
Abstract
To address the growing need for corneal transplants two main approaches are being pursued: allogenic and synthetic materials. Allogenic tissue from human donors is currently the preferred choice; however, there is a worldwide shortage in donated corneal tissue. In addition, tissue rejection often limits the long-term success of this approach. Alternatively, synthetic homologs to donor corneal grafts are primarily considered temporary replacements until suitable donor tissue becomes available, as they result in a high incidence of graft failure. Tissue engineered cornea analogs would provide effective cornea tissue substitutes and alternatives to address the need to reduce animal testing of commercial products. Recent progress toward these needs is reviewed here, along with future perspectives.
Introduction
A
To date, allogenic materials originating from human donors are the preferred choice in corneal graft replacement, 3 but this approach suffers from a number of disadvantages. The major drawbacks are limited availability of quality-donor graft material, and occurrence of tissue rejection. Although corneas are the most transplanted tissues, eye bank programs cannot fulfill the demand for transplants; therefore, long waiting lists are still a limiting factor. 4 Furthermore, over 10% of the transplant population rejects replacement cornea within the first year of implantation. 5
Recently, traditional penetrating keratoplasty, where all five layers of the cornea are transplanted, has been effectively supplanted by partial lamellar keratoplasty, such as endothelial keratoplasty and deep anterior lamellar keratoplasty, which has significantly increased the rate of implant success. 4 Specifically, endothelial keratoplasty selectively replaces only the endothelial layer, whereas in anterior lamellar keratoplasty only several layers of the stroma are transplanted. Large prospective studies have shown a 10-year graft survival rate for penetrating keratoplasty ranging from 89% to 35% depending on the initial pathological condition that lead to the transplant.6–8 Once the tissue rejection process begins, the transplanted corneal graft can be medically treated with topical corticosteroids such as dexamethasone at 0.1%, or prednisolone acetate at 1%, and if tissue rejection continues the corneal graft must be surgically removed and replaced. 3 Rates for regraft rejection can be as high as 50%. The tissue rejection process has been described as painful for the patient and can lead to permanent blindness. 5
In addition, there is an overwhelming need for transplantable cadaveric corneas in the developing world. 9 In many regions around the world, widespread cadaveric donation for corneal transplantation is limited due to religious and cultural factors, lack of general education, and absence of eye banking facilities. Therefore, there is an enormous demand for an alternative to cadaveric corneal transplantation.
The need for alternative options to cadaveric corneas will continue to grow in importance as a result of increasing incidence of transmissible diseases (e.g., human immunodeficiency virus), aging of the population, and the popularity of refractive surgery, which renders corneas unusable for later transplantation. In the context of severe ocular surface pathologies, where the risk of transplant rejection is significantly higher, synthetic homologs, known as keratoprostheses, are chosen as option to donor corneal grafts for full-thickness corneal replacement. Keratoprostheses are used to replace corneas at high risk of immunological rejection or endothelial failure after penetrating keratoplasty and in eyes with limbal stem cell deficiency. Several keratoprostheses are in clinical use but the Boston type-1 keratoprosthesis is by far the most common. It is comprised of front and back plates, an optical polymethylmethacrylate section, and a titanium-locking ring mounted on a donor cornea, which serves to anchor the device in the host eye. Short-term visual recovery is good but long-term prognosis is limited by various complications, including glaucoma and endophthalmitis, requiring a high level of medical intervention, thus, reducing the long term use of these devices. 4 Furthermore, osteo-odonto keratoprosthesis has shown good long-term anatomical survival rate and is currently the most common treatment in the case of end-stage inflammatory corneal disease, such as Stevens–Johnson syndrome and thermal and chemical burns. 10
In addition, increased interest in reducing animal testing for pharmaceutical and cosmetic products drives the need for in vitro preclinical cornea tissue models. The need within the cosmetics industry to produce tissue analogs for animal testing models continues to grow to replace eye irritation and toxicity tests. 11
In this review we provide insight into the human cornea with respect to the approaches being pursued to engineer the epithelium, stroma, endothelium, and full-thickness human cornea systems, and discuss the preclinical in vitro tissue models currently in clinical use.
