
Abstract
The biological interface between an orthopedic implant and the surrounding host tissue may have a dramatic effect upon clinical outcome. Desired effects include bony ingrowth (osseointegration), stimulation of osteogenesis (osteoinduction), increased vascularization, and improved mechanical stability. Implant loosening, fibrous encapsulation, corrosion, infection, and inflammation, as well as physical mismatch may have deleterious clinical effects. This is particularly true of implants used in the reconstruction of load-bearing synovial joints such as the knee, hip, and the shoulder. The surfaces of orthopedic implants have evolved from solid-smooth to roughened-coarse and most recently, to porous in an effort to create a three-dimensional architecture for bone apposition and osseointegration. Total joint surgeries are increasingly performed in younger individuals with a longer life expectancy, and therefore, the postimplantation lifespan of devices must increase commensurately. This review discusses advancements in biomaterials science and cell-based therapies that may further improve orthopedic success rates. We focus on material and biological properties of orthopedic implants fabricated from porous metal and highlight some relevant developments in stem-cell research. We posit that the ideal primary and revision orthopedic load-bearing metal implants are highly porous and may be chemically modified to induce stem cell growth and osteogenic differentiation, while minimizing inflammation and infection. We conclude that integration of new biological, chemical, and mechanical methods is likely to yield more effective strategies to control and modify the implant–bone interface and thereby improve long-term clinical outcomes.
Introduction
B
By physically or chemically modifying, and/or biologically enhancing highly porous metal implants, it may be possible to overcome the problem of fixing metal implants to deficient bone substrates. However, engineers are forced to work within certain constraints imposed by the behavioral properties of each metal. For example, galvanic corrosion results from the contact between two dissimilar metals, a process that should be carefully avoided within the context of orthopedic surgery. Major bone defects, resulting from acute traumatic injury, chronic disease, tumor resection, infection, or prior implant failure can present significant challenges to orthopedic surgeons. This is particularly true when affected areas are adjacent to one of the major load-bearing joints of the knee, hip, and shoulder. Examples of current strategies for repairing bone defects include autografts, allografts, synthetic implants, and cell-based therapies (Table 1). Each of these strategies, however, has potential drawbacks. Autografts can result in donor morbidity 6 such as pain, fracture, infection, and neurovascular injury. 7 Second, allograft supplies are limited, expensive, difficult to store, unaccepted by some cultures, and have the added risk of possible disease transmission from donor to recipient. 8 Synthetic implant materials, such as ceramics, metals, polymers, and gels have wide application in dentistry and orthopedics. 9 Yet the apparent advantages of some materials observed in laboratory settings do not necessarily predict their clinical performance, as they may not always incorporate into host tissues due to a variety of factors: lack of fixation, infection, mechanical failure, poor biocompatibility, or undesirable local reactions by the normal host tissue to the implant or implant material.10–12 Alternatively, cell-based orthopedic therapies are currently being tested in numerous animal models 13 and early stage clinical trials14,15 with varied but sometimes conclusive results. 16 Critical bone defects that fail to heal can significantly reduce the quality of life for patients and increase burden on the health care system, therefore, additional strategies and investigations are promptly necessary to improve clinical orthopedic practice.
Highly porous metals, with over 65% interconnected porosity by volume, may be fabricated from a variety of elements including Tantalum (Ta), Titanium (Ti), Titanium Alloy (Ti6Al4V), and numerous other metals used to make alloys. High percentages of interconnected void spaces are important for osseointegration and perfusion, and these materials have been used with considerable clinical success as an adjuvant treatment for implant fixation and bone defect management.5,17–24 Still, recent technological innovations in the fields of molecular biology, biochemistry, and biophysics provide numerous options for potentially increasing localized osseointegration and promoting both the rate and extent of bone regeneration. For example, injections of either bone marrow-derived mesenchymal stem cells or adipose-derived mesenchymal stem cells (AMSCs) are currently being used to treat osteoarthritis, 25 meniscus injury, 15 and avascular necrosis of the femoral head, 26 to name a few. It remains to be seen whether critical bone defects can be improved by implant manipulations that drive osteoblast lineage commitment, proliferation, and ultimately bone repair with functional joint restoration outcomes.
