
Abstract
The torn rotator cuff remains a persistent orthopedic challenge, with poor outcomes disproportionately associated with chronic, massive tears. Degenerative changes in the tissues that comprise the rotator cuff organ, including muscle, tendon, and bone, contribute to the poor healing capacity of chronic tears, resulting in poor function and an increased risk for repair failure. Tissue engineering strategies to augment rotator cuff repair have been developed in an effort to improve rotator cuff healing and have focused on three principal aims: (1) immediate mechanical augmentation of the surgical repair, (2) restoration of muscle quality and contractility, and (3) regeneration of native enthesis structure. Work in these areas will be reviewed in sequence, highlighting the relevant pathophysiology, developmental biology, and biomechanics, which must be considered when designing therapeutic applications. While the independent use of these strategies has shown promise, synergistic benefits may emerge from their combined application given the interdependence of the tissues that constitute the rotator cuff organ. Furthermore, controlled mobilization of augmented rotator cuff repairs during postoperative rehabilitation may provide mechanotransductive cues capable of guiding tissue regeneration and restoration of rotator cuff function. Present challenges and future possibilities will be identified, which if realized, may provide solutions to the vexing condition of chronic massive rotator cuff tears.
Introduction
T
The risk of repair failure (i.e., re-tear) is correlated with muscle degeneration, tear size, and patient age, all of which increase with tear chronicity.7–9 With propagation of a chronic rotator cuff tear, the unloaded muscles undergo degenerative changes, including increased fibrosis and fatty infiltration, which causes further medial retraction of the tendon edge.1,10 Concurrently, bone density of the humeral head decreases in the absence of mechanical stress.11,12 As a result, increased repair tension is required to surgically appose the tendon to the anatomical footprint of the now osteoporotic humeral head, both of which compromise repair integrity.10,13,14 Furthermore, the complex structure of the tendon–bone interface (i.e., enthesis) is not restored following surgical repair,15,16 causing a focal stress concentration as the compliant tendon abruptly adjoins stiff bone. Taken together, these factors predispose the surgical repair to fail, which occurs most frequently at the suture–tendon interface. 17 Moreover, the repair strength is further reduced due to the compromised tendon quality found in chronic tears (Fig. 1). 18
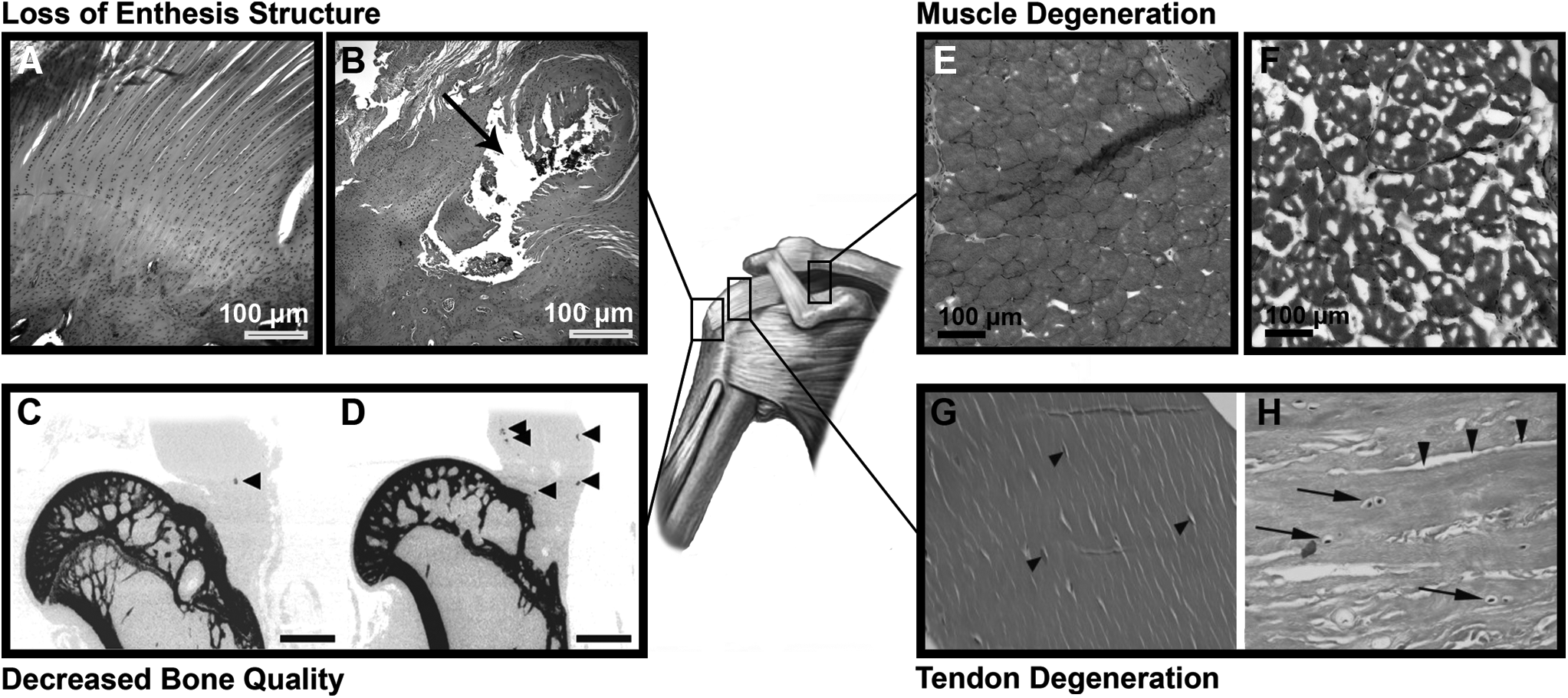
The effect of chronic, massive tears on the elements of the rotator cuff organ. The native enthesis
Novel surgical techniques have been developed in an effort to improve footprint coverage and reduce shear stresses at the suture–tendon interface, theoretically enhancing healing at the interface and reducing repair failure.19,20 While these techniques have shown promise in studies with cadaveric specimens, clinical studies have not consistently found improvements in structural healing or functional outcomes.21,22 The discrepancies between in vitro and in vivo findings suggest that increases in initial repair strength are insufficient to restore the integrated structure and function of the tissues that comprise the rotator cuff organ, including muscle, tendon, enthesis, and bone. Indeed, the degenerative muscle changes seen in chronic rotator cuff tears, including fatty infiltration and atrophy, do not improve despite successful surgical repair (i.e., no evidence of re-tear) and correlate with poor functional outcomes. 23 If progress is to be made in reducing the re-tear rate and improving clinical outcomes following repair of chronic massive rotator cuff tears, therapeutic strategies must address not only the mechanical integrity of the surgical repair but also the restoration of tissue structure, anatomy, and function.
