
Abstract
Background:
The regeneration of bone defects resulting from trauma, resection of tumors, infection, or congenital disease is a challenge, and bone grafts are utilized in a wide array of clinical settings to augment bone repair and regeneration. Diabetes mellitus (DM) is a chronic metabolic disease, which affects 8.3% of the world population, summing ∼387 million individuals. The consequences of the disease, for example, hyperglycemia, have been associated to a reduced capacity to form bone and poor bone quality, influencing bone healing. Our aim was to systematically review the literature to the effect of diabetic condition on bone regeneration in animal models, when using bone substitute materials from different origins, and perform a meta-analysis to quantitatively study the effect of DM on bone regeneration.
Methods:
An extensive search strategy was carried out through PubMed and EMBASE to identify the potential relevant studies published from database inception until July 1, 2015. Initially, the title and abstract of 1409 studies were screened, after which inclusion criteria sorted 29 studies for full-text evaluation. After using exclusion criteria, a final number of seven studies could be included in the review.
Results:
The seven included studies that passed our inclusion/exclusion criteria were all type 1 diabetes, comprising a total of 189 animals and 14 intrastudy comparisons. These studies presented a consistent and reduced risk of bias and showed a significant average effect size of −6.87% of bone formation for diabetes type 1 versus healthy condition [95% confidence interval: −10.55 to −3.18; I2 = 87.4%; p = 0.0003].
Interpretation:
These findings prove that DM type 1 negatively influences bone formation compared with a healthy condition, irrespective of the bone substitute material used.
Introduction
D
Type 1 diabetes (T1DM) is related to pancreatic β-cell destruction16,17 and accounts for 5–10% of the diabetic individuals.1,2,4 T1DM increases the risk of experiencing a bone fracture. 8 The occurrence of an osteopathic effect in youthful patients, even shortly after the commencement of T1DM, has led to the hypothesis that insulin works as a bone anabolic factor. The deficiency of insulin and the accumulation of advanced glycation end products (AGEs) of bone matrix proteins in T1DM are suggested to exert a negative influence on bone formation resulting in a decreased peak bone mass, as the disease often starts at a time when peak bone mass is not yet achieved.18–20
Diabetes type 2 (T2DM) is the most prevalent type of the disease, accounting for about 90–95% of the total number of diagnosed cases of diabetes.1,2,4 It is characterized by peripheral insulin resistance with a variable degree of hyperinsulinemia and impaired insulin secretion after metabolic challenge by glucose.16,21 However, in contrast to T1DM, the effects of T2DM on bone turnover remain uncertain, as in some studies, the bone mineral density was similar or even higher compared with nondiabetic patients.18,21 It is known that T2DM patients present an increased risk for bone fractures, but it has been postulated that these fractures occur as a result of diabetes complications related to eyesight and the increased propensity to fall. 22
Independent of the origin of the poor bone quality, linked to either T1DM or T2DM, the rising number of diabetic patients represent a challenge for several medical specialties, where the high number of procedures involving bone replacement or augmentation may be influenced by a delayed and/or impaired bone regeneration, directly compromising clinical outcome and increasing the number of clinical failures.20,23 Especially in dentistry and orthopedics, the use of bone substitutes in poorly controlled diabetic patients can be a contraindication in result of the impaired bone remodeling, resulting in an unsuccessful treatment.24–27
Taking into consideration the increasing number of both diabetic patients and the patients requiring bone regenerative treatment, our aim was to systematically review the literature and perform a meta-analysis with the obtained data to determine the effect of DM on bone regeneration using bone substitutes. The search strategy was restricted to animal models in result of the limited number of studies presenting histomorphometrical data of bone formation in humans.
Materials and Methods
Review protocol
A standardized protocol was followed to report and conduct the present systematic review and meta-analysis as per PRISMA and SYRCLE guidelines (Supplementary Figs. S1 and S2; Supplementary Data are available online at www.liebertpub.com/teb).28,29 The systematic literature search was conducted in July 2015 using PubMed and EMBASE databases without any restrictions on language or publication data. The search strategy had three main components: “Diabetes,” “Bone substitutes,” and “Animal studies.” For each component, the Medical Subject Headings (MeSH) terms were identified, and in addition several synonyms were searched in title or abstract. For the last component “Animal studies,” specifically designed animal filters were used.30,31 The full strategy for each individual component is presented in Table 1.