Foremost among the challenges of applying stem cell-based strategies to bone defect repair are assessing whether cells are efficacious in their ability to adhere and behave in ways that improve bone restoration and joint functionality. Although cellular adhesion to synthetic implants has been demonstrated for various scaffolds in vitro,27–40 the exact fate of seeded cells remains to be quantitatively characterized. Additionally, it is unclear if, or how many stem cells remain in the original delivery site and, therefore, what the optimal dose of cells might be.27–40 Cell behavior and disease state are likely coupled throughout the course of disease progression, but this relationship may not be linear or easily disentangled in vivo. Recently developed techniques for detailed data collection on secretomes should help to unravel this enigmatic theme. Furthermore, responses to cell-based therapies are likely patient specific and may be related to numerous factors such as age or medical history.41–43 Indeed, this variability serves as the foundation for individualized regenerative medicine. Due to their novelty, the long-term effects of stem-cell based approaches to enhance bone defect repair and implant fixation will remain elusive without focused research in this area.
Although the concept of designing and implementing biological implant materials is not new, recent advances in molecular genetics should allow for improved investigation and more thorough evaluation of several key questions regarding their use. In this study, we compare selected porous metal materials available for the repair of critical bone defects. The elastic modulus of each material, in reference to cortical and cancellous bone, is discussed within the context of clinical success. Although we recognize the extensive use of these materials in other fields, such as dentistry, we focus on their application in repairing large bone defects in orthopedic surgical procedures. Thus, exciting developments in stem cell-based therapies with potential utility in orthopedic application are highlighted, along with a discussion of prior attempts at biologically enhancing orthopedic implant performance by combining stem cell therapies and porous metal technologies. Future research should be directed at combining cell-seeded implant designs with biochemical and biophysical conditioning techniques that bolster positive biological effects and minimize undesirable outcomes.
Porous Metal Materials
Various solid, porous-coated, and highly porous metals have been tested in skeletal repair models (Table 2), and all have unique advantages and potential disadvantages. Solid metals such as stainless steel, for example, were the only materials used in early orthopedic surgeries, and despite low costs of manufacture, 44 they were less congruent with host bone than many subsequent metal materials. Importantly, solid stainless steel implants depend on some form of mechanical fixation through cement, screw, pin, or peg, 44 and thus do not provide for bone tissue attachment or osseointegration into the implant surface. By comparison, cobalt–chromium alloys (CoCr) are stronger than stainless steel, 45 and can undergo surface treatment by sintering of beads to create a porous surface for osseointegration. This CoCr alloy has a high modulus of elasticity, and is therefore stiff in comparison to host tissues. In fact, the composition of alloys exhibit remarkable variation in currently used metal-based implants. For example, Ti-based implants can range from commercially pure to ∼70% by total volume (Table 2).
Most recently, porous-surfaced and highly porous implant fabrications have gained widespread popularity due to increased clinical success when used for hip and knee arthroplasty.22,23,46 As fabrication methods improve, pore parameters such as size, density, and geometry are increasingly regulated and modified with greater precision and accuracy. 20 This has led to experimental comparisons specifically designed to optimize the parameters of implants used in critical bone defect repair. While a wide range of materials and manufacturing methods are available for the fabrication of such devices, Ti-based implants constitute the vast majority of uncemented arthroplasty implants in the United States. They are now considered to be a central component of many of the most effective devices for increasing the mechanical integrity of the bone to implant interface and joint functionality. 47
Cobalt–chromium