This review highlights the recent progress made in the application of tissue engineering strategies, including the independent or combined use of cells, scaffolds, and biomolecules (e.g., growth factors, gene therapy), to enhance healing of the tissues that comprise the rotator cuff organ—muscle, tendon, enthesis, and bone. While preclinical results are promising, an emerging understanding of both rotator cuff development and healing suggests that therapeutic strategies for treating individual tissues of the rotator cuff organ might provide synergistic benefit if combined. Moreover, the timing and delivery of these strategies must be considered in the context of current surgical techniques and rehabilitation protocols.
Tissue engineering strategies to augment rotator cuff repair have focused on three principal aims: (1) immediate mechanical augmentation of the surgical repair, (2) restoration of muscle quality and contractility, and (3) regeneration of native enthesis structure. Work in these areas will be reviewed in sequence, highlighting the relevant pathophysiology, developmental biology, and biomechanics, which must be considered when designing therapeutic applications. Thereafter, the role of mechanical loading, as might be controlled through postoperative physical therapy, will be discussed as a rehabilitative stimulus to promote restoration of the integrated tissues that comprise the rotator cuff organ. Present challenges and future possibilities will be identified, which if realized, may provide solutions to the vexing condition of the treatment of chronic massive rotator cuff tears.
Mechanical Augmentation of the Surgical Repair
Rotator cuff repairs fail most commonly in the early postoperative period (within the first 6 months)24–26 when the suture shears through the tendon. 17 Consequently, there has been considerable effort to develop novel strategies to increase the early strength of surgical repairs in hopes of reducing failure rates. Improved suture techniques, most notably the double row and its derivatives, have been shown to increase repair strength when loading cadaveric specimens to failure, but when applied clinically, neither reductions in re-tear rates nor enhanced shoulder function have been reported, as shown in meta-analyses.19–22
An alternative strategy to improve the mechanical strength of rotator cuff repairs is to augment the surgical repair with a scaffold,27,28 which could also serve as a delivery vehicle for cells and/or biomolecules intended to restore tendon quality. 29 To offload the repair, thereby improving failure mechanics, the scaffold should possess (1) material properties approaching those of the native tendon, and (2) suture retention strength equal to, or exceeding, that of the nonaugmented repair.30,31 When incorporated into surgical repairs of cadaveric human shoulders, both tissue-derived32–34 and synthetic 35 scaffolds have been reported to reduce gap formation upon cyclic loading while also enhancing ultimate failure load. In doing so, the mode of failure shifted from suture pull-through to suture breakage.34,35
Application of these scaffolds in large animal models demonstrated benefit in vivo as well. For instance, augmentation of an acutely transected and repaired infraspinatus tendon with a reinforced fascia patch (derived from human fascia lata) in a canine model increased the ultimate load at time 0 by 46%, as compared to nonaugmented repairs.
36
However, this advantage in mechanical strength provided by scaffold augmentation dissipated by 12 weeks, at which time there were no differences between groups.
36
Conversely, repair augmentation with a poly-
A similar pattern is seen in clinical studies. While several case series have documented improved shoulder function (both objective and patient-reported) following scaffold augmentation of rotator cuff repairs,40,41 only two prospective randomized trials have been performed (Table 1). Augmentation of surgical repairs of large and massive chronic rotator cuff tears with a porcine SIS patch (Restore; DePuy Orthopaedics) did not improve the rate of tendon healing or clinical outcomes scores, with a trend toward impaired healing in the augmentation group.
42
In a similar case–control study, no benefit was found when employing the same porcine SIS patch, but a pronounced inflammatory reaction to the xenograft was observed.
43
On the other hand, when repairs of large, but not massive, rotator cuff tears (i.e., 3–5 cm) were augmented with acellular human dermal matrix (GraftJacket; Wright Medical Technology), the healing rate and outcome scores were significantly greater than nonaugmented repairs.