Anatomy and Functions of the Human Cornea
The human cornea is a transparent, avascular, connective tissue that primarily provides an optical interface with substantial refractive power. Additionally, the cornea provides protection for the eye, both mechanical and from infections, and transparency. The adult human cornea measures between 12 and 13 mm in the horizontal and vertical diameters, 12 0.5 mm in thickness at the center and then progressively increases toward the sclera. 13 The cornea is an organ comprised of three distinct cellular layers, corneal epithelium, stroma, and endothelium, separated by two acellular collagenous interfaces referred to as Bowman's layer and Descemet's membranes (Fig. 1A). The cornea is rich in collagens and contains a unique class of small leucine-rich proteoglycans, including keratan sulfate glycosaminoglycan. The corneal epithelium is a stratified, nonkeratinized squamous tissue with 4–6 cell layers comprising 10% of the overall corneal thickness (40–50 μm). 14 The epithelium is one of the most highly innervated tissues in the body, and it is equipped with nociceptive nerve endings that terminate within the epithelial layers. 15 The epithelium provides a biological barrier function, essential for corneal transparency, which regulates transfer of water and all soluble components into or out of the stroma. The corneal epithelium in conjunction with the tear film presents a smooth interface at the anterior surface of the eye allowing coherent refraction of light as it enters the cornea. 16 In addition, the tear film functions as a reservoir for antibacterial and growth factors, crucial in the maintenance of epithelial homeostasis, proliferation, and repair. Bowman's membrane, (also termed the Anterior Limiting Lamina), is a 15 μm-thick acellular layer of amorphous condensed collagen immediately posterior to the epithelial basement membrane. Bowman's membrane may act as a molecular barrier and/or contribute to corneal shape. 