Historically, orthopedic implants were mostly made out of CoCr alloys consisting of cobalt, chromium, molybdenum, and nickel. Currently, CoCr is used in cemented procedures such as in the femoral stem of hip devices, and the femoral component of total knee devices. As a means to improve osseointegration, these alloy implants can be coated with materials that provide a porous surface, such as sintered beads, which augments their surface–tissue interface. These surface treatments improve implant osseointegration and increase survival rate, as a long-term clinical study demonstrated a survival rate of >97% at 20 years. 48 Similarly, CoCr alloys can be coated with materials, such as porous Titanium–Niobium, to increase porous complexity; a technique with numerous applications, including customized instrumentation. 49
Magnesium
Magnesium ions are naturally occurring within the human body and critical to many cellular functions, such as activating adenosine triphosphate and synthesizing DNA and RNA. 50 Certain characteristics of Mg make it particularly well-suited to applications that require malleable implant devices, or a material that is absorbed by the body over time. Due to its higher malleability relative to Ti, for example, Mg implants (and alloys) have mostly been used in pediatric orthopedics, maxillofacial reconstruction, 51 and devices for the internal fixation of fractures, although not always with favorable results. 52 Altogether, the use of Mg in orthopedic implants requires careful consideration; disruption of the Mg homeostasis could have severe consequences leading to diminished implant functionality or failure, particularly near the surface–implant interface. Compared to other metal implant materials, Mg is highly corrosive, absorbable, and less rigid (Young's elastic modulus=41–45 GPa; Table 2). 53 Also, because Mg is less dense and has lower fracture toughness, it is not amenable to increases in porosity, which may limit its potential for osseointegration with host tissue. These concerns led to variable interest in this material over time, especially as an alloying element in combination with other metals such as aluminum, calcium, manganese, zinc, zirconium, and rare earth elements. 50 Most importantly, alloying has been shown to improve the biocompatibility and corrosion resistance of Mg.50,52 For instance, Gadolinium has been considered as an appropriate alloying element for Mg-based implant materials because of improvements in strength, corrosion behavior, and adjustability of mechanical properties. 54 Compared to Ti and Ta, Mg is rarely used in the fabrication of devices that are used to reconstruct major load-bearing joints, yet the potential for this material to be improved upon is compelling given proper focused research and preclinical trials. 54
Titanium
With the highest strength–weight ratio of any metal, Ti has the advantage of remaining light and strong when fabricated. 55 Additionally, this element is abundant and widely distributed in natural mineral deposits (ilmenite and rutile) making it more accessible than rare elements. A fortiori, corrosion resistance, low electrical and thermal conductivity, high tensile strength, and low modulus of elasticity (Young's elastic modulus=2.6–110 GPa; Table 2) make Ti a common choice for heavy load-bearing orthopedic implant devices.56–58 Commercially pure Ti (cp-Ti) is either used alone, or is alloyed with other metals (e.g., Aluminum, Niobium, Iron, Molybdenum, Zirconium, and Ta; Table 2). The most common of the Ti alloys is Ti6Al4V (Titanium; 6% Aluminum; 4% Vanadium) (Fig. 1 and Table 2), but many other mixtures have been used to match the elastic modulus between cortical bone and implant. 45 An extreme example of alloying, Nitinol, is made from equal proportions of nickel and Ti to create a highly elastic material (Young's elastic modulus for Nitinol=48 GPa; Table 2) that can also be fabricated to have 70% porosity. 33 Although Nitinol is difficult to make and can be locally toxic if nickel debris is released, 33 it has been used with success in some procedures, such as intervertebral disc fusions. 59
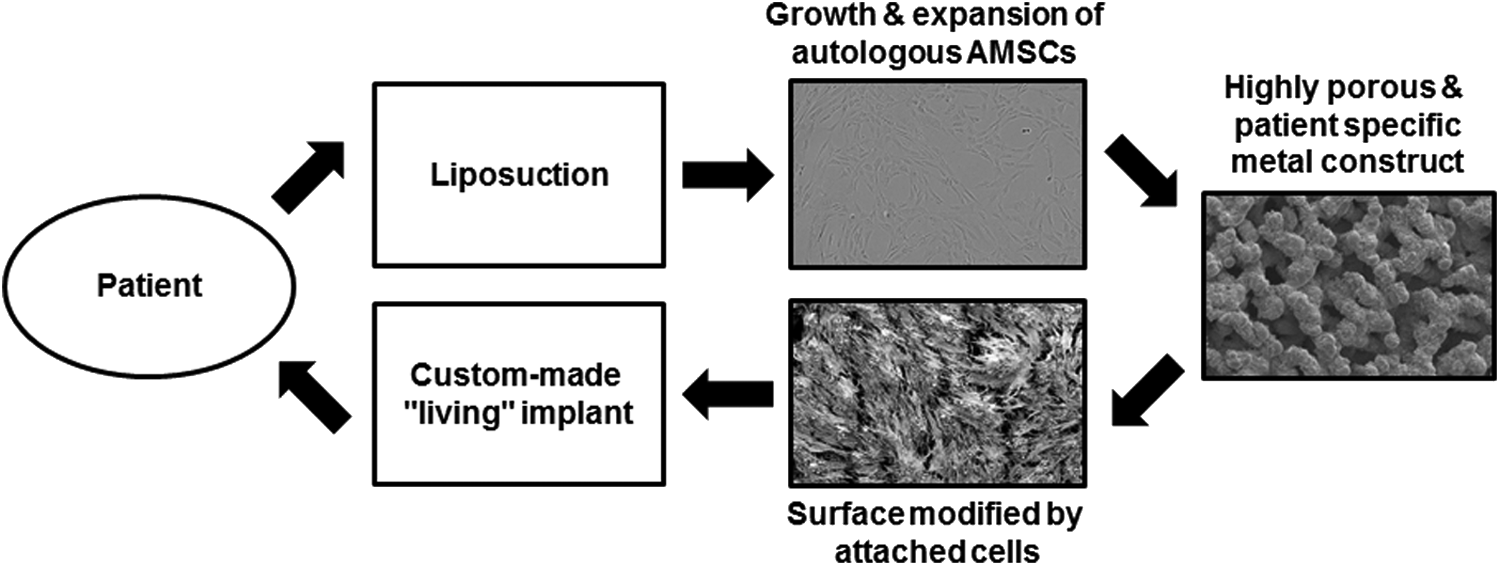
Conceptual schematic of biological enhancement of orthopedic implants: adipose-derived mesenchymal stem/stromal cells (AMSCs) are obtained from a patient using liposuction; AMSCs are cultured and expanded in platelet lysate-based culture medium; cells are seeded onto a highly porous metal implant (Ti6A14V pictured here) designed to match the patient's anatomy; cells are grown to create a modified implant surface; implant is inserted into the patient.
