
Abstract
Musculoskeletal injuries are a common problem in orthopedic practice. Given the long-term consequences of unaddressed cartilage and meniscal pathology, a number of treatments have been attempted to stimulate repair or to replace the injured tissue. Despite advances in orthopedic surgery, effective treatments for cartilage and meniscus injuries remain a significant clinical challenge. Tissue engineering is a developing field that aims to regenerate injured tissues with a combination of cells, scaffolds, and signals. Many natural and synthetic scaffold materials have been developed and tested for the repair and restoration of a number of musculoskeletal tissues. Among these, biological scaffolds derived from cell and tissue-derived extracellular matrix (ECM) have shown great promise in tissue engineering given the critical role of the ECM for maintaining the biological and biomechanical properties, structure, and function of native tissues. This review article presents emerging applications for tissue-derived ECM scaffolds in cartilage and meniscus repair. We examine normal ECM composition and the current and future methods for potential treatment of articular cartilage and meniscal defects with decellularized scaffolds.
Introduction
M
Once damaged, articular cartilage and meniscal fibrocartilage have very little capacity for spontaneous healing due to their intrinsically limited blood supply. Left untreated, articular cartilage defects cause progressive joint deterioration and OA.9,10 Likewise, the knee menisci are critical structures for maintaining normal knee homeostasis and function. Loss of meniscal tissue results in decreased joint stability, congruity, load bearing, shock absorption, lubrication, and nutrition. 11 Therefore, it is well documented that meniscal deficiency leads to progressive OA, pain, and disability.12–18
Despite advances in orthopedic surgery, effective treatments for cartilage and meniscus injuries remain a common and significant clinical challenge. Given the long-term consequences of unaddressed cartilage and meniscal pathology, a number of treatments have been attempted to stimulate tissue repair or to replace the injured tissue. For instance, microfracture is a commonly employed biological intervention intended to recruit bone marrow cells that promote repair of full-thickness cartilage defects. However, microfracture-induced replacement fibrocartilage is functionally and mechanically inferior compared with hyaline cartilage.9,19–22 This lack of function, durability, and prevention of OA limits the clinical utility of microfracture and other joint resurfacing procedures to small (<1 cm2) contained defects, thus necessitating alternative procedures aimed at functional cartilage restoration. 23
While there is a general consensus to preserve the meniscus whenever possible to ensure long-term health of the knee, partial meniscectomy remains one of the most common orthopedic procedures performed. 24 In an effort to avoid the need for partial meniscectomy by improving the healing process for avascular meniscal pathology, a myriad of biological repair strategies have been reported.25–41 Among these, fibrin clot serves as a widely reported biological scaffold for meniscus repair in the avascular zone by acting as a chemotactic and mitogenic stimulus for reparative cells.25–31 In the seminal translational canine study, 2 mm defects were surgically created in the avascular portion of the medial meniscus and filled with an exogenous fibrin clot. The healing response was evaluated with histology and autoradiography over 6 months and it demonstrated repair tissue similar to fibrocartilage, whereas the control defects remained empty. 25 Furthermore, there was a significantly lower rate of failure in isolated meniscus tears augmented with an exogenous fibrin clot compared with those treated without in a clinical case series. 27 These data support the potential for avascular meniscal healing when the appropriate biological stimuli are delivered to the site of repair.
When cartilage and meniscal pathology mandate direct replacement of lost or damaged tissue, synthetic and biological tissue grafts are potential treatment options. The TruFit plug (Smith & Nephew, Andover, MA) is a commercially available synthetic scaffold designed to promote osteochondral healing and remodeling. While the scaffold resulted in improved clinical symptoms and slowed joint degeneration in human patients, there is limited evidence that support superiority or equality of TruFit compared with other standard-of-care surgical and nonsurgical treatments for osteochondral lesions.42,43 Similarly, the Collagen Meniscus Implant (CMI; Ivy Sports Medicine, Montvale, NJ) is a commercially available treatment for irreparable meniscal pathology that supports new tissue ingrowth and improves meniscal function in patients with chronic meniscal injury. 44 Neither of these synthetic scaffolds have evidence for long-term benefits and as such have not realized significant clinical use.