17 The corneal stroma makes up ∼90% of the overall cornea thickness and consists of layers of aligned collagen fibrils termed lamellae. 18 Approximately 200 to 250 lamellae extend from limbus to limbus with collagen fibril orientation offset between adjoining layers. The lamellar collagen fibrils are heterotypic hybrids of type I and V, displaying remarkably small diameter (∼25 nm). Significant amounts of the fibril-associated collagens XII and XIV and nonfibrillar collagens type VI are also present. A high concentration of small leucine-rich proteoglycans, including decorin, lumican, keratocan, decorated with dermatan sulfate and keratan sulfate are present in the lamellae, credited with maintaining the interfibrillar spacing required for transparency, and contributing to regulation of corneal hydration.13,16 The regular lamellar layering becomes increasingly random in the anterior stroma where more oblique branching and interweaving is observed. 19 Interlamellar branching is also more extensive in the corneal periphery than in the center. 20 The interweaving of collagen bundles between neighboring lamellae provides an important structural foundation for shear (sliding) resistance and transfer of tensile loads between lamellae. The corneal stroma is populated by keratocytes, mesenchymal cells of neural crest origin. These cells are sandwiched between lamellae and maintain the matrix components of the lamellar connective tissue.21,22 The highly organized collagen lamellae provide mechanical support and biophysical properties required for transparency. 23 These include the uniquely small diameter, regular spacing, and tight packing of collagen fibrils. At the posterior of the stromal layer is Descemet's membrane, a thickened basement membrane rich in type VIII collagen, which provides anchoring for the corneal endothelial layer. 24 The endothelium provides a metabolic pump, removing water from the stroma and maintaining the correct level of stromal hydration responsible for corneal transparency (Fig. 1B).16,25
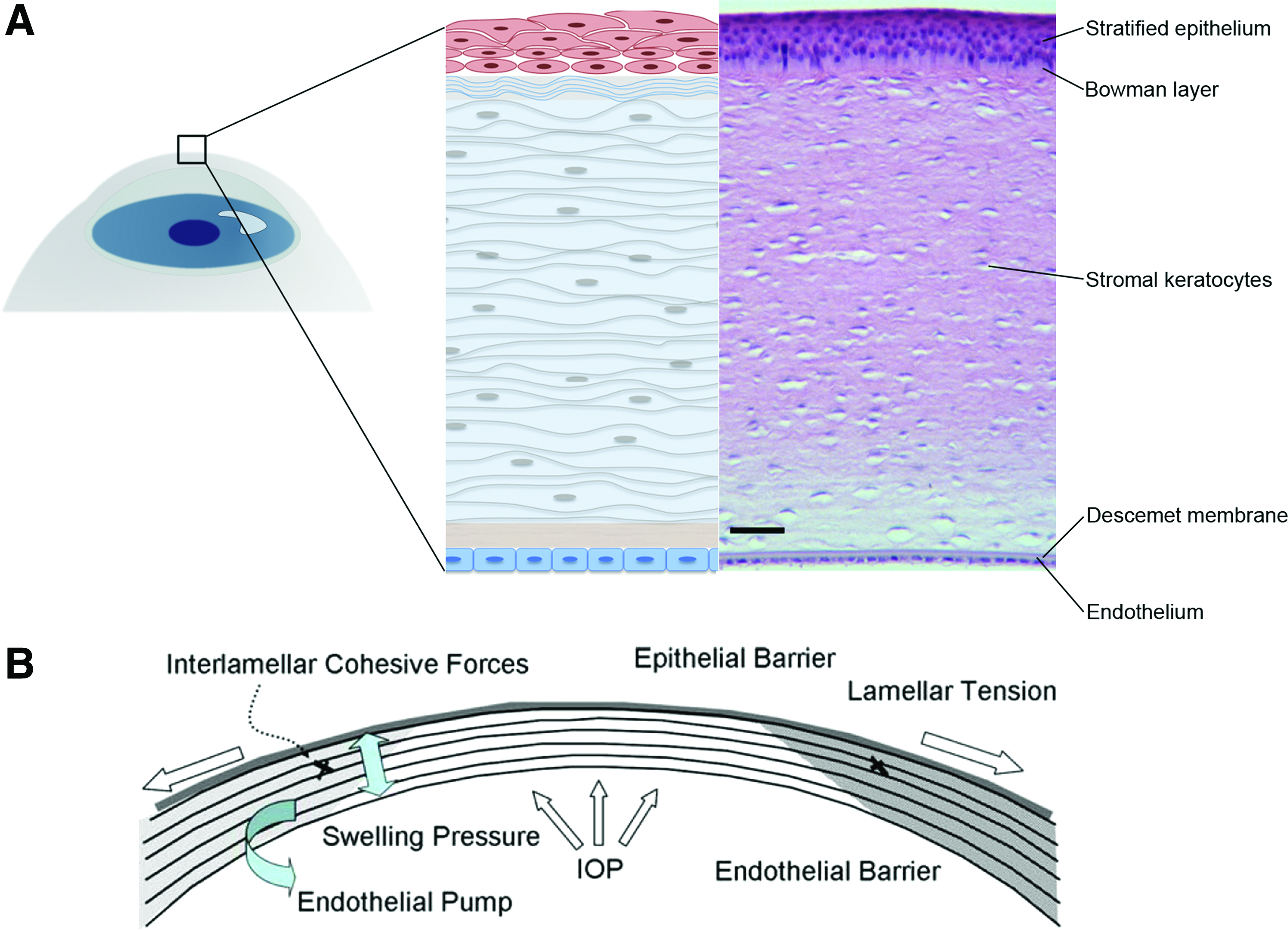
Human cornea structure and function.