As the principal component of numerous alloys, the strength and weight properties of Ti make it particularly well suited for progressive orthopedic implant design. Structurally complex devices such as cutting blocks and guides can be customized to match patient-specific anatomy and bone defects, although it is unclear whether patient-specific instruments are better than traditional methods and devices. 60 Remarkably, Ti implants can be made to withstand extreme loading scenarios that are much higher than average, such as in the case of obese patients that require a total joint replacement.61,62 Such Ti-based materials are not just used to make primary implant structures, but also have utility as adjunct surface preparations or coatings. For example, Ti wire mesh can be applied to a solid substrate (Ti or otherwise) to increase surface rugosity and potentially promote local osseointegration, a method long known to improve implant fixation. 63 Similarly, beads made out of Ti can be sintered onto a solid substrate of the same material to accomplish the same goal of increased osseointegration. Secondary surface modification, such as grit blasting 64 has also proven useful for ongoing product development.
Tantalum
Tantalum has a high melting point (the highest of any metal; 3017°C), and high corrosion resistance due to a protective oxide surface layer. 65 Unlike Ti, Ta is highly conductive of heat and electricity, and is relatively rare, found primarily in tantalite, and columbite, 66 and to a lesser extent coltan. Although Ta has been shown to have high biocompatibility in animals3,4,10 and humans, 2 it is costly to mine and manufacture, making it one of the most expensive of the commonly used orthopedic materials. 67 In response to this factor, researchers and manufacturers have attempted to reduce the cost of fabrication without losing the added benefit of high biocompatibility by creating vapor deposits of the material on scaffolds or by coating portions of solid Ti or CrCo implants with Ta. 65 The balance between material integrity (Young's elastic modulus=3 GPa; 68 Table 2), desirable clinical results, and offsetting costs of manufacture, has led to creative derivatives of Ta implant design. Similar to porous Ti, porous Ta devices are often structurally complex and increasingly patient-specific. Metaphyseal cones, for example, are largely asymmetrical. 69 Additionally, long-term bone ingrowth (osseointegration) has been demonstrated in both the acetabular and femoral components of porous tantalum hip devices. 22 One limitation of highly porous Ta is that thinner structures are more difficult to manufacture in such a way that ensures continuity and precision over all parameters, particularly those that prevent the material from fracturing. 70 A recent and extensive review 46 considered more than 2000 revision total hip procedures that used highly porous Ta components and revealed good short-term fixation (∼3.6 years), thereby demonstrating a highly successful application of Ta for orthopedic implants.
Metal Implant Fabrication and Modification
Biomaterials science is an innovative and multidisciplinary enterprise that continues to evolve in response to clinical demands and efforts directed at treating specific diseases. Hybrid biomaterials, comprised of both metal and nonmetal materials, are currently useful for obtaining the benefits of each material, for example, metals that are still strong when combined with polymers that are resorbable.71,72 Innovative metal materials, and more specifically, highly porous metals are the focus of this section.
