerve function. 4 Nerve allografts are possible5,6 and functional recovery is comparable to autografts, but the need for systemic immunosuppressants and rejection risk limits this option. Electrical stimulation and physiotherapy can also increase the success of grafting techniques. 7
Alternatively, nerve guides can be used for defects of 20–25 mm, eliminating the need to graft. While the number of commercially available nerve guides is still relatively small, a number of products have recently become Food and Drug Administration (FDA) approved, 8 (summarized in Table 1). These can be grouped into naturally-derived or synthetic materials. Natural materials include NeuraGen®, a type-I collagen conduit that degrades after 48 months and gives good outcomes up to 20 mm9 and NeuroMatrix/Neuroflex® (Collagen Matrix, Inc.) also made from type-I collagen which degrades after 7 months. Avance® is a decellularized allogeneic nerve graft which has shown promising results in a study of 10 nerve defects from seven patients. Defects were between 5 and 30 mm, with no infection or rejection. 10 AxoGuard™ (Cook Biotech) is a 2–4 cm long conduit made from porcine small intestinal submucosa and RevolNerve® is made from collagen type-I and III extracted from porcine skin 11 (which does not have FDA approval at the time of writing). Synthetic materials include Neurolac®, a 3 cm long transparent poly-DL-lactide-co-ɛ-caprolactone (PDLLA/CL) conduit made by Polyganics which takes around 16 months to degrade and can heal defects up to 20 mm within 12 months. 12 Neurotube® (Synovis) is a polyglycolic acid (PGA) conduit manufactured up to 4 cm long which degrades in approximately 6 months, 13 whereas SaluMedica manufacture both SaluBridge™ and SaluBridge cuffs made from a nondegradable polyvinyl alcohol hydrogel. These are available up to 6.35 cm in length.
Apart from Avance, QiGel™ and RevolNerve, all other listed nerve devices have been Food and Drug Administration (FDA) approved.
PDLLA/CL, poly-DL-lactide-co-ɛ-caprolactone; PGA, polyglycolic acid.
A recent study 14 comparing Neurolac, NeuraGen and Neurotube using a 10 mm rat sciatic nerve excision model demonstrated no difference in recovery between Neurolac and autograft. Repairs with NeuraGen had lower compound muscle action potentials (CMAP) than Neurolac but differences were not significant and the conduit remained structurally stable. Neurotube had completely collapsed by 12 weeks, and was associated with the poorest outcome. A parallel study 15 also found that NeuraGen had a significantly better outcome compared with Neurotube. In particular axonal sprouting was less organized and less dense with Neurotube compared with NeuraGen or autograft. Another study comparing Avance conduits with NeuraGen or autograft, 16 found Avance to be superior to NeuraGen at 6 weeks but no difference by 12 weeks.
Natural Versus Synthetic Nerve Guide Materials
Two important considerations for nerve guide design include the materials used and method of fabrication.17,18 Clinical and experimental data suggest that guides should ideally degrade and be absorbed in 1–2 years following implantation. Of note are that nonresorbable conduits such as silicone have been associated with chronic inflammation, necessitating surgical removal. 19 Naturally-derived materials have advantageous properties such as cell binding domains encouraging neuronal and glial attachment and migration. 20 However, these are usually from animal sources and carry a minor risk of disease transmission (although most natural materials commercially used have regulatory approval), and can be more expensive than synthetic alternatives. 21 Synthetic material usage gives versatility in the physical and chemical design and controllability over stiffness and degradation rate, and the introduction of micro- or nanosized features. A summary of the studies highlighted in this review is given in Table 2 and shown diagrammatically in Fig. 1.

A summary of the various approaches currently being studied for the development of cell-free and cell-containing nerve guides for peripheral nerve repair. Color images available online at www.liebertonline.com/teb
ADSCs, adipose tissue-derived stem cells; DRG, dorsal root ganglion; PCL, poly-ɛ-caprolactone; PHB, poly-3-hydroxybutyrate; PHEMA-MMA, poly(2-hydroxyethyl methacrylate)–methyl methacrylate; PLA, poly(lactic acid); PLGA, poly(lactic-co-glycolic) acid; PLLA, poly(L-lactic acid); PPy, polypyrrole.