44
Repair augmentation with synthetic scaffolds, such as those composed of biodegradable poly-
No clinical studies investigating cell or pharmaceutical strategies for reversing muscle degeneration were identified. Reviews of preclinical studies are not included here, but have focused on scaffold augmentation,31,57 tendon-bone healing,109,235 and muscle regeneration. 198
AG, augmented group; CG, control group; HG, high grade degeneration of both infraspinatus and supraspinatus; LG, low grade fatty degeneration of infraspinatus but high grade degeneration supraspinatus; MG, microfracture group; MPG, marrow stimulation and patch group; MRI, magnetic imaging resonance; MSC, mesenchymal stem cell; MSCG, mesenchymal stem cell group; PENN, PENN shoulder score; RCT, randomized controlled trial; SIS, small intestine submucosa; UCLA, University of California at Los Angeles score; US, ultrasound; VAS, visual analog scale.
For large to massive rotator cuff tears deemed irreparable, reconstruction with an interpositional auto/allograft has been employed to restore continuity between the humeral head and the torn rotator cuff. As reported in several cases series, reconstruction of massive tears with dermal tissue allografts improved pain and function in patients with minimal preexisting glenohumeral arthritis.47,48 Similarly, reconstruction with a fascia lata autograft reduced re-tear rates and improved clinical scores and strength as compared to partial repair in a cohort study of patients with large to massive irreparable tears and low-grade fatty degeneration of the infraspinatus muscle. 49
Given the anatomical proximity of the superior glenohumeral capsule and rotator cuff tendons, the former is often damaged concomitant with rotator cuff tears. 50 Reconstruction of the superior capsule has been shown in cadaveric models to restore stability, reducing the superior migration of the humeral head that often results from massive rotator cuff tears.51,52 In a limited number of case series, superior capsule reconstruction grossly restored superior glenohumeral stability and improved shoulder function, as reported by patients.53,54 Similar to augmented repairs, long-term outcomes following rotator cuff or superior capsule reconstruction are lacking.
As suggested by the equivocal results found across preclinical and clinical studies, consistent enhancement in surgical outcomes mediated by scaffold augmentation of rotator cuff repairs or reconstruction will require more than mere optimization of a scaffold's mechanical properties. In particular, the immune response to an implanted scaffold, particularly one derived from allo- or xeno-geneic tissue sources, appears to have a great influence in mediating any beneficial (or adverse) effect. The presence of cells 55 and nonhomologous protein epitopes56,57 in certain xenograft scaffolds may explain the null effects of scaffold augmentation noted above, as both have been associated with an M1 (proinflammatory) macrophage response, which can lead to poor healing and excessive scar tissue formation.58,59 At the same time, the ultrastructure and biochemical composition of scaffolds differentially affect the phenotype of tendon fibroblasts, with subsequent influence on extracellular matrix (ECM) deposition and scaffold remodeling. 60 Novel scaffolds designed to match the mechanical, topographical, and biochemical properties of native tendon, with resulting promotion of a tenogenic cell phenotype, have been recently reported but their in vivo effects remain unexplored.61,62
Additional consideration should also be given to the quality of the tendon tissue itself. Retracted tendons, as seen in chronic rotator cuff tears, exhibit frank deterioration characterized by increased collagen fibril crimp and collagen fibril atrophy and disorganization. 63 Similarly, cell apoptosis is seen throughout degenerated tendon,64,65 with concurrent elevations in inflammatory and catabolic mediators.66,67 These degenerative changes not only weaken the suture retention strength, thereby predisposing to surgical failure, 18 but also impair healing. Namely, it was recently reported that the severity of tendinosis, rather than tear size or fatty infiltration, was the greatest predictor of repair integrity at least 6 months after surgery. 68 Compromised tendon quality likely contributes as well to “failure with continuity,” in which there is no overt defect in the repaired rotator cuff tendon, yet the musculotendinous junction is medially retracted with associated disruption of muscle mechanics. 69
Chemical cross-linking of the degenerated tendon may enhance failure properties 70 but likely interferes with tissue remodeling and the restoration of native tendon structure and function. 58 Conversely, cell- and pharmaceutic-based therapies have shown benefit in reversing tendinopathic changes.71,72 However, animal models with chronic degenerative changes in the tendon have only recently been developed,73–75 with few studies exploring the effect of scaffold augmentation. An investigation in a chronic ovine model found that augmentation of a rotator cuff repair with polyurethane scaffold mesh (Biomerix RCR Mesh; Biomeric Corp.) increased the force at failure compared to nonaugmented controls at 12 weeks, but further analysis of tendon structure was not performed. 76 In a cohort study, the effect of augmenting arthroscopic repairs of large to massive rotator cuff tears with a fascia lata autograft patch was evaluated, distinguishing between shoulders with low-grade and high-grade fatty infiltration. 77 Interestingly, patch augmentation was not beneficial for massive tears with high-grade fatty infiltration, 77 highlighting the importance of considering the muscle quality when applying tissue engineering strategies intended to support the healing tendon–bone interface. To that end, restoring the structure and function of the degenerated muscle in the context of a chronic rotator cuff tear may further enhance the benefit of a scaffold applied to augment the surgical repair.