A number of biological, chemical, and physical engineering techniques have been developed to generate metallic implants and enhance their osseointegration potential. 73 Prototypes and custom-made devices are typically created by solid free-form machining and fabrication, whereas implants for routine clinical use are often forged or molded. Additional state-of-the-art approaches include additive manufacturing methods, such as laser-engineered net shaping,40,65,74 stereolithography, and numerous sintering strategies.75,76 These techniques are complemented by temperature-assisted implant manufacturing methods that use phase separation, heat sintering, and fused deposition molding. 77 Other interesting methods for developing the ideal metal surface have emerged, including using a space holder with the addition of powdered metal to make metal–foam scaffolds. 78 For example, the use of metal foams has been studied for use in intervertebral spine implants. 79
A combination of methods can also be used to achieve an optimal material for a certain application. For instance, porous Ti made using selective laser melting can be chemically (NaOH, HCl) and physically treated (heat) to produce a Ti oxide layer leading to a porous apatite formation, which has been tested favorably for bone ingrowth in rabbit femurs. 80 Another remarkable example is the creation of a porous Ti scaffold using a polymeric sponge that is immersed in TiH2 slurry and coated with sol–gel to create a material that has high biocompatibility and versatility, 81 two features often needed to customize implants. In the midst of the new material production technology, more effective strategies for generating custom-made devices by integrating patient-specific spatial information have also become the focus of greater technological input, for example, computer-aided designs. These technological advances have proven effective in some procedures such as total knee arthroplasty, 82 but their superiority over traditional approaches remains to be seen.83,84
Recently, biological manipulation of the device surface has gained traction and involves infusion of proteins, such as growth factors,85–87 and small molecules like bisphosphonates, 88 mesenchymal progenitor cells,28,33,35,37,51,89 and electromechanical stimulation of the implant interface.30,90 Engineering methods will continue to advance alongside conceptual evolution regarding metal implant physics, surface biochemistry, and the biology of implant osseointegration.
Factors that affect cellular health are known to influence osseointegration and should be carefully considered when designing porous metal orthopedic implants. First, porosity is measured as a percentage and, in part, determines the resulting strength and density of the bulk material. Depending on the percentage of porosity and porous construct geometry, the surface area available to cell adhesion is considerably influenced, as is the potential for vascularization and perfusion. 91 Second, pore sizes (macro-, micro-, and nanoscale) determine which cells and tissues will penetrate the material (Fig. 1). For example, fibrous tissue grows into pore sizes of 10–75 μm; unmineralized osteoid tissue grows into pores 75–100 μm; mineralized bone tissue penetrates pores ∼100 μm; and optimal bone infiltration/osseointegration occurs in pores sized between 150 and 500 μm. 92 Third, the pore interconnectivity (open vs. closed cell) can greatly influence the potential for osseointegration into an implant because the depth of tissue integration and perfusion of nutrients and oxygen throughout the ingrown tissue can become restricted when cell channels are sequestered or closed.9,93 Understanding pore parameters is of utmost importance to the design, utilization, chemistry, and biology of osseointegration into porous-coated and highly porous orthopedic implant devices.
Naturally, the pattern and degree of interconnected porosity within a material or implant surface will influence the geometry and extent of ingrown tissue. In addition, patient characteristics such as age, disease, bone quality, blood supply, bone health, and surgical technique can all influence tissue osseointegration type (fibrous vs. bone), rate, and extent, making it difficult to disentangle the potential reasons for clinical success or failure of an implant. Improving osseointegration of a porous-coated solid metal implant requires targeted, specific modification of the surface interface, and this can be achieved through physical, chemical, and/or biological treatments.
Biomedical Strategies to Improve Osseointegration and Osteoinduction
One key objective of current orthopedic repair strategies is to improve the microenvironment of metallic implants by enhancing osteoconduction, which is loosely defined as passive bone repair on a biomaterial surface support, by promoting osseointegration and osteoinduction. A number of studies have examined the natural course of implant receptivity, and survivorship rates greater than 95% have been reported, for example, with acetabular cup implantations after revision total hip procedures. 46 However, revision surgery is necessary in some of these cases where implant integration is perturbed through, for example, infection and/or osteolysis. Osseointegration can be achieved by improving the continuum between the implant surface and host bone, by creating a favorable microenvironment where cells (committed to the osteogenic lineage) are capable of proliferating and executing bone anabolic responses through production of a bone-specific extracellular matrix and maintaining a homeostatic balance with bone-resorbing osteoclasts. 94 Biological enhancement strategies include cell seeding, while chemical and physical treatments can be used to indirectly increase the likelihood of osteoblast proliferation, differentiation, lineage commitment, and engraftment of seeded cells. Exciting possibilities exist for combining these strategies, and physical and chemical methods should in principle be useful for preconditioning cells before biological enhancement by cell seeding.
