
Abstract
Hyaline cartilage lesions represent an important global health problem. Several approaches have been developed in the last decades to resolve this disability cause, including tissue engineering, but to date, there is not a definitive procedure that is able to promote a repair tissue with the same mechanical and functional characteristics of native cartilage, and to obtain its integration in the subchondral bone. The need of resolutive technologies to obtain a “more effective” tissue substitutes has led Butler to propose the “Functional Tissue Engineering” (FTE) paradigm, whose principles are outlined in a so-called FTE road map. It consists of a two-phase strategy: in vitro tissue engineering and clinically surgery evaluation. The first phase, based on construct development, should take into account not only the chondrocyte biology, as their sensitivity to biochemical and physical stimuli, the risk of dedifferentiation in culture, and the ability to produce extracellular matrix, but also the features of suitable scaffolds. The in vivo phase analyzes the inflammatory microenvironment where the construct will be placed, because the cytokines released by synoviocytes and chondrocytes could affect the construct integrity, and, in particular, cause matrix degradation. The use of pulsed electromagnetic fields (PEMFs) represents an innovative therapeutic approach, because it is demonstrated that this physical stimulus increases the anabolic activity of chondrocytes and cartilage explants with consequent increase of matrix synthesis, but, at the same time, PEMFs limit the catabolic effects of inflammatory cytokines, reducing the construct degradation inside the surgical microenvironment. PEMFs mediate an up-regulation of A2A adenosine receptors and a potentiation of their anti-inflammatory effects.
Introduction
Considering that articular cartilage has very limited regeneration capability, cartilage repair procedures will continue to increase. To treat articular cartilage damage effectively, it is necessary to fill the defect with a repair tissue with the same mechanical and functional characteristics of hyaline cartilage and to promote the integration of the repair tissue with the host cartilage and the subchondral bone. 5 To fulfil these aims, several procedures have been proposed such as chondroabrasion or microfractures that recruit medullary stromal cells from subchondral bone, and techniques which fill the cartilage damage with autologous ex vivo cultured chondrocytes, enriched bone marrow mesenchymal stem cells (MSCs), or osteochondral grafts. 6 So far, clinical research has failed to identify surgical procedures that can reproduce the biological composition and biomechanical properties of native cartilage. Although no definitive treatment for cartilage repair is available, significant effort has been made to optimize treatment modalities, in particular those based on engineered cartilage tissue to speed up and improve chondral and osteochondral regeneration, thus allowing patients a swift return to previous activity levels and preventing or, at least, delaying OA.
Tissue-engineering procedures aim at overcoming the current limitations of traditional surgical treatment by offering functional regeneration in the defect region. They require an initial step of in vitro culturing of chondrocytes or MSC alone or in the presence of natural or synthetic extracellular matrix (ECM)-based scaffolds followed by implantation into the cartilage defect. A one-step procedure involving bone marrow cellular pool transplantation has been proposed to avoid two surgical procedures and costs associated with cell expansion. 7 Another “simple” approach is to implant a bioactive scaffold that is capable of recruiting and stimulating the patient's own cells where tissue regeneration is obtained by a combination of chemistry, structure, or topography. 8
Despite recent progress, the challenges remain significant; in fact, after construct implantation, degeneration of the new tissue and surrounding host cartilage has been reported.9,10 Cartilage repair often results in fibrocartilaginous tissue without the stratified organisation of normal hyaline cartilage. 10 Where hyaline cartilage is produced, it is typically immature and does not show a true articular surface. Functionally, the repair tissue is not mechanically competent and fails to withstand the mechanical stress applied to articular cartilage. Furthermore, successful lateral integration between the host cartilage and repair tissue is largely lacking; so, future degeneration is almost inevitable. 10
Joint microenvironment is modified following a local surgical procedure or in OA patients; in particular, pro-inflammatory cytokine concentration increases in the synovial fluid. Furthermore, cartilage lesions that arise from a chronic degenerative process present even more additional, unsolved problems. The entire articular surface is diseased: Condrocytes and synoviocytes secrete inflammatory cytokines and proteolytic enzymes, which have a marked effect on engineered constructs and implanted cells.