Natural materials
Type-I collagen nerve guides demonstrate regeneration comparable to autografts for gaps up to 20 mm.2,9,11,22 Zhang et al. 23 inserted a xenogeneic acellular nerve guide into a rat nerve defect for 7 days, with an absence of host rejection. However the empty guide showed lower myelinated nerve fiber density and lower CMAP scores compared with an autograft control. Ao et al. 24 inserted a phosphate-buffered saline (PBS) filled chitosan conduit into a 12 mm sciatic nerve defect in rats for 3 months, however conduction velocities, cross section myelin, and muscle areas were half that of autograft controls. Fibrin has recently gained attention as a promising NGC material,25,26 with axons crossing a 10 mm sciatic nerve rat defect after 1 month. 27
Silk fibroin has been recently investigated, and is attractive due to favorable degradation properties and low inflammatory response.28–34 Yang et al. 31 implanted silk fibroin conduits into Sprague-Dawley rats for 6 months with positive results when evaluated by electrophysiology, histology, and retrograde tracing. Ghaznavi et al. 33 compared silk fibroin versus collagen guides in rats for 1, 4, and 8 weeks and reported a similar inflammatory reaction as collagen guides. The gastrocnemius weight of muscle from silk fibroin conduits was 27% lower than autograft, but greater numbers of proximal sprouts and distal connections were found. Wang et al. 29 studied an electrospun silk fibroin conduit blended with poly(L-lactic acid-co-ɛ-caprolactone) (P(LLA-CL)). The silk fibroin P(LLA-CL) blend outperformed the P(LLA-CL) in electrophysiological, immunohistochemical, and histological scores.
Synthetic materials
Synthetic nerve guides materials have been largely confined to polyesters such as PGA, poly(lactic acid) (PLA), poly-ɛ-caprolactone (PCL), and poly(L-lactic acid) (PLLA). These materials are used in many FDA approved devices such as sutures and orthopedic screws. A study by Weber et al. 35 compared PGA conduits versus autografts or direct coaptation in a clinical digital nerve reconstruction trial. PGA implants were scored as being 44% excellent, 30% good, and 26% poor, in comparison with 43% excellent, 43% good, and 14% poor for the coaptation/autograft control. In another study using PGA conduits for facial nerve defects, five out of seven patients reported good or very good facial muscle control, while two reported a fair recovery. 36 Given data on Neurotube guides collapsing after 12 weeks in a rat sciatic model, 14 PGA conduits may be suitable for injuries associated with areas of low load.
PCL has attractive properties as a biomaterial scaffold for regenerative medicine 37 and a PDLLA/CL blend (Neurolac) is used clinically. 12 Other polymer blends include PCL/PLA, 38 PGA/PCL and PCL/PGA 39 and poly(lactic-co-glycolic) acid (PLGA) 40 (natural material blends include gelatin, 41 chitosan 42 and collagen.43,44) Functionalisation and the addition of bioactive molecules45–48 has also been conducted using PCL. Chung et al. 45 compared PCL conduits conjugated with nerve growth factor (NGF) versus NGF and tirofiban. Conduits were implanted into a 12 mm rat sciatic nerve defect for 8 weeks, after which NGF plus tirofiban conduits stimulated heavier gastrocnemius muscle, stronger β-tubulin III and growth-associated protein-43 (GAP-43) staining. Klinkhammer et al. 49 reported on a conduit using PCL blended with NCO-poly(ethylene glycol)-stat-poly(propylene glycol) (PCL/sPEG), enabling attachment of the integrin binding peptide GRGDS. Results showed that Schwann cells migrated faster and had improved axonal growth. 48
PLGA can be blended to increase degradation rate compared with PLLA alone, 50 and an 85:15 PLGA foam inserted in to a 10 mm rat sciatic defect demonstrated regeneration after 12 weeks. 51 Similarly, 10:90 PLGA microbraided guides 40 demonstrated that while average nerve diameters were only half that of normal nerve, axons migrated into 9 out of 10 conduits (which separately degraded by ∼50% after 34 days in PBS). Compared with PLGA, PLLA is stiffer due to a higher degree of crystallinity and can take up to 3 years to degrade. 52 Evans et al. 53 found that after a 16 week rat sciatic study, significantly more axons had regenerated in a 10 mm PLLA guide compared with PLGA. An 8 month implantation study 54 showed that 12 mm PLLA conduits resulted in a sciatic functional outcome index similar to isografts.