Study selection and inclusion criteria
Two reviewers (W.A.C. and J.J.J.P.B.) independently performed both phases of the study selection (title and abstract screening and full-text screening). The exclusion criteria for the title and abstract screening phase included the following: (1) not the intervention of interest (i.e., no bone substitute used); (2) not the disease of interest (i.e., DM); and (3) not an animal study. The selected studies were further reviewed during the full-text screening, in which the following additional exclusion criteria were used: (1) not an original article; (2) no bone formation data available; (3) no healthy control group; (4) no bone defect created; and (5) no bone substitute used. Disagreement between the reviewers was solved by discussion until unanimity was reached.
Data extraction and quality assessment
In each publication, we extracted the histomorphometrical data of bone formation in diabetic versus healthy animals. The following details of the included studies were also extracted: author, species/strain, age and weight, animal sex, number of animals in experimental and control group, method for establishing DM condition, type of DM, type of bone substitute, location and size of bone defect, implantation period, and outcome measures (Table 2).
“*” stands for information not available in the respective paper.
The risk of bias was assessed using SYRCLE's Risk of Bias tool. 32 Two independent investigators (W.A.C. and J.J.J.P.B.) performed quality assessment of all included studies. Disaccords were resolved by discussion.
Data synthesis and statistical analysis
Data synthesis and statistical analysis were performed using R-Project software (version 3.1.5; the R Foundation for Statistical Computing, Vienna, Austria), which was also used to create the forest plot. All data were extracted in the same unit of analysis (IS/AAR%). For each independent comparison, we calculated an effect size as a raw difference in means (MD) of IS/AAR% and corresponding 95% confidence interval (CI).
We performed predefined subgroup analysis as per protocol 33 when three or more independent articles were present. The subgroup comparisons included the following: bone substitute origin (autologous, synthetic, or xenograft), animal species/gender, bone defect location, and implantation period (<4 or >4 weeks).
For this review/analysis, a meta-analysis with inverse variance weighting was performed and was expected to be heterogeneous. Therefore, the DerSimonian–Laird estimator was applied and the random-effect estimates were used. Heterogeneity was assessed using I2.
Results
Study identification and selection
The comprehensive search strategy using the components as described in Table 1 retrieved a total of 1681 records (1151 from PubMed and 530 from EMBASE). After removing duplicates, 1409 studies remained. A total of 1382 studies were excluded based on title and abstract, that is, (1) not an intervention of interest (i.e., no bone substitute used); (2) no DM; and (3) not an animal study, which left 29 studies for full-text screening. After studying these full records, 20 studies were excluded based on the following exclusion criteria: (1) not an original study34–36 ; (2) no bone formation data34,37–41; (3) no healthy control group42–49 ; (4) no bone defect40,50; and (5) no bone substitute.51–53 Finally, seven studies were included in the meta-analysis, summing a total of 14 comparisons (Fig. 1).43,54–59 None of the included studies presented T2DM condition, only T1DM.
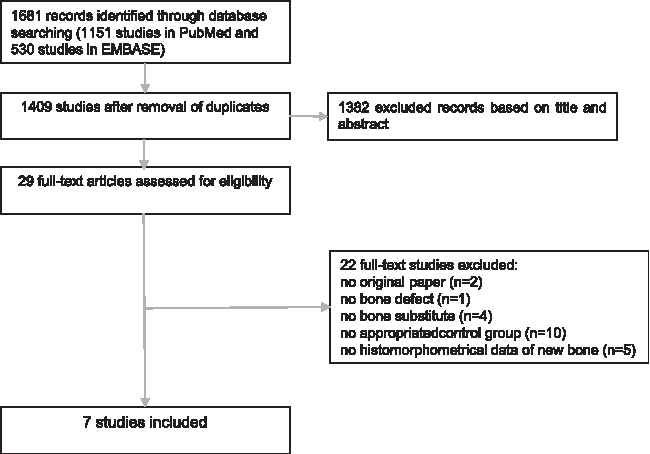
Flow diagram showing literature search and selection results.
