
Abstract
Progress in biomaterial science and engineering and increasing knowledge in cell biology have enabled us to develop functional biomaterials providing appropriate biochemical and biophysical cues for tissue regeneration applications. Tissue regeneration is particularly important to treat chronic wounds of people with diabetes. Understanding and controlling the cellular microenvironment of the wound tissue are important to improve the wound healing process. In this study, we review different biochemical (e.g., growth factors, peptides, DNA, and RNA) and biophysical (e.g., topographical guidance, pressure, electrical stimulation, and pulsed electromagnetic field) cues providing a functional and instructive acellular matrix to heal diabetic chronic wounds. The biochemical and biophysical signals generally regulate cell–matrix interactions and cell behavior and function inducing the tissue regeneration for chronic wounds. Some technologies and devices have already been developed and used in the clinic employing biochemical and biophysical cues for wound healing applications. These technologies can be integrated with smart biomaterials to deliver therapeutic agents to the wound tissue in a precise and controllable manner. This review provides useful guidance in understanding molecular mechanisms and signals in the healing of diabetic chronic wounds and in designing instructive biomaterials to treat them.
Introduction
T
After its emergence and soaring development with enthusiasm from business community in the 1990s, tissue engineering industry entered a dark period in the early 2000s, with the capital value of publicly traded tissue engineering companies reduced by 90% between 2000 and 2002. 6 Organogenesis (Canton, MA) and Advanced Tissue Sciences (La Jolla, CA), two leading companies that brought the first commercially-produced tissue engineering products to the market, engineered skin substitutes, declared bankruptcy in 2002. 8 This performance resulted in the reassessment of tissue engineering products, which are thought to be limited by their long preparation time, challenging quality control, complex distribution chains, and short shelf life. Fortunately, the reassessment resulted in viable products such as skin substitutes now commercially available through Organogenesis.
Recently, the focus of tissue engineering has undergone considerable evolution from replacement to regeneration in situ because it has been recognized that instead of recreating the complexity of living substitutes for transplantation, 9 we can develop instructive materials to harness body's innate power of self-repair. 10 In these scenarios, the matrix not only serves as a scaffold that provides mechanical support and defines the shape of tissue constructs but also provides a multitude of complex stimuli to regulate cell behavior in tissue remodeling.
Advances in biomaterial science and engineering combined with ever-growing knowledge in cell biology led to the design of biomaterials with appropriate biochemical cues and biophysical guidance for tissue regeneration in situ. Moreover, complexities in the matrix design and fabrication were enabled by innovative technologies with precise control and improved reproducibility.11,12 As the first category of commercial tissue engineering products, wound dressings witnessed these innovations. In this study, we review recent advances in designing acellular instructive matrix for wound healing applications, under the principle of facilitating the cell–extracellular matrix (ECM) interactions with biochemical and biophysical cues to induce or support native tissue regeneration.
Diabetic Chronic Wounds
Wound healing requires a well-orchestrated integration of biological and molecular events of cell migration and proliferation and ECM deposition and remodeling. This complex process can be described in three overlapping phases as follows: inflammation, proliferation (angiogenesis and reepithelialization), and remodeling. Transition between these phases is regulated by inflammatory mediators, growth factors, cytokines, and mechanical forces.13,14 However, the process can be impaired by some systemic complications, such as diabetes mellitus, and results in chronic wounds. Chronic wounds are pervasive worldwide, affecting more than 70 million people particularly in the senior population with harsh medical and social consequences. 15 In particular, diabetic foot ulcer affects 15% of people with diabetes and is the leading cause of nontraumatic amputation. 16
Denervation of local sympathetic nerve system is a hallmark of diabetic neuropathy and results in sensory deficits, so that the patients cannot respond to external stimuli such as pressure and heat. 17 Absence of protective symptoms leads to further deformities and infection. 18 Meanwhile, diabetic wound healing is challenged by vasculopathy. Vasculogenesis is limited by insufficient mobilization of circulating endothelial progenitor cells from the bone marrow 19 and their impaired homing to the wound site. 20 Impaired endothelium function also involves a reduction of nitric oxide (NO) synthesis and increased NO degradation by excess reactive oxygen species (ROS). 21 Moreover, excessive glycosylation of matrix proteins induced by hyperglycemia leads to basement membrane crosslinking and angiogenesis dysfunction. 22 Excessive activation of matrix metalloproteinases (MMPs) such as MMP-9 also impairs cell migration and degrades critical matrix proteins and growth factors. 23
On the cellular level, the resident cells in diabetic chronic wounds are associated with abnormalities. Fibroblasts isolated from diabetic chronic ulcers are senescent with decreased responses to growth factors, including transforming growth factor-β1 (TGF-β1), platelet-derived growth factor (PDGF), epidermal growth factor (EGF), insulin-like growth factor-1 (IGF-1), and basic fibroblast growth factor (bFGF).24–27 Macrophages in diabetic wounds show decreased release of cytokines, including tumor necrosis factor-α (TNF-α), interleukin (IL)-1β, and vascular endothelial growth factor (VEGF). 28 Attachment and migration of keratinocytes, the critical events in reepithelialization, are impaired in diabetic chronic wounds due to altered ECM composition and increased ECM degradation.29,30 Meanwhile, all resident cells in the wound are stressed by excessive production of ROS from macrophages and neutrophils caused by prolonged inflammation, coupled with impaired antioxidant defense in response to hyperglycemia.31–33
Wound Dressing Matrices
Wound dressing matrices were the first category of Food and Drug Administration (FDA)-approved tissue engineering products and have embraced numerous innovations ever since. In general, wound dressings can be categorized into skin substitutes with cells and acellular dressings. Living skin substitutes consist of dressing materials hosting dermal cells and/or epidermal cells. With current techniques, epidermal grafts capable of covering the entire boy surface area can be generated from a 3-cm2 biopsy from autologous tissue. 34 Mesenchymal stromal cells have also been reported to promote both normal and diabetic wound healing and clinical trials are under way. 35 However, commercial lessons have been hard won for living skin substitutes since they were limited by the costly and lengthy preparation, short shelf life, and difficulties in distribution. 36
Based on how acellular dressings interact with the native environment, they can be further grouped into bio-inert dressings and bioactive dressings. Bio-inert dressings mainly serve as a physical barrier and keep the wound environment moist. Winter first described that moisture-retaining dressings accelerated epithelialization of acute superficial wounds in pigs compared with air-exposed wounds 37 and similar results were later observed in human. 38 Moreover, some conformable bio-inert dressings can absorb exudate in the draining wounds. 39
A group of bioactive acellular wound dressings were developed to deliver bioactive agents to the wounds. Antibiotic drugs, including streptomycin, 40 minocycline, 41 vancomycin, 42 neomycin, 43 and ciprofloxacin,44,45 have been delivered and antiseptic agents have been applied such as iodine-releasing agents (e.g., Iodozyme™ and Hyiodine®), silver-releasing agents (e.g., SilverSeal®), and chlorhexidine (e.g., BACTIGRAS⋄).