Therefore, there is still the need to improve the presently available technologies that may lead to the development of more effective tissue substitutes leading to a long-lasting effective clinical outcome. These objectives were clearly defined by Butler, who proposed a Functional Tissue-Engineering (FTE) paradigm, whose principles were outlined in a FTE road map (Fig. 1).11,12 It can help design and fabricate effective tissue-engineered constructs, and is conceived in a two-phase strategy: (1) in vitro “tissue engineering”; (2) and clinical “surgery and evaluation.” 13
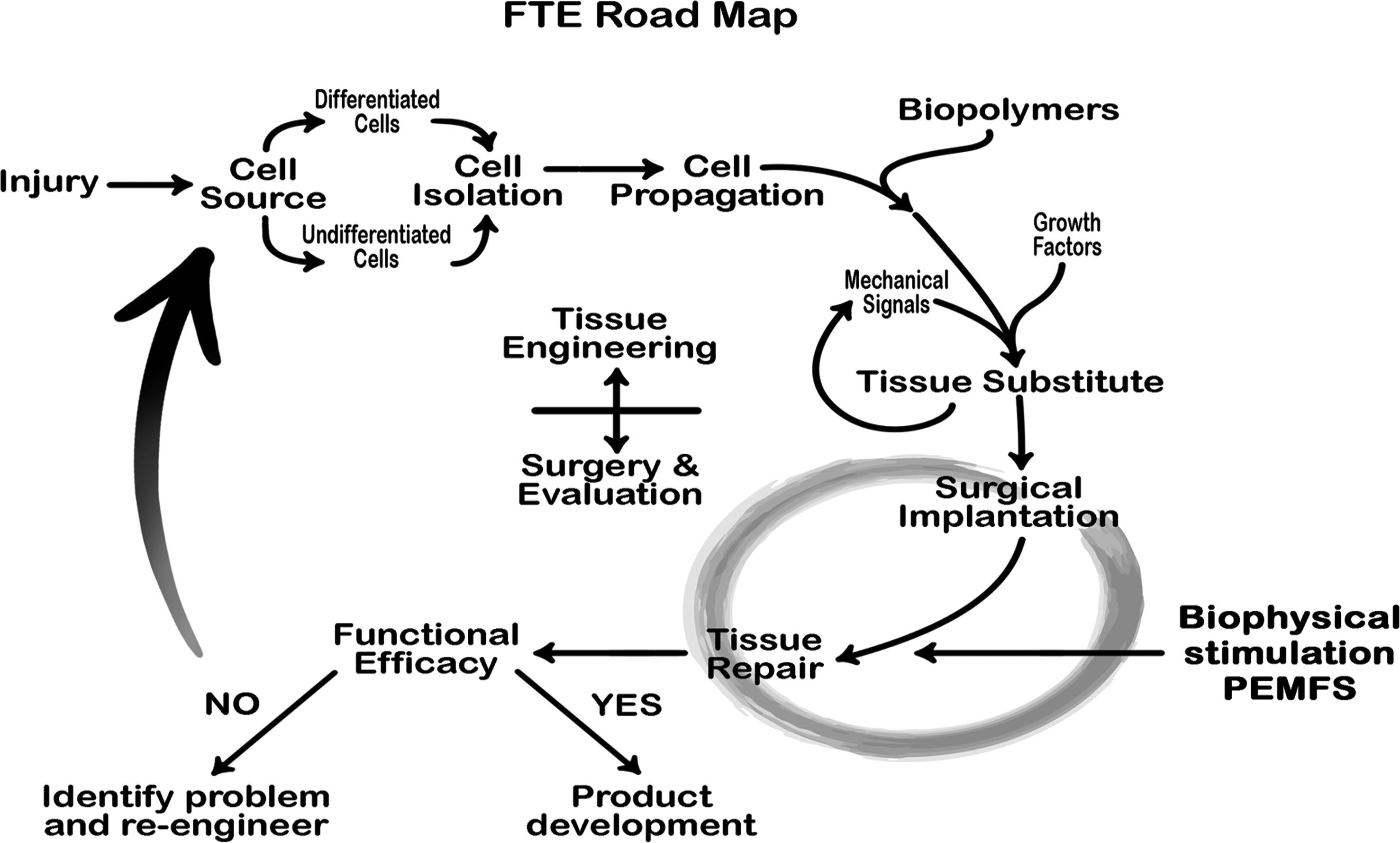
Functional Tissue Engineering (FTE) Road Map. Adapted from Ref. 13.
By reviewing the scientific literature on physical stimuli and tissue-engineering approaches for cartilage repair, the present article hypothesizes a double role for pulsed electromagnetic fields (PEMFs) stimulation: in vitro, by stimulating cells proliferation, colonization of the scaffold, and production of tissue matrix; in vivo, after surgical implantation of the construct, by favoring the anabolic activities of the implanted cells and surrounding tissues and protecting the construct from the catabolic effects of inflammation.
Tissue-Engineering Phase: Development and Manipulation of the Construct in Culture
Biological methods have been conceived to develop an engineered tissue in vitro starting from the patient's own chondrocytes or MSC. 14 The engineered tissue grown in vitro results from the combination of biomaterials and cells, whose activity can be controlled by the addition of signal molecules, such as growth factors or modulated by physical stimuli. Many different materials have been proposed as scaffolds (Table 1), which might support the proliferation, colonization, and, consequently, the ECM production of cultivated cells; furthermore, they might serve as a carrier for chondrocytes when implanted in the lesion site. 15 To obtain the engineered construct in vitro, the culture conditions (medium, growth factors [GFs], oxygen tension, and two- or three-dimensional [3D] culture) and the scaffold chemistry and morphology have profound implications on cell viability, proliferation, dedifferentiation/redifferentiation, and ECM synthesis.15,16 The addition to the culture of cytokines is used to favor cell proliferation and differentiation, as well as physical electric stimuli (PEMF, direct current, and electric fields) or mechanical stimuli (pressure, shear, and pulsed ultrasound) have been investigated to favor cell proliferation and anabolic action and, finally, EMC synthesis in vitro.
HA, hyaluronic acid; IGF-1, insulin-like growth factor-1; TGF, transforming growth factor.