The functions of the cornea dictate the three principal design requirements a corneal substitute or tissue model will need to satisfy: protection, transparency, and providing an optical interface with substantial refractive power. Particularly, the stroma is a highly organized, dense, avascular, and relatively acellular connective tissue. It consists of highly organized collagen fibrils, which provide lateral tensile strength. 26 In addition, the epithelium represents the external surface of the ocular system, therefore protecting the stroma and the endothelium from chemical injuries and infections. In addition, the cornea functions as filters to protect the retina from damaging UV light. 27 The transparency of the cornea is determined by to the collagen interfibrillar spacing, regulated by the hydrophilic stromal proteoglycans, which are ultimately regulated by the tissue state of hydration, through the endothelium pump. 13
Current Tissue Engineering Approaches for Corneal Replacement
Tissue engineering principles have been applied in an effort to generate viable cornea tissue equivalents at different levels of complexity, starting from engineering of epithelium, stroma, and endothelium layers, to approaches to recreate the native innervation. These approaches have culminated in full-thickness cornea tissue equivalents, implemented in clinical settings, by using a plethora of biomaterial systems (Table 1) and various cell types (Table 2). In particular, the main approaches can be divided in purely cell-based, decellularized, synthetic-, and natural polymer-based constructs in combination with different cell types.
Corneal epithelium
Epithelial and endothelial layers play pivotal roles in maintaining corneal deturgescence (relative state of hydration), and ultimately its transparency, through barrier and pump functions. 13 In vitro the corneal epithelial layer has been successfully generated by cell sheet engineering, and it has been shown to promote in vitro growth of a functional stratified epithelium.28–30 In addition, engineered epithelial tissue sheets, prepared using thermoresponsive polymeric substrates, have been clinically evaluated using autologous oral mucosal epithelium (Fig. 2A). However, major drawbacks of this technique are the high variability and the extended time in culture required to generate adequate structures for transplantation. 31 Similarly, human amniotic membranes have been extensively applied as substrates for corneal epithelial-derived in vitro expansion and for reconstruction of damaged cornea in several animal models (e.g., rat, rabbit, and goat).32–36 However, the high inter- and intra-tissue variability in morphological, chemical, and optical properties limit the use of the human amniotic membrane in clinical settings.37–39 Alternatively, human donor corneal stromal tissues have been proposed as substrates for human corneal epithelium growth, displaying, in vitro, features similar to the native limbal epithelium. 