Restoration of Muscle Quality and Contractility
Unfortunately, progressive deterioration in muscle quality is seen with increasing severity (and chronicity) of rotator cuff tears. 78 These degenerative changes, including muscle atrophy, fibrosis, and fatty infiltration, increase muscle stiffness79,80 and necessitate higher repair tension, which increases the risk for re-tear. 81 Stress deprivation of the humeral head in the context of chronic tears compromises bone density and architecture,11,82 which further contributes to poor healing. 83 Yet even with successful surgical repair, as defined by the continuity of tendon to bone on imaging, the degenerative changes in muscle are considered irreversible.23,84–88 Beyond increasing the risk for repair failure, muscle degeneration is directly correlated with clinical outcomes,7,89 likely due to adverse effects on musculotendinous mechanics, including disruption of myofibril architecture and reductions in contractility. 90 As a result, early rotator cuff repair is advocated in an effort to halt further muscle degeneration.87,91–93
The etiology and pathogenesis of muscle degeneration are multifactorial.94–96 It was hypothesized that increasing medial tendon retraction in the context of a chronic tear places undue tension on the suprascapular nerve as it passes through the suprascapular notch, resulting in a stretch-induced neuropathy. 97 However, the association of suprascapular neuropathy (SSN) with rotator cuff pathology remains unclear; SSN is correlated with tear size, but not fatty degeneration.98–100 Furthermore, the morphological patterns of fatty infiltration differ when comparing muscle changes following massive rotator cuff tears against those seen in isolated SSN. 101 Nevertheless, animal studies have consistently found worse muscle degeneration with combined tendon tear and neuromuscular compromise, induced by injecting Botulinum toxin A74,79,80 or transecting the suprascapular nerve.102,103 The necessity of chemical or surgical denervation to induce pronounced fatty infiltration and fibrosis following tendon transection in small animal models may be due to the robust scar formation that prevents muscle unloading to the same degree seen in human shoulders in which there is minimal scar formation.80,104 This may contribute to the noted differences between animals as passive muscle biomechanical properties influence motor endplate properties 105 and satellite cell behavior. 106 Additionally, the rotator cuff muscles may be particularly sensitive to denervation, as compared to other muscle groups, 107 although the mechanisms underlying such discrepancies remain uncertain.
Other studies have sought to elucidate the alterations in gene expression,104,108–110 proteostasis,111,112 and inflammation,111,113,114 underlying the noted structural and functional deficits. The Akt/mammalian target of rapamycin (mTOR) pathway has been implicated in both muscle atrophy and fatty infiltration following tendon rupture and/or denervation. 115 Regarding the latter, Akt/mTOR has been shown to regulate the transcription factor sterol regulatory element binding protein 1 (SREBP-1) and its downstream mediators of adipogenesis, peroxisome proliferator activated receptor gamma (PPARγ) and CCAAT/enhancer-binding protein alpha (C/EBPα).108–110 While PPARγ and C/EBPα are likely instrumental in promoting adipogenic differentiation in putative progenitor cells, the resulting ectopic fat accumulation may occur through noncanonical intramyocellular lipid storage and synthesis pathways. 116
At the same time, upregulation of transforming growth factor-beta (TGF-β) signaling is likely causative in promoting increased fibrosis following injury104,117 while also mediating some effect on fatty infiltration. 118 There is emerging data to suggest that the p38 mitogen-activated protein kinase (MAPK) molecule orchestrates many of these changes, as inhibition of p38 MAPK in a rodent model of a degenerative rotator cuff tear significantly reduced fibrosis and the accumulation of intramuscular lipid. 119 However, muscle is comprised of numerous cell types beyond the contractile myofibers, with each differentially contributing to the restoration or compromise of muscle function following cuff injury.
The satellite cell is central to muscle homeostasis, providing a reserve of renewable progenitor cells that can differentiate into contractile myocytes. Recent work has shown that the age-associated reduction in regenerative capacity of the muscle is at least partially attributable to cell-autonomous defects in satellite cell function driven by increased p38 MAPK signaling.120–122 Given the role of increased p38 MAPK in promoting fibrosis and fatty infiltration of muscles following rotator cuff tear, 119 it is reasonable to speculate that aberrant satellite cell function contributes to tear-induced degenerative changes, but definitive studies have not yet been performed. Furthermore, the sources of cells that ultimately become the adipocytes and fibroblasts of the degenerated muscle are unclear. Recent work found that Tie2+ muscle mesenchymal progenitors were the major source of fibroblasts while PDGFRα+ fibro/adipogenic progenitors (FAPs) principally became adipocytes following rotator cuff tear, 123 yet related work showed that FAPs can become fibroblasts as well. 124 Interestingly, FAPs appear to facilitate myogenic differentiation of satellite cells in healthy muscles but contribute to ectopic fat formation when the muscle is injured, suggesting the importance of environmental factors in mediating FAP function.124,125
Paracrine signaling from macrophages, as opposed to lymphocytes, 114 also contributes to degenerative changes, with prolonged macrophage infiltration worsening fibrosis and fatty infiltration following rotator cuff tears.111,113 A detailed understanding of how signaling networks and cellular composition evolve over location and time during rotator cuff disease pathogenesis will be essential for developing targeted therapeutic interventions. Differences in gene expression were found when comparing distal to proximal regions of the rotator cuff muscles following injury, 104 while upregulated expression of many genes in full thickness tears were noted to be largely blunted in massive tears, 110 perhaps contributing to the diminished healing capacity found with increasing tear size.1,102
Although much remains to be understood about the mechanisms of muscle degeneration, a growing body of research argues against an immutable progression of increasing fibrosis and fatty infiltration following a rotator cuff tear. Inhibition of TGF-β signaling by the small molecule inhibitor SB431542 reduced fibrosis and fatty infiltration in a mouse model when administered daily as an intraperitoneal injection following tendon and nerve transection. 118 Statins, likely through their effects on inflammation, 126 reduced collagen accumulation and preserved muscle fiber contractility when provided orally in a rat model of a massive rotator cuff tear. 127 Similarly, intramuscular injection of an anabolic steroid (nandrolone decanoate) immediately following tendon release in a rabbit 128 and sheep 129 model mitigated fatty infiltration over 6 or 16 weeks, respectively. However, treatment with steroids for 6 weeks subsequent to surgical repair in the sheep model, after 16 weeks of degeneration without steroids, could not reverse the fatty infiltration that previously accumulated. 129 These findings are consistent with clinical reports that surgical repair of rotator cuff tears may halt, but not reverse, degenerative changes in the muscles.1,86 As such, there may be limited clinical utility of any approach that requires administration at the time of initial injury given the insidious nature of most rotator cuff tears, where slow degenerative changes progress in the context of an asymptomatic, but propagating, tendon tear.