Description of the included studies
The characteristics of all included studies are presented in Table 2, including the name of the first author/year, species/strain, age and weight, animal sex, number of animals in control and experimental group, method for establishing DM condition, type of bone substitute, location and size of bone defect, time points, and outcome measures. The studies presented a high prevalence of rodents as laboratory animals (6 out of 7),50,54–58 although the characteristics of the animals and study design differed substantially among the studies. All studies focused on T1DM. Six studies used chemical induction of diabetes, predominantly streptozotocin,50,54–56,58 and only one study used a spontaneous autoimmune model. 59 Five studies used only male animals54–57,59; one study used female animals 58 ; and one study did not mention the animal's sex. 43 Six different bony sites were chosen for the bone defect models, including segmental femoral, 57 cylindrical posterior tibial,54,55 full-thickness cylindrical calvarial, 58 cylindrical mandibular, 56 cylindrical nasal, 59 and cylindrical parietal defect. 43
A variety of bone substitutes were evaluated for bone formation, including absorbable collagen sponge + recombinant human bone morphogenic protein-2, 57 Bio-Oss®, 58 autologous bone graft, 54 salicylic acid-based poly(anhydride-esters) + freeze-dried bone allograft or only freeze-dried bone allograft, 56 hydroxyapatite,55,59 and hydroxyapatite + B-TCP. 43 Moreover, the evaluation period within the studies could be divided in short (<4 weeks43,54,56–58) and long (>4 weeks55–57,59) implantation periods.
Risk of bias and quality of included studies
The risk of bias is categorized as low, unclear, or high. Figure 2 presents the general result of the risk of bias assessment of this systematic review. In view of selection bias, 100% of the included studies reported randomization of the experimental units between treatment groups. Only 43% of the studies indicated the followed randomization method, so that the adequacy of the method could be judged. Only 29% of the studies described that control and intervention groups were identical at the beginning of the experiment, and 57% presented insufficient information. Concerning the selection bias component “allocation concealment,” only 14% described whether or not the allocation to the different groups during the randomization process was concealed. In addition, 58% and 100% of the comprised studies registered unclear risk of bias regarding to performance bias items “random housing” and “blinding, during the course of the experiment,” subsequently. In relationship to the detection bias item “outcome adequately addressed,” 86% of the studies presented low or unclear risk of bias, and only 14% of the included studies were scored as high risk of bias, failing to address the outcome.
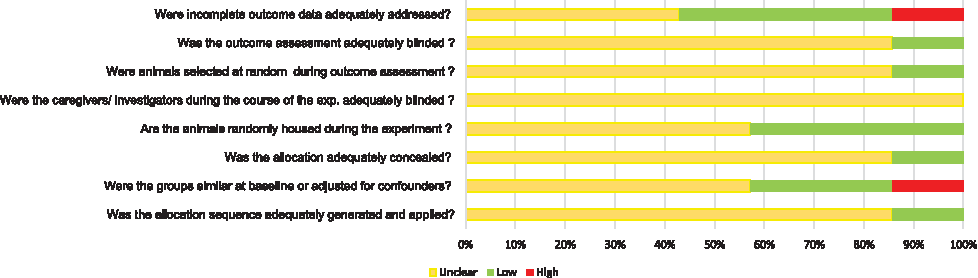
Risk of bias, average per item.
In summary, the majority of the studies presented a high number of unclear scores, which indicates incomplete information related to the study design, resulting in not fully reproducible experimental protocols and difficulty to access the actual risk of bias. In addition, one study presented high risk of bias for not using similar groups at baseline 55 and another study for not addressing the reason for the missing samples. 54
Meta-analysis of outcome measures
New bone formation
The seven included studies comprised 28 experiments or experimental groups, representing data from 189 bone defects. The overall effect of DM on new bone formation (i.e., mean difference between healthy and diabetic conditions) was −6.87% (p < 0.001) with 95% CI = [−10.55% to −3.18%], presenting considerable heterogeneity (I2 = 0.874). A forest plot of this analysis is presented in Figure 3.