Poly-3-hydroxybutyrate (PHB), a thermoplastic polyhydroxyalkanoate, has been investigated for various medical applications such as sutures and wound dressings and has good biocompatibility. 55 It has been suggested that PHB acts as a “neural protective” agent, on the basis that apoptotic cell number decreases when in contact with PHB versus tissue culture polystyrene. 56 Young et al. 57 found that a 4 cm injury in rabbits was bridged after 42 days, with a higher regenerating fiber area compared with autografts. Degradation rate was of the order of 18–24 months. When implanted into six patients, PHB wrap-around implants gave advantageous results compared with epineural suturing at 18 months. 58 However, Kalbermatten et al. 27 compared PHB to a fibrin glue conduit in a rat sciatic model. After a month, neuronal and Schwann cells were located deeper in the fibrin conduit compared with PHB.
The physical properties of nerve conduits has not been studied in detail, but hydrogel conduits have been designed on the basis that a high water content mimics the physical properties of nerve. 59 Poly(2-hydroxyethyl methacrylate) (PHEMA)-co-methyl methacrylate (MMA) conduits have shown comparable results to autografts at 4 and 8 weeks in a 10 mm rat sciatic model. 60 A follow-up study reported that 4 out of 14 PHEMA-MMA conduits had collapsed after 16 weeks, with some showing signs of chronic inflammation and calcification. 61 Katayama et al. 62 followed this by developing plain, corrugated, and coil-reinforced PHEMA-MMA conduits to improve mechanical strength. Coil reinforced conduits showed better performance in terms of patency and nerve regeneration with similar results to autografts after 16 weeks.
Piezoelectric materials such as polyvinylidene fluoride (PVDF) conduits have been studied for their electrical conductivity with varying success. Poled PVDF conduits are reported to increase myelinated axon number compared with unpoled nonconducting conduits in a 4 mm rat sciatic nerve model after 12 weeks. 63 Further, a PVDF and trifluoroethylene copolymer had a significantly greater number of myelinated axons. 64 Similarly, an electrically conducting polymer conduit of PDLLA/CL doped with polypyrrole (PPy) 65 had a similar number of myelinated axons and Schwann cells to native nerve after 2 months in an 8 mm rat sciatic model. Interestingly, when PC12 neuronal cells were cultured on a conducting polycaprolactone fumarate–PPy, the number of neurites per cell, percentage of neurite bearing cells, and neurite length increased when exposed to 10 μA constant current. Further increases occurred when an alternating current was used. 66
Nerve Guide Coatings
Nerve guide materials can be coated to improve cell attachment, proliferation, and migration, with extensive studies on extracellular matrix proteins. When grown on laminin, Schwann cells were found to increase the length of NG108-15 neurites specifically via the NF-κB pathway. 67 Laminin is known to direct axons within basal lamina tubes 68 and when blocked, grafts implanted in to a 1 cm rat sciatic nerve defect only had 48% regenerating axons compared with 92% in nonblocked controls. Armstrong et al. 69 found that laminin promotes higher Schwann cell proliferation compared with fibronectin, which in turn was higher than collagen. When coated with laminin and fibronectin, collagen type-I nerve guides had nerve fibers grow into the middle of a 1 cm rat sciatic defect after 30 days, in contrast to uncoated controls. 70 It is known that laminin synergistically works with factors including basic fibroblast growth factor (FGF), where enhanced neurite outgrowth of ex vivo rat dorsal root ganglion (DRG) cells on nanofibers is reported. 71
Synthetic polymers with appropriate degradation rates can be readily coated to improve their nerve regenerative properties. Plasma polymerization is a reproducible and scalable method for coating materials with defined chemical functionality, without altering the chemistry of the bulk material. Plasma coated acrylic acid and allylamine surfaces improved the adhesion of human SH-SY5Y neuroblastoma cells compared with polyethylenetherephtalate, 72 while acrylic acid surfaces increased cell coverage and extent of the differentiation marker neurofilament-200. In contrast, allyl amine promoted cell adhesion, but not differentiation. Ni et al. 73 grafted chitosan and FGF-1 on gold nanoparticle-containing PLA conduits, which showed superior results to conduits without chitosan or FGF-1 in a 12 mm rat sciatic defect.