40 The lack of corneal tissue donor availability significantly affects its clinical potential for corneal reconstruction. Among natural polymers, reconstituted type I collagen hydrogels can successfully encapsulate human corneal limbal epithelial cells, resulting in functional stratified epithelial layers. 41 Furthermore, collagen hydrogels have been used to engineer corneal limbal crypts through microcontact printing to generate three-dimensional (3D) in vitro human limbal epithelial stem cell niche, which contributes to the maintenance of the corneal epithelium regeneration. 29 Chemically cross-linked collagen hydrogels were also explored as corneal epithelium scaffold, due to the enhanced mechanical and optical properties in comparison to thermally driven collagen hydrogels. 42 Owing to the optical properties, mechanical robustness, and its versatile processability, 43 silk has been exploited as substrate for human epithelial cell growth and functional organization. 44 Particularly, silk film topography significantly influenced initial human epithelial cell attachment, proliferation, and growth.45,46 Further studies have shown that silk surfaces can be optimized by contact guidance to direct collective epithelial cell migration and the direction of tissue epithelialization. 47 Similarly, keratin-based substrates have been exploited for ocular surface reconstruction because of their good optical properties and ability to support epithelial cell growth in vitro.48,49
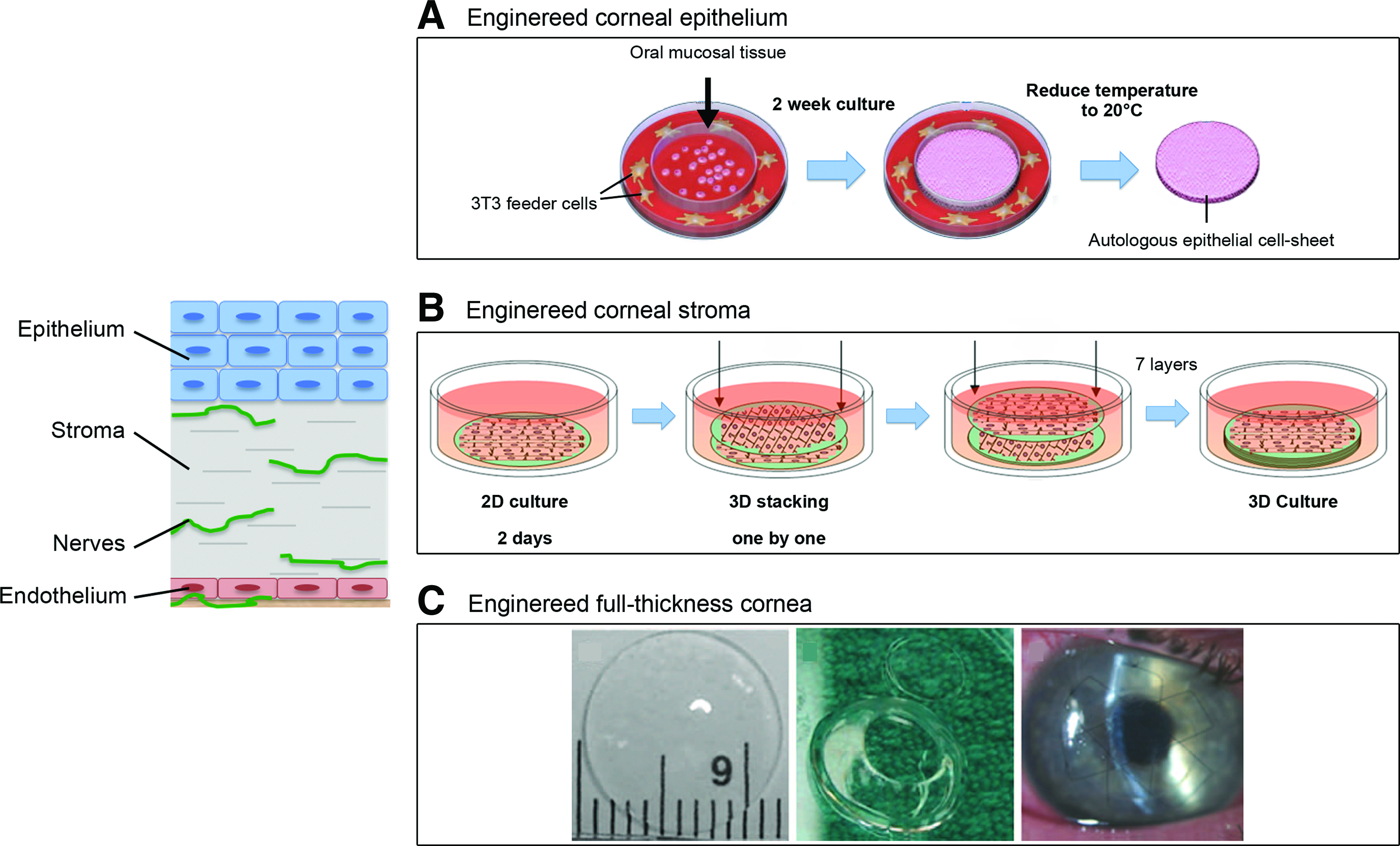
Tissue-engineered approaches for corneal reconstruction.
Corneal stroma
Reconstruction of corneal stroma is challenging due to its complex structure, mechanical strength and transparency. Therefore, engineering corneal stroma has been actively investigated by developing functional corneal stroma substrates through chemical, morphological, and mechanical cues.50–57
In particular, synthetic polymers have been explored for stromal corneal substrates because of their tunable mechanical properties. They have also been processed in micron- nano-sized fiber forms to direct stromal cell organization and differentiation in vitro, resulting in stratified collagen fibril lamellae in orthogonal orientations. A fibrous poly(ester urethane) urea substrate in combination with the use of human stromal stem cells, which are able to differentiate toward keratocyte lineages, showed promise for the in vitro engineering of the stroma via a two-dimensional (2D) approach, although lacking in adequate optical properties.
58
The combination of synthetic polymers together with natural-derived materials provides enhanced biological responses and more amenable optical properties.