On the other hand, continuous traction by a transcutaneous device in a sheep model was shown to gradually return a chronically torn tendon to its anatomical footprint, thereby restoring normal muscle architecture, partially reversing muscle atrophy, and arresting the progression of fatty infiltration.130,131 While promising, a transcutaneous device would present numerous clinical challenges, most notably a risk for infection. However, more recent studies employing pharmaceutical and cell-based therapies suggest reversal of muscle degeneration may be possible. Both inhibition of cyclooxygenase enzymes 132 and intramuscular injection of mesenchymal stem cells (MSCs)133,134 were found to reduce muscle fibrosis and lipid accumulation when administered following surgical repair of chronic rotator cuff tears. Additional benefit may also be possible by combining these strategies with interventions to prevent acute myofibril damage during repair. In particular, repair tension disrupts the myofibril membrane, 135 with resulting disruption in Ca+2 handling and deficits in specific force. 136 Damage may be mitigated by controlling repair tension 137 or inclusion of membrane-stabilizing compounds.136,138 The extent to which these various strategies can be combined synergistically is unknown. For an expanded discussion on muscle biology and therapeutic interventions to reverse muscle degeneration associated with chronic rotator cuff tears, see the excellent recent review. 139 Although efforts to reverse muscle degeneration are relatively new, their success will likely be required to optimize strategies intended to regenerate the structure and function of the tendon–bone interface at which most rotator cuff tears occur, given the known importance of in utero muscle contractions in enthesis development.
Regeneration of Native Enthesis Structure
The tendon–bone interface (i.e., enthesis) of the rotator cuff is a complex structure traditionally conceptualized as four distinct zones: (1) tendon, (2) uncalcified fibrocartilage, (3) calcified fibrocartilage, and (4) bone.140,141 Recent studies have demonstrated a more gradual transition across the interface, rather than discrete regions. It is this graded transition in mineral content,142,143 collagen fiber orientation,142,144 and biochemical composition,145,146 which minimizes the stress concentrations inherent in bi-material interfaces. 147 The complex structure of the native enthesis is not restored following injury, even if surgical repair is performed.15,16 The resulting stress concentration following innate healing is thought to contribute to the high re-tear rate of rotator cuff repair. Furthermore, augmentation of surgical repairs with overlying scaffolds has not been shown to recapitulate the native enthesis structure. 148 Composite scaffolds have been engineered with gradual or discrete transitions in fiber architecture, mineral content, biochemical composition, and cell phenotype.149–152 In vitro characterization of the composite scaffolds has shown region-specific differences in the target parameters, yet no study has explored the utility of these scaffolds when applied in vivo. Future studies must also consider how these composite scaffolds will be applied surgically 153 and scaled anatomically, given the technical constraints of arthroscopic approaches and the small size of the native enthesis (i.e., ≤1 mm from tendon to bone).
An alternative strategy to restore the structure and function of the healing enthesis is to identify, and subsequently manipulate, the biological mediators that inhibit regeneration. The intra-articular environment, in which tissues are surrounded by synovial fluid, is particularly inhospitable to tendon-bone healing.154–156 Although in the nascent stages, the spatiotemporal patterns of the molecular mediators involved in intrinsic enthesis healing have begun to be identified, at least in rodent models.157,158 Following surgical repair of an acutely transected supraspinatus tendon in a rat model, a wound healing response resulted in a histologically unorganized and mechanically inferior insertion site, even at the longest time point (56 days). 159 As scarless healing in embryonic tendons has been at least partially attributed to differences in TGF-β isoforms across the age of an organism—TGF-β3 predominates in in utero healing while TGF-β1 is principally expressed in the mature animal—it was hypothesized that an artificial predominance of TGF-β3 in the healing enthesis of a mature animal would promote better regeneration. 160 While neutralization of TGF-β signaling compromised healing, neither isoform preferential enhanced the mechanical properties of the repair when applied exogenously through an osmotic pump. 160 Overall, augmentation of the healing insertion site with growth factors,161,162 bone adhesives,163,164 or anti-inflammatory agents,165–167 has yielded equivocal results; structural changes, based upon histology, do not consistently correspond to changes in mechanical properties. These findings are reviewed in greater detail elsewhere. 168