Haptotactic Gradient Surfaces and Topographical Cues
It is known that cells respond to gradients and topographical cues and there is increasing research on the effect of grooves, channels, and ridges on neural cell responses. 74 Dodla et al. 75 reported that gradients of laminin and NGF contained within anisotropic agarose hydrogels stimulate nerve regeneration in a 20 mm rat sciatic model comparable to syngeneic grafts. However after 4 months a uniform distribution of laminin and NGF did not stimulate axonal regeneration, nor did isotropic gradients of laminin. Similarly, a 357 ng/mL/mm gradient of NGF in a PHEMA gel is reported to stimulate neurite extension and guide PC12 neurites. 76 Carboxyl group gradients attached by UV grafting and argon ion plasma are reported to increase C17.2 neuronal cell neurites 3.7-fold when growing down the gradient compared to the number of neurites at higher acid densities. 77 Gradients of the laminin IKVAV peptide also cause neurites of chick embryo DRGs to follow, then turn, and migrate along them. 78 Neurite velocity slowed when turning along the gradient but then increased when on a straight course. 20
Different surface topographies can influence cell morphology and differentiation. 79 Human mesenchymal stem cells (MSCs) cultured on nanopatterned surfaces expressed higher myelin-associated protein 2 (MAP-2) and neurofilament light protein (NLP). 80 Britland et al. 81 found that grooved surfaces 12 μm wide and 6 μm deep were optimal for DRG neuronal alignment. When combined with parallel laminin tracks, optimal neurite alignment was observed with 25 μm wide and 6 μm deep and grooves. Perpendicular chemical and topographical cues stimulated DRGs to predominantly follow the chemical cues when adsorbed to grooves with a depth of 500 nm. Similarly, micropatterned PLGA guides coated with laminin peptides or collagen type-I showed greater neurite alignment on 5 μm grooves compared with 10 μm, supporting the idea that neurite extension requires a precise physical space. 82 Similarly, Rajnicek et al. 83 found that rat hippocampal neurites perpendicularly orientated to 1 μm wide grooves with depths of 130–1100 nm, which reversed when grooves were increased to 4 μm width. Sun et al. 84 produced rolled microgrooved PCL nerve guides, on which NG108-15 neuronal cells and primary Schwann cells showed better alignment on patterns with a small 5 μm ridge width and bigger 20 μm groove width. A similar approach using PCL and PCL/PLA rolled conduits in a 1 cm rat sciatic model showed nerve cable formation after 2 weeks. 38
Intraluminal Guidance
A number of studies report on the presence of internal scaffolds either as synthetic polymers or as matrix proteins contained within the lumen of nerve guides for improved physical or chemical guidance.41,43,71,85–88 Cai et al. 85 reported on improved distal regeneration when PLA or silicone conduits contained 16 aligned PLLA microfilaments using a rat sciatic model. Improved regeneration was also reported when silicone tubes were loaded with collagen, laminin, and fibronectin gels. 89 But results are not always in agreement, as Valentini et al. 90 found that a laminin and collagen gel impeded nerve regeneration in a rat sciatic model.