59
As an example, hydrogels films prepared from chitosan blended with poly(ethylene glycol) and poly (
Corneal endothelium
Engineering of the endothelial layer has recently been explored mainly using natural polymer substrates, including type I collagen, gelatin, decellularized tissues, chitosan, and chondroitin sulfate, which showed evidence for the formation of a functional endothelium.60,69–74 Decellularized aminiotic membrane was clinically evaluated in combination with human corneal endothelial cells in a lamellar keratoplasty model, where the removal of the endothelium and part of the Descemet's membrane was performed and able to function as a corneal endothelium equivalent. 73
Corneal innervation
The cornea is one of the most innervated tissues in the human body, with nociceptive nerve protrusions, which end in the epithelial layer. The corneal nerves function as mechanical and thermal sensors, to maintain the overall cornea health. The progressive lack in innervation is at the base of the pathological conditions known as dry eye, resulting in a reduction in corneal sensitivity and ultimately in diffuse corneal ulcers. Despite the critical role of innervation in corneal functions, few attempts have been made to induce peripheral nerve proliferation within corneal tissue-engineered constructs. In vitro studies have shown that decoration of substrate with laminin-derived peptides promoted epithelial stratification and neuron growth. 75 Furthermore, functional nerve regeneration was observed in a deep lamellar keratoplasty porcine model using cross-linked collagen substitutes, recovering preoperative nerve density at 1-year postsurgery. 76
Full-thickness cornea equivalent
Direct in vivo implantation of corneal equivalent biomaterials without cells has been investigated to study the integration of implanted biomaterials with native corneal tissue.77,78 Efforts to mimic the three-layer structure of the cornea (epithelium, stroma, and endothelium) have been reported.42,79–81 Recent studies have been also focused on the use of decellularized biological material, as in the case of amniotic membrane and animal cornea. However, the results of an acellular porcine cornea in combination with amniotic epithelial cells in a rabbit lamellar keratoplasty resulted in degradation of the tissue-engineered cornea due to host rejection. 33 Further efforts have been undertaken to develop in vitro corneal stroma equivalents, in combination with the engineering of the epithelial layer and promoting nerve ingrowth, which ultimately culminated in engineered full-thickness cornea for tissue replacement, based on type I collagen in combination with a variety of synthetic polymers (e.g., polyacrylamide, poly(ethylene glycol)).82–85 Biosynthetic corneas from cross-linked recombinant human collagen type III were implanted in an anterior partial keratoplasty surgery in human patients, to enhance endogenous tissue regeneration. The implants were stably integrated, innervated, and avascularized up to 2 years (Fig. 2C). However, the retaining sutures of the implants delayed epithelial closure and there was concurrency of tissue thinning and fibrosis. 86 A 4-year follow-up showed the construct stably integrated without rejection, whereas future steps are focused on improving visual acuity based on materials with better shape retention. 87
Cell sources
In an effort to generate an in vitro 3D cornea tissue model and to address the need of surgical replacements for partial and full keratoplasty, the most extensively investigated cell populations are epithelial and stromal cell lines for early investigations, while primary human epithelial and stromal cells are mainly implemented in in vitro 3D tissue models and preclinical approaches (Table 2). Furthermore, several studies report methods to isolate and utilize limbal stem cells for regenerating corneal epithelium, stromal stem cells, and mesenchymal stem cells for corneal repair.32,34,88–90 Human stromal stem cells have been used to repopulate mouse corneas and restore stromal thickness, fibril deficits, and transparency in cloudy corneas found in lumican−/− mice, 91 and in natural and synthetic polymers-based in vitro systems.58,67 The cells were found to be stably integrated into the mouse cornea for >10 weeks. Importantly, the stem cells did not elicit an immune response, while under the same conditions corneal fibroblasts were immunogenic. The data suggest that a bioengineered cornea populated with such immune privileged cells could provide a viable supplement to corneal replacements and in vitro models. Therefore, human corneal stromal stem cells represent a promising avenue for clinical translational approaches.