Osteochondral allografts and meniscal allograft transplantation are state-of-the art biological treatments for joint restoration following cartilage and meniscus deficiency.45–47 However, considerations such as type of lesion, indications, donor tissue availability, size matching, infection, immunocompatibility, graft failure, patient comorbidities, cost reimbursement, and long-term outcomes necessitate a demand for alternative strategies.46,48–53 Thus, further research and clinical efforts to improve tissue healing and improve cartilage and meniscus replacement strategies are of utmost importance. 54
Tissue engineering is a vast and ever-growing field of research with emerging strategies that aim to restore, maintain, or improve tissue function. Scaffolds are one of the three key components of tissue engineering (Fig. 1), acting as templates for tissue repair, which emulate the natural biophysical properties of the target tissue. 55 Furthermore, the extracellular matrix (ECM) has a critical role for maintaining the biological and biomechanical properties, structure, and function of native tissues. 56 ECM bioscaffolds derived from decellularized tissues have been used to promote functional tissue repair in many tissue-engineering applications.57–68 Accordingly, ECM-derived scaffolds have shown promise for repair and restoration of the articular cartilage and knee menisci as the inextricably linked fields of tissue engineering and regenerative medicine continue to advance.
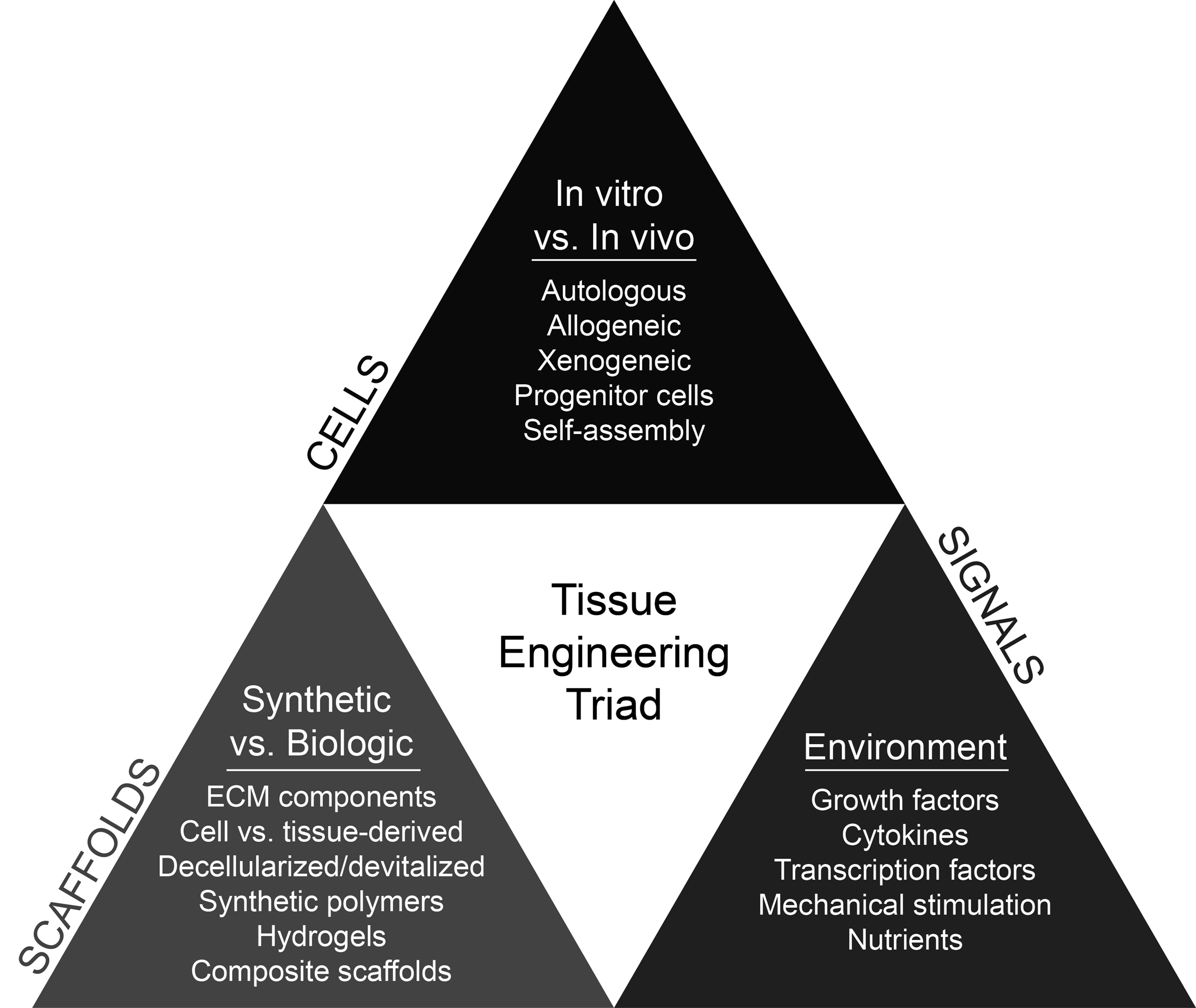
Summary of the tissue engineering triad, including examples for cells, scaffolds, and signaling molecules with potential application in musculoskeletal repair and regeneration.