Electrospun nano- and microfibers have attractive physical properties as intraluminal scaffolds and can be readily fabricated from a wide range of biocompatible materials. 88 Aligned fibers are found to be more effective at guiding Schwann and neuronal cells compared with nonaligned.29,34,41,44,86–88,91–94 Cho et al. 87 demonstrated that rat MSCs cultured on NGF conjugated aligned PCL nanofibers expressed higher levels of β-tubulin III, nestin, and MAP-2 versus nonaligned fibers. Irrespective of fibers, channels, or grooves, neuronal cells seem to be optimally guided with widths in the range of 5–20 μm and 10–20 μm in diameter. While aligned nanofibers demonstrate positive results 95 neuronal and Schwann cells tend to spread across nanofibers as a mat (reviewed in detail by Cunha et al. 96 ) rather than being restricted to a single cell/microfiber interaction (see Fig. 2).

Scanning electron micrographs of rat neural stem progenitor cells cultured on
Schnell et al. 43 reported that DRGs showed faster elongation on PCL aligned nanofibers (559±300 nm and 541±164 nm) versus PCL containing collagen, but had improved axonal guidance on PCL/collagen. Human Schwann cells upregulated myelin P0 when cultured on aligned PCL, which was not observed on random fibers. 86 Jha et al. 91 described a novel two-pole air gap electrospinnng method to fabricate a 10 mm nerve guide consisting of aligned fibers varying from 200 nm to 1.5–1.8 μm. Implantation into a rat sciatic model for 7 weeks bridged the defect with Schwann, neuronal, and blood vessel formation. In contrast to fibers, Yao et al. described a stainless steel wire template method for forming collagen multichannels, 97 which supported DRG explant outgrowth. NGCs containing multiple channels (four or seven) had better physical properties compared with a single channel, and Krych et al. 93 found more regenerating axons in 450 μm channels compared with 650 μm channels in a rat spinal cord defect. However, while Clements et al. 98 reported positive results using one intraluminal film of poly-(acrylonitrile-co-methylacrylate) contained in a polysulfone conduit, three films resulted in poor morphological organization and misaligned collagen bands.
New methods for studying neural cell interactions within 3D nerve guides includes work by Murray-Dunning et al. 99 who describe a closed-loop perfused bioreactor for introducing and culturing cells on experimental nerve scaffolds. Conduits of up to 8 cm in length and 1.2 mm internal diameter were studied using aligned intraluminal PLLA microfibers. Scaffold properties, including the surface modification of fibers by acrylic acid deposition showed enhanced Schwann cell survival. A similar investigation using Schwann cells in a rotating wall bioreactor found enhanced proliferation on spiral shaped scaffolds, compared to tubular or porous cylindrical shaped conduits. 100
Addition of Growth Factors
It is well known that neurotrophic factors enhance nerve regeneration, and a number of studies have incorporated neurotrophins in to nerve guides. It would appear that conjugation of growth factors directly to scaffolds rather than adsorption has an enhanced biological effect. 87 Positive results were reported on the slow release of NGF and glial-derived neurotrophic factor (GDNF) from ethylene vinyl acetate conduits in a 15 mm rat sciatic model, where cable formation was observed after 7 weeks in contrast to control. 101 GDNF alone stimulated more myelinated axons compared with NGF. Recently, a study incorporating GDNF as microspheres in a PCL conduit observed a significant increase in tissue integration after 6 weeks, compared with PCL alone. 102 Boyd and Gordon 103 investigated the effects of GDNF and brain-derived neurotrophic factor (BDNF) at 0.1 μg and 2 μg/day respectively on chronic and acute axotomy. After 28 days, GDNF significantly increased the number of motor neurons but the combination of GDNF and BDNF was more potent. Similarly, neurotrophin-3 is reported to increase myelinated axon number after 8 months when delivered from a fibronectin conduit at an optimal dose of 30–500 ng/mL. 104 While the beneficial effect of growth factors is clear, the cost of inclusion in to commercial nerve guides is a consideration.