Pelltari described how articular chondrocytes in two-dimensional cultures are accompanied by cellular de-differentiation (loss of Type II collagen or aggrecan). 17 Efforts to limit de-differentiation during expansion in monolayers by seeding cells onto dishes coated with proteins mimicking the ECM such as agarose gel (fibronectin, type I or II collagen) or in environments supporting a 3D-cell morphology, including gels, scaffolds, and porous microcarriers, did not show convincingly that maintenance of the native phenotype can be achieved in parallel with extensive proliferation. 18 On the other hand, chondrocytes expanded in the presence of specific GFs, which enhanced the process of de-differentiation, displayed a higher postexpansion cartilage-forming ability and could respond to chondrogenic stimuli more efficiently during subsequent culture in a 3D scaffold. 18
Similar to OA condrocytes, ex vivo cultured chondrocytes express a variety of pro-inflammatory chemokines, chemokine receptors, and cartilage proteolytic enzymes whose production is enhanced by increasing cell passaging and stimulation with interleukin (IL)-1β and tumor necrosis factor (TNF)α. 19
With regard to the seeding method, under static conditions, it is generally difficult to distribute cells within the scaffold with adequate efficiency and uniformity, and to subsequently supply them with sufficient nutrients that support growth, function, and viability throughout the full thickness of the construct. To overcome the limitations of not only static but also stirred cultivation systems, a system based on a direct, continuous, and monitored perfusion through the scaffold pores of a cell suspension for cell seeding, and a culture medium for subsequent culture is becoming increasingly popular. Direct perfusion systems have been reported to achieve high cell-seeding efficiencies at uniform distributions, maintaining cell viability within large constructs for extended periods of time. Flow-induced shear stresses in perfusion systems have also been used to improve cell proliferation and differentiation. 20
Lisignoli described the influence of transforming growth factor (TGF)β, associated with hyaluronan scaffold, in chondrogenic differentiation in vitro and mostly with MSC. 21 A similar in vitro model (mesenchymal cell/hyaluronan scaffold/TGFβ) was used to study the influence of this growth factor on the secretion of chemokines that contribute to the maintenance of cartilage homeostasis: IL-8, interferon-gamma-inducible protein-10, stroma-derived factor-1, B-cell-attracting chemokine-1, and their receptors. During in vitro human-MSC chondrogenic differentiation, chemokine and receptor expression was specifically induced or repressed, and this was in line with what the authors also found in normal articular cartilage, thus suggesting a role in differentiation and maturation of a cartilage-like structure in vitro and, consequently, the regulation of cartilage homeostasis. 22 Protease activity seems to be very important both in the simple chondrogenic process and in migration, fibrin clot remodeling, and growth factor activation. 23 In particular, matrix metalloproteases (MMPs) play a role in the transition of MSC to mature chondrocytes. 24 mRNA of MMP10, MMP11, and MMP13 is significantly up-regulated during differentiation in expanded human MSC, and MMP13 is considered as playing a key role in the late phase of chondrogenesis. 25 It is known that MMP13 induction is characteristic for terminally differentiating chondrocytes in the growth plate, but its expression in articular cartilage reveals a pathological process in progress.
The review by Ahmed highlights precisely how material and factors (chemical or physical) influence chondrocyte differentiation. 6 The different combination between scaffolds and bioactive agents: not only TGF-β1, TGF-β2, TGF-β3, bone morphogenetic protein (BMP)2, BMP-4, BMP-6, BMP-7, fibroblast growth factor (FGF)-2, insulin-like growth factor (IGF)-1, and parathyroid-hormone-related protein, but also calciumphosphate, increase cellular adhesion, proliferation, and ECM synthesis.
Finally, articular cartilage is exposed to a finely regulated gradient of relatively low oxygen percentages. Strobel and Wernik showed how a low oxygen percentage applied during the differentiation phases of chondrocyte culture enhances cell biosynthetic activity as well as reduces the activity of catabolic enzymes that are known to play key roles in the breakdown of cartilage matrix.26,27
Since the joint environment is mechanically demanding, physical stimuli play a crucial role during the normal development and homeostasis of cartilage and during the in vitro engineering phase. Trindade et al. showed how intermittent hydrostatic pressure inhibited matrix metalloproteinase and pro-inflammatory mediator release from human osteoarthritic chondrocytes in vitro. 28 Angele et al. found how the application of mechanical stimuli enhanced the cartilaginous matrix formation of mesenchymal progenitor cells differentiated in vitro. 29 Similar results were described by Miyanishi et al., who found a 10-fold increase of mRNA levels for each type II collagen, and aggrecan when applying intermittent hydrostatic pressure to adult human MSC in vitro. 30
Tanimoto described how an excessive mechanical stimulus can increase both secretion and activity of the degradation enzyme hyaluronidase (HYAL1 and HYAL2). 31
Wescoe investigated the role of the biochemical and biophysical environment in chondrogenic stem cell differentiation assay and cartilage tissue engineering, evidencing that spatiotemporal application of the stimuli and the time of transplantation of an engineered construct still need to be optimized. 32
By taking into consideration and controlling all the scaffold- and cell-related critical factors mentioned earlier, the final laboratory phase requires the evaluation of the tissue substitute's biomechanical and biological properties before it is implanted; the in vivo result depends on the capability of functional remodeling and integration with host tissue.
Surgery and Evaluation Phase: Implantation of the Construct to Repair the Tissue Defect and Outcome Evaluation
The lesion site scenario completely differs from the strictly controlled in vitro tissue conditions. In the joint environment, potent catabolic mediators could severely impact chondrocyte metabolism and ECM maintenance.19–33 Most cartilage tissue engineering is being done for trauma, which alters the physiological joint environment, leading to an increase of proinflammatory cytokines in the acute phase of inflammation. In the long term, the chronic presence of elevated levels of IL-1 and IL-6 in the synovial fluid could be responsible for cartilage catabolism, leading to development of OA.34–36 Chemokynes, protease (cathepsin K, metalloproteases, and aggrecanases), growth factors, and pro-inflammatory cytokines (IL-1, IL-6, and TNFα) are increased in the synovial fluid of OA patients.37–41 IL-1 was also shown to induce the expression of a number of MMPs, aggrecanases (ADAMTs, a disintegrin, and a metalloproteinase with thrombospondinmotif) with subsequent degradation of most of the ECM components. 42 This cytokine finally prevents the synthesis of enzyme inhibitors (the tissue inhibitors of MMPs), and markedly reduces the production of type II collagen and aggrecan.9,18–20 How the perturbation of joint homeostasis in OA may affect the clinical outcome in patients affected by degenerative chondral lesions and treated with regenerative procedures still needs to be determined.
Moreover, although it is well known that chemokynes, protease, growth factors, and cytokines are increased in the synovial fluids of OA patients,38–41 it is not sufficiently stressed that many other physiological and pathological conditions may influence the concentrations of these markers. 43 In addition, surgical procedures themselves trigger an inflammatory response that is detrimental to the engineered cartilage. The effect of the joint microenvironment on engineered constructs may be marked during the first days after surgery (Table 2). Increased IL-1 concentration has been documented after joint surgery, and its levels have been found to correlate with the severity of cartilage damage. 42
IL-1β, interleukin 1β; TNF, tumor necrosis factor; bFGF, basic fibroblast growth factor; TIMPs, tissue inhibitor of metalloproteinases; ECM, extracellular matrix; MMPs, matrix metalloproteases.