Wound dressing scaffolds can be categorized into naturally derived and synthetic biomaterials (Table 1). In general, they each target only one aspect of the wound healing process, whereas a multifaceted approach may be preferred for efficient and complete healing. Decellularized matrices have gone through minimum biochemical modification and still preserve the native ECM microstructure, which provides topographical guidance for tissue regeneration. Decellularization products that have been approved by the FDA for diabetic wounds include OASIS® (derived from porcine small intestinal submucosa), MatriStem® (derived from urinary bladder matrix), and AmnioFix® (derived from amnionic membrane). Naturally derived biomaterials, including proteins (e.g., collagen) and polysaccharides (e.g., chitosan), have wide biomedical applications and some of them have been approved by FDA as well. Their extensive use has been associated with thorough characterization and a small likelihood of side effects in new applications. 46 A key advantage of naturally derived biomaterials is their general capacity to support cell attachment, proliferation, and differentiation. 47 The inherent composition and structure of naturally derived biomaterials enable their biological recognition, including cell receptor binding and cell-triggered degradation and remodeling. 47 Type I collagen is the most popular option because of its close similarity to the native ECM.48,49 Other naturally derived biomaterials such as chitosan, 50 cellulose, 51 fibrin, 52 gelatin,53,54 silk, 53 and alginate 55 have also been used.
ECM, extracellular matrix; MMP, matrix metalloproteinase; PDGF, platelet-derived growth factor; PEG, polyethylene glycol; PGA, polyglycolic acid; PLA, polylactic acid; PU, polyurethane; PVA, polyvinyl alcohol.
In contrast, synthetic biomaterials provide precise control over material properties (e.g., biochemical composition, mechanical properties, topography, and structure), simplified purification process, and reduced possibilities of immunogenicity and pathogen transmission. 56 Rapid development of electrospinning and nanotechnology enables synthetic wound dressings with versatile nanoscale structure and function. In a recent study, Yu et al. synthesized an elastic, wearable crosslinked polymer layer that mimics normal youthful skin and demonstrated its application to decrease the herniation appearance of lower eyelids with rapid curing on the skin. 57
Instructive Cues to Promote Wound Healing
Because of the unmet clinical needs to treat diabetic wounds, there are growing efforts to develop matrices that are instructive and cost-effective. Recent advances in biotechnology and biomedical engineering have enabled novel approaches to mimic the wound healing microenvironment. These approaches can be generally categorized into biochemical cues and biophysical cues (Fig. 1 and Table 2).
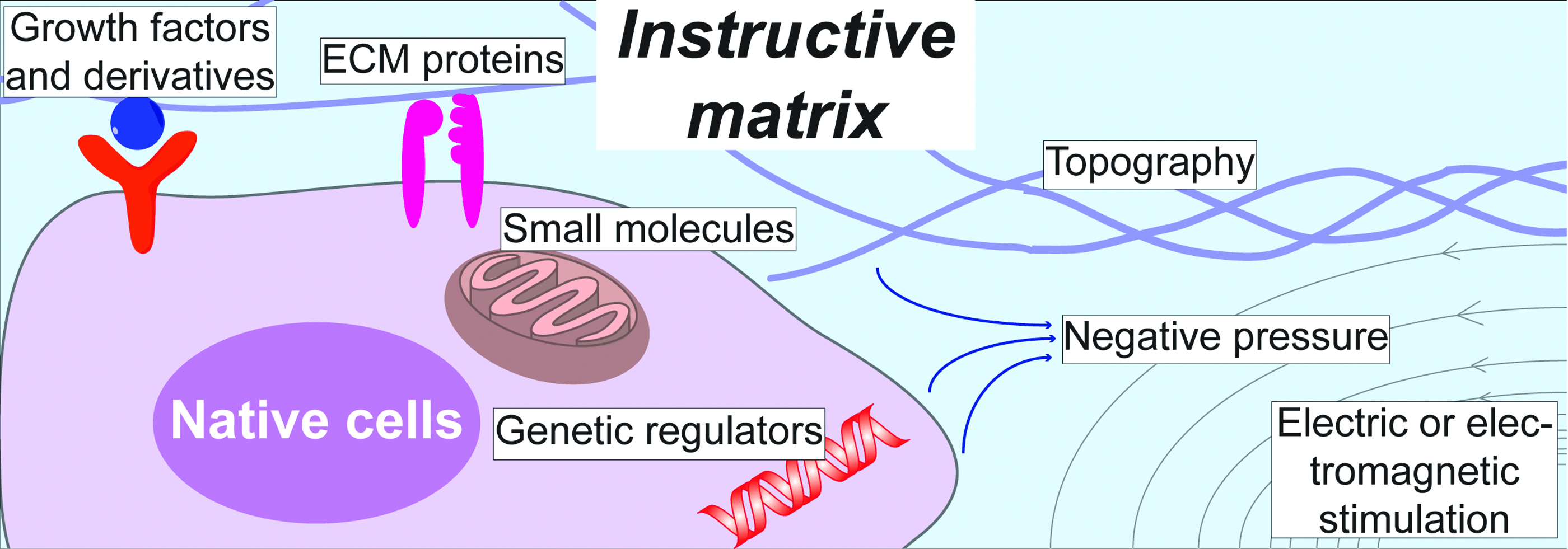
Various biochemical and biophysical cues provided by matrix to regulate the native cell response. Growth factors and derivatives can interact with native cells through their specific receptors. The composition of ECM proteins is usually recognized by integrins. Small bioactive molecules, including oxygen and NO, can diffuse into the cells and mainly affect mitochondrial activities. Genetic regulators, including cDNA, miRNA, and siRNA, can be delivered by nonviral vehicles and facilitate gene transcription and translation. Electric or magnetic cues can also influence cell responses such as migration. cDNA, complementary DNA; ECM, extracellular matrix; miRNA, microRNA; NO, nitric oxide; siRNA, small interfering RNA. Color images available online at www.liebertpub.com/teb
bFGF, basic fibroblast growth factor; cDNA, complementary DNA; EGF, epidermal growth factor; RGD, Arg-Gly-Asp; siRNA, small interfering RNA; TGF-β, transforming growth factor-β; VEGF, vascular endothelial growth factor.