Incorporation of Support Cells into Nerve Guide Conduits
The delivery of support cells known to secrete a range of growth factors and matrix proteins for assisting nerve repair has been studied. This predominantly includes Schwann cells, based on their essential role in repair.105,106 Schlosshauer et al. 107 found that axons can grow eight times faster than Schwann cells migrate on PLGA. However in vivo, axonal regeneration only proceeds to the extent at which Schwann cell migrate. It has therefore been suggested that Schwann cells are included in NGCs before implantation. The beneficial effects of Schwann cells on neuronal cells are widely reported, with work showing that primary Schwann cells on fibronectin, collagen, or laminin enhance the number, length, and percentage of neurites. 69 The presence of matrix proteins is reported to directly activate the neurotrophic properties of Schwann cells, but in addition reveals the physical effects of Schwann cells (most likely via matrix protein formation) for neuronal cell differentiation. An alternative to the traditional nerve guide has been recently proposed using a PHB strip for delivering Schwann cells implanted into 10 mm sciatic gap in rats, 108 where after 2 weeks superior nerve regeneration and Schwann cell migration was observed, compared to Schwann cells seeded on a PHB conduit.
Problems do however exist in the clinical translation of autologous Schwann cells, with limited tissue availability, long culture times, and donor site morbidity. Alternatively, allogeneic Schwann cells have been investigated and Mosahebi et al. 109 compared allogeneic and syngeneic Schwann cells in alginate within a PHB guide. A significant increase in rat sciatic regeneration was noted for both types of Schwann cells compared to acellular guides with no deleterious immune responses. However, Evans et al. 110 reported no positive effect from allogeneic Schwann cells in a collagen matrix when contained in a PLLA nerve guide.
To avoid problems with Schwann cell use clinically, stem cells have been differentiated toward a Schwann lineage. MSCs (first identified in 1966 111 ) show promising characteristics such as hypo-immunogenicity112,113 and a “homing” mechanism toward injury sites. 114 The International Society for Cellular Therapy suggests three identifying characteristics of MSCs 115 : (1) plastic adherence under standard conditions; (2) ≥95% population positive for CD105, CD73, and CD90, and (3) negative (≤2%) for CD45, CD34, CD14/CD11b, CD79/CD19, and human leukocyte antigen class II (HLA-DR). MSCs can be differentiated into glial-like cells and aid neuronal survival,116–126 however studies report that naive MSCs express neuronal and glial proteins before differentiation, which increase further during differentiation. 127 Differentiated mouse MSCs produced BDNF and NGF 128 and increased motor recovery together with myelinated sciatic axon number, when delivered in collagen tubes. 129 Similarly, decellularized allografts implanted into Rhesus monkeys containing autologous BMSCs showed improved electrophysiology after 8 weeks 130 and 6 months. 131 BMSC-derived Schwann cells 24 in chitosan conduits are also reported to perform as well as conduits containing Schwann cells, with comparable muscle fiber histology and a higher number of myelinated axons.