The purpose of this review is to explore emerging applications for tissue-derived ECM scaffolds in cartilage and meniscus repair. An overview of normal ECM composition and current and future methods for potential treatment of articular cartilage and meniscal defects with decellularized scaffolds will be discussed.
ECM Composition and Tissue Homeostasis
The ECM is the noncellular component of tissues that provides a scaffold for cells and regulates normal tissue morphogenesis, differentiation, matrix turnover, and homeostasis.69–72 The primary ECM functions are to provide the structural support and biomechanical properties for the tissue, to act as a barrier that protects the tissue, to deliver navigational cues to migratory cells, to give signals that alter cell behavior, and to sequester biologically active compounds such as growth factors. 73 The bioactive molecules found within the ECM drive tissue repair and regulate cells through a series of cell–cell and cell–matrix interactions. 74 For instance, the ECM regulates cell adhesion and migration through receptor-mediated signaling, such as through integrin binding; it also regulates through changes in cellular and extracellular mechanical tension within the three-dimensional microenvironment.75,76 The ECM can play a major role in the control of growth factor signaling for cell proliferation, differentiation, synthesis, and remodeling of the ECM. 77 The ECM, therefore, has a profound instructive role for normal cellular activities and tissue functions through a series of specialized ligand–receptor interactions.76,78
The primary ECM components are conserved across tissues and species. These include water; proteins such as collagen, fibronectin, and laminin; integrins; glycosaminoglycans (GAGs); growth factors; and cytokines. Tissue turnover is regulated by proteolytic enzymes, matrix metalloproteinases, and tissue inhibitors of metalloproteinases. Collagens are the dominant proteins in the ECM, and collagen types I, II, and III account for about 90% of all collagen in the body. 73 Fibronectins are a family of proteins that contain binding sites for other ECM molecules, including heparin sulfate, proteoglycan, integrins, and collagen. 73 Similarly, laminins are ECM proteins that contain binding sites for cell surface receptors and other ECM molecules. 73 Integrins are critical ECM proteins that mediate cell adhesion, resist mechanical stress, and facilitate the bidirectional flow of cell signals. 79 Proteoglycans, such as aggrecan, are comprised of a core protein decorated with GAGs. The proteoglycans serve a variety of functions, including promotion of cell–ECM adhesion, sequestration of growth factors, water retention, and regulation of the movement of molecules through the ECM. Importantly, both articular cartilage and menisci are dense, ECM-rich tissues with great potential for tissue-engineering biological scaffolds. Furthermore, the matrix composition and biological properties are critical for preserving normal biomechanical function. 80
In articular cartilage, the ECM is made of hyaline cartilage and primarily composed of collagen, proteoglycans, and smaller amounts of noncollagenous proteins and glycoproteins (Fig. 2).81,82 Approximately 95% of the dry weight is composed of type II collagen. Importantly, the cells and ECM components are organized in a unique zonal arrangement that allows the tissue to retain water and maintain unique viscoelastic properties under compressive and tensile loading. 