Concurrent studies have explored the utility of augmenting rotator cuff repairs with cells, most commonly employing adult tissue-derived MSCs. A reduced number of MSCs at the enthesis were found in patients with symptomatic rotator cuff tears, 169 suggesting potential benefit of exogenous MSC supplementation. Indeed, a recent cohort study found improved healing rates and tissue quality up to 10 years following repair of small- to medium-sized tears (i.e., 1.5–3.5 cm) augmented with autologous MSCs (Table 1). 170 On the other hand, the more extensive body of preclinical studies examining the efficacy of MSC supplementation of rotator cuff repairs contains mixed results. 171 Several investigations have reported benefit172–174 while others found no effect of cell augmentation, whether exogenously delivered175,176 or endogenously recruited.177,178 At present, it is unknown what factors contribute to the inconsistent effects of MSCs, but likely include differences in animal models, experimental design, delivery vehicle, MSC concentration, and MSC phenotype, which may be further modulated by concomitant inclusion of growth factors or viral gene transduction constructs.171,179,180 For instance, augmentation with MSCs overexpressing tenogenic growth factor bone morphogenetic protein-13 (BMP-13) did not improve rotator cuff healing over MSCs alone, 176 while MSCs overexpressing Scleraxis (Scx), a transcription factor associated with tenogenesis, did enhance histological and mechanical properties as compared to untransduced MSCs. 181 Of interest, Scx is required for the formation of a functional enthesis in development, whereas the role of BMP-13 remains uncertain.182–184
As regeneration recapitulates development, elucidating the mechanisms of enthesis formation will likely prove essential in guiding interventions to restore rotator cuff structure and function following injury.185,186 Recent work has begun to unravel the complex spatiotemporal expression patterns of numerous molecular mediators governing enthesis formation.145,187–190 Instrumental to the maturation of the nascent enthesis is the presence of postnatal mechanical loading provided through spontaneous muscle activity.191–193 Botulinum toxin-induced paralysis of the supraspinatus muscle immediately after birth in a mouse model delayed fibrocartilage formation and decreased bone mineralization, 193 resulting in sustained deficits in strength, modulus, and toughness. 192 In parallel studies, it was shown that ablation of hedgehog (Hh) signaling in progenitor cells that constitute the primordial enthesis results in loss of mineralized fibrocartilage with corresponding reductions in mechanical properties (Fig. 2A–D).194–196 Given the known roles of Hh signaling in endochondral ossification197,198 and mechanotransduction,199,200 it was hypothesized that mechanical loading in the early postnatal period drives enthesis formation by modulating Hh activity in the enthesis fibrocartilage cells.201,202 Indeed, botox-mediated muscle paralysis in the first week of postnatal development actually increased the number of Hh-responsive cells due to compensatory feedback. 202 On the other hand, ablation of these Hh-responsive cells resulted in a loss of mineralized fibrocartilage, with little remodeling up to 5 weeks later. 202 Taken together, these studies demonstrate that mechanical loading, through active muscle contractions, drive enthesis maturation by modulating Hh signaling in fibrocartilage cells.
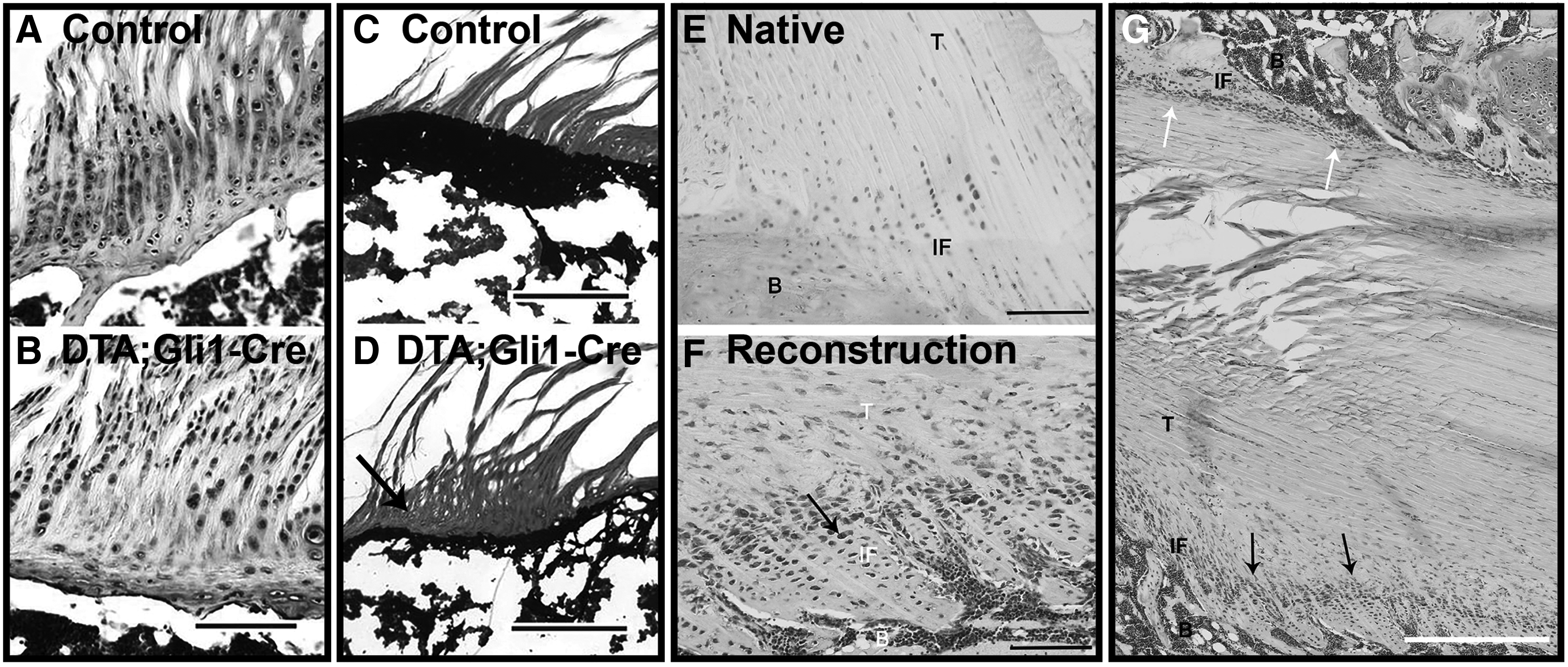
The role of hedgehog signaling in enthesis formation and healing. Parallel columns of fibrochondrocytes are embedded in a proteoglycan-rich extracellular matrix
The extent to which failed regeneration of enthesis following injury is attributable to aberrant mechanical loading or dysregulated Hh signaling in reparative cells remains unknown. However, positive Hh immunohistochemical staining was recently observed at the graft–bone tunnel interface at 3 and 6 weeks following anterior cruciate ligament (ACL) reconstruction in a rat model (Fig. 2E, F). 203 Interestingly, animals that received pretensioned tendon grafts showed increased staining area and intensity, suggesting an influence of mechanical stress on Hh signaling during tendon-bone healing. 203 As Indian Hedgehog (Ihh) and parathyroid hormone (PTH)-related peptide (PTHrP) are reciprocal mediators of a feedback loop controlling chondrogenesis and mineralization at the growth plate204,205 and enthesis,189,201 it was hypothesized that the subcutaneous supplementation of the related PTH might improve enthesis healing in rat model of acute supraspinatus transection and repair. 206 Although treatment with PTH increased bone and mineralized fibrocartilage formation and improved collagen fiber organization, this did not correspond to improved mechanical properties, 206 further demonstrating the complex interaction of soluble factors and mechanical stimuli in directing the emergence of enthesis structure and function.
Mechanical Loading in the Context of Tissue Engineering