Adipose tissue-derived stem cells (ADSCs) have significant advantages over BMSCs,132,133 including a less invasive isolation procedure and higher stem cell number recovered. 134 ADSCs biology is reviewed in detail elsewhere, 135 but of note is that 1 in 25,000–100,000 bone-marrow cells are stem-like compared with 2% from adipose tissue. 136 Di Summa et al. 137 compared differentiated rat MSCs to ADSCs in a fibrin conduit using a sciatic nerve defect (see Fig. 3). After 16 weeks the ADSC conduit showed a superior evoked potential at the gastrocnemius muscle and motor regeneration. Recently, Kaewkhaw et al. 138 highlighted the importance of the anatomical origin of ADSCs for differentiation to Schwann cells. Differences were revealed between subcutaneous, kidney, and epididymis fat sources, together with supporting evidence for ADSC differentiation to Schwann cells, glial protein expression, neurotrophin secretion, and neurotrophic function. An interesting approach by Zhang et al. 23 described a xenogenic porcine acellular nerve guide containing autologous differentiated ADSCs. Implantation into a rat was subcutaneously made for 28 days to suppress a potential immune response before insertion into a sciatic injury. Axonal regeneration was supported and differentiated cells were observed along the graft expressing NGF, GDNF, BDNF, glial fibrillary acidic protein (GFAP), and S100. Similarly, an allogeneic decellularized artery implanted into a rat facial defect seeded with ADSCs, dADSCs, or native Schwann cells 139 showed dADSC and Schwann cell groups performed similar to autograft.
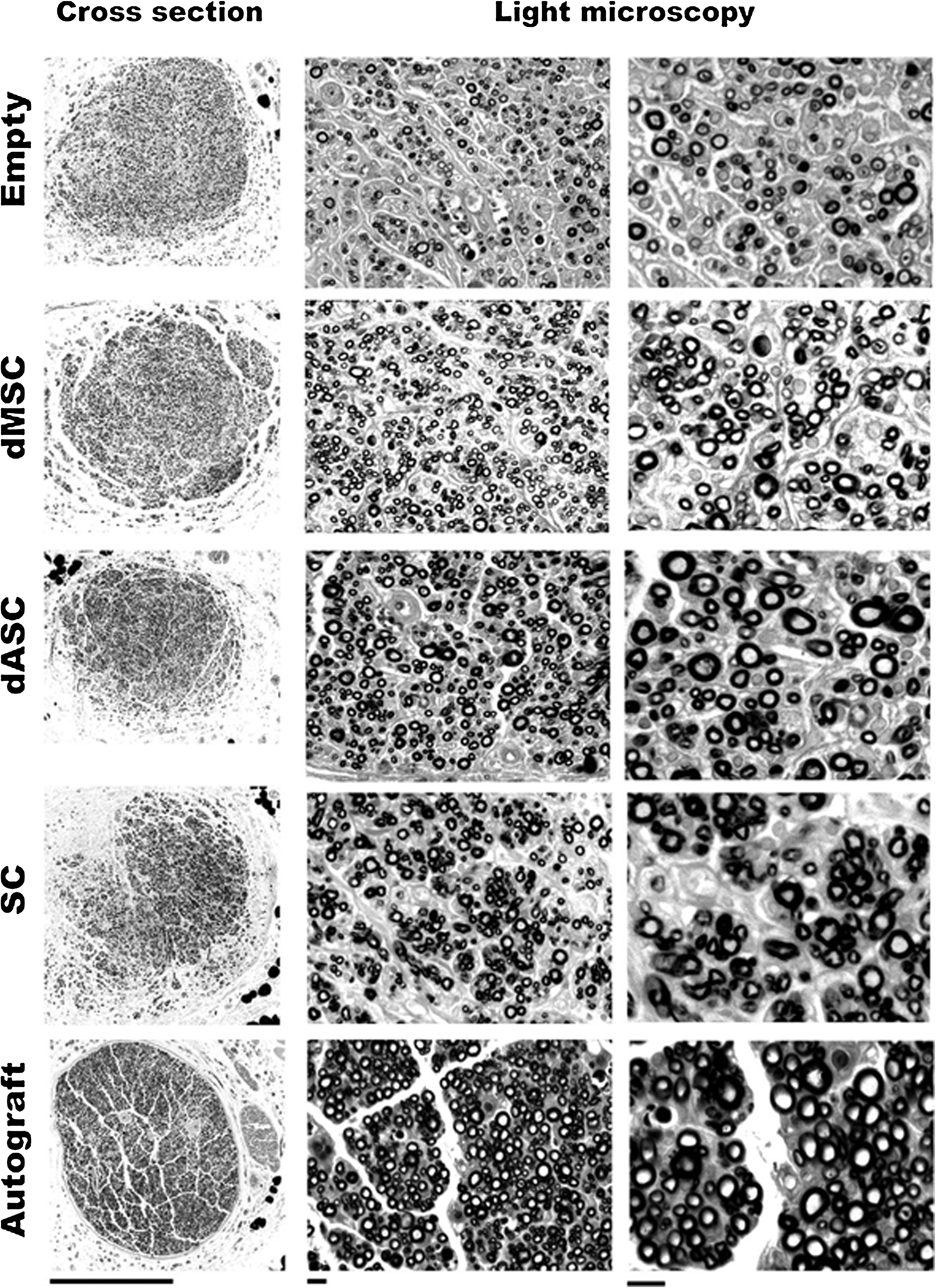
Light microscope images of sciatic nerve regeneration 16 weeks after the following treatments were applied to a 1 cm rat sciatic nerve defect: empty fibrin guide, fibrin nerve guide seeded with Schwann-like differentiated MSC (dMSC), Schwann-like differentiated ASC (dASC), primary Schwann cells (SC), and autografts. Columns from left to right: whole nerve cross sections (scale bar 500 μm), and nerve sections 1 mm distal to the suture site (scale bars are 10 μm for middle column and 20 μm for right hand column). Reproduced with permission.137
Human ADSCs have been injected into an RGD peptide coated PCL nerve guide and implanted into a 6 mm sciatic nerve defect in athymic rats. 140 However, little regenerative improvement was seen by week 12 and lipid droplet formation was observed, introducing the idea of whether ADSCs require predifferentiation before implantation. Erba et al. 141 reported on positive axonal outgrowth and Schwann cell infiltration