83 In the superficial zone, there are flattened chondrocytes, sparse proteoglycans, and dense collagen fibers that are tightly packed and aligned parallel to the articular surface to withstand shear stress. In the middle (transitional) zone of articular cartilage, there is a low density of chondrocytes, an increasing amount of proteoglycans, and thicker fibrils of collagen arranged oblique to the articular surface. The greatest amount of compressive resistance and load distribution occurs in the deep zone of articular cartilage, where there is the highest proteoglycan content. In the deep zone, collagen fibrils are large in diameter and arranged in a radial orientation, parallel to columns of chondrocytes, and perpendicular to the articular surface. 81

The menisci are composed primarily of water and a dense ECM combined with cells (Fig. 2).84–87 The ECM largely contains collagen, GAGs, and adhesion molecules. 86 Type I collagen is the main fibrillar component of the meniscus (80% composition of the matrix in dry weight), as well as collagen types II, III, IV, VI, and XIII.84,86 The outer zone predominantly contains type I collagen, whereas the inner (avascular) zone contains increasing amounts of type II collagen. 86
These zonal variations in collagen arrangement help to provide the mechanical functions and material properties of the meniscus. 85 For instance, bundles of type I collagen are arranged in a distinct pattern allowing them to be strong in tensile stress.88,89 The deep collagen fibers are oriented in a circumferential direction with radial tie fibers, and are continuous with the anterior and posterior meniscotibial ligaments. These attachments prevent radial extrusion and allow the menisci to maintain their structural integrity during load bearing. Elastin is another fibrillar component of the meniscus, although it comprises a small portion of the biochemical composition and its primary functions are not fully elucidated.80,84,86
The meniscus ECM is also composed of proteoglycans in a unique arrangement that enables the meniscus to absorb water and profoundly support the tissue under compression. 87 The main types of GAGs in normal menisci include chondroitin-6-sulfate, dermatan sulfate, chondroitin-4-sulfate, and keratin sulfate.86,90 Aggrecan is the primary, large proteoglycan of the meniscus, and biglycan and decorin are the main small proteoglycans. 91 The GAGs and surface zone proteins help facilitate the smooth, frictionless movement of the menisci over the articular surfaces of the tibia and femur. Furthermore, the menisci transfer compressive loads radially through their ligamentous attachments to the tibial plateau, producing a protective force known as hoop stress. Adhesion glycoproteins link the components of the ECM and cells. The primary adhesion glycoproteins in the meniscus include fibronectin, thrombospondin, and type VI collagen.92,93
During normal meniscal development, the vascularity and cellularity of the meniscus decreases, limiting the blood supply to only the periphery of the tissue (red zone). Based on its blood supply, the middle zone of the meniscus is a transitional region (red–white zone), and the inner region is the avascular (white) zone. This limited vascularity governs healing capacity and may have a huge impact on available treatment options. Therefore, surgical resection (rather than repair) following a meniscal tear is often deemed necessary. Since the amount of meniscal tissue resected directly affects the degree of joint dysfunction and subsequent OA progression, surgeons should attempt preservation and repair of the meniscus whenever possible.14,15,94 When repair with suture or other tissue fixation devices are not feasible, large resection may need to be performed and other methods for replacement or restoration of meniscal tissue may become necessary.