Biochemical cues
The importance of biochemical cues on cellular behavior and tissue morphogenesis is well recognized. Biochemical properties are often considered as the first parameter in biomaterial design for wound healing applications (Fig. 1). 10
Growth factors
Growth factors are potent regulators of cell activities, including migration, proliferation, differentiation, and survival. PDGF-BB as the Regranex® gel was the first growth factor approved by the FDA in 1997. It was used in the treatment of diabetic neuropathic ulcers. 58 Other growth factors investigated in the wound dressings include EGF, 59 VEGF, 60 bFGF, 61 and TGF-β. 62 Conventional delivery methods often provide growth factors in the soluble form, which results in a burst release causing severe side effects such as hypotension (e.g., VEGF) and nephrotoxicity (e.g., bFGF). 63 Recently, novel delivery strategies have been explored and a synergistic signaling between growth factor receptors and integrin ligands was proposed, 64 which motivates immobilizing growth factors in close affinity to ECM proteins. Martino et al. demonstrated that growth factors delivered by this method were effective at a lower dosage, 64 thereby reducing application cost and potential side effects. Dynamic release of different growth factors with independent release profile can recapitulate the dynamic environment in developmental pathways.65,66 Novel immobilization methods have been applied on instructive biomaterials to localize, enhance, and sustain growth factor bioactivities.67–70
Growth factor derivatives and peptide sequences
Peptides are short functional amino acid sequences derived from primary receptor domains of specific proteins and they bring an advantage of cost-effectiveness in scalable chemical synthesis compared to recombinant growth factor production. 71 While retaining similar or higher biological potency, peptides are more stable than native growth factors, which can simplify the preparation and modification of biomaterials. 10 The best characterized peptide is the integrin-binding Arg-Gly-Asp (RGD) sequence, which is found in many ECM proteins, including fibronectin, type IV collagen, and laminin.72–74 RGD sequence has been extensively applied in modifying synthetic biomaterials to provide cell-adhesive sites.56,75 Other peptides have been designed as mimics of growth factors (e.g., angiopoietin,76,77 VEGF, 78 and TGF-β179) or as novel delivery systems.80,81
Small bioactive molecules
Oxygen
The importance of oxygen in wound healing is well documented as high energy is required in the granulation tissue for cellular activities, including bacterial defense, cell proliferation, and cell migration. Oxygen level in chronic wound tissues is lower than that in normal wounds. 82 Historically, hyperbaric oxygen therapies (HBOTs) were developed in which the body is intermittently exposed to pure oxygen in a stationary pressure chamber. 83 HBOT delivers the oxygen through a systematic circulation; therefore, its efficacy is limited in tissues with poor circulation. Since the late 1960s, a topical oxygen therapy has been developed, which involves applying pure oxygen with sealing around wound tissues for about 90 min, once a day at a pressure slightly above ambient atmospheric pressure. 84 More recently, oxygen-releasing wound dressings (e.g., Oxyzyme™) have been commercialized to promote wound healing by eliminating cellular hypoxia after tissue damage. 83 Instead of attaching a bag filled with pure oxygen, the Oxyzyme system generates oxygen by chemical reaction.
Oxygen level is an important regulator of wound healing. Once recruited to the wound site, leukocyte's bactericidal activity is positively correlated to local oxygen concentration. 85 HBOT reversed diabetic defects by mobilizing endothelial progenitor cells from the bone marrow, critical for angiogenesis. 20 During remodeling, fibroblast proliferation and collagen synthesis are also oxygen dependent.86,87 Other than directly supplying energy for the cellular metabolism, oxygen is also critical for growth factor signaling. 88 Metabolically active cells in the wound area consume large amount of oxygen and this together with interrupted blood supply contributes to a hypoxia gradient in the wound. The discovery of hypoxia-induced factor 1α (HIF1α) highlighted the importance of hypoxia gradient in the wound healing process 89 and stabilized HIF1α expression, critical to improve diabetic wound healing. 90
Nitric oxide
Since the discovery of NO as an endothelial relaxing factor, 91 it has been intensively studied in virtually all organs and tissues under both normal and pathological conditions. 92 NO is generated by nitric oxide synthase (NOS) enzyme and three isoforms of NOS have been identified: two constitutively expressed isoforms (endothelial NOS [eNOS] and neuronal NOS [nNOS]) and one inducible NOS (iNOS) isoform.93–95 All three isoforms of NOS have been found in the skin: nNOS has been observed in keratinocytes and melanocytes96,97; eNOS has been detected in basal keratinocytes, dermal fibroblasts, endothelial capillaries, and eccrine glands98,99; and iNOS has been induced in keratinocytes,100,101 dermal fibroblasts, 98 and endothelial cells. 102
NO is involved throughout the three phases of wound healing as an important regulator of angiogenesis, inflammatory response, and collagen deposition.
103
During early inflammatory phase, NO regulates the infiltration of monocytes and neutrophils by activating pro-inflammatory cytokines (e.g., IL-8 and TGF-β1) and serves as a chemoattractant.104–106
NO promotes angiogenesis and keratinocyte migration in proliferation phase. Importantly, NO is vital for the VEGF activity as blockade of NOS prevents VEGF-induced endothelial cell proliferation.
107
NO also promotes endothelial cell proliferation and migration directly.