Biological implant modification
The potential exists to enhance osseointegration of prosthetic implants by modifying the biologic modulus at the implant interface with osteoblast-like progenitor cells that are capable of self-renewal and can be experimentally directed into an osteoblast lineage in vitro. 10 Human cells that have been used to seed porous metal implants vary in terms of their differentiation potential: embryonic stem cells, 29 fetal osteoblasts,30,74 mesenchymal precursors such as adipose tissue-, bone marrow-, or dental pulp-derived cells27,28,95–99 have high differentiation potential, whereas mature osteoblasts are fully committed to the osteogenic lineage (Table 3). Such cells have been used for seeding experiments primarily dealing with porous Ti and Ta, and various chemical and physical modifications have been applied to each material (Table 2). Thus far, in vitro experiments designed to seed cells onto porous metal scaffolds have not only demonstrated good adhesion,51,52 but also showed osteogenic differentiation,10,53 proliferation,54,55 and mineralized matrix formation.27,56 Other studies were inconclusive or failed to detect a change in cell behavior or gene expression after seeding 29 (Table 3). Nevertheless, most studies have presented results on a limited number of genes, which should improve with the advent of less costly sequencing technologies.
These exciting discoveries have led to increased interest in animal models and human clinical trials. For example, preliminary data from an osteochondral defect model in sheep demonstrated increased osseointegration (and cartilage regeneration) of porous Ti metal scaffolds seeded with mesenchymal stem cells when compared to those without cells. 98 Similarly, the use of porous Ti seeded with bone marrow-derived stem cells (BMSCs) increased new bone formation and improved the recovery of bone gap defects in mule sheep. 100 In humans, mesenchymal stem/stromal cells (MSCs) have promising potential in orthopedic surgery and ancillary treatments. 101 Not surprisingly, most studies regarding the use of MSCs to induce implant osseointegration have focused on the variability of their effectiveness. Some of the factors considered were cell type, anatomic location of cell harvest, gender, body mass index, and age class. Rider et al., 102 for example, compared BMSCs and AMSCs from six donors and found negligible differences in proliferation and differentiation potential. Jaager et al., 103 while examining adipose tissue-derived stromal cells from seven patients, found donor variability regarding lineage-specific gene expression values for the following: peroxisome proliferator-activated receptor gamma, fatty acid binding protein 4, runt-related transcription factor 2, alkaline phosphatase, sex determining region Y-box 9, and aggrecan, although the dataset did not exhaustively examine cell-specific biomarkers.
Additional studies support the notion that some factors may strongly influence the success of cell seeding experimentation: AMSCs from five anatomic locations (superficial abdomen, deep abdomen, thigh, arm, trochanter) from female patients across three age groups were tested, and revealed that cells collected from the superficial abdomen are more resistant to apoptosis.104,105 These and other studies have also shown that cell viability, proliferation capacity, and differentiation potential is higher in younger than older patients. 106 Moreover, although cells from low and high BMI donors appear to differentiate equally well, cells from high BMI donors have reduced proliferation and lower osteoinduction potential. 107 Aside from variability at the individual level, it also remains to be seen whether the short-term benefits of cell seeding will persist in long-term scenarios with increased physical demands upon a high load-bearing environment found within a total joint replacement, particularly hip or knee. Experimental recapitulation of natural events that lead to osteogenesis is lacking, as the biological processes involved need to be better understood and documented. 108 Similarly, the combination of coating porous metal implants with various biological coatings, such as hydrogel 34 or silk protein, 109 and cell seeding should continue to be an area of considerable interest. Preliminary results warrant further exploration of biological enhancement by cell seeding and the potential consequences for cells already residing within the troublesome joint space.
Chemical implant modification
Modulating the microenvironment
Numerous chemical strategies have been employed as a pretreatment in preparation for the permanent adherence of another material, or treatment of orthopedic implants toward the central goal of improving osseointegration, and by extension, biological fixation. 110 Considering the cell microenvironment, multiple extracellular ligands and osteogenic factors stimulate osteogenesis during normal skeletal development and bone homeostasis, including: bone morphogenic proteins, parathyroid hormones, wingless related integration sites, 60 transforming growth factor-β, insulin-like growth factors, fibroblast growth factors, 61 as well as the glucocorticoid dexamethasone. 62 Of particular interest is the potential for locally administering drugs using a porous metal implant as the delivery vehicle. For example, Clark et al. 111 devised a method for controlling the release of transforming growth factor-β from porous metal implants and demonstrated improved bone osseointegration and bone-to-implant contact in a rabbit model. Additional agents that support maturation of the bone extracellular matrix are ascorbic acid and β-glycerophosphate. 63 During fracture repair, there are additional contributions of inflammatory factors such as tumor necrosis factor alpha, platelet-derived growth factor, as well as various interleukins. 8 Furthermore, in vivo and ex vivo experiments have both demonstrated the potential utility of such reagents for producing osteoid tissue. 64 As a logical next step, osseointegration should, in principle, be improved by leveraging the osteogenic activities of bone stimulatory factors and attenuating inflammatory responses, especially if mechanisms for timed local delivery of these agents can be worked out.