In tissue engineering, manipulation of components found within the ECM has emerged as an essential subset of biomimetic scaffolds, including tissue-derived ECM scaffolds that are prepared from decellularized allogeneic or xenogeneic tissues. 95 Because the ECM components differ between musculoskeletal tissues, the use of homologous orthopedic tissues as scaffolds for tissue engineering may provide tissue-specific matrix components and subsequently influence cellular recruitment, growth, and differentiation.72,96–99 Thus, the use of tissue-derived ECM biomaterials can act as a substrate for cell attachment and proliferation, and provide appropriate biochemical and physical signals for functional tissue restoration. 96
Bioscaffolds Derived from ECM
Articular cartilage
The specialized ECM of articular cartilage is critically linked to its native form and function, greatly influencing the tissue's unique biological and biomechanical properties. In recent years, scaffolds derived from cartilage ECM have gained increased attention in tissue engineering, with high potential for clinical translation (Table 1). 97 In a number of elegant in vitro studies, chondrocytes exhibited survival on devitalized and decellularized cartilage; chondroprogenitor cells were also shown to repopulate articular cartilage grafts.100–103 These studies and others demonstrate ECM cytocompatibility and the positive influence of cartilage ECM on stem cell behavior, thereby affecting cell growth, differentiation, migration, and viability.104,105 The immunocompatibility and biocompatibility of decellularized cartilage have also been demonstrated in vitro and in vivo.106,107
IHC, immunohistochemistry; ECM, extracellular matrix; ELISA, enzyme-linked immunosorbent assay; MSC, mesenchymal stem cell; SEM, scanning electron microscopy; KOOS, Knee Injury and Osteoarthritis Outcome Score; PRP, platelet-rich plasma; N/A, not applicable.
Following successful decellularization of articular cartilage, numerous studies describing production of three-dimensional, ECM-derived scaffolds have been published. Examples include processing articular cartilage into acellular sheets, layered scaffolds, delivery in hydrogels, and decellularized osteochondral allografts.108–115 Among these, decellularized osteochondral allografts have been used as scaffolds in vivo with variable success for cartilage restoration.108,109 Chondrofix® (Zimmer Biomet, Warsaw, IN) is an FDA-approved biologic treatment composed of decellularized hyaline cartilage and cancellous bone. While clinical data are limited to support its use, a recent case series (58 patients, 61 knees) reported satisfactory patient outcomes at short-term follow-up. 111 In another case series, human patients were treated with a decellularized osteochondral allograft for cartilage knee injuries and 23/32 knees (72%) were considered failures within the first 2 years of implantation. 110 Accordingly, the use of decellularized osteochondral allografts for focal cartilage defects has demonstrated an overall lack of efficacy in preclinical and clinical case series. To overcome these limitations, further studies to delineate the optimal processing methods and indications for ECM scaffold use in cartilage repair and restoration need to be defined.
Effective decellularization is dependent upon tissue-specific factors, including cellularity, density, thickness, and lipid content. 116 While there is no current standard method for decellularization of articular cartilage, many techniques have been reported and have been comprehensively summarized.74,97,98 It is beyond the scope of this article to describe production of in vitro, cell-derived cartilage ECM scaffolds. 95 Techniques to produce tissue-derived ECM scaffolds include chemical, physical, and enzymatic decellularization methods, or combinations thereof, to isolate articular cartilage matrix. 97 Depending on the processing method, the cells and cellular components may not be completely removed from the decellularized tissue. Therefore, the immunogenic properties of the scaffold and regulatory standpoints need to be considered for optimal clinical translation, especially for evaluation of xenogeneic scaffolds.
Chemical decellularization uses detergents and other chemicals to result in a significant decrease in cells, cell nuclei, and DNA content from the tissue. However, there is also a loss of biochemical content, such as sulfated GAGs, and reduction in material properties. 101 Therefore, cartilage ECM scaffolds may be combined with other scaffolding materials to form composite scaffolds, to engineer scaffolds that more closely resemble the native tissue's biological and biomechanical properties. 117 Further work is necessary to determine whether these data translate to functional cartilage restoration in vivo.