108
Moreover, NO has been reported to promote proliferation of keratinocytes and inhibits their apoptosis.109,110 During remodeling, NO predominantly regulates the collagen synthesis in fibroblasts as treatment with NO donors (e.g., dietary
Over the past two decades, NO delivery devices/vehicles have been developed to transit the therapeutic potential of NO in chronic wounds. It is extremely difficult to handle NO as a gas molecule owing to its instability and its oxidation potential to the toxic nitrogen dioxide molecule. Therefore, various vehicles such as S-Nitrosothiols,114,115 diazeniumdiolates,116,117 and nanoparticles113,118,119 have been used to deliver NO and, thereby, improve the wound healing process.
Genetic regulators
Genetic therapies were originally developed from successful delivery of genes based on viral vectors. 120 However, use of viral vectors in humans faces safety challenges such as immune reactions. Therefore, nonviral vectors have been developed to deliver genetic regulators, including naked DNA 121 and RNA interference. 122 Efficient delivery and targeted release are the main challenges for genetic therapies and recent advances such as electroporation have significantly contributed to address them. 123 In this study, we review recent advances in genetic regulators delivered by nonviral vectors with a focus on wound healing applications.
Complementary DNA
Complementary DNA (cDNA) is a DNA copy synthesized from the target mRNA that encodes a specific protein through reverse transcription. Nonviral vectors, including cationic polymers, cationic liposomes, and naked plasmids, have been used to deliver cDNAs encoding for peptides (e.g., LL-37, 124 secretoneurin 125 ) and growth factors (e.g., VEGF, 126 keratinocyte growth factor 127 ) to regulate different wound healing phases. Sonic hedgehog is a prototypical morphogen that plays essential roles during the embryonic development and promotes angiogenesis in postnatal tissue remodeling. 128 Asai et al. demonstrated that topical sonic hedgehog gene vector accelerated wound healing in diabetic mice with promoted microvascular remodeling. 129 Park et al. delivered sonic hedgehog DNA intradermally as polyplexes formed with cationic poly(β-amino esters) and reported improved angiogenesis and wound healing. 130
The safety of cDNA delivery using naked plasmids has been demonstrated in a number of recent clinical studies using intramuscular injections of hepatocyte growth factor (HGF) DNA plasmids to treat critical limb ischemia.131–134 Importantly, local delivery of HGF plasmids did not cause peripheral edema and did not increase systemic HGF protein level. 132 Therapeutic benefits, including reduced pain, increased ankle-brachial index, and improved wound healing, were observed in these studies and some ischemic ulcers healed completely.131–134
cDNA transfection usually results in transient expression of exogenous genes; therefore, methods have been developed to prolong their expression. Kulkarni et al. encapsulated lipoplexes carrying eNOS encoding gene in fibrin microspheres and formed a “fibrin in fibrin” temporal release system. 135 Electrospun fibers have been immobilized with plasmids to sustainably deliver bFGF 136 and EGF. 137
Small interfering RNA
While cDNA transfection enables the production of a functional protein, small interfering RNAs (siRNAs) can silence disease-causing genes by complimentary binding to mRNA sequences of corresponding gene targets. Therefore, cDNA and siRNA can serve as controls for each other in recovery experiments.138,139 More importantly, siRNA posttranscriptional modifications have been applied to achieve transient local ablation of malignant genes at different phases of wound healing.
Chen et al. identified INT6/eIF3e as a regulator of HIF2α activity and reported that siRNA-Int6 promoted angiogenesis by accumulating HIF2α and downstream transcription of angiogenic factors in a hypoxia-independent manner. 140 Using a previously developed agarose matrix, Nguyen et al. achieved a near-complete local knockdown of p53 and accelerated wound healing in diabetic mice with upregulated vasculogenic cytokines such as VEGF and SDF-1. 141 Wetterau et al. delivered prolyl hydroxylase domain 2 (PHD2) siRNA with agarose matrix in diabetic mice and the suppression of PHD2 increased the expression of HIF1α and angiogenic regulators. 142
Remodeling phase is a therapeutic target because dysregulated remodeling results in hypertrophic and unaesthetic scars. Lee et al. first delivered Smad3 siRNA to inhibit skin fibrosis induced by radiation. 143 Similarly, Wang et al. inhibited TGF-β/Smad signaling by applying TGF-β1 receptor siRNA and reported reduced hypertrophic scarring. 144 To sustain the release of these TGF-β/Smad targeting siRNAs, delivery matrices, including trimethyl chitosan 145 and pressure-sensitive hydrogels, 146 were developed. MMP-responsive nanofiber matrix was developed for diabetic wound remodeling to control the release of MMP-2 siRNA, which restored the wound recovery rate. 147
More recently, Charafeddine et al. developed nanoparticles encapsulating siRNA to deplete Fidgetin-like 2 in vivo, which accelerated cell migration due to increased directional motility. 148 In another study, Randeria et al. demonstrated the delivery of siRNA in spherical nucleic acid-gold nanoparticles to suppress ganglioside-monosialic acid 3 synthase, a critical mediator of insulin resistance, reversing impaired diabetic wound healing. 149
MicroRNA
MicroRNAs (miRNAs) are a major group of noncoding RNAs and are important regulators of gene expression by posttranscriptional regulation. They are small and endogenously formed repressors that usually bind to the 3′-untranslated region of target mRNAs. Importantly, their interactions are noncomplimentary and a single miRNA can regulate multiple mRNAs simultaneously while a single mRNA can be regulated by various miRNAs. 150 Recent studies suggested that miRNAs play important roles in wound healing, including regulating angiogenesis, reepithelialization, and wound remodeling.151,152
Angiogenesis is critical for initiating wound healing and miRNAs have been shown as important angiogenic regulators. 153 In diabetic wounds, Chan et al. showed that downregulation of miR-200b promoted angiogenesis and accelerated healing by desilencing GATA binding protein 2 and VEGF receptor 2. 154 In another study, they described that downregulation of miR-199a-5p promoted angiogenesis both in vitro and in vivo by inducing Ets-1 and MMP-1 expression. 155
Reepithelialization has been a target for miRNA interventions as well. Biswas et al. reported that hypoxia induced miR-210 expression and downregulated the cell-cycle regulatory protein E2F3, resulting in impaired wound closure with limited keratinocyte proliferation. 156 miR-21 was reported to be induced by TGF-β 157 and promote keratinocyte migration in vitro and reepithelialization in vivo.158,159 However, Pastar et al. reported contradicting results showing that miR-21 inhibits wound healing with suppressed leptin receptor signaling. 160 miR-203 was also reported as an important regulator of mRNAs responsible for keratinocyte proliferation and migration such as RAN and RAPH1. 161 Sundaram et al. identified miR-198 as regulatory switch in controlling multiple genes to facilitate reepithelialization. 162 Li et al. identified miR-31 as another key regulator to promote keratinocyte proliferation and migration targeting epithelial membrane protein 1 (EMP-1). 163 In another study, they identified miR-132 as a regulator to facilitate transition from inflammation to proliferation phase and its implication in chronic wounds, which are stalled at the inflammation phase. 164
Remodeling is critically related to scar formation that can be caused by dysregulated collagen production and remodeling. 165 MiR-29 was identified as a key regulator of collagen expression in systemic sclerosis 166 and collagen deposit in skin fibroblasts. 167 Yang et al. reported that downregulation of miR-155 at wound sites did not accelerate wound closure, but led to a reduced fibrosis with less collagen and α-smooth muscle actin expression. 168
Biophysical cues
There is growing recognition that biophysical cues are essential regulators of cell–matrix interactions. 169 Besides intrinsic physical properties of the matrix, different instructive biophysical cues have been applied to promote tissue regeneration. Specifically, in this study, we present biophysical cues, including topographical guidance, negative pressure, electrical stimulation, and electromagnetic therapy, which have been applied in promoting wound healing.