when undifferentiated ADSCs were added to a PHB conduit in a rat sciatic model, suggesting a particular role in stimulating growth factors and recruiting Schwann cells. Some studies report that only differentiated MSCs stimulate nerve regeneration after transplantation,119,125 while others report that naive MSCs can stimulate axon growth in vivo by transdifferentiation to Schwann cells.140,142 Reversion of ADSCs to fat cells following transplantation 140 or conversion of dADSCs into fat cells remains to be fully established before their use clinically.
Conclusions
The current and future design and properties of clinical and experimental nerve guides is reviewed herein. Although nerve guides show clinical efficacy, their use presently is not widespread. 12 Both naturally-derived and biodegradable synthetic devices are reported to give good results for short gap injury repair with studies suggesting degradation rate should be controlled over a 1–2 year period. A remaining challenge is the limit of 20–25 mm for transection injuries. To address this, the future design of conduits is seeing a rapid integration of several technologies which can be grouped in to cell-free and cell-containing devices. Cell-free devices are attractive as off-the-shelf products, and more straightforward and cost effective to use. The next generation of nerve guides is likely to see significant improvements in the physical design of these, in conjunction with chemical and/or biochemical modifications. Rapid developments include intricate intraluminal structures present as channels or fibers and the introduction of surface chemistries for improving otherwise inert materials, together with the inclusion of growth factors. Such devices are close to being clinically translated (although considerable scope presently exists for the increased use of existing devices). Devices which contain support cells generally show improvements experimentally over cell-free devices and a number of recent studies report on the potential of mesenchymal and adipose-derived stem cells to improve repair, either as naive or predifferentiated cells. These approaches have considerable potential, but practical limitations exist for the clinical delivery of cells and therefore are likely to be several years away from becoming routine in clinical terms.
Footnotes
Acknowledgment
Juliet H.A. Bell is funded by an EPSRC Doctoral Training Award to the Department of Materials Science and Engineering at the University of Sheffield, United Kingdom.
Disclosure Statement
The authors have no competing financial interests.