Given the fundamental role of mechanical loading in rotator cuff development and homeostasis, investigation of its influence on healing naturally follows. To that end, it has been shown, principally through animal models, that the complete removal of load postoperatively is detrimental to rotator cuff healing 207 but premature loading risks surgical failure or tendon lengthening. As a result, controlled mobilization is advocated but its operationalization remains a challenge. 208 The early wound callus is mechanically weak with increased cellular content, including both progenitor cells and a time-specific predominance of a particular phenotype of inflammatory cell.209,210 As most rotator cuff repairs fail within the first 3–6 months,24–26 it had been hypothesized that botox-mediated unloading could transiently protect the repair site from damaging muscular forces, ultimately resulting in enhanced tissue structure and strength. 211
When applied in a rat model, botox-treated specimens showed accelerated formation of a normal tidemark and increased collagen fiber organization, but negligible or inferior mechanical properties and bone morphometry at weeks 4, 8, and 24. 212 Similar detriments were found in a rabbit model of chronic rotator cuff tears. 213 In a related study, an external fixator was applied to the tibiae and femurs of rats that underwent ACL reconstruction, eliminating tissue strain with the exception of 50 cycles of 2% strain applied daily and commenced (1) immediately postoperatively, (2) on postoperative day 4, (3) postoperative day 10, or (4) never (i.e., complete immobilization). 214 Specimens from the delayed immobilization group (i.e., postoperative day 10) demonstrated superior mechanical and histological properties along with greater bone formation when compared against the other loading conditions. 214 Similarly, immediate postoperative passive motion was detrimental to shoulder mechanics in a rat model of rotator cuff repair. 215 Lastly, scapular dyskinesis, as induced through transection of the accessory and long thoracic nerves, decreased mechanical properties, altered histology, and diminished tendon organization at the enthesis following rotator cuff repair. 216 Taken together, these studies validate the importance of controlled mobilization postoperatively as a means to optimize healing. In the clinical setting, where the practical postoperative loading protocols have been far more constrained than those investigated in animal studies, there is no long-term difference between early mobilization compared to delayed rehabilitation.217–219 However, there is growing evidence that in vivo mechanical loads can and should be considered if the promise of tissue engineering strategies for improved rotator cuff healing is to be realized.
In a seminal study, the influence of in vivo loading on a braided porcine SIS graft used to replace the rabbit Achilles tendon was examined. 220 After a 2-week immobilization period, unrestricted motion and weight bearing during the early remodeling phase accelerated tendon remodeling, as compared to totally immobilized joints. 220 In related work, acellular dermal matrix patches were used to reconstruct the rotator cuff in a rat model, with variable periods of immobilization to follow. Two weeks of immobilization yielded superior collagen organization and mechanical strength compared to no immobilization or 6 weeks of immobilization.221,222 Beyond scaffolds, the importance of in vivo loading also extends to the application of growth factors and cells. Injection of cartilage-derived morphogenetic protein 2 (CDMP-2) into unloaded rat tendons produced heterotopic bone formation, which was greatly reduced in loaded tendons. 223 Likewise, muscle-derived stem cells (MDSCs) formed more myofibrils and reduced fibrosis when injected into injured muscle of mice exposed to daily treadmill running, as compared to littermates that only engaged in normal cage activity. 224
Though limited, these studies suggest that the utility of many tissue engineering strategies will be influenced by the mechanical microenvironment of the injured tissue to which they are applied. With particular regard to efforts to enhance rotator cuff healing, it is important to consider all the elements that comprise the rotator cuff organ and the possibility of synergistic interactions of biological therapies heretofore applied to an individual element. For instance, a bioactive scaffold sheet that can offload the surgical repair may serve to reverse the degenerative changes in the tendinopathic tendon while also allowing earlier joint mobilization with the resulting strains at the healing enthesis providing mechanotransductive cues to exogenous Hh-responsive MSCs, thereby recapitulating the developmental signals essential for the formation of a mineralized fibrocartilage interface. These combinatorial approaches have yet to be systematically investigated, but may offer novel approaches to addressing the otherwise recalcitrant challenge that is the chronic rotator cuff tear. In a recent clinical study, arthroscopic repairs of massive rotator cuff tears that were augmented with both bone marrow stimulation and patch augmentation resulted in a significantly lower re-tear rate than conventional repairs. 225 Although the study design limits conclusions about any additive benefit of bone marrow stimulation and scaffold augmentation, the results were encouraging.