Topographical guidance
Advances in micro- and nanoscale fabrications significantly contributed to the growing recognition of topographical guidance on cell behavior. 169 Specifically, micropatterned surfaces with arrayed grooves or cell-recognizable adhesion sites have been utilized to guide skin cell migration in vitro, mimicking reepithelialization in vivo.170–172 Using photolithography, Kim et al. made nanogrooves with various spacing distances and found an optimal spacing ratio to promote fibroblasts migration, proliferation, and ECM deposition. 171 Marmaras et al. patterned grooves of 1-μm width and 0.6-μm height and applied it apically to guide dermal fibroblast migration 170 (Fig. 2a). Fu et al. developed ultrafine fibrous network on top of polycaprolactone/collagen nanofibrous matrices by collagen coating and observed phenotype change and increased motility of keratinocytes. 172 It is of note that cell spreading and migration depend on both feature size and the spacing between.
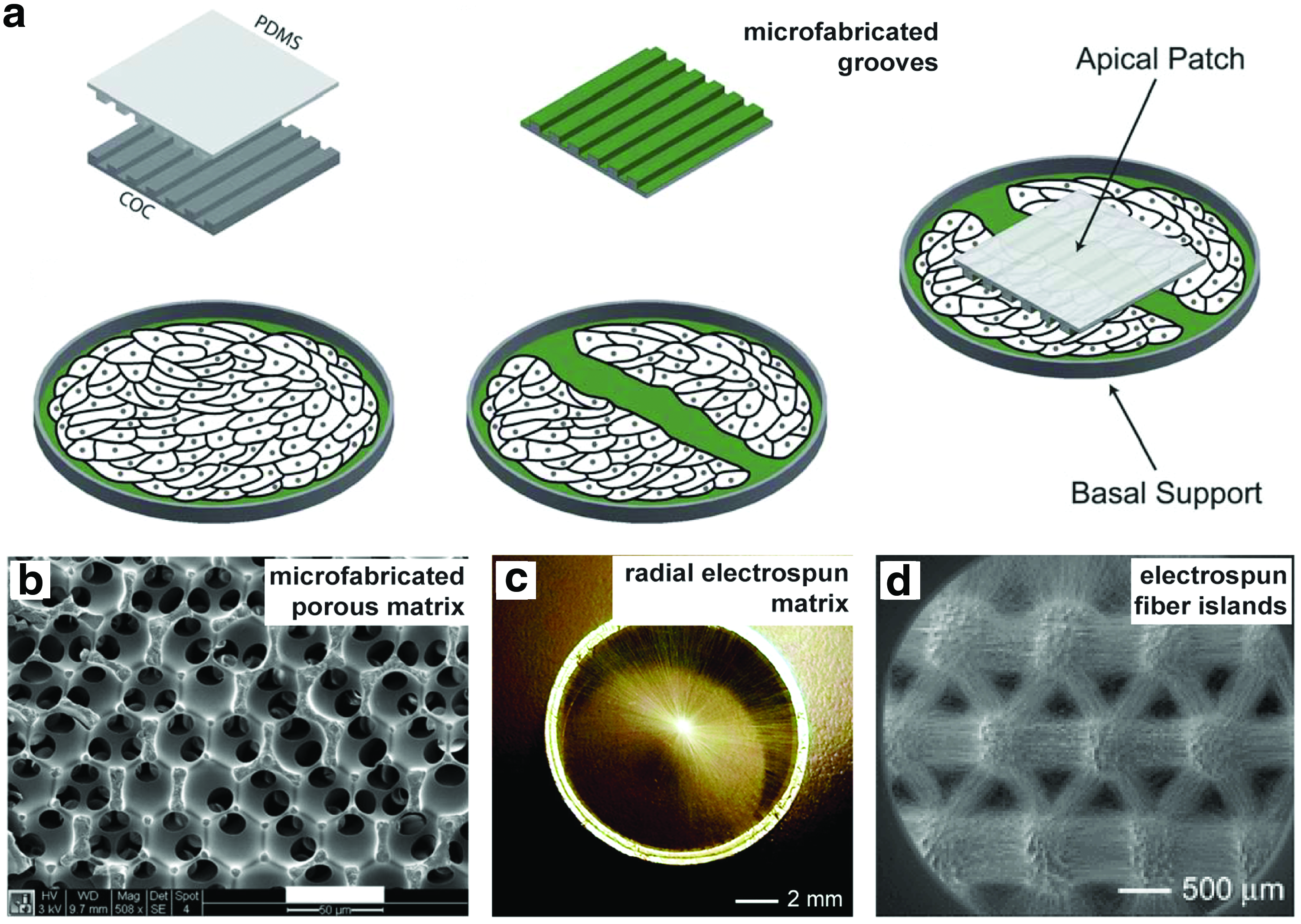
Engineered biomaterials using topographical guidance.