Schmal measured aggrecan, basic fibroblast growth factor, IGF-I, and IL-1β in the synovial fluid of either healthy patients (IL-1β not detectable) or those affected by chondral lesions undergoing autologous chondrocyte implant (ACI) or microfracturing. 44 IL-1β increased soon after surgery and positively correlated with reactive protein C.
The importance of controlling the joint environment for clinical success following tissue engineering procedures is supported by the finding that cartilage repair outcome with ACI is inversely proportional to the pro-inflammatory cytokine concentration in the synovial fluid at the time of surgery. 44 In the presence of IL-1, MSC differentiation is directed toward the fibroblast phenotype. Transplanted chondrocytes synthesize fibrocartilage, and an increase in catabolic activity and degradation of the ECM is observed in the presence of IL-1. In an inflammatory environment, prostaglandin E2 (PGE2) is released and it promotes chondrocyte apoptosis. In fact, a study by Lima showed that the engineered cartilage subjected to IL-1α at an early culture time does not develop functional mechanical properties even if IL-1α is removed from its culture environment. 33
This implies that even transitory exposure to chemical factors, which may arise from inflammation, might have long-lasting effects on the development of immature tissue within the joint. In addition, cell-based repair of lesions has been recently observed in an inflammatory microenvironment, because IL-1β and TNFα prevent chondroprogenitor cells from differentiation into chondrocytes after injuries or other diseases. In fact, IL-1β and TNFα inhibit the chondrogenic differentiation of human-MSC through nuclear factor kappa B (NF-kB)-dependent pathways. 45
To limit the damaging effect of pro-inflammatory cytokines on the engineered cartilage, it has been proposed that constructs should be implanted when the newly formed tissue is more functionally mature, because the presence of an ECM may protect cells mechanically and from chemical assault.19,33
The potentially negative role of OA and of the inflammatory response after joint surgery or trauma is recognized as an important target mainly in studies that are focused on avoiding post-traumatic OA. It has been suggested that caspase inhibitors, GFs, cytokine inhibitors, anti-inflammatory cytokines, inhibitors of ECM degrading enzymes, and antioxidants avoid impairment of the inflammatory response. 42 These pharmacological treatment options may be adopted to protect the newly formed cartilage and the engineered construct. 37
PEMFs as Strategy for Construct Defence
The rationale for using PEMFs in tissue-engineering techniques for cartilage repair is based on two important findings: (1) the increase in anabolic activity of chondrocytes and cartilage explants exposed to PEMFs and (2) preventing the catabolic effects of inflammation due to OA or surgical trauma and the lesion itself, thanks to the agonistic activity for the A2A adenosine receptor (AR).
In vitro tissue-engineering phase: anabolic effect of PEMFs on chondrocytes and cartilage
Several papers have analyzed the in vitro effects of PEMFs on chondrocytes, synoviocites, and articular cartilage explants (Table 3). Most of these studies have shown that PEMFs affect chondrocytes in several experimental models (monolayers, cartilage explants, and 3D scaffolds), by significantly increasing cell proliferation and synthesis of specific cartilage ECM components, including proteoglycans (PGs) and collagen type II.46–48,53,59,61 PEMFs counteract the IL-1β-triggered cartilage ECM degradation in healthy and osteoarthritic-joint-derived cells.49,50,52,60,62
PEMF, pulsed electromagnetic field; GAGs, glycosaminoglycans; FCS, fetal calf serum; PG, proteoglycans; SMF, static magnetic fields; A2A and A3, adenosine receptors; OA, osteoarthritis.
Moreover, using human cartilage explants, Ongaro showed that PEMFs increase PGs synthesis of the same magnitude as that induced by the IGF-1, the main cartilage anabolic growth factor. Moreover an additive effect of IGF-1 and PEMFs on the metabolic activity of chondrocytes was found. 60
Together, these in vitro data support the active role of PEMFs in the phase of development and manipulation of the construct in culture. In optimal experimental conditions, that is, the controlled in vitro environment in terms of medium, growth factors, oxygen tension, and scaffold characteristics, the application of physical stimuli favors cell proliferation and the cellular colonization of the engineered construct as well as the production and development of the ECM cartilage matrix. Some studies hypothesized the role of biophysical stimulation during cell culture on scaffolds, thus suggesting that the combination of tissue engineering and low-frequency PEMFs might improve cartilage repair techniques.55,61
Surgery phase: effect of PEMFs on the inflammatory microenvironment
It has been shown that PEMFs inhibit the negative effect of the cytokine IL-1β on the production of ECM components in cartilage explants,49,50,52,60 thus we hypothesized that PEMFs stimulation during the implantation phase may prevent the catabolic effects induced by inflammatory molecules on both implanted and host cells, thus protecting the construct in the long term.