Present Challenges and Future Perspectives
Despite a dramatic increase in research on rotator cuff repair over the past two decades, there is little evidence that clinical outcomes of rotator cuff repair have improved. 226 However, poor outcomes are disproportionately attributable to chronic massive tears, which remain a persistent challenge. 227 Increasingly sophisticated tissue engineering strategies may provide orthopedic surgeons with the capacity to restore the structure and function of the rotator cuff, which has traditionally been considered to possess a limited intrinsic healing capacity. In this review, we have highlighted the concept of the rotator cuff as an organ, for the various tissues that comprise it each exhibit degenerative changes in the context of a chronic tear. It is therefore posited that tissue engineering strategies aimed at regenerating one element might provide synergistic benefits when combined. Investigation of this hypothesis in animal studies is necessary, as are studies examining how mechanical loading of augmented repairs might provide mechanotransductive cues capable of promoting tissue-specific cell differentiation and favorable tissue remodeling.
The judicious application of loading protocols could be enhanced by further characterization of in vivo forces in both healthy and healing tissues228,229 and the use of these results as design parameters for novel biomaterials and computational models of rotator cuff mechanics.230–232 For instance, recent work has begun to elucidate how tear size and location affect tear propagation when tissues are cyclically loaded with forces likely experienced in postoperative rehabilitation.233,234 Parallel in vivo investigations have explored how conservative therapy (i.e., physical therapy) 2 and surgical stabilization 235 affect glenohumeral kinematics in patients. In combining these results, models may be developed that are predictive of the in vivo stresses experienced by a healing tissue and possibly prescriptive for the exercise protocols that constitute a rehabilitation program at a given time after surgery. 236 In the future, it may be possible to combine these emerging regenerative rehabilitation approaches with tissue engineering strategies to more consistently restore tissue structure and function at an accelerated pace without sacrificing safety.
The successful translation of tissue engineering strategies into clinical practice will also require continued refinement of animal models, such that the pathogenesis in the model organism more closely recapitulates that of human patients, notwithstanding insurmountable differences in anatomy and biology across species. With regards to rotator cuff pathology, increased consideration has been given to the effect of tear chronicity and aging on the healing potential of the injured shoulder. 179 By their very nature, chronic rotator cuff tears are most commonly seen in the context of increased age, which itself is correlated with poor postoperative rotator cuff integrity. 237 Until recently, most investigations of the potential benefit of tissue engineering strategies in enhancing rotator cuff healing were performed in young, healthy animals in which the tendon was acutely transected and immediately repaired with or without augmentation. Novel animal models of chronic degeneration have now been reported in mice,238,239 rats,75,103 and sheep,130,240 with associated impairment in healing potential.74,75 These animal models may be more predictive of the utility of a particular tissue engineering strategy when applied to patients. For instance, no benefit to augmenting repairs with a fascia lata autograft patch was found in patients with high-grade fatty infiltration of their muscles. 77 Preclinical models employing aged animals may also be of value, as older animals also experience age-associated exacerbation in muscle stiffness 241 and fatty infiltration 116 in addition to reduced healing capacity. 242
Conclusions
This review highlights the three principal aims toward which tissue engineering strategies have been applied in an effort to improve rotator cuff healing: (1) immediate mechanical augmentation of the surgical repair, (2) restoration of muscle quality and contractility, and (3) regeneration of native enthesis structure. Given the seamless integration of multiple tissues comprising the rotator cuff, and their concurrent degeneration in the context of chronic massive tears, it is instructive to consider the concept of the rotator cuff as an organ. In doing so, it is posited that combining the individual approaches to address the three principal aims may offer synergistic benefit. At the same time, it must be emphasized that the application of a tissue engineering strategy to any given tissue of the rotator cuff organ must likely be temporally discrete and spatially confined, as signaling pathways of putative benefit in one tissue may be detrimental in adjacent tissues. For instance, TGF-β-mediated upregulation of the tenogenic transcription factor Scx may reverse degenerative changes in the tendon midsubstance or enhance enthesis healing but could also exacerbate muscle atrophy and fibrosis if TGF-β delivery is inadequately localized. 243 Much work remains to validate this approach and will invariably require strong collaboration among engineers, biologists, and clinicians to bring the promise of tissue engineering and regenerative medicine to come to fruition in treating massive chronic rotator cuff tears.
Footnotes
Acknowledgments
This work was supported in part by the University of Pittsburgh Physicians Academic Foundation, the NIH (NIH R01 AR062947, and CATER Training Grant, 5T32 EB001026), and the U.S. Department of Defense (W81XWH-15-1-0104).
Disclosure Statement
No competing financial interests exist.