It has been well documented that porous biomaterials better integrate with native tissue compared with the same material fabricated into a solid form.173–175 Parkinson and Rea reported that porous anodic aluminum oxide membranes significantly improved the healing of burn injuries in pigs. 176 To investigate the effect of pore sizes, Marshall et al. developed a spherical templating method and fabricated constructs where every pore was in the same size and uniform interconnectivity (Fig. 2b). 177 By varying the pore sizes from 10- to 160-μm and investigating their integration and healing in vivo, the optimum healing characterized with maximum vascular density was obtained with 35-μm pores regardless of the polymer composition or implantation site. 177 By comparing the phenotype of macrophages on the surfaces of implants, they found activation polarization shift toward the M2 phenotype on sphere-templated implants. 178 This provides possible explanation for the improved healing and was further proved in vitro, where the monocyte/macrophage activation was significantly higher on porous surfaces. 179
Negative pressure
Topical negative pressure (TNP) therapy is a long established practice as an adjunctive therapy for chronic wounds since 1980s. 180 In 1993, Argenta and colleagues developed the V.A.C.® therapy system that generates uniform subatmospheric pressure using a proprietary reticulated foam customized into the shape of wound, a semi-permeable film to seal and maintain moisture, and proprietary track pad and tubing (Fig. 3).181,182 An intermittent therapy has been observed to achieve better healing outcomes compared with continuous negative pressure application. 182 Although there is no standard protocol yet, a negative pressure of 125 mm Hg has been suggested as the baseline setting for all wounds and lower negative pressure needs to be tailored for soft tissue to minimize potential ischemic effects. 183
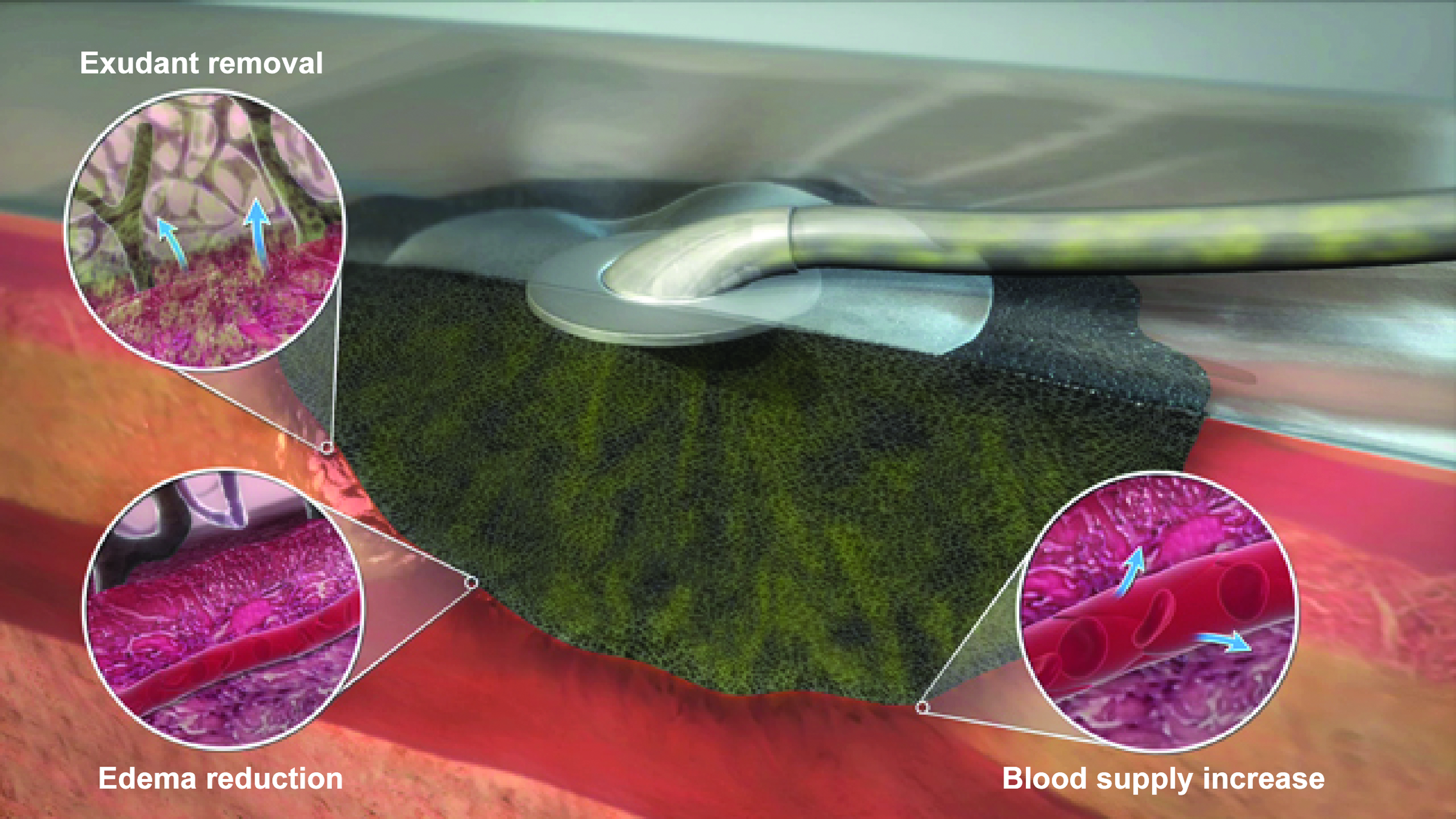
A commercially available vacuum-assisted wound closure device (KCI's proprietary V.A.C.® Therapy System). The macrostrain assists in the excessive fluid removal (arrows indicate exudant flow), tissue edema reduction, and blood flow optimization (arrows indicate vessel dilatation). Courtesy of KCI, an Acelity Company. © 2015 KCI. Color images available online at www.liebertpub.com/teb
Mechanisms that can be attributed to the benefits of TNP therapy have been investigated in basic research. The best described mechanisms are an increase in blood flow,182,184 the promotion of angiogenesis, 185 and granulation tissue formation. 186 Moreover, the local negative pressure induces deformation of ECM and generates microstrain on cells, which can promote cell proliferation and migration. Based on computer simulation, the strain levels the cells experience are comparable to the strain levels that promote cell proliferation in vitro. 187 Cyclic strain further promotes keratinocyte proliferation and migration 188 and this can be attributed to the superior outcome of intermittent TNP therapy compared with continuous treatment.