Recent data suggest that the IL-1β inhibitory activity on the expression of specific chondrocyte markers, including aggrecan and type II collagen and accumulation of PGs during TGFβ3-induced chondrogenic differentiation of human MSCs, can be counteracted by PEMF exposure (Fig. 2). It is known that synoviocytes largely contribute to the regulation of the joint environment by the secretion of a wide range of pro-inflammatory mediators such as PGE2. 63 Recent studies on synoviocytes show that PEMFs significantly inhibit the release of PGE2 and the proinflammatory cytokines IL-6 and IL-8, while stimulating the release of IL-10, an antinflammatory cytokine.62,64
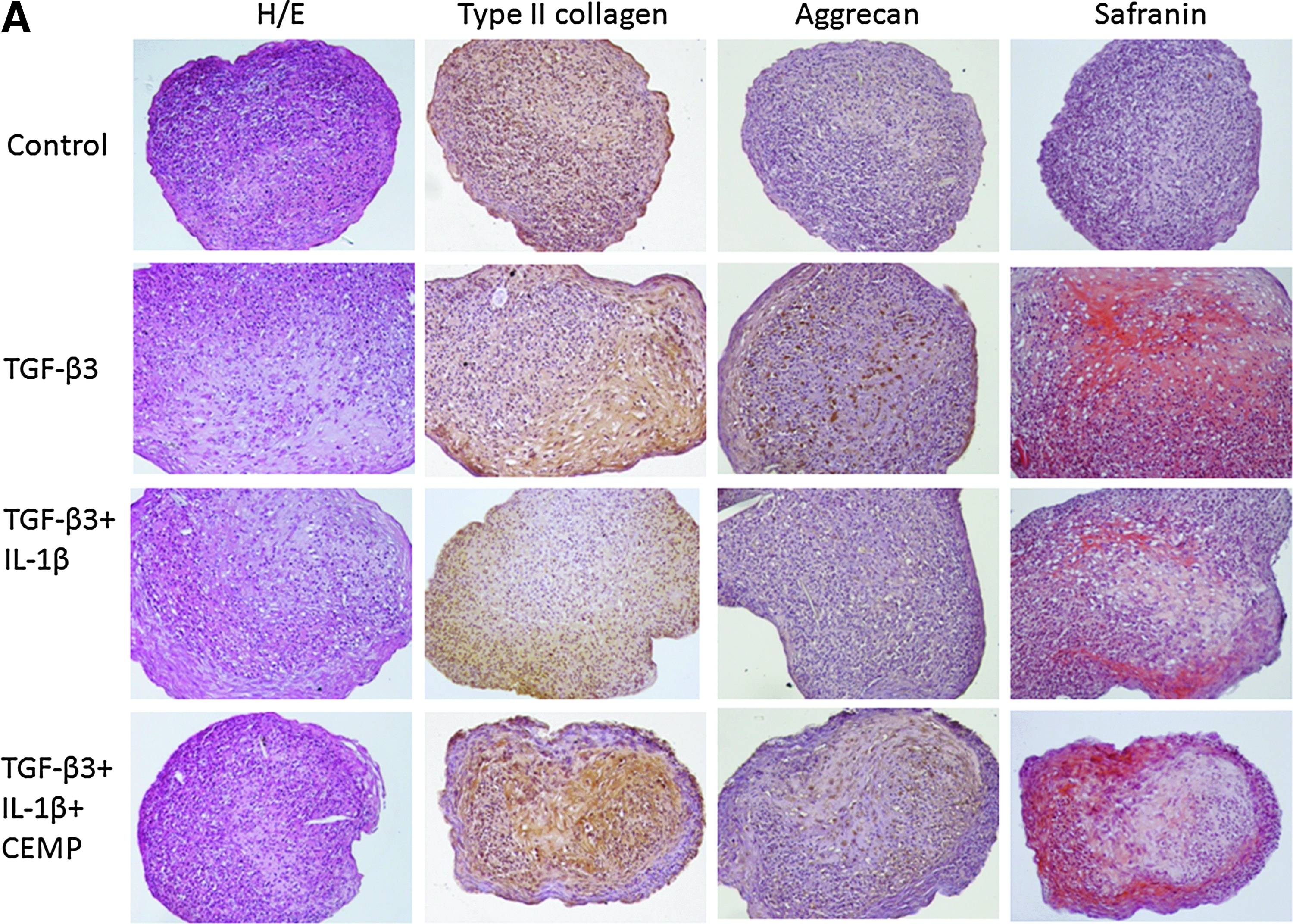
Effects of pulsed electromagnetic field (PEMF) on chondrogenic differentiation of human mesenchymal stem cells cultured in pellets in the presence of interleukin (IL)-1β. Pellets were maintained in culture for 28 days. (
Our hypothesis is that PEMFs also promote the maintenance of ECM, cartilage integrity, and a better integration of the implanted construct with the surrounding tissue. Although to date no in vivo studies reported the PEMF effects on implanted engineered constructs, it has been shown that PEMFs can favor graft integration and prevent its reabsorption in sheep undergoing autologous osteochondral grafts and that this effect is associated with a control of the inflammatory environment, as in the synovial fluid the concentration of IL-1β and TNFα was significantly lower compared with controls. 65
A2A AR up-regulation by PEMFs enhance their anti-inflammatory effects
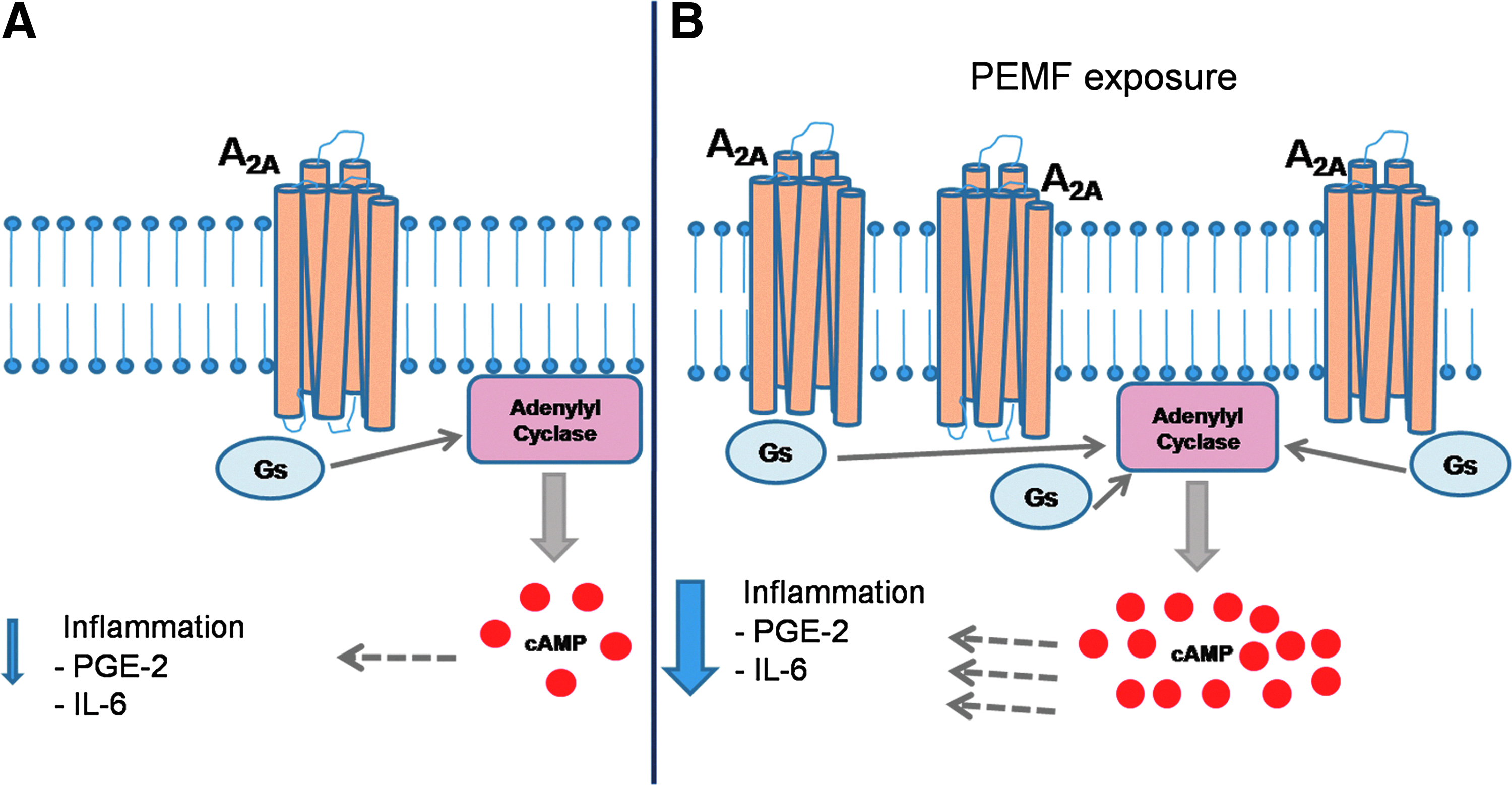
A large body of evidence supports the view that adenosine is constitutively present at low levels outside the cells but increases markedly after metabolic stress conditions such as hypoxia, ischemia, or inflammation.66,67 Adenosine induces different biological effects through the interaction with four receptor subtypes known as A1, A2A, A2B, and A3 ARs which are coupled to different G proteins.68,69 A2A and A2B ARs are linked to the G protein and stimulate the activity of the adenylate cyclase, mediating an increase in cAMP accumulation (Fig. 3). 70 The presence of cAMP mediates a number of various anti-inflammatory pathways, resulting in inhibition of TNFα and IL-1β and ameliorates the symptoms of joint inflammation.70,71 The stimulation of A2AARs inhibits the production of TNFα in human peripheral blood mononuclear cells. 72 The A2AAR pathway is indispensable for holding the balance between the response to infectious agents and protection from an aberrant inflammatory response. 73 Cell signaling pathways initiated by pro-inflammatory events converge on activation of the NF-kB, which promotes cytokine transcription and production. 