Modifying the implant surface
Acidic, basic, or oxidative treatments such as acid and alkaline treatments, fluoride, hydrogen peroxide, anodization, and ion implantation can be used to achieve roughened surfaces that promote osseointegration. 45 Acid–alkali treatments tend to reduce the mechanical strength of porous metals, whereas the reverse treatment of alkali–acid does not. 112 In addition, coating materials such as hydroxyapatite, tricalcium phosphate, bioglass, calcium phosphate or bone morphogenic protein-infused calcium phosphate, 85 polyglycolic acid, polylactic acid, and sol–gel are applied (usually after a pretreatment) by techniques best suited to the permanent attachment of each coating (Table 3). Other strategies include painted materials, anodizing agents, or plating constituents, all designed to improve the surface–implant interface, which primarily means reducing the potential for corrosion and bacterial adhesion, while increasing the likelihood of osseointegration. In general, these coatings need to be more reactive than the coated material, otherwise corrosion potential increases.47,109,113 Besides coating, the filling of pores of the implant material with a peptide amphiphile nanofiber matrix has been shown to increase the formation of new bone. 71 Clearly, the potential methods for chemical modification of orthopedic implants are still highly unexplored both in terms of improving the cell microenvironment and the implant surface itself, yet the continued convergence of biophysics, biochemistry, and molecular biology is likely to yield exciting discoveries that will improve the success rate of reconstructive orthopedic joint surgeries.
Physical strategies to improve the implant environment
Highly porous scaffolds tend to have higher osteoinductive and osteogenic potential, making them desirable for the repair of large bone defects compared with ceramic materials, for example, which are more osteoconductive and permit vascularization to support bone growth (e.g., in dental applications; see Holzapfel et al. 9 ). One way to physically improve the overall osseointegration is to increase the implant's surface roughness at multiple spatial scales (macro-, micro-, and nanometer 45 ; Fig. 1). Previous studies suggest an optimal surface roughness for hard tissue osseointegration 92 ; however, there exists a tradeoff between promoting osseointegration and preventing bacterial attachment. Curiously, these tradeoffs have not been thoroughly examined regarding pore size, or material-specific constraints that would promote a more desirable outcome.73,114 Aside from the challenge of infectious bacterial attachment to implant surfaces, considerable morphological manipulations, such as grit blasting with aluminum, Ti, or calcium phosphate, are thought to increase implant surface roughness and osseointegration. 115
Low-intensity pulsed ultrasound
In addition to surface blasting methods of physical modification to orthopedic implant surfaces, several minimally invasive postoperative stimulatory methods of enhancing osseointegration have been tested for clinical use: low-intensity pulsed ultrasound (LIPUS), extracorporeal shockwave therapy (ESWT), and electricity, such as pulsed electromagnetic fields (PEMF). Minimally invasive postoperative methods for physically improving osseointegration are attractive and altogether promising. At the root of these initiatives is the theoretical tenet (aka. Wolff's Law) that bones require mechanical stimulation for proper development (embryogenesis), osteogenesis, and homeostasis. 116 Therefore, application of a mechanical force should, at least theoretically, enhance osseointegration of a metal implant. One such mechanical force: LIPUS, is well known to improve bone fracture healing time, 117 and has recently been shown to promote osteogenic differentiation of mesenchymal progenitor cells. 118 Furthermore, porous-coated implants have been treated with LIPUS in dogs, which positively influenced bone osseointegration over both short (2–3 weeks; Tanzer et al. 119 ) and long (6 weeks; Tanzer et al. 120 ) time courses. A better understanding of the mechanisms responsible for improved fracture healing and osteogenic differentiation will be necessary to fully incorporate LIPUS as an adjuvant therapy for joint reconstructions with porous metal implants. Similar to LIPUS, ESWT has been the subject of experimentation regarding its potential efficacy toward enhancing bone growth.