Current Tissue Engineering Approaches for In Vitro Corneal Tissue Model
The need for in vitro preclinical cornea tissue models has increased in an effort to reduce animal testing for commercial products. In particular, the cosmetic and pharmaceutical industries encourage the development of viable tissue analogs for irritation and toxicity tests, driven by regulatory requirements. Analogous to the field of tissue-engineered skin, the Seventh Amendment of the European Union Cosmetics Directive requires that irritancy testing of cosmetic products needs to be carried out on in vitro models. 92 Engineered tissue analogs may provide effective alternatives to supplant the need for animal testing. In particular, a tissue-engineered cornea could be used in place of the gold standard model for eye irritancy, the Draize Test, which is based on observations upon topical application of a substance in the rabbit eye. 93 Furthermore, in vitro cornea models would also be beneficial for drug permeability studies, currently performed with bovine or porcine corneal explants, which have problems associated with reproducibility and species matching, similar to the Draize Test. 94 In vitro cornea models range from simple monolayer systems to stratified cell cultures, to epithelium-stroma multilayered systems, and culminate in 3D full-thickness corneal equivalents (Fig. 3).
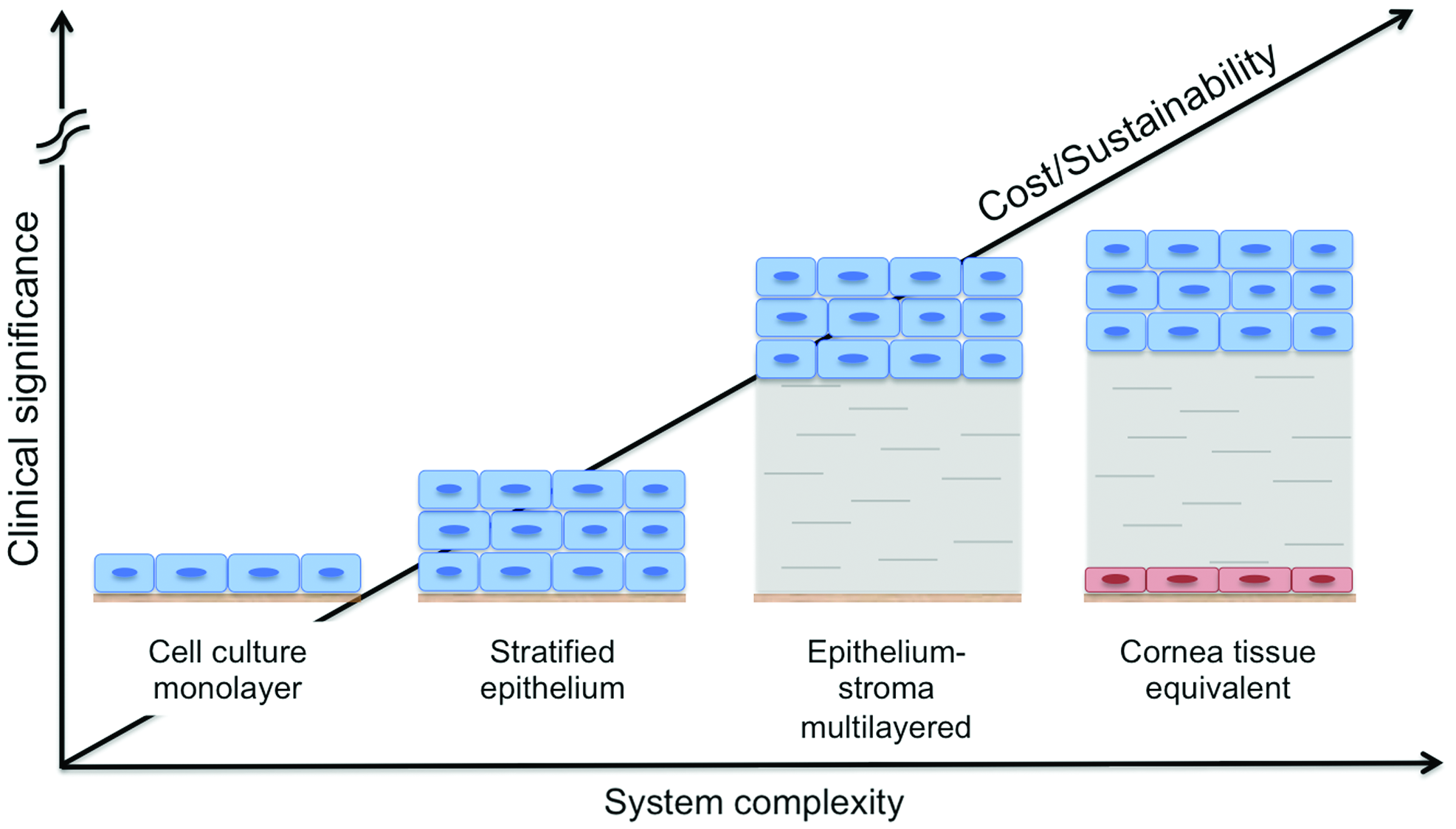
Schematic of cornea tissue models. In vitro cornea models range from simple monolayer systems to stratified cell cultures, to epithelium-stroma multilayered systems, and culminate in 3D full-thickness corneal equivalents, as function of system complexity, cost and culture sustainability, and clinical significance of each approach. 92 Color images available online at www.liebertpub.com/teb
The use of a 3D tissue-engineered cornea in the context of in vitro tissue models has been explored to recapitulate the three layers of the cornea (i.e., epithelium, stroma, and endothelium) in combination with human cells for the study of complex physiological and pathophysiological processes in a highly controlled 3D environment (Table 3). The in vitro testing platforms developed up to date mainly comprise a corneal epithelial model, where stratified human epithelium was cultured on a porous permeable polycarbonate substrate and used to test the irritancy of 20 test compounds in comparison to the Draize Test. 95 A simplified model based on the epithelium layer alone may be sufficient for acute surface irritancy testing, whereas a more complex tissue