74 Evidence shows that in different cellular models, including human synoviocytes, A2A or A3AR stimulation mediates the inhibition of NF-kB.70,75,76 In chondrocytes and synoviocytes, NF-kB is a key regulator of COX-2 and MMP expression, and it regulates the expression of a large number of genes in response to infection and inflammation.77,78 It has been postulated that NF-kB signaling plays a central role not only in the pro-inflammatory stress-related responses of chondrocytes to extra- and intra-cellular insults, but also in the control of their differentiation program. In particular, NF-kB influences the accumulation and remodeling of ECM proteins and has indirect positive effects on downstream regulators of terminal chondrocyte differentiation. 79 Since the NF-kB signaling pathway responds to most injurious stimuli that affect cartilage, NF-kB inhibition strategies could become an effective therapy for joint diseases. 80 Adenosine also suppresses the elevated levels of pro-inflammatory cytokines such as TNFα and IL-1β in the most common inflammatory musculoskeletal disease, rheumatoid arthritis.81–83 A2AAR have been pharmacologically characterized and their agonists inhibit cartilage damage when used in the treatment of septic arthritis by diminishing IL-8 expression and reduce rat adjuvant-induced arthritis. 84 In addition, A2AARs are primarily involved in tissue repair and their stimulation accelerated wound healing. 85
Effects of PEMF on A2AARs:
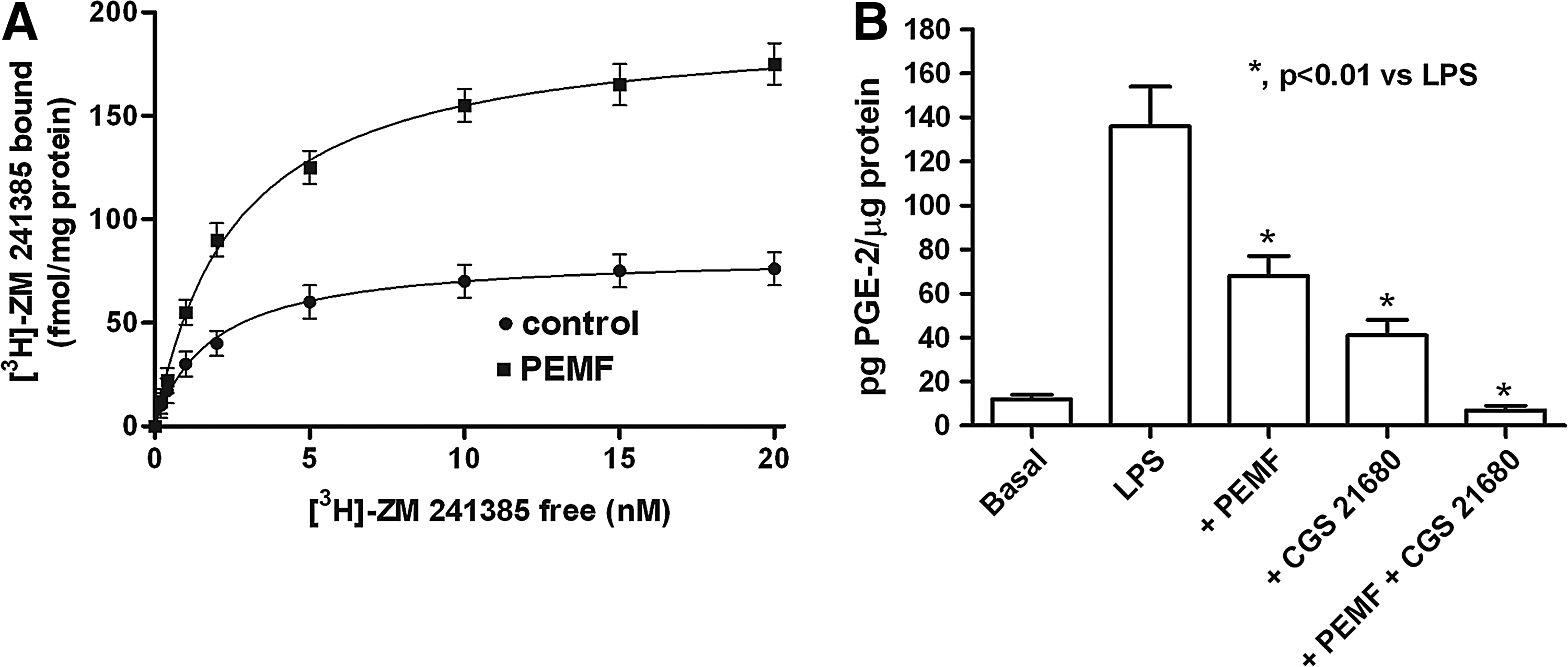
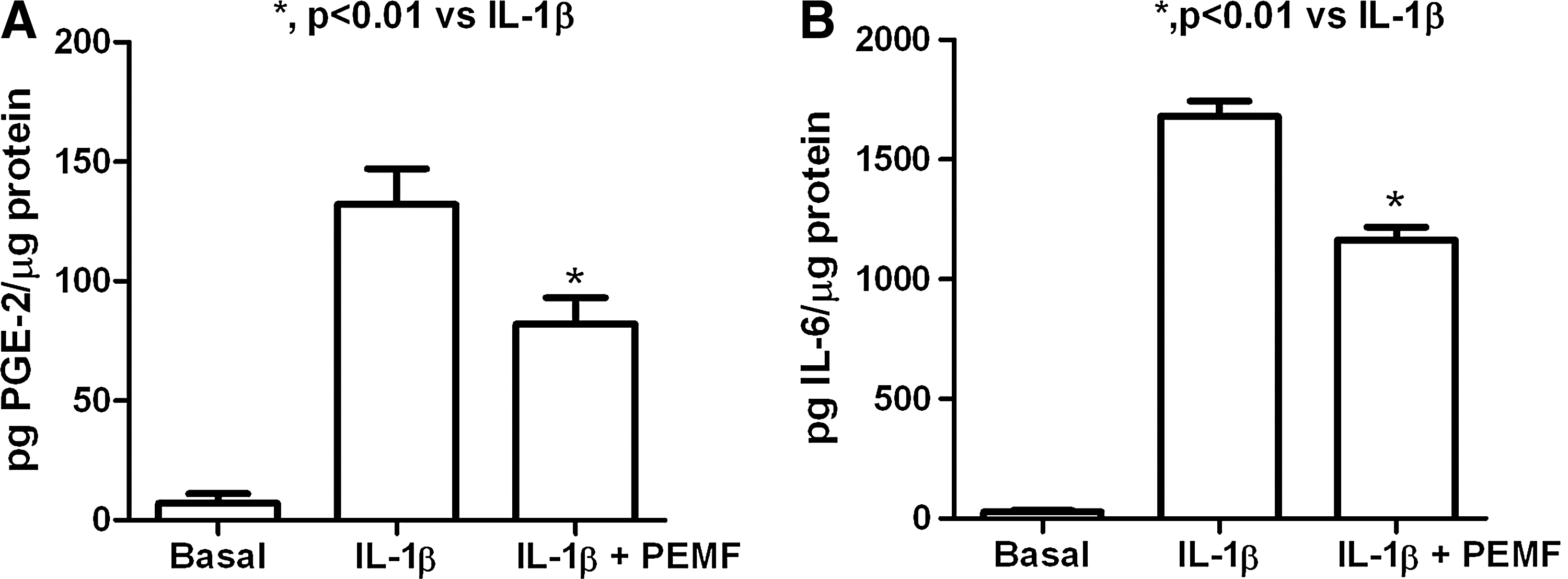
PEMFs may act on cell membrane receptors and may also affect membrane protein distribution.86,87 In vitro studies performed in human neutrophils have strongly suggested that PEMFs cause an alteration of functional responses such as adenylate cyclase activity and superoxide anion production as a result of the up-regulation of ARs located in the neutrophil surface (Fig. 3).88,89 PEMFs, by the involvement of A2AARs, may limit inflammatory activity, as they reduce cyclooxygenase 2 (COX2) expression and PGE2 production in bovine synoviocytes (Fig. 4). 64 These effects could be attributed to the capability of PEMFs to potentiate the activation of A2AARs, which, in turn, inhibit the NF-kB signaling pathway, resulting in decreased synthesis of inflammatory molecules. Interestingly, it has been reported that in bovine chondrocytes and synoviocytes, PEMFs mediated an up-regulation of A2A or A3ARs (Fig. 5). 57 Previous studies show that PEMFs is a viable therapeutic approach that is used to limit cartilage degradation and control inflammation associated to joint diseases, by modulating both chondrocyte and synoviocyte activity and in preclinical OA models, PEMFs are effective in preventing OA development and progression.90–92
Anti-inflammatory effect of PEMF:
Anti-inflammatory effect of PEMF:
Together, these data identify a molecular target for PEMFs, suggesting their potential use as anti-inflammatory agents acting via the up-regulation of A2AARs, thus promoting the anabolic activity of the chondrocytes and the transcription of the TGF-β super family.9,65,91,93–96 These in vitro effects of PEMFs translate in vivo into chondroprotection of cartilage. In sheep undergoing autologous osteochondral grafts, it has been shown that PEMFs favor graft integration and prevents its reabsorption. In the synovial fluid 6 months after surgery, the concentration of TFG-β was significantly higher in treated knees and IL-1 was significantly lower compared with controls. 65