Extracorporeal shockwave therapy
Lithotripsy is primarily used by nephrologists to ablate kidney stones, but this technology also has applications in orthopedics. Specifically, ESWT is used to treat plantar fasciitis, 121 and nonunions, 122 but may or may not be useful for treating a myriad of other orthopedic complications.123–125 Several key questions remain unanswered regarding the use of ESWT. For example, a consensus on the most favorable type of shockwave (focused or unfocused) is not clearly agreed upon, 126 nor is it well understood which orthopedic applications are best suited to these types of therapies. Recently, however, ESWT has been shown to induce osteogenic differentiation in MSCs derived from human bone marrow, 127 and osteogenic proliferation of MSCs derived from horse adipose tissue. 128 As further research is dedicated to discovering the specific mechanisms that most directly influence osteoblast characteristics (differentiation, proliferation, morphology, adhesion, function), the potential utility of ESWT to improve porous implant fixation and osseointegration will also increase. Even older than LIPUS and ESWT technologies are experimental devices that use electrical currents to improve orthopedic therapies and enhance tissue engineering.
Pulsed electromagnetic fields
Low doses of electricity in the form of PEMF have been shown to alter the biology of various cell types. 129 For example, differentiation, morphology, and proliferation are altered by the application of alternating currents to human osteoblasts and other cell types. 129 Numerous devices are currently in use for the treatment of nonunions and spinal fusions; however, much remains to be learned regarding the dose strength, duration, position, and application of such low-intensity electrical pulses. In combination with the appropriate porous metal implant, adjuvant therapies such as PEMF, ESWT, and LIPUS will remain attractive options for potentially improving orthopedic implant fixation and osseointegration, particularly when coupled with chemical and biological strategies (mentioned above).
Conclusions and Future Directions
The search for optimal implant osseointegration, creation of a continuous osteoinductive environment that promotes local vascularization, and improved fixation of orthopedic implants led to the development of innovative methods that combine progressive material technologies with physical, chemical, and biological manipulations to the implant surface. This resulted in a considerable change of what a state-of-the-art implant, and its adjuvant treatments, should be to improve the clinical outcomes. Research avenues for biologically enhancing porous metal implants are among the least focused upon, yet the most intriguing and likely to yield the next generation of individual-based devices in bone-related regenerative medicine. As a logical next step, the trophic effects of adipose-derived stromal/stem cells seeded onto highly porous open-cell Ti materials 65 need to be better characterized through the expanded integration of RNAseq and secretome data. 8 Ercan and Webster 30 demonstrated, for example, that combining various physical (electric stimulation), chemical (anodization), and biological (cell seeding) enhancement methods may hold the key to future endeavors leading to improved orthopedic implant osseointegration and fixation, particularly in cases where circumstances like poor bone stock or advanced disease states would not normally allow for good clinical outcomes. Individualized aspects of regenerative orthopedic medicine are already under way, and represent a trend that will likely continue.
We are of the opinion that each individual patient and clinical scenario will require a unique combination of implant type, manipulation, and biological intervention. More specifically, it remains possible (if not likely) that different anatomic locations, injury types, disease pathologies, and patient histories will require distinctive surgeon-assembled solutions. For example, in the case of revision arthroplasty, spacers are often put in place for ∼6 weeks to debride and disinfect a wound. During this time, autologous adipose-derived MSCs could be harvested from the patient and grown onto the porous metal implant surface for reimplantation during revision surgery. Toward this goal, we are currently working to establish a pathway for effective biological manipulation of porous metal implant surfaces to achieve improved osseointegration and reduced risk of infection. However, as the need for total joint surgeries rises, so too will the need for directed investigations that will test and develop biologically enhanced implant materials.
Footnotes
Acknowledgments
This work was supported by the following funding sources: NIH grants R01 AR049069 (to A.v.W.), R01 DE020194 (to J.J.W.), a Patrick J. Kelly Research Fellowship award (to S.M.R.), a career development award from the American Hand Society, and the National Center for Advancing Translational Sciences UL1 TR000135 (to S.K.). Intramural funds were also provided from the Center for Regenerative Medicine at Mayo Clinic (to E.A.L. and A.D.).
Disclosure Statement
Mr. Robert Cohen serves as the General Manager and Vice President at Mako Surgical Corp. Outside the submitted work, Dr. David Lewallen reports personal fees and other from Stryker Mako, Pipeline Biomedical, Zimmer, and Ketai Medical Devices. In addition, Dr. David Lewallen has patents on selected hip and knee implants with royalties paid by Zimmer, and is employed part time as the Medical Director for The American Joint Replacement registry. None of the other authors have competing financial interests.