model is required to test drug irritancy, toxicity, and permeability through the entire cornea thickness. A three-layer model was developed based on a collagen gel, where corneal endothelial, stromal, and epithelial cells were used for permeability testing protocols. The model was initially proposed with bovine-derived cells and then improved with the use of human cells. Construct permeability was measured the same in engineered corneal construct and explanted human cornea control. 96 However, construct material morphological and mechanical properties are far from native tissues. Furthermore, cornea tissue models for pathological chronic studies have mostly been implemented in 2D in vitro culture systems using immortalized corneal epithelial cells to study dry eye and gelatinous drop-like corneal dystrophy.97,98 The cornea in vitro disease model studies developed to date lack full recapitulation of the 3D multilayered native tissue structure, the interplay of the different cell types (i.e., epithelium, stroma, endothelium, and nerve), and sustained function, in case of chronic diseases.
Future Perspectives
In an effort to address the need for viable human corneas, significant advances in tissue engineering have been made in recent years. Both synthetic and naturally derived biomaterials in combination with primary cells have been used to regenerate and replace partial or full-thickness pathological corneas, starting from epithelial, stromal, endothelial layers, and full-thickness corneal tissues. Naturally derived corneal substitutes hold promise for long-term success having reached human clinical trials. In addition, purely cell-based approaches may also be viable alternatives for both cornea tissue replacements and in the context of in vitro tissue models to significantly reduce animal testing. Some additional attention will be needed to better match current systems to human physiological relevance and requirements, to match systems to suitable remodeling/regeneration time in vivo to provide a suitable crossover time frame between implants and the regeneration of native cornea tissue, and to allow the study of cornea diseases in vitro as discovery tools for new treatment options.
Footnotes
Acknowledgments
We thank the NIH (R01 EY020856 and P41 EB002520) for support for this work. We also thank our many collaborators who have been involved in our own studies of cornea tissue engineering, including Eun Seok Gil, Biman Mandal, Jeff Marchant, and James L. Funderburgh.
Disclosure Statement
No competing financial interests exist.