Electric stimulation
Electrical stimulation offers a safe, affordable, and facile approach for regulating cell behavior and function. 189 Electrical stimulation is a biomimicry tool in tissue regeneration representing bioelectrical signals in the body and has been widely used in wound healing applications190,191 and in the clinics. 192 Endogenous electric fields naturally arise after wounding and keratinocytes migrate in response to it, leading to wound closure. An external electrical stimulation aims to enhance the effect of naturally occurring electric fields on wound healing process. Electrical stimulation increased fibroblast proliferation and collagen synthesis both in vitro193,194 and in vivo.195,196 Moreover, electrical stimulation induced keratinocyte migration and differentiation in vitro. 197 Major clinical trials have used pulsatile waveforms or pulsed stimulations 198 and found wound healing depended on the stimulation parameters (e.g., current type, frequency, amplitude, and duration). 199 High frequency electric fields (>1000 Hz) better promote wound healing compared with low frequency ones (1–1000 Hz) because they can create polarity in the wound.
Several studies used electrical stimulation to treat diabetic wounds. Electroporation technique has been successfully used to accelerate diabetic chronic wound healing.200,201 In another study, an electrostimulation system (Fenzian™) was used for a pilot study of 21 diabetic patients with chronic ulcers. Results showed wound area and diameter decreased only in the patients who received the stimulation. 202 A bioelectric dressing that generates physiologic levels of microcurrent (2–10 μA) (Procellera®) (Fig. 4) has been reported to accelerate wound healing by promoting reepithelialization. 203 In another work, a wireless device was used to apply electrical stimulation to treat diabetic foot ulcers 204 by applying microcurrents to the wound surface noninvasively with reduced risk of infection.

Schematic diagram of design, application
Recent advances in material science and microfabrication technologies enabled us to produce smart bioelectric dressing devices with imbedded electronics for local, accurate, controllable electrical signal delivery. 205 Such devices can be used for the delivery of therapeutic agents (e.g., antibiotic drugs and RNAs) to wounds. 206 Smart and flexible bioelectronics within the device can sense and monitor physiological parameters in wound area (e.g., pH and temperature) and release therapeutic agents through electrical signals. It is hoped that such technologies would tackle current problems of chronic wound healing and play a major role in the treatment of patients with diabetic wounds.
Pulsed electromagnetic therapy
Pulsed electromagnetic therapy provides a facile, noninvasive, and safe approach for wound treatment. 207 A major trust for clinical applications of pulsed electromagnetic therapy was derived from its successful application in treating chronically broken bones. 208 In vitro studies showed that electromagnetic field affects keratinocytes and fibroblasts by upregulating a variety of genes that modulate inflammatory response. 209 Interaction of pulsed electromagnetic field with endogenous electric fields resulted in upregulation of multiple growth factors and NO, which regulated cell migration and angiogenesis. 192 Pulsed electromagnetic field increased the tensile strength of diabetic wounds in rat models. 210 The treatment significantly accelerated wound closure and reepithelialization after 10 days. A large variety of devices and protocols have been proposed and used in electromagnetic therapy, including the RecoveryRx® medical device (Fig. 5). 211 Next steps would be computerized control of electromagnetic field and real-time monitoring and assessment of its biological effects to achieve personalized treatments.
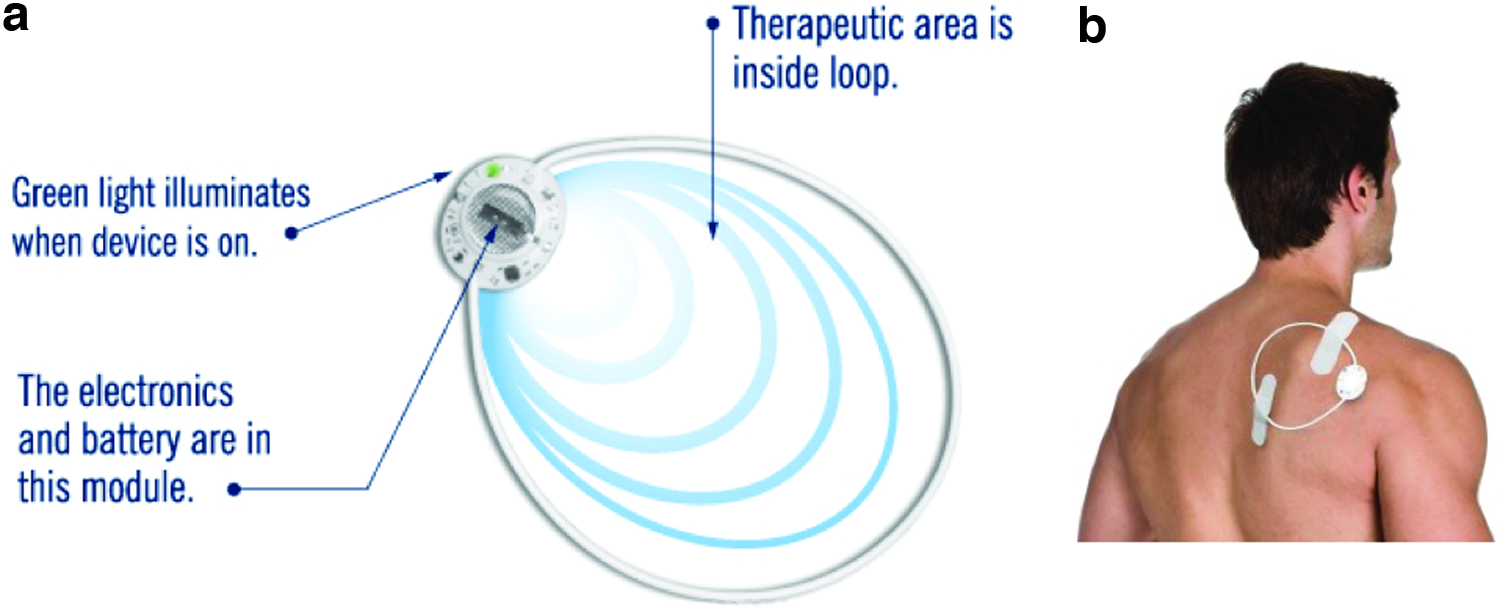
Diagram of the design and magnetic field generated by RecoveryRx® medical device
Microfabrication Technologies to Provide Biochemical and Biophysical Cues in Matrices
Recent advances in top-down and down-top microfabrication technologies have increased the versatility and resolution of these techniques in biomedicine. 212 Microfabrication technologies are able to provide biochemical and biophysical cues within biological structures mimicking the structure and function of ECM. Such biochemical and biophysical cues can regulate cell adhesion, migration, proliferation, differentiation, and ultimately, tissue morphogenesis and function. Therefore, microfabrication technologies have widely been used in different tissue regeneration applications and other biological studies. 213 In this study, we review and discuss commonly used microfabrication technologies (i.e., electrospinning, microfluidics, molecular self-assembly, and phase separation techniques) in providing biochemical and biophysical signals in wound healing matrices.