Given the dense ECM of articular cartilage, cellular repopulation and infiltration into the deep zone of decellularized scaffolds are not always efficient or feasible without causing disruption of the biochemical composition and material properties.97,116,118 Therefore, use of particulate cartilage ECM scaffolds has also been described.105,119–122 Physical decellularization methods, such as freeze–thaw processing or mechanical abrasion, may more effectively preserve the native tissue's biochemical properties. 97 Furthermore, disruption of the cartilage macrostructure may improve the chondroinductive behavior of the issue and improve cellular infiltration and migration within the scaffold given the otherwise nonporous structure of acellular articular cartilage.112,123 While one must consider the intended application of the scaffold and delivery options, particulate ECM scaffolds may promote superior cellular integration and enhanced chondrogenesis in articular cartilage defects. 120
When cultured on porous, devitalized cartilage scaffolds, human adipose-derived stem cells differentiated into a chondrogenic phenotype with or without genipin crosslinking, producing ECM with an increasing aggregate modulus after 28 days of culture.67,119 In another study, particulate ECM from shattered articular cartilage demonstrated in vitro cell adherence, proliferation, and differentiation of bone marrow-derived mesenchymal stem cells (MSCs) with evidence of in vivo matrix production in a subcutaneous mouse model. 121
BioCartilage (Arthrex, Inc., Naples, FL) is a commercially available, FDA-approved product that holds promise for repair augmentation of articular cartilage defects. 124 BioCartilage is a biological scaffold derived from allograft articular cartilage that has undergone proprietary physical processing; this results in a particulate ECM. The scaffold contains key components of articular cartilage ECM, including type II collagen, proteoglycans, and growth factors. BioCartilage is indicated for augmentation of cartilage repair with concurrent microfracture. 125 In a preclinical equine model, BioCartilage was combined with platelet-rich plasma to augment healing of 10-mm, full-thickness cartilage defects in the trochlear ridge of both knees. 126 Outcomes at 13 months included serial arthroscopy, MRI, micro-CT, and histology. No complications were reported and the augmented defects exhibited improved cartilage repair compared with microfracture alone. Clinical data to support the use of BioCartilage in human patients are limited to a few case reports.127,128 However, a prospective clinical trial to compare BioCartilage versus standard-of-care marrow-stimulating procedures for knee cartilage defects is under investigation. 129
In summary, decellularization affects tissue microstructure, including collagen II and proteoglycan content, and the choice of processing method is largely influenced by the intended clinical application. For instance, physical decellularization methods, such as cryogrinding, for preparing particulate ECM scaffolds are an emerging alternative to complete decellularization and preparation of full-thickness grafts, with promising in vivo results for cartilage repair augmentation. Given the inherently dense composition of articular cartilage, fabrication of particulate scaffolds may have less adverse effects on biochemical composition than chemical decellularization of full-thickness tissue, and promote more uniform cellular adhesion and expansion within the scaffolds in vivo. 118 However, the immunogenicity of decellularized articular cartilage remains to be explored given the potential for reactions to remaining cell membranes or other cellular components, and regulatory aspects should be considered in designing future in vitro experiments and preclinical studies.
Menisci
Preparation of decellularized scaffolds for application in meniscus repair and replacement is a relatively new area in tissue engineering research (Table 2). The intact menisci are critical structures for maintaining normal knee joint homeostasis and function. The highly specialized ECM of the meniscus is necessary for support of the complex biological and biomechanical properties. Therefore, recapitulating normal meniscus structure and function following resection or injury poses a unique challenge. Accordingly, tissue engineering with scaffolds similar to native fibrocartilage brings promise for treatment of meniscal defects that have no viable treatment options available. A decellularized meniscus has also been suggested as a scaffold to support cartilage repair. 130
SEM, scanning electron microscopy; SDS, sodium dodecyl sulfate.
Several published reports describe decellularization methods and characterization of decellularized meniscal tissue. Stapleton et al. described a method for decellularizing porcine menisci with 0.1% sodium dodecyl sulfate. They noted a 59.4% loss of GAGs after decellularization, but no change in the histoarchitecture or biomechanical properties. In addition, the scaffold was biocompatible based on contact cytotoxicity and extract cytotoxicity tests. 65 In a follow-up investigation, the acellular porcine meniscal scaffolds supported the attachment and infiltration of human fibroblasts and porcine meniscal cells. The scaffolds also demonstrated in vivo immunocompatibility in galactosyltransferase knockout mice. 66
Maier et al. described a method for decellularization of sheep menisci with an enzymatic process. Complete cell removal was observed with histology and scanning electron microscopy, with preservation of significant viscoelastic material properties. The scaffold was cytocompatible to autologous fibrochondrocytes and supported cellular adhesion and survival within the scaffold after 4 weeks of culture. 131
Sonication decellularization has also been reported to prepare decellularized meniscus bioscaffolds with no significant reduction in biomechanical properties. 132 Sheep menisci underwent a multistep decellularization process followed by in vitro cytotoxicity testing. The scaffolds were biocompatible and had increased porosity and secondary ECM changes, but retained biomechanical properties. 133 Decellularized porcine medial menisci also maintained their biomechanical properties with higher permeability and a lower elastic modulus compared with native menisci. 134 Similar data have also been reported for decellularized human menisci. 135 It is uncertain how any of the mentioned changes to matrix composition and biomechanical properties would affect the biocompatibility and material properties of decellularized meniscal grafts in vivo.