The role of TGF-β is of paramount importance in cartilage healing. TGFβ-1 stimulates collagen II synthesis and counteracts pro-inflammatory cytokine production. 63 Boopalan studied PEMFs on full-thickness articular osteochondral defects in rabbit knees, made in the trochlear groove and filled with calcium phosphate scaffold, which provides the structural support for cells from the marrow to migrate and regenerate. They found that there was complete healing of osteochondral defects in the animals treated with PEMFs. 97
Some authors evaluated the dose-response effect of PEMF (amplitude, frequency, and exposure time) on cells and cartilage explants to identify the optimal exposure conditions to be used subsequently in vivo and in clinical studies. 53 Other research results supported the finding of a strict relationship between the physical characteristics of PEMFs and the response of the exposed biological system, thus explaining the lack of effects reported in some studies.58,91
On the basis of these considerations, physical stimuli may be useful in promoting the formation of the new cartilage in the engineered construct during its preparation in vitro, to protect the construct when surgically implanted in an inflammatory environment and to favor the its integration with the surrounding host tissue.
Clinical studies
Zorzi in a prospective, randomized double-blind study that evaluated the effect of PEMFs after arthroscopic treatment of cartilage lesions in the knee. 98 They hypothesized that patients might benefit from PEMFs, thus leading to early inflammation control and a return to normal activity. 98 Indeed, the outcome for patients in the active group was more favorable than for those in the control one in terms of pain, NSAIDs assumption, and function even at 3 years of follow-up. On the basis of the preclinical knowledge, they concluded that the PEMFs was able to effectively control inflammation, ultimately resulting in chondroprotection. In another study, Benazzo showed that PEMFs reduced the recovery time of patients undergoing anterior cruciate ligament reconstruction and allowed an early return to sport activity. 99 Another clinical study showed that PEMFs can favor clinical recovery in patients undergoing ACI. Patients were treated for 60 days; the treated group showed better performance in daily and sports activity (85% vs. 33%) at 2 years of follow-up compared with the untreated control group. 100