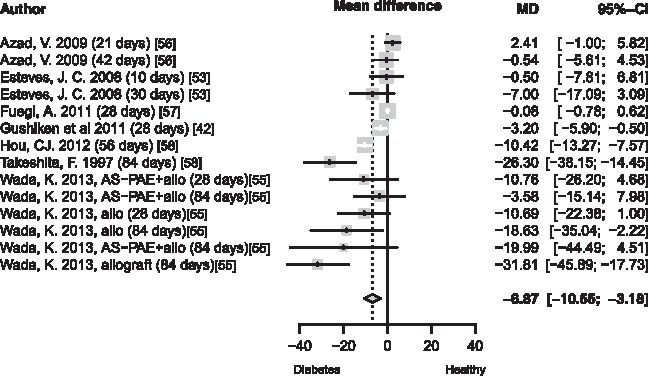
Forest plot of overall mean difference of bone formation in healthy versus diabetic condition.
New bone formation for short implantation periods (<4 weeks)
Five of the experimental groups43,54,56–58 compared diabetic and healthy conditions with an implantation period less than 4 weeks. The mean difference for DM was −1.35% (p = 0.0328) with 95% CI = [−3.75% to −1.05%], I2 = 0.563 (Fig. 4).
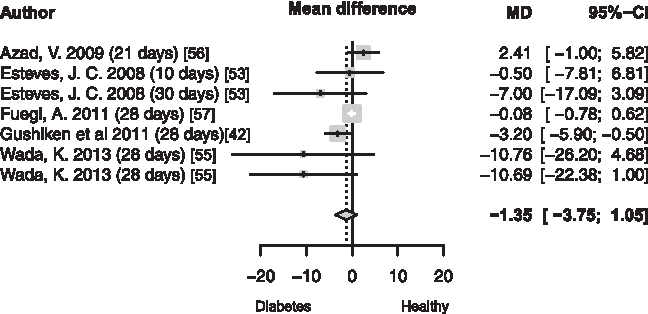
Forest plot of mean difference of bone formation during short implantation periods in healthy versus diabetic condition.
New bone formation for long implantation periods (>4 weeks)
Four of the experimental groups55–57,59 evaluated bone formation after a longer implantation period and the mean difference indicated an effect size of −13.98% (p < 0.001) with 95% CI = [−21.69% to −6.27%], I2 = 0.816, regarding bone formation for DM (Fig. 5).
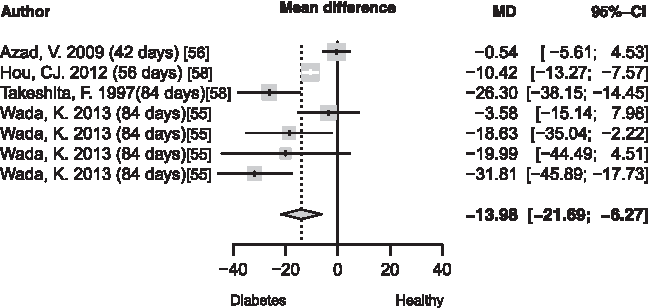
Forest plot of mean difference of bone formation during long implantation periods in healthy versus diabetic condition.
Meta-analysis comparisons regarding bone substitute origin, bone defect location, and animal species/gender were not possible due to the reduced number of studies.
Discussion
The objective of this study was to systematically appraise the prevailing evidence for the influence of DM on bone regeneration when using bone substitutes. We searched two different databases (PubMed and EMBASE) using the following search components: Bone substitutes, Diabetes, and Animals; summing an initial number of 1409 and 7 studies after implementing inclusion/exclusion criteria as described previously in this study. The findings from the present analysis demonstrate that (1) studies of bone substitute materials are usually performed in diabetes type 1 animal model and (2) the bone regeneration performance is time dependent of insulin deficiency.