Electrospinning is a widely used microfabrication technique by which polymeric micro- and nanofibers can be made from the polymer melt or solution using electric field. The technology has a long history of development and was first proposed to produce electrospun fibers in the late 1930s. 214 Nowadays, electrospinning technology has found numerous applications in science and technology ranging from biomedicine, 215 fabrication of functional composites, 216 filtration, 217 energy, 218 and electronics. 219
In particular, electrospinning is a powerful technique to provide structures similar to the collagen structure in the ECM. For example, Rho et al. fabricated biodegradable electrospun fibers of type I collagen and used them as the wound dressing in rat models. 220 Electrospun nanofibers with different topographic features as random, aligned, nanoporous, or yarn fibers have been developed for skin tissue engineering. 221 More recently, using a collector composed of a central point electrode and a peripheral ring electrode, Xie et al. generated radially aligned electrospun nanofibers (Fig. 2c). 222 In the subsequent studies, they generated microisland arrays of nanofibers with uniaxially aligned nanofibers in between (Fig. 2d) 223 and demonstrated that the nanoscale topographical guidance promoted skin cell migration in vitro and reepithelialization in vivo. 224
Microfluidics is defined as the manipulation of small amounts of fluids in microchannels. 225 Microfluidics has influenced a wide range of research fields and applications, such as chemical synthesis, 226 biology, 227 optics, 228 and information technology. 229 The use of microfluidic systems in wound dressing matrices is primarily due to capillary or vessel formation within the matrices. 230 Such microfluidic systems can lead to the fabrication of large skin substitutes with well-controlled pore structures. Chin et al. used a microfluidic bioreactor in producing porous glycosaminoglycan-collagen gels as an artificial skin substitute. They showed that migration of fibroblasts was enhanced within the fabricated collagen because of high porosity of structures. 231 Zheng et al. fabricated a microfluidic system of alginate and collagen and used it to study vascular cell invasion in an animal wound model. 232 The system enhanced the host tissue invasion and blood vessel formation compared with uniform collagen material.
The microfluidic template can further be developed to include heterogeneous and biologically relevant structures with high fidelity in pore size and interconnectivity, which modulate the host tissue response and formation of functional blood vessels. As a novel and alternative approach, three-dimensional (3D) printing can be used to fabricate microfluidic systems within biomaterials for wound healing applications.233–235 Three-dimensional bioprinting technology is able to provide mechanically strong, scalable, and structurally integrated vascularized systems within biomaterials guiding cells to promote microvascularization.
Molecular self-assembly is defined as the autonomous assembly and organization of components initiating from the molecular level to final structure or state without external intervention.
236
Molecular self-assembly approach can be used to fabricate hydrogels of therapeutic agents.
237
Therapeutic agents in hydrogel forms can be self-deliverable or delivered using external stimuli. For example, Yang et al. fabricated supramolecular hydrogels based on
Phase separation does not require any specific equipment and is able to produce 3D and porous materials. The process is composed of five major steps as follows: material dissolution in suitable solvent, phase gelation and separation, solvent extraction from the gel, and freeze drying the remaining material. 240 The material porosity can be varied by changing the solvent. Siafaka et al. prepared sponges of chitosan with 2-hydroxyethyl acrylate through phase separation technique. The sponges loaded with levofloxacin as the wound dressing showed a great inhibitory effect on bacteria growth. 241 Mi et al. also used a phase separation technique in the preparation of chitosan films containing antibacterial agents as the wound dressing. 242 The porosity of films ensured a sustained release of antibacterial agents. In addition, porous films allowed oxygen permeability and controlled moisture of wound area and drainage of wound exudates. Phase separation technique stands as a common approach to fabricate polymeric membranes as the wound dressing. 243 However, these techniques may be time consuming and cannot be considered as completely green because of solvent residue in fabricated materials.
Concluding Remarks
Wound dressings were among the first tissue engineering products to be approved and their development was founded on wound healing biology. There is a relatively mature understanding of cell biology and cell–matrix interactions in the wound microenvironment. Commercialization of the wound dressings based on living cells was difficult and there is a consensus now that in the design of wound dressings for clinical use, the products must be user-friendly and cost-effective.
Acellular wound healing products enabled by novel technologies have been developed to deliver instructive cues to stimulate or restore the native regeneration potential and serve as promising alternatives to skin substitutes. Although numerous matrices and devices have been investigated in basic research or tested in clinical studies, optimal wound treatment still requires substantial improvement and joint effort from different fields, including biomaterial science, gene therapy, microfabrication technology, and electrical and electromagnetic engineering. Moreover, the implementation of these novel technologies and devices for clinical use requires further interdisciplinary collaboration and education of healthcare workers.
Footnotes
Acknowledgments
Our work is supported by the National Sciences and Engineering Research Council of Canada (NSERC) Steacie Fellowship to M.R., the Canadian Institutes of Health Research (CIHR) Operating Grant (MOP-126027), the Heart and Stroke Foundation GIA, NSERC-CIHR Collaborative Health Research Grant, and NSERC Discovery Grant.
Authors’ Contributions
All authors have made contributions by writing the article.
Disclosure Statement
No competing financial interests exist.