Acellular collagen-based biomaterials, including porcine subintestinal submucosa, have previously shown promise to enhance meniscus repair. However, the investigations have been limited to animal models.39–41,136,137 Therefore, further research endeavors are indicated to explore the potential utility of acellular bioscaffolds in meniscus repair and replacement. Emerging applications for decellularized meniscal scaffolds include the use of a meniscus-derived ECM hydrogel. Wu et al. developed an injectable ECM hydrogel from enzymatically decellularized porcine meniscus. The hydrogel was easily injected with tunable compression properties. In addition, the hydrogel was cytocompatible and promoted growth of bovine chondrocytes and mouse 3T3 fibroblasts after 8 weeks of culture. The scaffold was also cytocompatible in vivo in mouse subcutaneous tissue. 138 These data may hold promise for future application of ECM-derived biomaterials in meniscus repair.
Similarly, we have recently described a method for the fabrication of a novel scaffold derived from particulate, meniscus ECM for potential augmentation of full-thickness meniscal defects. 139 Canine medial and lateral menisci were decellularized with a combination of chemical and physical treatments and then cryoground into a powder, with no significant reduction of collagen content in the scaffold. Cytotoxicity assays showed that the scaffold was cytocompatible to meniscal fibrochondrocytes, synoviocytes, and whole meniscus tissue. The scaffold promoted cellular survival and proliferation ex vivo. Future studies are aimed at evaluation of the scaffold's potential to induce cellular differentiation and functional meniscal fibrochondrogenesis.
In summary, a handful of experimental studies have emerged that investigate the fabrication and initial safety of decellularized meniscal scaffolds with variable physical properties and potential application. Decellularized scaffolds are advantageous in tissue engineering since they theoretically maintain meniscal geometry for partial meniscal replacement, or could provide the appropriate signals for fibrochondrogenesis and meniscal repair by preserving the native ECM. 140 However, given the unique challenges involved in effective decellularization of the meniscus with preservation of the native tissue's structure and function, an optimal strategy for preparation–and well-defined indications–for decellularized meniscal scaffolds has yet to be discovered. Future research endeavors are necessary to investigate the biological potential for acellular meniscal scaffolds to undergo cellular repopulation in vivo, with exploration of graft survival and the clinically relevant biomechanical properties.
Conclusions and Future Directions
Evaluation of tissue-derived ECM scaffolds is a growing area of research in orthopedic tissue engineering; it shows great potential for repair and restoration of articular cartilage and meniscal defects. Physical decellularization methods, such as cryogrinding, for preparing particulate ECM scaffolds are a potential alternative to complete decellularization of full-thickness grafts, with promising in vivo results for cartilage repair augmentation. These methods provide the bioactive cues necessary for cellular survival, proliferation, and differentiation. While there are limited commercially available, off-the-shelf treatment options available for clinical use, micronized allogeneic cartilage holds promise for augmented repair of focal osteochondral defects and is under clinical investigation.108–111,124–129 Further studies are necessary to delineate the optimal processing methods and indications for the use of ECM scaffolds for cartilage and meniscal defects. Overall, tissue-derived ECM scaffolds are promising biomaterials in cartilage and meniscus tissue engineering. The likelihood for regulatory approval and immediate clinical application is favorable.
Footnotes
Acknowledgments
The authors wish to thank Steve C. Friedman, senior editor, University of Missouri, for his extensive editorial contributions and Stacy T. Cheavens, certified medical illustrator, University of Missouri, for creating the figure illustrations.
Disclosure Statement
No external funding was used in this study and the authors have no potential financial interest in this review. JLC is a patent holder with royalties on BioCartilage-related materials.