We observed that in all studies T1DM was used as a study model to bone regeneration, and the reason is that many authors suggest that only T1DM can be completely related to impaired bone healing.6,60 However, different from T1DM, there are no ideal animal models to study the effects of T2DM on bone physiology, especially in small animals (i.e., rodents), because the onset of diabetes is often before skeletal maturation and bone mass is low, in contrast to what is seen in adult humans. 61
T1DM is characterized by an autoimmune destruction of the pancreatic cells, provoking lack of insulin production. This process can be easily achieved in different animal models through a variety of mechanisms, extending from chemical ablation of the beta cells to breeding rodents that spontaneously generate autoimmune diabetes. 62 The insulin deficiency leads to an increased production of proinflammatory cytokines 20 ; accumulation of glucose-mediated AGEs; and modifications related to chondrocytes, osteoblasts, mesenchymal stem cells, and osteoclasts have been observed; this results in bone loss due to a reduced bone formation and increased bone resorption.7,20,63,64 Campos Pastor et al. 65 also demonstrated that the low bone mass was caused by the lack of insulin in an uncontrolled investigation of 57 patients with T1DM, who were assessed before intensive insulin therapy and 7 years afterward. Insulin therapy led to substantial enhancement of bone turnover biomarkers and bone mass. 65
The search strategy method of this systematic review allowed an evaluation of multiple studies, which provided the means to perform a consistent meta-analysis. However, some limitations to this approach remain. Ideally, all experiments should be conducted in a similar way when their results are being combined in a meta-analysis. However, the studies present experimental variation for the utilized animal species and sex, diabetic induction method, bone defect size and type, different bone substitutes, and implantation period. Not surprising, substantial heterogeneity was found, which can be contributed, in part, to the variability between experiments.66,67 To explain the expected heterogeneity, a random-effects model was used. Furthermore, subgroup analyses (i.e., short and long implantation period; bone substitute origin; animal species/gender) were used in an attempt to explain the heterogeneity, but these subgroup analyses did not demonstrate to substantially reduce the heterogeneity.
The meta-analysis further demonstrated that diabetic experimental groups with implantation periods less than 4 weeks showed no significant effect of DM on bone regeneration. This result indicates that only after a certain period of diabetic condition the bone remodeling process starts to deteriorate. The decreased level of insulin presented in DM conditions results in hyperglycemia, which is bone anabolic and may affect bone health, affecting osteoblast and osteoclast and alter the bone remodeling process. Time of insulin deprivation is also directly linked to poor bone healing.5,20,68 As shown in this systematic review, longer implantation periods and, hence, a higher number of days under the negative influence of insulin deficiency presented an overall significant 10-fold lower rate of bone amount/mass (i.e., <4 weeks −1.35% vs. >4 weeks −13.98%). Linking this result to humans, we may assume that patients with controlled glycemic level and/or glycated hemoglobin (HbA1c) in normal range are expected to present similar bone response to subjects without DM. However, these findings require cautious interpretation, as animal models not always fully simulate the human condition.69,70
Conclusion
In conclusion, this systematic review and meta-analysis suggest that in reference to animal experimental work involving bone defects treated with bone substitutes under both diabetic and healthy conditions, T1DM has a significant negative effect (i.e., −6.87%) on bone regeneration compared with the healthy animals under the same experimental procedure using the same bone substitute material. These results provide important information to anticipate outcomes and access the risk of using bone substitute materials in poor-controlled diabetic patients, as well raise the question whether decreased bone remodeling (bone mass) is also found when animals are treated with insulin.
Footnotes
Acknowledgments
This research was supported by grant 0888/14-1 from CAPES Foundation, Ministry of Education of Brazil, Brasília—DF 70040-020.
Authors' Contribution
All authors participated in the structure of the review. W.A.C. and J.J.J.P.B. did the study selection, data extraction, and risk of bias assessment. W.A.C. prepared the first draft and the subsequent versions. All authors commented on the study design, contributed to writing, and approved the final version.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.