Overall, the clinical studies collected show that PEMFs results in early resolution of joint inflammation (short-term effects) and maintenance of the results at 2–3 years of follow-up (long-term results). Furthermore, it is noteworthy that the coils generating the magnetic field are designed to allow the contemporary exposure of all joint structures: the whole cartilage extension and thickness, the subchondral bone, and the synovia. The short-term effect can be explained by the anti-inflammatory effect of PEMFs consequent to the activation of the A2AARs. To explain long-term effects, we hypothesized that early control of inflammatory events may prevent the catabolic effect of pro-inflammatory cytokines on whole joint articular cartilage, resulting in its preservation. Furthermore, the anabolic effect on chondrocytes resulting in an increase of PG synthesis may preserve the mechanical competence of the cartilage.
Discussion and Conclusions
The importance of the different techniques for regenerative medicine is well recognized. Nevertheless, the clinical results of tissue engineering for cartilage repair are extremely variable and sometimes conflicting. 95 Harris found that the current body of knowledge does not allow us to conclude that there is any difference between ACI and osteochondral autograft transplantation. 100 It was also reported that “there are patient-specific and defect-specific factors that do influence clinical outcome after ACI.” 101
Several authors underline the need to improve the quality of the repair tissue after treatment of cartilage defects. Numerous conditions may jeopardize the success of a procedure, and they are often difficult to control; nevertheless, local inflammation is probably the most detrimental condition in tissue engineering. Therefore, the local microenvironment of the treated joint should be considered the most important variable that affects the success of regenerative therapy; it has a strong impact on in situ degradation, the survival of cartilage-engineered constructs, and the success of local repair activity. Controlling the microenvironment is also important for cartilage in situ regeneration by marrow stimulation after subchondral bone perforation or for chondrogenic differentiation of MSC. 23 The surgical procedure required to implant the engineered cartilage triggers an inflammatory response, which represents a potentially harmful event for the articular cartilage and the engineered construct, which may ultimately jeopardize the positive effects expected by regenerative medicine.
Research results and available clinical studies suggest that PEMFs can play a fundamental role in the success of tissue engineering, and the road map to FTE should foresee the use of PEMFs after construct implantation to protect against the catabolic effect of inflammatory cytokines and to stimulate the anabolic action of both transplanted and host cells.
Footnotes
Acknowledgments
The research was partially supported by Regione Emilia Romagna, Project POR-FERS “Nuovo dispositivo per il trattamento di lesioni cartilaginee,” and Rizzoli Orthopedic Institute. This grant partially financed the in vitro and in vivo tests reported in the article. Some of the reported studies have been performed by the authors in cooperation with IGEA (Carpi, Italy).
Disclosure Statement
No competing financial interests exist.